Embed Size (px)
Citation preview

British Journal ofOphthalmology, 1982, 66, 450-454
Solitary extramedullary plasmacytoma of thepalpebral conjunctivaJOHANNA M. SEDDON,' JOEL M. CORWIN,' JOHN J. WEITER,2JANE U. BRISBANE,3 AND FRANCIS C. SUTULA'
From the 'Department ofOphthalmology, Tufts-New England Medical Center, 2Eye Research Institute ofRetinaFoundation, and 3Departnent of Pathology, Boston VA Medical Center, Boston, Massachusetts, USA
SUMMARY A 63-year-old man had a solitary extramedullary plasmacytoma of the conjunctiva forseveral years with no history of ocular inflammation or systemic abnormalities. Immunoperoxidasestaining was consistent with a neoplastic lesion. This is the only well documented such case in therecent literature to the best of our knowledge. This rare condition is contrasted with reactive plasmacell granuloma, a benign inflammatory condition, which comprises most of the cases previouslyreported as plasmacytomas. Since extraskeletal plasmacytomas may be the first manifestation ofmultiple myeloma, these patients deserve appropriate diagnostic evaluation and close follow-up.
Plasma cell tumours of the conjunctiva are uncom-mon. When first described in the early twentiethcentury they were referred to as plasmacytomas orplasmomas.`8 By today's criteria, however, most ofthese tumours would not be considered true plasma-cytomas (rare neoplastic growths consisting of plasmacells) but benign reactive plasma cell granulomassecondary to inflammation.9"' True plasmacytomasare rare; they occur most frequently in the upperrespiratory tract. " An extramedullary plasmacytomacan occur as an isolated lesion or as a manifestation ofsystemic multiple myeloma. To the best of our know-ledge this is the only well documented case of solitaryextramedullary plasmacytoma of the conjunctiva inthe recent literature.
Case report
A 63-year-old man was first seen by us in September1978. He had had adult-onset diabetes mellitus for 16years and was referred by the medical clinic for anocular examination. He mentioned that he had had apainless 'growth' on his right lower lid for severalyears and that it had increased only slightly in size. Hehad also noted decreasing visual acuity in the right eyefor a few years. There was no complaint of ocular
Correspondence to John J. Weiter, MD, Eye Research Institute, 20Staniford Street, Boston, MA 02114, USA.
Dr. Seddon is currently at the Massachusetts Eye and EarInfirmary, Boston, Mass.
pain, tenderness, or discharge and no history ofocularinflammation or trauma.On ophthalmological examination his visual acuity
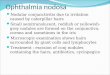
was 6/60 (20/200) in the right eye and 6/24 (20/80) inthe left. The middle of the right lower lid was notablyswollen. When the lid was everted, a discrete reddish-tan mass measuring 16 mm in largest diameter and 8mm in height was noted on the palpebral conjunctiva.It was firm, not tender, and adherent to lid tissuealong the full length of its base (Fig. 1).
Neither eye showed a papillary or follicular con-junctival reaction. The right upper lid and both leftlids appeared normal. There was no bulbar conjuncti-val injection or discharge, comeal staining, or anteriorsegment inflammation in either eye. Rubeosis waspresent in the left eye. Intraocular pressure was 12mmHg in both eyes. Ophthalmoscopic examinationdisclosed disc neovascularisation, haemorrhages, andexudates in the posterior pole of both eyes.
After the nature and implications of the patient'sproblems were explained to him we advised excisionof the tumour in the right eye and panretinal photo-coagulation for the proliferative retinopathy in botheyes. However, the patient refused any treatment.Then on 16 May 1980 he had a sudden loss of vision inthe left eye to 6/75 (20/300). Gonioscopic examinationdisclosed that rubeosis in the left eye had becomemore marked and neovasculansation of the angle atthe 9-o'clock position was present in both eyes. Avitreous haemorrhage obscured the view ofthe fundus
450
on March 2, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.66.7.450 on 1 July 1982. D
ownloaded from

Solitary extramedullary plasmacytoma ofthe palpebral conjunctiva
Fig. 1 Discrete tumour with mottled discolorationinvolving the palpebral conjunctiva ofthe right lower lid.
