Embed Size (px)
Citation preview

oft tissue surgical techniques that can beperformed in birds have increased substan-tially over the last decade because of thewidespread use of isoflurane anesthesia, the
introduction of microsurgical techniques to the avianpractice, improvement in microsurgical instrumen-tation, improvements in bipolar radiosurgical instru-mentation and the growing expertise of avian sur-geons. Board certified surgeons are becomingattracted to the field for the purpose of developingand refining avian procedures. Procedures that wereonce considered impossible are now performed on aroutine basis.
The most substantial limitation to soft tissue surgeryof the abdomen is the small size (<100 grams) ofmany avian patients. Some of these problems can beovercome with the use of magnification, but othersare a result of having limited surgical access to anarea, and are difficult to overcome. Surgery of thethoracic area, even in large companion birds, pre-sents a similar problem, in that the organs of interestare covered by the sternum and heavy musculature.Continued improvements in the endoscopic surgicalequipment available in human medicine will un-doubtedly improve the surgeon’s ability to performsurgery in difficult-to-reach areas of the avian body.
The avian surgeon should practice surgical tech-niques on cadavers prior to performing the proce-dures on clinical patients. The delicate avian tissuestear in the presence of slight autolysis; therefore, theuse of fresh specimens will give the surgeon an ap-preciation of avian tissue characteristics and allowthe surgeon to explore the capabilities of surgicalinstrumentation.
When necropsies are necessary, the clinician shouldapproach this procedure from the perspective of asurgeon rather than of a pathologist, by dissectingand reviewing anatomy from a regional approachrather than by performing the necropsy strictly fromthe traditional ventrodorsal approach.
SC H A P T E R
41SOFT TISSUE
SURGERY
R. Avery BennettGreg J. Harrison
Surgery of the Skin
The skin and subcutaneous tissues of birds differfrom those of mammals. Birds have relatively thin,dry epidermis, and the dermis is attached to theunderlying muscle fascia with little subcutaneoustissue.19,33 In feathered areas, the skin is generallyonly ten cells thick. Compared to mammals, the skinis only loosely attached to underlying structures,except in the distal extremities where it is firmlyadherent to underlying bone.
Passerine Leg Scales
Passerine leg scale syndrome is characterized by thedevelopment of abnormally large scales of the legsand feet, possibly as a result of mite infection ormalnutrition (see Chapter 43). These scales can coa-lesce and act as a constricting band. They also pre-dispose the bird to bacterial pododermatitis (usuallyStaphylococcus spp). If present, the shiny, convexcarapace of the female Knemidocoptes mite can usu-ally be visualized, with the aid of the operating mi-croscope, inside the burrows they create. In mostinstances, lesions resolve after treatment with iver-mectin or correction of nutritional deficiencies. Insevere cases, it may be necessary to surgically de-bride the proliferative scales to prevent vascularcompromise. A 22 or 25 ga needle with the point bentto a 90° angle can be used to lift the scales and scabs,which can then be grasped with the micro-forceps.Skin softeners may also be beneficial.
Toe Necrosis (Constricted Toe Syndrome)
Avascular necrosis of digits may occur secondary tocircumferential constriction caused by fibers, scabsor necrotic tissue (see Color 24). These constrictionscause edema and if untreated, sloughing of the digitdistal to the constriction.4 This condition is generallynot life-threatening, and amputation should be con-sidered only after less aggressive therapies havefailed. Removal of the offending tissue or fibers andsupportive care are frequently successful. Avascularnecrosis of the digits has been described in passerinebirds and Amazon parrots. Scabs should be debridedor incised to prevent vascular compromise, and hy-droactive dressings should be applied to the affected
digits to prevent the formation of additional scabs.Complete healing may require weeks to months.
In small birds (eg, Passeriformes), constricting fibersmay be visualized using the operating microscope(see Figure 43.4). A bent 25 ga needle is helpful forremoving constricting fibers. The tip can be used toelevate the fiber, which can then be cut by gentlyrolling the needle such that the beveled edge seversthe fiber. Microsurgical forceps may be used to un-tangle the fibers. Even severely swollen digits withexposed tendons may heal without incident once thefibers are removed. A hydroactive dressing should beplaced on any wounds created by the fibers to preventdesiccation and the formation of a constricting scab.
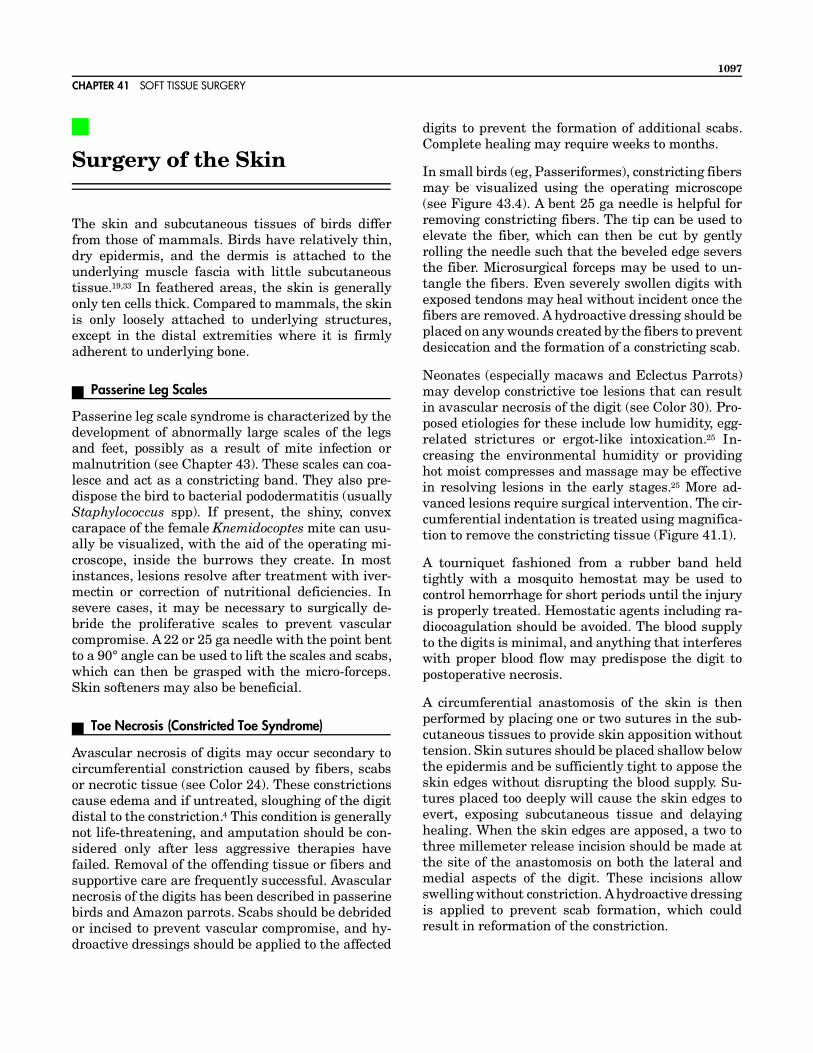
Neonates (especially macaws and Eclectus Parrots)may develop constrictive toe lesions that can resultin avascular necrosis of the digit (see Color 30). Pro-posed etiologies for these include low humidity, egg-related strictures or ergot-like intoxication.25 In-creasing the environmental humidity or providinghot moist compresses and massage may be effectivein resolving lesions in the early stages.25 More ad-vanced lesions require surgical intervention. The cir-cumferential indentation is treated using magnifica-tion to remove the constricting tissue (Figure 41.1).
A tourniquet fashioned from a rubber band heldtightly with a mosquito hemostat may be used tocontrol hemorrhage for short periods until the injuryis properly treated. Hemostatic agents including ra-diocoagulation should be avoided. The blood supplyto the digits is minimal, and anything that interfereswith proper blood flow may predispose the digit topostoperative necrosis.
A circumferential anastomosis of the skin is thenperformed by placing one or two sutures in the sub-cutaneous tissues to provide skin apposition withouttension. Skin sutures should be placed shallow belowthe epidermis and be sufficiently tight to appose theskin edges without disrupting the blood supply. Su-tures placed too deeply will cause the skin edges toevert, exposing subcutaneous tissue and delayinghealing. When the skin edges are apposed, a two tothree millemeter release incision should be made atthe site of the anastomosis on both the lateral andmedial aspects of the digit. These incisions allowswelling without constriction. A hydroactive dressingis applied to prevent scab formation, which couldresult in reformation of the constriction.
CHAPTER 41 SOFT TISSUE SURGERY
1097
Feather Cysts
Feather cysts are generally the result of trauma tothe feather shaft, feather follicle or, as in the case of“soft-feathered” canaries, the result of abnormallydeveloped feathers (see Color 24).
Feather cysts may occur within any feather follicle,but those on the wing and tail are the most challeng-ing to the surgeon. In canaries, feather cysts are mostcommon in Norwich, Gloucester and their cross-breeds. These birds have been genetically selected toproduce an extra downy type of feather (soft feather-ing) that may predispose them to this syndrome (seeColor 24).3 In other birds, malformed and cysticfeather development have been associated withtrauma, malnutrition and viral, bacterial or parasiticinfections. If damage is sustained to one side of the
follicle, feather growth becomes asymmetrical andthe feather may grow in a curled fashion inside thefollicle, resulting in a feather cyst.
Feather cysts on the wing that are treated by lancingand curettage frequently recur. Fulguration with aradiosurgical unit has been reported to be successfulin some cases; however, the depth of destruction isdifficult to control, resulting in damage to adjacentfollicles. These damaged follicles can then developfeather cysts. Use of laser for follicle excision does notappear to improve the long-term clinical results.
Blade excision appears to be the treatment of choice.A tourniquet can be applied to aid in hemostasis. Theentire follicle, including any bony attachments,should be excised. Adjacent follicles and their bloodsupply should be carefully avoided. In the postop-
FIG 41.1 a) Constriction of the digits (arrows) is common in some macaw and Eclectus Parrot neonates. b) The lesion is repaired by usingan operating microscope to remove the circumferential scab and create a fresh tissue margin. c) The wound edges are then apposed withshallowly placed sutures, and longitudinal incisions are made through the constriction on the medial and lateral sides of the digit tocompensate for swelling and growth. d) The wound is covered with a hydroactive dressing to keep it clean and prevent dehydration.
SECTION SIX SURGERY
1098

erative period, the wing should be bandaged to preventmovement at the site of follicle excision while healingoccurs by second intention. As adjacent feathers beginto regrow, debris should be gently removed by flushingwith warm sterile saline several times daily.
With a single cyst or a large feather, the follicle maybe saved by marsupializing the lining of the cyst withthe skin surrounding the follicle. An incision is madecentered on the cyst, parallel to the direction offeather growth. Hemorrhage is controlled with 6-0ligatures, not with radiocautery. The lining of thecyst is cultured and the debris is removed. Redun-dant tissue is excised and the follicle is thoroughlylavaged with sterile saline. The margin of the cyst isthen sutured to the skin using a simple continuouspattern of fine suture. New feather growth must beclosely monitored.
Feather cysts of the tail may be severe and disfigur-ing, requiring amputation of the pygostyle. Bluntdissection to the coccygeal vertebrae allows disar-ticulation at the sacrococcygeal junction without en-tering the cloaca. Soft tissues are closed routinely.
Feather cysts on the body are easily removed usingelliptical or fusiform excision followed by primaryskin closure.3 Treatment of individual feathers isgenerally unrewarding in cases where an entirefeather tract is involved. A technique for radical exci-sion of an entire pteryla of affected feathers in canar-ies has been described.3 A fusiform incision is madefrom the flank to the thoracic inlet around the af-fected pteryla. The main vascular supply to the tractis located centrally at the cranial third of the pteryla.Large cysts may be supplied by relatively large indi-vidual vessels that should be coagulated or ligated.Despite the significant-sized defect, skin appositionis easily accomplished using a monofilament suturein a simple continuous pattern (braided materialmay damage the skin). Removal of one or more ptery-lae from the body wall does not seriously affect thecosmetic appearance of the bird.
Xanthomas of the Wing Tip
Xanthomatosis is characterized by the deposition ofa rubber-like proteinaceous material within the skinand is frequently associated with inflammation ofunderlying tissues (see Color 25). Xanthomas at thewing tip may cause the wing to droop, resulting intrauma to the mass. Probucola (25 mg/day for anAmazon parrot) and dietary management should beused in combination with surgical excision of themass. Medical management is ineffective alone butmay help prevent recurrence. Serum cholesterol lev-els should be closely monitored because they areusually elevated in birds with xanthomatosis andshould be medically reduced to a normal level priorto surgery. The diet should be low in protein (13%)and fat (5.5%).
A monopolar, wire electrode functions well for re-moval of xanthomatous masses. The wound is left toheal by second intention. The wound may be pro-tected with tissue adhesive or a hydroactive dress-ing, which should be changed every three to fivedays. Complete healing often requires several weeks.If subcutaneous tissues are involved (especiallybone), the affected wing may require amputation.
Excision of the Uropygial Gland
Impaction of the uropygial gland may respond tomedical management using hot, moist compressesand gentle expression of the contents. In some cases,the gland may rupture, causing inflammation andscar tissue formation in the surrounding tissues.Chronic debilitation and death may follow.31 Excisionof the gland should be considered in cases whereimpaction recurs, the gland has ruptured, a tumor ispresent or chronic infection of the gland is not re-sponsive to medical management.
A fusiform incision is made along the dorsal midlineto incorporate the papillae of the gland. The skin isreflected with the aid of blunt dissection and radioco-agulation of damaged vessels. The gland is bilobed,and each lobe receives its blood supply from a vesselthat branches at the cranial, middle and caudal por-tions of the gland. The gland may extend deeply tothe synsacrum and caudally to the insertion point ofthe tail feathers. The vessels are identified and co-agulated or ligated. Bipolar coagulation should beused to minimize damage to the follicles of the rec-trices. Dissection is continued, beginning at the cra-nial extent of the gland proceeding circumferentiallyuntil its removal is possible. The deep fascia is closed
CL INICAL APPL ICAT IONSFeather cysts are particularly common in line-breed canaries.
Feather cysts may occur secondary to any factor that dam-ages the follicular epithelium.
For feather cysts on the wing, blade excision appears to bethe treatment of choice.
Feather cysts of the tail may require amputation of thepygostyle.
Feather cysts on the body are removed using elliptical orfusiform excision followed by primary skin closure.
CHAPTER 41 SOFT TISSUE SURGERY
1099
with monofilament absorbable material in a continu-ous or interrupted pattern, depending upon theamount of tension present. Subcutaneous and skinclosures are routine.
Extensive dissection and debridement are necessary ifthe gland has ruptured. An additional caudal incisionperpendicular to the dorsal midline incision may benecessary.31 In these cases, extensive tissue traumaincreases the likelihood of postoperative dehiscenceand damage to the follicles of the rectrices.31 Dehis-cence usually occurs at the junction of the two perpen-dicular incisions. If possible, it is preferable to removea diseased uropygial gland prior to its rupture.
Surgery of the Eye
Lateral Canthoplasty for Inferior Ectropion
Idiopathic paralysis of the inferior eyelid occurs withsome degree of frequency in cockatiels and occasion-ally in Umbrella Cockatoos (see Color 26). Clinicalsigns generally include exposure keratitis with sec-ondary epiphora and corneal ulceration. Sympto-matic treatment involves the use of ophthalmic oint-ment to lubricate and protect the cornea. A lateralcanthoplasty will create a smaller aperture, reducingthe risk of exposure keratitis and associated condi-tions (Figure 41.2). Postoperatively the eye is medi-cated with an antibiotic ophthalmic ointment TID toQID, and the eye is cleaned as needed with an appro-priate eye wash solution.
Conjunctival Masses
Masses involving the palpebral conjunctiva occurwith some frequency in cockatiels. These may be theresult of tissue edema, cyst formation or discretemasses. They are usually easy to remove with radio-surgical bipolar forceps. These masses may be secon-dary to chlamydiosis, mycoplasmosis, eyelid paralysisor oropharyngeal abscessation from hypovitaminosisA (see Chapters 22, 26).
Indolent Corneal Ulcers
Successful treatment of indolent corneal ulcers inbirds appears to require debridement of the entiresuperficial layer of the cornea. Under the operating
microscope, a cotton-tipped applicator moistenedwith 10% acetylcysteineb is used to gently debride theedge of the ulcer toward the limbus. Once the affectedepithelium has been debrided, it should be excisedusing a #11 scalpel blade or a corneal knife. Standardulcer treatment is instituted postoperatively. Thecorneal surface will re-epithelialize from the limbus.
Lens Removal
Trauma (blunt or penetrating) and senile lenticulardegeneration have been speculated as causes for cata-ract formation in birds.7,27 In canaries, cataracts areinherited, and surgical removal has been recom-mended.50 The avian eye is large, conforms closely tothe orbit and has limited mobility.52 Scleral ossicles helpsupport the eye and prevent collapse during surgery.
In a study of older macaws, immature cataracts werepresent in at least one eye of most birds over the ageof 35.7 In many cases, the cataracts remained imma-ture for several years without completely obstructingvision. The change from an incomplete, immaturecataract progressed rapidly to a complete, maturecataract seemingly skipping a complete, immaturestage. Those birds with rapidly developing cataractsfrequently became blind due to phacolytic uveitis.Lens removal was performed on 13 eyes in 8 birdsbecause of visual impairment or uveitis.7
For lens removal in these macaws, no attempt wasmade to dilate the pupil preoperatively. The macawcornea is approximately seven millimeters in diame-ter, which is too small for phacoemulsification instru-mentation, and the cataracts were removed usingstandard surgical technique (Figure 41.3). In theimmediate postoperative period, the eyes weretreated with a topical steroid-antibiotic ointment,cfollowed by weekly subconjunctival injections oftriamcinoloned for up to a total treatment period offour weeks. Hemorrhage, synechiae of the iris andsloughing of the corneal epithelium were reportedcomplications; however, postoperative inflammationwas minimal in most cases.
Ten of the 13 eyes were visual after surgery. One birdhad bilateral posterior synechiae and pigment mi-gration that obstructed vision. A third eye remainedblind because of a pre-existing intraocular inflamma-tion that caused a change in consistency of the lensmaterial and retention of the lens protein.7
Ultrasonic phacoemulsification may be successful inremoving the lens of birds with large eyes (such as
SECTION SIX SURGERY
1100

