Embed Size (px)
Citation preview

Dyslexia Plan
2007-2008

Table of Contents
I. Definition of Dyslexia 3
II. Screening for Dyslexia 3
III. Referral Process 4
IV. Assessment of Dyslexia 5
V. English Language Learners 6
VI. Committee of Knowledgeable Persons 7
VII. Program Entrance Criteria 9
VIII.Program Description & Options 12
IX. Timeline 14
X. Program Exit Criteria 14
XI. Monitoring of Students 15
XII. District Contacts 15
XIII. Flow Chart 17
XIV. Forms 18
2

Definition of DyslexiaAs defined in Texas Education Code §38.003
(1) “Dyslexia” means a disorder of constitutional origin manifested by a difficulty in learning to read, write, or spell, despite conventional instruction, adequate intelligence, and sociocultural opportunity.
(2) “Related disorders” includes disorders similar to or related to dyslexia such as developmental auditory imperception, dysphasia, specific developmental dyslexia, developmental dysgraphia, and developmental spelling disability.
The definition of the International Dyslexia Association states:
Dyslexia is a specific learning disability that is neurological in origin. It is characterized by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in the phonological component of language that is often unexpected in relation to other cognitive abilities and the provision of effective classroom instruction. Secondary consequences may include problems in reading comprehension and reduced reading experience that can impede growth of vocabulary and background knowledge. (Adopted by the International Dyslexia Board of Directors, November 12, 2002).
The primary difficulties of a student identified as having dyslexia occur in phonemic awareness and manipulation, single-word decoding, reading fluency, and spelling. Secondary consequences of dyslexia may include difficulties in reading comprehension and/or written expression. These difficulties are unexpected for the student’s age, educational level, or cognitive abilities. Additionally, there is often a family history of similar difficulties.
Screening for DyslexiaIn accordance with TEC §28.006, Decatur I.S.D. administers early reading instruments in kindergarten, first, and second grades to determine students’ reading development and comprehension. If, on the basis of the reading instrument results, students are determined to be at risk for dyslexia and other reading difficulties, the students’ parents/guardians are notified. In addition, an accelerated (intensive) reading program that appropriately addresses students’ reading difficulties and enables them to “catch up” with their typically performing peers is implemented. Should students continue to struggle with reading, writing, and spelling during the intensive reading instruction, then Decatur I.S.D. will initiate procedures to recommend these students for assessment for dyslexia. The information from the early reading instruments will be one source of information in deciding whether or not to recommend a student for assessment for dyslexia.
3

Screening for dyslexia of students in grades 3 – 12 may include, but is not limited to: performance on state mandated test(s), a student’s grades/performance in reading, writing and spelling, and teachers’ observations of the characteristics of dyslexia. This information will be utilized when deciding whether or not to recommend a student for assessment for dyslexia.
Referral Process At any time that a student continues to struggle with one or more components of reading, Decatur I.S.D. will collect additional information about the student. The information will be used to evaluate the student’s academic progress and determine what actions are needed to ensure the student’s improved academic performance. Information to be considered includes the results from some or all of the following:
Vision screening Hearing screening Teacher reports of classroom concerns Data-based documentation of student progress during instruction - Response to
Intervention(RtI) Academic progress reports and/or report cards Samples of school work Parent conferences Testing for limited English proficiency The K-2 reading instrument as described in TEC §28.006 State student assessment program as described in TEC §39.002
Among the actions that Decatur I.S.D. has available for the student is a recommendation that the student be assessed for dyslexia. Decatur I.S.D. recommends assessment for dyslexia if the student demonstrates the following:
Poor performance in one or more areas of reading and the related area of spelling that is unexpected for the student’s age/grade, and;
Characteristics of dyslexia.
Primary Reading/Spelling Characteristics of Dyslexia:
Difficulty reading real words in isolation Difficulty accurately decoding nonsense words Slow, inaccurate, or labored oral reading (lack of reading fluency) Difficulty with learning to spell
The reading/spelling characteristics are the result of difficulty with the following: The development of phonological awareness, including segmenting, blending, and
manipulating sounds in words Learning the names of letters and their associated sounds Phonological memory (holding information about sounds and words in memory)
4

Rapid naming of familiar objects, colors, or letters of the alphabet
Secondary consequences of dyslexia may include the following: Variable difficulty with aspects of reading comprehension Variable difficulty with aspects of written composition A limited amount of time spent in reading activities
The Student Assistance Team will evaluate the collected data and make a recommendation for further assessment when these criteria are met.
Assessment of DyslexiaStudents enrolling in Decatur I.S.D. shall be assessed for dyslexia and related disorders at appropriate times (TEC §38.003(a)). The appropriate time depends upon multiple factors including the student’s reading performance, reading difficulties, poor response to supplemental, scientifically based reading instruction, teachers’ input, and parents’ or guardians’ input. Additionally, the appropriate time for assessing is early in a student’s school career (19 TAC §74.28), the earlier the better. While earlier is better, students will be recommended for assessment for dyslexia even if the reading difficulties appear later in a student’s school career.
The procedures followed for assessment include:1. Notify parents or guardians of proposal to assess student for dyslexia2. Inform parents or guardians of their rights under §5043. Obtain parent or guardian permission to assess the student for dyslexia4. Assess student, being sure that individuals/professionals who administer assessments have training in the evaluation of students for dyslexia and related disorders (19 TAC §74.28).
Tests, assessments, and other evaluation materials will (§504): Be validated for the specific purpose for which they are used Include material tailored to assess specific areas of educational need and not merely
materials that are designed to provide a single general intelligence quotient Be selected and administered so as to ensure that, when a test is given to a student with
impaired sensory, manual, or speaking skills, the test results accurately reflect the student’s aptitude or achievement level, or whatever other factor the test purports to measure, rather than reflecting the student’s impaired sensory, manual, or speaking skills
Include multiple measures of a student’s reading abilities such as informal assessment information. Be administered by trained personnel and in conformance with the instructions provided by the producer of the evaluation materials
Assessment of Special Education Students
If a student is already in special education, but exhibits the characteristics of dyslexia or related disorders and is referred for assessment, assessment procedures for students under the Individuals with Disabilities Act (IDEIA 2004) will be followed. Assessment data from prior special
5

