Embed Size (px)
Citation preview

Sonographic DifferentialDiagnosis of Acute ScrotumReal-time Whirlpool Sign, a Key Sign of Torsion
S. Boopathy Vijayaraghavan, MD, DMRD
Objective. The purpose of this study was to prospectively investigate the role of high-resolution andcolor Doppler sonography in the differential diagnosis of acute scrotum and testicular torsion in par-ticular. Methods. Patients who underwent sonography for acute scrotum between April 2000 andSeptember 2005 were included in the study. Gray scale and color Doppler sonography of the scrotumwas performed. The spermatic cord was studied on longitudinal and transverse scans from the inguinalregion up to the testis, and the whirlpool sign was looked for. Results. During this period, 221 patientsunderwent sonography for acute scrotum. Sixty-five had epididymo-orchitis with a straight spermaticcord, a swollen epididymis, testis, or both, an absent focal lesion in the testis, and increased flow oncolor Doppler studies along with the clinical features of infection. Three had testicular abscesses.Sonography revealed features of torsion of testicular appendages in 23 patients and acute idiopathicscrotal edema in 19. Complete torsion was seen in 61 patients who had the whirlpool sign on grayscale imaging and absent flow distal to the whirlpool. There was incomplete torsion in 4 patients inwhom the whirlpool sign was seen on both gray scale and color Doppler imaging. Nine patients hadsegmental testicular infarction, and 1 had a torsion-detorsion sequence revealing testicular hyperemia.In 14 patients, the findings were equivocal. There was a complicated hydrocele, mumps orchitis, andvasculitis of Henoch-Schönlein purpura in 1 patient each. Five patients had normal findings. Fourteenwere lost for follow-up. Conclusions. Sonography of acute scrotum should include study of the sper-matic cord. The sonographic real-time whirlpool sign is the most specific and sensitive sign of torsion,both complete and incomplete. Intermittent testicular torsion is a challenging clinical condition with aspectrum of clinical and sonographic features. Key words: acute scrotum; color Doppler sonography;segmental infarction; sonography; testicular torsion; whirlpool sign.
Received December 12, 2005, from SonoscanUltrasonic Scan Centre, Coimbatore, India. Revisionrequested January 5, 2006. Revised manuscriptaccepted for publication February 9, 2006.
I thank V. R. Ravikumar, MS, MCh (PediatricSurgery), for initiating this study; all the urologistsand pediatric surgeons—S. V. Kandasamy, MS, MCh,in particular—for cooperation during this study; andD. Anandakumar MBBS, DNB, MRCS, S. Sreedharan,and R. Padma for assistance.
Address correspondence to S. BoopathyVijayaraghavan, MD, DMRD, 16 B VenkatachalamRd, R. S. Puram, Coimbatore 641 002, India.
E-mail: [email protected] or [email protected]
AbbreviationsITT, intermittent testicular torsion
cute scrotal pain may have many causes. Themore common causes are testicular torsion,epididymo-orchitis, torsion of the testicularappendages, and acute idiopathic scrotal edema.
The most important aim of imaging in these patients is torule in or out testicular torsion, which warrants emergen-cy surgery to avoid testicular impairment. At the sametime, the investigation should be specific enough to avoidunnecessary surgery. Testicular torsion can be extravagi-nal, intravaginal, or mesorchial. Intravaginal torsion, themost common type, occurs between 3 and 20 years of age,with an incidence of 65% between 12 and 18 years.1 It isgenerally associated with a preexisting anomaly of fixationof the testis, termed “bell and clapper testis.” Here theintrascrotal portion of the spermatic cord lacks posterioradhesion to the scrotum and remains surrounded by thetunica vaginalis, thus predisposing to rotation of the
© 2006 by the American Institute of Ultrasound in Medicine • J Ultrasound Med 2006; 25:563–574 • 0278-4297/06/$3.50
A
Article
Video online at www.jultrasoundmed.org.
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 563

testis and cord. A 12% incidence of bell clapperdeformity was found in one autopsy series.2 Thehorizontal lie of the testis has been linked with thebell clapper deformity in 100% of patients whohave had surgery.3–5 In most people, this anomalyis bilateral,5 which warrants orchidopexy of thecontralateral testis in cases of torsion of the testis.This procedure is necessary to avoid the risk ofmetachronous torsion of the contralateral testisand anorchia, the reported incidence of which is30% to 43% of cases.6–8 Hence, a definitive diag-nosis of testicular torsion is essential even in caseswith late appearance, partial torsion, or intermit-tent testicular torsion (ITT). Even though thereare clinical signs of differentiation between thevarious conditions causing acute scrotum, theyare not accurate. There are gray scale sonograph-ic features of the testis and its environment in dif-ferentiating these conditions, but they fail inaccuracy. High-resolution color Doppler sonog-raphy has been shown to be the most accurateand important modality in the differential diag-nosis of acute scrotal pain,9–12 but there are somedifficulties encountered. Arce et al13 and Baud etal14 described rotation of the cord as a very usefulsign of acute spermatic cord torsion. More recent-ly, the incidence of ITT or the torsion-detorsionsequence with a varying spectrum of clinical andsonographic features has been reported by manyauthors.3,4,15–18 Intermittent testicular torsion is aclinical syndrome defined by a history of unilater-al scrotal pain of sudden onset and of short dura-tion that resolves spontaneously.15 The intensityof pain may or may not be as severe as that seenwith acute torsion. The mean number of painfulepisodes reported is 4.3, and the range is 1 to 30over 2 to 48 months.3,5,16 The mean age of initialappearance is reportedly 12 years (range, 1.7 to 58years).3,5,17 The objective of this study was toprospectively investigate the role of high-resolu-tion and color Doppler sonography in the differ-ential diagnosis of acute scrotum and testiculartorsion in particular, with a real-time technicalmodification of the sign of rotation of the cord inthe form of the whirlpool sign.
