Embed Size (px)
Citation preview

(740) 356-7490www.somc.org/cancer/reports
SOMC Cancer Center1121 Kinneys Lane | Portsmouth, OH 45662
SOMC Cancer Services
Annual Report2015


www.somc.org/cancer/reports/ (740) 356-7490
Contents1
1
2
2
3
5
6
7
SOMC Cancer Services
Highlights & Happenings
A Message from Cancer Registry
Cancer Committee Members 2015
SOMC Case Accession Summary for Combined Calendar Years 2012, 2013, and 2014
SOMC Site Distribution Data Illustration for Diagnosis Years 2012, 2013, and 2014
Results that Demonstrate Quality Care
Lung Cancer Special Report
SOMC Cancer Center1121 Kinneys Lane
Portsmouth, OH 45662
the somc cancer services
2015 Annual Report

www.somc.org/cancer/reports/ (740) 356-7490
1
SOMC Cancer Services Southern Ohio Medical Center (SOMC) is committed to providing quality cancer care in our region. We honor our commitment by offering a state-of-the-art center; innovative cancer screenings and prevention strategies; experienced, credentialed staff, physicians, and providers; top-notch cancer-fighting technology and procedures, National Cancer Institute clinical trials, and dynamic patient-centered relationships.
The cancer program’s connection to SOMC enables the team with a full complement of support services including nutrition counseling, genetic counseling and testing, patient navigation, survivorship care planning, palliative and hospice care, social work, rehabilitation, complementary medicine, behavioral health, and inpatient care.
The excellent care provided is recognized through American College of Radiology (ACR) accreditation in radiation oncology, American College of Surgeons Commission on Cancer (ACoS) accreditation with commendations, SOMC’s Joint Commission accreditation, and participation in the National Community Oncology Research Program (NCORP) that provides patients access to National Cancer Institute clinical trials.
Over the years the SOMC Cancer program has grown and changed. In the fall of 2015, the team welcomed Elliot Navo, MD to Radiation Oncology. Dr. Navo received his medical degree at the State University of New York: Downstate Medical Center College of Medicine in Brooklyn, NY. He completed his residency in Radiation Oncology at SUNY Downstate Medical Center in Brooklyn, NY. Additionally, SOMC Cancer Services added a fourth provider to complement the team, John Harcha, PA-C. John received a bachelor of science from Shawnee State University and his Master of Science in Physician Assistant Studies at Marietta College in Marietta, Ohio. John will participate in the management of cancer patients and cancer care and will further develop the process through which patients receive chemotherapy education, immediate acute-care visits, and survivorship care. Lastly, our cancer program has expended much effort in the further development of lung care, adding a lung navigator, Jennifer Woodyard, RRT, CPFT and introducing a lung nodule clinic. The lung navigator has a role along continuum of lung care through:
+ Referring high-risk patients for early detection low-dose CT screening
+ Analyzing information and taking action to facilitate patient wellness and healing
+ Collaborating with the patient and the patient’s family to ensure they are receiving the best care possible
+ Coordinating patient care between specialties
+ Facilitating provider recommendations for patient care to ensure understanding and compliance
+ Helping patients with financial needs find resources for assistance
+ Providing educational and emotional support
Highlights & Happenings
Still, the SOMC cancer program is probably best known for extensive involvement in the region promoting cancer prevention strategies such as iDon’t.iWon’t, cancer screenings and education, and healthy lifestyle education and programming. The SOMC Compassion Fund is extended to patients undergoing active cancer care. The SOMC Compassion Fund is widely supported by the region and every year access to assistance for the cancer patient population in our community grows.
Elliot Navo, MD
John Harcha, PA-C
Jennifer Woodyard, RRT, CPFT

