Embed Size (px)
Citation preview

Review
Sonography of Neck Lymph Nodes.Part I: Normal Lymph Nodes
M. YING*, A. AHUJA†
*Department of Optometry and Radiography, The Hong Kong Polytechnic University, Hung Hom, Kowloon, HongKong SAR, People’s Republic of China and †Department of Diagnostic Radiology and Organ Imaging, Prince of
Wales Hospital, Shatin, New Territories, Hong Kong SAR, People’s Republic of China
Received: 16 July 2002 Revised: 13 November 2002 Accepted: 20 November 2002
Grey scale and power Doppler sonography play an important role in assessment of cervicallymphadenopathy. However, before examination of pathological nodes, a clear understanding of theanatomy of cervical nodes, scanning technique and sonographic appearances of normal cervicalnodes is essential. This article reviews these topics in order to provide a baseline for sonographicexamination of cervical lymphadenopathy. Ying, M., Ahuja, A. (2003). Clinical Radiology 58: 351–358.
q 2003 The Royal College of Radiologists. Published by Elsevier Science Ltd. All rights reserved.
Key words: ultrasound, cervical lymph nodes, normal.
INTRODUCTION
Assessment of cervical lymph nodes is important for
patients with head and neck carcinomas, and is useful in
determining patient prognosis, and in selecting treatment
[1–5]. High-resolution sonography has been commonly used
to evaluate cervical lymphadenopathy and the role of grey-
scale sonography in the assessment of cervical lymph nodes is
well established [4–8]. With the advent of power Doppler
sonography (PDS), the distribution of intranodal vessels and
perfusion of the cervical nodes can be evaluated, and the blood-
flow velocity and vascular resistance of the intranodal vessels
can also be measured [9–13]. Grey-scale ultrasound has a high
sensitivity (97%), and a high specificity (93%) when used in
conjunction with ultrasound-guided fine-needle aspiration
cytology (FNAC) [2]. It has also been reported that ultra-
sound-guided FNAC is more accurate than the conventional or
blinded FNAC in differentiating metastatic and non-metastatic
cervical nodes, with fewer false-negative (1 and 8%, respect-
ively) and false-positive (1 and 5%, respectively) findings [14].
Familiarity with lymphatics is essential for examination of
the head and neck. For the beginner, ultrasound evaluation ofneck nodes may be a daunting prospect because there areapproximately 800 lymph nodes in the body and 300 of themare in the neck. The nodes vary in size from 3 to 25 mm, areembedded within the soft tissues of the neck either partly orcompletely surrounded by fat. However, most of the neck nodesare quite superficial in location and are readily identified byhigh-resolution ultrasound, and despite the complicatedanatomy of the neck, the location, distribution and drainingareas of these nodes is fairly constant. Therefore if theradiologist is familiar with the anatomy and the sonographicappearances of these nodes, assessing them is not as difficult asit first seems.
NORMAL ANATOMY
Cervical lymph nodes are solitary structures composed oflymphoid tissue and are distributed along the course oflymphatic vessels in the neck. Each is divided into two mainregions, the cortex and the medulla. The cortex is composed ofdensely packed lymphocytes, which group together to formspherical lymphoid follicles. The intermediate area between thecortex and the medulla is known as the paracortex, and is atransitional area for lymphocyte migration [15–17]. Themedulla of the lymph node is composed of medullarytrabeculae, medullary cords, and medullary sinuses. The
0009-9260/03/$30.00/0 q 2003 The Royal College of Radiologists. Published by Elsevier Science Ltd. All rights reserved.
Guarantors of study: Dr M. Ying and Dr A. Ahuja.Author for correspondence: Dr Anil Ahuja, Department of DiagnosticRadiology and Organ Imaging, Prince of Wales Hospital, Shatin, NewTerritories, Hong Kong SAR, People’s Republic of China. Tel: þ852-2632-2290; Fax: þ852-2636-0012; E-mail: [email protected]
Clinical Radiology (2003) 58: 351–358doi:10.1016/S0009-9260(02)00584-6, available online at www.sciencedirect.com

medullary trabeculae have a similar composition to the capsule,whereas the structural base for the medullary cords andmedullary sinuses is the reticular tissue, which is composedof reticulum cells. As medullary trabeculae are composed ofdense connective tissue, similar to the capsule, and have a well-established network branching from the capsule, they provideguidance for blood vessels and nerves to other regions of thelymph node. The medullary cords are arranged in a parallelpattern and contain numerous lymphoid cells, mainly plasmacells and small lymphocytes. The medullary sinuses are filledwith lymph and are part of the sinus system of the lymph node[15–17].