Materials and Methods
All patients who had acute pain with or withoutswelling of the scrotum between April 2000 andSeptember 2005 were included in the study. Theages of the patients and the clinical features wererecorded. There were no laboratory investiga-
tions available at the time of sonography. High-resolution sonography and color Doppler sonog-raphy were done on all the patients with a Linear5- to 12-MHz probe (HDI 3500 and HDI 5000;Philips Medical Systems, Bothell, WA). Gray scaleimaging started in the inguinal region of thesymptomatic side and extended along the sper-matic cord to end in the scrotum. Both longitudi-nal and transverse scans were done. Thefollowing features were looked for: (1) tortuosityof the cord, (2) an acute change in the direction ofthe cord, and (3) the presence of the whirlpoolsign. The whirlpool sign was elicited in the fol-lowing manner. When tortuosity of the spermat-ic cord was seen, a short axis scan of the cordabove the level of tortuosity was obtained. Thenthe transducer was moved down along the cord,and a rotation of the cord structures was lookedfor. If an acute rotation was seen, it was taken asa positive whirlpool sign. The location of thewhirlpool sign and the axis of rotation werenoted. If it was not seen, the same maneuver wasrepeated in all possible angles of the tortuouscord. The gray scale features of the testis and epi-didymis were studied. If a hydrocele was present,its nature was noted. Then the same techniquewas repeated with color Doppler sonography.Spectral tracing was done in appropriate situa-tions. The same procedure was repeated on theopposite side. Those patients who did not havesurgery underwent laboratory investigations.
Results
During the study period, there were 221 patientswith acute scrotal pain. An overview of the diag-noses and the numbers of the cases is given inTable 1.
There were features characteristic of epididy-mo-orchitis in 65 patients, including a straightspermatic cord, a swollen epididymis, testis, orboth, an absent focal lesion in the testis, with orwithout a hydrocele, and increased flow on colorDoppler studies in the epididymis and testis orepididymis alone associated with clinical andlaboratory features of infection or urinary tractinfection, such as fever, dysuria, and leukocyto-sis. The disease involved the right testis in 39(60%) patients and the left testis in 26 (40%). Theage of the patients ranged from 5 months to 76years. Four of the 65 patients underwent surgicalexploration and were confirmed to have epididy-mo-orchitis. The rest were treated appropriately.
564 J Ultrasound Med 2006; 25:563–574
Sonographic Differential Diagnosis of Acute Scrotum
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 564

They were followed with clinical examination orsonography or by telephone conversation withthe patient or his parents after a minimum of 8weeks in patients with a good response and asrequired by clinical condition in others. Duringfollow-up, there were testicular or epididymalabscesses in 18 patients, which were treatedappropriately. All the other patients were con-firmed to have normal-sized testis after 8 weeks.
Three patients in this series with scrotal painand high fever had testicular abscesses. Thetestis was swollen with a large hypoechoic area.On color Doppler imaging, there was lack of flowin the hypoechoic area, whereas there wasincreased flow in the rest of the testis and epi-didymis. They underwent orchidectomy, whichconfirmed the diagnosis.
The sonographic diagnosis was torsion of thetesticular appendage in 23 patients. These patientshad a straight spermatic cord and a normal testis.There was a mass of varying size and echo patternin relation to the head of the epididymis andupper pole of the testis. A minimal hydrocele waspresent in 16 (76%) patients. On color Dopplerstudy, there was increased flow seen in the testisand epididymis in 8 patients and in the epi-didymis only in 15 patients. There was no flowseen in the masses in all the patients. The age ofthe patients ranged from 4.5 to 15 years. Five ofthem underwent surgical exploration, whichrevealed torsion of the testicular appendage in 4and the epididymal appendage in 1. The rest of thepatients were treated conservatively and followedclinically or sonographically and were confirmedto have an uneventful recovery.
Nineteen patients had features of acute idio-pathic scrotal edema, which revealed a normaltestis and edema of the scrotal wall. The age ofthese patients ranged from 3 days to 10 years.