www.somc.org/cancer/reports/ (740) 356-7490
2
The SOMC Cancer Registry Department supports all cancer activities within SOMC. The registrar oversees collection, quality assurance, lifetime follow-up, and analysis of data from patients diagnosed with cancer who receive all or part of their care at SOMC and those deemed reportable. Local, state and national cancer agencies use registry data in defined areas to make important health decisions that maximize the effectiveness of limited public health funds, such as the placement of screening programs. This contribution of information advances cancer knowledge and ultimately impacts cancer patient care.
The primary responsibility of the cancer registrar is to ensure that timely, accurate, and complete data is incorporated and maintained on all types of cancer diagnosed and/or treated within SOMC. The ultimate goal is to learn from the data and reduce cancer death and illness nationwide. Collection and reporting of the data is of utmost importance. Registry data also serves as an ongoing resource to the cancer committee in determining the most effective allocation of resources, in determining community education and outreach initiatives, and monitoring program quality.
The realm of a cancer registrar is ever changing, and seems to be changing even faster with the advancement of computers and the ability to capture data and report the data similarly for comparisons. In an effort to ensure SOMC’s data is comparable to those collected at other programs around the country, the registrar adheres to established data rules. Keeping up with these changes is challenging, but the SOMC Cancer Registry department understands the significance of this work and is committed to continuously raising the bar.
Thomas Summers, DO, FACOIMedical Oncology/HematologyCancer Committee ChairQuality Improvement Coordinator
Ben Gill, MBAAdministration
Vincent Scarpinato, MD, FACS, MBAGeneral Surgeon/Breast Cancer SurgeonCancer Liaison Physician Scott Logan, MDDiagnostic Radiology Janan Alkilidar, MDDiagnostic Radiology
Bambi Overacre, RT(R)(MR)(CT)Medical Imaging
Donna Corcoran, RT(R)(CT)(M)Breast Imaging
Stephanie Hale, BSN, RN, CN-BNBreast Navigation
Melissa Hutchens, BS, RT (R), RDMSMedical Imaging Christopher Shiepis, DOUrology
Meghan SextonAmerican Cancer Society
Rachelle Collins, RN, BSN, OCNOutpatient OncologyCommunity Outreach Coordinator
Brooke CoriellOutpatient Rehabilitation
Valerie DeCamp, RN, BSN, MHA, NE-BCInpatient Nursing
Ann Fankell, LSW, MSW, NADIIICancer Center Social WorkPsychosocial Services Coordinator
Kristi Coleman, BS, CTRCancer Registrar
Linda Horner, RN, BSN, OCN, PCCNInpatient Oncology Nursing
Jamie Arnett, RN, OCNClinical Research Representative
Aubrey RoyCommunity Relations
Debbie DanielsPhysician Liaison
Wendi Waugh, R.T. (R)(T) CMD, CTR, BSAdministrator Cancer ServicesCancer Registry Quality Control Chair
Vincent Randaisi, DO, FACPPathology
Jill Preston, RN, MSNCommunity Health & Wellness
Kimberlee Richendollar, RN, BSN, OCNNurse Navigation
Jennifer Woodyard, RRT, CPFTLung Navigation
Chad Lore, MS, NP-CHospice and Palliative Care
Jenny Smathers, RN, BSN, CHPNPalliative Care
Elie Saab, MDPulmonology
Yinong Liu, MD, PhDMedical Oncology/HematologyCancer Conference Chair
Elliot Navo, MD Radiation Oncology
Jessica Suber, MDPlastic Surgery
George Shahade, DOENT, Otolaryngology
Andrea BargerPulmonology Office
A Message from Cancer Registry
2015 SOMC Cancer Committee Members

