-
Somatic TP53 Mutations in the Era of GenomeSequencing
Pierre Hainaut1 and Gerd P. Pfeifer2
1University Grenoble Alpes, Institut Albert Bonniot, Institut
National de la Santé et de la RechercheMédicale (INSERM), 823
Grenoble, France
2Center for Epigenetics, Van Andel Research Institute, Grand
Rapids, Michigan 49503
Correspondence: [email protected]
Amid the complexity of genetic alterations in human cancer, TP53
mutation appears as analmost invariant component, representing by
far the most frequent genetic alteration overall.Compared with
previous targeted sequencing studies, recent integrated genomics
studiesoffer a less biased view of TP53 mutation patterns,
revealing that .20% of mutations occuroutside the DNA-binding
domain. Among the 12 mutations representing each at least 1% ofall
mutations, five occur at residues directly involved in specific DNA
binding, four affect thetertiary fold of the DNA-binding domain,
and three are nonsense mutations, two of them inthe carboxyl
terminus. Significant mutations also occur in introns, affecting
alternative splic-ing events or generating rearrangements (e.g., in
intron 1 in sporadic osteosarcoma). Inaggressive cancers, mutation
is so common that it may not have prognostic value (all
thesecancers have impaired p53 function caused by mutation or by
other mechanisms). In severalother cancers, however, mutation makes
a clear difference for prognostication, as, forexample, in
HER2-enriched breast cancers and in lung adenocarcinoma with EGFR
muta-tions. Thus, the clinical significance of TP53 mutation is
dependent on tumor subtype andcontext. Understanding the clinical
impact of mutation will require integrating mutation-specific
information (type, frequency, and predicted impact) with data on
haplotypes and onloss of heterozygosity.
In 1989, 10 years after the discovery of the p53protein, studies
by Baker et al. (1989), Nigroet al. (1989), and Takahashi et al.
(1989) re-vealed that the TP53 gene was frequently mu-tated in many
forms of human cancer. Morethan 25 years later, in the era of
genome-widesequencing of cancer DNA, TP53 is confirmedas the most
frequently mutated gene associatedwith cancer in general. This
finding is one ofthe most surprising lessons from cancer ge-
nome sequencing. There is no a priori reasonwhy candidate
gene-centered sequencing ap-proaches would have correctly
identified oneunique gene among 20,000 genes as the mostfrequently
mutated one. Indeed, a comparisonof significantly mutated genes
(SMGs) detectedby whole-exome analysis in 15 types of solidtumors
shows that TP53 is the most fre-quently mutated gene in 11 of them
(gliobla-stoma, clear cell renal cell carcinoma, head and
Editors: Guillermina Lozano and Arnold J. Levine
Additional Perspectives on The p53 Protein available at
www.perspectivesinmedicine.org
Copyright # 2016 Cold Spring Harbor Laboratory Press; all rights
reservedAdvanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
mailto:[email protected]:[email protected]:[email protected]://www.perspectivesinmedicine.orghttp://www.perspectivesinmedicine.orghttp://www.perspectivesinmedicine.orghttp://perspectivesinmedicine.cshlp.org/
-
neck squamous cell cancer, serous ovarian car-cinoma,
non-small-cell lung cancer, small-celllung cancer, gastric cancer,
hepatocellular carci-noma [HCC], cholangiocarcinoma, breast can-cer
[BC], prostate cancer) (average: 25%–60%),whereas it ranks second
to KRAS in pancreaticand colorectal cancer, and third to BRAF
andNRAF in melanoma (Watson et al. 2013). Inhematopoietic
malignancies, TP53 mutationsare less frequent (10%–15%) but are
amongthe 10 most frequent SMGs in five of six docu-mented
malignancies (the exception is pediatricacute lymphoblastic
leukemia [Zhang et al.2012]).
The first studies on TP53 mutations focusedon tumors with
allelic deletions at the TP53locus (17p13.1) and showed that
mutations re-sulting in single amino acid substitutions
werefrequent on the allele that was retained. Thisobservation was
consistent with the theoreticalhallmarkof a tumor-suppressor gene
and Knud-sen’s two-hit hypothesis. Soon, however, it wasnoted that
tumors that retained both parentalalleles also frequently carried
point mutationson one allele, suggesting a form of dominanteffect
of the mutation. Indeed, independentof the allelic context, nuclear
accumulation ofmutant p53 protein was detected in a widespectrum of
primary and metastatic lesions,suggesting a selective retention of
mutant p53during tumor development and dissemination(Bartek et al.
1990). In 1991, distinct patternsof somatic TP53 mutations were
revealed, re-spectively, in UV-induced nonmelanoma skincancers
(Brash et al. 1991) and in aflatoxin-re-lated HCC (Bressac et al.
1991). These mutationpatterns were consistent with the ones
inducedby these mutagens in experimental assays, con-firming the
idea that “carcinogens [can] leavefingerprints” in TP53 sequence as
evidence oftheir etiological role in carcinogenesis (Vogel-stein
and Kinzler 1992).
In subsequent years, the results literallysparked an industry of
sequencing TP53 exonsusing the Sanger technique of
chain-terminat-ing inhibitors in cancer tissues. From a few
hun-dred at the turn of the 1990s, the number ofsomatic TP53
mutations identified in cancergrew steadily to more than 10,000 by
the end
of the millennium (Hainaut and Hollstein2000). Soon,
computational resources were de-veloped to compile, retrieve, and
compare thealready identified somatic mutations. In 1994,two
databases collecting and annotating muta-tions detected by
sequencing and published inthe peer-reviewed literature were
established,and they have been since maintained continu-ously: the
TP53 database at the InternationalAgency for Research on Cancer
(IARC), initiat-ed by Monica Hollstein and Curtis Harris
(p53.iarc.fr) (Olivier et al. 2002), and the UMD-p53database,
initiated by Thierry Soussi (p53.fr/index.html) (Beroud and Soussi
1998). Thesedatabases currently contain more than 30,000annotated
mutations and provide a numberof flexible tools to analyze the
distribution ofmutations across cancers. They have been thebasis of
several comprehensive reviews discuss-ing the variability and
heterogeneity of TP53mutation patterns with respect to
mutagenicprocesses, cancer etiology, or potential impactson cancer
biology (Greenblatt et al. 1994; Hai-naut and Hollstein 2000;
Petitjean et al. 2007;Soussi 2014).
In recent years, the development of second-generation sequencing
technologies (also callednext-generation sequencing [NGS]) has
en-abled the systematic analysis of cancer exomesand genomes,
expanding our understanding ofmutation patterns far beyond the
knowledgederived from single genes such as TP53. How-ever, despite
numerous studies reporting anassociation between somatic TP53
mutationsand poor prognosis and unfavorable treatmentoutcomes
(Olivier et al. 2010; Robles and Har-ris 2010), the only accepted
recommendationfor clinical testing to date is for chronic
lympho-cytic leukemia (CLL), in which somatic TP53mutation is
predictive of poor response to con-ventional therapies
(Stilgenbauer et al. 2014).Thus, the clinical significance of
somatic TP53mutations remains elusive in most forms ofcancer. In
this review, we revisit our under-standing of TP53 mutation
patterns in the lightof recent data generated by next-generation
se-quencing, and we discuss how somatic TP53mutation testing may
contribute to inform clin-ical practice.
P. Hainaut and G.P. Pfeifer
2 Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://p53.iarc.frhttp://p53.iarc.frhttp://p53.iarc.frhttp://p53.fr/index.htmlhttp://p53.fr/index.htmlhttp://p53.fr/index.htmlhttp://p53.fr/index.htmlhttp://perspectivesinmedicine.cshlp.org/
-
TOWARD AN UNBIASED SOMATIC TP53MUTATION SPECTRUM
TP53 occupies �19.14 kb of genomic DNA onchromosome 17p13.1 and
is oriented on theminus strand, antisense to other genes in
theneighborhood. It comprises 14 exons, including10 exons
constituting the coding sequence of thecanonical, full-length p53
protein of 393 aminoacids, one noncoding exon 1, and three
alterna-tive exons, exon 2/3, exon 9b, and exon 9g (exon9a being
the regularly spliced form of exon 9)involved in the synthesis of
alternatively splicedtranscripts encoding p53 protein isoforms
(Fig.1A). The noncoding exon 1 is separated from therest of the
coding sequence by a highly conservedintron that covers more than
half of the gene(10,738 bp). Another gene, WRAP53, is
locatedupstream of the TP53 coding sequence on theopposite (plus)
strand. It overlaps with exon 1and the proximal part of intron 1
and encodesantisense transcripts that are complementary toexon 1
transcripts (Mahmoudi et al. 2009). Twomain promoter domains, P1
and P2, have beenidentified. P1 is the main promoter and is
locat-ed upstream of exon 1. P2 is located within in-tron 1 at
about 1000 bp of the 30 end of exon 1and regulates the expression
of an intronic poly-adenylated transcript of 1125 b,
Hp53int1(D17S2179E, GenBank: U58658.1) (Reismanet al. 1996). The
p53 gene has a complex expres-sion pattern with a single major
transcript (en-coding the full-length p53 protein) and morethan 12
documented transcripts of variableabundance generated by
alternative splicingand/or internal promoter usage (a weak
pro-moter has been identified in a region encom-passing exons 2–4
[Marcel et al. 2010]). Thesetranscripts encode protein isoforms
that differfrom canonical p53 by the lack of amino-termi-nal
domains (D40p53, lacking residues 1–39;D133p53, lacking residues
1–132) or by alter-native carboxyl-terminal domains (p53b andp53g)
(Courtois et al. 2004; Khoury and Bour-don 2010; Marcel et al.
2011). Although the pre-cise functions of these isoforms is still
poorlyunderstood, there is strong experimental evi-dence that
amino-terminally truncated p53 var-iants may counteract the
suppressor functions
of full-length p53 protein (reviewed in Marcelet al. 2011; see
also Joruiz and Bourdon 2016).
