Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Sonographic assessment of carpal tunnel syndrome in rheumatoidarthritis: prevalence and correlation with disease activity
Omer Karadag • Umut Kalyoncu • Ali Akdogan • Yesim Sucullu Karadag •
Sule Apras Bilgen • Senay Ozbakır • Emilio Filippucci • Sedat Kiraz •
Ihsan Ertenli • Walter Grassi • Meral Calguneri
Received: 15 December 2010 / Accepted: 8 May 2011 / Published online: 24 May 2011
� Springer-Verlag 2011
Abstract Carpal tunnel syndrome (CTS) is one of the
most frequent extra-articular manifestations of rheumatoid
arthritis (RA). High frequency ultrasonography (US) is a
sensitive and specific method in diagnosis of CTS. This
study is aimed to: firstly assess diameter frequency of
CTS in RA with US and compare with a control group;
secondly, investigate relationship of CTS with disease
activity. One hundred consecutive RA patients (women/
men: 78/22) fulfilling ACR 1987 RA criteria and 45
healthy controls (women/control: 34/11) were enrolled
into study. Disease activity parameters, RA and CTS
patient global assessment and health assessment ques-
tionnaire (HAQ-DI) were recorded. Both patient and
control group were questioned about secondary causes of
CTS, and Katz hand diagram, Boston CTS questionnaire
and Phalen ve Tinel tests were applied once for each
hand. Wrist joint and carpal tunnel were assessed with US
grey scale and power Doppler US, then cross-sectional
area of median nerve (CSA) was calculated. Patients with
median nerve CSA between 10.0 and 13.0 mm2 were
evaluated with electromyography (EMG). CTS was
diagnosed if CSA of median nerve [13.0 mm2 or CTS
was shown with NCS. Although there was no difference
between RA patients and controls in age, sex, history of
DM (?) and goitre, CTS was more frequent in RA group
(respectively, 17.0% vs. 4.4%, P = 0.038). In RA group
with CTS, age, history of DM, disease duration, HAQ-DI
score, CTS patient global score, Boston symptom severity
and functional status scores were elevated compared to
without CTS [respectively, 57 (36–73) vs. 50 (24–76),
P = 0.041; 35.3% vs. 6.0%, P \ 0.001; 108 (12–396)
months vs. 72 (6–360) months, P = 0.036; 1.93 (0.75–
2.87) vs. 1.125 (0–2.75), P = 0.013; 52 (1–97) vs. 25
(0–91), P = 0.001; 2.81 (1.18–4.17) vs. 2.0 (1.0–4.01),
P = 0.01; 3.37 (1.37–5.0) vs. 2.25 (1.0–5.0), P = 0.008].
No difference was found between CTS (?) and (-) RA
patients in acute phase reactants, disease activity and US
findings (P [ 0.05). Sensitivity of Katz hand diagram was
higher than Tinel and Phalen tests (respectively, 100,
60.0, 66.7%). Boston symptom and functional scores of
RA patients with CTS diagnosed by EMG were increased
than patients CTS (-) by EMG [respectively, 3.05
(1.90–4.27) vs. 1.55 (1.0–2.90), P = 0.002; 3.25 (1.73–
3.82) vs. 1.12 (1.0–2.10), P = 0.008]. CTS frequency in
RA was found higher than normal population, especially
in patients with additional risk factors of CTS. There was
no relationship between CTS and disease activity.
CTS group had long disease duration and worse func-
tional status. CTS could be a result of the chronic course
in RA. In patient with CSA between 10 and 13 mm2,
Boston CTS questionnaire might give additional idea
about CTS.
Keywords Rheumatoid arthritis � Carpal tunnel
syndrome � Ultrasonography � Electromyography �Boston carpal tunnel syndrome questionnaire
O. Karadag (&) � U. Kalyoncu � A. Akdogan �S. A. Bilgen � S. Ozbakır � S. Kiraz � I. Ertenli � M. Calguneri
Department of Internal Medicine Unit of Rheumatology,
Hacettepe University, Incesu Caddesi No: 72/2, Ankara, Turkey
e-mail: [email protected]
Y. S. Karadag
Ankara Numune Education and Research Hospital 1st Neurology
Clinic, Ankara, Turkey
E. Filippucci � W. Grassi
Rheumatology Department, Universita Politecnica della Marche,
Ancona, Italy
123
Rheumatol Int (2012) 32:2313–2319
DOI 10.1007/s00296-011-1957-0

Introduction
Carpal tunnel syndrome (CTS) is one of the most frequent
extra-articular manifestations of rheumatoid arthritis (RA)
[1]. Nerve conduction studies (NCS) are the standard
diagnostic test for CTS [2]. High frequency ultrasonogra-
phy (US) is a non-invasive, cheaper, sensitive (89%) and
specific (83%) method in diagnosis of CTS [3, 4]. More-
over, US gives us opportunity to determine median nerve
and carpal tunnel pathologies [5]. Additionally, a CTS
severity algorithm based on the cross-sectional area (CSA)
of median nerve at proximal inlet of carpal tunnel has been
suggested (CSA 7.0–10.0 mm2: normal, 10.0–13.0 mm2:
mild, 13.0–15.0 mm2: moderate,[15.0 mm2: severe CTS)
[6]. The usefulness of this algorithm in RA was shown [7].