www.somc.org/cancer/reports/ (740) 356-7490
3
SOMC Case Accession Summary for Combined Calendar Years 2012, 2013, & 2014
Total % Male % Female %
Oral Cavity & Pharynx 26 2.2 18 3.4 8 1.2
Tongue 7 0.6 4 0.8 3 0.4
Salivary Glands 1 0.1 0 0 1 0.2
Gum & Other Mouth 3 0.3 2 0.4 1 0.2
Nasopharynx 2 0.2 2 0.4 0 0
Tonsil 9 0.8 6 1.2 3 0.4
Oropharynx 2 0.2 2 0.4 0 0
Other Oral Cavity & Pharynx 2 0.2 2 0.4 0 0
Digestive System 192 16.5 111 22.3 81 12.1
Esophagus 16 1.4 14 2.8 2 0.3
Stomach 11 0.9 8 1.6 3 0.4
Small Intestine 3 0.3 2 0.4 2 0.3
Colon Excluding Rectum 96 8.2 49 9.8 47 7.0
Cecum 9 4 5
Ascending Colon 3 2 1
Hepatic Flexure
Appendix 5 2 3
Splenic Flexure 1 0 1
Descending Colon
Sigmoid Colon 11 4 7
Large Intestine, NOS 65 36 28
Rectum & Rectosigmoid 33 2.8 22 4.4 11 1.6
Rectosigmoid Junction 7 4 3
Rectum 26 18 8 1
Anus, Anal Canal & Anorectum 1 0.1 0 0 1 0.1
Liver & Intrahepatic Bile Duct 7 0.6 4 0.8 3 0.4
Gallbladder 2 0.2 0 0 2 0.3
Peritoneum, Omentum, Mesentery 2 0.2 0 0 2 0.3
Pancreas 18 1.5 11 2.2 7 1.0
Respiratory System 282 24.2 152 30.5 130 19.5
Larynx 8 0.7 4 0.8 4 0.6
Lung & Bronchus 273 23.4 148 29.7 125 18.7
Trachea, Mediastinum & Other Respiratory Organs

www.somc.org/cancer/reports/ (740) 356-7490
4
Soft Tissue 2 0.2 2 0.4 0 0.0
Skin Excluding Basal & Squamous 53 4.5 28 5.6 25 3.7
Melanoma -- Skin 48 4.1 24 4.8 24 3.6
Other Non-Epithelial Skin 5 0.4 4 0.8 1 0.1
Breast 272 23.3 1 0.2 271 40.6
Female Genital System 49 4.2 0 0 49 7.3
Cervix Uteri 9 0.8 0 0 9 1.3
Corpus & Uterus, NOS 31 2.7 0 0 31 4.6
Ovary 6 0.5 0 0 6 0.9
Vagina 1 0.1 0 0 1 0.1
Vulva 2 0.2 0 0 2 0.3
Male Genital System 68 5.8 68 13.7 0 0
Prostate 60 5.1 60 12.0 0 0
Testis 7 0.6 7 1.4 0 0
Penis and Other 1 0.1 1 0.2 0 0
Urinary System 43 3.7 35 7.0 8 1.2
Urinary Bladder 34 2.9 29 5.8 5 0.7
Kidney, Renal Pelvis & Ureter 86 0.7 5 1.0 3 0.4
Brain & Other Nervous System 5 0.4 4 0.8 1 0.1
Endocrine System 33 2.8 11 2.2 22 3.3
Thyroid 31 2.7 9 1.8 22 3.3
Other Endocrine including Thymus 2 0.2 2 0.4 0 0
LYMPHOMA 51 4.4 22 4.4 29 4.3
Hodgkin Lymphoma 3 0.3 2 0.4 1 0.2
Non-Hodgkin Lymphoma 48 4.1 20 4.0 28 4.2
Myeloma 11 0.9 6 1.2 5 0.7
Leukemia 26 2.2 14 2.8 12 1.8
Lymphocytic Leukemia 6 0.5 4 0.8 2 0.3
Myeloid &Monocytic Leukemia 9 0.8 3 0.6 6 0.9
Other Leukemia 11 0.9 7 1.4 4 0.6
Mesothelioma 3 0.3 2 0.4 1 0.1
Kaposi Sarcoma 1 0.1 1 0.2 0 0
Miscellaneous 49 4.2 23 4.6 26 3.9
Total 1,166 498 668
SOMC Case Accession Summary for Combined Calendar Years 2012, 2013, & 2014