raptors).27 Phacoemulsification is a form of extracap-sular lensectomy achieved by ultrasonic fragmenta-tion of the lens cortex and nucleus. Medical therapyis instituted preoperatively using a neomycin, po-lymyxin B and dexamethasone solution applied topi-cally to the eye at least TID for one to three days.Periocular skin and feathers are prepared asepti-cally, and a wire, self-retaining eyelid speculum ispositioned. A lateral canthotomy is performed usingscissors. Because the avian eye has limited mobilitywithin the globe, perilimbal stay sutures are notrequired. Mydriasis may be induced with 0.045 to0.09 mg d-tubocurarine chloride injected into theanterior chamber.
FIG 41.2 a) Idiopathic paralysis of the eyelid (arrow) may result inexposure keratitis and epiphora that can be corrected with acanthoplasty. b) The superior and inferior eyelids are incised usingscissors to remove the lid margin and associated glandular tissue.A thin strip of eyelid is removed for a distance approximatelyone-fourth the total eyelid length. c) The eyelids are suturedtogether starting at the lateral canthus and extending toward themedial extent of the incision. d) Only the skin surface requiressuturing, as the conjunctival surface will be held in apposition.Monofilament nylon sutures (8-0 to 10-0) are placed in a simpleinterrupted pattern.
CHAPTER 41 SOFT TISSUE SURGERY
1101

The phacoemulsification tip requires a 3 mm incisionat the limbus or perilimbus at approximately the 10and 3 o’clock positions. A #11 scalpel blade or a vonGraefe cataract knife is used to make these incisions.Prior to making the second incision, a 22 ga needleconnected to an IV set (containing lactated Ringer’ssolution supplemented with aqueous sodium bicar-bonate without preservative to a final concentrationof 25 mEq/l) is inserted through the first incision.
The depth of the anterior chamber is maintainedusing a continuous infusion of this solution while thesecond incision is made.
A cystotome or 27 ga needle with a bent tip is insertedthrough the second incision and used to create a tearin the anterior lens capsule at its periphery. Theanterior capsule is not removed in order to helpcontain the fragments of lens material. After thecapsulotomy is created, the needle is removed and
FIG 41.3 Cataract removal can be performed using phacoemulsification in most raptorial birds with large eyes. For most companion birdswith small eyes, standard surgical techniques are used. a) Under the operating microscope, a small corneal incision is made. b) A 26 gaone-inch needle with the tip bent is inserted into the anterior chamber and used to tear the anterior lens capsule. c) A needle is then insertedinto the lens through the anterior capsule to break down the lens and d) it is flushed out of the anterior chamber with lactated Ringer’ssolution. The corneal incision is closed with one or two simple interrupted sutures.
SECTION SIX SURGERY
1102

the phacoemulsification tip is inserted through thesecond incision, through the capsulotomy incisionand under the anterior capsule. The tip is hollowwith a 0.75 mm internal diameter and is used toaspirate materials or vibrate at 40,000 cycles/second.It is preferable for the lens to be removed without theuse of ultrasonic waves. The posterior lens capsule isleft intact. Once the entire lens is removed, the ante-rior capsule is removed by grasping it with Colibriforceps or the cystotome and tearing it from its at-tachments. The incisions are closed with 8-0 poly-glactin 910 in a simple interrupted pattern. The firstincision is closed while the infusion needle is main-tained. Some fluid is lost during closure of the secondincision but the depth of the anterior chamber isreestablished within a few minutes. The lateral can-thotomy is closed using 5-0 polyglactin 910 in a sim-ple interrupted pattern. At present, lens replacementdevices are not commercially available in a size ap-propriate for avian patients.
Postoperatively, topical neomycin-polymyxin B-dex-amethasone is applied at least TID for approximately14 days and exercise is restricted for several weeks.Minimal evidence of uveitis has been noted in thepostoperative period.27,38 Corneal edema generallyoccurs only at the corneal incision sites. Optimumresults are achieved when minimal surgical traumaoccurs. The corneal endothelium must not be dis-turbed by touching the inner corneal surface withinstruments or by directing the flow of the irrigationsolution toward the cornea.
The ciliary processes fuse to the lens capsule in theregion of the annular pad (see Chapter 26). Theposterior capsule is adhered to the anterior vitreous.Care must be taken to avoid shearing the fusedciliary processes and producing hemorrhage. Poste-rior capsule opacification may occur as a sequela toextracapsular lensectomy, possibly due to retainedlens cortex or iris pigment migration from synechiae.
Enucleation
Enucleation is indicated for treatment of conditionsthat cannot be managed by other methods, such asneoplasia, overwhelming infection and severe trauma(Figure 41.4). The technique is similar to that describedfor mammals, except that birds have a very short opticnerve, and excessive traction on the globe can result inpressure trauma to the brain. Visualization of the mus-cles and blood vessels is enhanced by collapsing theglobe at the start of the procedure. After the cornea isincised, the lens and vitreous are expressed through
the incision. The lid margins must be excised toeliminate glandular tissue and provide a cut edge forthe blepharoplasty. It is also important to remove allconjunctival tissues and any secretory tissue.
One enucleation technique involves suturing the eye-lids together to improve the precision of the incisionof the skin, which needs to be made a few millimetersfrom the lid margin circumferentially (Figure 41.5).The dissection is continued subcutaneously aroundthe globe such that the palpebral conjunctiva will beexcised with the globe. Hemorrhage is controlled withthe bipolar radiosurgical forceps. Once all attach-ments have been transected except for the optic nerveand associated vessels, hemostatic clips are placed onthis neurovascular bundle. Two clips should be ap-plied to assure hemostasis. Curved appliers facilitateplacement of the clips caudal to the globe and mini-mize traction on the optic nerve. The optic nerve issevered and the globe is removed. Any remaininghemorrhage is controlled using radiosurgery. An ocu-lar prosthesise may be used to prevent the sunkenappearance characteristic of avian enucleation. Theskin margins are sutured together routinely. Drainsor bandages are not indicated in most cases.
FIG 41.4 A mature female cockatiel was presented several daysafter a traumatic injury that resulted in rupture of the globe. Theeye was necrotic, and multiple gram-negative bacteria were de-tected by cytologic examination of periocular discharge. The eyewas not salvageable and was removed. Enucleation is a cosmeticsolution to ocular neoplasia and severe unresponsive ocular infec-tions.
CHAPTER 41 SOFT TISSUE SURGERY
1103
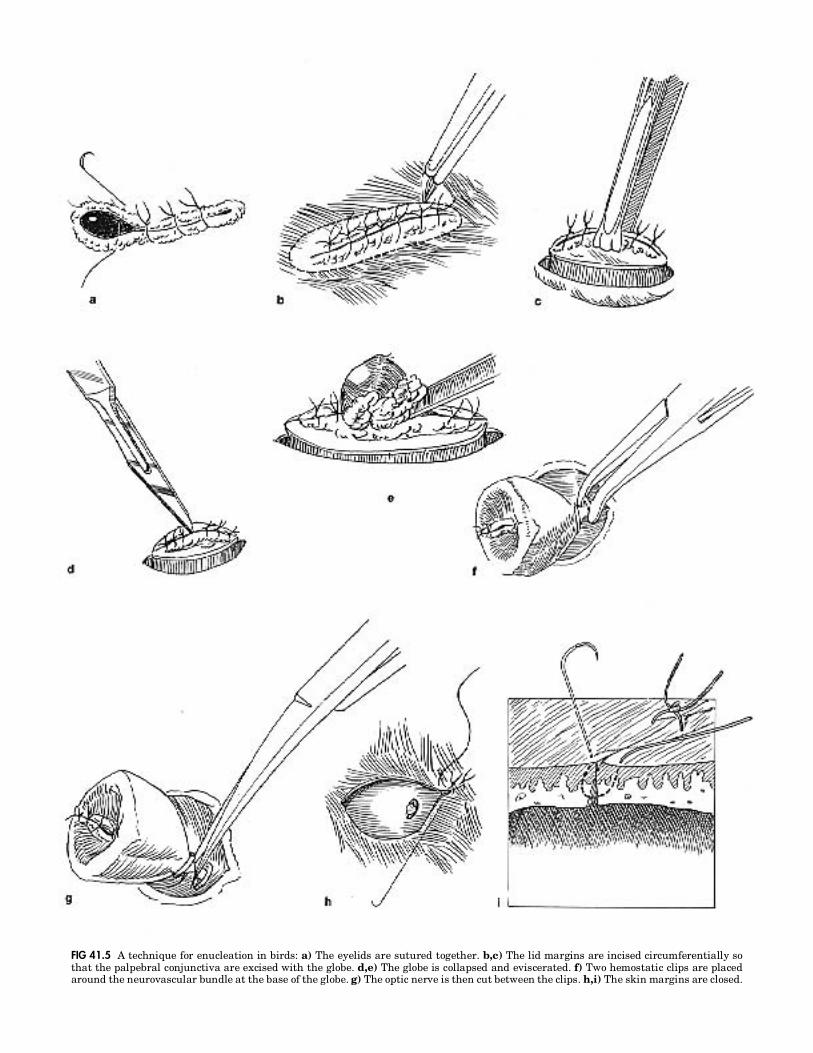
FIG 41.5 A technique for enucleation in birds: a) The eyelids are sutured together. b,c) The lid margins are incised circumferentially sothat the palpebral conjunctiva are excised with the globe. d,e) The globe is collapsed and eviscerated. f) Two hemostatic clips are placedaround the neurovascular bundle at the base of the globe. g) The optic nerve is then cut between the clips. h,i) The skin margins are closed.

Surgery of theRespiratory System
Rhinoliths
Rhinoliths may occur secondary to chronic malnutri-tion and rhinitis (Figure 41.6). These masses, formed ofdesiccated secretions and debris, cause a physical ob-struction to respiration, which may result in respira-tory distress and disfiguring atrophy of the nares (Fig-ure 41.7). Clinical signs include sneezing, upper
respiratory sounds and inflation of the infraorbitalair sac during expiration. Rhinoliths are difficult todiagnose, and identification requires probing undermagnification and a strong light source. Once thetechnique for visualizing these concretions has beenmastered, their occurrence will seem quite common.
Removal of rhinoliths requires magnification. Nasaltissues are friable and bleed easily when trauma-tized, which also predisposes the mucosa to infection.A wooden applicator stick broken to create a longbevel works well to begin the gentle removal of themass (Figure 41.6). The beveled applicator stick isused to elevate the concretion from the margin of thenaris followed by slow, precise, gentle probing withpressure to separate the mass from the wall of the
FIG 41.6 a) A feathered wooden applicator stick can be used to gently break apart and remove rhinoliths. b) These masses start as anaccumulation of debris frequently located caudal to the operculum. 1) probe 2) rhinolith 3) operculum 4) conchae.
FIG 41.7 a) A conure was presented with a three-week history of progressive dyspnea and inflation of the sides of the face on expiration.The right nostril was partially occluded with dried crusty material, and the area around the nostril was hyperemic; the left nostril shownin this view is relatively normal. b) The necrotic material was removed and the nostrils were flushed daily with sterile saline. c) Rhinolithsthat are allowed to persist can cause disfiguring atrophic rhinitis-type lesions.
CHAPTER 41 SOFT TISSUE SURGERY
1105
nasal cavity. Once the margins of the mass areclearly identified, a slightly thicker metal spatulamay be used to finish the dissection. The lith usuallybreaks during manipulation and is retrieved in frag-ments. Fragments may fall caudally into the nasalcavity and must be flushed from their resting placebehind the turbinates.
Once the rhinolith is removed, the lining of the nasalcavity should be swabbed and evaluated cytologicallyand by culture for mycotic and bacterial pathogens.The nares should be flushed with dilute chlor-hexidine, and any fungal or bacterial componentshould be treated systemically with appropriate an-timicrobial medications.
Infraorbital Sinusitis
Infraorbital sinusitis in birds may lead to secondarylacrimal and conjunctival infections, chronic rhinor-rhea and other upper respiratory problems. Effectivetreatment requires a definitive diagnosis. Fre-quently, nutritional problems such as hypovitami-nosis A predispose a bird to secondary infections withbacteria, yeast and fungi. A sinus flush technique canbe used to obtain samples for cytology and cultures(see Chapters 10 and 22).
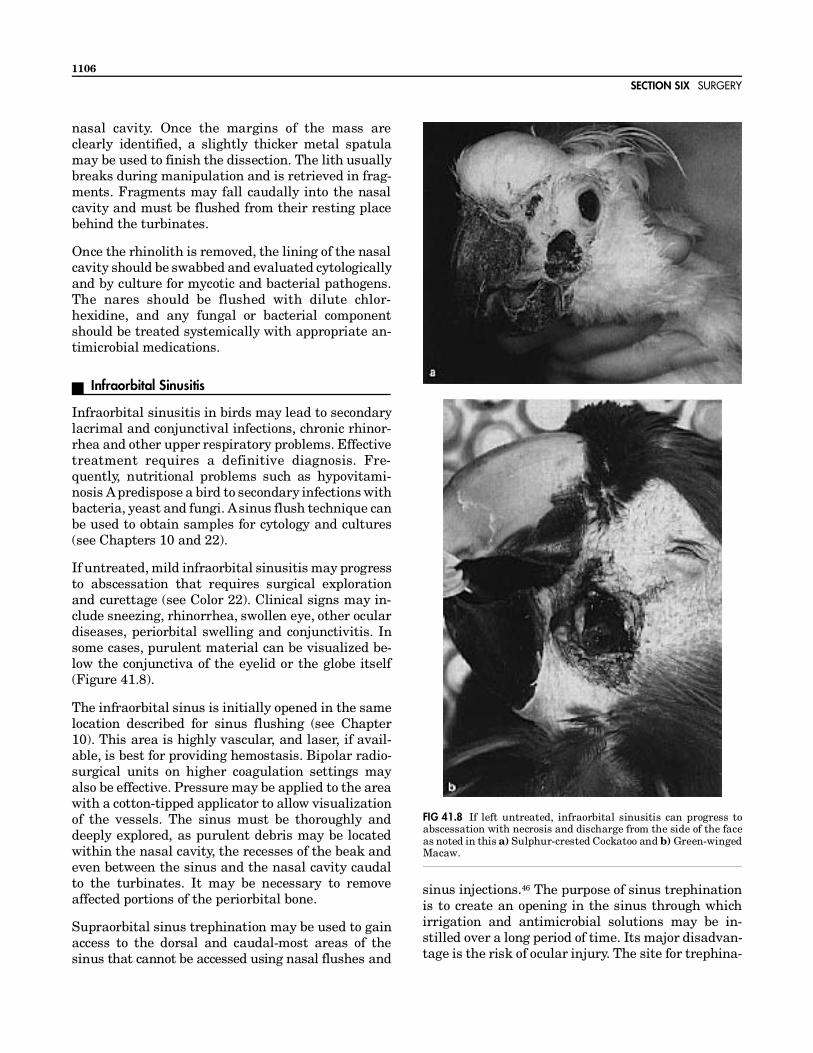
If untreated, mild infraorbital sinusitis may progressto abscessation that requires surgical explorationand curettage (see Color 22). Clinical signs may in-clude sneezing, rhinorrhea, swollen eye, other oculardiseases, periorbital swelling and conjunctivitis. Insome cases, purulent material can be visualized be-low the conjunctiva of the eyelid or the globe itself(Figure 41.8).
The infraorbital sinus is initially opened in the samelocation described for sinus flushing (see Chapter10). This area is highly vascular, and laser, if avail-able, is best for providing hemostasis. Bipolar radio-surgical units on higher coagulation settings mayalso be effective. Pressure may be applied to the areawith a cotton-tipped applicator to allow visualizationof the vessels. The sinus must be thoroughly anddeeply explored, as purulent debris may be locatedwithin the nasal cavity, the recesses of the beak andeven between the sinus and the nasal cavity caudalto the turbinates. It may be necessary to removeaffected portions of the periorbital bone.
Supraorbital sinus trephination may be used to gainaccess to the dorsal and caudal-most areas of thesinus that cannot be accessed using nasal flushes and
sinus injections.46 The purpose of sinus trephinationis to create an opening in the sinus through whichirrigation and antimicrobial solutions may be in-stilled over a long period of time. Its major disadvan-tage is the risk of ocular injury. The site for trephina-
FIG 41.8 If left untreated, infraorbital sinusitis can progress toabscessation with necrosis and discharge from the side of the faceas noted in this a) Sulphur-crested Cockatoo and b) Green-wingedMacaw.
SECTION SIX SURGERY
1106