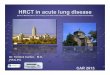
Complete testicular torsion was seen in 61patients who had the whirlpool sign in the sper-matic cord on real-time gray scale imaging(Video 1) and absent intratesticular flow on colorDoppler studies. On a static image, the mass ofthe whirlpool had the appearance of a doughnut,a target with concentric rings, a snail shell, or astorm on a weather map (Figure 1). The appear-ance was best seen with the transducer at differ-ent angles. The whirlpool sign was seen in alongitudinal scan of the spermatic cord in 12(20%) patients and in a transverse scan in 20(32%) patients. The axis was oblique of varyingdegrees in 29 (48%) patients. The mass of thewhirlpool was seen just outside the external ring(Figure 1B), at a varying distance above the testis(Figure 1, C and D), or posterior to the testis(Figure 2 and Table 2). In 1 child of 3 months, thetestis was undescended and seen in the inguinalcanal. A whirlpool sign was seen close to it(Figure 3). The maximum width of the mass ofthe whirlpool was 20 mm. The testis and its envi-ronment had varying features on the gray scaleimaging of the testis, which are summarized inTable 3. On color Doppler studies, there was noflow in the cord distal to the whirlpool and with-in the testis (Video 2) in 56 patients. In 5patients, there was flow seen in the proximalpart of the mass of the whirlpool and no flow inthe distal part and the testis (Figure 4 and Video3). Ages of these patients were between 3months and 57 years. The interval between theonset of acute scrotal pain and sonographyranged from 3 hours to 5 days. A history of a pre-vious episode of testicular pain was present in24 (40%) patients. Eight of these 24 patients hada sonographic diagnosis of epididymo-orchitisduring the previous episode. The conditioninvolved the right testis in 14 (23%) patients andthe left testis in 47 (77%). Surgical explorationwas done in 48 of these patients and confirmedtesticular torsion in all of them. In 40, the testiswas gangrenous; therefore, ipsilateral orchidec-tomy and contralateral orchidopexy were done.In 8 patients, the condition of the testisimproved on derotation of the cord; therefore,bilateral orchidopexy was done. Contralateralorchidopexy alone was done in 13 patients whoreported late. These 13 patients were followed
565
Vijayaraghavan
Table 1. Sonographic Diagnoses
Diagnosis No. of patients
Acute epididymo-orchitis 65Testicular abscess 3Torsion of appendage of testis 23Acute idiopathic scrotal edema 19Complete torsion of testis 61Incomplete torsion of testis 4Segmental infarction of testis 9Torsion-detorsion with hyperemia 1Equivocal features 14Complicated hydrocele 1Mumps orchitis 1Henoch-Schönlein purpura vasculitis 1Normal 5Lost for follow-up 14Total 221
J Ultrasound Med 2006; 25:563–574
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 565

566 J Ultrasound Med 2006; 25:563–574
Sonographic Differential Diagnosis of Acute Scrotum
Figure 1. Various appearances of a whirlpool mass (betweenarrows) on static images resembling a doughnut (A), a targetwith concentric rings (B), a snail shell (C), a snail (D), and a stormon a weather map (E).
D E
B C
A
clinically or sonographically and were con-firmed to have a decrease in the size of thesymptomatic testis, a feature taken as confirma-tive of torsion.
In 4 patients, the whirlpool sign was seen in themass of the spermatic cord on both gray scaleand color Doppler imaging (Figure 5 and Video4). On color Doppler studies, the visualized ves-sels were seen to rotate around the central axis.
Blood flow was seen in the distal cord, too. In 1 ofthese patients, the whirlpool sign was seen onlyon a dynamic real-time study, and a whirlpoolmass was not seen on a static image. In thesepatients, the appearance of the testis was vari-able. In 1 patient, the testis was swollen andhypoechoic without any focal changes. On acolor Doppler study, there were sparse vesselsseen in the testis. In the other 3 patients, the testis
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 566
was swollen and revealed focal hypoechoic areasof varying size. On color Doppler studies, therewas no flow seen in the hypoechoic areas, sug-gestive of segmental infarction. The rest of thetestis with a normal echo pattern showed a nor-mal flow pattern in 2 patients and hyperemia in1. The visualized intratesticular vessels revealeda normal flow pattern on spectral tracing in all 4patients. These 4 patients underwent surgicalexploration. There was torsion of the cord(Figure 5D) in all of them. The testis was swollenwith features of ischemia or segmental infarc-tion. After detorsion of the cord, there wasimprovement in the appearance of the testis;therefore, bilateral orchidopexy was done. In 2patients, the testis was normal in appearance onfollow-up sonography performed 8 weeks later
and also on color Doppler studies. On the initialscan, 1 of these 2 patients did not show focalchanges, and the other showed hyperemia. Inthe other 2 patients, the testes had atrophied.These 4 patients were concluded to have partialor incomplete torsion.