Similar to the lymph nodes in other body regions,cervical lymph nodes are permeated by blood vessels. Themain artery enters the lymph node at the hilus, where itbranches into several smaller arteries and arterioles. In thecortex, arterioles further branch off into several sinuouscapillaries and supply the lymphoid follicles, as well as thelymphocytes. Some of the arterioles reach the capsule viatrabeculae of the lymph node and then anastomose withother branches [16–18].
The venous system consists of venules, small veins and amain vein, which have a similar route to the hilus as thearterial system. In the cortex, the venules converge to formsmall veins. In the medulla, the small veins further convergeto form the main vein, which leaves the lymph node at thehilus [16–18].
CLASSIFICATION OF LYMPH NODES
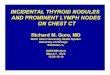
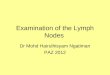
The cervical lymph nodes used to be classified intogroups according to their location in the neck (Table 1).However, due to the complexity and difficulty of thisclassification, the American Joint Committee on Cancer(AJCC) classification is now commonly used, especially bysurgeons and oncologists. The AJCC classification dividedpalpable cervical lymph nodes into seven levels, or groups,which are based on the extent and level of cervical nodalinvolvement by metastatic tumour (Fig. 1) [19–21].
Although the AJCC classification is now commonly usedin identifying the location of lymph nodes, some importantnodes, such as the parotid and retropharyngeal nodes, arenot incorporated into this classification [21]. As the AJCCclassification is not limited to ultrasound but is also used incomputed tomography (CT) and magnetic resonance ima-ging (MRI), some of the lymph nodes included in thisclassification system may not be accessible by ultrasound,such as the prelaryngeal, paratracheal and upper mediastinalnodes.
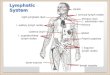
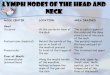
Another classification of lymph nodes, which is also basedon the location of the lymph nodes was established by Hajeket al. [22] to simplify ultrasound examination of the neck. Thelymph node regions are classified into eight regions accordingto the location in the neck (Fig. 2). One must note, that thisclassification is merely to simplify the sonographic examin-ation of the neck. It is designed to ensure that a radiologistexamines all areas in the neck in a systematic way in order notto miss a lesion. It does not reflect the staging of cancers whichis based on the AJCC classification.
EQUIPMENT AND SCANNING TECHNIQUE
A 7.5 MHz linear transducer is the basic requirement forultrasound examination of the neck. Higher frequency
Fig. 1 – Schematic diagram of the neck showing the AJCC classification ofcervical lymph nodes. Level I nodes are submental and submandibularnodes; level II nodes are upper internal jugular chain nodes; level III nodesare middle internal jugular chain nodes; level IV nodes are lower internaljugular chain nodes; level V nodes are spinal accessory chain nodes andtransverse cervical chain nodes; level VI nodes are anterior cervical nodes;level VII nodes are upper mediastinal nodes.
Fig. 2 – Schematic diagram of the neck showing the classification of thecervical lymph nodes to facilitate the evaluation of nodal distribution withultrasound. 1 Submental, 2 submandibular, 3 parotid, 4 upper cervical(above the level of hyoid bone), 5 middle cervical (between the level ofhyoid bone and cricoid cartilage), 6 lower cervical (below the level ofcricoid cartilage), 7 supraclavicular fossa, 8 posterior triangle.