After initial studies reported that somaticmutations were
clustered over �1200 bases inconserved regions of exons 5–8, most
studieshave sequenced only these regions. Convention-al sequencing
methods are optimized for thedetection of small sequence
alterations (sin-gle-base mutations, short indels). Larger indelsor
rearrangements are not readily scored bythese techniques. These
biases have caused anunderrepresentation of somatic mutations
oc-curring outside exons 5–8, many of which areindels. Whole-genome
sequencing (WGS) andwhole-exome sequencing (WES) mutation
datagenerated by NGS may be, in principle, less bi-ased toward an a
priori selection of “hotspot”mutation areas. The COSMIC database
main-tained at the Sanger Institute (Hinxton, UnitedKingdom) is the
largest public database de-signed to store and display somatic
mutationinformation relating to cancer. The Whole Ge-nomes Resource
(v73) of this database (cancer.sanger.ac.uk/wgs) compiles a total
of �5000TP53 mutations detected in WGS/WES proj-ects, corresponding
to 1206 different mutationevents (as of May 1, 2015). Of those,
only 12mutations are highly recurrent, representingeach at least 1%
of the entire mutation dataset (Table 1). These mutations represent
muta-tional DNA “hotspots.” Of note, 11 of thesehotspots occur at
CpG sites and constitute amolecular signature of the random
deamina-tion of unstable 5-methylcytosine. Altogether,the 12 DNA
hotspots represent �25%–30% ofthe total number of mutations. In
contrast, 773mutations are rare events, each occurring onlyonce or
twice in the data set, representing alto-gether �20% of the total
number of mutations.Because several DNA hotspot mutations
fallwithin the same codons (e.g., 245, 248, or273), only six “major
hotspot” codons compriseeach at least 2% of all mutations (175,
213, 245,248, 273, and 282). Another 13 codons repre-sent “mini
hotspots,” comprising each between1% and 2% of all mutations (158,
176, 179, 193,195, 196, 220, 249, 266, 278, 306, 337, and
342).Figure 1B shows the distribution of WGS/WESmutations along the
p53 coding sequence and
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/wgshttp://perspectivesinmedicine.cshlp.org/
-
5
4
3
2
1
0
1
2
3
4
5
6
COSMIC WholeGenomes data set
B
WRAP53
Hp53int1
TP53
a2/3 a9βa9γ
(10 kb)1 2 3 4 5 6 7
19.136 kb
133
ATG
1 40BR
A
8 9 10 11
175
248
273
MissenseNonsenseIndels
Missense andnonsensemutations
176
158
193195196
220
249266 278
306 342
337
CTDODJDDBDPRRTAD2TAD1
213
245 282
179
7
6
7
IARC TP53 database
% o
f all
mut
atio
ns
Figure 1. TP53 mutation spectrum in human cancer. (A) TP53 locus
on chromosome 17p13.1, showing mainintron/exon structure (coding
exons, red; noncoding exon 1 and 30 UTR in exon 11, gray) and
alternative exons2/3, 9a, and 9b (orange). The position of Hp53int1
in intron 1 is shown, as well as the region of exon1/intron
1overlapping with alternative exons 1 of WRAP53. All introns and
exons are represented to scale, except intron1. Blue bar, location
of rearrangement breakpoints in osteosarcoma. Red arrows, position
of the main (þ1) andalternative (þ40, þ133) protein initiation
sites. Green arrowheads, orientation of the coding sequences
(TP53is located on the minus strand of DNA, WRAP53 on the plus
strand). (Legend continues on following page.)
P. Hainaut and G.P. Pfeifer
4 Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
compares it with the distribution compiledfrom the IARC mutation
data set in 2010, beforethe systematic usage of NGS (of note, the
latestrelease of the IARC database [p53.iarc.fr] hasincluded 866
mutations identified by WGS/WES [3% of the data set]). Although
these dis-tributions look very similar, the WGS/WESpattern shows
that mutations outside exons5–8 represent 22.5% of the total,
almost doublethat estimated by Sanger sequencing (10%–15%). The
higher number of silent mutationsdetected by NGS explains only 1.5%
of this dif-ference. Within the DNA-binding domain ofthe p53
protein, NGS data show that mutationsat codon 213 (80% nonsense,
p.R213�) and co-don 220 (90% missense, p.Y220C) are hotspotsalmost
as high as the well-defined hotspot co-dons 245 and 282. NGS data
also show a fre-quently mutated area in the oligomerizationdomain
(residues 326–355, 5% of all muta-
tions). Within this domain, codon 342 (91%nonsense, p.R342�)
constitutes a minor hotspotcodon. Thus, the Sanger data set appears
to bebiased toward underrepresentation of muta-tions outside exons
5–8 and overrepresentationof the mutations known as major
hotspots(codons 175, 245, 248, 273, and 282), perhapsbecause of a
tendency of investigators to notfully analyze exon 6 (which is
GC-rich andhard to sequence) and to preferentially reportmutations
detected at codons in exons 5, 7, and8. Interestingly, the newly
scored hotspot co-dons 213 and 342 contain CpG
dinucleotidesequences, as do the standard hotspot codons175, 245,
248, 273, and 282.
About 2% of all mutations occur at intron/exon boundaries and
affect splicing donor oracceptor sites. Genome-wide splicing
mutationanalysis has identified TP53 as the gene mostcommonly
affected by splicing mutation in BC
Table 1. TP53 mutation “hotspots”: 12 mutations representing
each of at least 1% of all mutations in the COSMICWhole Genome
Dataset (cancer.sanger.ac.uk/wgs)
Position
(codon)
cDNA/base
change
Protein/amino
acid change Type of mutation %
CpG
site Mutation effect
175 c.524G.A p.R175H Substitution/missense 4.0 Yes Structural196
c.586C.T p.R196� Substitution/nonsense 1.4 Yes Structural213
c.637C.T p.R213� Substitution/nonsense 2.1 Yes Null220 c.659A.G
p.Y220C Substitution/missense 1.5 No Structural245 c.733G.A p.G245S
Substitution/missense 1.3 Yes Structural248 c.742C.T p.R248W
Substitution/missense 2.1 Yes DNA-binding248 c.743G.A p.R248Q
Substitution/missense 2.6 Yes DNA-binding273 c.818G.A p.R273H
Substitution/missense 2.6 Yes DNA-binding273 c.817C.T p.R273C
Substitution/missense 2.9 Yes DNA-binding282 c.844C.T p.R282W
Substitution/missense 2.2 Yes DNA-binding306 c.916C.T p.R306�
Substitution/nonsense 1.1 Yes Carboxy-terminal truncation342
c.1024C.T p.R342� Substitution/nonsense 1.3 Yes Carboxy-terminal
truncation
Structural, mutation affecting the folding of the DNA-binding
domain; null, mutation predicted to impair protein
synthesis; DNA-binding, mutation replacing an amino acid making
direct and specific contact with DNA; carboxy-
terminal truncation, mutation predicted as generating a protein
lacking the entire (p.R306�) or part of (p.R342�) carboxy-terminal
oligomerization domain.
Figure 1. (continued) (B, top) Codon distribution of mutations
(missense, nonsense, and indels) in the codingsequence of TP53,
based on mutation data derived from integrated genomic studies
compiled in the WholeGenomes Resource (v73) of the COSMIC mutation
database (cancer.sanger.ac.uk/cosmic/signatures), showingthe
position of major hotspots (.2% of all mutations) and mini hotspots
(1%–2% of all mutations). (Bottom)Codon distribution of missense
and nonsense mutationsbased on studies using conventional targeted
sequencingapproaches and compiled from the International Agency for
Research on Cancer (IARC) TP53 mutation database(version R.13, 2008
[Olivier et al. 2010]). The IARC distribution is displayed as a
mirror image of the COSMICdistribution. TAD1, TAD2, Transcriptional
activation domains 1 and 2; PRR, proline-rich region; DBD,
DNA-binding domain; JD, junctional domain; OD, oligomerization
domain; CTD, carboxy-terminal domain.
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/wgshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://perspectivesinmedicine.cshlp.org/
-
(Dorman et al. 2014). However, significant so-matic variations
occur in TP53 introns at sitesother than those implicated in splice
junctions,which are not covered in many conventionalor
exome-sequencing programs and thus arenot reported in mutation
databases. In BC, mu-tations in intron 9 colocalizing with
alternativeexons 9a and 9b have been detected using yeastfunctional
assays (Iggo et al. 2013). These mu-tations alter the balance
between fully splicedand alternatively spliced p53 transcripts,
leadingto the preferential synthesis of a protein thatlacks part of
the oligomerization domain. Inosteosarcoma, somatic rearrangements
in in-tron 1 have been detected by WGS in �20%of the cases (Ribi et
al. 2015). The rearrange-ment breakpoints are located across the
entiresequence of intron 1, but most of them cluster ina region of
1.7 kb located immediately upstreamof the locus encoding the
intronic Hp53int1transcript, suggesting that breakpoint may
befacilitated by open chromatin conformation atthis locus (Fig. 1A)
(Chen et al. 2014; Ribi et al.2015). So far, intron 1
rearrangements have notbeen observed in other sporadic cancers and
thereason for the narrow tissue specificity is un-known. The impact
of these rearrangementson p53 function remains to be analyzed, but
itis noteworthy that an intron 1 rearrangement(455-kb inversion)
cosegregates with inheritedrisk of several cancers in a Li–Fraumeni
family.The tumors of these patients show impairedTP53 transcription
and loss of heterozygosity(LOH) affecting the wild-type allele
(Ribi et al.2015). Osteosarcoma has been considered as atype of
cancer with low rate of TP53 mutationsin exons 2–11 (20%), partly
balanced by fre-quent functional inactivation of p53 proteinthrough
amplification of MDM2 (Ladanyiet al. 1993). The finding of intron 1
rearrange-ments in about half of sporadic osteosarcomasleads to a
call for reconsidering them as a cancerwith a high rate of somatic
TP53 mutations.
BEYOND MUTATIONS: IMPACT OF TP53HAPLOTYPES
TP53 contains more than 100 validated natural-ly occurring
single-nucleotide polymorphisms
(SNPs; see p53.iarc.fr/TP53GeneVariations.aspx) but only a few
of them have been stud-ied for their effect on p53 functions.