tion varies with the species, and the anatomy shouldbe carefully studied prior to attempting this procedure.
To create an opening in the supraorbital sinus, theskin is incised exposing the frontal bone. Holes aremade in the bone with a sterile rotary toolf aboutone-half to two-fifths the distance between the ros-tral-most plane of the eye and the naris. The hole isangled toward the midline. Cortical bone is removeduntil the cancellous bone above the supraorbital si-nus is visualized. Drilling proceeds into the supraor-bital sinus and may then be widened to an appropri-ate diameter. Samples for cytology and culture areobtained, and the sinus is flushed with irrigationsolution. The passage of irrigation solution throughthe choana and into the oral cavity confirms that thehole is properly placed. The periorbital tissue willbulge when fluids are introduced, and these tissuesshould not be over-distended. If indicated, this proce-dure may be performed bilaterally in some Passeri-formes, whereas a single trephination site is suffi-cient in Psittaciformes in which the infraorbitalsinuses communicate (see Chapter 22).
The trephination sites may be irrigated as often asindicated with appropriate antimicrobial solutions.The incisions heal rapidly and may need to be openedperiodically. When therapy is no longer indicated, thetrephination sites heal with minimal scarring.
Hyperinflation of the Cervicocephalic Air Sac
This condition is thought to occur secondary to trauma,but the location of leakage of air into the subcutaneousspace is generally not identifiable. Generalized subcu-taneous emphysema usually occurs in small birds,while in larger species the emphysema is generallyconfined to the dorsum of the neck (see Figure 22.11). Aprocedure for surgically implanting a cutaneous stentat the poll of the head to allow the air to escape (in alocation where the bird cannot remove the device) hasbeen described.12 A Teflon stent,h with a 5 mm outer rimthat allows the skin to be placed under its edge toprevent the dermis from closing over the opening, isused for the procedure.
A skin incision is made just large enough for theinsertion of the stent. Sutures are pre-placed throughthe four pairs of holes in the flange of the stent suchthat the suture enters one hole from the externalside, doubles back and passes through the other holefrom the internal side. Once all four sutures areplaced, the stent is implanted. A 22 ga needle isinserted through the skin at the proper location for
one tail of suture material to be inserted through theneedle to be exteriorized through the skin. This pro-cedure is repeated so that each of the four suturespasses through the skin, one hole of the stent, dou-bles back, passes through the other hole of the stentand exits the skin. The four sutures should be placedone on each of the four sides of the incision. Thesutures can then be tied. The main postoperativeproblem is a transient occlusion of the stent withdried tissue fluids, which is easily resolved using aswab or needle.
This syndrome has also been treated in an Amazonparrot using a one-way valve connecting the cervico-cephalic air sac to the clavicular air sac. The ap-proach is through the left lateral thoracic inlet, andthe tube is inserted into the hyperinflated air sac. Itis then directed caudally along the esophagus,through the thoracic inlet and into the cranial aspectof the clavicular air sac. The tube is sutured to thelongus coli muscles to prevent migration. No attemptis made to suture the air sac around the tube. Skinclosure is routine.
Thoracic Surgery
Tracheal/Syringeal ObstructionSeed or other foreign body aspiration,9,19 fungalgranulomas resulting from aspergillosis or candidi-asis36 or concretions of epithelial cells and mucusmay occlude the trachea or syrinx resulting in respi-ratory distress. Some birds present with no premoni-tory signs, while others have a history of voice changeand a more gradual onset of dyspnea.
Therapy depends upon the size of the patient and theconfiguration of the trachea. The trachea of somebirds such as swans and cranes is coiled and encasedwithin the sternum, making retrieval of distal tra-cheal foreign bodies extremely difficult (see Figure12.17).19 Care must be taken not to push the foreignbody into the sternal portion of the trachea. In aSarus Crane, a 22 ga spinal needle was passed trans-versely through the trachea to prevent a kernel ofcorn from migrating farther down the trachea whileit was being surgically removed.19 The avian tracheais composed of complete tracheal rings, which aregenerally cartilaginous, although calcified rings havebeen reported in adult Amazon parrots and adultcranes.19 Annular ligaments connect adjacent rings.40
In some species, the pessulus (a midline laryngealcartilage) may be present, providing an additionalchallenge to foreign body retrieval.19
CHAPTER 41 SOFT TISSUE SURGERY
1107
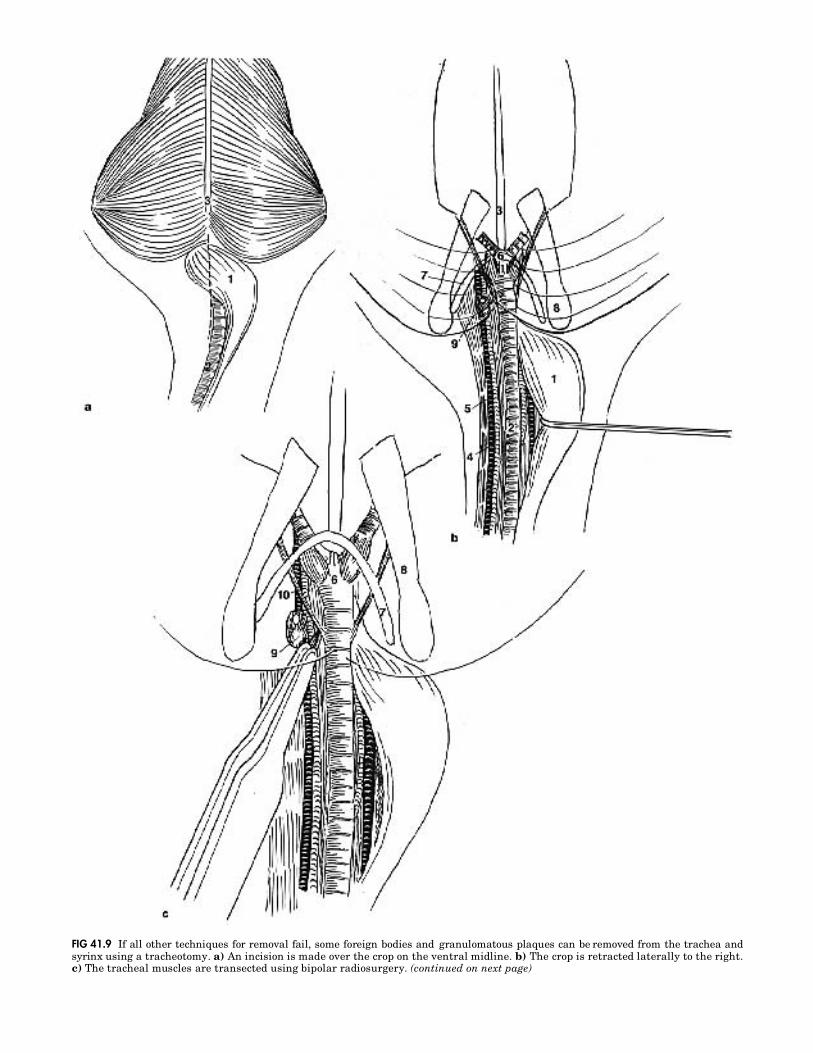
FIG 41.9 If all other techniques for removal fail, some foreign bodies and granulomatous plaques can be removed from the trachea andsyrinx using a tracheotomy. a) An incision is made over the crop on the ventral midline. b) The crop is retracted laterally to the right.c) The tracheal muscles are transected using bipolar radiosurgery. (continued on next page)

d) A spay hook is used to gently pull the syrinx into the thoracic inlet. e) The trachea is transected. f) A blunt probang or suction devicecan be used to remove debris. g) Closure is completed by apposing the tracheal rings. 1) crop 2) trachea 3) sternum 4) internal carotid artery5) jugular vein 6) syrinx 7) clavicle 8) coracoid 9) thyroid 10) sternotracheal muscle 11) esophagus 12) primary bronchi 13) pulmonary arteryand 14) aorta; lateral arrows show primary bronchi to lungs.

Establishment of a patent airway is crucial. Place-ment of an air sac cannula will allow the patient toventilate through an alternate airway until the ob-struction can be removed. It may be beneficial toplace the bird in an oxygen-enriched environmentprior to manipulating the patient for placement ofthe air sac cannula.
In small birds (cockatiels and smaller), the trachealdiameter (approximately 1.5 mm for cockatiels) pre-cludes use of an endoscope to retrieve a foreign bodyor granuloma. If the obstruction is the result of agranuloma or inspissated cells and mucus, a suctiontube (urinary catheter) slightly smaller than the di-ameter of the trachea may be utilized to removematerial from the trachea and syrinx (see Chapter22).30 By maintaining anesthesia with an air saccannula, the trachea may be occluded with the suc-tion tube without compromising respiration. Ifsquamous metaplasia secondary to hypovitaminosisA is suspected, dietary modification and vitamin Asupplementation should be instituted.
In medium to large birds, a rigid or flexible endoscopecan be used to evaluate the cause of an obstructionand potentially aid in its removal. In some cases, theendoscope may allow visualization of the object, butthe tracheal diameter may be too small to use a wirebasket or grasping forceps to remove the object.19 Inthese cases, the endoscope can be used to brush offplaques or physically alter lesions sufficiently toopen the airway, and the loosened plaques can beremoved with a suction tube. Cytologic evaluation ofsamples obtained from the suction tube, or the end ofthe endoscope, may be used to determine the identityof an etiologic agent. Following this procedure, thepatient should be treated using nebulization, intra-tracheal medications and systemic therapies as indi-cated (see Chapter 22).
In some cases, tracheal foreign bodies may be re-trieved using grasping forceps, a Foley catheteri or aFogarty catheter28 with the aid of an endoscope. Thesize of the patient’s tracheal diameter will determinewhich catheter is most appropriate. The catheter ispassed beyond the foreign body and the balloon isinflated sufficiently to occlude the airway but not toprevent it from being withdrawn. With the ballooninflated, the catheter is withdrawn, resulting in re-moval of the foreign body.19,28
As a last ditch effort in medium- to large-sized birds(parrots, raptors, doves, pheasants and peafowl), thethoracic inlet may be approached surgically for re-
moval of tracheal or syringeal foreign bodies (Figure41.9). The patient is positioned in dorsal recumbencyon a surgical restraint board. A tube should be placedin the esophagus to allow for its easy identification toprevent iatrogenic trauma. The skin is incised fromthe right clavicular/sternal junction to the clavicu-lar/coracoid junction just cranial to the crop. The skinis elevated from the crop, and the right lateral aspectof the crop is gently dissected from surrounding tis-sues. Major blood vessels are easily avoided usingblunt dissection. Once the crop is freed from its cla-vicular attachments, it should be reflected to theright. The trachea is identified by its complete carti-lage rings. The sternotracheal muscles are identifiedtraversing obliquely to their caudolateral attach-ments, and both sets of sternotracheal muscles aretransected. A large blood vessel between the musclebellies should be coagulated prior to transection ofthe muscles. A small canine vaginal speculum mayaid in visualization.
At this point, the use of the operating microscope be-comes essential. The restraint board should be elevatedat the cranial end such that the operating microscopecan be used to visualize the structures deep in thethoracic inlet. It may take some time and patience toachieve proper positioning and focus, but this tech-nique allows the surgeon to visualize critical structureswhile having both hands free for manipulations.
The interclavicular air sac is bluntly dissected toexpose the syrinx. A blunt hook is looped over thesyrinx, which is gently pulled into view. In Amazonparrots, small macaws and smaller birds, this proce-dure may result in avulsion of the bronchi from thelung. For these patients, a left lateral approach to thesyrinx is recommended as a last desperate attempt.
A transverse tracheotomy (50% of diameter) can alsobe created on the ventral surface to allow retrieval ofthe foreign material. Foreign bodies have been re-moved through longitudinal tracheal incisions;35,36,44
however, these incisions provide limited visibilityand access due to the inward twisting of the cut rings,and are more prone to iatrogenic trauma duringmanipulation, are more difficult to close than a trans-verse tracheotomy and are more prone to strictureformation.15,46 Unless absolutely mandatory, the tra-chea should not be completely transected in order tomaintain its alignment, reduce tension on the closureand prevent complete disruption of the blood sup-ply.19 Stay sutures placed around the tracheal ringsadjacent to the tracheotomy allow atraumatic ma-nipulation of the trachea. Foreign materials located
SECTION SIX SURGERY
1110

cranial to the tracheotomy site can be pushed out ofthe trachea with a sterile probang. Those locatedcaudal to the tracheotomy site can be removed bysuction. If the trachea completely separates duringmanipulations, anastomosis may be performed. Theincision should be closed with a small-sized, mon-ofilament, absorbable suture material encompassingat least one tracheal ring on each side of the trache-otomy incision.19 A simple interrupted pattern is bestperformed by pre-placing the encircling sutures.Knots should be placed external to the tracheal lu-men. Intraluminal granuloma formation at the su-tures is common. Soft tissue, skin and subcutaneousclosure are routine.
A lateral thoracic approach to the trachea can be usedin very small birds where there is no other means toapproach and evaluate the syringeal area. Practice andmicrosurgical techniques are essential for this proce-dure. The patient is positioned in right lateral recum-bency. An incision is made over the second and thirdribs. These ribs are exposed using blunt dissection, andthey are transected at both ends to allow their completeremoval. This will expose the cranial portion of thelung. Using a moistened cotton-tipped applicator, thecranial extent of the lung is gently dissected and re-flected from its attachments. The jugular vein, pulmo-nary artery and branches of the subclavian artery maybe identified and should be avoided. Dissecting be-tween these vessels allows visualization of the syrinx,which is incised (2 to 3 mm) using bipolar radiosurgicalforceps at its junction with the left primary bronchus.A foreign body may then be removed using a combina-tion of tracheal endoscopy, visualization and suctionthrough the syringeal incision.
The syringeal incision is allowed to close by secondintention. The ribs are not replaced. The lung isrepositioned in its normal location. Soft tissues areapposed and the remainder of the closure is routine.This is a difficult procedure that should be used onlyas a life-saving technique when all other methods forforeign body removal have failed.
DevocalizationThe authors and editors consider devocalization acruel and unethical practice; therefore, a procedurewill not be described. Birds with vocalization pat-terns that are unacceptable to a client should beplaced in new homes.
PneumonectomyRemoval of lung tissue may be indicated in the treat-ment of abscesses or granulomas. In some instances,
a surgical lung biopsy may be required instead of anendoscope-guided biopsy for diagnosis of a respira-tory disease.20
In birds, there is no distinct pleural space, and thevisceral and parietal pleura are in close approxima-tion. The pulmonary parenchyma is contoured to thedorsal aspect of the ribs and the intercostal spaces.This makes the lungs easy to approach surgically.Compared with mammalian lungs, those of birds aremore vascular and the intrinsic clotting mechanismappears to be less efficient.
The lungs can be approached through the caudal tho-racic air sac or the intercostal space by removing one ormore ribs as described for the lateral approach to thesyrinx. The affected lung tissue is elevated from theribs and surrounding structures using a moistenedcotton-tipped applicator or a spatula. The affected areais isolated using vascular clips, and the tissue to beremoved is incised such that the clips remain with theviable portion of lung. No studies have been conductedto determine the amount of lung that may be removedor the physiologic effects of partial pneumonectomy;however, clinically, partial pneumonectomy patientsappear to function normally.20
Closure is accomplished using wire suture to opposethe intact ribs on each side of the thoracotomy site. Fora caudal thoracotomy, the pubis may be utilized to aidin closure of the gap created by the removal of ribs.
Surgery of theGastrointestinal System
Pharyngostomy Feeding Tube
Pharyngostomy feeding tubes are indicated when itis necessary to aliment the patient while bypassingthe oral cavity, esophagus or crop. The technique issimple and straightforward. The right side of theneck at the caudal extent of the lower mandible isprepared for surgery. A small incision is madethrough the skin, and the esophagus is identified. Amoistened cotton-tipped applicator is inserted per osinto the esophagus to aid in identification and toprevent the incision from penetrating the oppositeside of the esophagus. A small (1 to 2 mm) stabincision is made into the esophagus to allow passage
CHAPTER 41 SOFT TISSUE SURGERY
1111
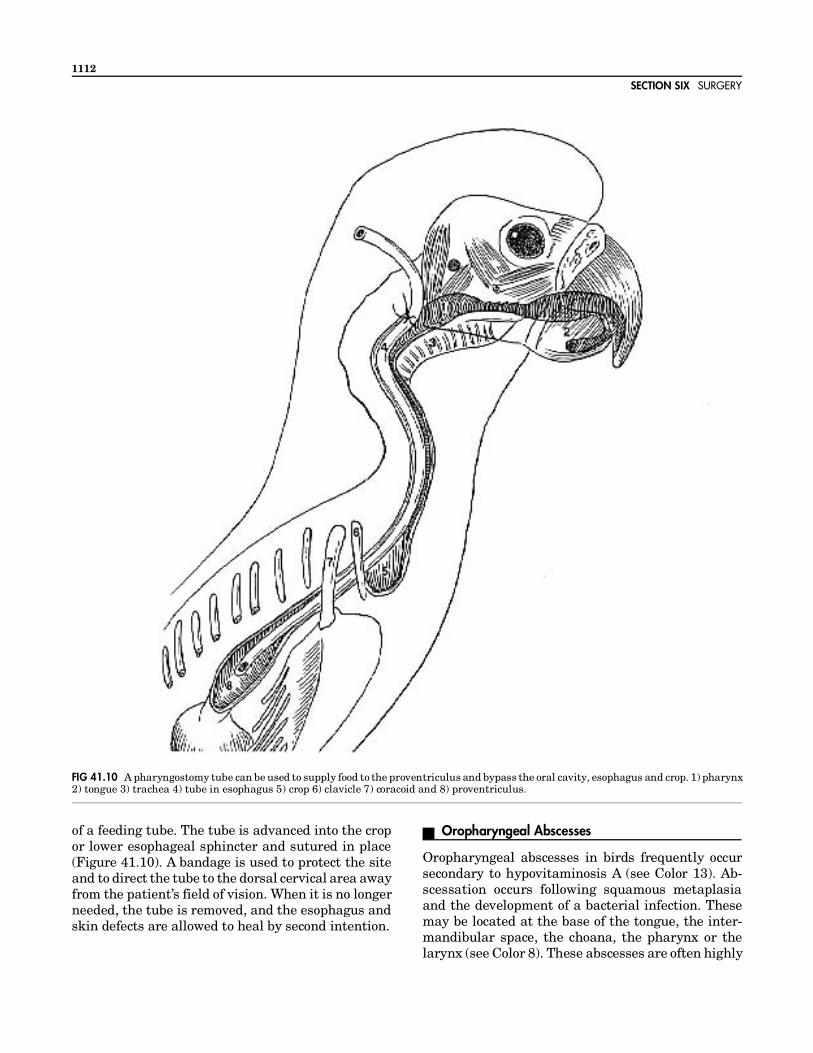
of a feeding tube. The tube is advanced into the cropor lower esophageal sphincter and sutured in place(Figure 41.10). A bandage is used to protect the siteand to direct the tube to the dorsal cervical area awayfrom the patient’s field of vision. When it is no longerneeded, the tube is removed, and the esophagus andskin defects are allowed to heal by second intention.
Oropharyngeal Abscesses
Oropharyngeal abscesses in birds frequently occursecondary to hypovitaminosis A (see Color 13). Ab-scessation occurs following squamous metaplasiaand the development of a bacterial infection. Thesemay be located at the base of the tongue, the inter-mandibular space, the choana, the pharynx or thelarynx (see Color 8). These abscesses are often highly
FIG 41.10 A pharyngostomy tube can be used to supply food to the proventriculus and bypass the oral cavity, esophagus and crop. 1) pharynx2) tongue 3) trachea 4) tube in esophagus 5) crop 6) clavicle 7) coracoid and 8) proventriculus.
SECTION SIX SURGERY
1112