CLINICAL RADIOLOGY352

Table 1 – Classification of cervical lymph nodes according to their location in the neck
Nodal groups Locations Number of nodes Drainage areas Efferent pathways
Submental Submental triangle 1 to 8 Chin Submandibular nodesMiddle part of lower lipCheeksAnterior gingivaFloor of mouthLower incisorsTip of the tongue
Submandibular Submandibular triangle 3 to 6 Lateral chin Internal jugular chain nodesUpper lipLower lip (except medial part)CheeksNoseAnterior nasal cavityGumsTeeth except lower incisorsPalateMedial part of the eyelidsFloor of mouthSubmandibular and sublingual sali-vary glands
Parotid Extra-parotid: pre-auricular Extra-parotid: 3 to 4 Skin of the head and neck Internal jugular chain nodesSubcapsular: pre-auricular and within the tailof the parotid gland
Subcapsular: pre-auricular, 1 to 2;parotid tail, 3 to 4
Parotid glands
Intra-glandular: within the superficial lobeand the fascia between the superficial anddeep lobes
Intra-glandular: 3 to 4 Forehead and temporal region
Middle and lateral part of the faceAuricleExternal auditory canalEustachian tubePosterior cheekBuccal mucous membraneGums
Internal jugular chain Along the course of the internal jugular veinand adjacent to the carotid sheath
15 to 40 Submandibular, parotid and retro-pharyngeal nodes
Right side: right lymphatic duct,subclavian vein, internal jugular vein
Tonsil Left side: thoracic duct, subclavianvein, internal jugular vein
PharynxLarynxOesophagusThyroid glands
Supraclavicular chain (transversecervical chain)
Above the clavicle and along the course ofthe transverse cervical vessels
1 to 10 Internal jugular nodes Right side: right lymphatic duct,subclavian vein, internal jugular vein
Posterior triangle nodes Left side: thoracic duct, subclavianvein, internal jugular vein
Infraclavicular areasSkin of the anterolateral part of theneck
(continued on next page)
TH
ES
ON
OG
RA
PH
YO
FN
EC
KL
YM
PH
NO
DE
S.
PA
RT
I:N
OR
MA
LL
YM
PH
NO
DE
S3
53

Table 1 (continued)
Nodal groups Locations Number of nodes Drainage areas Efferent pathways
Posterior triangle chain (spinal acces-sory chain)
Along the course of the spinal accessorynerve and in the posterior triangle of the neck
4 to 20 Parotid region Supraclavicular chain and internaljugular chain
Occipital regionLateral part of the neckShoulder
Anterior cervical Pre-tracheal chain: along the course of theanterior jugular vein and anterior to the strapmuscles
7 to 20 Pre-tracheal chain: skin and musclesof the anterior neck
Right side: thoracic duct, anteriormediastinal node
Pre-laryngeal chain: midline in location andanterior to the cricothyroid membrane
Pre-laryngeal chain: mainly the lar-ynx
Left side: lowest internal jugularchain node, highest intrathoracicnode
Para-tracheal chain: lateral to the trachea andposterior to the thyroid in the tracheoeso-phageal groove
Para-tracheal chain: supraglottic andsubglottic larynx, pyriform sinus,thyroid, trachea and esophagus
Occipital Apex of the posterior triangle, between theoccipital bone, sternomastoid and trapezius
3 to 10 Occipital region Posterior triangle chain
Mastoid Behind the ear and near the mastoid process 1 to 4 Parotid region Parotid nodesParietal area of the vault Upper internal jugular chain nodesAuricleExternal auditory meatus
Facial Subcutaneous tissues of the face 5 to 10 Eyelids Submandibular nodesCheekMiddle portion of face
Sublingual Between the genioglossus muscles and alongthe anterior lingual vessels
Uncertain Tongue Submental nodes
Floor of the mouth Submandibular nodesInternal jugular chain nodes
Retropharyngeal Retropharyngeal space 2 to 5 Nasopharynx Upper internal jugular chain nodesOropharynx
CL
INIC
AL
RA
DIO
LO
GY
35
4

transducer, i.e. 10 MHz or above, allows better resolution forsuperficial structures but there is a trade-off with a lack ofpenetration. A 5 MHz convex transducer is sometimes usefulfor the assessment of deep lesions, whereas the use of a standoffgel block may allow better visualization of large or superficialmass. Colour Doppler applications are now standard on mostultrasound machines, and beginners may find it useful foridentifying vascular structures. However, there will be lessdependence once they are familiar with the sonographicanatomy. PDS is desirable for the assessment of vasculaturein small structures, such as lymph nodes and thyroid. Whenusing PDS, the Doppler setting should be optimized fordetecting small vessels, i.e.:
† high sensitivity† low wall filter† pulsed repetition frequency (PRF) 700 Hz† medium persistence† the colour gain is first increased to a level which shows
colour noise, and then decreased to the level where thenoise just disappears.
