Embed Size (px)
Citation preview

J Korean Radiol Soc 1998; 39: 693- 698
Solitary Nodular Bronchioloalveolar Carcinoma ofthe Lung: Prediction ofHistology at High-Resolution CT
1
Hyun-JungJang, M.D., Kyung Soo Lee, M.D. , Yookyung Kirn, M.D. 2 Myung-HeeShin, M.D.3, In Wook Choo, M.D., SeungHoon Kirn, M.D.
WonJae Lee, M.D., Hong SikByun, M.D. , SangJin Kirn, M.D. 4
Purpose : The purpose of this study is to describe the characteristic high-resolution (HR) CT findings of solitary nodular bronchioloalveolar carcinoma (BAC) of the lung which are valuable for specific diagnosis ofthe disease.
Materials and Methods : HRCT scans of 46 patients (31 with malignant and 15 with benign lesion) with a solitary pulmonary nodule seen on chest radiograph were distributed in random order and analyzed retrospectively . Two blinded observers jointly analyzed the marginal and internal characteristics of nodules as seen on HRCT, and decisions on the findings were reached by consensus. Stepwise discriminant analysis for characteristic findings ofBAC was performed.
Results : The most frequent CT findings ofBAC (n= 15) were internal bubble lucency (1 4/15 , 93 %)(p=O .-OOl), area of ground-glass opacity (12 /1 5, 80 % ; average 58 % of tumor volume)(p=O.OOOl), pleural tag(12/15 , 80 % ; p=0.097), and lobulated and spiculated margin(8 /1 5, 53 % ; p=0 .459). Findings of ground-glass opacity (p=O.OOOl) and bubble lucency (p=0.0187) appeared to be discriminant in the diagnosis of BAC.
Conclusion : Peripheral pulmonary nodules containing an area of ground-glass opacity associated with internal bubble-lucency are characteristic ofBAC. Specific histologic diagnosis of solitary nodular BAC can be suggested by careful analysis ofHRCT findings.
Index words : Lung, CT Lung, nodule Lung neoplasms, diagnosis Lung neoplasms, CT
Bronchioloalveolar carcinoma (BAC) of the lung is a subtype of adenocarcinoma(1 - 4). Its unique features are its histologic lepidic growth pattern using the alveolar septa as a stroma and its mode of aerogenous spread(5 -7). BAC displays a broad spectrum ofradi이ogic features that can be categorized as solitary nodular, segmental or lobar, or the diffuse multinodular
'Depar tment of Radiology, Samsung Medical Center, College of Medicine, Sung Kyun Kwan University
'Department of Diagnost ic Radiology, College of Medicine, Ewha W omans Uni. versity
JDepartment of Center for Health Promotion, Samsung Medical Center 'Department of Diagnost ic Radiology, Yongdong Severance Hospital Received November 3, 1997; Accepted July 24, 1998
Address reprint requests to : Kyung Soo Lee, M.D. , Department of Radiology Samsung Medical Center, # 50 Irwon.Dong, Kangnam-Ku Seoul 135.230, South Korea. Tel. 82. 2.3410.25 11 Fax.82. 2.341O. 2559
- 693
type(7, 8). With its favorable prognosis and distinctive radiologic features, solitary nodular BAC, the most commonly presenting form, is generally considered a separate clinical entity(5 , 7, 9). Reported CT findings of solitary nodular BAC include a peripheral subpleural location, internal bubble lucency or pseudocavitation, heterogeneous attenuation, irregular margins and pleural tag. These findings are not specific, however, they are frequently observed in adenocarcinoma and large cell carcinoma ofthe lung( lO).