Thebest characterized exonic SNP is a nonsilentsubstitution at
codon 72 in exon 4 (rs1042522,g.7520197G.C, p.R72P), which is
present atminor allele (P) frequency between 10% (Cau-casians,
Northern Europe) and 50% (Africans,Yoruba), depending on population
(Whibleyet al. 2009). Several studies have shown thatthis SNP
specifies protein variants with differ-ent functional properties in
vitro and in ex-perimental in vivo models. The form of p53with R
(arginine) at codon 72 (p53R72) moreeffectively induces
p53-mediated apoptosisthan p53P72 (proline), partially through
tar-geting p53 to the mitochondria (Dumont et al.2003). Meanwhile,
p53P72, when comparedwith p53R72, more efficiently induces
cell-cyclearrest and DNA repair (Pim and Banks 2004;Siddique and
Sabapathy 2006). The ability ofmutant p53 to bind p73, neutralize
p73-in-duced apoptosis, and experimentally transformcells in
cooperation with EJ-Ras is enhancedwhen the mutant protein carries
an arginine atposition 72 (Marin et al. 2000). In addition,
R72alleles appear to be preferentially mutated andretained in
squamous cell carcinomas arising inpatients who are R72P germline
heterozygotes.Thus, this intragenic polymorphism may actas a
modifier of mutant TP53 effect, suggest-ing that mutations and /or
LOH may occurat different rates on different TP53 haplotypes.This
hypothesis is supported by results fromMechanic et al. (2007) who
analyzed 14 intra-genic TP53 SNPs in a case-control study oflung
cancer and uncovered an association be-tween several combinations
of SNPs and therisk of somatic mutation. The SNPs associatedwith
mutation were located between intron2 and intron 7, including
R72P/rs1042522(exon 4), rs9895829 (intron 4,
c.376-125T.C),rs1625895 (intron 6, c.672þ62A.G), andrs12951053
(intron 7, c.782þ92T.G), defin-ing the haplotype containing R-T-A-G
as morelikely to carry a mutation. The reason why thishaplotype is
preferentially mutated is unknown.In HCC carrying the
aflatoxin-induced p.R249Smutation, analysis of 19 SNPs spanning
the
P. Hainaut and G.P. Pfeifer
6 Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://p53.iarc.fr/TP53GeneVariations.aspxhttp://p53.iarc.fr/TP53GeneVariations.aspxhttp://p53.iarc.fr/TP53GeneVariations.aspxhttp://p53.iarc.fr/TP53GeneVariations.aspxhttp://perspectivesinmedicine.cshlp.org/
-
entire TP53 locus has shown a strong associa-tion between
mutation and haplotypes thatcarry a combination of two SNPs
(rs17882227and rs8064946) defining a linkage disequili-brium block
extending from upstream of non-coding exon 1 to the first half of
intron 1. Thisdomain contains two coding sequences over-lapping
with TP53 (WRAP53 and Hp53int1)(Ortiz-Cuaran et al. 2013). It is
possible thatthese SNPs may modulate the p53 antisenseactivity of
these transcripts, thus having an im-pact on p53 expression levels
and therefore onthe rate at which specific mutant alleles occurand
are retained during tumor development. Asimple way to rationalize
this notion is to con-sider that different haplotypes express p53
atdifferent levels, defining a continuum of func-tional p53
responses from “weak” to “strong”TP53 alleles, which may differ for
different bi-ological p53 effects (e.g., cell-cycle arrest,
apo-ptosis, control of metabolism, or DNA repair)(Fig. 2).
Mutations on a “weak” haplotype maybe more likely to require the
loss of the “strong”wild-type allele to exert a significant effect.
Incontrast, mutation on a “strong” haplotype mayhave disrupting,
dominant effects even if aweaker wild-type allele is present.
MUTATION PATTERNS AS SIGNATURESOF MUTAGENIC PROCESSES
TP53 mutations have been extensively used asclues for the
etiology of endogenous and exog-enous mutagenic processes that
operate duringcarcinogenesis in humans. Multiple indepen-dent
studies have been conducted by Sangersequencing of TP53 in tumors
selected fortheir suspected association with a mutagenor mutagenic
processes. The spectra producedby the aggregation of these somatic
mutationswere compared with the mutations experimen-tally generated
by the suspected mutagensin vitro or in vivo systems (Hollstein et
al.1999; Pfeifer 2015). Table 2 summarizes the“molecular
signatures” identified in TP53,caused by specific agents or
mutagenic process-es identified in TP53. This information has
beenextensively discussed in previous reviews(Greenblatt et al.
1994; Hainaut and Hollstein
2000; Olivier et al. 2004, 2010; Robles and Har-ris 2010;
Pfeifer 2015). Nonmelanoma skin can-cer (basal and squamous cell
carcinoma) andmelanoma show a predominance of G:C.A:Ttransitions at
dipyrimidine sites (mutated baseunderlined), including about 10% of
CC.TTtandem mutations, a type of mutation resultingfrom
UV-light-induced covalent coupling ofC¼C double bonds at adjacent
pyrimidines.These mutations are not caused by other
knowncarcinogens and are almost never observed intumors of internal
organs (Luo et al. 2001). InHCC, a unique transversion at codon
249(p.R249S; G:C.T:A) is highly prevalent in geo-graphic areas in
which the mycotoxin aflatoxinis a widespread contaminant of the
food (partsof Africa, Eastern Asia, South America) (re-viewed in
Gouas et al. 2009). In lung cancer,�30% of TP53 mutations are G:C
to T:A trans-versions in smokers, but not in never-smokers.This
class of mutation is the main mutageniceffect of polycyclic
aromatic hydrocarbons(PAHs) from the tar fraction of cigarette
smoke.Exposure of human bronchial cells to the diolepoxide of the
PAH benzo[a]pyrene causesDNA damage at the same G:C pairs that
arefrequently mutated into T:A in lung cancersfrom smokers
(Denissenko et al. 1996; Tretya-kova et al. 2002). Recently, a
mutational finger-print of aristolochic acid has been reportedin
urothelial carcinomas of subjects with a his-tory of exposure to
herbal remedies and foodproducts containing seeds of Aristolochia
clema-titis (Hollstein et al. 2013; Poon et al. 2013).Last, all
cancer types harbor at least 20% ofG:C.A:T mutations at
hypermutable CpG di-nucleotides, attributed to the normal
cellularevent of deamination of 5-methylcytosine tothymine. This
process is enhanced by inflam-mation, resulting in a high
prevalence of thesemutations in cancers associated with
chronicinflammation (Ambs et al. 1999; Cooks et al.2014). CpG
mutations are exceptionally com-mon in a few specific types of
cancer includingcolorectal, gastric, and esophageal cancers
(fre-quently occurring from precursor inflammato-ry lesions) as
well as in brain cancers.
The introduction of NGS has provided astepping-stone for a giant
leap in our under-
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
standing of the signatures of mutational pro-cesses in human
cancer. In addition to accessto large data sets (between a few
hundred and.10,000 mutations per tumor genome), NGSdata have
supported the development of acomputational framework that allows
decon-structing distinct but overlapping patternsfrom a set of
cancer samples (Alexandrov et al.2013a,b). Somatic mutations in the
genome ofany cancer are the result of cumulative muta-
genic processes encompassing endogenous andexogenous mechanisms,
each operating withdifferent temporal patterns and with
differentstrengths. Often, the cumulative pattern incancer does not
match any of the known sin-gle-operative mutational processes. By
usingalgorithms that decipher the minimal set ofmutagenic
signatures that optimally explainthe proportion of each mutation
type in eachcancer, it is now possible to estimate the contri-
MT WT
Mutation
MT WT
LOH
A
B
Figure 2. Variability and potential impact of TP53 haplotypes.
(A) Linkage disequilibrium (LD) plot in theHapMap Panel for
Caucasians, using 29 tag SNPs (tSNPs) for typing TP53 haplotypes
(Garritano et al. 2010). Thedegree of LD is indicated by shades
from black (strong LD) to white (no LD). This figure shows that
most tSNPsin intron 1 and the TP53 promoter are in strong LD,
forming a conserved haplotype block. (B) Model for loss
ofheterozygosity (LOH) at the wild-type (WT) allele depending on
the interplay between “strong” (red) and “weak”(green) mutant
haplotypes. (Top row) If the mutation (MT) occurs on a “strong”
haplotype, its effects maydominate the residual WT “weak”
haplotype, making LOH not compulsory. In all other haplotype
combinations,LOH is required to eliminate a WT haplotype stronger
than or equally strong as the one carrying the mutation.
P. Hainaut and G.P. Pfeifer
8 Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
Tabl
e2.
TP53
muta
tion
pat
tern
sas
asi
gnat
ure
ofm
uta
tional
pro
cess
es
Bas
ech
ange
(under
lined
)Ty
pe
Mec
han
ism
/
agen
t
Pro
muta
genic
lesi
on
Typic
alTP53
muta
tions
Can
cers
Ref
eren
ces
CC
.T
Tta
nd
emTr
ansi
tio
nSo
lar
UV
Dip
yrim
idin
ed
imer
sp
.S12
7F,
p.Q
136�
,p
.R15
8C,
p.H
179Y
,p
.R19
6�,
p.R
248W
,p
.R27
8F,
p.R
282W
No
nm
elan
om
ask
inB
rash
etal
.19
91
G:C
.T
:ATr
ansv
ersi
on
Afl
ato
xin
(AF
B1)
AF
B1-
N7-
guan
ine
add
uct
sp
.R24
9SL
iver
(hep
ato
cell
ula
rca
rcin
om
a)B
ress
acet
al.
1991
G:C
.T
:ATr
ansv
ersi
on
Tob
acco
smo
kePA
H-N
2-gu
anin
ead
du
cts
p.V
157F
,p
.R15
8L,
p.G
245V
,p
.G24
5C,
p.R
248L
,p
.R24
9M,
p.R
273L
,p
.D28
1E,
p.E
298�
Bro
nch
us
and
lun
g,h
ead
and
nec
k,es
op
hag
us
Den
isse
nko
etal
.19
96;
Tret
yako
vaet
al.
2002
A:T
.T
:ATr
ansv
ersi
on
Ari
sto
loch
icac
idA
rist
ola
ctam
-DN
Aad
du
cts
p.Q
104L
,p
.N13
1Y,
p.K
139�
,p
.K16
4�,
p.R
209�
,p
.R28
0S,
p.K
291�
Bla
dd
er/u
roth
eliu
mH
oll
stei
net
al.
2013
G:C
.A
:Tat
Cp
GTr
ansi
tio
nR
and
om
dea
min
atio
n5-
met
hyl
cyto
sin
ep
.R17
5S,p
.R21
3�,p
.R24
8Q,p
.R24
8W,
p.R
282W
,p
.R30
6�,
p.R
342�
All
can
cers
,in
par
ticu
lar,
colo
n,
sto
mac
h,
bra
inA
mb
set
al.
1999
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
bution of different signatures to each cancermutation
spectrum.