In 9 patients, the spermatic cord was straight,and the axis of the testis was horizontal. Thetestis was swollen in 8 of them and smaller in 1.The testis revealed hypoechoic lesions of varyingsize. On color Doppler studies, there was nodetectable flow in these hypoechoic areas. Thearea of the testis with the normal echo patternrevealed a normal arterial flow pattern in 7patients and hyperemia in 2 (Figure 6). The epi-didymis was either normal or increased in sizeand showed increased flow on color Dopplerstudies in all these patients. In 1 patient, therewas wide separation of testis and epididymis,suggestive of a long mesorchium. All thesepatients gave a history of acute testicular pain ofvarying but short durations, which was sponta-neously relieved. They were free of symptoms for5 hours to 10 days before scanning. None ofthem had fever or evidence of conditions associ-ated with vasculitis. All these patients underwentsurgical exploration, and the testis was swollenin 8 and normal in size in 1. All the testes revealedischemic regions of various sizes suggestive ofsegmental infarction of the testis (Figure 6D). In 1patient, a long mesorchium was confirmed. Onneedle prick, there was a subnormal bleedingresponse. Orchidectomy with contralateral orchi-dopexy was done in 7 patients. Histopathologicexamination confirmed segmental hemorrhagicinfarction in all of them. In 2 patients, bilateralorchidopexy was done. On follow-up, both ofthem had a decrease in the size of the testis. In allthese patients, the features seen in the testis weresuggestive of segmental infarction of the testis.None of them proved to have a preexisting vas-cular disease to explain the infarction. All thepatients gave a history of acute testicular pain ofshort duration with spontaneous relief. The testiswas placed horizontally in all of them. Because ofall these features, the patients in this group wereconcluded to have segmental testicular infarc-tion due to a torsion-spontaneous detorsionsequence or ITT.
One patient aged 23 years gave a history of 3attacks of acute left testicular pain lasting for 5to 10 minutes with spontaneous relief of painstarting from the age of 8 years. He sought care
567
Vijayaraghavan
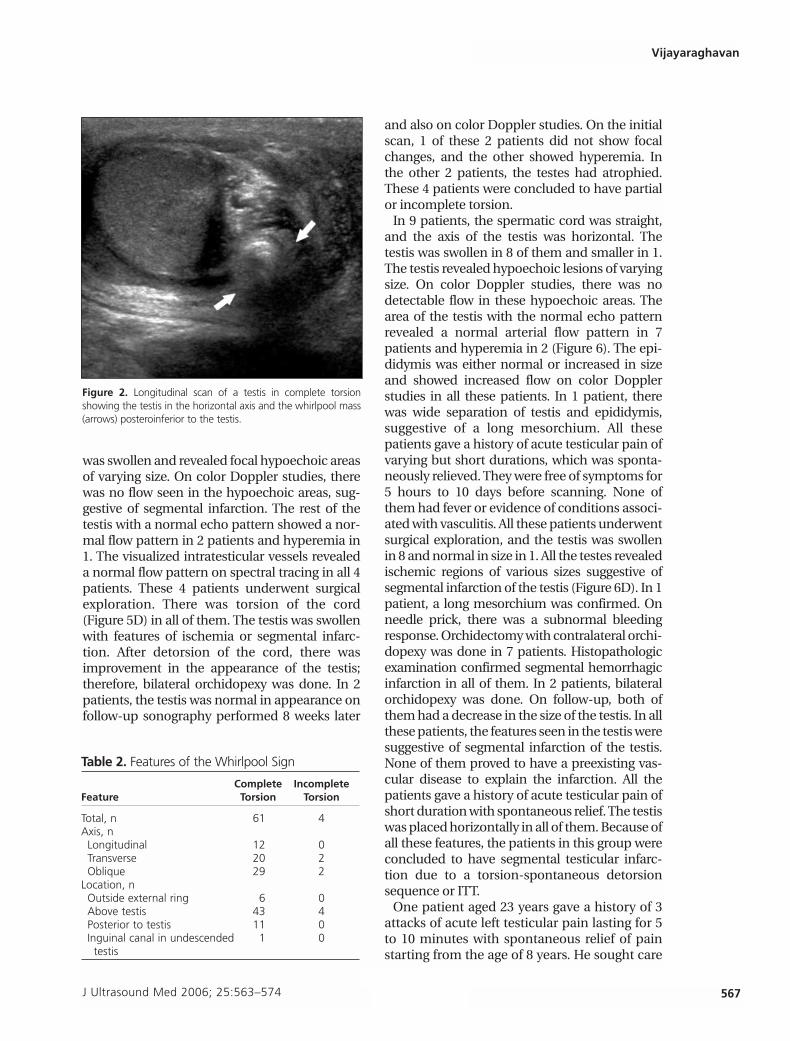
Figure 2. Longitudinal scan of a testis in complete torsionshowing the testis in the horizontal axis and the whirlpool mass(arrows) posteroinferior to the testis.
Table 2. Features of the Whirlpool Sign
Complete IncompleteFeature Torsion Torsion
Total, n 61 4Axis, nLongitudinal 12 0Transverse 20 2Oblique 29 2
Location, nOutside external ring 6 0Above testis 43 4Posterior to testis 11 0Inguinal canal in undescended 1 0testis
J Ultrasound Med 2006; 25:563–574
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 567

6 hours after the most recent episode. He didnot have a fever. On sonography, the spermaticcord was straight. The testis was placed alongthe horizontal axis. The testis and epididymisshowed subtle increases in size with decreasedechogenicity, which could be recognized onlyon meticulous comparison with the contralat-eral testis. On a color Doppler study, there wasunequivocal increased flow seen in the left testisand epididymis (Figure 7). It was concluded to
be a torsion-detorsion sequence. Bilateralorchidopexy was done after 1 month, at whichtime both the testes were normal.
