Embed Size (px)
Citation preview
Somatoform and
Dissociative DisordersDr.Saman Anwar Faraj
psychiatristM.B.Ch.B, F.I.B.M.S (psych)
I. Somatoform Disorders
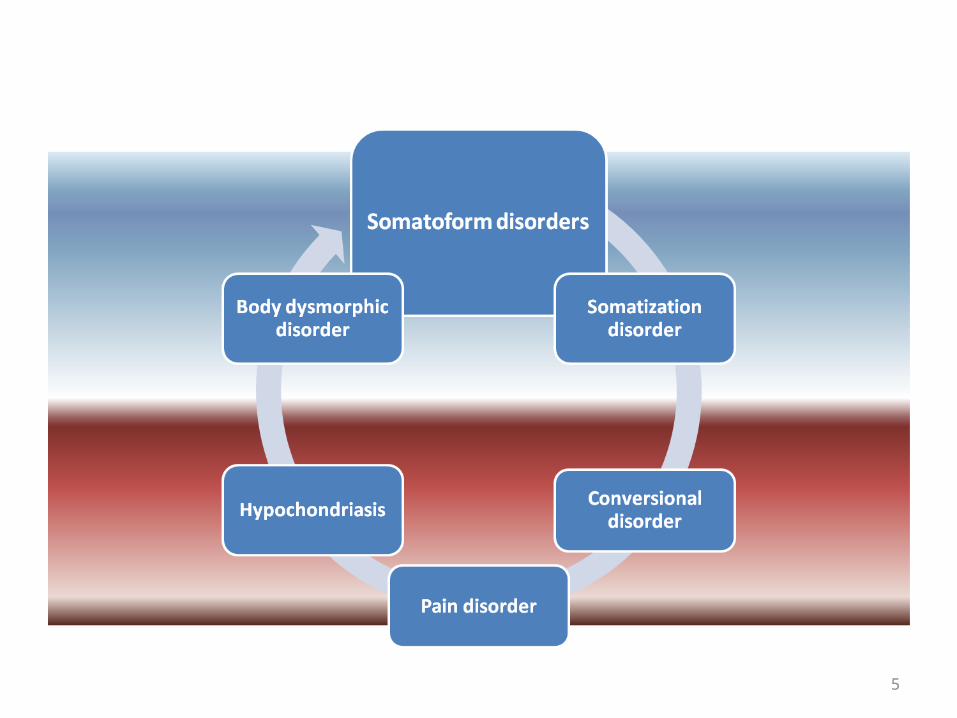
• Somatoform disorders describe a group of disorders that share in common the presence of physical symptoms that suggest a general medical condition but are not fully explained by a general medical condition or the effects of a substance or another mental disorder. Some somatoform disorders are better understood than others, although most have not received the research attention that other Axis I disorders (e.g., depression) have received. Thus, these are among the most poorly understood of the mental disorders.
4
Soma = BodyForm = LikeSomatoform = Body likeAre group of Mental disorders characterized by
physical symptoms that are not explained by organic factors.
Somatoform disorders are differentiated from malingering and factitious disorder because symptoms in somatoform disorders are not seen as intentional, voluntary, and consciously produced. However, elaboration of symptoms in patients with somatoform disorders may sometimes have a component of volition.
Somatoform disorders
5
Sick Role
• Have you ever “played sick” in order to get out of something? How did that work out (did you get what you wanted)?
• Sick attention (friends, family, medical) = secondary gains
• Likely link between secondary gains and somatoform disorders
• Some medical condition may actually exist
• People who are sick get lots of attention from medical personnel, families, friends, etc. and this attention can be very psychologically rewarding. Although somatoform disorders are more complex than simply an elaborate scheme to achieve secondary gains from the sick role, there is likely a link between these gains (which are reinforcing) and the continuation of the presentation of the disorder. It is also important to note that the person suffering from a somatoform disorder may in fact have a medical condition of some sort, but that medical condition does not account for the entirety of the physical symptom complaints put forth by the patient.