In over 70 % of patients, nod ular BAC less than 3 cm in diameter responds to surgery (ll) and when less than 2cm, the reported five-year survival rate is 98. 2 %(3). Early recognition is therefore important. In a recent study involving a small number of patients, we

Hyun-Jung Jang. et al : S이itary Nodular 8ronchioloalveolar Carcinöma of the Lung
reported that a localized area of ground-glass opacity, with internal bubble lucency on high-resolution CT (HRCT), is an early finding of BAC(12). The result of 2-[fluorine-181-fluoro-2-deoxy-D-glucose (FDG) positron emission tomography(PET), however, may be negative(12 - 14). In addition, presumably because of sparse cellularity, we have experienced false negative results of percutaneous needle aspiration biopsy of these lesions. So as not to overlook this surgically curable disease, solitary nodular BAC needs to be recognized , if possible, on the basis of specific imaging features.
The aim of this stud y is to determine the findings which most effectively discriminate between solitary nodular BAC and other pulmonary nodules. Our approach involves the use of HRCT followed by stepwise discriminant analysis.
Materials and Methods
Selection of patients and image acquisition
This study involved 46 patients in whom solitary pulmonary nodules were seen on chest radiographs, and who underwent HRCT between November 1994 and May 1997. Nodules were consecutively proved by surgery and satisfied the following inclusion criteria on chest radiographs: less than 3 cm in maximal dimension, a location peripheral to that of segmental bronchi,
and with no enlarged hilar or mediastinal lymph nodes. The patients were 20 men and 26 women, and were aged between 16 and 78 (mean, 58.8) years. All underwent surgery and definite diagnoses were made on the basis of histopathologic examination of specimens. Pathologic entities included lung cancer(n=30) ; BAC(n = 15), adenocarcinoma(n = 11), squamous cell carcinoma(n=2), large cell carcinoma(n= l), and mucoepidermoid carcinoma(n=1), and benign nodules(n= 16); aspergilloma(n=7), hamartoma(n=5), and tuberculoma(n =4)
For CT examinations , a GE HiSpeed Advantage scanner (General Electrical Medical Systems, Milwaukee, WI, U.S.A) was used. Before obtaining conventional CT images using the helical technique (lO-mm collimation, pitch of one) with administration of contrast(lOOmL of Iopamiro 300: IopamidoL Bracco, Milan, Italy), thin-section (1-mm collimation) CT scans of all patients were obtained at 3-mm (n=19) or 5-mm (n=27) intervals throughout the nodule. Scan data were reconstructed using a bone algorithm(HRCT). Images were obtained both at mediastinal (WW: 400, WL: 30) and lung window (WW: 1500H, WL: -700) settings.
- 694
Image interpretation The HRCT scans of all patients were randomly dis
tributed and assessed by two experienced chest radiologists, whose decisions were consensual. Observers had no knowledge of clinical or pathologic data other than the age and sex of the patients; they were not aware of which diseases were included in the study nor, the frequency ofindividual diseases.
The evaluated HRCT findings included the followings : (a) size (b) edge, classified as smooth, lobulated , spiculated , or lobulated and spiculated; the presence of (c) open bronchus sign, (d) positive bronchus sign, (e) bubble lucency, (f) pleural tag, (g) satellite lesion, (h) air-crescent sign, (i) ground-glass opacity and the percentage of the nodule it accounted foι estimated visually; and (j) calcification and its characteristics, classified as central, laminated, popcorn-like, nodular, or stippled. Open bronchus sign (previous CT air bronchogram) was considered to be present if there was patent branching airway structure(s) within a nodule (15 , 16). Positive bronchus sign was regarded as present if a bronchus extended up to, and entered the nodule(17). Bubble lucency was considered to be present if there were small scattered areas of air attenuation (oval or round) within a nodule(15). 'Pleural tag' was defined as linear structure(s) originating from the margin of a nodule and extending peripherally to contact the pleural surface. ‘Satellite nodule' was defined as one or more micronodule(s) surrounding the dominant nodule. 'Air-crescent sign' was defined as curvilinear air density around a nodule.
Statistical analysis Using the chi square test, the frequency of each CT
finding of BAC was compared with that of other nodules. A p-value less than 0.05 was considered significant.