The first NGS studies focusing on muta-tion patterns were
published in Nature in 2010and reported the patterns of somatic
mutationsin malignant melanoma (Pleasance et al. 2010a)and
small-cell lung carcinoma (Pleasance et al.2010b). These studies
confirmed the wide-spread impact of UV light and tobacco
carcin-ogens, respectively, in these cancers. Since then,many
international consortia have undertakenthe sequencing of large
numbers of cancer sam-ples, and mutational signature genomic
pat-terns have been identified for many of them(Alexandrov et al.
2013a; Roberts and Gordenin2014). The COSMIC database website
providesa resource documenting up to 30 mutationalsignatures based
on pooled NGS data from10,952 exomes and 1048 whole genomes
across40 different types of cancers (accessible
atcancer.sanger.ac.uk/cosmic/signatures). Sever-al of these
signatures confirm and refine mu-tational processes already
described in TP53(COSMIC signature 1, spontaneous deamina-tion of
5meC; signature 4, tobacco smoke; sig-nature 7, UV light; signature
22, aristolochicacid; and signature 24, aflatoxin).
Surprisingly, there are only a few new mu-tational signatures
informing on exogenous car-cinogen exposure in addition to those
alreadydetected in TP53. One example is signature 11,which
corresponds to a distinct C.T mutationpattern caused by the
alkylating agent temozo-lomide in recurrent glioblastoma
multiformeof patients that have undergone this type ofchemotherapy.
On the other hand, NGS mu-tational signatures provide new insights
intoendogenous mutation processes, including mu-tational signatures
caused by the error-pronepolymerase h (signature 9, detected in
chroniclymphocytic leukemia and malignant B-celllymphomas), by
proofreading defects attribut-ed to polymerase 1 (signature 10, in
subsets ofcolorectal and uterine cancers), by defectivemismatch
repair (signatures 6, 15, 30, and 26,in gastric, colorectal, and
endometrial cancer),and by defective repair of DNA strand
breaksassociated with germline and somatic BRCA1and BRCA2 mutations
(signature 3, breast, pan-
creatic, and ovarian cancers). Several new mu-tation signatures
are still to be assigned to aspecific mechanism (signatures 5, 8,
12, 14,17–19, 21, 23, 25, 28, and 30). For example,esophageal
adenocarcinomas carry a very un-usual type of mutation, A-to-C
mutations at50 AA dinucleotides (Pfeifer 2015). There areno known
mutational processes, either endog-enous or exogenous, that have
been shown ex-perimentally to result in these types of muta-tions.
Because these events are highly specificfor a tissue traversed by
ingested materials, itis plausible that these mutations are caused
byexposure to an exogenous mutagen. Further-more, in addition to
the aforementioned expo-sures to aflatoxins, liver cancer genomes,
unlikeother cancer genomes, have very diverse pat-terns of
mutations targeting A/T base pairs.Because the liver is the primary
organ for me-tabolism of xenobiotics, it would not be surpris-ing
if these A/T-targeted mutations were causedby metabolites of
environmental carcinogens.
Some of the most interesting new data pro-vided by NGS is the
identification of an endog-enous pathway involving cytidine
deaminasesof the AID/APOBEC family (signatures 2 and13). Abnormal
targeting of cytidine deaminasesto random chromosomal locations
appearsto cause frequent C.T mutations at the cyto-sine of 50TpC
dinucleotides. The human ge-nome encodes eight APOBEC enzymes
(sevenof them located at the APOBEC3 gene cluster)that normally
serve to restrict viral infection andretrotransposon mobility by
deaminating cyto-sines during the ssDNA stage of their
replicationstages. These enzymes target TCA/TCT trinu-cleotides in
ssDNA in which they deaminateC to U, which is either directly
copied to Tor excised by uracil DNA glycosylase, followedby copying
of the resulting abasic site into C.Tor C.G mutations. Because of
the processivityof APOBEC enzymes, these mutations oftenoccur in
clusters. AID/APOBEC signatures arepresent in many forms of cancer,
and a germlinedeletion polymorphism affecting APOBEC3Aand APOBEC3B
is associated with large num-bers of them (Nik-Zainal et al.
2014).
It is now possible to revisit TP53 mutationpatterns in the light
of these extended and re-
P. Hainaut and G.P. Pfeifer
10 Advanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://cancer.sanger.ac.uk/cosmic/signatureshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://cancer.sanger.ac.uk/cosmic/signatureshttp://perspectivesinmedicine.cshlp.org/
-
fined mutational signatures. Recent studies haveidentified
APOBEC mutation patterns in TP53in BC (Lindley 2013) and lung
adenocarcinoma(Waters et al. 2015). Although these studiesare
useful to better understand the sequenceand codon context of
mutation formation inTP53, the amount of etiological
informationthey reveal is limited compared with multigenestudies
using NGS.
FUNCTIONAL DIVERSITY OF TP53MUTATIONS
The spectrum of TP53 mutation in cancer cellsand tissues is the
result of combined processesacting as filters that select cancer
mutationsamong a broad range of possible
mutations.Sequence-context-dependent mutagenesis andDNA repair
represent two of these filters. Thebiological selection of
functionally “meaning-ful” mutations represents a third filter.
Howev-er, what is a “meaningful” human cancer mu-tation is still
largely unclear.
The lowest common denominator of cancermutations is loss of
transcriptional function(LOF) altering the p53-dependent
transcrip-tional repertoire. Not all mutants are equal inthis
respect. The use of standardized yeast-basedassays to test for LOF
at total of 2314 mutantsrepresenting all possible substitutions
through-out the protein has shown that LOF is virtuallycomplete for
frequently occurring mutants (in-cluding hotspots) but that some of
the rarelyoccurring mutants retain quasi-wild-type func-tionality
for transactivation (Kato et al. 2003).Most of these rare
functional mutants and occuronly once or twice in the COSMIC
WGS/WESdata set (representing ,3% of all mutations).They may simply
represent passenger mutationswith no functional significance,
detected onlybecause of their accidental presence in an ex-panded
clone of transformed cells. An interest-ing parallel exists between
these mutants andthose occasionally detected in noncancer
tissuessuch as rheumatoid arthritis (RA), a noncancerprecursor
chronic inflammatory disease charac-terized by oligoclonal
proliferation of nontrans-formed synoviocytes. RA tissues
frequently con-tain clusters of cell clones with atypical TP53
mutations that include a high proportion ofsilent mutations
(14%), mutations retainingwild-type transactivation capacity (60%),
andmutations rarely found in any cancer (70% ofthem are either
absent or reported only once inthe WGS/WES COSMIC data set)
(Firesteinet al. 1997; Yamanishi et al. 2002). Such mutantsare
unlikely to be selected during carcinogenesisbut are carried over
as passengers in expandingsubclones of RA synoviocytes.
There is compelling experimental evidencethat TP53 mutations
induce functional changeswell beyond the scope of LOF. Many
missensep53 mutants are expressed as stable proteinsthat exert
dominant negative (DN) effects byinterfering with the product of
the remainingwild-type allele. A “prion-like” effect of somemutant
p53 over wild type has been shown invitro, in which the mutant
enforces wild-typeprotein to adopt a denatured, mutant-like
con-formation (Milner and Medcalf 1991). DNeffects may also result
from a “sponge” effect ofstable mutant p53 protein, absorbing the
low-abundance wild-type proteins into oligomersdominated by mutant
forms. Aside from DNeffects, gain-of-function (GOF) effects
havebeen demonstrated through which mutant p53exerts a number of
prooncogenic biochemi-cal activities. GOF effects have been
extensivelystudied in experimental cell systems and in ge-netically
modified mouse models (Brosh andRotter 2009; Muller and Vousden
2014). A num-ber of mechanisms have been proposed for mu-tant p53
GOF, including direct binding to DNAchanging (rather than
abolishing) gene expres-sion, binding to a large panel of
transcriptionfactors enhancing or impairing their function(e.g.,
binding to the p53 family members p63and p73), binding to a number
of proteins notdirectly involved in transcription (e.g., bindingto
the MRE11-RAD50-NSB1 complex, disrupt-ing its function), and
regulating microRNA net-works (e.g., miR130b, miR155, and
miR205)(Brosh and Rotter 2009; Muller and Vousden2014). Recently,
several p53 mutant proteinshave been shown to up-regulate a number
ofchromatin regulatory genes, including themethyltransferases
MLL1/KMTA2A and MLL2(KMT2D) and the acetyltransferase
MOZ/KAT6A,
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
resulting in a global increase in histone methyl-ation and
acetylation and suggesting that mutantp53 may induce GOF effects
through sweepingchanges in the epigenetic control of
chromatindynamics (Zhu et al. 2015). The functional con-sequences
of these GOF effects encompass theentire spectrum of the “hallmarks
of cancer”(Hanahan and Weinberg 2011; Solomon et al.2011). Thus, in
contrast to LOF, there is no sim-ple standard assay for scoring GOF
effects. Fur-thermore, there is no clear understanding of
thestructural properties of mutant p53 that supportGOF effects.
Given the multiplicity of GOFmechanisms, it is unlikely that all
effects dependon a single structural feature. In addition, mu-tants
with the most perturbed protein structureare not necessarily those
with the strongest GOFeffects. In contrast, these effects are
expected tobe subtle and context-dependent, because theyrequire
interactions between mutant p53 andproteinsthatare themselves
expressed in atissue-and context-dependent manner. The subtlety
ofGOF effects is illustrated by p.R249S, the mutantcaused by
aflatoxin-induced mutagenesis inHCC arising in a context of chronic
hepatitis B(HB) infection. This mutant is a clear LOF mu-tant, but
is not commonly considered as GOF inmost studies. However, its
mechanism of actioninvolves the binding of the HB antigen HBx,
ac-tivating it as a viral oncogene in liver cells (Jianget al.
2010; Gouas et al. 2012). This effect is atypical context-dependent
GOF effect. Thebinding specificity of p.R249S to HBx may ex-plain
the surprisingly narrow spectrum of afla-toxin-induced TP53
mutations in HCC, becauseother mutants potentially induced by
aflatoxinmay not bind HBx with the same efficacy asp.R249S,
preventing their selection during HB-dependent hepatocarcinogenesis
(Denissenkoet al. 1998).