Somatization Disorder
1. Historical perspective• In the medical/clinical nomenclature since the
mid-1600’s • Known as “Hysteria,” “hypochondriasis,” and
“melancholia” until 1800’s when mental disorders were differentiated
• Briquet’s syndrome, named for the French physician who initially defined it in 1859
• Term “somatization disorder” was first used in DSM-III (1980)
Somatization (cont.)
DSM-IV criteriaA. History of many physical complaints beginning before age 30 occurring over several years resulting in treatment being sought or significant impairment in functioning
DSM-IV criteria (cont.)
B. Each of the following met at some point during disorder:
1) 4 pain symptoms2) 2 gastrointestinal symptoms3) 1 sexual symptom4) 1 pseudoneurological symptom
DSM-IV criteria (cont.)
C. Either:1) symptoms in Criterion B cannot be
fully explained by a known GMC or 2) when a GMC does exist, the
symptoms in Criterion B are in excess of what would be expected based on medical factsD. Symptoms not intentionally feigned or produced
Somatization (cont.)
***Additional descriptive information• Report of symptoms usually colorful or
exaggerated; factual info usually lacking• Lab findings do not support somatic complaints• Treatment sought from several doctors at once
hazardous mix of treatments• Other disorders, such as anxiety disorders, mood
disorders, and personality disorders, often co-exist
Additional info (cont.)
• Primary relationships are with doctors; personal relationships usually have problems
• Often seem indifferent about what symptoms represent– Concerned with individual symptoms, not what symptoms
might indicate in terms of a disease
• Physical symptoms become part of their identity (ego syntonic)

Somatization (cont.)
4. Statistics and course– Lifetime prevalence:
• 0.2 – 2% in women• less than 0.2% in men• Rates affected by rater, method of assessment, and
demographic variables:– Non-physicians diagnose it less frequently– In primary medical care settings, rate is 4.4 – 20%– Typical demographic is lower SES unmarried woman
Somatization (cont.)
5. Causesa) familial/genetic
• Genetic influence (30-50%) on somatization symptoms
b) Social learning• Parents may reinforce somatic complaints in children gain
attention (sick role)• Research shows somatization features and help seeking for
illness in parents of somatizing children
Causes (cont.)
c) Cultural– Cultural differences in type of symptoms– Different rates across cultures– Possible differences in the use of somatic
references in communication (not a disorder, just differences in communication?)
d) Societal– More acceptance of medical vs. psychological
problems
Somatization (cont.)
6. Treatment– No treatment shown to be effective– Behavioral approach limit doctor visits
• Use a gatekeeper physician
– Train patient to relate to others without using physical complaints
18
Hysteria=(Hystero) (Uterus-Greek)Conversion=a process where by psychological distress was converted
into physical symptoms.
• Descriptions of conversion disorders appeared as far back as 1900 BC when multiple symptoms were attributed by Egyptian physicians to a wandering of the uterus within the body.
• The term conversion was first used by Sigmund Freud and his associate Josef Breuer.
Conversional disorder
19
Sudden onset, sudden termination, sudden reappearanceMostly women; men in combatOften misdiagnosed: Overpathologized
• Conversion disorder is an illness of symptoms or deficits that affect voluntary motor or sensory functions, which suggest another medical condition, but that is judged to be caused by psychological factors because the illness is preceded by conflicts or other stressors.
• The symptoms or deficits of conversion disorder are not intentionally produced, are not caused by substance use, are not limited to pain or sexual symptoms, and the gain is primarily psychological and not social, monetary, or legal.

20
A. The patient complain of symptoms or deficits.
Motor symptoms (weakness, difficulty in swallowing, aphonia, impaired coordination)
Sensory symptoms (blindness, deafness, loss of touch or pain sensation).
Seizure or convulsions
Mixed presentation (more than one symptoms)
Clinical features
21
B. The temporal relation of symptoms to a stressful event suggest association of psychological factors.
C. Symptoms are not explained by an organic etiology or another mental illness.
D. Symptoms result in significant functional impairment.
22
• The onset of conversion disorder is generally from late childhood to early adulthood and is rare before 10 years of age or after 35 years of age, but onset as late as the ninth decade of life has been reported.
• When symptoms suggest a conversion disorder onset in middle or old age, the probability of an occult neurological or other medical condition is high.