in the left eye. The lid tumour appeared unchanged,with no evidence of growth. Because of his failingvision the patient then agreed to enter hospital forophthalmic treatment.General physical findings included small ulcers over
the pretibial areas bilaterally, absent peripheralpulses, grade 2/6 systolic ejection murmur, andperipheral and ulnar neuropathy. There was nolymphadenopathy. Laboratory tests gave moderatelyraised fasting blood glucose levels which ranged from140 to 170 mg/100 ml (7-8-9-4 mmol/l). The re-mainder of his laboratory values were normal; theseincluded white blood cell count of 8x 109/l with aXi
¢
*F a~ , *
* * .. *M
normal differential count, a haemoglobin of 14-2 g/dl,haematocrit of 40 0%, normal electrolytes,prothrombin time, partial thromboplastin time,chemistry profile, blood urea nitrogen, creatine, andurine analysis. Total protein measured 7-3 g/100 ml(73 g/l) with an albumin of 4-3 g/100 ml (43 g/l). Chestroentgenograms revealed diffuse interstitial markingsconsistent with early congestive heart failure, whichon follow-up roentgenograms had resolved. Electro-cardiogram showed normal sinus rhythm and a leftbundle branch block.On 22 May 1980 the patient underwent an ex-
cisional biopsy of the lesion of the right lower lid. Themost likely diagnosis at this time was a granulomatousnodule, such as a reaction to a foreign body. A scleralgraft was placed at the base of the wound. Because ofpersistent corneal staining the graft was later removedand a conjunctival flap was advanced over the base ofthe wound.The tumour was a well circumscribed, oval, pale
tan, fleshy mass measuring 15 x 16x8 mm. Histologi-cally it consisted of sheets of relatively mature plasmacells with characteristic eccentric nuclei and abundantcytoplasm often containing a paranuclear clear space(Golgi space) (Fig. 2). No other cells, such as lympho-cytes, histiocytes, or any other type, were present. AWright-stained touch imprint accentuated thespokewheel configuration of the nuclear chromatin(Fig. 2). Congo red stain for amyloid was negative.Immunoperoxidase staining showed that the plasmacells within the tumour contained cytoplasmic IgMand IgG and lambda light chain only. Electron micro-scopic examination further confirmed the plasmacyticnature of the neoplastic cells, whose cytoplasm con-
Fig. 2 Left: Plasmacytoma tissuesection showing uniform pattern ofplasma cells with characteristiceccentric nuclei. (Haematoxylinand eosin, x 475). Right: Touchimprint accentuating spokewheelconfiguration ofnuclearchromatin.(Wright stain, x 1333).*
.4
451
IRW"
adbibil
p
on March 2, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.66.7.450 on 1 July 1982. D
ownloaded from

Johanna M. Seddon, Joel M. Corwin, John J. Weiter, Jane U. Brisbane, and Francis C. Sutula
tained many parallel strands of rough endoplasmicreticulum (Fig. 3).A systemic examination showed no evidence of
multiple myeloma. Bone marrow biopsy revealednormocellular bone marrow with no evidence ofplasmacytosis. Serum protein electrophoresis waswithin normal limits, as were the immunoglobinmeasurements: IgG 1060 mg/100 ml (10-6 g/l)(normal, 700-1500 (7-15 g/l)), IgA 348 mg/100 ml(3 5 g/l) (normal, 55-350 (0 5-3 5 g/l)), IgM 257mg/100 ml (2-6 g/l) (normal, 50-265 (0-5-2-7 g/l)).Urine was negative for Bence Jones protein. A bonescan revealed a lesion in the vertex of the skull withmore diffuse uptake in the right frontal area. This wasconsistent with trauma to that area which the patienthad sustained several years earlier. Skull roentgeno-grams, long bone survey, and thoracic and lumbarspine roentgenograms showed no evidence of a lyticlesion. The palpebral conjunctival lesion was there-fore classified as an isolated extramedullaryplasmacytoma.During the hospital course the right lower lid healed
without complications. The vitreous haemorrhage inthe left eye cleared partially and visual acuity im-proved to 6/15 (20/50). In March 1981 the patient hada sudden loss of vision in the left eye to hand move-ments. Examination revealed in the left eye arhegmatogenous retinal detachment with traction; itwas repaired by closed vitrectomy and scleralbuckling. He is also being followed up in the haema-tology clinic for evaluation of potential systemicdisorders related to the plasmacytoma. In March 1981his haemoglobin, haematocrit, and serum proteinswere within normal limits.
Fig. 3 Electron micrograph showing abundant roughendoplasmic reticulum ofneoplastic plasma cells. (x2800).