www.somc.org/cancer/reports/ (740) 356-7490
5
SOMC Site Distribution Data Illustration for Diagnosis Years 2012, 2013, & 2014
Thyroid - 22 (3%)
Lung & Bronchus - 125 (19%)Breast - 271(41%)
Kidney & Renal Pelvis - 3 (<1%)
Ovary - 6 (<1%)Uterine Corpus – 31 (5%)Colon & Rectum - 58 (9%)
Non-Hodgkin Lymphoma - 28 (4%)Melanoma of the Skin - 24 (4%)Leukemia - 12 (2%)
All Other Sites - 88 (13%)
Oral Cavity & Pharynx – 18 (4%)
Lung & Bronchus - 148 (30%)
Pancreas - 11 (2%)Kidney & Renal Pelvis - 5 (<1%)
Urinary Bladder - 29(6%)
Prostate - 60 (12%)Colon & Rectum - 69 (14%)
Non-Hodgkin Lymphoma - 20 (4%)Melanoma of the Skin - 24 (5%)
Leukemia - 14 (3%)
All Other Sites - 98 (20%)
*** The number next to the site represents the number of cases diagnosed at SOMC diagnosis years 2012, 2013 and 2014 combined and the number in parenthesis represents
the percentage this cancer site represents at SOMC for those same diagnosis years.