CLASSIFYING TP53 MUTATIONS FORCLINICAL USE
Although a multitude of experimental studieshave shown different
effects of various mutantson proliferation, apoptosis, or responses
to cy-totoxic drugs, there is surprisingly little clinicalevidence
for association between different types
of mutations and clinicopathological variables,prognostics, or
prediction of therapeutic re-sponses. This does not imply that such
associ-ations do not exist. Perhaps the best evidence forclinically
relevant differences between differentmutations is found in
subjects who carry germ-line TP53 mutations. In a recent report on
322TP53 mutation carriers from French Li–Frau-meni families, the
mean age of tumor onset wasstatistically different between carriers
of mis-sense mutations (23.8 years) and those carryingnonsense
mutations or genomic rearrange-ments (28.5 years). The difference
was evenlarger when comparing hotspot mutations,such as p.R175H or
p.R248W (mean age of tu-mor onset, 15–20 yr) with complete deletion
ofthe TP53 gene (38.5 yr) (Bougeard et al. 2015).Assuming that
complete deletion of TP53 rep-resents a “straight” LOF effect,
these observa-tions suggest that the more severe clinical
phe-notype of hotspot mutants is caused by theircapacity to impair
the wild-type allele (DN ef-fects) and/or by specific GOF effects.
It is likelythat similar genotype–phenotype correlationsoccur for
somatic mutations.
Many clinical studies have tried to subdividesomatic mutations
into severity classes basedon localization and predicted structural
effects.Small clinical cohorts, suboptimal methodsused to assess
TP53 mutations status, and lackof consistency in how the mutations
are classi-fied have hindered a robust correlation withclinical
features. Computational approaches us-ing sequence similarities
such as SIFT (sortingintolerant from tolerant) generate
relativelyaccurate prediction for loss of transactivationfunction
in vitro (specificity, 90%; sensitivity,70% [Mathe et al. 2006])
but their clinical use-fulness is limited to the identification of
rarepassenger mutations. Two simple classificationalgorithms have
been used with some success(Fig. 3). The Poeta algorithm classifies
muta-tions into two a priori classes, disruptive andnondisruptive
mutations. Disruptive muta-tions combine predicted-null mutations
(non-sense, frameshift, and splice site) and chemical-ly
deleterious substitutions in loops formingthe DNA-binding surface
of the protein (Poetaet al. 2007). Nondisruptive mutations
include
P. Hainaut and G.P. Pfeifer
12 Advanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
Disruptive
No stableprotein
Stable mutant protein
0
0.0
0.2
0.4
0.6
0.8
Disruptive
0.0364NRNR27 41
76
Median timeto LRR (mo)
5-year freedomfrom LRR (%) P
Nondisruptive
Wild type
1.0
20 40
Follow-up (mo)
Pro
port
ion
of p
atie
nts
with
out L
RR
60 80 100
Non-missenseMissense DBM
Missense non-DBM
Mutations, codons 96–296
Olivier/hainaut algorithm (Olivier et al. 2006)
Poeta algorithm (Poeta et al. 2007)Locoregional recurrence, head
and neck
squamous cell carcinoma
Nondisruptive
Changingcharge/polarity
Othermotifs
L2/L3loops
Introducing aSTOP
Nonsense Missense
Mutations, codons 96–296
Wild typeNondisruptiveDisruptive
A
B1.0
0.9
0.8
0.7
0.6
0.5 p < 0.0001
Pro
port
ion
surv
ivin
g
Non-missense
DBM
Non-DBM
Wild type
Overall survival, breast cancer
0
No. at risk:1492
57178
65
135749
145
47
120840
117
38
103030
101
27
7692771
20
5692349
16
4101539
12
20 40 60
Time in months
80 100 120
Nonsense,frameshiftsplicing
Figure 3. TP53 mutation classification algorithms. (A) The Poeta
algorithm (left) (Poeta et al. 2007) classifiesmutations occurring
in the DNA-binding domain in two groups, disruptive (D) and
nondisruptive (ND)mutations. D mutations either preclude the
synthesis of p53 (nonsense mutations) or cause a
structurallyimportant amino acid change in the L2/L3 loops of the
DNA-binding domain. Other missense mutationsare classified as ND.
(Right) D and ND mutations have different prognostic value for
locoregional recurrence(LRR) in a cohort of 74 patients with
squamous head and neck cancer (Skinner et al. 2012). (B) The
Olivier/Hainaut algorithm (left) classifies mutations in three
groups: mutations predicting a null p53 protein (non-missense),
missense mutations in DNA-binding motifs (missense DBM), and
missense mutations outside theDNA-binding motif (missense non-DBM).
(Right) These three categories show different prognostic values
foroverall survival in a cohort of 1794 patients with breast cancer
(Olivier et al. 2006).
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
any other missense mutation. In head and necksquamous cell
cancer (HNSqCC), disruptivemutations are associated with decreased
overallsurvival, whereas there is no significant associ-ation with
nondisruptive mutations. Moreover,disruptive mutations predict
locoregional re-currence and HNSqCC cell lines with
disruptivemutations are significantly more radioresistantthan those
expressing nondisruptive mutations(Skinner et al. 2012). The
Olivier/Hainautalgorithm specifies three classes of
mutations,predicted-null, missense mutation in the DNA-binding
motif (DBM), and missense mutationin non-DNA-binding motif
(non-DBM) (Oliv-ier et al. 2006). The distinction between DBMand
non-DBM mutations is purely topologi-cal, based on the observation
that interspeciesconservation of amino acids in the loops ofthe DBM
is higher than in b-strands and shortintervening loops of the
non-DBM. The non-DBM is thus predicted to be more tolerant
tomutations than the DBM (Mathe et al. 2006). Ina large series of
1791 BCs from European pa-tients, the algorithm identified
predicted-nullmutations as having the strongest associationwith
poor survival, followed by DBM, whereasnon-DBM were just marginally
worse thanwild-type TP53 (Olivier et al. 2006). In theMETABRIC BC
cohort (1420 patients), no sta-tistical difference was found
between the threemutation classes, although DBM mutations ap-pear
to have a marginally more severe effect(Silwal-Pandit et al. 2014).
Incidentally, thefact that the two different classes of
missensemutations appear to have the same (or less)effects as
predicted-null mutations arguesagainst DN or GOF effects of
missense muta-tions in BC. When applied to non-small-celllung
cancer (NSCLC), the algorithm does notidentify any prognostic value
associated witheither mutation class. However, in a random-ized
trial of platinium-based therapy after sur-gery (525 patients, 221
with mutation; 42%),non-DBM mutations were associated withpoor
overall survival in the group that receivedchemotherapy but not in
the group treated bysurgery only (Ma et al. 2014). This effect was
notseen with predicted null or DBM mutations.This observation
suggests that non-DBM may
exert DN and/or GOF effects that confer resis-tance to adjuvant
therapy. It is interesting tonote that non-DBM mutations are
frequent inNSCLC of smokers, because of the frequent tar-geting by
tobacco carcinogens of codons encod-ing residues located in the
hydrophobic core ofthe protein (Le Calvez et al. 2005). The
selectionof these mutations may contribute to a form ofdrug
resistance in tumor cells.
Overall, these results indicate that the clinic-al severity of
mutations is tumor- and context-dependent. Thus, the same mutations
do notcarry the same clinical consequences in differentcancers.
Although it can be assumed thatthe LOF effects of mutations might
be roughlyequivalent in different tissue contexts, DN ef-fects are
dependent on the retention, expression,and activity of the
wild-type allele, and GOF ef-fects may depend on factors that are
expressed ina tissue- and context-dependent manner.
TP53 IN THE GENOMIC LANDSCAPEOF CANCER: SEEING THE NEEDLE
WITHINTHE HAYSTACK
Until recently, TP53 mutations have been most-ly approached as
stand-alone events in studiesof limited size and statistical power.
The de-velopment of integrative genomics combiningWGS/WES with DNA
copy number alterationsand studies on mRNA and protein
expressionprovides an unprecedented view of the generalgenomic
contexts in which TP53 mutations oc-cur (Kristensen et al. 2014).
In recent months,large consortium studies have combined
multi-dimensional molecular approaches to charac-terize the
landscape of genomic alterations inhuman cancers. These studies are
generating awealth of information that remains to be fullyexplored
using TP53 mutation as a magnifyinglens. Here, we briefly highlight
some of the newknowledge that integrative genomics is bring-ing to
our understanding of TP53 mutationsin breast and non-small-cell
lung cancer.
Breast Cancer (BC)
With mutation in 20%–25% of all cases, TP53ranks first in a
series of seven genes that are
P. Hainaut and G.P. Pfeifer
14 Advanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
mutated in .10% of BCs (including PIK3CA,ERBB2, MYC,
FGFR1/ZNF703, GATA3, andCCND1) (Stephens et al. 2012). A global
studyof the genomic and transcriptomic architectureof breast
cancers has identified up to 10 molec-ular subtypes (integrative
clusters) in whichTP53 mutations occur at significantly
differentfrequencies (Curtis et al. 2012). A detailed anal-ysis of
the TP53 mutation spectrum in the 1420BCs of the METABRIC cohort
has identifiedmutations in 28.3% of the cases (402 patients),with
significant variations across BC subtypes(Silwal-Pandit et al.
2014). Mutations are fre-quent in basal-like and HER2-enriched
tumors(65% and 53.4%, respectively), rare in luminalA and
normal-like tumors (9.3% and 11%, re-spectively), and occur at an
intermediate rate inluminal B tumors (24.8%). LOH at the TP53locus
is observed in 80.9% of the mutated tu-mors, independently of
molecular subtype.However, in TP53 wild-type cases, the frequen-cy
of LOH varies across subtypes (from 24%in basal-like to 52% in
luminal B). The distri-bution of mutations show striking
differencesbetween subtypes, with hotspot mutationsdominating the
spectrum of basal-like tumors,whereas a more uniform mutation
distributionis seen in other subtypes.
When examining the associations betweenmutation and prognosis,
TP53 mutation ap-pears to be strongly correlated with poor
overallsurvival in ER-positive patients but not in ER-negative
patients. In fact, the presence of a mu-tation seems to wipe out
the prognostic benefi-cial effect of ER positivity (Olivier et al.
2006;Silwal-Pandit et al. 2014). This observation sug-gests that
p53 may function as a rate-limitingfactor for ER signaling in BC, a
conjecture sup-ported by experimental data implicating p53in
estrogen responses in breast cancer cells (Fer-nandez-Cuesta et al.