Discussion
Classification of plasma cell disorders is complex.Azar9 has proposed that plasma cell neoplasms bedivided into the following categories: multiple plasmacell myeloma, disseminated nonosteolytic myeloma-tosis, solitary myeloma, plasma cell leukaemia,lymphoplasmacytic lymphomas, malignant lymph-omas with M components, and extraskeletal plasma-cytoma. These should be differentiated from benignconditions such as reactive plasmacytoses and plasmacell granulomas. Benign monoclonal and polyclonalgammopathies without evidence of systemic diseasecan also be included."2 It is important to distinguishamong these categories, as the causes, prognoses,and treatments differ. Particularly when confrontedwith a plasma cell tumour of the conjunctiva adistinction among 3 entities should be made:(1) manifestation of systemic multiple myeloma, (2)solitary extramedullary (or extraskeletal) plasma-cytoma, and (3) plasma cell granuloma.
Multiple myeloma is a systemic disease associatedwith plasma cell infiltration of bone marrow andusually osteolytic lesions as well as the presence of amonoclonal immunoglobin in serum and/or urine.These patients commonly have anaemia and bonepain, and there may be associated extraskeletalspread of myeloma.
Solitary extramedullary plasmacytomas arise with-out evidence of solitary myeloma of bone or multiplemyeloma. The bone marrow, urine, serum electro-phoresis, and haemoglobin are normal at diagnosis ofthe localised tumour. Abnormal findings with spreadof tumour to soft tissue or bone may develop later, atwhich point the tumour is no longer an independentsolitary lesion.9 13-iS Histologically the tumour con-sists of sheets ofmature plasma cells which may invadesurrounding tissue.A reactive plasma cell granuloma, a benign lesion,
is not associated with concurrent or subsequentsystemic findings (serum protein abnormalities orbone changes). It is induced by an inciting foreignantigen having produced previous inflammation andis adequately treated by excision. Histologically it iscomposed not only of mature plasma cells but also ofhistiocytes, lymphocytes, eosinophils, fibroblasts, andcapillary endothelial hyperplasia. The term'granuloma' has also been used for reactive lesionseven in the absence of histiocytes.Plasma cell tumours of the conjunctiva were
reported occasionally in the early twentieth centuryas 'plasmomas' or 'plasmacytomas.' These cases,however, were documented with inadequate clinicaland laboratory evaluations. Most authors believedchronic inflammation to be the cause.18 In fact mostcases occurred in patients with trachoma, and all
452
on March 2, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.66.7.450 on 1 July 1982. D
ownloaded from

Solitary extramedullary plasmacytoma ofthe palpebral conjunctiva
occurred in endemic trachoma regions. In 1915Verhoeff and Derby reviewed the literature onplasmacytoma and concluded that 'the evidence athand points to an inflammatory origin for thiscondition. The clinical fact that it has occurredfrequently in conjunctiva showing evidence ofexistingor previous trachoma points in this direction.'7 Mostlater reports of conjunctival 'plasmacytomas' alsosuggest inflammation as the cause. " Most of theselesions would be classified today as plasma cellgranulomas. For this reason Dolin and Dewar did notinclude cases involving the conjunctiva in their reviewof extramedullary plasmacytomas.20One well documented case involving the conjunc-
tiva resembles a true plasma cell neoplasm thatoccurred with an orbital mass as a terminal event in apatient with known multiple myeloma.2' Jampol andassociates described a lymphoplasmacytic tumour ofthe conjunctiva associated with systemic lymphomaand a monoclonal IgA gammopathy.22 Plasma cellinfiltration appearing as diffuse thickening of the con-junctiva or conjunctivitis rather than a discrete masshas also been noted.23 24 In one of these cases a mixedcellular infiltrate was associated with cytoplasmiccrystals consisting of IgG.23 The other case, accord-ing to the authors,24 probably represented a reactivechronic inflammatory response rather than neoplasia.
In contrast the patient described here had a fairlywell circumscribed mass with no history of ocular in-flammation or medical illness. Histopathologicalexamination revealed a lesion consisting ofonly sheetsof mature plasma cells without a mixed cellularpopulation and no fibrovascular proliferation. Thefinding of only lambda light chain on immunoperoxi-dase staining supported the diagnosis of neoplasia.The presence of more than one heavy chain, as in ourcase, has been reported in rare cases of myeloma.25Clinical, haematological, biochemical, and radiolo-gical investigations ruled out systemic disease. Thislesion therefore meets the diagnostic criteria for atrue solitary extramedullary plasmacytoma of theconjunctiva. Long-term stability of both symptomsand myeloma protein production may occur inpatients with indolent myeloma and in those withlocalised plasmacytoma.26 The long history of the lidlesion which remained localised in our case is there-fore not inconsistent with the diagnosis ofplasmacytoma.
