Embed Size (px)
Citation preview

Somatization and its Discontents: Rates, Predictors and Correlates of Somatic Symptoms in Rheumatic Disease Patients
Robert S. Katz1, Frederick Wolfe2. 1Rush University Med Center, Chicago, IL; 2National Data Bank for Rheumatic Diseases, Wichita, KS
ABSTRACT
PURPOSE: Patients with many somatic symptoms are problems for clinicians, presenting with a multitude of complaints, usually thought to be more than can be explained by medical illness. Such patients may be characterized as “somatizers,” but it is not clear that there is a cutoff point where non-medical factors predominate In addition, the predictors or correlates of somatic symptom expression have not been fully explored in rheumatic diseases. We address these issues in this study.
METHODS: 21,845 persons (RA 76.9% , OA 18.5% , fibromyalgia 4.6%) participating in long-term rheumatic disease outcome study completed a check-list of 36 symptoms. A symptom count score (SYMP) that ranged from 0 to 36 was computed. High levels of symptoms were operationally defined as scores ≥ the 75th percentile (SYMP75) and extreme levels (SYMP90) occurred at ≥ 90th percentile: values of 13 and 17, respectively.
RESULTS: The mean (median, IQR) symptoms count was 8.1 (7, 3-12) for the study sample, and was 13.7 (13, 9-18) for patients with fibromyalgia). SYMP75 was more common in women, odds ratio (OR) 2.1 (95% C.I.: 1.9 to 2.3). We constructed a multivariable model to predict SYMP75. Using a logistic regression containing HAQ, pain, fatigue, patient global, regional pain scale (RPS), lifetime comorbidity index, age and sex, the receiver operating curve AUC was 0.90, and the model correctly predicted 87.0% of cases. A simpler model using only fatigue and RPS (a count of painful non-articular regions) resulted in a ROC value of 0.86 and a correct classification of 84.6%. Fatigue and RPS were significantly better predictors than all other variables. Predicting SYM90 with the complex model yielded an AUC ROC of 0.91 and a correct classification of 92.8%, while the simpler 2-variable model had an AUC ROC of 0.88 and a correct classification of 91.8. 47.6% of fibromyalgia patients had SYMP75 and 27.2% had SYMP90. For persons without fibromyalgia, SYMP75 was 15.6% and SYMP90 was 6.8%. We constructed a composite variable for SYMP75 predictors using the 2-variable model and principal component analysis, and examined graphically the results of regressing SYMP75 on the composite variable using fractional polynomial regression. Analyses showed the relationship to be linear without evidence of a cut-off. Nor did cluster or factor analysis provide such evidence of a discrete somatising group. Person with SYMP75 had higher total semiannual medical costs (US$ 5,287 vs. 3,702) and lower quality of life (mapped EQ5D 0.38 vs. 0.64).
CONCLUSIONS: High levels of somatic symptoms are part of a triad that includes fatigue and widespread pain (RPS). At high levels of these variables this cluster is often recognized as fibromyalgia in some patients. Somatic symptoms have no simple cutoff, and the relation between variables is well-described by linear models. The concept of a single point for “somatization” does not fit the continuum of somatic symptoms identified in this study.
Men and women have different levels of symptom count. EXPECTED SCORE: MEAN (":" INDICATES HALF-SCORE POINT) (BY OBSERVED CATEGORY)-5 -4 -3 -2 -1 0 1 2 3 4 5|-----+-----+-----+-----+-----+-----+-----+-----+-----+-----| ITEM00 00 : 01 01 Vomiting00 00 : 01 01 Hives00 00 : 01 01 Fever00 00 : 01 01 Loss, change in taste00 00 : 01 01 Chest pain00 00 : 01 01 Raynaud's00 00 : 01 01 Wheezing00 00 : 01 01 Rash00 00 : 01 01 Sun sensitivity00 00 : 01 01 Mouth ulcers00 00 : 01 01 Loss of appetite00 00 : 01 01 Pain/cramps in lower abd00 00 : 01 01 Nausea00 00 : 01 01 Diarrhea00 00 : 01 01 Loss of hair00 00 : 01 01 Pain in upper abdomen00 00 : 01 01 Dizziness00 00 : 01 01 Constipation00 00 : 01 01 Nervousness00 00 : 01 01 Hearing difficulties00 00 : 01 01 Depression00 00 : 01 01 Shortness of breath00 00 : 01 01 Insomnia00 00 : 01 01 Blurred vision00 00 : 01 01 Ringing in the ears00 00 : 01 01 Itching00 00 : 01 01 Heartburn00 00 : 01 01 Dry eyes00 00 : 01 01 Headache00 00 : 01 01 Dry mouth00 00 : 01 01 Trouble thinking/remembering00 00 : 01 01 Muscle weakness00 00 : 01 01 Numbness/tingling in hands/feet00 00 : 01 01 Muscle pain00 00 : 01 01 Easy bruising00 00 : 01 01 Fatigue|-----+-----+-----+-----+-----+-----+-----+-----+-----+-----| ITEM-5 -4 -3 -2 -1 0 1 2 3 4 51 1 1 1 1 1 1111116 3 13 7 517 5542008779443421117 1 65 3 572 67218174185354253076422 1 13 0 14 81738 42827519291458806221433 722 9 26 1 1 PERSONS T S M S T
0.0
00
.25
0.5
00
.75
1.0
0S
ens
itivi
ty
0.00 0.25 0.50 0.75 1.001 - Specificity
Area under ROC curve = 0.8817
Models of somatization: variables, ROC AUC and % correct
ROC curve for full model (roc=0.86
Symptom scale fulfills Rasch Model Differential Item function
List of items in symptom scale. Item bias for sex exists when item score difference is greater than 0.50. Positive scores (+) indicate items that are more “difficult” for women. Negative (-) scores indicate items that are “easier” for women. Degree of item bias indicates that that analyses cannot be combined on the basis of a simple score.
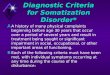
A composite variable made from the major predictor of the regression model (Regional pain scale, fatigue and comorbidity) demonstrates a linear relationship between the somatising scale (symptom count) and the predictor variables. This shows that there is no cut-off for somatization.
In the clinic, a somatising patient is one who has many more symptoms than he or she should have, given the patient’s clinical status. Clinicians easily recognize such patients. However, such a definition falls short of the Disease and Statistical Manual (DSM-IV) definition of a somatization disorder. It also runs up against several other problems. The more severe a patient’s illness is the more somatic symptoms he will have, leading to the problem that somatization and illness severity are confounded. Somatization is also confounded by the differences between the sexes. Women report more somatic symptoms than men, and they also have higher scores for pain, fatigue and functional disability. The result of the issues is that are few studies about somatization in rheumatic disease. One may know what it is, but be unable to define it. We explore “somatization using a symptom count cut-off at the 75th percentile for men and women, separately.
Somatising is present in 67% of persons satisfying survey fibromyalgia criteria and 18% of those not satisfying the criteria
There is no clear cut-off for somatization.
Somatising characteristics are predicted by the Regional Pain Scale and fatigue.
Men and women see the importance of somatic symptoms differently.
If one cut-off for somatization is chosen then women will be seen to be somatising more frequently than men.
There is no simple answer to the problem of identifying somatization.
The data presented here are an exploration, but not a satisfactory explanation
01
02
03
0S
ymp
tom
co
unt
-2 0 2 4 6Composite variable: Regional pain scale, fatigue scale and comorbidity
Relation between somatization predictors and symptom count