Additionally, RA patients with CSA between 10 and
13 mm2 are recommended to further evaluation with NCS.
But we could not find a US study investigating relationship
of disease activity with CTS in English literature. This
study was aimed to: firstly assess the prevalence of CTS
diagnosed by US in RA patients and healthy subjects
secondly, investigate relationship between CTS and disease
activity in RA.
Patients and methods
Patients
The study is approved by local ethics committee of
Hacettepe University. One hundred consecutive RA
patients (women/men: 78/22) fulfilling ACR 1987 RA
criteria and seen between May and November 2008 and 45
healthy control (women/men: 34/11) from check-up unit
were enrolled into study.
Clinical examinations
Demographic characteristics, swollen and tender joint
count, acute phase reactants [erythrocyte sedimentation
rate, C-reactive protein, complete blood count], RA patient
global assessment visual analogue scale (VAS 0–100 mm),
Health assessment questionnaire disability index (HAQ-
DI), disease activity score (DAS 28) and treatment
modalities were evaluated. Both patient and control group
were questioned about secondary causes of CTS [diabetes
mellitus (DM) and goitre]. CTS patient global score (VAS
0–100 mm), Katz hand diagram [8], Levine Boston CTS
questionnaire (BQ) [9], Phalen ve Tinel tests [10] were
applied once for each hand.
The BQ evaluates CTS in two subjects: Symptom
severity (BQ-sympt.) consisting of 11-items and functional
status (BQ-funct.) testing 8-items. A Turkish version of BQ
validated by Sezgin et al. [11] was used. The BQ was
presented in multiple-choice format, and scores were
assigned from 1 point (mildest) to 5 points (most severe).
Each score was calculated as the mean of the responses of
the individual items. Patients were divided into 4 groups
according to their mean score: extreme (4.1–5.0 points),
severe (3.1–4.0 points), moderate (2.1–3.0 points), mild
(1.1–2.0) points.
Ultrasonography
Sonographic evaluation of wrist joint and carpal tunnel
was performed by a rheumatologist (OK) blinded to the
physical and electrophysiologic findings of the subjects.
A MyLab 70 US system (Esaote Biomedica–Genoa, Italy)
equipped with a broadband 6–18-MHz linear transducer
was used. Patients were seated in a comfortable position
facing the sonographer, with the forearm resting on the bed
and fingers semi-flexed.
Wrist joint cavity widening and intra-articular power
Doppler signal (PDS) were assessed using a multi-planar
dorsal examination and adopting a semi-quantitative scor-
ing system from 0 to 3 (0: normal, 1: mild, 2: moderate, 3:
marked) [12, 13]. The median nerve was located superficial
to the echogenic flexor tendons. The full course of median
nerve in the carpal tunnel was assessed in longitudinal and
transverse planes. The main hallmark of tenosynovitis is
irregularities of tendon margins and presence of fluid in the
tendon’s sheath. The cross-sectional area of the median
nerve was measured at the proximal inlet of the carpal
tunnel using the pisiform bone as landmark by tracing a
continuous line within the hyperechogenicity boundary of
the nerve. No additional compression was applied on the
tissues under examination other than the weight of
the probe to avoid causing any artificial nerve deformity.
The cross-sectional area was measured three times, and the
mean value was used for further analysis. Each 10th patient
was asked to return within 24 h for assessing intra-observer
US reliability. A total of 9 CTS patients were assessed for
this purpose.
Nerve conduction studies
Hammer HB et al. [7] showed 10% of RA patients without
CTS symptoms had CSA areas reported in patients with
mild idiopathic CTS. And NCS are recommended for
patients with CSA 10.0–13.0 mm2.