vascular necessitating careful dissection and hemo-stasis for removal.
Surgical management of an oral abscess involvespretreatment with antibiotics and vitamin A (if indi-cated). A fine-needle aspirate may be used for cultureand sensitivity. In cases of hypovitaminosis A, paren-teral vitamin A administration will help encapsulatethe abscess and reduce inflammation and vasculari-zation. In some cases, beta carotene therapy hasresulted in complete resolution of the abscess with-out the need for surgical intervention.
Abscesses that are lanced and curetted frequentlyrecur because minute fragments of material may belocated within the tissue surrounding the abscess.The abscess will reform when the mucosa heals overthe trapped necrotic debris. Removing the tissue sur-rounding the abscess is preferable. In some locations,such as with intermandibular abscesses, the abscessand its capsule may be removed intact. Dissection ismeticulous and time-consuming, and accurate hemo-stasis is imperative.
Choanal abscesses must be lanced to remove necroticmaterial followed by surgical removal of the abscess.Laser or radiosurgery are best for controlling hemor-rhage in this highly vascular area. Invasive ab-scesses may erode the palatine artery and result insevere hemorrhage.
Oropharyngeal Papillomas
Oral papillomas are uncommon except in some ma-caw species. These masses can be removed usingcryosurgery, radiosurgery or chemical cautery (silvernitrate). Papillomatous growths that extend into thecrop and proventriculus are currently considered un-treatable, and are eventually fatal.
Esophageal Perforation
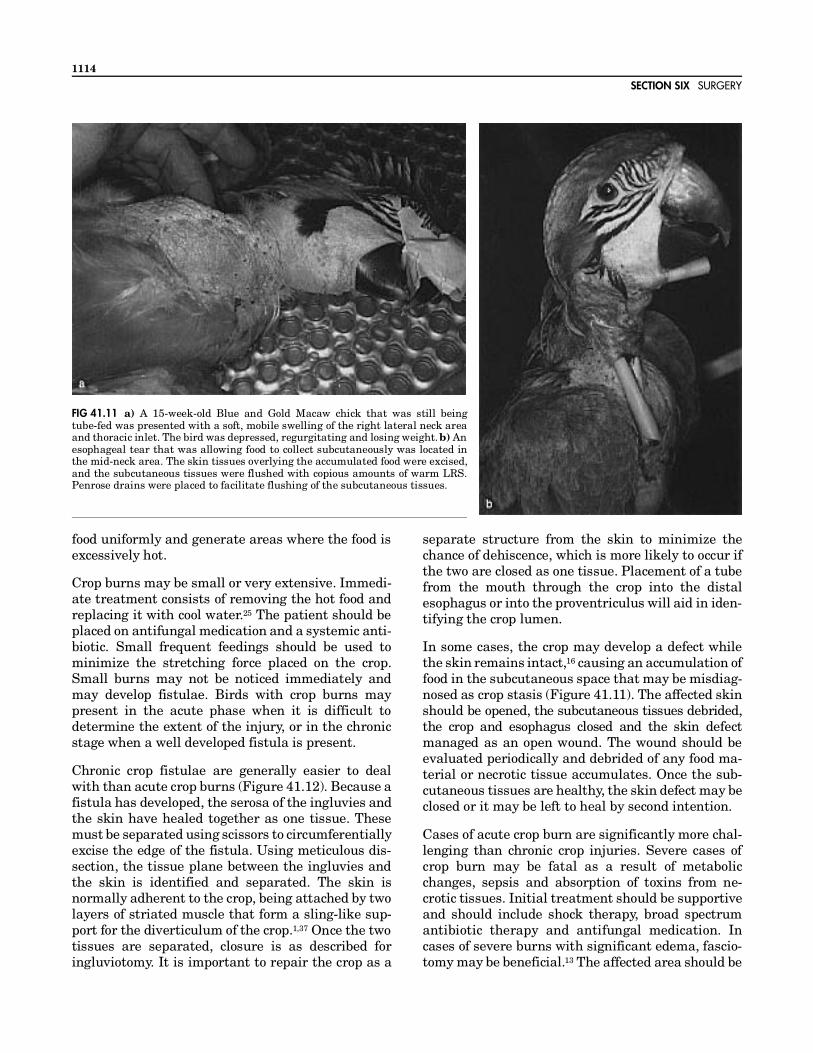
Esophageal perforation may occur from using a rigidfeeding tube for supportive alimentation in a strug-gling bird, in enthusiastic, violently bobbing neo-nates or from feeding overheated formula (see Color30). As the tube penetrates the esophagus, food ormedication may be deposited in the subcutaneoustissues (Figure 41.11). Additional material may accu-mulate during subsequent feedings. Edema, sepsisand toxemia occur in response to the foreign mate-rial. Emergency and supportive care should be insti-tuted. A proventricular feeding tube should be placedto bypass the damaged esophageal tissue. Fascio-
tomy, copious irrigation, debridement, topical anti-septics and systemic antimicrobials are indicated.Surgical debridement and closure may be possible inthree to five days when the affected tissues begin togranulate and appear healthy. Extensive fasciotomyand copious irrigation are probably the most impor-tant portions of the initial treatment.
Esophageal Strictures
A case of esophageal stricture of undetermined etiol-ogy in a Hyacinth Macaw was successfully treated bybougienage.56 The stricture was located in the tho-racic esophagus and was believed to be obstructingthe flow of ingesta to the proventriculus. Initially a 5Fr rubber feeding tube was the largest bougie thatcould be inserted. Three sessions of bougienage sepa-rated by a few months produced an increase in lumensize to accommodate an 11 Fr bougie. Attempts topass larger tubes produced an intense vagal re-sponse. Following this treatment, the patient wasable to eat solid food. No steroids were administered;however, the owner instituted therapy involving non-steroidal anti-inflammatory medications (ibuprofenand naprosyn).
Crop Fistula Repair
The primary function of the crop is storage of food.When the crop is full of food, it is often prominent andpendulous, making it more susceptible to trauma.16
Penetrating wounds can result in the formation of afistula in the crop. Such wounds are often the resultof animal bites, improperly assisted feeding tech-nique, foreign body ingestion, trauma and consump-tion of excessively hot food items.16 A permanentfistula may form because food will pass continuouslyfrom the crop through the defect in the crop and skinand out into the environment (see Color 30).
Crop fistulae occur most commonly in neonates beinghand-fed. The crop of neonates is more fragile andsusceptible to injury than the adult ingluvies.16 Onesource of injury to the neonatal crop is penetrationresulting from improper or careless gavage tube-feeding. This allows food to escape from the esopha-gus or crop and collect under the skin, creating anabscess and potential toxemia. Early diagnosis andtreatment are essential for optimum recovery.1,16,25
Crop burns may also occur if a hair dryer is used todry a wet bird.1 Crop burns most frequently occurwhen food is warmed in a microwave oven and notthoroughly mixed.1,4,25 Microwave ovens do not heat
CHAPTER 41 SOFT TISSUE SURGERY
1113
food uniformly and generate areas where the food isexcessively hot.
Crop burns may be small or very extensive. Immedi-ate treatment consists of removing the hot food andreplacing it with cool water.25 The patient should beplaced on antifungal medication and a systemic anti-biotic. Small frequent feedings should be used tominimize the stretching force placed on the crop.Small burns may not be noticed immediately andmay develop fistulae. Birds with crop burns maypresent in the acute phase when it is difficult todetermine the extent of the injury, or in the chronicstage when a well developed fistula is present.
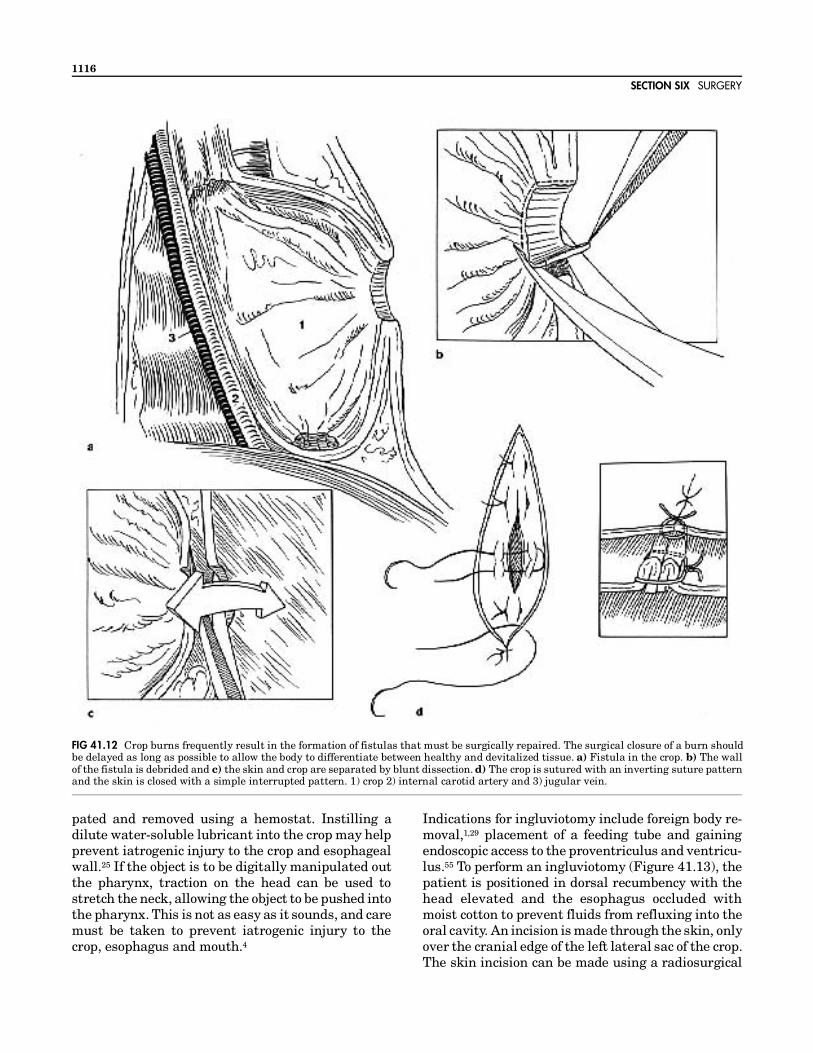
Chronic crop fistulae are generally easier to dealwith than acute crop burns (Figure 41.12). Because afistula has developed, the serosa of the ingluvies andthe skin have healed together as one tissue. Thesemust be separated using scissors to circumferentiallyexcise the edge of the fistula. Using meticulous dis-section, the tissue plane between the ingluvies andthe skin is identified and separated. The skin isnormally adherent to the crop, being attached by twolayers of striated muscle that form a sling-like sup-port for the diverticulum of the crop.1,37 Once the twotissues are separated, closure is as described foringluviotomy. It is important to repair the crop as a
separate structure from the skin to minimize thechance of dehiscence, which is more likely to occur ifthe two are closed as one tissue. Placement of a tubefrom the mouth through the crop into the distalesophagus or into the proventriculus will aid in iden-tifying the crop lumen.
In some cases, the crop may develop a defect whilethe skin remains intact,16 causing an accumulation offood in the subcutaneous space that may be misdiag-nosed as crop stasis (Figure 41.11). The affected skinshould be opened, the subcutaneous tissues debrided,the crop and esophagus closed and the skin defectmanaged as an open wound. The wound should beevaluated periodically and debrided of any food ma-terial or necrotic tissue accumulates. Once the sub-cutaneous tissues are healthy, the skin defect may beclosed or it may be left to heal by second intention.
Cases of acute crop burn are significantly more chal-lenging than chronic crop injuries. Severe cases ofcrop burn may be fatal as a result of metabolicchanges, sepsis and absorption of toxins from ne-crotic tissues. Initial treatment should be supportiveand should include shock therapy, broad spectrumantibiotic therapy and antifungal medication. Incases of severe burns with significant edema, fascio-tomy may be beneficial.13 The affected area should be
FIG 41.11 a) A 15-week-old Blue and Gold Macaw chick that was still beingtube-fed was presented with a soft, mobile swelling of the right lateral neck areaand thoracic inlet. The bird was depressed, regurgitating and losing weight. b) Anesophageal tear that was allowing food to collect subcutaneously was located inthe mid-neck area. The skin tissues overlying the accumulated food were excised,and the subcutaneous tissues were flushed with copious amounts of warm LRS.Penrose drains were placed to facilitate flushing of the subcutaneous tissues.
SECTION SIX SURGERY
1114