Age, sex, and CT features were evaluated using stepwise discriminant analysis; this identifies the discriminant CT findings that most accurately measure the characteristics of solitary nodular BAC 뻐d permit differentiation between various cell types of lung cancer and benign nodules. The objective is to maximize separation of groups by weighting and combining the discriminant variables in some linear form. A user-selected criterion is applied, and the single best discriminating variable is selected. All remaining potential variables are then tested(18, 19). In this study, the ability to classify cases correctly using the discriminant function was measured using Fischer’s exact test. The mag nitude of the coefficient in the resulting discriminant function reflects the unit of measurement as well as its

J Korean Radiol Soc 1998; 39 : 693- 698
relative contribution. SAS software (system for Windows version 6.11) was used
Results
Solitary nodular BAC was found in seven men and eight women, aged between 39 and 72 (mean, 59) years The BAC ranged in size from 1.5 to 3.0 (mean, 2.4)cm.
The most frequent CT findings of BAC were internal bubble lucency (14/1 5, 93 %) (p=O.OOI) (Figs. 1 and 2), area of ground-glass opacity (1 2/15, 80 %, [average 58 % of tumor volume]) (p=O.OOOI) (Figs. 1-3), pleuraltag (12/15 , 80 %) (p=0.097) (Figs. 1 and 3), and lobulated and spiculated margin (8 /1 5, 53 %) (p=0.459) (Figs. 1 and 3) (Table 1). Open bronchus sign, positive bronchus sign, calcification, and satellite nodule were seen in four(27 %), three(20 %), one(7 %), and one (7 %) patient, respectively ; all p values were greater than O.
05. Calcification was stippled . Stepwise discriminant analysis showed that areas of
ground-glass opacity (p=O.OOOl) and bubble lucency (p=0.0058) individually were useful for distinguishing BAC from other cell types of lung cancer and benign lesions(Table 2).
Discussion
Kuhlman et al (10) reviewed the thin-section CT (2 - 5 mm collimation) findings of solitary nod ular BAC in 30 patients. In their series, peripheral or subpleural location(25/30, 83 %), irregular margins forming a star pattern(22/30, 73 %), pleural tag(70 %), pseudocavitation(18/30, 60 %), and heterogeneous attenuation (17 / 30, 57 %) were suggested CT criteria for solitary nodular BAC. In their study, however, there is considerable overlap of CT findings of BAC, particularly between
2
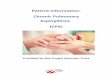
Fig. 1. Bronchioloalveolar carcinoma in a 63-year-old woman. High-resolution CT scan obtained at level of azygos arch shows area of groundglass opacity showing internal bubble lucencies (arrows) and open bronchus sign (arrowhead) in right upper lobe. Pleural tag is seen. Fig. 2. Bronchioloalveolar carcinoma in a 60-year-old woman. Lung window of high-resolution CT scan obtained at level of great vessels shows localized area of ground-glass opacity in right upper lobe. AIso note internal bubble lucency(arrow).