Fourteen children had acute scrotum withoutfever. Sonography revealed a straight spermaticcord and a swollen testis and epididymis. Oncolor Doppler studies, there was unequivocalincreased flow in the testis and epididymis. Theydid not have evidence of infection or urinarytract infection. They were treated with antibi-otics. Twelve of them had a normal-sized testisafter 8 weeks. These patients could have hadeither epididymo-orchitis or ITT. In 2 of these 14patients, the testis had atrophied, indicating thatthey most probably had ITT.
There was a complicated hydrocele alone in 1patient. In 2 patients, there were precedingillnesses of mumps and Henoch-Schönlein pur-pura. In both patients, sonography showed aswollen, hypoechoic testis with hyperemia, sug-gestive of orchitis due to these etiologies.Sonographic findings were normal in 5 patients.Fourteen patients were lost for follow-up.
Discussion
Acute scrotal pain can have diverse causes. Themost important objective of treatment of thesepatients is to rule in or rule out testicular torsion.
568 J Ultrasound Med 2006; 25:563–574
Sonographic Differential Diagnosis of Acute Scrotum
A B
Figure 3. Scans of the left inguinal region showing a swollen and hypoechoic undescended testis in the inguinal canal secondary totorsion (A) and a whirlpool mass (arrows) just lateral to the testis (B).
Table 3. Gray Scale Features of Torsion
Complete IncompleteFeature Torsion Torsion
Total, n 61 4Whirlpool sign, n 61 4Size of testis, nSwollen 58 4Smaller 3 0
Echo texture, nUniformly hypoechoic 30 1Uniformly hypoechoic with echogenic septa 3 0Uniform echo pattern with hypoechoic septa 5 0Focal hypoechoic areas 23 3
Axis, nLongitudinal 10 0Transverse 51 4
Hydrocele, nSimple 31 2Septated 5 0
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 568

J Ultrasound Med 2006; 25:563–574 569
Vijayaraghavan
A B
Figure 4. A, Color Doppler image showing the vessels in the proximal part of a whirlpool mass (arrows). B, Flow is absent in the dis-tal part of the whirlpool (arrows).
Figure 5. Incomplete torsion of the testis. A, Longitudinal scan of a horizontally placed testis showing a large hypoechoic area(arrows) in the upper two thirds of the testis and a normal echo pattern (arrowhead) in the lower third. B, Color Doppler image show-ing no flow in the hypoechoic area with a few vessels seen in the poles. C, Color Doppler image of the whirlpool mass showing thevisualized vessels going around the central axis. D, Ischemic testis with the segmental infarction of the upper two thirds and torsionof the spermatic cord (arrow).
C D
A B
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 569

It requires immediate intervention to avoid infarc-tion of the affected testis.19 Conversely, if torsioncan be confidently ruled out, unnecessary surgicalintervention can be avoided. Intermittent testicu-lar torsion or a torsion-detorsion sequence is aclinical syndrome defined by a history of unilater-al scrotal pain of sudden onset and of short dura-tion that resolves spontaneously.15 The naturalhistory of ITT varies. Some patients may haveacute torsion at a later date. This is evidenced bythe observation that up to half of patients withacute torsion report previous episodes of testicu-lar pain.3 In this series, the incidence of previousepisodes was 40%. Some patients have continuedattacks, which, if lasting enough, can result inischemic damage to the testis, although definiteevidence of this is lacking.4,16,18
Currently, a sonographic study of acute scrotumis focused on evaluation of the testis, epididymis,
and scrotal wall on gray scale sonography andstudy of the intratesticular vascular flow by colorDoppler imaging.9–12,14,20–23 However, there are sit-uations that may show inconclusive results oncolor Doppler studies. The torsion-detorsionphenomenon may show testicular hyperemia,mimicking an inflammatory process.23,24 Thereare reports of spermatic cord torsion with pre-served testis perfusion on color Doppler stud-ies.11,25–28 Arce et al13 and Baud et al14 concludedthat all these pitfalls occur because of indirectevaluation of a condition that is caused else-where, and they proposed to study the spermat-ic cord directly because actual torsion occursthere. Baud et al14 and Kalfa et al29 studied thespermatic cord in its entire length, including theinguinal canal, and described a spiral twist of thecord at the external inguinal ring diagnostic oftorsion, irrespective of the color Doppler findings
570 J Ultrasound Med 2006; 25:563–574
Sonographic Differential Diagnosis of Acute Scrotum
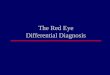
Figure 6. Segmental testicular infarction. A, Longitudinal scan of the straight spermatic cord (arrows). B, Longitudinal scan showinga transverse section of a swollen testis with a large hypoechoic area (arrows) in the lower part and a normal echo pattern (arrowhead)in the upper part. There is a septated hydrocele (HC). C, Color Doppler image showing lack of flow in the hypoechoic area with a fewvessels in the periphery of the left testis (LT). D, Ischemic testis with segmental infarction.