According to this recommendation, electro-diagnostic
studies were carried out for all subjects with CSA between
10.0 and 13.0 mm2 according to the protocol proposed by
the American Academy of Neurology [14]. All testings
were done in the same room and in room temperature
conditions using Nihon Kohden 4 ME 8 elektrode entrance
2314 Rheumatol Int (2012) 32:2313–2319
123

4 record channel device by a neurologist (YSK) blinded to
clinical findings. Skin temperature on the hand was mea-
sured and maintained between 32.0 and 34.0�C. All par-
ticipants underwent median and ulnar nerve sensorimotor
NCS. Standard techniques of supramaximal percutaneous
stimulation with a constant current stimulator and surface
recording were used for NCSs. A ground electrode was
placed on the dorsum of the hand. The active electrode was
located over the thenar eminence (abductor pollicis brevis
muscle) for the median nerve and over the hypothenar
eminence (abductor digiti minimi) for ulnar nerve to record
compound muscle action potentials. The reference elec-
trode was placed over the first or fifth metacarpophalangeal
joint. The median and ulnar nerves were stimulated at the
wrist and elbow (antecubital region for median nerve, ulnar
fossa for ulnar nerve) at a distance of 8 cm from the wrist
to the active electrode. Sensory responses were obtained
antidromically.
Ring electrodes were used to obtain sensory nerve action
potentials. Electrodes were placed over the second finger
for the median nerve and fifth finger for the ulnar nerve.
The active recording electrode was placed more proxi-
mally, closest to the stimulator. The median and ulnar
nerves were stimulated at the wrist and elbow (antecubital
region for median nerve, ulnar fossa for ulnar nerve). The
severity of electrophysiological CTS impairment was
assessed by a previously reported neurophysiological
classification into 5 groups [15].
• Negative: nerve conduction studies are normal, no
electrophysiological evidence of CTS.
• Mild: slowing of the median sensory nerve conduction
velocity and normal distal motor latency.
• Moderate: slowing of the median sensory nerve con-
duction velocity and prolonged distal motor latency.
• Severe: absence of sensory response and prolonged
distal motor latency.
• Extreme: absence of motor and sensory responses.
The diagnosis of CTS was accepted in two situations:
1. CTS symptomatology ? CSA of median nerve
[13 mm2
2. CTS diagnosed with NCS in wrist with CSA
10.0–13.0 mm2
CTS Statistical analysis
Statistical analysis was performed with SPSS 11.0. Data
are presented as mean ± SD or median (range). CTS fre-
quency of RA patients was compared with control group.
Correlation between CSA of median nerve and age, disease
duration and CTS symptom duration was investigated.
Differences between CTS (?) and (-) RA groups
regarding age, sex, disease duration, RA treatments were
evaluated. Comparison of RA patients and controls for
numeric data was done with student t-test (for parametric
data) or Mann–Whitney U-test (for non-parametric data),
for nominal data with chi-square test. Correlation analysis
was made with Pearson’s or Sperman correlation test. In
the comparison of groups, P B 0.05 was accepted as
significant.
Results
One hundred consecutive RA patients (M/F: 22/78) were
recruited into the study. Patients mean age was
50.9 ± 12.6 years (range 24–76), and mean disease dura-