23
Management:
Medical and psychiatric hx. From patient and relatives. Full examination and investigation to exclude physical causes. Sympathetic but positive reassurance that the patient is suffering
from an acute temporary condition and doesn't have disabling medical disorder.
Discussion of the expected rapid recovery. Avoidance of reinforcement of disability or symptoms. Offering continuing assessment and treatment of related psychiatric
or social problems.
24
• Resolution of the conversion disorder symptom is usually spontaneous, although it is probably facilitated by insight-oriented supportive or behavior therapy. The most important feature of the therapy is a relationship with a caring and confident therapist. With patients who are resistant to the idea of psychotherapy, physicians can suggest that the psychotherapy will focus on issues of stress
and coping. • Telling such patients that their symptoms are imaginary often
makes them worse.• Hypnosis, Anxiolytic, and behavioral relaxation exercises are
effective in some cases.• Parenteral amobarbital or lorazepam may be helpful in obtaining
additional historic information, especially when a patient has recently experienced a traumatic event.
• The longer the duration of these patients' sick role and the more they have regressed, the more difficult the treatment.
25
Course and Prognosis• The onset of conversion disorder is usually acute. Symptoms or
deficits are usually of short duration, and approximately 95 percent of acute cases remit spontaneously, usually within 2 weeks in hospitalized patients.
• Recurrence occurs in one fifth to one fourth of people within 1 year of the first episode. Thus, one episode is a predictor for future episodes.
• A good prognosis is heralded by acute onset, presence of clearly identifiable stressors at the time of onset, a short interval between onset and the institution of treatment, and above average intelligence.
• Paralysis, aphonia, and blindness are associated with a good prognosis, whereas tremor and seizures are poor prognostic factors.
Pain Disorder
• Main symptom is pain• May be exacerbated by psychosocial factors• May be maintained by gain: Eugene
– Primary gain– Secondary gain
Hypochondriasis
• No physical symptoms are necessary• Preoccupied with the possibility that normal
sensations are symptoms of serious disease• Frequent visits to physicians• Persists despite medical reassurance• Over-report bodily sensationsPrevalence is 6-15% in general medical clinic.Men and women equally affected.
28
A. Preoccupation with fear of having a serious disease, based on misinterpretation of symptoms.
B. The patient is not assured by a negative medical evaluation.
C. The disorder result in significant functional impairment.
D. Duration is greater than 6 months.
F. Symptoms are not accounted for by another mental disorder
Clinical features
29
• Measures to control investigation, correct misattributions.
• Cognitive behavioral treatment.
• Medication (fluoxetin) may beneficial.
Treatment
Body Dysmorphic Disorder
• Excessive concern with real or imagined defects in appearance, especially facial marks or features.
• Frequent visits to plastic surgeons• Culturally-influenced, but not culture-bound• May be a symptom of more pervasive
disorders: Obsessive-compulsive or delusional disorder, for example.
Do advertisements affect BDD?
“Your nose is central to the way you feel about your appearance and the way other people first perceive you.“If you are in the slightest way unhappy about it, and feel it detracts from your looks, you will probably always be unhappy about it.”