C D
A B
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 570

in the testis. They described high sensitivity andspecificity of this sign. The rate of unnecessarysurgery was 0%. The same sign was elicited inthis series with a real-time modification in theform of downward movement of the transduceralong the spermatic cord to look for thewhirlpool sign. The mass of torsion of the cord
had the appearance of a doughnut, a target, asnail shell, or a storm on a weather map. Themovement of the transducer in a downwarddirection perpendicular to the axis of this massbrought on the whirlpool sign. The whirlpoolmass is seen in various locations: just distal tothe external ring, above the testis or posterior tothe testis, and in the inguinal canal if the testis isundescended. The angle at which it is best seenalso varies. This sign was seen in 65 patients inthis series, all of whom were proved to have tes-ticular torsion, complete in 61 and incomplete in4. In complete torsion, the whirlpool sign is seenonly on gray scale sonography with absentintratesticular flow on color Doppler imaging. Inincomplete torsion, there is flow in the vessels ofthe whirlpool mass, distal to it, and in the testis.The whirlpool sign is seen on gray scale as well ascolor Doppler imaging. The incomplete torsionprobably explains the cases reported in earlierreports as missed torsion or torsion with pre-served testicular perfusion, and the whirlpoolsign helps in diagnosis of torsion in suchpatients. Hence, the real-time whirlpool sign isthe most definitive sign of torsion because it has100% specificity and sensitivity; there were nofalse-positive or -negative findings of torsion inthis series.
The second group of patients has a straightspermatic cord, a swollen testis, epididymis, orboth, absent focal changes in the testis, andunequivocal increased flow in the testis and epi-didymis. Sometimes the flow may be increasedin the epididymis alone with normal flow in thetestis. These features may be seen in either acuteepididymo-orchitis or ITT,5 and the differentia-tion is based on the presence or absence of clin-ical or laboratory evidence of infection.5 Patientswith acute epididymo-orchitis have some clini-cal features suggestive of epididymo-orchitis,such as fever, dysuria, and laboratory evidence ofleukocytosis or urinary tract infection, seen in 65patients in this series. The patients with ITT lackthese clinical features of epididymo-orchitis, andinstead they may give a typical history of acutepain of short duration with spontaneous relief,which is usually associated with vomiting. Theaxis of the testis is horizontal. We had 1 patientwith this diagnosis. The finding of epididymal ortesticular hyperemia or both in ITT is indicativeof reactive hyperemia and is seen in 17% ofpatients with ITT. A consistent sonographic signdescribed in ITT is the horizontal lie of the testis.5
J Ultrasound Med 2006; 25:563–574 571
Vijayaraghavan
C
B
A
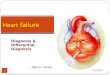
Figure 7. Intermittent testicular torsion. A, Transverse scan of ascrotum showing the short axis of the right testis (RT) and longaxis of the left testis (LT) indicating the horizontally placed lefttestis. The left testis is slightly hypoechoic compared with theright testis. B, Color Doppler image of the right testis showing anormal flow pattern. C, Color Doppler image showing increasedflow in the left testis.
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 571

In 14 children in this series, who had a straightspermatic cord and hyperemia, a diagnosis couldnot be offered because there was lack of any dif-ferentiating clinical or laboratory features. Theusefulness of the horizontal testicular axis in ITT5
was not yet known during that period of study;hence, the observation was not looked for inthose patients. This observation may be a usefulsonographic sign in such patients.
The fourth group has a straight spermatic cord,a horizontally oriented testis, a swollen testis andepididymis, focal changes in the testis, andincreased flow in the spermatic cord and epi-didymis with decreased or increased flow in thetestis. The focal hypoechoic areas in the testislack blood flow on color Doppler imaging. Thepossible diagnoses in these patients are segmen-tal infarction (due to ITT or vasculitis) and epi-didymo-orchitis with suppuration of the testis.The differentiation is by clinical or laboratoryevidence of infection for a testicular abscess andthe lack of such evidence with a horizontal axis ofthe testis for ITT.30 In this series, there were 12patients with these features, and 9 of themturned out to have ITT with segmental infarctionand 3 to have testicular abscesses.
There was no case of unnecessary surgery inthis series (0%). There were only 2 cases ofmissed torsion in this series of 207 patients (1%)who were followed for at least 8 weeks, whichincluded all forms of torsion. These 2 patientshad equivocal sonographic features with testicu-lar hyperemia. The limitation of the study is thatthe patients with acute epididymo-orchitis (65cases) and those with testicular or epididymalhyperemia who were not given a sonographicdiagnosis (14 cases) were followed for a period of8 weeks only, which is short considering the pos-sibility of ITT occurring after a gap of even years.Follow-up extending for more time is not possi-ble in the health care system existing in thiscountry. The length of follow-up, however, wouldform a good subject of study in a society with aclosed health care system, where patients couldbe followed for many years; that would give thetrue incidence of ITT versus acute epididymo-orchitis in the presence of testicular or epididy-mal hyperemia.