PDS may be difficult for lesions adjacent to major artery andin uncooperative patients. It is because evaluation of vascularpattern of the lymph nodes is difficult when there is flashartefact due to movement of the lesions. Deep nodes in obesepatients’ necks are also difficult to be evaluated with PDS.
In measuring the vascular resistance (resistive index, RI;pulsatility index, PI), the more prominent vessels are usuallyselected. Measurements are obtained from the average of threeconsecutive Doppler spectral waveforms in order to get a moreaccurate value. The smallest sample volume should be chosen.If blood flow velocity (peak systolic velocity, PSV and enddiastolic velocity, EDV) is measured, angle correction shouldbe made at an angle of 608 or less.
An adjustable and mobile examination table is essential inultrasound of the neck, which allows easy positioning so thatthe patient’s neck is at the level of the ultrasound monitor andwithin the scanning range of the operators.
The patient should be positioned supine with the neckhyper-extended. A pillow or triangular soft pad should beplaced under the shoulders and lower neck for support. Theexamination is started with a transverse scan of the submentalarea. The transducer is then swept laterally to one side of theneck while the patient’s head rotates towards the opposite sideto allow free manipulation of the transducer. The submandib-ular region is examined with a transverse scan along the inferiorborder of the mandibular body. The transducer should beangled cranially as some of the submandibular nodes arelocated in the submandibular niche hidden by the mandibularbody. The parotid nodes are assessed with longitudinal andtransverse scans along the ramus of the mandible. The internaljugular chain nodes are examined in transverse scan with thetransducer scans along the internal jugular vein and commoncarotid artery from the tail of parotid gland to the junctionbetween internal jugular vein and the subclavian vein. Theinternal jugular chain nodes can be divided into three groups:upper cervical (above the level of hyoid bone), middle cervical(between the level of hyoid bone and cricoid cartilage) andlower cervical (below the level of cricoid cartilage). From the
lower cervical region, the transducer is then swept laterally tothe supraclavicular fossa and the supraclavicular nodes areassessed with transverse scan. The posterior triangle nodes areexamined with transverse scans from the mastoid and along theimaginary line of the spinal accessory nerve, which is betweenthe sternomastoid and the trapezius. The same scanningprotocol is used on the opposite side of the neck so that themajor nodal chains in the neck are covered.
The monitor should be positioned for comfortable viewingwhen performing a FNAC biopsy. A monitor with a moveablearm is ideal. The patient’s neck should be close enough to theoperator so that both the hand holding the transducer and thehand holding the needle or biopsy gun are relaxed.
SONOGRAPHIC APPEARANCES OF NORMALCERVICAL NODES
Number and Distribution
Normal cervical lymph nodes are detectable with ultrasoundin healthy people. At least five or six normal cervical nodes areidentified routinely by sonography [8,23], and there is nosignificant racial [23] or sexual [24] difference in the averagenumber of normal cervical lymph nodes. The number ofcervical lymph nodes that can be detected by ultrasounddecreases with advancing age [24]. Among the different regionsof the neck, normal cervical lymph nodes are commonly foundin submandibular (19–23%), parotid (15–16%), upper cervical(18–19%) regions and posterior triangle (35–37%) [23–25].Therefore, patients with multiple lymph nodes in other regionsshould raise the suspicion of pathology.
Size
The size of normal cervical lymph nodes varies with thelocation in the various regions of the neck, age and sex. Lymphnodes in the upper neck, including submandibular and uppercervical nodes, tend to be larger than the lymph nodes in otherregions [8,26–29]. This may be because inflammation in the
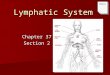
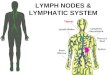
Fig. 3 – Grey scale sonogram showing an oval, hypoechoic normal cervicallymph node (arrows). Note the echogenic hilus (arrowheads) continuouswith the adjacent fat.
THE SONOGRAPHY OF NECK LYMPH NODES. PART I: NORMAL LYMPH NODES 355

oral cavity predisposes to the development of reactivehyperplasia in the upper neck nodes.