education assessments may be utilized, and/or additional assessment may be conducted by personnel trained in assessment to evaluate students for dyslexia and related disorders. In this case, the ARD committee will serve as the committee of knowledgeable persons.
Assessment of Students Identified Outside the District
Students identified as having dyslexia or related disorders from an outside source will be evaluated for eligibility in the district’s program. Decatur I.S.D. may choose to accept the outside assessment, or may re-assess the student. In either situation, the committee of knowledgeable persons will determine the identification status of a student enrolled in Decatur I.S.D., and the placement of the student in the dyslexia program(s).
Domains to Assess
Decatur I.S.D. administers measures that are related to the student’s educational needs. Depending upon the student’s age and stage of reading development, the following are the areas related to reading that should be assessed:
Reading real and nonsense words in isolation (decoding) Phonological awareness Letter knowledge (name and associated sound) Rapid naming Reading fluency (rate and accuracy) Reading comprehension Written spelling
Based on the student’s academic difficulties and characteristics, additional areas that can be assessed include vocabulary, written expression, handwriting, and mathematics.
English Language Learners (This refers to students served in Bilingual and ESL programs as well as students designated Limited English Proficient (LEP) whose parents have denied services.)Much diversity exists among English Language Learners (ELLs). The identification and service delivery process for dyslexia must be in step with the student’s linguistic environment and educational background. In Decatur I.S.D., the LPAC (Language Proficiency Assessment Committee) will be involved in the decision making process.
Additional data to be gathered when assessing English Language Learners: Language Proficiency Assessment Committee (LPAC) documentation which includes the
following:o Home language surveyo Assessment related to identification for limited English proficiency (oral language proficiency tests
and norm-referenced tests)o TAKS documentation when available
6

o Texas English Language Proficiency system (TELPAS) information (Reading Proficiency Test in English (RPTE) and Texas Observation Protocol (TOP)).
o Type of language programming provided and language of instructiono Linguistic environment and second-language acquisition developmento Previous schooling in and outside of the United States.
Additional assessment when assessing English Language Learners: Comprehensive oral language proficiency testing should be completed in English and the
student’s native language whenever possible If the student has received academic instruction in his/her native language, as well as
English, then the “Domains to Assess” need to be completed in both languages to the appropriate extent.
Interpretation:Test results of English Language Learners will be interpreted in light of the student’s: language development (in both English and the student’s native language), educational history, linguistic background, socioeconomic issues, and any other pertinent factors that affect learning.
Committee of Knowledgeable PersonsA team or committee of knowledgeable persons determines whether the student has dyslexia. The team must be knowledgeable about:
The student being assessed The reading process Dyslexia and related disorders Dyslexia instruction District or charter school, state, and federal guidelines for assessment The assessments used The meaning of the collected data
This committee determines the identification of dyslexia after reviewing all accumulated data including the following areas:
The observations of the teacher, district or charter school staff, and/or parent/guardian Data gathered from the classroom (including student work and the results of classroom
measures) and information found in the student’s cumulative folder (including the developmental and academic history of the student)
Data-based documentation of student progress during instruction/intervention (Response to Intervention – RtI)
Language Assessment Proficiency Committee (LPAC) documentation, when applicable The results of administered assessments All other accumulated data regarding the development of the student’s learning and his/her
educational needs
7

The student’s difficulties in the area of reading will reflect one or more of the primary characteristics of dyslexia with unexpectedly low performance for the student’s age and educational level in the following areas:
Reading real words in isolation Decoding nonsense words Reading fluency (both rate and accuracy) Written spelling (an isolated difficulty in spelling would not be sufficient to identify
dyslexia)
This unexpectedly low reading performance will be the result of a deficit in phonological processing, including the following:
Phonological awareness Rapid naming Phonological memory
Many students with dyslexia will have difficulty with the secondary characteristics of dyslexia, including reading comprehension and written composition.
The committee of knowledgeable persons will also incorporate the following guidelines from TEC §38.003 and 19 TAC §74.28:
The student has received conventional (appropriate) instruction The student has an unexpected lack of appropriate academic progress (in the areas of
reading and spelling) The student has adequate intelligence (an average ability to learn in the absence of print or
in other academic areas) The student exhibits characteristics associated with dyslexia The student’s lack of progress is not due to sociocultural factors such as language
differences, irregular attendance, or lack of experiential background.
If the committee determines that the student has dyslexia, the committee of knowledgeable persons also determines whether the student has a disability under the Rehabilitation Act of 1973, §504. Not all students with dyslexia are automatically eligible for §504. A student is considered to have a disability under §504 if the condition substantially limits the student’s learning. Students with additional factors that complicate their dyslexia may require additional support or referral to special education. (See Flow Chart)
At any time during the assessment for dyslexia, identification process, or instruction related to dyslexia, students may be referred for evaluation for special education. At times, students will display additional factors/areas complicating their dyslexia and requiring more support than what is available through dyslexia instruction. At other times, students with severe dyslexia or related disorders will be unable to make adequate academic progress within any of the programs for dyslexia or related disorders. In such cases, a referral to special education for evaluation and possible identification as a child with a disability within the Individuals with Disabilities Improvement Act of 2004 (IDEIA) will be made as needed.
8

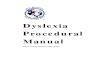
Characteristic Profile of Dyslexia – Revised 2007
NAME: DATE OF BIRTH: AGE:
SCHOOL: DATE OF TEST: GRADE:
Percentile 1 5 10 20 30 40 50 60 70 80 90 99
Standard Score 55 70 85 100 115 130
UNDERLYING CAUSE: PHONOLOGICAL PROCESSING BELOW AVERAGE
Below 90AVERAGE
90 - 109ABOVE AGEVAGE
110+
PHONOLOGICAL AWARENESS
Phonological Memory RAPID NAMING
Letter Knowledge
CHARACTERISTICS DECODING
WORD RECOGNITION
ORAL READING FLUENCY RATE ACCURACY
SPELLING
OUTCOMES: Variable Impact READING COMPREHENSION
Written Expression
COGNITIVE/ACADEMIC ABILITY
COEXISTING COMPLICATIONS OR ASSETSCOMPLICATION ASSET
Oral Language
Attention
Mathematics
Handwriting
Behavior / Emotions
“Dyslexia is a specific learning disability that is neurological in origin. It is characterized by difficulties with accurate and /or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in the phonological component of language that is often unexpected in relation to other cognitive abilities and the provision of effective classroom instruction. Secondary
9

consequences may include problems in reading comprehension and reduced reading experience that can impede growth of vocabulary and background knowledge.” Adopted by the Board of Directors, International Dyslexia Association, November 2002.
Texas Scottish Rite Hospital for Children 1995-2007, Gladys Kolenovsky, M. A.Please see back for Application Guidelines
10