From the data of this series and those of recentpublications, one can draw the following conclu-sions about ITT. The sonographic features of thissyndrome will depend on the time betweensonography and the event, the severity of the tor-
sion, and the duration of the event. If the patientreports after a few days of a mild event, the sono-graphic findings may be normal. If he reportswithin a few hours after severe torsion and com-plete detorsion, the testis would be slightlyswollen and hypoechoic, and the spermatic cordwould be straight. There would be hyperemia ofthe testis on color Doppler imaging. The same fea-tures are also seen in acute epididymo-orchitis.The differentiation of ITT and epididymo-orchi-tis in this situation is only clinical. One useful andconsistent sonographic finding in ITT is the hor-izontal lie of the testis.3,5 Some of these patientswith a torsion-detorsion sequence showing tes-ticular hyperemia and mimicking epididymo-orchitis have testicular atrophy later, which iswell documented.16 It was seen in 2 patients inthis series. Eight patients in this series who hadclassic features of acute torsion had reports of anearlier sonographic diagnosis of acute epididy-mo-orchitis because of testicular hyperemia,indicating that they had a torsion-detorsionsequence on the previous occasion, which alsocorroborates this phenomenon.
The third group of the patients with ITT, whohave severe torsion with complete detorsion andreport early, reveal sonographic features of seg-mental testicular infarction.30 The horizontallyplaced testis reveals focal hypoechoic areas thatlack blood flow, with the rest of the testis showinga normal echo pattern. These areas with a normalecho pattern either show normal blood flow insparse arteries or show hyperemia. The epi-didymis may show increased blood flow. Althoughpolycythemia, sickle cell anemia, and acute angi-tis have been linked to segmental infarction, thecause of most reported cases is unknown,30–33 andthese were probably in fact cases of ITT. The dif-ferential diagnosis of this condition can be severeorchitis with suppuration. The differentiation ofthese conditions is by the clinical features of infec-tion seen in epididymo-orchitis and the history ofacute pain with spontaneous relief, a history of aprevious episode, and a horizontal testicular axisin ITT.
In conclusion, testicular torsion is a complexcondition with a spectrum of clinical and sono-graphic features. In complete torsion, there is awhirlpool sign on gray scale sonography andabsence of flow in the distal cord, testis, and epi-didymis. In incomplete torsion, there is awhirlpool sign on gray scale and color Dopplersonography and varying amounts of vessels
572 J Ultrasound Med 2006; 25:563–574
Sonographic Differential Diagnosis of Acute Scrotum
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 572

within the testis. The sonographic real-timewhirlpool sign is the most specific sign of torsion,either complete or incomplete, because it revealsthe actual anomaly. Alternatively, the torsionmay present a challenging spectrum of clinicalfeatures that may be due to ITT. The symptomsare acute onset of severe scrotal pain with spon-taneous relief after a short time. The sonograph-ic spectrum of this condition varies dependingon the severity and duration of the event and thetime between the event and sonography. Theremay be features of segmental testicular infarc-tion, testicular hyperemia, or a normal testis.
The following algorithm is suggested for sonog-raphy in a case of acute scrotal pain:
1. When the clinical history and physicalexamination are sufficiently alarming andunequivocal for testicular torsion and sonog-raphy is not possible immediately, surgicalexploration is done without any imaging.
2. When there are unequivocal sonographic fea-tures of the following conditions, the patient istreated accordingly: testicular torsion show-ing total absence of intratesticular blood flow,torsion of the testicular appendage, and acuteidiopathic scrotal edema.
3. When there is symmetric or asymmetricarterial flow seen in the testis, the spermaticcord is studied in detail to look for thewhirlpool sign. The real-time whirlpool signis the most specific sign of both completeand incomplete testicular torsion.
4. Features of segmental testicular infarctionand a horizontal lie of the testis in a patientwithout features of systemic vascular diseaseor infection are diagnostic of ITT. Prophylacticcontralateral orchidopexy should be per-formed to preserve the normal testis becauseof the high association of future contralateraltorsion.
5. In a case with features of a straight cord anda swollen testis and epididymis with hyper-emia, acute epididymo-orchitis and ITT areboth possible. The diagnosis of acute epi-didymo-orchitis is made when there are clin-ical or laboratory features of infection orurinary tract infection. A history of pain withspontaneous relief and a horizontal testicu-lar axis indicate ITT. When these differentiat-ing features are absent, the patients need
active follow-up. This is essential becauseITT is a possibility. The challenges of clinicaldecision making in these patients lie in therecognition that there is no definitive diag-nostic test to confirm ITT. Only by halting thepattern of recurrent pain can the diagnosisbe made, albeit retrospectively.18 When thereis a clinical history typical of ITT and a hori-zontal testicular axis, bilateral orchidopexy isdone immediately.
References
1. Williamson RC. Torsion of the testis and allied conditions.Br J Surg 1976; 63:465–476.
2. Caesar RE, Kaplan GW. Incidence of the bell-clapper defor-mity in an autopsy series. Urology 1994; 44:114–116.
3. Kamaledeen S, Surana R. Intermittent testicular pain: fixthe testes. BJU Int 2003; 91:406–408.
4. Schulsinger D, Glassberg K, Strashun A. Intermittent tor-sion: association with horizontal lie of the testicle. J Urol1991; 145:1053–1055.
5. Eaton SH, Cendron MA, Estrada CR, et al. Intermittent tes-ticular torsion: diagnostic features and management out-comes. J Urol 2005; 174:1532–1535.
6. Krarup T. The testes after torsion. Br J Urol 1978; 50:43–46.
7. Chakraborty J, Hikim AP, Jhunjhunwala JS. Quantitativeevaluation of testicular biopsies from men with unilateraltorsion of spermatic cord. Urology 1985; 25:145–150.