Solitary extramedullary plasmacytoma of the orbit,as of the conjunctiva, occurs rarely.27 Somewhat morecommon are plasma cell pseudotumours28 and orbitalplasma cell tumours which represent an extraskeletalmanifestation of multiple myeloma.28-30 In the lattercategory in 23 of the 30 patients studied by Rodmanand Font proptosis was the initial manifestation of thedisease .28
The diagnosis of plasmacytoma rather than plasmacell granuloma is liberally applied to a number ofplasmacytic growths at other sites. 80% of thereported 'extramedullary plasmacytomas' develop inthe oral cavity or respiratory tract.3' Some of these,however, may be benign inflammatory processes eventhough they appear as a discrete mass.9 Following infrequency are plasmacytomas involving the gastro-intestinal tract and lymph nodes.'532 Skin and softtissue are more rarely involved.33Not only do the causes differ but prognosis and
treatment of plasma cell disorders also vary. Unlikereactive plasma cell granuloma, extramedullaryplasmacytoma is considered to be of low-grademalignancy, and the clinical course after excision isnot entirely benign. Studies of nonocular cases haveshown that multiple myeloma may develop afterseveral months or even years in up to 30% ofcases.3435 Involvement of lymph nodes and develop-ment of new foci of tumour cells in soft tissue andbone can occur. ' 34Treatment for both plasmacytomaand plasma cell granuloma consists of excision, butradiotherapy is recommended in addition for theneoplastic growth.36 Although no such cases havebeen reported, it is conceivable that patients withextraskeletal plasmacytoma of the conjunctiva mayalso subsequently develop systemic manifestations ofmultiple myeloma. Therefore periodic systemicevaluation is warranted. We decided to follow up ourpatient closely after complete excision of the tumourrather than to treat him with radiotherapy.We thank Ingrid von Saltza for help with translations.
References
I Pascheff C. Plasmacellulare Bildungen (Plasmomen) derBindehaut und der Hornhaut. Albrecht von Graefes Arch KlinOphthalmol 1908; 68:114-25.
2 Pascheff C. Weitere Mitteilungen iiber die plasmacellularenBildungen der Bindehaut-conjunctivitis plasmacellularis.Albrecht von Graefes Arch Klin Ophthalmol 1909; 71: 569-72.
3 Baurmann M. Uber das Plasmom der Conjunctiva und seineBeziehung zum Amyloid. Albrecht von Graefes Arch KlinOphthalmol 1922; 109: 236-51.
4 Kreibig W. Uber die Plasmocytome der Bindehaut. Albrecht vonGraefes Arch Klin Ophthalmol 1933; 131: 89-1(01.
5 Rados A. Uber Plasmome der Bindehaut. Z Augenheilkd 1913;29: 125-34.
6 Hoffman W. Ein Beitrag zur Plasmomfrage. Z Augenheilkd 1925;55: 164-80.
7 Verhoeff FH. Derby GS. Plasmoma of the lacrimal sac. ArchOphthalmol 1915; 44: 252-64.
8 Hellwig CA. Extramedullarv plasma cell tumors as observed invarious locations. Arch Pathol 1943; 36: 95-111.
9 Azar HA. Pathology of multiple myeloma and related growths.In: Azar HA. Potter M. eds. Multiple Msyeloma and RelatedDisorders. New York: Harper and Row. 1973; 1: 2-26.
I() Bahadori M. Liebow AA. Plasma cell granulomas of the lung.Cancer 1973; 31: 191-208.
11 Fu YS. Perzin KH. Nonepithelial tumors of the nasal cavity.paranasal sinuses and nasopharynx. A clinicopathologic study.IX. Plasmacytomas. Cancer 1978; 42: 2399-406.
453
on March 2, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.66.7.450 on 1 July 1982. D
ownloaded from

Johanna M. Seddon, Joel M. Corwin, John J. Weiter, Jane U. Brisbane, and Francis C. Sutula
12 Kyle RA. Monoclonal gammopathy ofundetermined significance.Natural history in 241 cases. Am J Med 1978; 64: 814-26.
13 Wiltshaw E. The natural history of extramedullary plasmacytomaand its relation to solitary myeloma of bone and myelomatosis.Medicine 1976; 55: 217-38.