www.somc.org/cancer/reports/ (740) 356-7490
6
Results that Demonstrate Quality of CareOur accreditation by the American College of Surgeons Commission on Cancer allows the center to compare treatment standards and quality of care. The Commission on Cancer partners with the National Quality Forum (NQF), the American Society for Clinical Oncology (ASCO), and the National Comprehensive Cancer Network (NCCN). These organizations have identified quality cancer measures. The following graphs demonstrate the results of SOMC Cancer Care team compared to all approved East Central ACS, all approved programs with a similar type of accreditation as we hold-Community Hospital Cancer Program-(CHCP), and all Commission on Cancer (CoC) approved programs for the CoC Accountability measures. We are very proud of our results. These results represent the latest published data, calendar year 2013.
Radiation Therapy is Considered or Administered following Mastectomy for Women with ≥4 + Nodes | 2013 Performance
Radiation is Administered within 1 Year of Diagnosis for Women Receiving Breast Conserving Surgery | 2013 Performance
80
84
88
92
96
100
All Approved CoC Programs
CoC Community Cancer Centers
East Central ACS
SOMC80
84
88
92
96
100
All Approved CoC Programs
CoC Community Cancer Centers
East Central ACS
SOMC
Combination Chemotherapy is Considered or Administered within 4 months for AJCC T1cNO, or Stage IB-III Hormone Receptor Positive Breast Cancer | 2013 Performance
Aromatase Inhibitor is Considered or Administered within 1 year of Diagnosis for AJCC T1c or IB-III Hormone Receptor + Breast Cancer| 2013 Performance
80
84
88
92
96
100
All Approved CoC Programs
CoC Community Cancer Centers
East Central ACS
SOMC80
84
88
92
96
100
All Approved CoC Programs
CoC Community Cancer Centers
East Central ACS
SOMC
Adjuvant Chemotherapy is Considered or Administered within 4 months for AJCC III Colon Cancer | 2013 Performance
80
84
88
92
96
100
All Approved CoC Programs
CoC Community Cancer Centers
East Central ACS
SOMC
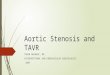
Cancer is the second leading cause of death in Ohio and in the United States. In 2015, 65,010 persons in Ohio are expected to be diagnosed with cancer of which about 10,000 cases will be lung cancer (fig 1).
Number of New Invasive Cancer Cases for the Leading Cancers in Ohio, 2012
Cancer is the second most common cause of death in Ohio and the United States, accounting for nearly one of every four deaths. Cancer claimed the lives of more than 25,000 Ohioans in 2012, at a rate (182.0 per 100,000) 9 percent higher than the U.S. rate (166.5 per 100,000).
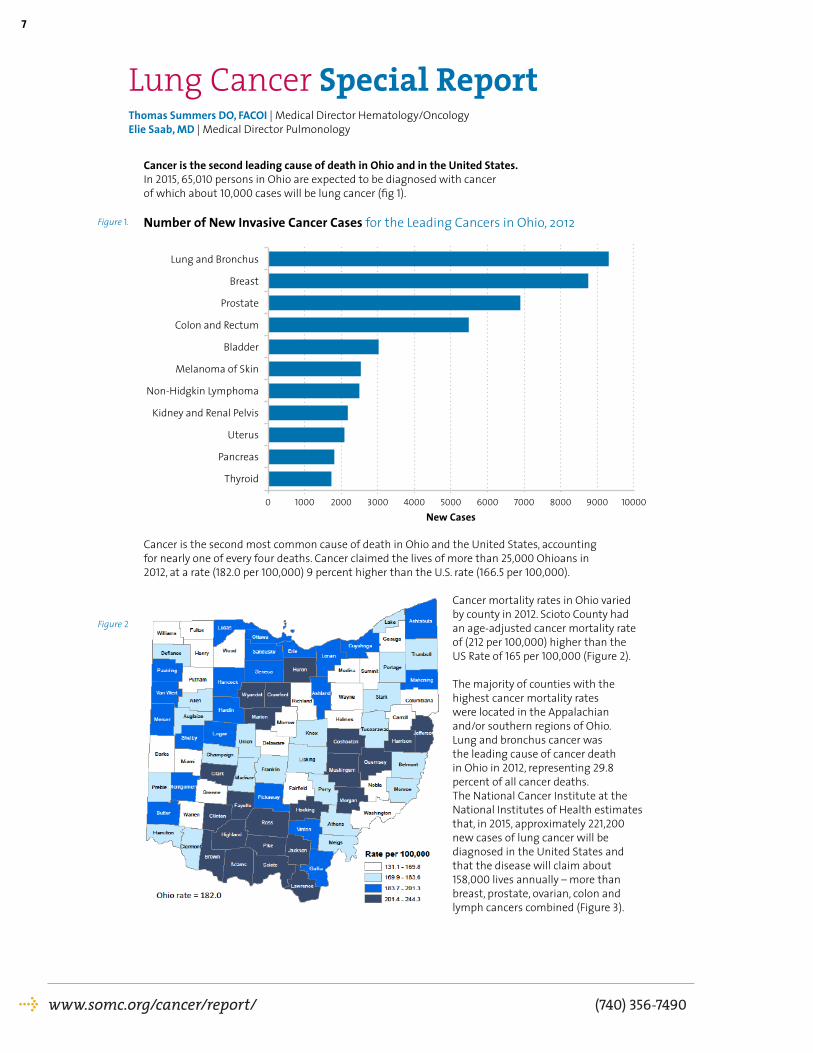
Cancer mortality rates in Ohio varied by county in 2012. Scioto County had an age-adjusted cancer mortality rate of (212 per 100,000) higher than the US Rate of 165 per 100,000 (Figure 2). The majority of counties with the highest cancer mortality rates were located in the Appalachian and/or southern regions of Ohio. Lung and bronchus cancer was the leading cause of cancer death in Ohio in 2012, representing 29.8 percent of all cancer deaths. The National Cancer Institute at the National Institutes of Health estimates that, in 2015, approximately 221,200 new cases of lung cancer will be diagnosed in the United States and that the disease will claim about 158,000 lives annually – more than breast, prostate, ovarian, colon and lymph cancers combined (Figure 3).
www.somc.org/cancer/report/ (740) 356-7490
7
Lung Cancer Special ReportThomas Summers DO, FACOI | Medical Director Hematology/OncologyElie Saab, MD | Medical Director Pulmonology
Figure 2
Lung and Bronchus
Breast
Prostate
Colon and Rectum
Bladder
Melanoma of Skin
Non-Hidgkin Lymphoma
Kidney and Renal Pelvis
Uterus
Pancreas
Thyroid
0 1000 2000 3000 4000 5000
New Cases6000 7000 8000 9000 10000
Figure 1.