Normal cervical nodes in younger subjects (aged 20–39years) tend to be smaller than those in older subjects (aged $40years) [24]. This is explained by the increase in intranodal fattyinfiltration with age [30]. Fatty infiltration also makes thelymph nodes, especially those that are small, difficult todifferentiate from the surrounding soft tissue [24].
The upper limit of the maximal short axis axial diameter fornormal cervical nodes is controversial with two values beingconsidered: 5 and 8 mm. Hajek et al. [22] and Solbiati et al.[31] suggested that the normal upper limit of the maximal shortaxis axial diameter of the cervical lymph node is 5 mm.However, Bruneton et al. [29] and Ying et al. [8] reported thatnormal cervical lymph nodes have a maximal short axis axialdiameter of 8 mm or less. A maximal short axis axial diameterof 8 mm is preferred as the normal upper limit as it gives ahigher specificity than a maximal short axis axial diameter of5 mm. However, one should note that a higher cut-off alsoresults in a lowered sensitivity.
Shape
Shape has been suggested to be a useful criterion indistinguishing normal from malignant nodes. The shape oflymph nodes is usually assessed by the S:L ratio. A lymph nodewith an S:L ratio less than 0.5 is oval in shape, whereas an S:Lratio greater than or equal to 0.5 indicates round node [7,8,31,32,33]. An oval node indicates normality (Fig. 3), whereasmalignant nodes tend to be round [4,5,7,31,32,34]. However,
the normal submandibular and parotid nodes are usually round,S:L $ 0.5 (95 and 59%, respectively) [8]. Although, 0.5 iscommonly used as the cut-off value in differentiating normaland abnormal nodes [4,5,31,32], it has been reported that theoptimum cut-off value of S:L ratio is different in differentregions of the neck (Table 2) [35]. Also, when the optimum S:Lratio and maximum transverse diameter of the lymph nodes arecombined, different optimum cut-off values of the maximumtransverse diameter were found in different regions of the neck(Table 2) [35]. The shape of normal cervical nodes varies invarious regions of the neck [8], but not with the age and sex[24].
Echogenic Hilus
An echogenic hilus is a normal sonographic feature of mostnormal cervical lymph nodes (75–100%) [8], but is morecommonly seen in larger nodes than in smaller nodes (Fig. 3).This is because limited branching and separation of walls of thelymphatic sinuses and blood vessels in smaller nodes do notprovide enough interfaces to reflect the ultrasound waves tomake the hilus echogenic [36]. About 90% of normal cervicallymph nodes with maximum transverse diameter greater than5 mm showed an echogenic hilus [36].
The echogenic hilus was previously considered to beintranodal fatty tissue [30,34]. Solbiati et al. [31] subsequentlynoted that the echogenic hilus consisted of sinuses, smallintranodal arteries and veins, and fatty tissue. Rubaltelli et al.[37] suggested that the echogenic pattern of the nodal hilusmainly corresponds to the presence of lymphatic sinuses, and
Table 2 – Performance of optimum short axis and optimum S:L ratio in different regions of the neck
Regions Optimum short axis when combined with the optimum S:L ratio Sensitivity (%) Specificity (%) PPV (%) NPV (%) Accuracy (%)
Submental 3 mm (0.5) 93 76 76 93 84Submandibular 8 mm (0.7) 22 86 42 70 66Parotid 5 mm (0.5) 67 98 89 91 91Upper cervical 4 mm (0.4) 82 79 81 80 80Middle cervical 3 mm (0.3) 78 91 95 63 82Posterior triangle 3 mm (0.4) 76 89 92 69 81
S:L, short axis to long axis ratio.
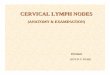
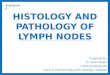
Fig. 4 – Power Doppler sonogram of a normal cervical lymph nodeshowing central hilar vascularity (arrows).
Fig. 5 – Power Doppler sonogram showing a normal cervical node withoutany vascular signal (arrows), i.e. apparently avascular.
CLINICAL RADIOLOGY356

fatty tissue makes the echogenic nodal hilus more obvious butis not essential for its visualization. This was further proven byVassallo et al. [4,5] who reported that the echogenic hiluscorresponds to the abundance of collecting sinuses, whichprovide acoustic interfaces to reflect a portion of the ultrasonicwave, making the hilus echogenic.