2011a,b). Patients withmutant TP53 may thus not respond as well
toendocrine breast cancer therapy as patients withwild-type TP53.
In a recent study, p53 proteinaccumulation has been identified as a
strongpredictor of recurrence in ER-positive BC pa-tients treated
by aromatase inhibitor. It remainsto be shown whether this
accumulation is asso-ciated with mutant p53 (Yamamoto et al.
2014).
The association between TP53 mutation andBC prognosis is not
uniform across subtypes.Mutations are significantly associated with
poorsurvival in HER2-enriched, luminal B, and nor-mal-like but not
in basal-like or luminal A, sug-gesting a diverse role and impact
for TP53 muta-tions (Fig. 4) (Silwal-Pandit et al. 2014). In
basal-like cancers, disruption of the p53 pathway maybe an obligate
mechanism in virtually all tumors,either by mutation or byother
mechanisms. Pres-ence of wild-type TP53 may therefore not implyan
intact p53 pathway, explaining the lack ofprognostic value of TP53
mutations. In HER2-enriched cancers, mutation may disable the
ca-pacity of p53 to operate a safeguard mechanismagainst
oncogene-driven cell proliferation in-duced by activated HER2. In
luminal B and nor-mal-like cancers, disruption of TP53 function
isan optional mechanism and the occurrence of amutation and/or LOH
makes a significant differ-ence for tumor growth and progression,
thus en-tailing a clear negative prognostic value. In con-trast, in
luminal A cancers, mutation is a rareevent that may be relatively
unimportant. Thefact that luminal A mutations rarely occur at
hot-spots suggest that manyof them might be passen-ger mutations.
There is no significant differencein prognostic value between
different classes ofmutations in any of the subtypes.
With respect to predictive value of muta-tions, it has long been
suggested that docetaxelmay confer a greater therapeutic advantage
overanthracyclines in BC with mutated comparedwith wild-type TP53.
This hypothesis has notbeen substantiated in two large clinical
trials,which have confirmed the prognostic value ofmutant TP53 but
have not provided evidencefor a predictive effect of mutation on
responseto therapy (Bonnefoi et al. 2011; Fernandez-Cuesta et al.
2012).
Non-Small-Cell Lung Cancer (NSCLC)
NSCLC comprises two major histological enti-ties, squamous cell
carcinoma (SqCC) andadenocarcinoma (AdC), and several minor
his-tological subtypes including large-cell carcino-mas (LCCs). WES
reveals TP53 mutations in81% of SqCC, a frequency at the higher end
of
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 15
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
those reported in studies using Sanger sequenc-ing (range,
50%–80%), in which TP53 muta-tion load in SqCC appeared to
correlate withsmoking history (Le Calvez et al. 2005). TP53is by
far the most frequently mutated gene inSqCC, ahead of MLL2 (20%),
PI3KCA (16%),CDKN2A (15%), NFE2L2 (15%), and KEAP1(12%) (Clinical
Lung Cancer Genome Project2013). There is no obvious difference in
the pat-terns of mutated genes between TP53-mutatedand wild-type
cases, suggesting that disruptionof the p53 pathway is an obligate
mechanism inthe pathogenesis of SqCC. However, the highfrequency
precludes using TP53 mutations as aclassifier for identifying
molecular subtypes orfor investigating prognostic and predictive
val-ue. In AdC, mutations occur in 46% of the cases,ahead of KRAS
(33%), KEAP1 (17%), STK11(17%), EGFR (14%), NF1 (11%), and
BRAF(10%). It is striking to note that TP53 is theonly gene that is
commonly mutated in bothmajor histological types of NSCLC. In
bothAdC and SqCC, the pattern of TP53 mutationsis characterized by
a high rate of transversionsoccurring at G bases on the
nontranscribedstrand, a typical signature of mutations inducedby
tobacco smoke. This pattern is seen in all
histological subtypes but less marked in AdCthan SqCC. In AdC,
this pattern is not detectedin EGFR-mutated cases, which mostly
developin never smokers, and in which TP53 mutationsoccur at a
lower frequency than in smoking-re-lated KRAS-mutated cases (30%
vs. 60%, re-spectively). Independent of this associationwith
smoke-related mutation signatures, TP53mutation does not appear to
be associated withany specific molecular feature of AdC.
A multitude of cohort studies has failed toidentify a prognostic
effect for TP53 mutationson NSCLC survival, even in AdC and after
sep-arating TP53 into different classes (see, e.g.,Scoccianti et
al. 2012; Ma et al. 2014). However,in a comprehensive analysis of
1255 clinicallyannotated lung cancers by the Clinical LungCancer
Genome Project (CLCGP), TP53 muta-tion was found to be associated
with a signif-icant negative prognostic value in AdC withmutated
EGFR (Fig. 4) (Clinical Lung CancerGenome Project 2013). In fact,
AdC with mu-tated EGFR seems to have a more favorableprognosis than
AdC with other driver oncogenemutations, including KRAS. Although
TP53mutation does not appear to have an effect onthe prognosis of
AdC with mutated KRAS, it
0
0.0
0.2
0.4
BC
SS
pro
babi
lity
0.6
0.8
1.0
7385
6671
5248
3937
3430
2615
1614
96
wtmut
24 48
P = 0.030
TP53 mutant (e = 44)
TP53 wild type (e = 27)
72 96
Survival time (mo)
120 144 168 192
Breast cancerHER-2-enriched (n = 158)
1.0
0.8
0.6
0.4
0.2
0.0
0 10 20
12 15
16 TP53wt
TP53wt
Non-small-cell lung cancerEGFR mutant (n = 80)
TP53mut
TP53mut
StageI/II III/IV
37
P = 0.028 P = 0.01
30 40 50 60
Figure 4. Prognostic value of TP53 mutation in breast and lung
cancer driven by oncogenes of the EGF receptorfamily. (Left)
Prognostic value of TP53 mutations in patients with HER2-enriched
breast cancer subtype (Silwal-Pandit et al. 2014). (Right)
Prognostic value of TP53 mutations in patients with adenocarcinoma
of the lung withmutant EGFR (Clinical Lung Cancer Genome Project
2013).
P. Hainaut and G.P. Pfeifer
16 Advanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
cancels the apparent beneficial effect of EGFRmutation. It
should be noted that this beneficialeffect is not only attributable
to the responseof these patients to targeted EGFR therapies. Itis
also observed in a retrospective series of AdCpatients who have
been treated with conven-tional therapies. These observations
suggestthat wild-type p53 functions as a limiting factorin AdC
driven by oncogenic activation of EGFR.There is a striking
parallelism between the effectof TP53 mutation in EGFR-mutated lung
AdCand in HER2-enriched breast cancer (Fig. 4).
TP53 mutations have been reported as hav-ing a predictive effect
on the survival of patientstreated with adjuvant platinum-based
therapy,a standard treatment regimen for stage II–IIIcompletely
resected NSCLC (Ma et al. 2014).This effect predicts a marginal
benefit of adju-vant therapy in patients with wild-type TP53and
marginal detrimental effect in patientswith mutated TP53 mutation.
There is no effectof TP53 mutation in patients who are treatedby
surgery alone. As discussed above, this effectis significant only
for non-DBM mutations, aclass of mutations occurring in regions
encodingthe hydrophobic core structure of the p53 DNA-binding
domain. Mutations in the hydrophobiccore domain are frequent in
lung cancers ofsmokers, because of the targeting of codons inthis
region by carcinogens from tobacco smoke.These mutations may carry
GOF effect that, al-though having no impact on natural tumor
de-velopment (no prognostic value), accelerates tu-mor progression
or relapse under adjuvanttreatment (negative predictive value).
This par-ticular situation is a rare illustration of a possibleGOF
effect of mutant TP53 in a large random-ized clinical trial.
Presence of a non-DBM mu-tation appears to be associated with an
adverseeffect of adjuvant therapy, suggesting that thesetreatments
should be restricted to wild-typeTP53 cases. The molecular basis of
this effectremains to be identified.
CONCLUDING REMARKS: SOLVINGTHE TP53 MUTATION EQUATION
The biological and clinical significance of TP53mutation is the
result of a complex equation that
combines structural and functional terms. Themain structural
terms are the mutation itself(position, type, and effect on p53
protein struc-ture), the retention (or not) of a
functionalwild-type allele (LOH at TP53 locus), and thehaplotype
structure of both wild-type and mu-tant alleles, which may be
critical in the fine bal-ancing act by which one allele may
dominateover the other. Current sequencing strategiesare tailored
to assess only the first of these terms,and only in an incomplete
manner because moststudies remain focused on mutations occurringin
exons. A recent initiative of researchers in theTP53 mutation
field, led by Thierry Soussi, isrecommending that the entire
sequence of theTP53 gene should be taken into considerationwhen
developing mutational analysis strategiesto assess TP53 status. As
a next step, it will beimportant to design algorithms that enable
theassignment of haplotypes and LOH from se-quencing data, thus
providing the technical basisfor an assay capable of scoring all
the structuralterms of the mutant TP53 equation.
The functional terms of the equation areeven more complex.
Although the major gener-ic term is LOF, DN and GOF represent
addi-tional variables that may be extremely context-dependent.
There is currently no simple androbust assay to score DN and GOF
functionsin a clinical setting. This complexity is com-pounded by
the fact that, in many cancers, thep53 pathway may be disrupted by
other mech-anisms than structural alteration of the TP53gene, so
that tumors that apparently retain in-tact alleles actually do not
have an intact p53pathway. Many studies have analyzed the
tran-scriptomic patterns of TP53 dysfunction incancer cells and
tissues but so far no robustconsensus signature has emerged.
Although anumber of confirmed p53 target genes exist,their aberrant
expression in cancer tissue maynot be detectable without an inducer
or treat-ment, or the expression of these genes in can-cer tissue
may be altered by p53-independentmechanisms. Efforts should be
continued toidentify surrogate biomarkers of a disruptedp53
pathway. A promising approach is to inves-tigate p53-regulated long
and short noncodingRNA networks (Donzelli et al. 2014).
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 17
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
Integrative genomics studies are confirmingthat somatic TP53
mutation lies at the very cen-ter of the patterns of alterations
that character-ize the genomic landscape of cancer. They
alsoconfirm that the biological and clinical signifi-cance of TP53
mutation is very context-depen-dent, with large differences among
histologicalsubtypes of the same cancers. We propose todistinguish
three patterns of association be-tween TP53 and genomic landscapes,
highlight-ing their contrasting clinical messages.