Application of a Definition-Based Processto the Identification of Dyslexia – Revised 2007
For the identification of dyslexia in Texas public schools, all procedures and guidelines outlined in The Dyslexia Handbook – Revised 2007 should be followed, including data gathering, parent notification, examiner qualifications, test selection and administration, and procedures for English language learners. The Dyslexia Handbook – Revised 2007 is available in electronic format at www.region10.org/dyslexia/Documents/Dyslexia Handbook2007English.pdf
The following procedures provide support for the use of the Characteristic Profile of Dyslexia – Revised 2007 as a tool in the identification of dyslexia.
A. Test all dyslexia UNDERLYING CAUSE, CHARACTERISTIC and OUTCOME skills listed in all CAPs on the profile and test additional skills as needed for individual students.
B. Utilize norm-referenced tests and report standard scores whenever possible. Criterion-referenced, screening, and achievement group test scores are informative as historical, secondary, or response to intervention progress measures, but are weaker dyslexia identification tools if they are the only measure of a skill.
C. Plot test scores on profile. Utilize X for norm-referenced standardized tests results and √ for criterion, group or screening measures. Include test standard scores along left margin for reference. Test names may also be noted. Plot parent and teacher observations from questionnaires with P and T.
D. Use individual subtest scores rather than composite or cluster scores.Examples: Consider both the Elision and Blending Words scores on the CTOPP rather than the Phonological Awareness composite. Plot both the Rate and Accuracy subtest from the GORT rather than the Fluency Composite or Oral Reading Quotient. Always consider the subscales of an intelligence or ability test.
E. Apply the following differential identification questions in sequence.1. Does the student demonstrate one or more of the primary reading characteristics of
dyslexia in addition to a spelling deficit?2. Are the reading and spelling difficulties the result of a phonological processing deficit?3. Are the reading, spelling and phonological processing deficits unexpected? Does the
student demonstrate cognitive ability to support age level academic learning?4. Are there secondary characteristics of dyslexia evident in reading comprehension and
written expression?5. Does the student have strengths that could be assets. Are there coexisting deficits
that may complicate identification and the response to intervention and may deserve further assessment and intervention?
Detailed guidance for the interpretation of these differential questions is available in The Dyslexia Handbook – Revised 2007 and in the companion to this profile, The Thinking Person’s Step-by-Step Identification Process for Dyslexia – Revised 2007. For training information on the use of this profile, contact Texas Scottish Rite Hospital for Children, Dyslexia Identification Seminar, 214-559-7800 or www.tsrhc.org.

Program Description & OptionsOnce it has been determined that a student has dyslexia, Decatur I.S.D. shall provide an appropriate instructional program for the student (TEC §38.003). The following procedures will be followed:
Instructional decisions for a student with dyslexia are made by a team that is knowledgeable about the student, the meaning of the evaluation information, and instructional components and approaches for students with dyslexia.
Decatur I.S.D. has adopted the Texas Scottish Rite Take Flight: A Comprehensive Intervention for Students with Dyslexia. as the instructional program to be used with students identified as Dyslexic. The curriculum teaches students with dyslexia specific strategies and techniques to compensate for the difficulties they will encounter.
Decatur I.S.D. will provide each identified student access at his/her campus to the services of a teacher trained in dyslexia and related disorders. The district may, with the approval of each student’s parents or guardians, offer additional services at a centralized location. Such centralized services shall not preclude each student from receiving services at his or her campus (19 TAC§ 74.28).
Parents/guardians of students eligible under the Rehabilitation Act of 1973, §504, will be informed of all services and options available to the student under that federal statute.
Teachers who provide the appropriate instruction for students with dyslexia will be trained in the professional development activities specified by the district and/or campus decision making committee. As stated in 19 TAC, §74.28, the teachers who provide appropriate instruction for students with dyslexia must be trained and be prepared to implement instructional strategies that utilize individualized, intensive, multisensory, phonetic methods and a variety of writing and spelling components. They may serve as trainers and consultants in the area of dyslexia and related disorders to regular, remedial, and special education teachers.
Decatur I.S.D. will provide a parent education program for the parents/guardians of students with dyslexia and related disorders. The program will include:
Characteristics of dyslexia and related disorders Information on assessment and diagnosis of dyslexia Information on effective strategies for teaching students with dyslexia Awareness of information on classroom accommodations and especially of
accommodations allowed on standardized testing (19 TAC §74.28)
12

Components of InstructionThe instructional program will be offered in a small class setting and include reading, writing, and spelling as appropriate. The major instructional strategies will utilize individualized, intensive, and multisensory methods as appropriate. Components of instruction, as appropriate for the reading needs of the student, include:
Phonemic awareness instruction that enables students to detect, segment, blend, and manipulate sounds in spoken language
Graphophonemic knowledge (phonics) instruction that takes advantage of the letter-sound plan in which words that carry meaning are made of sounds and sounds are written with letters in the right order. Students with this understanding can blend sounds associated with letters into words and can separate words into component sounds for spelling and writing
Language structure instruction that encompasses morphology (the study of meaningful units of language such as prefixes, suffixes, and roots), semantics (ways that language conveys meaning), syntax (sentence structure), and pragmatics (how to use language in a particular context)
Linguistic instruction directed toward proficiency and fluency with patterns of language so that words and sentences are carriers of meaning
Strategy-oriented instruction in the strategies students use for decoding, encoding, word recognition, fluency, and comprehension that students need to become independent readers
Instructional approaches, as appropriate to meet the instructional needs of the student, include:
Explicit, direct instruction that is systematic (structured), sequential, and cumulative. Instruction is organized and presented in a way that follows a logical sequential plan, fits the nature of language (alphabetic principle) with no assumption of prior skills or language knowledge, and maximizes student engagement. This instruction proceeds at a rate commensurate with students’ needs, ability levels, and demonstration of progress
Individualized instruction that meets the specific learning needs of each individual student in a small group setting; a reading curriculum that matches each student’s individual ability level and contains all of the Components of Instruction mandated in 19 TAC §74.28
Intensive, highly concentrated instruction that maximizes student engagement, uses specialized methods and materials, produces results, and contains all the components of instruction mandated in 19 TAC §74.28
13

Meaning-based instruction that is directed toward purposeful reading and writing, with an emphasis on comprehension and composition
Multisensory instruction that incorporates the simultaneous use of two or more sensory pathways (auditory, visual, kinesthetic, tactile) during teacher presentations and student practice
Decatur I.S.D. utilizes the following programs:
Take Flight: A Comprehensive Intervention for Students with Dyslexia.
TimelineThe following timeline applies to students in regular education programs, or who may qualify as §504:
-Upon receipt of parent permission to assess until assessment is completed shall be 30 school days or less.-From the completion of the assessment to the committee of knowledgeable persons meeting for determination of dyslexia and program placement shall be 30 school days or less.-Following the committee of knowledgeable persons meeting until program begins (if it is determined the student is eligible for the dyslexia program) shall be 30 school days or less.
Special education students shall follow the timelines required by federal law, under IDEIA 2004.
Program Exit CriteriaUpon successful completion of the district dyslexia program(s), as measured by program mastery checks (assessments) completed at regular intervals, students will be exited from the district dyslexia program(s). Additional criteria for exit may include but is not limited to: grades from progress reports or report cards, state assessment data, benchmarks, teacher and/or parent observations/checklists, and individual dyslexia program requirements.
Program Exit CriteriaTake Flight: A Comprehensive Intervention for Students with Dyslexia.
Upon completion of the two year program.
14