tion was 96.6 ± 80.3 month (Table 1). Demographic and
clinical findings of RA patients were shown in Table 1.
All of the patients were on DMARD treatment. Patients’
treatment protocols and per cents are shown in Table 3. Fif-
teen per cent of patients were on treatment of anti-tumour
necrosis factor a (TNF-a) agent ? DMARD combination.
Mean daily prednisolone dose was 1.43 ± 1.36 mg.
Seventy-one per cent of RA patients were rheumatoid
factor (RF) positive, and 69% of patients were anti-CCP
(cyclic citrulinnated peptide) positive. Sixty-two per cent
Table 1 Demographic and clinical findings of RA patients
Age, years (mean ± SD) 50.9 ± 12.6
Disease duration, month 96.6 ± 80.3
0–2 year, % 18
2–10 year, % 48
[10 year, % 34
Sex (female/male) 78/22
Diabetes mellitus, % 11
Hypothyroidism
Euthyroidism with treatment, % 16
Extra-articular involvement
Rheumatoid nodule, % 11
Pulmonary involvement, % 8
Treatment protocols
Mono-therapy 0
Double combination 15
Triple combination 57
Four agent combination 11
Anti-TNF ?DMARD combination 15
Anti-TNFa agent, % 15
Infliximab, % 5
Etanercept, % 3
Adalimumab, % 7
Combination treatments are consist of (hydroxychloroquine, metot-
rexate, sulphasalasine, leflunomide)
Rheumatol Int (2012) 32:2313–2319 2315
123
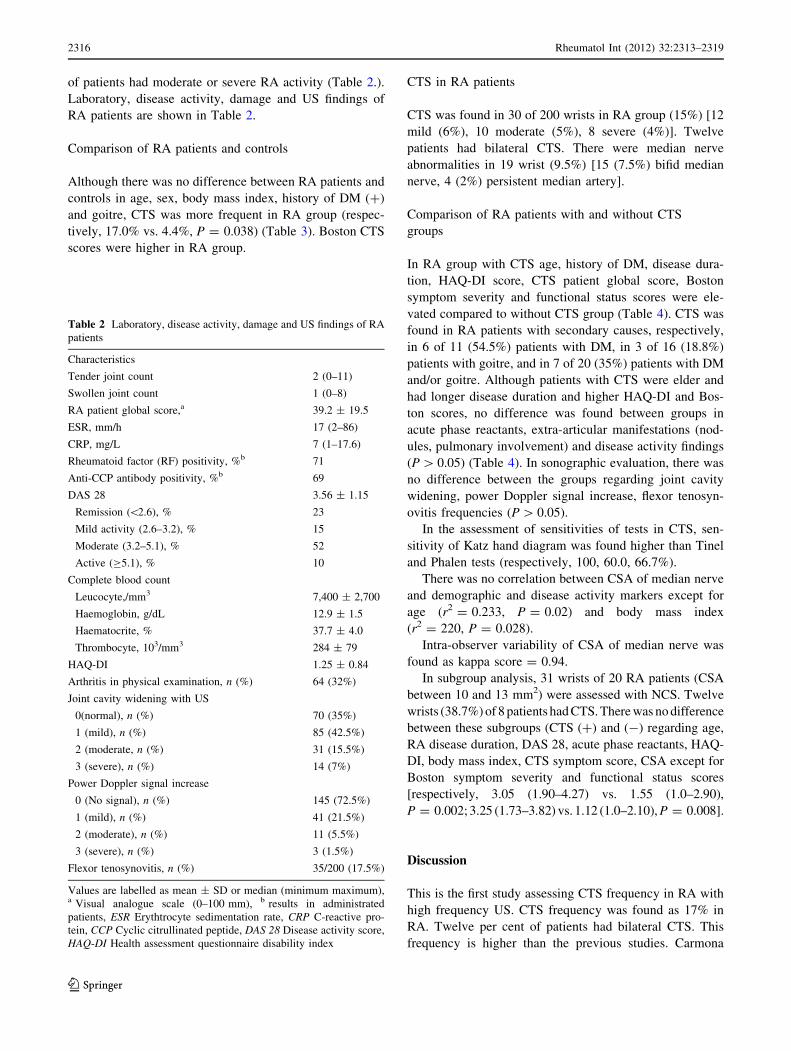
of patients had moderate or severe RA activity (Table 2.).
Laboratory, disease activity, damage and US findings of
RA patients are shown in Table 2.
Comparison of RA patients and controls
Although there was no difference between RA patients and
controls in age, sex, body mass index, history of DM (?)
and goitre, CTS was more frequent in RA group (respec-
tively, 17.0% vs. 4.4%, P = 0.038) (Table 3). Boston CTS
scores were higher in RA group.
CTS in RA patients
CTS was found in 30 of 200 wrists in RA group (15%) [12
mild (6%), 10 moderate (5%), 8 severe (4%)]. Twelve
patients had bilateral CTS. There were median nerve
abnormalities in 19 wrist (9.5%) [15 (7.5%) bifid median
nerve, 4 (2%) persistent median artery].
Comparison of RA patients with and without CTS
groups
In RA group with CTS age, history of DM, disease dura-
tion, HAQ-DI score, CTS patient global score, Boston
symptom severity and functional status scores were ele-
vated compared to without CTS group (Table 4). CTS was
found in RA patients with secondary causes, respectively,
in 6 of 11 (54.5%) patients with DM, in 3 of 16 (18.8%)
patients with goitre, and in 7 of 20 (35%) patients with DM
and/or goitre. Although patients with CTS were elder and
had longer disease duration and higher HAQ-DI and Bos-
ton scores, no difference was found between groups in
acute phase reactants, extra-articular manifestations (nod-
ules, pulmonary involvement) and disease activity findings
(P [ 0.05) (Table 4). In sonographic evaluation, there was
no difference between the groups regarding joint cavity
widening, power Doppler signal increase, flexor tenosyn-
ovitis frequencies (P [ 0.05).
In the assessment of sensitivities of tests in CTS, sen-
sitivity of Katz hand diagram was found higher than Tinel
and Phalen tests (respectively, 100, 60.0, 66.7%).
There was no correlation between CSA of median nerve
and demographic and disease activity markers except for
age (r2 = 0.233, P = 0.02) and body mass index
(r2 = 220, P = 0.028).
Intra-observer variability of CSA of median nerve was
found as kappa score = 0.94.