High Mutation Frequency in Tumors withProfoundly Rearranged
Genomes
In many subtypes of cancer (in particular insolid tumors), the
mutation frequency is sohigh that it can be assumed that
deregulationof the p53 pathway is an obligate mechanism
forcarcinogenesis. These cancers often show verydisorganized
genomes with high overall muta-tion load, often associated with
intense expo-sure to endogenous or exogenous mutagens.They are
poorly responsive to either convention-al or pathway-targeted
therapies. This is the sit-uation observed in basal-like breast
cancer or inSqCC of the lung. The overarching role of TP53mutation
in these cancers might be to promoteand maintain metabolic and/or
epigenetic pro-grams essential for the expansion of
aggressivecancer cells with stem-like phenotypes. In turn,loss of
p53 function may promote genomic in-stability by favoring the
occurrence of massivecatastrophic genomic rearrangements such
aschromothripsis (Rausch et al. 2012). In thesetumors, TP53
mutation in itself may not be ofmuch clinical significance for
subclassifyingcases or stratifying patients. However, a
deeperevaluation of all structural terms of the TP53mutation
equation may uncover significant dif-ferences in the clinical
behavior of cancers withdifferent mutants. Despite having an
overallpoor prognosis, these tumors with frequentTP53 mutation show
a range of clinical behav-iors that may depend on factors that
modulatethe penetrance of TP53 mutation, such as LOH,haplotypes,
and alteration of regulators of p53function. In breast cancer,
combining TP53mutation, LOH, and MDM2 overexpression re-
veals an additive negative prognostic effect, sug-gesting that
several mechanisms of p53 inacti-vation may cooperate within the
same tumor(Silwal-Pandit et al. 2014).
Intermediate Mutation Frequency inOncogene-Driven Cancers
Knowledge of TP53 mutation status is provingof more direct
relevance in tumors with inter-mediate TP53 mutation frequencies,
such asEGFR-mutated lung AdC and HER2-enrichedBC. In these
oncogene-driven cancers, TP53mutation occurs at frequencies between
30%and 50% and is a clear indicator of poor prog-nosis. In both
cases, the driving event is theoncogenic activation of a
cell-surface tyrosinekinase receptor of the EGF superfamily and
itis plausible that TP53 mutation has similar con-sequences in both
cancers. An interesting hy-pothesis is that this effect is caused
by the in-volvement of p53 in regulating cell responsesto oncogenic
signaling through the p14arf–Mdm2 pathway. Inactivation of p53 by
muta-tion may switch off this pathway, thus eliminat-ing a natural
safeguard against excessive cellproliferation (Lomazzi et al.
2002). In supportof this hypothesis, we have reported that
p14arfexpression is often down-regulated in lungAdC with mutated
EGFR and wild-type TP53,suggesting that this pathway is under
strong neg-ative selection pressure in EGFR-mutated lungcancers
(Mounawar et al. 2007; Cortot et al.2014). However, why this effect
is seen withEGFR mutation or HER2 enrichment and notwith KRAS
mutation is not clear. Manipulatingthe p53 pathway to increase and
stabilize wild-type responses may prove a valuable
companionapproach in the treatment of these cancers, inparticular
with targeted therapies.
Low Mutation Frequencies in Tumorswith Actionable Wild-Type
TP53
A broad range of cancers has rare TP53 muta-tions, in particular
at early stages. These cancersinclude lesions of overall good
prognosis suchas adenoma of the colon or luminal A breastcancers,
in which rare TP53 mutations might
P. Hainaut and G.P. Pfeifer
18 Advanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
just be occasional passengers. Most of these le-sions are
adequately curated by surgery. How-ever, TP53 mutations are also
rare in severalcancer types requiring more aggressive treat-ment,
such as melanoma (6%) or osteosarcoma(10%–12%). In these cases, a
reassessment ofTP53 mutation status is warranted. It is
possiblethat significant structural alterations in TP53have been
missed in conventional studies be-cause they occur in regions of
the gene thatare not routinely screened. A dramatic exampleof such
a situation is observed in osteosarcoma,in which frameshift
alterations/translocationsare detected in intron 1 in �50% of the
caseswith no mutation in the coding sequence (Chenet al. 2014; Ribi
et al. 2015). Another potentialintragenic mechanism of inactivation
is over-expression of dominant-negative p53 isoforms,either caused
by deregulation of transcriptionand/or splicing, or by mutations in
intronsthat activate the expression of naturally occur-ring
isoforms (Marcel et al. 2011). For melano-ma, the frequent deletion
or mutation of theCDKN2A locus, which includes alterationsof
p14/ARF, may be a contributing factor forthe lower mutation
prevalence in the TP53gene itself (Hodis et al. 2012). The fact
thatmany of these tumors have in common the re-tention of a
potentially functional p53 pathwaysuggests that it may be possible
to pharmaco-logically “resuscitate” a suppressor function. Aproof
of principle has been given in cutaneousmelanoma, in which
overexpression of MDM4promotes the survival of human metastatic
mel-anoma by antagonizing p53 proapoptotic func-tion (Gembarska et
al. 2012). Inhibition of theMDM4–p53 interaction restores p53
functionin melanoma cells, resulting in increased sensi-tivity to
cytotoxic chemotherapy and to inhib-itors of the BRAF (V600E)
oncogene, thus iden-tifying MDM4 as a promising target for
therapyin melanoma.
In the coming years, TP53 mutation datawill continue to grow at
an unprecedented, ex-ponential pace because at least the
frequentlymutated exons of TP53 are included in mostcurrent
next-generation sequencing panels.During the weeks of redaction of
this article(May–July 2015), the COSMIC WGS/WES
TP53 mutation data set grew by more than1000 units. A large
concerted effort is neededto mine and annotate this enormous mass
ofinformation and to turn it into a source of de-tailed knowledge
for the biologist, the clinicianand, ultimately, for the benefit of
the patients.
REFERENCES�Reference is also in this collection.
Alexandrov LB, Nik-Zainal S, Wedge DC, Aparicio SA, Beh-jati S,
Biankin AV, Bignell GR, Bolli N, Borg A, Borresen-Dale AL, et al.
2013a. Signatures of mutational processesin human cancer. Nature
500: 415–421.
Alexandrov LB, Nik-Zainal S, Wedge DC, Campbell PJ,Stratton MR.
2013b. Deciphering signatures of muta-tional processes operative in
human cancer. Cell Rep 3:246–259.
Ambs S, Bennett WP, Merriam WG, Ogunfusika MO, OserSM,
Harrington AM, Shields PG, Felley-Bosco E, Hus-sain SP, Harris CC.
1999. Relationship between p53 mu-tations and inducible nitric
oxide synthase expression inhuman colorectal cancer. J Natl Cancer
Inst 91: 86–88.
Baker SJ, Fearon ER, Nigro JM, Hamilton SR, Preisinger AC,Jessup
JM, vanTuinen P, Ledbetter DH, Barker DF, Naka-mura Y, et al. 1989.
Chromosome 17 deletions and p53gene mutations in colorectal
carcinomas. Science 244:217–221.
Bartek J, Bartkova J, Vojtesek B, Staskova Z, Rejthar A,
Ko-varik J, Lane DP. 1990. Patterns of expression of the p53tumour
suppressor in human breast tissues and tumoursin situ and in vitro.
Int J Cancer 46: 839–844.
Beroud C, Soussi T. 1998. p53 gene mutation: Software
anddatabase. Nucleic Acids Res 26: 200–204.
Bonnefoi H, Piccart M, Bogaerts J, Mauriac L, Fumoleau P,Brain
E, Petit T, Rouanet P, Jassem J, Blot E, et al. 2011.TP53 status
for prediction of sensitivity to taxane versusnon-taxane
neoadjuvant chemotherapy in breast cancer(EORTC 10994/BIG 1-00): A
randomised phase 3 trial.Lancet Oncol 12: 527–539.
Bougeard G, Renaux-Petel M, Flaman JM, Charbonnier C,Fermey P,
Belotti M, Gauthier-Villars M, Stoppa-LyonnetD, Consolino E,
Brugieres L, et al. 2015. Revisiting Li–Fraumeni syndrome from TP53
mutation carriers. J ClinOncol 33: 2345–2352.
Brash DE, Rudolph JA, Simon JA, Lin A, McKenna GJ,Baden HP,
Halperin AJ, Ponten J. 1991. A role for sunlightin skin cancer:
UV-induced p53 mutations in squamouscell carcinoma. Proc Natl Acad
Sci 88: 10124–10128.
Bressac B, Kew M, Wands J, Ozturk M. 1991. Selective G to
Tmutations of p53 gene in hepatocellular carcinoma fromsouthern
Africa. Nature 350: 429–431.
Brosh R, Rotter V. 2009. When mutants gain new powers:News from
the mutant p53 field. Nat Rev Cancer 9: 701–713.
Chen X, Bahrami A, Pappo A, Easton J, Dalton J, Hedlund
E,Ellison D, Shurtleff S, Wu G, Wei L, et al. 2014.
Recurrentsomatic structural variations contribute to
tumorigenesisin pediatric osteosarcoma. Cell Rep 7: 104–112.
Somatic TP53 Mutations in the Era of Genome Sequencing
Advanced Online Article. Cite this article as Cold Spring Harb
Perspect Med doi: 10.1101/cshperspect.a026179 19
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
Clinical Lung Cancer Genome Project (CLCGP). 2013.
Agenomics-based classification of human lung tumors. SciTransl Med
5: 209ra153.
Cooks T, Harris CC, Oren M. 2014. Caught in the cross fire:p53
in inflammation. Carcinogenesis 35: 1680–1690.
Cortot AB, Younes M, Martel-Planche G, Guibert B, Isaac
S,Souquet PJ, Commo F, Girard P, Fouret P, Brambilla E,et al. 2014.
Mutation of TP53 and alteration of p14arf
expression in EGFR- and KRAS-mutated lung adenocar-cinomas. Clin
Lung Cancer 15: 124–130.
Courtois S, Caron de Fromentel C, Hainaut P. 2004. p53protein
variants: Structural and functional similaritieswith p63 and p73
isoforms. Oncogene 23: 631–638.
Curtis C, Shah SP, Chin SF, Turashvili G, Rueda OM, Dun-ning MJ,
Speed D, Lynch AG, Samarajiwa S, Yuan Y, et al.2012. The genomic
and transcriptomic architecture of2,000 breast tumours reveals
novel subgroups. Nature486: 346–352.