liberally opened, copiously irrigated and left to healby second intention or a delayed closure performed ata later date. In less severe cases, clinical signs maysimply be consistent with a “sick bird:” lethargy,anorexia and fluffed appearance.16
The feeding regimen will need to be changed in orderto bypass the damaged tissues. This can be accom-plished using a needle catheter intestinal feedingtube11 or by tube-feeding directly into the proven-triculus. It is important to instruct the owner onproper methods for tube-feeding, and it must bestressed that the proventriculus cannot hold thesame volume of food as the ingluvies; therefore, feed-ings will be more frequent and of smaller volume.
In most cases, it will be three to five days before thedelineation between healthy and devitalized tissuesbecomes apparent,1 and it may take as long as 7 to 14days.45 Prior to this, it will be difficult to determinewhat tissue should be removed and what is viableand should remain. Burned tissue becomes pale andedematous and then becomes dry, dark and leathery.Eventually, the devitalized tissue will separate fromviable tissue and the edges of the crop and skin willheal together, forming a fistula (see Color 30).
Any tissue that is obviously necrotic should be de-brided to reduce the body’s burden of necrotic tissue.If a skin and crop defect result from this debride-ment, this defect can be used to intubate the proven-triculus for nutritional support and also to cleanseand apply topical antiseptics to reduce the chances ofdeveloping fungal or bacterial infections.
The definitive correction should be postponed untilapproximately five days after the injury when thedemarcation between healthy and devitalized tissueis apparent.1 It is often beneficial to endoscopicallyexamine the crop prior to planning the surgery. Asmall catheter can be used to inject air and dilate thecrop, and an endoscope can be used to detect avascu-lar, darkened areas. It is important to evaluate theentire crop, because devitalized mucosa may occuraway from the primary burn. The aboral extent of thecrop at the thoracic inlet is a location where devital-ized areas are often missed.
At surgery, all necrotic tissue must be removed andthe tubular structure of the esophagus and ingluviesreestablished. In some cases this may be very chal-lenging, as major portions of crop may be devitalized.If possible, the length of the crop should be main-tained even if only a thin strip of esophageal tissueremains. Esophageal strictures are more likely to
occur if a resection and anastomosis have been per-formed than if a thin strip of normal esophagus ispreserved and allowed to granulate over a stent. Ifenough viable tissue remains, it may be suturedaround a pharyngostomy feeding tube, throughwhich the patient can receive alimentation while thecrop is healing. The crop will stretch in time, but thepatient must be fed frequently small volumes of softor liquid diets until the capacity of the ingluviesincreases.1 Where indicated, a Penrose drain may beplaced to provide postoperative local drainage andmay also be used for wound irrigation.16
In cases where there is extensive tissue loss, thedefect may be allowed to heal by second intentionwhile maintaining the patient with a pharyngostomyfeeding tube. If the defect is so large that woundcontraction cannot occur, a dermoplasty may be per-formed once there is a healthy bed of granulationtissue. A rotating skin flap will generally providetissue to cover the defect.
Ingluviotomy
Neonates are susceptible to ingestion of foreign ob-jects such as substrate materials, especially if theyare underfed. Feeding tubes, small toys and unhulledseed may also be ingested.4 These objects may inter-fere with the passage of food and may irritate thelining of the ingluvies.4 Palpation of a persistentlump in the crop, food retention, delayed crop empty-ing and regurgitation are clinical signs associatedwith crop foreign bodies.
Small objects may be retrieved from the crop using aflexible endoscope and a biopsy instrument. Manyforeign bodies including feeding tubes can be pal-
CLINICAL APPL ICAT IONSHow to Repair a Crop Fistula (Figure 41.12)
Intubate the patient and pack the esophagus with moistenedgauze to prevent flush solution from entering the pharyngealarea.
Remove any necrotic tissue and thoroughly clean the under-lying bed of granulation tissue with a dilute chlorhexidinesolution.
Once the tissue defect is thoroughly cleaned, debride theedges of the fistula to remove granulation tissue and com-pletely separate the crop from overlying skin.
Separate the skin and crop further by careful blunt dissectionwith strabismus scissors.
Perform the closure in two layers. The crop is initially closedwith an inverting suture pattern making certain that theincision line extends past the defect on both ends. The skincan be closed in a simple interrupted pattern.
CHAPTER 41 SOFT TISSUE SURGERY
1115
pated and removed using a hemostat. Instilling adilute water-soluble lubricant into the crop may helpprevent iatrogenic injury to the crop and esophagealwall.25 If the object is to be digitally manipulated outthe pharynx, traction on the head can be used tostretch the neck, allowing the object to be pushed intothe pharynx. This is not as easy as it sounds, and caremust be taken to prevent iatrogenic injury to thecrop, esophagus and mouth.4
Indications for ingluviotomy include foreign body re-moval,1,29 placement of a feeding tube and gainingendoscopic access to the proventriculus and ventricu-lus.55 To perform an ingluviotomy (Figure 41.13), thepatient is positioned in dorsal recumbency with thehead elevated and the esophagus occluded withmoist cotton to prevent fluids from refluxing into theoral cavity. An incision is made through the skin, onlyover the cranial edge of the left lateral sac of the crop.The skin incision can be made using a radiosurgical
FIG 41.12 Crop burns frequently result in the formation of fistulas that must be surgically repaired. The surgical closure of a burn shouldbe delayed as long as possible to allow the body to differentiate between healthy and devitalized tissue. a) Fistula in the crop. b) The wallof the fistula is debrided and c) the skin and crop are separated by blunt dissection. d) The crop is sutured with an inverting suture patternand the skin is closed with a simple interrupted pattern. 1) crop 2) internal carotid artery and 3) jugular vein.
SECTION SIX SURGERY
1116
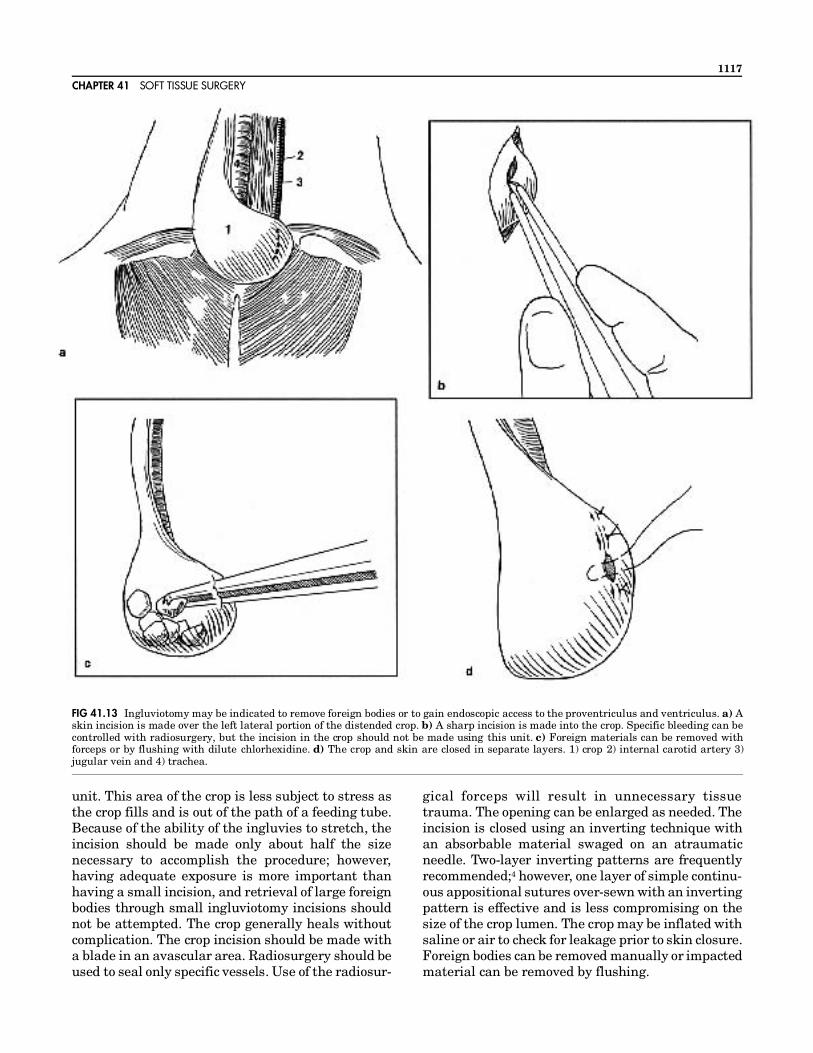
unit. This area of the crop is less subject to stress asthe crop fills and is out of the path of a feeding tube.Because of the ability of the ingluvies to stretch, theincision should be made only about half the sizenecessary to accomplish the procedure; however,having adequate exposure is more important thanhaving a small incision, and retrieval of large foreignbodies through small ingluviotomy incisions shouldnot be attempted. The crop generally heals withoutcomplication. The crop incision should be made witha blade in an avascular area. Radiosurgery should beused to seal only specific vessels. Use of the radiosur-
gical forceps will result in unnecessary tissuetrauma. The opening can be enlarged as needed. Theincision is closed using an inverting technique withan absorbable material swaged on an atraumaticneedle. Two-layer inverting patterns are frequentlyrecommended;4 however, one layer of simple continu-ous appositional sutures over-sewn with an invertingpattern is effective and is less compromising on thesize of the crop lumen. The crop may be inflated withsaline or air to check for leakage prior to skin closure.Foreign bodies can be removed manually or impactedmaterial can be removed by flushing.
FIG 41.13 Ingluviotomy may be indicated to remove foreign bodies or to gain endoscopic access to the proventriculus and ventriculus. a) Askin incision is made over the left lateral portion of the distended crop. b) A sharp incision is made into the crop. Specific bleeding can becontrolled with radiosurgery, but the incision in the crop should not be made using this unit. c) Foreign materials can be removed withforceps or by flushing with dilute chlorhexidine. d) The crop and skin are closed in separate layers. 1) crop 2) internal carotid artery 3)jugular vein and 4) trachea.
CHAPTER 41 SOFT TISSUE SURGERY
1117

Celiotomy
Surgical approaches to the abdomen involve invasionof the air sac, allowing anesthetic gas to escapethrough the celiotomy site. This effect can be mini-mized by packing the borders of the incision withsaline-moistened gauze sponges. Additionally, an airsac cannula may be introduced into the abdominalair sac on the side contralateral to the surgical inci-sion. This will allow anesthetic gas to enter an intactair sac, pass through the lung and out the trachea.Using this technique, anesthetic gas does not escapefrom the surgery site, and waste gas can be scav-enged from the trachea. For any celiotomy, the pa-tient should be positioned with the cranial part of thebody elevated 30 to 40° to prevent irrigation fluidsfrom flowing craniad and entering the lungs follow-ing incision of the air sacs. Similarly, patients withascites should have the fluid removed from thecoelomic cavity prior to opening the air sacs. Mois-tened cotton may be placed in the caudal pharynx toocclude the esophagus and prevent proventricularreflux from entering the oral cavity and causing as-piration pneumonia. The celiotomy approaches usedfor access to the avian abdomen include left lateral,ventral and transverse. Skin incisions can be madein varying arrangements and combinations depend-ing on the surgical procedure and the degree of ab-dominal exposure that is required (Figure 41.14).
Left Lateral CeliotomyA left lateral celiotomy provides the best exposure ofthe proventriculus, the ventriculus, the female repro-ductive tract and the left kidney (Figure 41.15).15,24
With the patient in right lateral recumbency, thecaudodorsal border of the sternum can be palpated.The pelvic bones, including the cranial extent of thepubis, should be identified. The left leg should beretracted as far caudally as possible, creating a foldof skin (knee web) in the flank extending from thestifle to the lateral margin of the sternum. In smallpatients, lung tissue can be visualized per cutane-ously through the intercostal spaces between thefifth, sixth and seventh ribs. In larger birds, thelatissimus dorsi and iliotibialis cranialis muscles ob-scure visualization of the lung. The skin incision willextend from the cranial extent of the pubis to justdorsal to the uncinate process of the fifth or sixth rib.The incision is started in the knee web and continuedventral and caudal following the boundaries of thepostventer and postlateral regions, passing throughthe groove of the groin web caudally to the region ofthe pubic bone. Care should be taken to incise onlythe skin, which is easily accomplished using the
modified bipolar radiosurgical forceps. Once the skinis incised, the left leg may be further retracted cau-dally and somewhat dorsally to expose the abdomi-nal wall. A branch of the superficial medial femoralartery and vein should be identified passing over thelumbar fossa toward the pubis. These vessels shouldbe sealed or ligated prior to incising the musculature.The radiosurgical body wall incision is initiated inthe external abdominal oblique muscle, just caudalto the last rib. The incision is extended caudallythrough the internal abdominal oblique and trans-versus abdominis muscles to the cranial extent of thepubis.
The intercostal vessels coursing along the cranialborder of the last two or three ribs should be ligatedor coagulated. In small birds, these vessels may besealed by inserting the indifferent electrode insidethe thoracic wall, lightly opposing the electrodes,withdrawing the electrodes until the cranial aspect ofthe rib is encountered, then activating the electrodes.In larger birds, it is best to cut the rib, clamp thevessel cranial to the rib to achieve hemostasis, thenidentify the vessel visually and apply a hemostaticclip. In larger birds, the caudal-most two or three ribswill need to be transected at their dorsal and ventralextents and removed to achieve adequate visualiza-tion of the viscera. In small birds, excision of the ribsmay not be required. They may be fractured andretracted dorsally to provide proper exposure. Thismethod is preferred, because closure of the incision iseasier. Once the incision is made through the muscu-lature, the shiny surface of the caudal thoracic or theabdominal air sac is visualized. In some patients, thelung extends caudally as far as the seventh rib. Caremust be taken to prevent lacerating the lung, whichcan be gently elevated using a moistened cotton-tipped applicator if necessary.
A Heiss, Alm or mini-Balfour retractor should bepositioned to maintain retraction of the body wall.Entering the air sac, the surgeon can visualize thelung parenchyma and the hilus of the caudal thoracicair sac entering the lung at its craniodorsal extent.Dorsally, the liver lobes become thin at their margins,and the wall of the proventriculus can be observed. Ifthe abdominal air sac is entered instead of the caudalthoracic air sac, the lung is not visible, but will liedorsolateral to the incision rather than cranial asobserved when entering through the caudal thoracicair sac. Medially, the proventriculus can be seensuspended by the air sacs and suspensory ligaments.Often the intestines are the first structures encoun-tered. They can be gently retracted using a cotton-
SECTION SIX SURGERY
1118

FIG 41.14 Several different celiotomy incisions can be used to gain access to the abdomen of birds. 1) sternum 2) eighth rib 3) femur 4) pubisand 5) vent.
CHAPTER 41 SOFT TISSUE SURGERY
1119
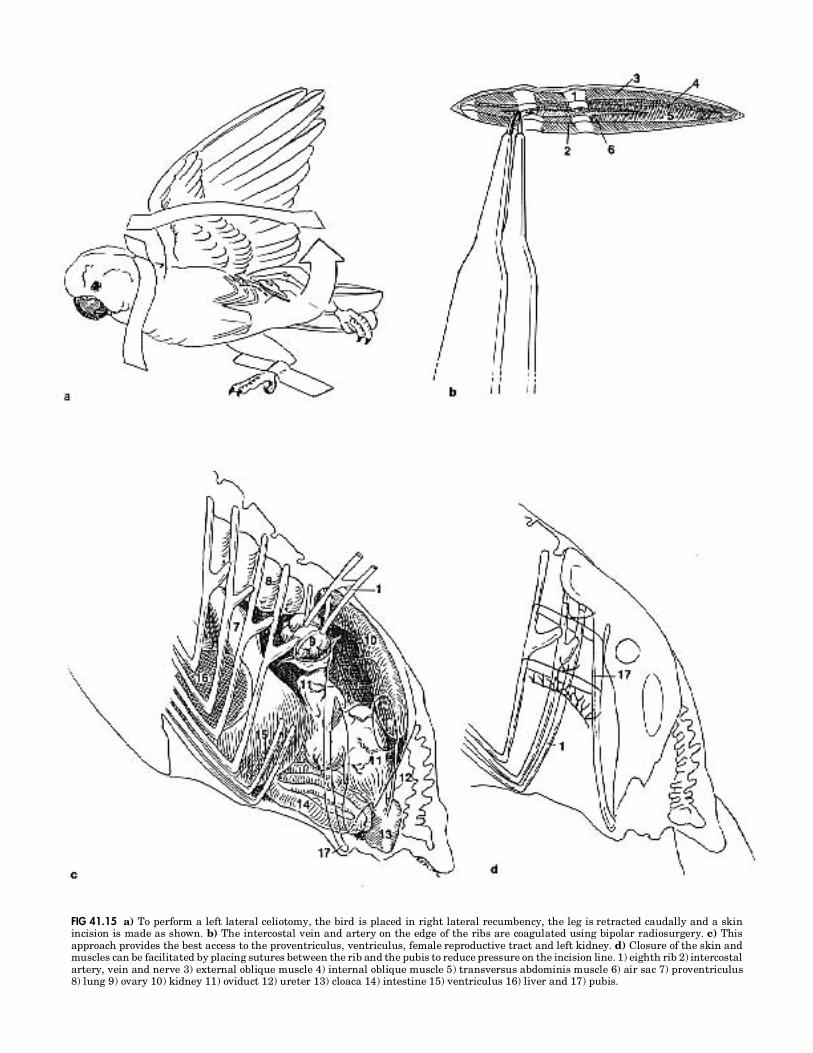
FIG 41.15 a) To perform a left lateral celiotomy, the bird is placed in right lateral recumbency, the leg is retracted caudally and a skinincision is made as shown. b) The intercostal vein and artery on the edge of the ribs are coagulated using bipolar radiosurgery. c) Thisapproach provides the best access to the proventriculus, ventriculus, female reproductive tract and left kidney. d) Closure of the skin andmuscles can be facilitated by placing sutures between the rib and the pubis to reduce pressure on the incision line. 1) eighth rib 2) intercostalartery, vein and nerve 3) external oblique muscle 4) internal oblique muscle 5) transversus abdominis muscle 6) air sac 7) proventriculus8) lung 9) ovary 10) kidney 11) oviduct 12) ureter 13) cloaca 14) intestine 15) ventriculus 16) liver and 17) pubis.