In subgroup analysis, 31 wrists of 20 RA patients (CSA
between 10 and 13 mm2) were assessed with NCS. Twelve
wrists (38.7%) of 8 patients had CTS. There was no difference
between these subgroups (CTS (?) and (-) regarding age,
RA disease duration, DAS 28, acute phase reactants, HAQ-
DI, body mass index, CTS symptom score, CSA except for
Boston symptom severity and functional status scores
[respectively, 3.05 (1.90–4.27) vs. 1.55 (1.0–2.90),
P = 0.002; 3.25 (1.73–3.82) vs. 1.12 (1.0–2.10), P = 0.008].
Discussion
This is the first study assessing CTS frequency in RA with
high frequency US. CTS frequency was found as 17% in
RA. Twelve per cent of patients had bilateral CTS. This
frequency is higher than the previous studies. Carmona
Table 2 Laboratory, disease activity, damage and US findings of RA
patients
Characteristics
Tender joint count 2 (0–11)
Swollen joint count 1 (0–8)
RA patient global score,a 39.2 ± 19.5
ESR, mm/h 17 (2–86)
CRP, mg/L 7 (1–17.6)
Rheumatoid factor (RF) positivity, %b 71
Anti-CCP antibody positivity, %b 69
DAS 28 3.56 ± 1.15
Remission (\2.6), % 23
Mild activity (2.6–3.2), % 15
Moderate (3.2–5.1), % 52
Active (C5.1), % 10
Complete blood count
Leucocyte,/mm3 7,400 ± 2,700
Haemoglobin, g/dL 12.9 ± 1.5
Haematocrite, % 37.7 ± 4.0
Thrombocyte, 103/mm3 284 ± 79
HAQ-DI 1.25 ± 0.84
Arthritis in physical examination, n (%) 64 (32%)
Joint cavity widening with US
0(normal), n (%) 70 (35%)
1 (mild), n (%) 85 (42.5%)
2 (moderate, n (%) 31 (15.5%)
3 (severe), n (%) 14 (7%)
Power Doppler signal increase
0 (No signal), n (%) 145 (72.5%)
1 (mild), n (%) 41 (21.5%)
2 (moderate), n (%) 11 (5.5%)
3 (severe), n (%) 3 (1.5%)
Flexor tenosynovitis, n (%) 35/200 (17.5%)
Values are labelled as mean ± SD or median (minimum maximum),a Visual analogue scale (0–100 mm), b results in administrated
patients, ESR Erythtrocyte sedimentation rate, CRP C-reactive pro-
tein, CCP Cyclic citrullinated peptide, DAS 28 Disease activity score,
HAQ-DI Health assessment questionnaire disability index
2316 Rheumatol Int (2012) 32:2313–2319
123
et al. [16] had found CTS frequency 10.7%. Symptom-
atology of CTS plus Phalen and/or Tinel test positivity or
previous diagnosis with NCS or previous surgery was
accepted as CTS diagnosis. In nerve conduction studies
detecting neuropathies in patients with RA, CTS frequency
was found as 10.1 and 12.5% [17, 18]. Although NCS is the
mostly accepted method in assessing CTS, it is expensive,
time-consuming, partly invasive and could not be reachable
in centres [19]. It does not give information about aetiology