www.somc.org/cancer/reports/ (740) 356-7490
8
1992
80
60
40
20
01995 2000
year
New Cases
Deaths
num
ber
per
100,
000
pers
ons
2005 2012
Estimated New Cases in 2015 221,200
% of All New Cancer Cases 13.3%
Estimated Deaths in 2015 158,040
% of All Cancer Deaths 26.8
Percent Surviving 5 Years
17.4%2005-2011
Lung cancer is more common in men than women, particularly African American men. The number of new cases of lung and bronchus cancer was 58.7 per 100,000 men and women per year based on 2008-2012 cases (Figure 4). The median age at diagnosis is 70 (Figure 5).
70.1 All Races 50.2
70.3 White 52.7
90.9 Black 50.8
49.0 Asian | Pacific Islander 28.5
47.6 American Indian | Alaska Native 34.5
37.9 Hispanic 25.1
74.2 Non-Hispanic 53.5
male female
Number of New Cases per 100,000 Persons by Race/Ethnicity & Sex: Lung and Bronchus Cancer
<20
40
35
30
25
20
15
10
5
00%
20-34 35-44 45-44age
Perc
ent o
f New
Cas
es
55-64 65-74 75-84 >84
9.1%
27.6%31.9%
21.4%
8.4%
1.2%0.3%
Lung and bronchus cancer is most frequently diagnosed among people
aged 65-74.
Median Age At Diagnosis
70
Percent of New Cases by Age Group:Lung and Bronchus Cancer
Lung cancer is the leading cause of cancer deaths in both men and women. This should not be the case, as lung cancer is also one of the most preventable cancers.
It is generally accepted that more than 60% of all cancers are related to personal lifestyle or environmental factors, such as smoking and diet, and are therefore preventable. According to the 2014 Surgeon General’s Report, 87% of lung cancer deaths are preventable. Other factors such as age, gender and family history of cancer are also associated with the development of cancer and aid in the identification of people at high risk. Early detection is stressed, but for some cancers, prevention is much more beneficial. Lung cancer is a disease that takes many years to develop and often spreads
Figure 3
Figure 4
Figure 5

www.somc.org/cancer/reports/ (740) 356-7490
9
to other parts of the body before it is detected. Early detection options have been limited and routine radiographic screening for specific patients may be helpful. In response to this, the National Institute of Health conducted the National Lung Cancer Screening Trial (NSLT). The trial included 50,000 patients and demonstrated a reduction of all-cause of mortality by 6.7% and lung cancer relative death risk rate reduction of 20% (NEJM). The United States Preventative Task Force [USPSTF) subsequently recommended the use of low-dose CT scans for screening for patients with high-risk criteria:
+ 55 to 77 years of age
+ Tobacco smoking history of at least 30-pack-years
+ Either a current smoker or one who has quit smoking within the last 15 years
+ No diagnostic CT of chest in the past 18 months
+ No prior history of lung cancer
+ No active signs or symptoms
In November of 2014 the Centers for Medicare and Medicaid released a coverage decision providing payment under the Accountable Care Act. This coverage will extend to an estimated 4 million people, many of whom are at greatest risk for the disease. Scans would cost recipients nothing; the coverage would apply to beneficiaries that meet the established criteria. Under the Affordable Care Act, private insurers must also cover such screenings.
SOMC responded to the coverage decision and is leading the way in our community with the development of a robust lung cancer screening program coupled with smoking cessation teaching and intervention strategies. A task force comprised of radiology, pulmonology, surgery, oncology nursing, and respiratory therapy disciplines has built upon our “Lungs for Life“ program. Under this program, patients with high-risk criteria were enrolled and received CT scan provided by SOMC, Radiologists, and the Scioto Foundation. Additions to the program in 2015 include the introduction of a dedicated pulmonary nodule clinic, shared decision-making provider visits, and lung navigation. SOMC also recently purchased a software program to maintain data and report results to the ACR registry. The screening program is certified by the ACR (American College of Radiology) as an accredited center for lung cancer screening. Much like the breast cancer registry the lung registry data will be entered and referred to the ACR by CMS. It is our desire to meet the need of patients in a timely fashion while maintaining a high standard of detection and management according to the latest evidence-based guidelines. It is important to highlight that smoking cessation is an integral part of this program. Nearly 50% of the scans will have an abnormality, 96% of which will be false positive meaning that patients most likely will be observed with serial CT scans.
Patients should talk with their healthcare providers about the benefits, limitations and potential harm of lung cancer screening. Screening should only be done at facilities like SOMC through which ACR accreditation has been achieved and the center has met all the criteria to perform the screening exams.
Smoking is the leading cause of preventable death in the United States and is by far the leading risk factor for developing lung cancer.
It is estimated 80% of lung cancers and 30% of other types of cancer result from smoking. Smokers exposed to radon and asbestos are at even higher risk. Cigar and pipe smoking are almost as likely to cause lung cancer as cigarette smoking. Nonsmokers who breathe in second-hand smoke are also at a 20% increased risk. Air pollution and increased age are factors, and women who smoke seem at greater risk for developing cancer than men who smoke. Stopping smoking at any age lowers the subsequent risk of developing lung cancer.
Smoking kills more people than alcohol, AIDS, automobile accidents, illegal drugs, murders and suicides combined.
Figure 6 graphically shows 70% of the lung cancer patients diagnosed at SOMC resided in Scioto County. Surrounding Ohio counties and neighboring counties in Kentucky represent