MonitoringStudents that have been dismissed (exited) from the Decatur I.S.D. dyslexia program will receive regular monitoring. These checks will occur as follows:
Time after Dismissal Monitoring IntervalFirst Year Once a six weeksSecond Year Once a semesterThird Year and Beyond Annually each May
Monitoring may include, but is not limited to the collection/evaluation of:-progress reports-report cards-state assessment data-teacher reports/checklists-parent reports/checklists-counselor reports-other program reports-additional assessment data
Students qualifying for dyslexia services that are identified as §504 or Special Education will follow monitoring/re-evaluation requirements outlined in federal law.
Contacts for Dyslexia
Location Name Phone NumberDecatur I.S.D. District Office
Cassandra Darst 940-393-7260
Carson Elementary Carol Donovan 940-393-7500Rann Elementary Sharon Montgomery 940-393-7600Decatur Intermediate Shana Howland 940-393-7400Decatur High School Cassandra Darst 940-393-7260
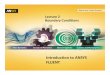
Flow ChartThe process for assessment, identification, and instruction for students with dyslexia is represented in the following visual for ease of use. It is not meant to represent every aspect of the Decatur I.S.D. dyslexia process, but should give a general overview of the district procedures.
15

Decatur I.S.D. does not discriminate on the basis of age, color, creed, disability, marital status, veteran status, national origin, race, or gender in the educational programs and activities which it operates.
Flow Chart for Dyslexia2007 Handbook
16

Parents (or guardians) of students in Grades K, 1, and 2 will be notified if the student is determined to be at-risk for dyslexia or other reading difficulties (TEC Section 28.006)Parents (or guardians may request dyslexia assessment or Special Education evaluation at any time.
Student exhibits poor performance on early reading assessment. (1)OR Student fails to respond to scientifically-based reading instruction at any grade.
Classroom teacher intensifies reading instruction and provides classroom accommodations.
Teacher monitors reading progress.
Student is provided more intensive intervention in addition to the core reading instruction.
Teacher monitors reading progress. (2)
Student makes reading progress Student does not make adequate reading progress AND The student exhibits characteristics of dyslexia.
(Campus committee of knowledgeable persons should consider all collected information.
Student is reintegrated into traditional reading instruction in the classroom
Special education evaluation should be
conducted whenever it appears to be
appropriate. Some students will NOT
proceed through all steps before being referred for
a Full Individual Evaluation (FIE). A
dyslexia evaluation may be incorporated into the FIE completed through
Special Education.
Student has characteristics of dyslexia. Direct, systematic
and intensive reading instruction is provided.
Student recommended for dyslexia assessment. Section 504 procedures must be followed (Notification of evaluation, parent informed of rights under 504, and permission to assess).
Student does not have characteristics of dyslexia.
Student makes adequate reading progress. Student does not make adequate reading progress
---------------------------------------------------------------------------------------------------------
Tier 1
---------------------------------------------------------------------------------------------------------
Tier 2
Tier 3
Need for 504 accommodations is considered, including TAKS accommodations for students with dyslexia.
17

Forms forDecatur I.S.D.
Dyslexia Program
18

NOTICE OF RIGHTS FOR DISABLED STUDENTS AND THEIR PARENTS UNDER §504 OF THE REHABILITATION ACT OF 1973
The Rehabilitation Act of 1973, commonly known in the schools as ''Section 504,'' is a federal law passed by the United States Congress with the purpose of prohibiting discrimination against disabled persons who may participate in, or receive benefits from, programs receiving federal financial assistance. In the public schools specifically, §504 applies to ensure that eligible disabled students are provided with educational benefits and opportunities equal to those provided to non-disabled students. Under §504, a student is considered ''disabled'' if he or she suffers from a physical or mental impairment that substantially limits one or more of their major life activities, such as learning, walking, seeing, hearing, breathing, working, and performing manual tasks. Section 504 also applies to students with a record of having a substantially-limiting impairment, or who are regarded as being disabled even if they are truly not disabled. Students can be considered disabled, and can receive services under §504, even if they do not qualify for, or receive, special education services. The purpose of this Notice is to inform parents and students of the rights granted them under §504. The federal regulations that implement §504 are found at Title 34, Part 104 of the Code of Federal Regulations (CFR) and entitle parents of eligible students, and the students themselves, to the following rights:
1. You have a right to be informed about your rights under §504. [34 CFR 104.32] The School District must provide you with written notice of your rights under §504 (this document represents written notice of rights as required under §504). If you need further explanation or clarification of any of the rights described in this Notice, contact appropriate staff persons at the District's § 504 Office and they will assist you in understanding your rights.
2. Under §504, your child has the right to an. appropriate education designed to meet his or her educational needs as adequately as the needs of non-disabled students are met. [34 CFR 104.33].
3. Your child has the right to free educational services, with the exception of certain costs normally also paid by the parents of non-disabled students. Insurance companies and other similar third parties are not relieved of any existing obligation to provide or pay for services to a student that becomes eligible for services under §504. [34 CFR 104.33].
4. To the maximum extent appropriate, your child has the right to be educated with children who are not disabled. Your child will be placed and educated in regular classes, unless the District demonstrates that his or her educational needs cannot be adequately met in the regular classroom, even with the use of supplementary aids and services. [34 CFR 104.34].
5. Your child has the right to services, facilities, and activities comparable to those provided to non-disabled students. [34 CFR 104.34].
6. The School District must undertake an evaluation of your child prior to determining his or her appropriate educational placement or program of services under §504, and also before every subsequent significant change in placement. [34 CFR 104.35].
19

7. If formal assessment instruments are used as part of an evaluation, procedures used to administer assessments and other instruments must comply with the requirements of §504 regarding test validity, proper method of administration, and appropriate test selection, [34 CFR 104.35]. The District will consider information from a variety of sources in making its determinations, including, for example: aptitude and achievement tests, teacher recommendations, reports of physical condition, social and cultural background, adaptive behavior, health records, report cards, progress notes, parent observations, and scores on TAKS tests, among others. [34 CFR 104.35].
8. Placement decisions regarding your child must be made by a group of persons (a §504 committee) knowledgeable about your child, the meaning of the evaluation data, possible placement options, and the requirement that to the maximum extent appropriate, disabled children should be educated with non-disabled children. [34 CFR 104.35].
9. If your child is eligible for services under §504, he or she has a right to periodic evaluations to determine if there has been a change in educational need. Generally, an evaluation will take place at least every three years. [34 CFR 104.35].
10. You have the right to be notified by the District prior to any action regarding the identification, evaluation, or placement of your child. [34 CFR 104.36].
11. You have the right to examine relevant documents and records regarding your child (generally documents relating to identification, evaluation, and placement of your child under §504). [34 CFR 104.36].
12. You have the right to an impartial due process hearing if you wish to contest any action of the District with regard to your child's identification, evaluation, or placement under §504. [34 CFR 104.36]. You have the right to participate personally at the hearing, and to be represented by an attorney, if you wish to hire one.
13. If you wish to contest an action taken by the §504 Committee by means of an impartial due process hearing, you must submit a Notice of Appeal or a Request for Hearing to the District's §504 Coordinator at the address below:
Cassandra DarstDISD 504 Coordinator, 940-627-7391 501 East Collins, Decatur TX 76234
A date will be set for the hearing and an impartial hearing officer will be appointed. You will then be notified in writing of the hearing date, time, and place.
14. If you disagree with the decision of the hearing officer, you have a right to seek a review of that decision before a court of competent jurisdiction (normally, your closest federal district court).
20