tipped applicator. The intestines are fragile andshould not be manipulated with toothed forceps,which will create severe bruising and potential per-foration. Once the intestines are retracted caudally,the kidney may be identified at the dorsomedial as-pect of the coelom. The ovary or left testicle should beencountered at the cranial division of the kidney. Theadrenal gland is located between the gonad and thecranial division of the kidney, but may be obscured ifthe gonad is large. Obesity and hepatomegaly resultin topographical changes in the abdominal anatomy,emphasizing the need to practice on a variety ofcadavers with a variety of conditions prior to per-forming a celiotomy in a clinical patient.
If the seventh and eighth ribs have been removed,closure will require the placement of tension suturesfrom the abdominal musculature to the sixth rib.Sutures passed around the pubic bone may be neces-sary when closing large incisions.
Ventral Midline CeliotomyA ventral midline celiotomy is used primarily forsurgery of the small intestines, liver biopsy, egg-re-lated peritonitis, abdominal masses, egg binding andrepair of a cloacal prolapse. This approach providesaccess to both sides of the coelomic cavity.
The skin is incised in the midpostventer region fromthe sternum to the interpubic space (see Figure41.14). The linea alba is usually broad and easilyidentified. It must be incised carefully because theduodenum crosses from left to right just inside thebody wall. It is best to initiate the incision betweenthe pubic bones over the cloaca. Once a two millime-ter incision is initiated, it may be extended craniadto the level of the sternum. If exposure is limited, theincision may be extended to one or both sides ap-proximately two millimeters from the sternal bordercreating a muscular flap. Further exposure isachieved by extending the incision along one or bothsides of the pubic bones in a similar fashion. Thisapproach provides the best exposure to mid-abdomi-nal masses, uterine masses and generalized abdomi-nal disease (peritonitis). The size of the incisionshould be sufficient to allow a procedure to be per-formed, but as small as possible to minimize tissuedamage and air sac disruption, and to make it easierto maintain anesthesia. If it is necessary to approacha large area of the abdomen, it is often best to openand close each area before proceeding on to anotherarea.
Closure of the body wall is accomplished using sim-ple interrupted or simple continuous, monofilament,synthetic, absorbable suture material. Skin closureis routine.
Transverse CeliotomyTransverse celiotomy provides exposure to a largearea of the abdomen.1,24,51,53 The bird is positioned indorsal recumbency and the postventer region is pre-pared. A transverse skin incision is made midwaybetween the sternum and the vent (see Figure 41.14).1The abdominal wall is lifted and incised with care toavoid lacerating the underlying intestines. The ven-triculus and duodenum are the first organs encoun-tered, but may be reflected to expose the cranialaspect of the cloaca, the middle and caudal lobes ofthe kidneys and the lower reproductive tract of hens.The abdominal wall and skin are sutured separatelyusing 4-0 to 6-0 synthetic, monofilament, absorbablematerial in a continuous or interrupted pattern.
Proventriculotomy and Ventriculotomy
The stomach of birds is divided into an orad, glandu-lar portion (the proventriculus) and the aborad mus-cular ventriculus (gizzard). The isthmus or interme-diate zone separates these two structures, and thepylorus controls the emptying of ingesta from theventriculus into the duodenum. In carnivorous birds,the crop is underdeveloped so the bird relies on thestomach for digestion and as a storage organ. Thesebirds often have a large, thin-walled stomach with apoorly developed isthmus and little distinction be-tween the proventriculus and ventriculus. Theproventriculus tears easily when excessive tension isapplied. The ventriculus is composed of dense muscleand fascia and holds sutures well, but is more diffi-cult to seal with suture and cannot be inverted.
Proventriculotomy is most often indicated for theremoval of foreign objects or toxic materials (such aslead or zinc-containing coins) from the proventricu-lus or ventriculus that cannot be retrieved using rigidor flexible endoscopes.10 A definitive diagnosis ofneuropathic gastric dilatation requires a ventricularbiopsy, although there are some discussions that bi-opsies of the crop may provide similar information.In an Umbrella Cockatoo that had ingested sticks,the proventriculus was determined to be distendedbased on radiographs.21 The tentative diagnosis ofneuropathic gastric dilatation could not be confirmedby biopsy of the ventriculus. Several pieces of glitterand 72 small green sticks were surgically removed.Although techniques for ventriculotomy have been de-
CHAPTER 41 SOFT TISSUE SURGERY
1121

FIG 41.16 a) A proventriculotomy is indicated in patients with foreign bodies that cannot be removed by lavage or endoscopy. Theproventriculus is approached through a left celiotomy incision site as shown. b) Stay sutures can be placed in the ventriculus (not theproventriculus) to improve control over the position of the organ. c) The incision into the proventriculus should be made with a blade andextended into an avascular area with scissors. Note that stay sutures are used to exteriorize the proventriculus, and the abdomen has beenisolated with moistened gauze pads. (continued next page)
SECTION SIX SURGERY
1122

scribed they are generally avoidedbecause of the vascularity and slowhealing characteristic of this or-gan.1,5,6,10,22
A left lateral celiotomy approach willprovide exposure of the ventriculusand proventriculus (Figure 41.16).The ventral suspensory structuresare bluntly dissected to allow theproventriculus to be retractedcaudally. The proventriculus in somebirds is quite fragile and toothed for-ceps should be avoided. Stay suturesmay be placed in the ventriculus toaid with exteriorization and manipu-lation of the proventriculus. Stay su-tures should not be placed in theproventriculus. The coelomic cavityshould be packed off with moistgauze sponges to prevent contamina-tion of the abdominal cavity withgastric contents.
The isthmus or intermediate zone isidentified as a constriction betweenthe ventriculus and the proventricu-lus. The vessels on the surface of theproventriculus are easily identifiedand avoided. The proventriculotomyincision is initiated at the isthmusand extends orad into the body of theproventriculus. Hemorrhage fromthe cut edge of the proventriculusmay be controlled using radiocoagu-lation. Thumb forceps may be used togently clamp the cut edge to occludethe vessel, allowing it to be identifiedand appropriately coagulated.Proventricular contents should beremoved using suction. Small spoonsor curettes may be used to removesolid contents. A combination of irri-gation and suction is useful to com-pletely evacuate the proventriculusand ventriculus. A small diameterflexible endoscope may be used peros, or through the proventriculotomyto assure that all foreign objects havebeen removed.
The proventriculotomy is closed us-ing a simple continuous appositionalpattern of a fine, synthetic, monofila-
d) Radiosurgical forceps should be used only for controlling hemorrhage and not formaking incisions into viscera. e) Closure is routine, using an inverting suture pattern. 1)esophagus 2) crop 3) proventriculus 4) ventriculus 5) duodenum 6) isthmus 7) stay sutures.
CHAPTER 41 SOFT TISSUE SURGERY
1123

ment, absorbable material over-sewn with a continu-ous or interrupted inverting pattern such as a Cush-ing or Lembert pattern. The inverting pattern shouldextend beyond the actual incision to ensure an ade-quate seal. The closure may be evaluated for leakageusing an orogastric tube to insufflate the proven-triculus with air or sterile saline.
Food and water should be offered in the immediatepostoperative period. The wound strength immedi-ately following suture placement is stronger thanduring the debridement phase of wound healing,which occurs three to five days postoperatively. Un-less one intends to withhold food until woundstrength begins to increase again (the phase of fibro-plasia), fasting for one to two days postoperatively isnot indicated. Incisional leakage of gastric contentsoccurs with some frequency in birds.35 The lack of anomentum may be partially responsible for this com-plication. Meticulous attention to proper closure isvital to prevent leakage. A small, atraumatic needleshould be used with a continuous suture pattern toprovide the best seal. If the proventricular wall ap-pears thin and friable, the potential for postoperativeincisional leakage may warrant placement of a duo-denal feeding tube. This will allow enteral alimenta-tion of the patient while bypassing the gastric incision.
The ventriculus is best approached through aproven-triculotomy incision. The incision in the isth-mus is extended aborad toward the ventriculus. Theopening into the ventriculus can be gently dilated toallow the introduction of instruments appropriate forremoval of ventricular contents. Some surgeons sug-gest that a ventriculotomy (transverse abdominalapproach) is easier than a proventriculotomy (leftlateral approach). The lighter-colored, elliptical areaof the ventriculus, where the muscle is thin and thefibers can be seen to course in a different directionfrom the remainder of the ventriculus, is the locationwhere the incision is made (see Anatomy Overlay).1The incision is made transversely across the musclefibers into the lumen. At closure, sutures must beplaced close together to prevent leakage, because aserosal seal cannot be created by using an invertingsuture pattern.
Intestinal Surgery
Surgery on the intestines may be necessary to repairan accidental enterotomy created during a ventralmidline celiotomy or to debride necrotic bowel secon-dary to constrictions caused by adhesions (see Color14). These cases generally carry a poor-to-grave prog-
nosis. A midline, flap or transverse celiotomy may beappropriate, depending on the location of the lesion.In most circumstances, microsurgical technique isindicated due to the extremely thin nature of theavian intestine. The blood supply to the small intes-tine is via the celiac artery (to the duodenum) and thecranial mesenteric artery (jejunum and ileum). Thetechnique used to anastomose the bowel requiresmicrosurgical manipulation of 6-0 to 10-0 monofila-ment suture on a one-fourth circle atraumatic needle.Typically, six to eight sutures are used for an end-to-end anastomosis in a simple interrupted appositionalpattern. Side-to-side anastomosis may prove to bemore appropriate in birds and is easier to perform.
Intestinal Feeding TubesEnteral feeding tubes may be indicated for a varietyof conditions in which a diseased portion of the ali-mentary tract must be bypassed to provide nutri-tional supplementation to anorectic and debilitatedpatients. A variety of medical and surgical conditionsincluding crop infections, impaction, injury or in-flammation, esophageal perforation or laceration,proventricular dilatation, beak disorders, pharyngealdisorders and any condition resulting in hypophagiaor anorexia places a nutritional demand on the pa-tient that may not be met by oral alimentation.Proper attention to the patient’s nitrogen balancecan make the difference between success and failureof therapy (see Chapters 15 and 40).
A technique for placement of a duodenostomy tubehas been described in domestic pigeons.11 Four of thefive catheterized birds had minor weight loss after 14days of total nutritional support through the enteros-tomy tube (4% to 10%). Within seven days of tuberemoval, all the birds had regained their normalweight.
The catheter is placed through a ventral midlineincision. The ascending duodenum is easily identifiedby its close association with the pancreas (see Anat-omy Overlay). A “through-the-needle” catheter (in-dwelling jugular catheter) is used with the needlepassing first through the left abdominal wall, theninto the descending loop of duodenum. The catheterdiameter should be less than one-third the diameterof the intestine.11 The catheter is advanced throughthe descending and ascending loops of duodenum (4to 6 cm), and the needle is withdrawn from theintestine and body wall. One or two sutures areplaced between the left body wall and the duodenumat the entry site of the catheter to secure the intestineto the body wall and allow a seal to form (monofila-
SECTION SIX SURGERY
1124

ment 5-0 prolene). The midline celiotomy is closedroutinely.
The catheter is secured to the outside left abdominalwall using a “finger trap” technique. The needle isprotected within its “snapguard,” and the snapguardis bent to conform to the contour of the bird’s body.The snapguard is then sutured to the skin to secureit in place. The catheter is brought caudal to the legand under the wing. The excess is coiled and thecatheter is secured to the lateral and dorsal body wallusing two sutures. The catheter is flushed with sa-line to assure patency, and an injection cap is placedto create a sealed system for alimentation.
Once the caloric need is calculated (see Chapter 40),the amount of liquid diet required is calculated basedon the caloric density of the diet (usually 1 ml = 1kcal). A variety of liquid diets is commercially avail-able and their compositions have been described (seeChapter 15).41 The amount should be divided intoequal volumes and injected four to six times daily ata rate of approximately 1 ml/15 seconds to allow theintestine to accommodate the volume. The cathetershould be flushed with water or LRS (1 to 2 ml) beforeand after injection of the diet to prevent plugging.
The catheter should be maintained a minimum offive days to allow a seal to form between the intestineand the body wall.11 If the catheter is dislodged pre-maturely, leakage of intestinal contents may occur.Once the catheter is no longer needed, the finger trapsuture is cut, the catheter removed and the defect leftto heal by second intention.
Hypertonic diets may cause osmotic diarrhea. Dailyweight and biochemistry changes can be used to alterthe volume and content of the liquid diet. Patientsthat have a tendency to disturb the catheter shouldbe fitted with a neck brace.k
Cloacal Prolapse
Cloacopexy is indicated to correct problems withchronic cloacal prolapsing. This condition appears tobe most common in Old World psittacine birds, espe-cially cockatoos, and is associated with reducedsphincter tone. Chronic gram-negative enteritis maybe an initiating factor,2 underscoring the need forcloacal cultures as part of the patient evaluationprocess. The attachments of the cloaca are damaged,allowing the entire structure to prolapse, which maycause occlusion of the ureters and colon. Minor pro-lapses may respond to placement of a mattress su-
ture on either side of the cloaca; however, when theentire organ prolapses, this method of treatment isineffective. If mattress sutures are used, they mustallow for the passage of droppings. An alternativemethod involves the placement of two sutures trans-versely across the vent. These must be placed closeenough together to prevent recurrence of the pro-lapse, but far enough apart to allow the normal pas-sage of droppings. These sutures may be left in placefrom a few days to several weeks depending on theclinical situation. Purse-string sutures are contrain-dicated due to frequent postsurgical cloacal atonysecondary to nerve damage.
A percutaneous cloacopexy may be performed as atemporary or definitive treatment for cloacal pro-lapse.33 The prolapse is reduced using a moistenedcotton-tipped applicator. The applicator is main-tained within the cloaca to help identify its limits,and two or three sutures are placed percutaneouslythrough the skin, body wall and urodeum. The su-tures should be removed in two to four weeks. Thisprocedure carries the risk of inadvertently entrap-ping or perforating the ureters, rectum, duodenumand pancreas.
In some cases, prolapse is due to atony of the ventsphincter. This condition may be treated by surgi-cally narrowing the vent opening. One-half to three-fourths of the margin of the circumference of the ventis incised to provide a cut surface for healing. Simpleinterrupted sutures are placed from one side of thevent to the other in order to partially close the open-ing. This will decrease the size of the vent openingpermanently, preventing prolapse of the cloaca.
A rib cloacopexy is an effective treatment for severecloacal prolapse.47 A ventral midline celiotomy is per-formed and the cloaca is identified (Figure 41.17).This approach provides exposure to the entire cloacaand its associated structures. It may be necessary touse a moistened cotton-tipped applicator or the fin-ger of a gloved assistant to reduce the prolapse anddefine its limits intraoperatively. Fat on the ventralsurface of the cloaca should be excised. This appearsto be crucial for a successful surgery.48 The ribs arepushed caudally using the thumb, and the surgicalincision is elevated with the index finger, bringingthe ribs into view to facilitate suture placement. Asuture is placed around the last rib on each side ofthe bird and passed through the full thickness of theventral aspect of the craniolateral extent of theurodeum. The suture should be tied with enoughtension to slightly invert the vent. Large sections of
CHAPTER 41 SOFT TISSUE SURGERY
1125