www.somc.org/cancer/reports/ (740) 356-7490
10
the other 30% of the diagnoses. Last year, SOMC diagnosed 52 female and 45 male patients. The majority of female patients were diagnosed within the age group of 50-59 while the male patient majority was diagnosed in the 60-69 age group. The average age at diagnosis nationally for both genders is the 60-69 age group (Figure 7).
Depending on how cells appear when examined
under a microscope, lung cancer is divided into two main categories: small cell/neuroendocrine/carcinoid (nationally 20% of the diagnoses) or non-small cell (NSCLC) (80%). The treatment courses are very different based on the histology. Small cell occurs almost exclusively in smokers and non-small cell encompasses several similar sub-types: adenocarcinoma, squamous cell carcinoma and large cell carcinoma. Figure 8 shows the national distribution compared to the 2014 SOMC distribution.
All NSCLC specimens are processed for
molecular testing. Identifying targeted therapies and applying them when appropriate is proving beneficial. Patients are also enrolled in clinical trials when appropriate. The interventional bronchoscopy lab is equipped with the latest tools available for less invasive techniques. The staff is skilled in computerized navigational bronchoscopy, peripheral bronchoscopy and central airway bronchoscopy. Central airway bronchoscopy is mainly used to obtain specimens from lymph nodes surrounding the tracheobronchial tree and is an essential tool for staging. Patients with lymph node involvement around the trachea should undergo a nonsurgical therapeutic approach. The interventional radiology staff complements the team obtaining percutaneous aspirates when required. Rapid on-site (ROSE) cytology specimens are analyzed real-time to help guide sampling. The cytopathologist assists in the bronchoscopy suite to provide feedback to the sampling bronchoscopist. SOMC encourages a multidisciplinary approach to the diagnoses of lung cancer and the following therapeutic interventions. The yield of the SOMC bronchoscopy lab specimens is higher than the national average. In fact, with our approach SOMC diagnoses more patients in earlier stage than nationwide in both NSCLC and small cell lung cancers (Figure 9 & Figure 10).
Kentucky
Highland
Brown
Adams
Pike
Scioto
2014 County Distribution of Lung Cancer Accessioned by SOMC
Figure 6
Figure 7SOMC 2014 Lung Cancer Cases Age at Diagnosis
0
5
10
15
20
25
30
35 Women Men
90+80-8970-7960-6950-5940-49
National Lung Cancer Histology SOMC 2014 Histology
Other
Non-small cell-not specified
Adenocarcinoma
Squamous
Small Cell
All Other
Acinar
Carcinoid
Adenocarcinoma
Squamous
Small Cell
Figure 8