15. With respect to other issues surrounding your child's education that do not specifically involve identification, evaluation, or placement, you have a right to present a grievance or complaint to the District's §504 Coordinator (or their designee), who will then investigate the situation, taking into account the nature of the complaint and all necessary factors, in an effort to arrive at a fair and speedy resolution.
16. You also have a right to file a complaint with the Office for Civil Rights (OCR) of the Department of Education. The address of the OCR Regional Office that covers Texas is:
Director Office for Civil Rights, Region VI 1999 Bryan Street, Suite 2600
Dallas, Texas 75201 Tel. (214) 880-2459
My signature below indicates I have received this notice and understand its contents.
____________________________________________________________________________________________________________Date Signed Signature of Parent, Surrogate Parent, Guardian, or Adult Student Date Signed
____________________________________________________________________________________________________________Date Signed Signature of Interpreter, if used Date Signed
21

AVISO A PADRES DE ESTUDIANTES INCAPACITADOS DE SUS DERECHOS LEGALES BAJO LA SECCION 504 DEL DECRETO DE
REHABILITACION DE 1973 El Decreto de Rehabilitación de 1973, conocido generalmente como la ''Sección 504,'' es una ley federal legislada por el Congreso de los Estados Unidos. El propósIto de esta ley es de prohibir discriminación contra estudiantes incapacitados y asegurar que tengan oportunidades y beneficios educativos tan adequados como los de estudiantes sin incapacidades. Bajo la Sección 504, un estudiante es considerado incapacitado si padece de un impedimento o condición física o mental que limita substanciálmente una de sus actividades vitales, como la de aprender, caminar, ver, oir, hablar, respirar, trabajar y desempeñar tareas manuales. La ley tambien protege a estudiantes que han tenido un impedimento o condición física o mental substancial en el pasado, o que son considerados incapacitados aunque realmente no lo son. Estudiantes pueden ser considerados incapacitados bajo la Sección 504 y pueden recibir asistencia educativa bajo esa ley aunque no reciban educación especial. El propósito de este Aviso es de explicarle los derechos legales garantizados bajo la Sección 504 a estudiantes incapacitados y a sus padres. Los reglamentos federales que dan efecto a la Sección 504 (los cuales se encuentran en el Título 34, Parte 104 del Código Federal de Reglamentos, o CFR) otorgan a los padres de familia y a estudiantes incapacitados los siguientes derechos:
1. Usted tiene derecho a ser informado de sus derechos bajo la Sección 504. [34 CFR 104.32]. El distrito escolar debe darle información escrita sobre sus derechos (este Aviso precfsamente sirve para informarle de sus derechos). Si necesita que le expliquen o clarifiquen cualquier de los siguientes derechos, los dirigentes apropiados del distrito escolar le ayudardn a resolver sus preguntas.
2. Bajo la Sección 504, su hijo/a tiene derecho a una educación apropriada diseñada para satisfacer sus necesidades educativas individuales tan adecuddamente como las de estudiantes sin incapacidades. [34 CFR 104.33].
22

3. Su hijo/a tiene derecho a servicios educativos gratuitos, con la excepción de costos que normalmente se les cobran tambien a estudiantes sin incapacidades (o a sus padres). Compañías de seguros, y otras terceras personas similares, no son libres de sus obligaciones normales para proporcionar o pagar por servicios para un estudiante considerado incapacitado bajo la Sección 504. [34 CFR 104.33]. El recibir asistencia educativa bajo la Sección 504 no disminuye su derecho a recibir otra asistencia pública o privada de cualquier tipo.
4. Su hijo/a tiene derecho a ser colocado en el ambiente educativo que permita máximo contacto y relaciones con estudiantes sin incapacidades. [34 CFR 104.34]. A menos que sus necesidades educativas no puedan ser satisfechas ahí, su hijo/a será colocado en clases regulares.
5. Su hijo/a tiene derecho a equipo, clases, edificios, servicios y actividades comparables a las que son proporcionadas a estudiantes sin incapacidades. [34 CFR 104.34].
6. Su hijo/a tiene derecho a una evaluación antes de determinar una colocación educativa o programa de asistencia bajo la Sección 504, y tambien antes de cualquier cambio importante en colocación subsequente. [34 CFR 104.35].
7. Procedimientos utilizados para administrar pruebas y otras evaluaciones educativas deben cumplir con los requisitos de la Sección 504 en cuanto a la validez de las pruebas, su forina de administración, y las areas necesarias de evaluación. [34 CFR 104.35]. El distrito considerará información de diversas fuentes y orígenes, incluyendo, por ejemplo: pruebas de aptitudes y aprovecharmento, recomendaciones de maestros, reportes de condición física, antecedentes sociales y culturales, análysis de comportarniento adaptado, reportes médicos, calificaciones, reportes de progreso, observaciones de los padres, anécdotas de maestros, y calificaciones en los exámenes TAKS, entre otras. [34 CFR 104.35].
8. Las decisiones de colocación educativa deben realizarse por un grupo de personas (Ilamado el comité 504) que conocen la situación de su hijo/a, el significado de los resultados de las evaluaciónes, las opciones de colocación, y la obligación legal de asegurar el ambiente educativo que permita el máximo contacto con estudiantes no incapacitados. [34 CFR 104-35].
9. Si es considerado incapacitado bajo la Sección 504, su hijo/a tendrá derecho a que se le den nuevas pruebas y evaluaciones a ciertos tiempos, para determinar si sus necesidades educativas han cambiado. Generalmente evaluaciones educativas se pondrdn al corriente para cada niño incapacitado por lo menos cada tres años. [34 CFR 104.35].
10. Usted tiene derecho a que el distrito escolar le avise antes de tomar cualquier acción en relación a la identificación, evaluación o colocación educativa de su hijo/a. [34 CFR 104.36].
23