14 Conklin R, Alexanian R. Clinical classification of plasma cellmyeloma. Arch Intern Med 1975; 135: 139-43.
15 Nelson MG, Lyons AR. Plasmacytoma of lymph glands. Cancer1957; 10:1275-80.
16 Mathur SP. Conjunctival plasmoma. Br J Ophthalmol 1959; 43:499-500.
17 Abboud I. Plasmoma of the bulbar conjunctiva. Bull OphthalmolSoc Egypt 1962; 55: 29-32.
18 Dayal Y, Agarwal PK, Agarwal LP. Plasmocytoma of the pal-pebral conjunctiva. Orient Arch Ophthalmol 1964; 2: 40-1.
19 Bhargava S, Gupta MC, Vyas K, Saxena BP. Solitary plasmo-cytoma of conjunctiva. J All-India Ophthalmol Soc 1967; 15:38-9.
20 Dolin S, Dewar JP. Extramedullary plasmacytoma. Am J Pathol1956; 32: 83-103.
21 Benjamin 1, Taylor H, Spindler J. Orbital and conjunctivalinvolvement in multiple myeloma. Report of a case. Am J ClinPathol 1975; 63: 811-7.
22 Jampol LM, Marsh JC, Albert DM, Zimmerman LE. IgAassociated lymphoplasmacytic tumor involving the conjunctiva,eyelid and orbit. Am J Ophthalmol 1975; 79: 279-84.
23 Rao NA, Font RL. Plasmacytic conjunctivitis with crystallineinclusions. Arch Ophthalmol 1980; 98:836-41.
24 Yee RD, Savage DD, Cogan DG, Nienhuis AW, Minna JD.Plasma cell infiltration of the conjunctiva associated with pan-
cytopenia, dermatitis, and polyclonal gammopathy. Am JOphthalmol 1976; 82: 486-91.
25 Taylor CR, Russell R, Chandor S. An immunohistologic study ofmultiple myeloma and related conditions, using an immuno-peroxidase method. Am J Clin Pathol 1978; 70: 612-22.
26 Alexanian R. Plasma cell neoplasms. CA 1976; 26: 38-49.27 Cogan JF. Extramedullary plasmocytoma of the orbit. Br J
Ophthalmol 1956; 40: 681-5.28 Rodman HI, Font RL. Orbital involvement in multiple myeloma.
Arch Ophthalmol 1972; 87: 30-5.29 Mewis-Levin L, Garcia CA, Olson JD. Plasma cell myeloma of
the orbit. Ann Ophthalmol 1981; 13: 477-81.30 Clarke E. Plasma cell myeloma of the orbit. Br J Ophthalmol
1953; 37: 543-54.31 Pahor AL. Extramedullary plasmacytoma of the head and neck,
parotid and submandibular salivary glands. J Larvngol Otol 1977;91: 241-58.
32 Remigio PA, Klaum A. Extramedullary plasmacytoma ofstomach. Cancer 1971; 27: 562-8.
33 Canlas MS, Dillon ML, Loughrin JJ. Primary cutaneous plasma-cytoma. Report of a case and review of the literature. ArchDermatol 1979; 115: 722-4.
34 Corwin J, Lindberg RD. Solitary plasmacytoma of bone vs.
extramedullary plasmacytoma and their relationship to multiplemyeloma. Cancer 1979; 43: 1007-13.
35 Todd ID. Treatment of solitary plasmacytoma. Clin Radiol 1965;16: 395-9.
36 Woodruff RK, Whittle JM, Malpas JS. Solitary plasmacytoma. I.
Extramedullary soft tissue plasmacytoma. Cancer 1979; 43:2340-3.
454
on March 2, 2020 by guest. P
rotected by copyright.http://bjo.bm
j.com/
Br J O
phthalmol: first published as 10.1136/bjo.66.7.450 on 1 July 1982. D
ownloaded from
![Palpebral Involvement as a Presenting and Sole ...downloads.hindawi.com/journals/tswj/2010/672487.pdfdermatomyositis[9], granuloma annulare[10], and granuloma faciale[11]. Palpebral](https://img.pdfslide.us/doc/110x75/5e5d2f5139526a648b02a0fa/palpebral-involvement-as-a-presenting-and-sole-dermatomyositis9-granuloma.jpg)




![National Library of Serbia...feronasa] bulbar conjunctiva [61 According to some references, pans of conjunctiva higher goblet cell density are Inferonasal bulbar conjunctiva, tarsal](https://img.pdfslide.us/doc/110x75/6084bbb33561423ad20313c4/national-library-of-feronasa-bulbar-conjunctiva-61-according-to-some-references.jpg)