FIG 41.17 A rib cloacopexy is indicated to permanently correct chronic cloacal prolapse. a) The cloaca is pushed cranially with a moistenedcotton-tipped applicator and sutures are placed between the cranio-lateral border of the cloaca and the eighth rib. b) Pushing the eighthrib caudally with a finger will help in the placement of sutures. c) Lateral view of the cloacopexy procedure showing the placement of thesuture between the cloaca and the eighth rib, and the suturing of the cloaca to the abdominal wall during closure. 1) eighth rib 2) skinincision 3) cloaca 4) vent 5) swab 6) intestines and 7) pubis.
SECTION SIX SURGERY
1126

tissue must be used for suture placement, and itappears to be important to penetrate the cloacallumen. Several other sutures are then placed be-tween the body wall and the wall of the cloaca. Thecloaca may be sutured to the caudal border of thesternum instead of the ribs, if the rib sutures placeexcessive inverting tension on the cloaca. This proce-dure may not be effective in birds with a thin-walledcloaca.
Another method for performing a cloacopexy hasbeen described.23 A 2 to 5 mm incision is made in theserosal surface of the coprodeum parallel to its lengthand 5 to 10 mm from the midline (Figure 41.18). Acorresponding paramedian incision is made in theperitoneal surface of the body wall at a point that willmaintain the cloaca in a position that will result inslight inversion of the vent. Three or four sutures areplaced between each side of the two incisions suchthat the serosal surfaces are sutured and the subse-rosal surfaces of the two structures are apposed. Thisprocedure is repeated on the contralateral parame-dian side.
Alternatively, a routine ventral midline incision maybe made, the cloaca reduced and the associated fatexcised. The abdomen is closed incorporating thecloaca. The suture passes through one side of thebody wall, through the full thickness of the cloacaand through the other side of the body wall in a
simple interrupted pattern (Figure 41.19). Skin isclosed over this layer.
A transverse abdominal cloacopexy may providemore even distribution of tension than a ventralmidline approach.2 The transverse incision is made
FIG 41.18 An alternative cloacopexy technique is to make a ventral midline incision and place three or four sutures that appose thesubserosal surfaces of the cloaca and internal body wall. 1) cloacal wall 2) pleuro-peritoneum 3) seromuscular layer of the cloaca and 4) body wall.
FIG 41.19 A simple cloacopexy technique that involves full-thick-ness suturing of the cloaca into a ventral midline incision may beeffective in resolving mild cases of cloacal prolapse. 1) cloacal wall2) body wall and 3) peritoneal cavity.
CHAPTER 41 SOFT TISSUE SURGERY
1127

through the skin and abdominal musculature in thepostventer region. The cloaca is incised to the level ofthe submucosa, and the seromuscular layer is thensutured to the incision in the abdominal wall. Theabdomen and skin are closed routinely.
Surgery of theReproductive Tract
Surgery on the female reproductive tract is mostoften indicated in cases of egg binding, ectopic ovula-tion, soft-shelled eggs, congenital atresia of the ovi-duct, damage to the uterus, salpingitis, neoplasia,abnormal egg production, biopsy and culture of theoviduct and egg-related peritonitis.8,14,24,42,48,57 Gener-ally, only the left side of the female reproductive tractis functional. The right oviduct may become cystic inolder fowl,43 and this condition has been reported ina budgerigar (see Color 29).18 A left lateral flap orventral midline celiotomy approach may be used,depending upon which portion of the reproductivetract is to be evaluated.
Egg Binding
Egg binding occurs commonly in companion birdsand has been associated with a genetic predisposi-tion, improper nutrition, atony of the uterus, over-sized eggs, inexperience of the hen, tumors of thereproductive tract and extraluminal compression ofthe reproductive tract by abdominal masses.14,18,34,48,53
In one case of egg binding, a cystic right oviduct wascompressing the left reproductive tract, preventingnormal migration of the egg.18 Both oviducts weresuccessfully removed, relieving the dystocia. In anIsle of Pines Amazon Parrot, an oviduct defect al-lowed deposition of uncalcified eggs into the abdomi-nal cavity. Five eggs were successfully removed fromthe coelom. A hysterectomy was performed after twomore eggs were deposited into the abdomen andsurgically removed the following year.57
Egg binding in birds is most commonly the result ofmalnutrition. If the egg remains in the uterus (shellgland), it will continue to deposit shell material ontothe egg, further lowering systemic calcium levels.Any bird presenting for egg binding should be evalu-ated for hypocalcemia prior to planning surgery, and
any abnormalities should be addressed. Medicalmanagement including ovocentesis should be at-tempted prior to considering surgical intervention.
Prolapse of oviduct or uterine tissue occurs withsome degree of frequency in egg-bound birds, espe-cially budgerigars and cockatiels.47,48 It may occurfollowing egg binding or from straining. The tissuemay have been expelled through the vaginal openinginto the cloaca and potentially externalized throughthe vent. As the tissue protrudes through the cloaca,it undergoes axial torsion, making it difficult to iden-tify the lumen. Exposed uterine tissue becomes dryand necrotic within 30 to 60 minutes.
OvocentesisIf medical management of egg binding fails, ovocen-tesis and collapsing the egg may be successful. Undergeneral anesthesia, the opening of the vagina intothe cloaca is identified. A blunt probe is used to dilatethe opening. Once the egg is visualized, a needle canbe inserted into the egg to aspirate its contents.Following ovocentesis, the egg can be collapsed andthe shell fragments removed (see Chapter 29). Thevagina and uterus should be flushed repeatedly toverify that all egg material has been evacuated. It isprudent to reconstruct the egg to be certain that allshell fragments have been retrieved. Alternatively, aradiograph may be valuable to rule out the presenceof another egg or remaining fragments.
If the lumen is not identifiable, the prolapsed tissuemay be incised to deliver the egg. Once the egg isremoved, the layers of uterine wall should be suturedwith a fine (6-0 to 10-0) monofilament, absorbablematerial on an atraumatic needle in a simple apposi-tional or inverting pattern. If the patient’s conditionpermits, necrotic tissues should be excised and viabletissues reconstructed. With critical patients, thedamaged tissue should be replaced into the cloacaafter removal of the egg, and debridement should bepostponed until the patient’s condition improves. Ifan egg or shell fragments remain in the oviduct, aceliotomy is indicated.
If the egg is near or within the pelvic canal, it may bedelivered using an episiotomy-type incision.33 Theincision is made on the ventral midline through thecloacal sphincter extending craniad through theurodeum. If necessary, the incision may extend intothe uterus. After the egg is removed, the uterus andcloaca are closed with a simple interrupted or simplecontinuous pattern of a slowly absorbable material.Closure of the body wall and skin are routine. This is
SECTION SIX SURGERY
1128

a radical procedure and is indicated only in criticalcases in which the hen is likely to die or the egg is ofmajor importance for species propagational purposes.
In cases where the egg is lodged farther cranial in theoviduct, it may be best to perform a midline celio-tomy, and hysterotomy may be the best technique forremoving the egg. The hysterotomy incision shouldbe closed with a simple appositional continuous orinverting pattern of a fine monofilament syntheticabsorbable material. Postoperatively, hormone ther-apy or photoperiod regulation should be used to pre-vent subsequent laying until the hysterotomy hashealed. If hysterectomy is indicated, a left lateralapproach is preferred to gain access to the entireoviduct.
Salpingohysterectomy
This procedure involves removal of both the uterus(shell gland) and the oviduct; therefore, the termsalpingohysterectomy is most appropriate. Althoughhysterectomy is the term commonly used to refer tothis procedure, the ovary is not removed. Salpingo-hysterectomy is indicated to terminate pathologicegg laying, alleviate egg binding, remove an infectedor ruptured oviduct and to treat a prolapsed oviductand recurring egg-related peritonitis.
Salpingohysterectomy carries a significant degree ofrisk and is generally not recommended as a preven-tive measure. Although cockatiels continue to havecopulatory, nesting, territorial and egg-laying behav-ior following salpingohysterectomy, there is no evi-dence that problems related to the deposition of yolksinto the abdomen occur.14,34 Presumably, a hormonalfeedback loop from the uterus to the ovary preventsfollicular development and release of ova.15,33,48 In aretrospective study of 30 birds on which salpingohys-terectomy was performed, five were evaluated la-paroscopically several months postoperatively.34 Fol-licular development was noted; however, no largefollicles were observed. Continued yolk release withsubsequent yolk-related peritonitis was reported in aCalifornia Quail and a duck following routine salpin-gohysterectomy.48
The size of the oviduct and uterus varies with thereproductive and physiologic status of the patient.The reproductive tract of a cockatiel that is not inbreeding condition is narrow (2 to 3 mm). A bird inpoor condition may also have a small, inactive ovary.A young bird in good condition with exposure to a
male may have a well developed ovary with largefollicles and a large reproductive tract.
Salpingohysterectomy may be accomplished througha left lateral celiotomy (Figure 41.20). The ovary maybe visualized following lateral and ventral retractionof the proventriculus. The oviduct and uterus lieconvoluted along the dorsal aspect of the body cavity.The oviduct is identified and elevated away from thelarge caudal vena cava. Minor damage to this vesselwill result in life-threatening hemorrhage. The ven-tral ligament causes the convolutions in the uterusand oviduct. The ligament courses caudally and col-lects as a muscular cord at the vagina. There are novessels in this ligament, and it should be dissected toallow the oviduct and uterus to be stretched into alinear configuration.
The fibria of the infundibulum lie caudal to the ovaryand may be elevated to expose the dorsal attach-ments. At the base of the infundibulum and coursingcaudally along the uterus, the dorsal ligament sus-pends the uterus and a branch of the ovarian artery.A small blood vessel can be identified coursing fromthe ovary through the infundibulum. This vesselshould be coagulated or a hemostatic clip should beapplied to control hemorrhage. If it is inadvertentlytransected or broken, it will retract under the ovaryin a virtually unretrievable location. A small piece ofabsorbent gelatin spongeg may be packed against theovary to achieve hemostasis. The remainder of thissuspensory structure may then be dissected with thebipolar radiosurgical forceps.
Once the infundibulum is free, the oviduct is re-tracted ventrally and caudally, exposing the dorsalsuspensory ligament. Several small blood vessels,branches of the ovarian artery, can be seen in thisstructure perpendicular to the oviduct and uterus.These should be identified and coagulated. Each vas-cular stump should be inspected for residual hemor-rhage before closure. As this dissection is continuedcaudally toward the cloaca, the ureter can be identi-fied as a white tubular structure extending from thekidney to the cloaca. This structure should beavoided. As the dissection approaches the cloaca, theuterus courses along with the terminal colon andenters the cloaca (see Anatomy Overlay). The uterusshould be ligated at its junction with the vagina byplacing one or two hemostatic clips a short distancefrom the cloaca. In cases where the vaginal tissue hasbeen damaged, the clips may be applied at the cloaca,being careful not to entrap the ureter. The clipsshould be secure with the entire width of the uterus
CHAPTER 41 SOFT TISSUE SURGERY
1129

SECTION SIX SURGERY
1130

within the clips to prevent leakage. If the clips be-come dislodged or do not completely occlude theuterus, feces and urates may reflux into the abdomen.
Egg-related Peritonitis
Egg-related peritonitis occurs most commonly incockatiels, budgerigars, lovebirds, ducks, gallina-ceous birds and macaws (see Color 29).48 Diagnosis ismade by clinical signs, hematology, radiography, ab-dominocentesis and laparotomy. A severe inflamma-tory response is typical of the hemogram.
Mild cases may respond to antibiotic therapy andsupportive care (see Chapter 29). Surgical interven-tion is usually necessary to resolve severe cases.33,48
In some cases, surgery should be postponed and thepatient treated medically until the condition stabi-lizes. A ventral midline celiotomy is preferred be-cause fluids are easily drained out the incision ratherthan down into the air sacs, and potentially into thelungs. Once the celiotomy is performed, the intes-tines should be retracted using moistened cotton-tipped applicators or other suitable atraumatic in-struments. Any yolk or tissue debris should beremoved. The cavity should be copiously irrigatedprior to closure. Implantation of Penrose drains maybe indicated in some cases, but do not generallyprovide adequate coelomic drainage. This conditionwarrants a guarded-to-poor prognosis. Birds that re-cover frequently have abdominal adhesions, disten-tion and muscular dysfunction.
Removal of the Gonads
Carbon dioxide laser destruction of gonadal tissuehas been attempted; however, the procedure is verytime-consuming and costly, and controlling damageto surrounding tissues, especially the adrenals, isvery difficult. Removal of the gonads with laser incompanion birds is often followed by severe hemor-rhage either intraoperatively or postoperatively.
Alternatively, the vascular supply to the ovary maybe destroyed using vascular clips, but this is a diffi-
cult procedure, performed without being able to visu-alize vital structures. Microsurgical equipment isessential. Clients should be informed that this proce-dure is extremely difficult and the possibility of com-plications is higher. The patient should be treatedmedically to reduce the size of the ovary and improvevisualization. Through a left lateral celiotomy, theovary is identified. A hemostatic clip is applied dorsalto (under) the ovary to occlude all ovarian vessels. Insmall birds, one clip applied from a caudal to cranialdirection is adequate. Two clips, one from a cranialdirection and the other from a caudal direction, maybe required for large birds. Angled appliers should beused to place the clips under the ovary parallel to thespine, which reduces the possibility of inadvertentlyentrapping the aorta or peripheral nerves.
Orchidectomy
Neutering a male is theoretically easier than neuter-ing a female because the testicles are not as adherentto deeper structures as the ovary, making clip appli-cation easier and safer. However, orchidectomy mustbe performed bilaterally, making a ventral approachmore applicable than a left lateral approach. Theplacement of vascular clips is similar to that de-scribed for the ovary. Orchidectomy in companionbirds is extremely difficult and many birds do notsurvive the surgery.
A technique for orchidectomy in ostriches has beendescribed.49 The procedure is indicated to controlaggressive behavior in birds that present a danger tokeepers, handlers, the public or other birds. Thesurgical approach is through the costal notch andlumbar fossa on each side. The skin and body wall areincised adequately to allow introduction of a glovedhand. The testicle on the corresponding side is pal-pated, grasped and twisted until it is torn from anyattachments. It is recommended that the procedurebe performed at the onset of breeding season whenthe testicles have begun to increase in size so theycan be easily located. If performed during the breed-ing season, excessive hemorrhage may result fromavulsion of the hypertrophied testicular vascularsupply. Body wall, subcutaneous tissue and skin areclosed routinely. The procedure can be accomplishedthrough a single, lateral celiotomy incision if thesurgeon has hands small enough to reach through tothe contralateral testicle. Minor postoperative sub-cutaneous emphysema and occasional incisional de-hiscence are the only reported complications.
FIG 41.20 (opposite) a) A salpingohysterectomy is performedthrough a left lateral celiotomy incision and is indicated to termi-nate pathologic egg laying and to prevent egg-related peritonitissecondary to a diseased oviduct. b) Regional anatomy for salpin-gohysterectomy. c, d) Hemostatic clips are shown passing througha left lateral celiotomy incision to provide a more realistic impres-sion of the visibility through the incision site. 1) eighth rib 2)proventriculus 3) lung 4) aorta 5) ovary 6) kidney 7) ureter 8)suspensory ligament of oviduct 9) cloaca 10) rectum 11) infundibu-lum 12) oviduct 13) celiotomy incision and 14) hemostat clip.
CHAPTER 41 SOFT TISSUE SURGERY
1131
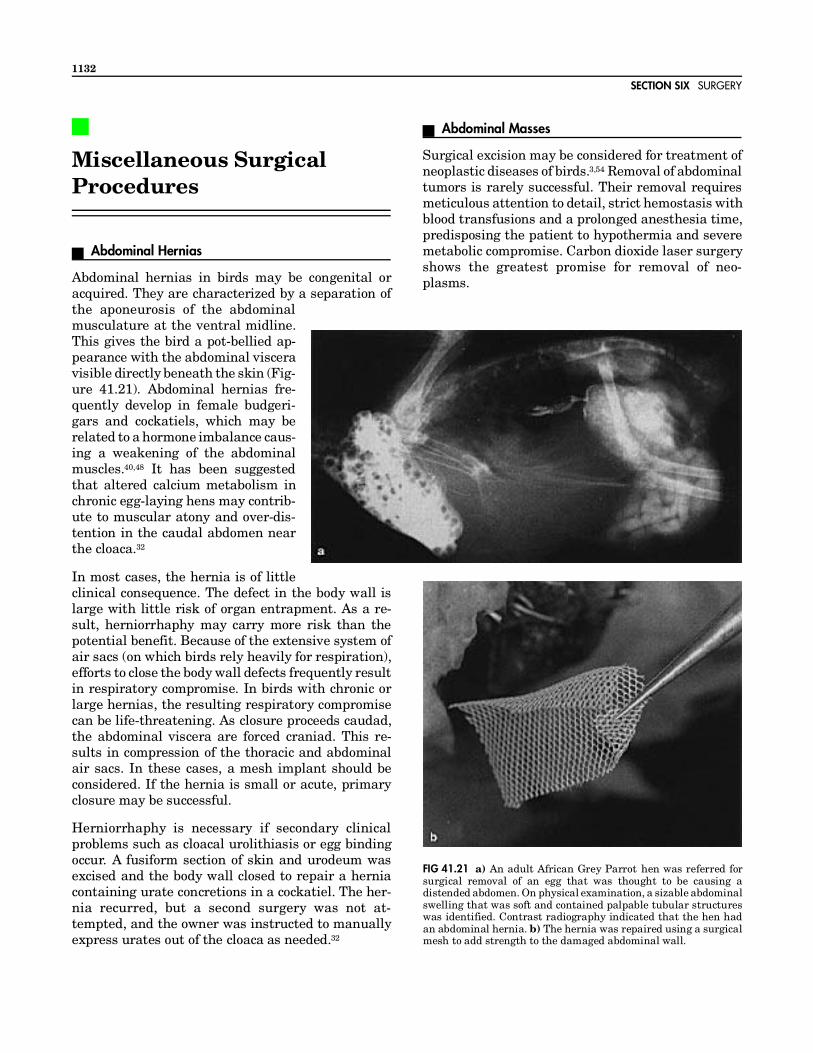
Miscellaneous SurgicalProcedures
Abdominal Hernias
Abdominal hernias in birds may be congenital oracquired. They are characterized by a separation ofthe aponeurosis of the abdominalmusculature at the ventral midline.This gives the bird a pot-bellied ap-pearance with the abdominal visceravisible directly beneath the skin (Fig-ure 41.21). Abdominal hernias fre-quently develop in female budgeri-gars and cockatiels, which may berelated to a hormone imbalance caus-ing a weakening of the abdominalmuscles.40,48 It has been suggestedthat altered calcium metabolism inchronic egg-laying hens may contrib-ute to muscular atony and over-dis-tention in the caudal abdomen nearthe cloaca.32
In most cases, the hernia is of littleclinical consequence. The defect in the body wall islarge with little risk of organ entrapment. As a re-sult, herniorrhaphy may carry more risk than thepotential benefit. Because of the extensive system ofair sacs (on which birds rely heavily for respiration),efforts to close the body wall defects frequently resultin respiratory compromise. In birds with chronic orlarge hernias, the resulting respiratory compromisecan be life-threatening. As closure proceeds caudad,the abdominal viscera are forced craniad. This re-sults in compression of the thoracic and abdominalair sacs. In these cases, a mesh implant should beconsidered. If the hernia is small or acute, primaryclosure may be successful.
Herniorrhaphy is necessary if secondary clinicalproblems such as cloacal urolithiasis or egg bindingoccur. A fusiform section of skin and urodeum wasexcised and the body wall closed to repair a herniacontaining urate concretions in a cockatiel. The her-nia recurred, but a second surgery was not at-tempted, and the owner was instructed to manuallyexpress urates out of the cloaca as needed.32
Abdominal Masses
Surgical excision may be considered for treatment ofneoplastic diseases of birds.3,54 Removal of abdominaltumors is rarely successful. Their removal requiresmeticulous attention to detail, strict hemostasis withblood transfusions and a prolonged anesthesia time,predisposing the patient to hypothermia and severemetabolic compromise. Carbon dioxide laser surgeryshows the greatest promise for removal of neo-plasms.
FIG 41.21 a) An adult African Grey Parrot hen was referred forsurgical removal of an egg that was thought to be causing adistended abdomen. On physical examination, a sizable abdominalswelling that was soft and contained palpable tubular structureswas identified. Contrast radiography indicated that the hen hadan abdominal hernia. b) The hernia was repaired using a surgicalmesh to add strength to the damaged abdominal wall.
SECTION SIX SURGERY
1132