v m
않 」때 않 아 아 ν싸
…… …r ”r
」ωk
m
J싸 m ”m
양 m
O
’h
·m T
나A i
ti
J」O
e
리 O
K
K
s a p n
m m
μω 이뺑
W
%
m m
때 m
빼“
m
ιM Tι 뻐 때 않 um m
a m Fι H
갔 d
h ·E
g
,
ε 따 b J
α 껑 R
、% x
r w m e Lh
@
따 m x o n h M
m
야 ω m m U
iA
, ‘ ιu c y
U
f
j
S
·U
’n ·l
1i
I
F
3
때 ·m p h .m .m
η mi m
페
M
$
뼈 빠 에 ’않 % @
싸M
K
뻐 d
g
M
s m“
‘베
L
%
m w m m ·k
야 외 γ L…
갱 m
얘 얀 ‘야 W
£ m
μI s--m
1
,t
f
·히 U
--떼 갱
k
l
m n‘ ( o p e j
qL
C
h
s ‘r
α b
e
값 ’μ
뼈 뼈 뼈 m m m 이 ·m
뻐 따 때 hm
캔 이핑 .삐 땅 뼈 뿌
hm
ψ F
:
,밍 잉 h
$
e b
c m n
리 H
C
·π 시」
3
m
m
업 야 .n
#」뼈 K m
d
야 뼈 1
·m
녀 따 ·뻐 여 빠 m
&
께“ 때‘
·m C
’ι 4b
N
뼈 R
μω ”ω 때 따 d
따 얀 4b
’b
5
πr e n s ,d
L
a lL
」n e o m n u 1d
fι
3 6
아ι 비 ·m
맹 m
아 l
,양”
4
I
P ·m -M
α t
m ·m
. U
빼 때 따 낌 m
.와 mr
않 ·n‘ M
m
따 바 ’ t
4뺑 m k
F ·n
E
n o a g d
징 h F
o p c o u n g
이
.m 。“
m m m 않
l vι
때
.κ
앵
-li o 뼈
pi
뼈
cJ ·m
4
뺑
때
a‘ 민
e 띠 뼈
아
n ·m n nu nr 때
’n -mi ,‘
-695 -

Hyun-Jung ‘ Jang, et al : Solitary Nodular Bronchioloalveolar Carcinoma of the Lung
Table 1. CT Findings of 46 Nodules with Various Histology
Histology ofPulmonary Nodules
CTFindings BAC Adeno Squ따no Large Mucoepi Tuberc Hamar Asper (n=15) (n= ll) (n=2) (n=l) (n=l) (n=4) (n=5) (n=7)
Internal bubble lucency* 14(93)+ 2 (18) 1 ( 50) 0 1 (100) 3 (75) 0 3 (42) Area of ground-glass opacity* 12 (80) 2 (18) 0 0 0 1 (25) 0 4(58)
average % oftumor volume 58 15 0 0 0 20 0 13
Pleural tag 12 (80) 9 (82) 1 ( 50) 0 0 3 (75) 0 4(58) Lobulated & Spiculated margin 8 (53) 5 (46) 2 (100) 0 1 (100) 2 (50) 0 2 (29) Open bronchus sign 4 (27) o ( 0) 0 0 1 (100) o ( 0) 0 2 (29) Positive bronchus sign 3 (20) 3 (27) 1 ( 50) 0 0 0 0 0 Calcification 1 ( 7) 2 (18) 0 0 1 (100) 1 (25) 2(4이 2 (29) Satellite nodule 1 ( 7) 1 ( 9) 0 0 1 (100) 3 (75) 0 5 (71) Air crescent sign 0 0 0 0 0 0 0 5 (71)
* statistically significant in BAC compared to frequency of other nod ules, + numbers in parenthesis are percentage, BAC: bronchioloalveolar carcinoma, Adeno : adenocarcinoma, Squamo: squamous cell carcinoma, Large : large cell carcinoma, mucoepi : mucoepidermoid carcinoma, Tuberc : tuberculoma , Hamar: hamartoma, Asper : aspergilloma
Table 2. CT Factors Ranked by Stepwise Discriminant Analysis in Ability to Enable Differentiation ofBronchioloalveolar Carcinoma from Other Histologic Types of Pulmonary Nodules
Factors Partial R2 F Statistics probability
Area of ground-glass 0.4631 37.790 0.0001 opacity
Bubble lucency 0.1638 8.424 0.0058 Age 0.1254 6.022 0.0184
R2: a measure ofthe goodness offit ofthe model. F: a value of the distribution of the model divided by that of error
adenocarcinoma and large cell undifferentiated carci noma. In our study, the most frequent CT findings of BAC were internal bubble lucency or pseudocavitation(93 %), area of ground-glass opacity (80 %) with an average of 58 % of tumor vo1ume, p1eural tag(80 %), and lobulated and spicu1ated margin(53 %). In stepwise discriminant ana1ysis, areas of ground-g1ass opacity appeared to be the most discriminant finding, followed by bubble 1ucency, for distinguishing BAC from other histo1ogic types ofpulmonary nodules.