11. 11. Usted tiene derecho a examinar archivos y documentos relacionados a la educación de su hijo/a (normalmente archivos y documentos con relación a la identificación, evaluación o colocación educativa de su hijo/a). [34 CFR 104.36].
12. Usted tiene derecho a una audiencia imparcial si no esta de acuerdo con las acciones del distrito en relación a la identificación, evaluación, o colocación educativa de su hijo/a. Usted tiene la oportunidad de participar personalmente en tal audiencia y de ser representada por un abogado, si desea contratarlo. [34 CFR 104.36].
13. Si desea protestar o disputar las acciones del Comité 504 del distrito a traves de una audiencia imparcial, debe presentar un Aviso de Apelaclón escrito ante el Coordinador 504 del distrito, en la siguiente dirección:
Cassandra DarstDISD District Coordinator
501 East Collins, Decatur TX 76234 Se fijará una fecha para una audiencia ante un oficial imparcial, y serán notificados por escrito de la fecha, hora, y lugar de la audiencia.
14. Si usted está en desacuerdo con la decisión final del oficial imparcial de audiencia, tiene derecho a apelar esa decisión a una corte de jurisdicción adequada; normalmente, la corte federal local. [34 CFR 104.36].
15. En cuanto a otros aspectos de la Sección 504 que no tengan que ver con la identificación, evaluación y colocación educativa de su hijo/a, usted tiene el derecho a presentar una queja local ante el Coordinador 504 del distrito (o su representante), quien investigará la situación, teniendo en consideración la situación, en un esfuerzo de Ilegar a una resolución rápida y justa.
16. Usted también tiene el derecho a presentar una queja ante la Oficina de Derechos Civiles de el Departamento de Educación de los Estados Unidos. La dirección de la Oficina Regional a la cual pertenece Texas es:
Director, U.S. Department of Education Office for Civil Rights, Region VI 1999 Bryan Street, Suite 2600
Dallas, Texas 75201 Tel. (214) 880-2459
Mi firma debajo de indica he recibido esta nota y entiendo su contenido. La firma de Padre, de Padre Sustituto, del Guardián, o de Estudiante Adulto La fecha Firmó La firma de Intérprete, si usó La fecha Firmó
Permission to TestFor
Dyslexia Program
Date:
Dear ________________________
24

Your child, _________________________, is having difficulty in reading, writing, spelling, and/or language. In order to better diagnose his/her needs, it is necessary to collect and compile information such as test scores currently available, parent information, teacher information, and attendance records. It is likely that additional testing in the areas mentioned above will also be needed.
In order to collect this data and administer further testing, we need your signature below. You will be informed about testing results and program recommendations as soon as the information is compiled. Please sign, date, and return the form below as soon as possible.
Sincerely,
Dyslexia Teacher
___ I give permission for information to be collected from school records, teachers, and will complete the requested parent information form for my student____________________________.
___ I also give permission for additional testing to determine the appropriate instructional setting for my child.
___ I choose not to allow further information to be gathered at this time. I also deny any additional testing to determine the appropriate instructional setting for my child.
__________________________________ ____________________Parent/Guardian Signature Date
Permiso de examenpara el
Programa de Dislexia
Fecha:
Estimado ___________________________
Su hijo/hija __________________________ esta teniendo dificultades en lectura, escritura, ortografia, y/o lenguaje. Para major diagnosticar sus necesidades, es
25

necesario reunir información, tal como resultados de exámenes disponibles actualmente, información dado por padres y maestros, y el record de asistencia. Es probable que exámenes adicionales sean suministrados en las áreas antes mencionadas.
En orden de reunir la información y administrar los exámenes, necesitamos su firma. Usted será informado sobre los resultados de los exámenes y las recomendaciones del programa tan pronto que recibamos resultados pertinentes. Favor de firmar, escribir la fecha, y regresar la forma lo mas pronto possible.
Sinceramente,
La maestro de dyslexia
________________________________________________________________________
____ Yo doy permiso para que se reúna información de los expedients escolares, y d sus maestras, ye llenare la información disponible para mi hijo/hija __________________________.
____ También doy permiso para examinación adicional para determiner la instrucción apropiada para mi hijo/hija.
____ Yo no doy permiso para reunir información en este momento. También no doy permiso para examinación adicional para determiner instrucción apropiada para mi hijo/hija.
______________________________________ _____________________Firma del Padre Fecha
Teacher Information Form
Student ________________________ Teacher_______________ Date ________
Date of Birth _______________________________ Grade _______
26

Reason for Referral:
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Estimated Reading Level: ________ TPRI Reading Level __________
Star Test Level: ____________ ITBS/Achievement Reading Level: _____
Other: ___________
The Student: Yes Sometimes Never
Exhibits high cognitive ability level, especially verbally
____ _____ ____
Exhibits good reasoning ability ____ ____ ____
Exhibits strong listening comprehension ____ ____ ____
Exhibits strong reading comprehension ____ ____ ____
Attends class regularly ____ ____ ____
Maintains passing grades ____ ____ ____
Completes assignments in class ____ ____ ____
Is having difficulty, but keeps up with additional help
____ ____ ____
Hands in completed homework ____ ____ ____
Is able to follow directions: Verbal Written
________
________
________
Functions at high level of frustration ____ ____ ____
27

Has adequate attention span ____ ____ ____Yes Sometimes Never
Produces written work which reflects ability ____ ____ ____
Participates in tutorial program when needed ____ ____ ____
Has difficulty in: Reading—word recognition Reading comprehension Handwriting Written Expression Spelling Math
________________________
________________________
________________________
Please attach documentation to demonstrate educational need. Examples are copies of report card, progress reports, samples of student work, reading benchmark level, or etc.
HEALTH INFORMATION
28

School: _______________________________________ Date: _____________________________
Student Name: _________________________________ DOB: ____________________________
Student ID#: __________________________________ Grade: _____________________________
Vision: Date of Screening: ___________________________________________
Person Conducting Screening: _________________________________
Position: ___________________________________________________
Results: ____________________________________________________
YES NO
____ ____ Did the screening indicate a need for further assessment of adjustment?
If yes, explain: _________________________________________________________________________________________________________
____ ____ Has further treatment been recommended?If yes, explain: __________________________________________________________________________________________________________
Hearing: Date of Screening: ___________________________________________
Person Conducting Screening: _________________________________
Position: ___________________________________________________
Type of Screening: ___________________________________________
Results: ____________________________________________________
YES NO
____ ____ Did the screening indicate a need for further testing?If yes, explain: ____________________________________________________________________________________________________________
Health:YES NO
29

____ ____ Is there a health condition which adversely affects the student’s learning?
If yes, explain: ____________________________________________________________________________________________________________
____ ____ Is the student currently on medication?If yes, explain: ____________________________________________________________________________________________________________
3Parent Interview Form
Child’s Name: _________________________________ Parent’s Name: ___________________________
Completed by: ________________________________________ Date: ____________________________
1. Has your child ever had difficulty in school before?
2. Has your child ever repeated a grade in school? If so, when and where?
3. Has anything happened recently, which might be affecting his/her learning?
4. What strategies have previous teachers used that have worked?
30