On ultrasound, the nodal hilus is seen to be continuous withthe surrounding fatty tissue [8,38].
In routine clinical practice, radiologists should be aware thatthe absence of the echogenic hilus on grey-scale sonographydoes not imply the absence of hilar vascularity on PDS [39].
There is no racial difference in the incidence of echogenichilus within cervical lymph nodes [23]. The incidence ofvisualizing-echogenic hilus within cervical nodes increasessignificantly with advancing age, but does not vary significantlybetween men and women [24]. The age-related variation of theincidence of echogenic hilus is believed to be due to theincreased fatty deposition in lymph nodes in elderly, whichmakes the nodal hilum more obvious [24,30,36].
Vascular Features
Normal cervical lymph nodes may show hilar vascularity(Fig. 4) or appear avascular (Fig. 5), but none should showperipheral vascularity [25]. Among the different regions of theneck, the parotid and posterior triangle nodes tend to beapparently avascular (52 and 60%, respectively). This isprobably due to the smaller size of the lymph nodes in theseregions, which makes detection of intranodal vasculaturedifficult [25]. The degree of vascularity of submental andsubmandibular nodes is significantly higher than that of otherregional nodes. Submental nodes have a higher RI and PI, inassociation with lower EDV, than other regional nodes,whereas there is no significant difference in PSV betweenlymph nodes in different regions [25].
The incidence of detected vascular signals and blood flowvelocity (PSV and EDV) within normal cervical nodesincreases with the size of the nodes, and about 90% of normalcervical nodes with a maximum transverse diameter greaterthan 5 mm showed hilar vascularity [36]. The increased bloodflow velocity in bigger nodes is probably explained by the factthat the vessels are larger in bigger nodes allowing faster flowof blood [36], which can be readily detected. The RI and PIdoes not vary with the size of lymph nodes.
The degree of vascularity of normal cervical nodes is notrelated to the age or gender [25], but the detection rate ofvascular signals and vascular resistance are significantly higherin elderly. This is thought to be due to the higher stiffness ofvessels in the elderly making the small vessels less compres-sible, and thus blood flow is easily detected [25]. Blood flowvelocity, however, does not vary with age. Blood flow velocityand vascular resistance do not vary between men and women[25].
With the use of spectral Doppler, the blood flow velocity(PSV and EDV) and vascular resistance (RI and PI) of normalcervical nodes can be measured. However, its role in routineclinical practice is very limited.
Ultrasound and ultrasound-guided FNAC are usefulmethods to differentiate metastatic from non-metastatic
cervical nodes [2,14]. Ultrasound-guided FNAC can detectmetastasis in cervical lymph nodes when clinical examination,ultrasound, CT and MRI are negative [40]. Therefore, it hasbeen suggested that ultrasound-guided FNAC should be usedfor patients with or without palpable nodes, and patients with orwithout positive findings in clinical or radiological examin-ations [40–42]. Ultrasound-guided FNAC can monitor theneedle tip which enables sampling from different regions of thesame lymph node so that individual nodes can be assessedcompletely, and thus more accurate results can be obtained.Monitoring of the needle tip using ultrasound guidanceprevents accidental puncture of vital structures such as thecommon carotid artery.
Although ultrasound-guided FNAC is useful in evaluationof cervical lymphadenopathy, it is difficult to collect adequatetissue volume from small lymph nodes (less than 4 mm inmaximal short axis axial diameter) and from post-radiationnodes. It has been reported that 15% of specimens fromultrasound-guide FNA did not provide an accurate diagnosisdue to uncertain diagnosis or inadequate sample [43]. In theneck, FNA is usually difficult in lymph nodes situated in deepsubmandibular area.
REFERENCES
1 Baatenburg de Jong RJ, Rongen RJ, De Jong PC, et al. Screening forlymph nodes in the neck with ultrasound. Clin Otolaryngol, 1988;13:5–9.
2 Baatenburg de Jong RJ, Rongen RJ, Lameris JS, et al. Metastatic neckdisease. Palpation vs ultrasound examination. Arch Otolaryngol HeadNeck Surg, 1989;115:689–690.