With regard to the prevalence of characteristic findings of BAC, our resu1ts were somewhat different from those of Kuhlman et a1( 1O). However, there is a significant difference in scan technique that may be partly responsib1e for the different prevalence. They used a variety of window widths and 1evels which ranged from 1, 164 to 1,800 and from - 180 to - 500, respectively; we, on the other hand, used a standard window width of 1,500 and window 1evel of - 700. In
- 696
addition, their study used a thicker (2 - 5 mm collimation) CT section than ours(I .0-mm collimation). Ground-g1ass opacity could not, therefore, be appropriate1y assessed in their study, and there might be differences in the assessment of edge characteristics as well as nodu1e size.
In our previous study invo1ving a small number of cases, we concluded that a focal area of ground-g1ass opacity, seen on HRCT, is “ one of a variety of appearances of BAC"(12). The present study demonstrated that areas of ground-g1ass opacity within a nodu1e is the most va1uab1e finding for discriminating BAC from other pu1monary nodu1es, is a common and generally applicable finding(80 %).
Our results can be exp1ained on the basis of current patho1ogic concepts for adenocarcinoma( 2 - 4, 20) Most adenocarcinomas are believed to deve10p either de novo or through the stage of atypica1 adenomatous hyperp1asia (bronchioloa1veo1ar adenoma [BAA])(2, 4, 21). The latter concept ofmultistep carcinogenesis and progression has been described by Miller et a1. as an adenoma-carcinoma sequence, which is well known in the co1on(20). Bronchio1oa1veolar carcinoma with replacement growth pattern is often accompanied by BAA at the periphery and may consist of hetero geneous components showing different stages of differentiation that strong1y supports the 1atter way of deve1opment. In contrast, nonreplacement-type adenocarcinoma, which shows a pattern of largely solid and destructive growth, is thought- because ofthe absence of such stepwise progression - to be de novo type(2). It has been well documented that BAA appears as a small

J Korean Radiol Soc 1998; 39: 693-698
nodule with ground-glass opacity(22). Our previous study revealed that nonmucinous nodular BAC, in which pathologic findings showed that the tumor grows as a single celllayer along alveolar walls, can also manifest as a focal area of ground-glass opacity(12). In a study by Noguchi et al(2), BACs were grouped into three distinctive structural patterns: type A, with minimal thickening of alveolar septa; type B, with a similar appearance to type A but with fibrotic foci due to alve이ar c이lapse; type C, with foci of fibroblastic pr이iferation which appeared to be an advanced stage of types A and B. For these two types the prognosis is excellent, with a five-year survival rate of 100 %. For type C, on the other hand, the rate is 74.8 %, which is similar to the average for overall small adenocarcinomas. In the light of those studies, we can speculate that areas of ground-glass opacity within the nodule is the most representative feature of BAC to re f1ect its developing nature.
We found that among non-BAC cancers, adenocarcinoma occasionally simulated the findings of BAC,
with-in two of eleven patients-areas of ground-glass opacity and bubble lucency(Fig. 4). The pathology of those two cases was 'adenocarcinoma with BAC features'. It is therefore more plausible to regard this similar appearance as a re f1ection ofmicroscopic (BAC) features, as seen on HRCT, than to consider those findings as nonspecific for BAC. Though there is no pathologic explanation, our experience has shown that simple pulmonary eosinophilia can totally mimic such characteristic features of BAC when it occurs as a soli tary lesion. Because ofits transient and f1eeting nature,
follow-up CT scans obtained within six to eight weeks-if these indicate the disappearance of focal area of ground-glass opacity-can solve the problem(23).