5. Does your child have any health problems that might be affecting his/her progress?
6. Do you have any other suggestions for helping your child be successful?
7. Please list all schools previously attended:
31

Decatur Independent School DistrictParent Conference
IDENTIFYINGDate: ____/____/____
Student’s Name ___________________________________ Phone __________________________
Student’s Address: ____________________________________ City, Zip: ___________________
Sex: __________ Race: _________________________ Date of Birth: _______________________
FAMILY DATA:
Mother’s Name: __________________________________ Home Phone: ____________________
Mother’s Address: ________________________________ City, Zip: ________________________
Mother’s Occupation: _____________________________ Business Phone: ___________________
Mother’s Education (last grade completed): _____________________________________________
Father’s Name: _________________________________ Home Phone: ______________________
Father’s Address: ________________________________ City, Zip: ________________________
Father’s Education (last grade completed): _____________________________________________
Child lives with: ________________________________________________________________________________
32

Brothers Age
Sisters Age
Others Age
Length of residence in present home: _________________________ (months) (years)
Number of family members living in home: ______________________________________________
Any significant factors relating to child’s birth: ___________________________________________
________________________________________________________________________________
________________________________________________________________________________
DEVELOPMENTAL HISTORY:
Did you child exhibit any significant developmental delays in the following areas:
_______ Speech _______ Motor _______ Social ________ Physical
If YES, please describe: _____________________________________________________________________________________________________________________________________________________________________________________________________________________________
HEALTH HISTORY:
Please describe any significant health problems and/or medications which you feel are affecting your child’s educational development:
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
33

Please list any examinations (example: physical, visual, speech, hearing, neurological, educational) that your child has had in the past. Please list dates of such examinations, who examined the child, and addresses where copies of examination results may be obtained:
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
EDUCATIONAL HISTORY:
List names and dates of school districts your child as attended: ________________________________________________________________________________
________________________________________________________________________________
Has your child every attended private schools? _______________ If YES, list schools and date (s) of attendance: ________________________________________________________________________________________________________________________________________________________________
Did your child attend kindergarten? ___________________________________________________
Has your child ever been retained? _______________________If YES, list grade (s) ___________________________________________________________________________________________
Has your child ever been in special education? _____________ If YES, list dates, handicapping condition,and services provided: -______________________________________________________________
List the learning problems you feel your child has:_______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Please comment on any other significant factors relating to your child’s educational history:__________
________________________________________________________________________________
________________________________________________________________________________
34

________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
DISTRIOT ESCOLAR INDEPENDIENTE DECATUR INFORMACION DE LOS PADRES
DATOS DE IDENTIDAD FECHA: _____/_____/____
Nombre De Alumno: _______________________________________ Tel’Efono: ______________
Dirección:_______________________________________________________________________
Ciudad, Zona Postal: ___________________________________________________________________
Sexo: ________________ Raza: ________________________
Fecha De Nacimiento: __________________________________
FAMILIA:
Madre
Nombre:__________________________________________________________________________
35

Teléfono del domicilio: ________________________________
Dirección:_______________________________________________________________________
Ciudad, zona postal: ___________________________
Profesión:________________________________________________________________________
Teléfono del empleo: __________________________
Educación (último grado completado): __________________________
Padre
Nombre:_________________________________________________________________________
Teléfono del domicilio: ______________________________
Dirección:_______________________________________________________________________
Ciudad, zona postal: _______________________________
Profesión:________________________________________________________________________
Teléfone del empleo: _______________________________
Educación (último grado completado): ___________________________________________
El Alumno vive con: ________________________________________________________________
Hermanos Edad
Hermanas Edad
Otros Edad
36

Espacio de tiempo en el domicilio presente: ______________________ (meses, años).
Número de miembros de la familia que resident en el hogar:________________________________________________________________________________________________________________
CRECIMIENTO Y DESARROLLO:
Indique sis u higo/hija ha tenido algun retraso significante en el desarrollo de las siguientes areas:
__________Lenjuaje ___________ Motora ___________Social ________Salud
Si su respuesta es sí, por favor explique:
________________________________________________________________________________
________________________________________________________________________________
Salud:Describa caulquier problema con las salud de su hijo/hija, o con las medicinas que toma, que usted considere que afectan ele desarrollo educional de su hijo/hija
________________________________________________________________________________
________________________________________________________________________________
Haga una lista de cualquier examen (por ejempio, fisico, visual, de lenguaje, auditorio, neurológiico o académico) que su hijo/hija haya tendio en el pasado. Pong alas fechas de dihos examenes, quien los llevo a cabo, y las direcciones adonde se pueden pedir copias de dichos examenes:
________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
EDUCACION
Ponga los nombres y las fechas de los distritos escolares a que su hijo/hija ha asistido:
37

________________________________________________________________________________
________________________________________________________________________________
________________________________________________________________________________
¿Su hijo/hija ha asistido a escuelas privadea? ________________Si la respuesta es sí, ponga lost nombres de las escuelas y las fechas en que asistió:__________________________________________________________________________________________________________________________________________________________
¿Asistió su hijo/hija retendio alguna vez? _________________ Si la respuesta es sí, ponga el grado: ____
¿Ha recibiod su hijo/hija educación especial? __________ Si la respuesta es sí, pong las fechas,naturaleza del impedimento y los servicios proveídos:_____________________________________________________________________________________________________________________
Formulario de entrevista con el padre
Nombre del nino: ______________________________ Nombre del padr/madre: _______________
Completado por: _______________________________ Fecha: _____________________________
38

1. Ha tenido su nino dificultades en las escuela anteriormente?
2. Ha repetido su nino algun grado? Si es asi, cuando y donde fue?
3. Ha habido algun incidente recientemente que le peua haber afectado su habilidad para aprender?
4. Que estrategias han usado los maestros anteriormente que hayan dado Buenos rwesultados?
5. Tiene su nino algun problema de salud que le pueda estar afectando su progreso academico?
6. Tiene usted alguna sugerencia que now pueda servir de ayuda para que podamos ayudar a su hijo/hija a salir exitoso?
39

7. Por favor enumere todas las escuelas a las cuales su hijo/hija haya asistido anteriormente.
Decatur Independent School DistrictReceipt of 504 Rights
40

Name of Student: __________________________________________________________________
Date of Birth: _________________________________ School: ____________________________
This is verifying that I have received a copy of the “Notice of Parent and Student Rights under Section 504, The Rehabilitation Act of 1973,” which informs me of my rights.
____________________________________________ ________________________________Name Relationship
____________________________________________Date
I understand that my rights include the right to receive answers from campus personnel to additional questions I may have. Questions my also be addressed to the district:
Cassandra DarstDistrict 504 Coordinator
501 E. CollinsDecatur, TX 76234
(940) 393- 7160(940) 627-1088 fax
My signature below indicates that I received the handout and understand its content.
____________________________________________ ______________________________Signature of Parent, or Adult Student Date
(Please return to school personnel if you received this notice by mail.)
41