3 Ishii JI, Amagasa T, Tachibana T, et al. US and CT evaluation ofcervical lymph node metastasis from oral cancer. J Cranio-Max-FacSurg, 1991;19:123–127.
4 Vassallo P, Wernecke K, Roos N, Peters PE. Differentiation of benignfrom malignant superficial lymphadenopathy: the role of high-resolution US. Radiology, 1992;183:215–220.
5 Vassallo P, Edel G, Roos N, et al. In-vitro high-resolution ultrasono-graphy of benign and malignant lymph nodes. A sonographic–pathologic correlation. Invest Radiol, 1993;28:698–705.
6 van den Brekel MW, Stel HV, Castelijns JA, et al. Cervical lymph nodemetastasis: assessment of radiologic criteria. Radiology, 1990;177:379–384.
7 Ahuja A, Ying M, King W, Metreweli C. A practical approach toultrasound of cervical lymph nodes. J Laryngol Otol, 1997;111:245–256.
8 Ying M, Ahuja A, Brook F, et al. Sonographic appearance anddistribution of normal cervical lymph nodes in a Chinese population.J Ultrasound Med, 1996;15:431–436.
9 Ariji Y, Kimura Y, Hayashi N, et al. Power Doppler sonography ofcervical lymph nodes in patients with head and neck cancer. AJNR Am JNeuroradiol, 1998;19:303–307.
10 Giovagnorio F, Caiazzo R, Avitto A. Evaluation of vascular patterns ofcervical lymph nodes with power Doppler sonography. J ClinUltrasound, 1997;25:71–76.
11 Wu CH, Chang YL, Hsu WC, et al. Usefulness of Doppler spectralanalysis and power Doppler sonography in the differentiation ofcervical lymphadenopathies. AJR Am J Roentgenol, 1998;171:503–509.
12 Wu CH, Hsu MM, Chang YL, Hsieh FJ. Vascular pathology ofmalignant cervical lymphadenopathy: qualitative and quantitativeassessment with power Doppler ultrasound. Cancer, 1998;83:1189–1196.
13 Steinkamp HJ, Mueffelmann M, Bock JC, et al. Differential diagnosisof lymph node lesions: a semiquantitative approach with colourDoppler ultrasound. Br J Radiol, 1998;71:828–833.
THE SONOGRAPHY OF NECK LYMPH NODES. PART I: NORMAL LYMPH NODES 357

14 Baatenburg de Jong RJ, Rongen RJ, Verwoerd CD, et al. Ultrasound-guided fine-needle aspiration biopsy of neck nodes. Arch OtolaryngolHead Neck Surg, 1991;117:402–404.
15 Qizilbash AH, Young JEM, Eds. Lymph nodes. In Guides to ClinicalAspiration Biopsy: Head and Neck. New York: Igaku-Shoin 1988;117–203.
16 Hall FG. The functional anatomy of lymph nodes. In Stansfeld AG,d’Ardenne AJ, eds. Lymph Node Biopsy Interpretation. London:Churchill Livingstone, 1992; 3–28.
17 Castenholz A. Architecture of the lymph node with regard to itsfunction. In Grundmann E, Vollmer E, eds. Reaction Patterns of theLymph Node. Part 1. Cell Types and Functions 1. New York: Springer-Verlag, 1990; 1–32.
18 Papadimitriou CS, Kittas CN. Normal structure and function of lymphnodes. In Pangalis GA, Polliack A, eds. Benign and malignantlymphadenopathies. Chur: Harwood Academic Publishers, 1993;113–130.
19 Vogl TJ, Balzer J, Mack M, Steger W, Eds. Oral cavity, oropharynx,and oral floor. In Differential Diagnosis in Head and Neck Imaging.Stuttgart, New York: Georg Thieme Verlag, 1999; 287–310.
20 Som PM. Lymph nodes. In Som PM, Curtin HD, eds. Head and NeckImaging St Louis: Mosby, 1996; 772–793.
21 Harnsberger HR. Squamous cell carcinoma: nodal staging. In Hand-book of Head and Neck Imaging, 2nd edn St Louis: Mosby, 1995;283–298.