www.somc.org/cancer/reports/ (740) 356-7490
11
Based on type and stage of cancer, treatments include surgery, radiation therapy, chemotherapy and targeted therapies. Early stage cancer may be treated only with surgery, and later stage cancer usually is treated with several modalities. The SOMC first course of treatment combinations are pictured below (Figure 11).
The national one-year relative survival for all lung cancers combined increased from 34 percent in 1975-77 to approximately 51 percent in 2003-08, largely due to improvements in surgical techniques and combined therapies. Figure 12 reflects the one-year survival (all stages combined) for analytic cases diagnosed at SOMC compared to NCDB.
The national five-year survival rate is 54% for cases detected when the disease is still localized, 26% for patients with regional disease and 4% for patients with distant-stage disease. SEER data shows reflecting the national five-year survival rates. The graph below compares SOMC (solid line) to NCDB (dashed line) five-year survival by Stage using AJCC Staging Manual 6th Edition for Analytic NSCLC patients (Figure 13).
SOMC Compared to NCDB NSCLC Stage at Diagnosis2012-2013 Data
SOMC Compared to NCDB Small Cell Lung Cancer Stage at Diagnosis2012-2013 Data
Figure 9 Figure 10
01020304050607080 NCDB SOMC
Stage IVStage IIIStage IIStage I
NCDB SOMC
05
1015
2025303540
Stage IVStage IIIStage IIStage I
2014 SOMC Lung Cancer First Course of Treatment
05 10 15 20 25Other
S, CR
D, S, R, CD, SD, R
SD, PD, C
D, R, CD
D=Diagnostic BiopsyR=RadiationC=ChemotherapyP=PalliativeS=Surgery
Figure 11
Figure 12All Stages One-Year Observed Survival Analysis Cases of NSCLC Comparing SOMC to NCDB
Observed 5-Year Survival for SOMC Analytical NSCLC 2003-2008 Compared to NCDB
Figure 13
SOMC - 46.4
NDCB - 50.7
001 22 43 64 86 0
20
40
60
80
100
Number of Months
Perc
enta
ge S
urvi
ving
Stage IV NDCB
Stage III NDCB
Stage II NDCB
Stage I NDCB
Stage IV
Stage III
Stage II
Stage I

www.somc.org/cancer/report/ (740) 356-7490
12
As displayed there are some differences in survival especially in the early stages. Several factors may explain the differences and several strategies have been implemented to lessen the gap such as ebus, navigational bronchoscopy, better staging techniques, better targeted treatment techniques and lastly management of the entry points into the comprehensive lung navigation program.
As illustrated in Figure 14 below, pulmonary nodules identified through screening or diagnostic CTs lead to expected next steps and a diagnosis of lung cancer if applicable. Upon diagnosis, the tumor board committee meets again to discuss options and therapeutic recommendations. These discussions are documented and the recommendation can be found in the patient’s medical record. Consideration of the functional capacity, physiological determinants, radiographic analysis, and clinical stage drive the patient’s treatment recommendations. The final AJCC stage, pathology, and molecular characteristics are important in determining what therapeutic modalities are recommended. Stage I and stage II lung cancers are evaluated for lung resection or stereotactic ablative radiation therapy. The SOMC Cancer Committee has adopted NCCN guidelines as guiding principles in both management and recommendations for all stages of lung cancer diagnosed in the institution.
The Cancer Committee also monitors detection to diagnosis, diagnosis to treatment, and other indicators of surgical resection specimen adequacy as required by the national guidelines.
2013 SOMC Performance Data
Indicator PerformanceAverage detection to diagnosis elapsed 29 days
Average report to biopsy 27 days
Average pathology turnaround 2 days
Average diagnosis to treatment 45 days
At least 10 regional lymph odes are removed for resected AJCC IA to IIB NSCLC 11%
Systemic chemotherapy is administered within 4 months pre-op or 6 months post-op when appropriate 100%
Screening CT Diagnostic CT
LR4 or Higher
tumorboard
pulmonaryvisit
diagnostic surgical
procedure or pet
LR3 Pulmonary Visit for FUP Discussion
LR1 /LR2 Return Subsequent
Year for Repeat Screen
PulmonaryNodule
Figure 14

www.somc.org/cancer/report/ (740) 356-7490
13
The SOMC Cancer Committee is focused on decreasing detection to diagnosis and detection to treatment elapsed days. In addition SOMC Cancer Committee has issued a Standard of Care for both Lung Surgery and Lung Screening. These Standards of Care are aimed to educate and hold staff increasingly accountable for these important standards (Figure 15 and Figure 16).
There is an abundant need for further work in the field of lung cancer. Our team is dedicated and proud of the accomplishments and even more excited about the work underway.
Figure 15 Figure 16




SOMC Cancer Center1121 Kinneys Lane | Portsmouth, OH 45662(740) 356-7490
www.somc.org/cancer/reports/