In comparison to other studies of equal or greater sample size( lO, 15), the proportion of BAC relative to adenocarcinoma was much higher (15 versus 11) in this study. Although the incidence of BAC varies widely, from three percent of all pulmonary carcinomas in a Baltimore series to 38 percent in a Japanese series(4), It is thought to be partly due to differences in study design. In the study of Zwirewich et al. (15), the mean diameter of adenocarcinoma and that of BAC are 3.5cm and 3.1 cm, respectively. On the other hand , our study was strictly limited to solitary pulmonary nodules consecutively proved by surg
m m
Kurokawa et al (3) and 74.2 % (175/236) according to Noguchi et al. (2). Those studies showed that BAC accounted for a considerable proportion of small resectable adenocarcinomas.
Because we included only nodules confirmed by surgery, there might be selection bias in interpreting the CT appearances of benign nodules. In fact, except for symptomatic aspergillomas with typical CT features of air crescent sign, the appearance of all benign nodules in this study was somewhat malignant or equivocal. Conversely, because we included cases of surgically confirmed benign nodules of malignant appearance, the discriminant findings suggested by our study may in clinical practice be more helpful in distinguishing nodules according to their histologic differences.
In conclusion, among many reported features of solitary nodular BAC seen on HRCT, an area of groundglass opacity appears to be the most discriminant finding for distinguishing BAC from other histologic types of pulmonary nodules, followed by bubble lucency. Being familiar with these discriminative findings in combination with other characteristic findings discussed, we can strongly suggest a specific histologic diagnosis of solitary nodular BAC. This unique lung cancer with favorable prognosis cannot, therefore, be missed even when the results of percutaneous needle aspiration biopsy are negative.
References
1. Kreyberg L. Hist%gica/ typing of /ung tumors. Vol l. Inter
national histological classification of tumors, Geneva, 1967,
Wold Health Organization.
2. Noguchi M, Morikawa A, Kawasaki M, et al. Small adenocar
cinoma of the lung. Histologic characteristics and prognosis.
Cancer 1995 ; 75: 2844-2852
3 ‘ Kurokawa T, Matsuno Y, Noguchi M , Mizuno S, Shimosato Y
Surgically curable “ early" adenocarcinoma in the periphery of
the lung. Am J Surg Patho/ 1994; 18: 431-438
4. Clayton F. The spectrum and significance of bronchioloalveolar
carcinomas. Patho/ Annu 1988 ; 23: 361-394
5‘ Epstein DM. Bronchioloalve이ar carcinoma. Semin Roentgeno/
1977; 12: 207-214
6. Edward cw. Alveolar carcinoma: a review. Thorax 1984; 39
166-174
7. Hill CA. Bronchioloalveolar carcinoma: a review. Radi%gy
1984; 150: 15-20
8. Adler B, Padley S, Miller RR, Mííller NL. High-Resolution CT
of bronchioloalveolar carcinoma AJR 1992; 159 : 275-277
9. Miller WT, Husted J , Firman D, Atkinson B, Pietra G
Bronchioloalveolar carcinoma: two clinical entities with one