Denissenko MF, Pao A, Tang M, Pfeifer GP. 1996. Preferen-tial
formation of benzo[a]pyrene adducts at lung cancermutational
hotspots in P53. Science 274: 430–432.
Denissenko MF, Koudriakova TB, Smith L, O’Connor TR,Riggs AD,
Pfeifer GP. 1998. The p53 codon 249 muta-tional hotspot in
hepatocellular carcinoma is not relatedto selective formation or
persistence of aflatoxin B1 ad-ducts. Oncogene 17: 3007–3014.
Donzelli S, Strano S, Blandino G. 2014. microRNAs:
Shortnon-coding bullets of gain of function mutant p53 pro-teins.
Oncoscience 1: 427–433.
Dorman SN, Viner C, Rogan PK. 2014. Splicing mutationanalysis
reveals previously unrecognized pathways inlymph node–invasive
breast cancer. Sci Rep 4: 7063.
Dumont P, Leu JI, Della Pietra AC, George DL, Murphy M.2003. The
codon 72 polymorphic variants of p53 havemarkedly different
apoptotic potential. Nat Genet 33:357–365.
Fernandez-Cuesta L, Anaganti S, Hainaut P, Olivier M.2011a. p53
status influences response to tamoxifen butnot to fulvestrant in
breast cancer cell lines. Int J Cancer128: 1813–1821.
Fernandez-Cuesta L, Anaganti S, Hainaut P, Olivier M.2011b.
Estrogen levels act as a rheostat on p53 levelsand modulate
p53-dependent responses in breast cancercell lines. Breast Cancer
Res Treat 125: 35–42.
Fernandez-Cuesta L, Oakman C, Falagan-Lotsch P, SmothKS, Quinaux
E, Buyse M, Dolci MS, Azambuja ED, Hai-naut P, Dell’orto P, et al.
2012. Prognostic and predictivevalue of TP53 mutations in
node-positive breast cancerpatients treated with anthracycline- or
anthracycline/taxane-based adjuvant therapy: Results from the
BIG02-98 phase III trial. Breast Cancer Res 14: R70.
Firestein GS, Echeverri F, Yeo M, Zvaifler NJ, Green DR.1997.
Somatic mutations in the p53 tumor suppressorgene in rheumatoid
arthritis synovium. Proc Natl AcadSci 94: 10895–10900.
Garritano S, Gemignani F, Palmero EI, Olivier M, Martel-Planche
G, Le Calvez-Kelm F, Brugieres L, Vargas FR,Brentani RR,
Ashton-Prolla P, et al. 2010. Detailed hap-lotype analysis at the
TP53 locus in p.R337H mutationcarriers in the population of
Southern Brazil: Evidencefor a founder effect. Hum Mutat 31:
143–150.
Gembarska A, Luciani F, Fedele C, Russell EA, Dewaele M,Villar
S, Zwolinska A, Haupt S, de Lange J, Yip D, et al.2012. MDM4 is a
key therapeutic target in cutaneousmelanoma. Nat Med 18:
1239–1247.
Gouas D, Shi H, Hainaut P. 2009. The aflatoxin-inducedTP53
mutation at codon 249 (R249S): Biomarker ofexposure, early
detection and target for therapy. CancerLett 286: 29–37.
Gouas DA, Villar S, Ortiz-Cuaran S, Legros P, Ferro G, KirkGD,
Lesi OA, Mendy M, Bah E, Friesen MD, et al. 2012.TP53 R249S
mutation, genetic variations in HBX and riskof hepatocellular
carcinoma in The Gambia. Carcinogen-esis 33: 1219–1224.
Greenblatt MS, Bennett WP, Hollstein M, Harris CC.
1994.Mutations in the p53 tumor suppressor gene: Clues tocancer
etiology and molecular pathogenesis. Cancer Res54: 4855–4878.
Hainaut P, Hollstein M. 2000. p53 and human cancer: Thefirst ten
thousand mutations. Adv Cancer Res 77: 81–137.
Hanahan D, Weinberg RA. 2011. Hallmarks of cancer: Thenext
generation. Cell 144: 646–674.
Hodis E, Watson IR, Kryukov GV, Arold ST, Imielinski
M,Theurillat JP, Nickerson E, Auclair D, Li L, Place C, et al.2012.
A landscape of driver mutations in melanoma. Cell150: 251–263.
Hollstein M, Hergenhahn M, Yang Q, Bartsch H, Wang ZQ,Hainaut P.
1999. New approaches to understanding p53gene tumor mutation
spectra. Mutat Res 431: 199–209.
Hollstein M, Moriya M, Grollman AP, Olivier M. 2013.Analysis of
TP53 mutation spectra reveals the fingerprintof the potent
environmental carcinogen, aristolochicacid. Mutat Res 753:
41–49.
Iggo R, Rudewicz J, Monceau E, Sevenet N, Bergh J, SjoblomT,
Bonnefoi H. 2013. Validation of a yeast functional assayfor p53
mutations using clonal sequencing. J Pathol 231:441–448.
Jiang W, Wang XW, Unger T, Forgues M, Kim JW, HussainSP, Bowman
E, Spillare EA, Lipsky MM, Meck JM, et al.2010. Cooperation of
tumor-derived HBx mutantsand p53–249ser mutant in regulating cell
proliferation,anchorage-independent growth and aneuploidy in a
tel-omerase-immortalized normal human hepatocyte-de-rived cell
line. Int J Cancer 127: 1011–1020.
� Joruiz SM, Bourdon JC. 2016. p53 isoforms: Key regulatorsof
the cell fate decision. Cold Spring Harb Perspect Meddoi:
10.1101/cshperspect.a026039.
Kato S, Han SY, Liu W, Otsuka K, Shibata H, Kanamaru R,Ishioka
C. 2003. Understanding the function–structureand function–mutation
relationships of p53 tumor sup-pressor protein by high-resolution
missense mutationanalysis. Proc Natl Acad Sci 100: 8424–8429.
Khoury MP, Bourdon JC. 2010. The isoforms of the p53protein.
Cold Spring Harb Perspect Biol 2: a000927.
Kristensen VN, Lingjaerde OC, Russnes HG, Vollan HK,Frigessi A,
Borresen-Dale AL. 2014. Principles and meth-ods of integrative
genomic analyses in cancer. Nat RevCancer 14: 299–313.
Ladanyi M, Cha C, Lewis R, Jhanwar SC, Huvos AG, HealeyJH. 1993.
MDM2 gene amplification in metastatic oste-osarcoma. Cancer Res 53:
16–18.
P. Hainaut and G.P. Pfeifer
20 Advanced Online Article. Cite this article as Cold Spring
Harb Perspect Med doi: 10.1101/cshperspect.a026179
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
on June 5, 2021 - Published by Cold Spring Harbor Laboratory
Press http://perspectivesinmedicine.cshlp.org/Downloaded from
http://perspectivesinmedicine.cshlp.org/
-
Le Calvez F, Mukeria A, Hunt JD, Kelm O, Hung RJ, TaniereP,
Brennan P, Boffetta P, Zaridze DG, Hainaut P. 2005.TP53 and KRAS
mutation load and types in lung cancersin relation to tobacco
smoke: Distinct patterns in never,former, and current smokers.
Cancer Res 65: 5076–5083.
Lindley RA. 2013. The importance of codon context
forunderstanding the Ig-like somatic hypermutation strand-biased
patterns in TP53 mutations in breast cancer. CancerGenet 206:
222–226.
Lomazzi M, Moroni MC, Jensen MR, Frittoli E, Helin K.2002.
Suppression of the p53- or pRB-mediated G1checkpoint is required
for E2F-induced S-phase entry.Nat Genet 31: 190–194.
Luo JL, Tong WM, Yoon JH, Hergenhahn M, Koomagi R,Yang Q,
Galendo D, Pfeifer GP, Wang ZQ, Hollstein M.2001. UV-induced DNA
damage and mutations in Hupki(human p53 knock-in) mice recapitulate
p53 hotspotalterations in sun-exposed human skin. Cancer Res
61:8158–8163.
Ma X, Rousseau V, Sun H, Lantuejoul S, Filipits M, Pirker
R,Popper H, Mendiboure J, Vataire AL, Le Chevalier T, etal. 2014.
Significance of TP53 mutations as predictivemarkers of adjuvant
cisplatin-based chemotherapy incompletely resected non-small-cell
lung cancer. MolOncol 8: 555–564.
Mahmoudi S, Henriksson S, Corcoran M, Mendez-Vidal C,Wiman KG,
Farnebo M. 2009. Wrap53, a natural p53antisense transcript required
for p53 induction uponDNA damage. Mol Cell 33: 462–471.
Marcel V, Vijayakumar V, Fernandez-Cuesta L, Hafsi H,Sagne C,
Hautefeuille A, Olivier M, Hainaut P. 2010.p53 regulates the
transcription of its D133p53 isoformthrough specific response
elements contained within theTP53 P2 internal promoter. Oncogene
29: 2691–2700.
Marcel V, Dichtel-Danjoy ML, Sagne C, Hafsi H, Ma D,Ortiz-Cuaran
S, Olivier M, Hall J, Mollereau B, HainautP, et al. 2011.
Biological functions of p53 isoformsthrough evolution: Lessons from
animal and cellularmodels. Cell Death Differ 18: 1815–1824.
Marin MC, Jost CA, Brooks LA, Irwin MS, O’Nions J, TidyJA, James
N, McGregor JM, Harwood CA, Yulug IG, et al.2000. A common
polymorph










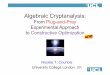


![Cryptographic Protocols and Smart Cards - Nicolas Courtois · Cryptographic Protocols and Smart Cards Nicolas T. Courtois 1, ex. 2 1 -University College of London , UK 2 = [Axalto+Gemplus]](https://img.pdfslide.us/doc/110x75/5cd03ea288c993924d8d9d7c/cryptographic-protocols-and-smart-cards-nicolas-cryptographic-protocols-and.jpg)






![Computer Security 1 [COMPGA01] Nicolas T. Courtois - University College London](https://img.pdfslide.us/doc/110x75/56649c9e5503460f9495de17/computer-security-1-compga01-nicolas-t-courtois-university-college-london.jpg)