of CTS and structures in carpal tunnel. Moreover, in
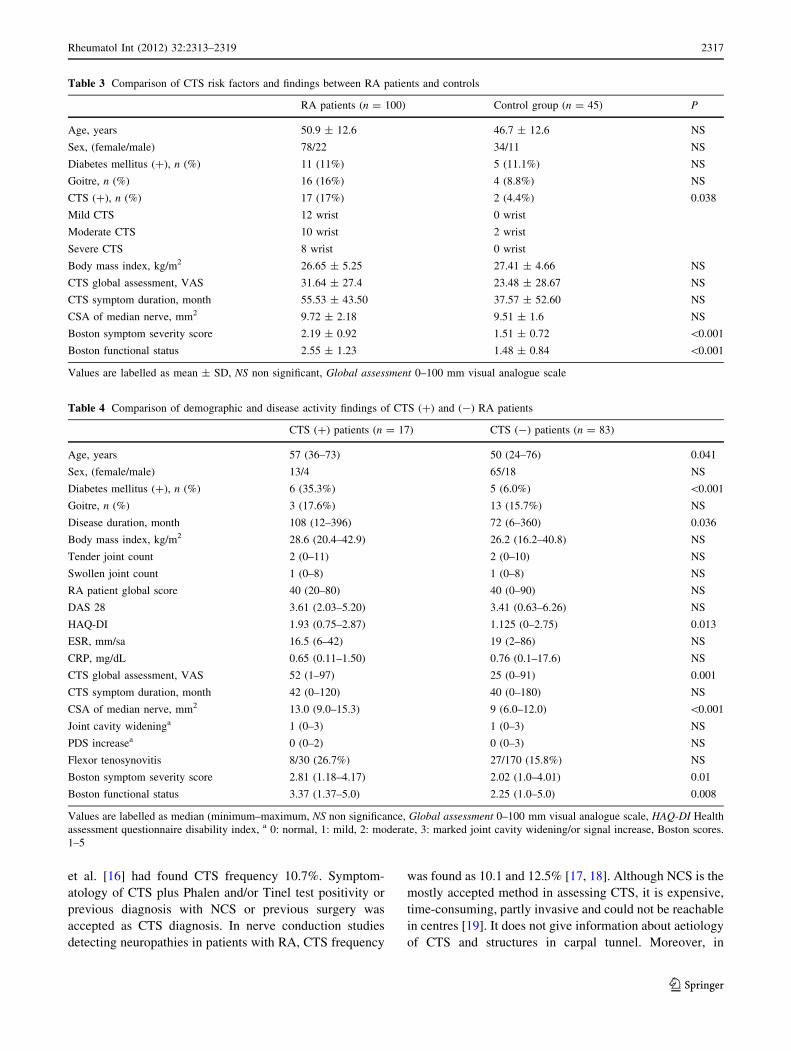
Table 3 Comparison of CTS risk factors and findings between RA patients and controls
RA patients (n = 100) Control group (n = 45) P
Age, years 50.9 ± 12.6 46.7 ± 12.6 NS
Sex, (female/male) 78/22 34/11 NS
Diabetes mellitus (?), n (%) 11 (11%) 5 (11.1%) NS
Goitre, n (%) 16 (16%) 4 (8.8%) NS
CTS (?), n (%) 17 (17%) 2 (4.4%) 0.038
Mild CTS 12 wrist 0 wrist
Moderate CTS 10 wrist 2 wrist
Severe CTS 8 wrist 0 wrist
Body mass index, kg/m2 26.65 ± 5.25 27.41 ± 4.66 NS
CTS global assessment, VAS 31.64 ± 27.4 23.48 ± 28.67 NS
CTS symptom duration, month 55.53 ± 43.50 37.57 ± 52.60 NS
CSA of median nerve, mm2 9.72 ± 2.18 9.51 ± 1.6 NS
Boston symptom severity score 2.19 ± 0.92 1.51 ± 0.72 \0.001
Boston functional status 2.55 ± 1.23 1.48 ± 0.84 \0.001
Values are labelled as mean ± SD, NS non significant, Global assessment 0–100 mm visual analogue scale
Table 4 Comparison of demographic and disease activity findings of CTS (?) and (-) RA patients
CTS (?) patients (n = 17) CTS (-) patients (n = 83)
Age, years 57 (36–73) 50 (24–76) 0.041
Sex, (female/male) 13/4 65/18 NS
Diabetes mellitus (?), n (%) 6 (35.3%) 5 (6.0%) \0.001
Goitre, n (%) 3 (17.6%) 13 (15.7%) NS
Disease duration, month 108 (12–396) 72 (6–360) 0.036
Body mass index, kg/m2 28.6 (20.4–42.9) 26.2 (16.2–40.8) NS
Tender joint count 2 (0–11) 2 (0–10) NS
Swollen joint count 1 (0–8) 1 (0–8) NS
RA patient global score 40 (20–80) 40 (0–90) NS
DAS 28 3.61 (2.03–5.20) 3.41 (0.63–6.26) NS
HAQ-DI 1.93 (0.75–2.87) 1.125 (0–2.75) 0.013
ESR, mm/sa 16.5 (6–42) 19 (2–86) NS
CRP, mg/dL 0.65 (0.11–1.50) 0.76 (0.1–17.6) NS
CTS global assessment, VAS 52 (1–97) 25 (0–91) 0.001
CTS symptom duration, month 42 (0–120) 40 (0–180) NS
CSA of median nerve, mm2 13.0 (9.0–15.3) 9 (6.0–12.0) \0.001
Joint cavity wideninga 1 (0–3) 1 (0–3) NS
PDS increasea 0 (0–2) 0 (0–3) NS
Flexor tenosynovitis 8/30 (26.7%) 27/170 (15.8%) NS
Boston symptom severity score 2.81 (1.18–4.17) 2.02 (1.0–4.01) 0.01
Boston functional status 3.37 (1.37–5.0) 2.25 (1.0–5.0) 0.008
Values are labelled as median (minimum–maximum, NS non significance, Global assessment 0–100 mm visual analogue scale, HAQ-DI Health
assessment questionnaire disability index, a 0: normal, 1: mild, 2: moderate, 3: marked joint cavity widening/or signal increase, Boston scores.
1–5
Rheumatol Int (2012) 32:2313–2319 2317
123

13–27% CTS patients, NCS is normal and additional
imaging methods are required [10]. It was shown that US
could be used in these patients [20].