pathologic diagnosis. AJR 1978 ; 130: 905-912
10. Kuhlman JE, Fishman EK, Kuhajda FP, et al. Solitary bronchiol
oalveolar carcinoma: CT criteria. Radi%gy 1988 ; 167: 379-382

Hyun-Jung Jang. et al : Solitary Nodular Bronchioloalveolar Carcinoma of the Lung
II ‘ Greco RJ, Steiner RM, Goldma n S, Cotler H, Patchefsky A,
Cohn HE. Bronchioloalveolar cell carcinoma of the lung ‘ Ann
Thorac Surg 1986; 41: 652-656
12. Jang HJ, Lee KS, Kwon OJ, Rhee CH, Shim YM, Han J
Bronchioloalveolar Carcinoma: focal area of ground-glass at
tenuation at thin-section CT as an early sign. Radiology 1996;
199 : 485-488
13. Kim BT, Lee KS, Kim Y, et al. Solitary nodular bronchioloal
veo lar carcinoma of the lung: FDG PET findings. AJR (in press)
14. Scott WJ, Schwabe JL, Gupta NC, Dewan NA, Reeb SD, Sug
imoto JT. Positron emission tomography of lung tumors and
mediastinal Iymph nodes using [18F] fluorodeoxyglucose. Ann
Thorac Surg 1994; 58 : 698-703
15. Zwirewich CV, Vedal S, Miller RR, Müller NL. Solitary pul
monary nodule: high-resolution CT and radiologic-pathologic
correlation. Radiology 1991 ; 179: 469-476
16. Kuriyama K, Tateishi R, Doi 0 , et al. Prevalence of air
bronchograms in small peripheral carcinomas of the lung on
thin-section CT: comparison with benign tumors. AJR 1991;
156: 921-924
17. Swensen SJ. Focal lung di sease: CT and high-resolution CT
applications. RadioGmphics 1994; 14: 169- 181
18. Armitage P. Statistica/ methods in medical research. 3rd ed
Oxford: Blackwell , 1974; 302-344
19. Kleinbaum DE, Kupper LL. Applied regression an띠)잉s and other
mu/tivariate methods. North Scituate, Mass: Duxbury , 1978;
41 4-446
20. Miller RR, Nelems B, Evans KG, Mtiller NL, Ostrow DN
Glandular neoplasia of the lung. A proposed analogy to colonic
tumors. Cancer 1988 ;61: 1009-1014
21. Shimosato Y, Noguchi M, Matsuno Y. Adenocarcinoma of the
lung: its development and malignant progression. Lung Cancer
1993; 9: 99-108
22. Kushihashi T, Munechika H, Ri K, et al. Bronchioloalveolar ad
enoma of the lung: CT-pathologic correlation . Radiology 1994;
193: 789-793
23. Kim Y, Lee KS, Choi D-C, Primack SL, 1m J -G. The spectrum of
eosinophilic lung disease ‘ radiologic find ings. J Comput Assist
Tomogr 1997 ; 21 ‘ 920-930
대한밤사선의학회지 1998; 39 : 693- 698
단일폐결절성 세기관지폐포암 : 고해상전산화단충촬영상의 조직학적 예단1
1 성균관대학교 의과대학 방사선과학교실 2이화대학교 의과대학 방사선과학교실 3성균관대학교 의과대학 예방의학교실 4연세대학교 의과대학 방사선과학교실
장현정 · 이경수 · 검유경 2 • 신명희3 • 주인욱 · 김승훈 · 이원재 · 변홍식 · 김상진4
목 적 : 단일폐결절성 세기관지 폐포암에서 조직학적으로 진단을 예측할 수 있는 특징적인 고해성 전산화단
층촬영 (HRCT) 소견을기술하고자하였다.
대상 및 방법 : 단순흉부촬영상 단일폐결절을 가진 46명의 환자를 무작위로 배열하여 HRCT 소견을 후향적으 로분석하였다.31명은 악성, 15명은 양성 결절을가지고 있었다. 병리진단을모른 채 두명의 방사선과의사가합
의로 폐결절의 경계 빛 내부 소견을 분석하였으며 세기관지 폐포암의 특정적 소견을 알기 위해 다단계 식별분석
을시도하였다.
결 과 · 기관지 폐포암(n=15)의 가장 흔한 소견은 내부 기포형 저음영(14/15, 93%) (P=O.OOl), 간유리형
병변(12/15, 80%, 종괴의 58% 용척) (P=O.OOl), 늑막꼬리(12/ 15, 80%) (P=0.097) 및 엽성 및 침상 경계 (8/15, 53%) 였다. 간유리형 병변 (P=O.OO1)과 내부 기포형 저음영 (P= 0.0187)은 세기관지 폐포암의 진단에 있
어 가장 식별 능력이 있는소견이었다.
결 론 : 내부에 기포형 저음영을 가진 간유리형 병변을 포함하는 원위부 폐결절은 세기관지 폐포암의 특징적
소견이다. 그러므로 HRCT 소견을 세멸하게 분석하면 단일폐결절성 세기관지 폐포암을 특이적으로 진단할 수 있다.
- 698 -