8. Skoglund RW, McRoberts JW, Ragde H. Torsion of thespermatic cord: a review of the literature and an analysis of70 new cases. J Urol 1970; 104:604--–607.
9. Burks DD, Markey BJ, Burkhard TK, Balsara ZN, HaluszkaMM, Canning DA. Suspected testicular torsion andischemia: evaluation with color Doppler sonography.Radiology 1990; 175:815–821.
10. Paltiel HJ, Connolly LP, Atala A, Paltiel AD, Zurakowski D,Treves ST. Acute scrotal symptoms in boys with an indeter-minate clinical presentation: comparison of color Dopplersonography and scintigraphy. Radiology 1998; 207:223–231.
11. Kravchick S, Cytron S, Leibovici O, et al. Color Dopplersonography: its real role in the evaluation of children withhighly suspected testicular torsion. Eur Radiol 2001; 11:1000–1005.
12. Aso C, Enriquez G, Fite M, et al. Gray-scale and colorDoppler sonography of scrotal disorders in children: anupdate. Radiographics 2005; 25:1197–1214.
13. Arce JD, Cortes M, Vargas JC. Sonographic diagnosis ofacute spermatic cord torsion. Rotation of the cord: a key tothe diagnosis. Pediatr Radiol 2002; 32:485–491.
J Ultrasound Med 2006; 25:563–574 573
Vijayaraghavan
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 573

14. Baud C, Veyrac C, Couture A, Ferran JL. Spiral twist of thespermatic cord: a reliable sign of testicular torsion. PediatrRadiol 1998; 28:950–954.
15. Creagh TA, McDermott TE, McLean PA, Walsh A.Intermittent torsion of the testis. BMJ 1988; 297:525–526.
16. Sellu DP, Lynn JA. Intermittent torsion of the testis. J R CollSurg Edinb 1984; 29:107–108.
17. Blumberg JM, White B, Khati NJ, Andrawis R. Intermittenttesticular torsion in a 58-year-old man. J Urol 2004; 172:1886.
18. Stillwell TJ, Kramer SA. Intermittent testicular torsion.Pediatrics 1986; 77:908–911.
19. Kass EJ, Stone KT, Cacciarelli AA, Mitchell B. Do all childrenwith an acute scrotum require exploration? J Urol 1993;150:667–669.
20. Patriquin HB, Yazbeck S, Trinh B, et al. Testicular torsion ininfants and children: diagnosis with Doppler sonography.Radiology 1993; 188:781–785.
21. Middleton WD, Middleton MA, Dierks M, Keetch D, DierksS. Sonographic prediction of viability in testicular torsion:preliminary observations. J Ultrasound Med 1997; 16:23–27.
22. Wilbert DM, Schaerfe CW, Stern WD, Strohmaier WL,Bichler KH. Evaluation of the acute scrotum by color-codedDoppler ultrasonography. J Urol 1993; 149:1475–1477.
23. Middleton WD, Siegel BA, Melson GL, Yates CK, AndrioleGL. Acute scrotal disorders: prospective comparison ofcolor Doppler US and testicular scintigraphy. Radiology1990; 177:177–181.
24. Ralls PW, Larsen D, Johnson MB, Lee KP. Color Dopplersonography of the scrotum. Semin Ultrasound CT MR1991; 12:109–114.
25. Bentley DF, Ricchiuti DJ, Nasrallah PF, McMahon DR.Spermatic cord torsion with preserved testis perfusion: ini-tial anatomical observations. J Urol 2004; 172:2373–2376.
26. Steinhardt GF, Boyarsky S, Mackey R. Testicular torsion: pit-falls of color Doppler sonography. J Urol 1993; 150:461–462.
27. Allen TD, Elder JS. Shortcomings of color Doppler sonogra-phy in the diagnosis of testicular torsion. J Urol 1995;154:1508–1510.
28. Ingram S, Hollman AS, Azmy A. Testicular torsion: misseddiagnosis on colour Doppler sonography. Pediatr Radiol1993; 23:483–484.
29. Kalfa N, Veyrac C, Baud C, Couture A, Averous M, GaliferRB. Ultrasonography of the spermatic cord in children withtesticular torsion: impact on the surgical strategy. J Urol2004; 172:1692–1695.
30. Ledwidge ME, Lee DK, Winter TC III, Uehling DT, MitchellCC, Lee FT Jr. Sonographic diagnosis of superior hemi-spheric testicular infarction. AJR Am J Roentgenol 2002;179:775–776.
31. Costa M, Calleja R, Ball RY, Burgess N. Segmental testicularinfarction. BJU Int 1999; 83:525.
32. Baratelli GM, Vischi S, Mandelli PG, Gambetta GL, Visetti F,Sala EA. Segmental hemorrhagic infarction of testicle. J Urol 1996;156:1442.
33. Bird K, Rosenfield AT. Testicular infarction secondary toacute inflammatory disease: demonstration by B-scanultrasound. Radiology 1984; 152:785–788.
574 J Ultrasound Med 2006; 25:563–574
Sonographic Differential Diagnosis of Acute Scrotum
vol25_no5_jum_online.q 4/14/06 10:25 AM Page 574