22 Hajek PC, Salomonowitz E, Turk R, et al. Lymph nodes of the neck:evaluation with US. Radiology, 1986;158:739–742.
23 Ying M, Ahuja A, Brook F. Gray scale and power Doppler sonographyof normal cervical lymph nodes: comparison between Chinese andwhite subjects. J Ultrasound Med, 2002;21:59–65.
24 Ying M, Ahuja A, Brook F. Sonographic appearances of cervical lymphnodes: variations by age and sex. J Clin Ultrasound, 2002;30:1–11.
25 Ying M, Ahuja A, Brook F, Metreweli C. Power Doppler sonography ofnormal cervical lymph nodes. J Ultrasound Med, 2000;19:511–517.
26 Som PM. Lymph nodes of the neck. Radiology, 1987;165:593–600.27 DePena CA, Van Tassel P, Lee YY. Lymphoma of the head and neck.
Radiol Clin North Am, 1990;28:723–743.28 Swartz JD, Yussen PS, Popky GL. Imaging of the neck: nodal disease.
Crit Rev Diagn Imaging, 1991;31:413–469.29 Bruneton JN, Balu-Maestro C, Marcy PY, et al. Very high frequency
(13 MHz) ultrasonographic examination of the normal neck: detectionof normal lymph nodes and thyroid nodules. J Ultrasound Med, 1994;13:87–90.
30 Marchal G, Oyen R, Verschakelen J, et al. Sonographic appearance ofnormal lymph nodes. J Ultrasound Med, 1985;4:417–419.
31 Solbiati L, Cioffi V, Ballarati E. Ultrasonography of the neck. RadiolClin North Am, 1992;30:941–954.
32 Tohnosu N, Onoda S, Isono K. Ultrasonographic evaluation of cervicallymph node metastases in esophageal cancer with special reference tothe relationship between the short to long axis ratio (S/L) and the cancercontent. J Clin Ultrasound, 1989;17:101–106.
33 Sakai F, Kiyono K, Sone S, et al. Ultrasonic evaluation of cervicalmetastatic lymphadenopathy. J Ultrasound Med, 1988;7:305–310.
34 Ahuja A, Ying M. Grey-scale sonography in assessment of cervicallymphadenopathy: review of sonographic appearances and features thatmay help a beginner. Br J Oral Maxillofac Surg, 2000;38:451–459.
35 Ying M, Ahuja A, Brook F, et al. Nodal shape (S/L) and its combinationwith size for assessment of cervical lymphadenopathy: which cut-offshould be used? Ultrasound Med Biol, 1999;25:1169–1175.
36 Ying M, Ahuja A, Brook F, Metreweli C. Vascularity and grey-scalesonographic features of normal cervical lymph nodes: variations withnodal size. Clin Radiol, 2001;56:416–419.
37 Rubaltelli L, Proto E, Salmaso R, et al. Sonography of abnormal lymphnodes in vitro: correlation of sonographic and histologic findings. AJRAm J Roentgenol, 1990;155:1241–1244.
38 Evans RM, Ahuja A, Metreweli C. The linear echogenic hilus incervical lymphadenopathy—a sign of benignity or malignancy? ClinRadiol, 1993;47:262–264.
39 Ahuja A, Ying M, King A, Yuen HY. Lymph node hilus: gray scale andpower Doppler sonography of cervical nodes. J Ultrasound Med, 2001;20:987–992.
40 Atula TS, Varpula MJ, Kurki TJ, et al. Assessment of cervical lymphnode status in head and neck cancer patients: palpation, computedtomography and low field magnetic resonance imaging compared withultrasound-guided fine-needle aspiration cytology. Eur J Radiol, 1997;25:152–161.
41 Atula TS, Grenman R, Varpula MJ, et al. Palpation, ultrasound, andultrasound-guided fine-needle aspiration cytology in the assessment ofcervical lymph node status in head and neck cancer patients. HeadNeck, 1996;18:545–551.
42 van den Brekel MW, Stel HV, Castelijns JA, et al. Lymph node stagingin patients with clinically negative neck examinations by ultrasound andultrasound-guided aspiration cytology. Am J Surg, 1991;162:362–366.
43 Robinson IA, Cozens NJ. Does a joint ultrasound guided cytology clinicoptimize the cytological evaluation of head and neck masses? ClinRadiol, 1999;54:312–316.
CLINICAL RADIOLOGY358