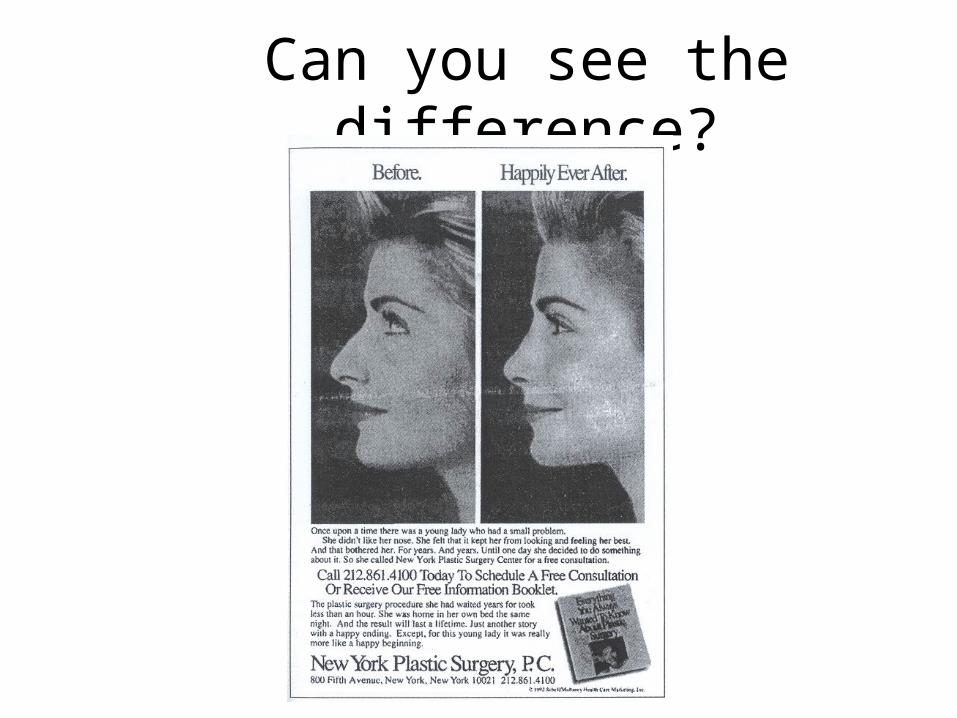
Can you see the difference?
33
• Surgical, dermatological, medical treatment are unsuccessful.
• Psychotherapy
• Medication( SSRI, Clomipramine)
Treatment
More somatoform-like disorders
• Malingering• Factitious disorder
– Personal: Symptoms only when observed– By proxy (NOS)
• Undifferentiated Somatoform Disorder• Somatoform Disorder NOS
– Pseudocyesis (no everted umbilicus)– Hypochondriacal symptoms < 6 months
Somatoform and Dissociative Disorders
II. Dissociative Disorders
Overview
• Disorders are marked by disruption in the usually integrated functions of consciousness, memory, identity, or perception of the environment
• What are some “normal” dissociative experiences that people have sometimes?
• arriving home but not remembering the drive; intending to go to your friend’s house but end up heading to work/school out of habit; calling a friend and being surprised when your mom answers because you misdialed
Some General Considerations
• The four diagnoses are hierarchical and only one can be used at any given time– Dissociative Identity Disorder– Dissociative Fugue– Dissociative Amnesia– Depersonalization Disorder
A. Common Features of Dissociative Disorders
1. Depersonalization = distortion in perception such that a sense of reality is lost
2. Derealization = losing a sense of the external world
• e.g., things change size or shape
B. Dissociative Identity Disorder (DID)
• Formerly known as multiple personality disorder
1. DSM-IV criteriaA. presence of 2 or more distinct identities or personality statesB. At least 2 identities/personalities recurrently take control of the person’s behavior
1. DSM-IV criteria (cont.)
C. Inability to recall important personal information (goes beyond ordinary forgetfulness)D. Not due to effects of a substance or GMC; in children, symptoms not attributable to imaginary playmates or fantasy play
Dissociative Fugue• The predominant disturbance is sudden, unexpected travel
away from home or once customary place of work, with inability to recall one's past.
• Confusion about personal identity or assumption of a new identity.
• The disturbance does not occur exclusively during the course of Dissociative Identity Disorder and is not due to direct physiologic effects of a substance or a general medical condition.
• The symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning
Depersonalization Disorder• Persistent or recurrent experiences of feeling detached
from, and as if one is an outside observer of, one's mental processes or body (e.g., feeling like one is in a dream).
• During the depersonalization experience, reality testing remains intact.
• The depersonalization causes clinically significant distress or impairment in social, occupational, or other important areas of functioning.
• The depersonalization experience does not occur exclusively during the course of another mental disorder, such as Schizophrenia, Panic Disorder, Acute Stress Disorder, or other Dissociative Disorder, and is not due to the direct physiologic effects of a substance or a general medical condition.
Summary
• Somatoform disorders involve a focus on physical symptoms that are either not real or are exaggerated
• Dissociative disorders involve a disturbance in normally integrated functions (memory, identity, etc.)
• Course is usually chronic• Causes for most are unknown
Thank you