Distrito Escolar Independiente De Decatur ISDAcuso de recido de “Derechos de los Padres” de la Seccion 504
Nombre del estudiante: ___________________________________________________________
Fecha de nacimiento: _________________________________________ Escuela: ____________
Por este documento certifico haver recibido copia del aviso sobre los derechos de padres y Estudiantes, segun la Seccion 504, de la Ley de Rehabilitation de 1973, la cual me informa de mis derrechos. Estos derechos me los explico:
___________________________________________ ________________________________Nombre Posicion
Fecha _____________________________________
Entiendo que mis derechos incluyen el de recibir respuestas del personal escolar, a cualquier pregunta adicional que yo pudiera tener. Las preguntas tambien pueden dirigirse al distrito:
Cassandra DarstDistrict 504 Coordinator
501 E. CollinsDecatur, TX 76234
(940) 393-7160(940) 627-1088 fax
Mi firma a continuacion, indica que recibi el material y entiendo su contenido
__________________________________________ ________________________________Firma del padre/encargado, o de un estudiante Fechaadulto
(Si usted rebibio este aviso por correo, por favor regreselo a la escuela)
42

DECATUR INDEPENDENT SCHOOL DISTRICT
Identification for Dyslexia Program Placement
Student ____________________________________________________ Campus ______________
Teacher ____________________________________________________ Conference Date ______
_________________________________________________________ is educationally identified
with Dyslexia according to district and state guidelines. ________________________________________________________________________________
will be placed in a program that meets appropriate instructional components as described in the Dyslexia
Handbook: Procedures Concerning Dyslexia and Related Disorders (February, 2007), Chapter V.
AgreeDisagree
_____________________________________________________ ______ _______Parent/Guardian
_____________________________________________________ ______ _______Administrator
_____________________________________________________ _______ _______Classroom Teacher
_____________________________________________________ _______ _______Counselor
43

_____________________________________________________ _______ _______Dyslexia Therapist/Reading Specialist
Copy to:Parent Dyslexia Therapist/Reading SpecialistAdministrator Permanent FileClassroom Teacher Dyslexia FileCounselorParents,I have completed Dyslexia Testing on your child,
________________________________________________________________________________
If possible, I would like you to come by the school and review the test results.
I am available ________________________________________________________________.I just need to know when you are coming so I will be sure to be in my room at that time. If you are unable to attend in person, you may call the school, and we can have a phone conference.
Please fill out the bottom portion of this paper and return it to me.
Thanks,
________________________________________________________________________________
_____ I will come to school for a conference on _______________________ at _______________
________________________________________________________________________________Date Time
_____ I will call the school and have a phone conference.
44

_____ I will not be able to come to school or have a phone conference, please send the information home.
Child’s Name ______________________________________
Parent’s Name ____________________________________
________________ Date
Dear _____________________________,
Several weeks ago you gave us permission to administer additional tests and compile information concerning ______________________________ progress in reading, spelling, language and handwriting. After reviewing the tests results, we feel your child would benefit from specialized help in these areas.
Therefore, we would like your permission to place your child in the Dyslexia/Alternative Reading Program which will offer intense instruction in the areas of difficulty. The curriculum is based on phonics and the method of teaching is multisensory. Numerical or letter grades will not be given. I will send a progress report each 6 weeks, which will be in with your child’s regular report card.
Please sign and date the bottom of this letter and return it as soon as possible to your child’s teacher.
If you have any questions, please contact us.
Sincerely,
________________________________________________________________________________
45

I understand the findings of the testing on _____________________________________________ and the reason he/she has been recommended for the Dyslexia/Alternative Reading Program. I understand the curriculum and the methods used in this program.
_____ Yes, I want _______________________ to participate in the Dyslexia/Alternative Reading Program.
_____ No, I do not want _________________________ to participate in the Dyslexia/Alternative Reading Program.
_____________________________________________ __________________________Parent/Guardian Signature Date
Estimado_____________________________
Hace varios semanas usted nos dio permiso para administrar las pruebas adicionales y compiler informacion concerniendo _____________________________ progreso a leer, el deletreo, el idioma y la escritura. Despues que reviser los resultados de pruebas, nosotros nos sentimos que su nino(a) beneficiaria de a ayuda especializada en estas areas. Por lo tanto, nosotros apreciariamos que su permiso coloque su nino(a) en la Dislexia/el Programa de Leer de Alternativa que ofrecera la instruccion intense en las areas de dificultad. El curriculumis basado en un phonics y el metodo de ensenar es mutisensory. Numerico o los grados de carta no se daran. Mandare un porgreso el infome cada 6 smenans, que estaran en con su tarjeta regular del informe de nino. Por favor firme y fecha el fondo de esta carta y lo vuevle tan pronto como sea possible a su maestro del nino(a). Si usted tiene caluquiera pregrnta, por favor nos avisa.
Sinceramente,
__________________________________________________________________________________________
Entiendo los hallazgos del probar en __________________________ y la razon porque el/ella ha sido recomendada para el Programa de Leer de Alternativa de Dislexia. Entiendo el plan y los metodos usados en el programa este.
46

_____ Si, yo quiero que ____________________ tome parte en el Programa de Leer de Alternativa de Dislexia.
_____ No, yo no quiero que ___________________ tome parte en el Programa de Leer de Alternativa de Dislexia.
Firme _________________________________________________________________________
Fecha:_________________________________________________________________________
DECATUR INDEPENDENT SCHOOL DISTRICT
Dyslexia Exit FormElementary/Intermediate/Middle/High
____________________________________________________ is being exited from the Dyslexia program for the following reason(s):
____ On/above grade level on decoding and comprehension post-test
____ Successful completion of program
____ Passing TAKS Reading at _________ grade level
____ Performing on/above grade level
____ Parental request
____ Other: _______________________________________________________________
47

_____________________________________________________________________
_____________________________________________________________________
Dyslexia Team _________________ agrees _____________disagrees
____ Withdrawal from district: _______________________________________________
Exit Status:
Entry Date: ______________________ Exit Date: __________________________
Curriculum Summary: _________________________________________________
Signatures:
Parent: _____________________________________________ Date: ________
Administrator: _______________________________________Date: ________
Dyslexia Therapist: ___________________________________ Date: ________
EXIT COMPLETIONOF
DYSLEXIA PROGRAM
Date:
Dear Parent/Guardian:
48

Your student _____________________________________ has completed the Dyslexia Reading Program and will be exited from the daily instructional component. Hopefully your student will be able to transfer and apply the skills they have learned in the regular educational setting. Your student will continue to be monitored to ensure continued academic growth.
It has been a pleasure to serve your child, and we thank you for your support. If you have any questions or concerns, please contact the school.
Sincerely,
49