High frequency US can assess structures in carpal tunnel
in addition to median nerve [5]. In CTS, enlargement of
median nerve occurs at the proximal site of compression.
Standardization of measurement of CSA was analysed, and
it was found 89% sensitive and 83% specific in detecting
CTS [3]. An algorithm evaluating CTS severity based on
CSA of median nerve was suggested [6].
It was shown that in patients with arthritis, CSA of
median nerve was increased [21]. The same study group
found CSA of median nerve in patients without CTS was
similar to healthy subjects [7]. But 10% of patients without
CTS, measures could overlap with that of mild CTS
(10.0–13.0 mm2). Additional NCS is recommended to this
subgroup.
Wrist arthritis and flexor tenosynovitis could bring
additional risk in CTS development [22]. High frequency
US could detect possible causes of CTS like flexor teno-
synovitis, median nerve abnormalities, persistent median
artery and accessory muscle [5]. We assessed joint cavity
widening and PDS increase in wrist joint. We could not
find a difference between the CTS (?) and (-) RA patients
in findings of arthritis, tenosynovitis and carpal tunnel
pathologies.
Rheumatoid arthritis disease activity and damage were
evaluated with tender and swollen joint count, patient
global assessment, DAS 28, acute phase reactants and
HAQ-DI. Whilst there was no difference in disease activity
parameters, disease duration and HAQ-DI were higher in
CTS group (P = 0.013). Agarwal et al. [17] found no
association with CTS and disease activity, duration and
HAQ score. Our patients had higher disease duration.
Longer disease duration could result with worse functional
status (high HAQ-DI). CTS might be partly reflects worse
functional status. Disease activity findings and acute phase
reactants reflect condition of a distinct period of disease.
Since there was no relation between disease activity and
patients with CTS had higher disease duration, worse
functional capacity might suggest CTS could develop in
chronic course.
RA patients and control group were similar in age, body
mass index, CTS risk factors. However, CTS frequency
was higher in RA (17% vs. 4.5%, P = 0.036). In subgroup
analysis 6 of 11 (54.5%) DM patients there were CTS. RA
patients with additional CTS risk factors (DM, goitre, older
age, obesity) should be carefully evaluated about CTS.
Weight loss and life style changes could suggest to these
patients to prevent CTS.
There are additional tests and questionnaires widely
used in CTS like (Tinel and Phalen tests, Katz hand dia-
gram and Boston CTS questionnaire [8, 15]. But we could
not find a study that had used these tests in RA. In our
study, sensitivity and specificity of Katz hand diagram was
higher than Tinel and Phalen tests. Also Katz hand diagram
is simple and gives opportunity to better localization of
symptoms. Thus, Katz hand diagram could be a screening
test in assessing CTS in RA patients.
Boston CTS questionnaire is widely used in evaluating
treatment response in CTS. Both symptom severity and
functional status scores were higher in CTS group. Another
aim of our study was to determine patients with CSA
10–13 mm2. Boston scores were found higher in CTS (?)
subgroup. Although NCS is suggested to this subgroup,
higher Boston CTS scores might give idea about CTS in
this group.
Limitations
US do not give information about peripheral neuropathy,
radiculopathy and other entrapment neuropathies.
Conclusion
CTS frequency in RA is found higher than normal popu-
lation, especially in patients with additional risk factors of
CTS. There was no relationship between CTS and disease
activity, and CTS group had long disease duration and
worse functional status. CTS could be a result of the
chronic course in RA. In patients with CSA between 10 and
13 mm2, Boston CTS questionnaire might give additional
idea about CTS.
Conflicts of interest none.
References
1. Young A, Koduri G (2007) Extra-articular manifestations and
complications of rheumatoid arthritis. Best Pract Res Clin
Rheumatol 21(5):907–927
2. Jablecki CK, Andary MT, Floeter MK, Miller RG, Quartly CA,
Vennix MJ, Wilson JR; American Association of Electrodiag-
nostic Medicine; American Academy of Neurology; American
Academy of Physical Medicine and Rehabilitation (2002) Prac-
tice parameter: Electrodiagnostic studies in carpal tunnel syn-
drome. Report of the American Association of Electrodiagnostic
Medicine, American Academy of Neurology, and the American
Academy of Physical Medicine and Rehabilitation. Neurology
58(11):1589–1592
3. Wong SM, Griffith JF, Hui AC, Tang A, Wong KS (2002) Dis-
criminatory sonographic criteria for the diagnosis of carpal tunnel
syndrome. Arthritis Rheum 46(7):1914–1921
4. McQueen FM, Ostergaard M (2007) Established rheumatoid
arthritis–new imaging modalities. Best Pract Res Clin Rheumatol
21(5):841–856
5. Filippucci E, Iagnocco A, Meenagh G, Riente L, Delle Sedie A,
Bombardieri S, Valesini G, Grassi W (2006) Ultrasound imaging
for the rheumatologist II. Ultrasonography of the hand and wrist.
Clin Exp Rheumatol 24(2):118–122
2318 Rheumatol Int (2012) 32:2313–2319
123

6. El Miedany YM, Aty SA, Ashour S (2004) Ultrasonography
versus nerve conduction study in patients with carpal tunnel
syndrome: substantive or complementary tests? Rheumatology
(Oxford) 43(7):887–895
7. Hammer HB, Haavardsholm EA, Kvien TK (2007) Ultrasono-
graphic measurement of the median nerve in patients with
rheumatoid arthritis without symptoms or signs of carpal tunnel
syndrome. Ann Rheum Dis 66(6):825–827
8. D’Arcy CA, McGee S (2000) The rational clinical examination.
Does this patient have carpal tunnel syndrome? JAMA
283(23):3110–3117
9. Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG,
Fossel AH, Katz JN (1993) A self-administered questionnaire for
the assessment of severity of symptoms and functional status in
carpal tunnel syndrome. J Bone Joint Surg Am 75(11):1585–1592
10. Aroori S, Spence RA (2008) Carpal tunnel syndrome. Ulster Med
J 77(1):6–17
11. Sezgin M, Incel NA, Serhan S, Camdeviren H, As I, Erdogan C
(2006) Assessment of symptom severity and functional status in
patients with carpal tunnel syndrome: reliability and functionality
of the Turkish version of the Boston Questionnaire. Disabil
Rehabil 28(20):1281–1285
12. Brown AK, Quinn MA, Karim Z, Conaghan PG, Peterfy CG,
Hensor E, Wakefield RJ, O’Connor PJ, Emery P (2006) Presence
of significant synovitis in rheumatoid arthritis patients with dis-
ease-modifying antirheumatic drug-induced clinical remission:
evidence from an imaging study may explain structural pro-
gression. Arthritis Rheum 54(12):3761–3773
13. Filippucci E, Iagnocco A, Salaffi F, Cerioni A, Valesini G, Grassi
W (2006) Power Doppler sonography monitoring of synovial
perfusion at the wrist joints in patients with rheumatoid arthritis
treated with adalimumab. Ann Rheum Dis 65(11):1433–1437
14. Practice parameter for carpal tunnel syndrome (summary state-
ment) (1993) Report of the quality standards subcommittee of the
American academy of neurology. Neurology 43(11):2406–2409
15. Padua L, Pazzaglia C, Caliandro P, Granata G, Foschini M,
Briani C, Martinoli C (2008) Carpal tunnel syndrome: ultrasound,
neurophysiology, clinical and patient-oriented assessment. Clin
Neurophysiol 119(9):2064–2069
16. Carmona L, Gonzalez-Alvaro I, Balsa A, Angel Belmonte M,
Tena X, Sanmartı R (2003) Rheumatoid arthritis in Spain:
occurrence of extra-articular manifestations and estimates of
disease severity. Ann Rheum Dis 62(9):897–900
17. Agarwal V, Singh R, Wiclaf F, Chauhan S, Tahlan A, Ahuja CK,
Goel D, Pal L (2008) A clinical, electrophysiological, and path-
ological study of neuropathy in rheumatoid arthritis. Clin Rheu-
matol 27(7):841–844
18. Lanzillo B, Pappone N, Crisci C, di Girolamo C, Massini R,
Caruso G (1998) Subclinical peripheral nerve involvement in
patients with rheumatoid arthritis. Arthritis Rheum 41(7):1196–
1202
19. Ziswiler HR, Reichenbach S, Vogelin E, Bachmann LM, Villiger
PM, Juni P (2005) Diagnostic value of sonography in patients
with suspected carpal tunnel syndrome: a prospective study.
Arthritis Rheum 52(1):304–311
20. Koyuncuoglu HR et al (2005) The value of ultrasonographic
measurement in carpal tunnel syndrome in patients with negative
electrodiagnostic tests. Eur J Radiol 56(3):365–369
21. Hammer HB, Hovden IA, Haavardsholm EA, Kvien TK (2006)
Ultrasonography shows increased cross-sectional area of the
median nerve in patients with arthritis and carpal tunnel syn-
drome. Rheumatology (Oxford) 45(5):584–588
22. Khurana R, Berney SM (2005) Clinical aspects of rheumatoid
arthritis. Pathophysiology 12(3):153–165
Rheumatol Int (2012) 32:2313–2319 2319
123






















![[18'] Carpal](https://img.pdfslide.us/doc/110x75/577d20351a28ab4e1e924083/18-carpal.jpg)