Lipomas
Lipomas are frequently the expression of obesity.Central necrosis and ulceration may occur. Somelipomas are covered by xanthomatous skin. Effortsshould be made to reduce the size of the mass medi-cally before attempting surgical extirpation. Dietand exercise are effective over a period of severalmonths. Lipomas are generally well encapsulatedand shell out easily.
Leg Amputation
When a leg must be amputated, it is best performedat mid-femur. If the stump is too long, the bird maycontinue to use it for ambulation, causing traumaand granuloma formation to the stump. A mid-femo-ral amputation allows adequate soft tissue coverageof the end of the bone and prevents the patient fromtraumatizing the surgical site. Because the majorityof the femur is contained within the skin of the bodywall, a mid-femoral amputation is also cosmetic.Most companion birds with one leg are able to func-tion normally. Psittacine birds compensate particu-larly well because they use their beak as an aid toambulation. Pododermatitis of the contralateral foot,as occurs commonly in raptor amputees, is rarely aproblem in companion birds on a formulated diet.
The skin incision should be made along the knee webto conform to the contour of the abdomen. A semicir-cular incision is created both medially and laterallyat about the level of the stifle. This will allow ade-quate skin for tension-free closure. The musclesshould be transected at the stifle. Use of the radio-scalpel will aid in hemostasis. The muscles are ele-vated from the femur to the mid-diaphyseal regionusing a periosteal elevator. The ischiatic nerveshould be injected with lidocaine or bupivacaine priorto transection for temporary postoperative analge-sia. The femur may be cut with a bone cutter, anosteotome, a gigli wire, a sagittal saw or other suit-able instruments appropriate for the patient’s size.Following the osteotomy, the muscles are suturedover the end of the bone to provide padding. Subcu-taneous tissues and skin are closed routinely.
Toe Amputation
Indications for toe amputation include avascular ne-crosis, trauma and infection. Hemostasis is aided bythe use of a tourniquet. Hemostatic agents should beavoided. The heavily keratinized scale surfaces maybe gently debrided exposing the more supple epider-
mis below. This improves tissue handling for sutureplacement. The site of amputation should be at thejoint proximal to the affected area. The skin shouldbe incised distal to the joint to provide adequate skinfor closure (Figure 41.22). A hydroactive dressing willpromote healing and prevent contamination (seeChapter 16).
Wing Amputation
Amputation of the humerus at the junction of themiddle and proximal thirds of the bone providesadequate soft tissue coverage and creates a stumpshort enough to prevent self trauma. The skin inci-sion should be made at the distal humerus, justproximal to the elbow. If additional skin is needed forclosure, the patagium may be utilized. The musclesare transected at their musculotendinous junctionsnear the elbow. The radial and medianoulnar nervesshould be injected with lidocaine or bupivacaine forshort-term postoperative analgesia prior to theirtransection. Brachial musculature is mobilized byblunt dissection to remove attachments from thehumerus. The humerus should be transected at theproximal third, to provide sufficient muscle distallyto be sutured over the stump. Subcutaneous and skinclosure are routine.
In situations where use of the wing for balance isimportant, it may be beneficial to amputate as dis-tally as possible.19,39 This function is especially im-portant when working with birds to be used in breed-ing programs and as surrogate parents. It may bedifficult to obtain adequate soft tissues for stumpcoverage with distal amputations.
Vascular Access Devices
In avian patients, intravenous catheters are viableonly for short-term therapies. Avian veins are rela-tively small, thin-walled and fragile, with a propen-sity for hematoma formation following venipuncture.The intraosseous placement of a needle provides ac-cess to the vascular space for administration of fluidsand therapeutics for up to 72 hours. Vascular accessdevices provide a route for long-term administrationof therapeutics into the vascular system.8,17 Theyhave been used for long-term administration of am-photericin B in a Cassins Auklet17 and MagellanicPenguins and for total parenteral nutrition in pigeons.8
Vascular access devices are subcutaneously im-planted devices with a reservoir that is accessedthrough surgically prepared skin using a non-coring
CHAPTER 41 SOFT TISSUE SURGERY
1133

needle (Huber point needle). Risk of sepsis andthrombosis is minimized because the catheter is notexposed to the environment. These have been main-tained in humans for years and in birds for up to 12weeks.17 Vascular access devices have a number ofsynonyms, some of which are proprietary names,such as portacath, infusaport, dome, vascular accessport and subcutaneous port.
The material, construction, surface finish and tipconfiguration influence the thrombogenicity of thecatheter. Silicone and hydromer-coated polyurethaneare considered the least thrombogenic materials cur-rently in use. The catheter can be implanted into avein, artery or other hollow organ and connected tothe reservoir.
The right jugular vein is the preferred site for im-plantation. The patient is positioned in left lateral
recumbency, and the area over the right jugular veinis prepared for surgery. In many avian patients,there is no need to remove feathers because there isan apterium in this location. The skin is moved dor-sally and an incision is made over the jugular vein.When the skin is released, the incision site will beventral to the jugular vein and not over the reservoir.The jugular vein is identified and isolated for a dis-tance of approximately 15 mm. Dissection must pro-ceed cautiously as the vein is very fragile. Two liga-tures are placed around the vein, one at the cranialextent and the other at the caudal extent of theisolated area. The caudal suture is elevated to oc-clude blood flow. The jugular vein will distend andthe cranial suture is then tied off permanently oc-cluding jugular flow. This does not seem to affectcerebral hemodynamics.
FIG 41.22 Two techniques may be used for toe amputation: a,b) The skin may be incised, creating a semicircular flap on both the dorsaland the plantar surfaces of the digit. This skin pattern will provide adequate tissue for closure over the distal end of the bone. c,d)Alternatively, the plantar skin may be incised to create a flap of plantar skin that will cover the end of the bone. The plantar skin is somewhatstronger than the dorsal skin, providing additional protection over the end of the bone. Because the metaphysis and epiphysis of thephalanges are larger than the diaphysis, it may be beneficial to remove the exposed joint surface with rongeurs prior to skin closure. Theskin is sutured as described for the repair of toe necrosis (see Figure 41.1).
SECTION SIX SURGERY
1134

At this point, a small segment of the jugular veinremains distended. Using fine iris scissors and mag-nification, a transverse venotomy is created in thedistended portion of the vein. This incision will nottransect the vein but will allow the catheter to beinserted. After the blood from the distended segmentis cleared, the end of the catheter is inserted into thevenotomy site. The tension on the caudal ligaturewill have to be loosened to allow the catheter to pass,but enough tension should be maintained to preventreflux hemorrhage. The venotomy may be widenedusing fine forceps or a vascular introducer. Thecatheter is advanced to the right atrium and securedin place by suturing above and below the retentionring at the venotomy site to prevent the catheterfrom advancing or backing out.
A Huber needle attached to a three-way stopcock anda saline-filled syringe is used to test the ease ofinjection and withdrawal of a sample. The position ofthe catheter tip should be evaluated using contrastradiography. Some catheters are radiopaque. Withthose that are radiolucent, the position can be evalu-ated by injecting a vascular contrast medium.
A subcutaneous pocket is created dorsal to the jugu-lar vein large enough to accommodate the reservoir,which is placed into the pocket and sutured in placeto the fascia of the neck musculature. A 2 to 4 cm loopof catheter is left to allow for neck movements. Sub-cutaneous and skin closure are routine. During re-covery, feathers over the reservoir should be removedand the skin aseptically prepared. The device shouldthen be filled with heparin at 100 IU/ml. Only non-coring needles should be used with these devices.With a minimal amount of practice, these devices canbe implanted in 10 to 15 minutes.
The skin area above the port must be asepticallyprepared before each use. Chlorhexidine has beenshown to be three to four times more effective atpreventing bacterial colonization of the catheter thanpovidone iodine.17 The individual administering thetherapy should wear sterile gloves and use sterileequipment. The non-coring needle is inserted intothe reservoir until it hits the base plate and theinjection can then be made.
These devices can be maintained for extended peri-ods of time but require some maintenance.17 Cathe-ters were maintained in chickens for 12 weeks usinga 1000 IU/ml heparin lock and weekly flushing. Ingeese, the catheters were flushed every four dayswith 1.0 ml physiologic saline and locked with 0.25
ml heparin at 100 IU/ml. When catheters are useddaily or several times daily, there is no need forheparin locks, which eliminates the potential forheparinizing the patient. However, there is a higherpotential for thrombus formation with small gaugecatheters, and a heparin lock may still be necessary.17
Removal of the device requires a surgical approach tothe vein and the reservoir. The sutures holding thereservoir are removed as is the suture holding thecatheter in the vein. A ligature is pre-placed aroundthe vein and the catheter is removed. The ligature istightened to prevent reflux of blood. Closure of theskin and subcutaneous tissues is routine.
Perinatal Surgery
Many aviculturists do not seek veterinary assistancewith embryonal and neonatal matters, attempting tomanage problems themselves. Rarely are these at-tempts successful. Neonatal tissues are challengingto suture. Compared with adult tissues, they have ahigh moisture content, making them very friable,with reduced tensile strength. With practice andmanagement, fine suture (8-0 to 10-0) and an atrau-matic needle can be used for closure of the umbilicus.However, hemostatic clips are more appropriate forapplication to the umbilicus than suture ligatures.Featherless neonates are highly prone to developinghypothermia. Anesthesia and surgery time should beless than 15 minutes, and the operating room tem-perature should be elevated to 75 to 85°F.1 Bodytemperature should be carefully monitored through-out the procedure, and supplemental glucose shouldbe provided through an intraosseous cannula asnecessary.
Because of their small blood volume, perinatal pa-tients are more likely to require transfusion if majorblood loss occurs or if the hematocrit is below 20 to25%. Respiratory movements may be difficult to ob-serve in perinatal patients, making the use of cleardrapes and small non-rebreathing bags essential.The crop of altricial avian neonatal patients is usu-ally full, increasing the risk of regurgitation andaspiration. The patient may be fasted until the cropvolume has diminished or the contents may be re-moved by aspiration. Elevating the head and packingthe thoracic esophagus with moist cotton will alsohelp prevent reflux of crop contents.
Yolk Sac RemovalThe yolk sac is a diverticulum from the small intes-tine attached by the yolk stalk and accompanying
CHAPTER 41 SOFT TISSUE SURGERY
1135

vasculature. It is normally internalized prior tohatching. Yolk is absorbed during incubation throughthe endodermal cells of the yolk sac and, at least inchickens, nutrients are absorbed through a duct thatconnects the yolk stalk to the intestines. Yolk pro-vides nourishment, minerals, fat-soluble vitaminsand maternal antibodies to the developing embryoand the neonatal bird. After the yolk has been com-pletely absorbed, the remnant of the yolk sac be-comes the vitelline or Meckel’s diverticulum.
A procedure for removal of unabsorbed yolk sacs hasbeen successful in decreasing mortality in affectedchicks (see Chapter 48). Candidates for surgery demon-strate one or more of the following clinical signs: ab-dominal distention, exercise intolerance or dyspnea,weight loss and anorexia, failure to grow or inability tostand or walk. Abdominal palpation and radiographysupport the diagnosis of unabsorbed yolk sac. Radiog-raphically, the yolk mass displaces the viscera craniallyinto the thoracic space, compromising the caudal air
sacs. This results in exercise intolerance and dysp-nea. Yolk sac removal is most effective if performedbefore the chick becomes dyspneic. Percutaneous as-piration of the yolk should not be attempted as theyolk sac is very thin and will leak yolk into thecoelomic cavity resulting in peritonitis. Injecting an-tibiotics directly into the yolk sac carries the samerisk. Systemic antibiotics are not effective alone.26
Products Mentioned in the Texta. Lorelco, Merrell Dow Pharmaceuticals Inc., Cincinnati, OHb. Mucomyst, Mead Johnson, Evansville, INc. Maxitrol ophthalmic ointment, Alcon Laboratories,
Fort Worth, TXd. Vetalog, Solvay Animal Health, Mendota Heights, MNe. Jardon Eye Prosthetics Inc., Southfield, MIf. Moto-tool, Dremel, Racine, WIg. Gelfoam, Upjohn Co, Kalamazoo, MIh. McAllister Technical Services, Coueur d’Alene, IDi. Bard Urological Division, CR Bard, Murray Hill, NJj. Norfolk Medical Products, Access Technologies, Skokie, ILk. Avian Restraint Collar, Vet Specialty Prod., Boca Raton, FL
References and Suggested Reading
1. Altman RB: Avian neonatal and pedi-atric surgery. Sem Avian Exotic PetMed 1(1):34-39, 1992.
2.Avgeris S, Rigg D: Cloacopexy in a sul-phur-crested cockatoo. J Am AnimHosp Assoc 24:407-410, 1988.
3.Bauck L: Radical surgery for thetreatment of feather cysts in the ca-nary. AAV Today 1(5):200-201, 1987.
4.Bond MW: Avian pediatrics. Proc As-soc Avian Vet, 1991, pp 153-160.
5.Bush M, Kennedy S: Ventriculostomyfor removal of foreign bodies fromsaurus cranes. J Am Vet Med Assoc173:1107-1110, 1978.
6. Calle PP, Ensley PK: What is your di-agnosis? J Am Vet Med Assoc189:1230-1231, 1986.
7.Clubb SL, Karpinski L: Aging in ma-caws. Proc Assoc Avian Vet, 1992, pp83-86.
8.Degernes LA, et al: Preliminary re-port on the use of total parenteral nu-trition in birds. Proc Assoc Avian Vet,1992, pp 19-20.
9.Doster GL: Aspirated corn kernelscause death of cannon-netted wildturkeys. J Wildl Manag 38:578, 1974.
10.Gasthuys F, DeMeurichy W: Success-ful ventriculostomy for removal of for-eign bodies in a kiwi (Apteryx austra-lis mantelli). J Zoo Anim Med18(4):166-167, 1987.
11.Goring RL, et al: Needle catheter duo-denostomy: A technique for duodenalalimentation of birds. J Am Vet MedAssoc 189:1017-1019, 1986.
12.Harris JM: Teflon dermal stent forthe correction of subcutaneous em-physema. Proc Assoc Avian Vet,1991, pp 20-21.
13.Harrison GJ: Initial treatment of se-vere crop wounds. J Assoc Avian Vet5(3):126, 1991.
14.Harrison GJ: Reproductive medicine.In Harrison GJ, Harrison LR (eds):Clinical Avian Medicine and Surgery.Philadelphia, WB Saunders Co, 1986,pp 625-626.
15.Harrison GJ: Selected surgical proce-dures. In Harrison GJ, Harrison LR(eds): Clinical Avian Medicine and
Surgery. Philadelphia, WB SaundersCo, 1986, pp 577-595.
16.Harrison GJ: Surgical repair of cropinjuries. AAV Today 1(2):63, 1987.
17.Harvey-Clark C: Clinical and researchuse of implantable vascular accessports in avian species. Proc AssocAvian Vet, 1990, pp 191-209.
18.Hochleithner M, Lechner C: Egg bind-ing in a budgerigar (Melopsittacus un-dulatus) caused by a cyst of the rightoviduct. AAV Today 2(3):136-138,1988.
19.Howard PE, et al: Surgical removal ofa tracheal foreign body from a whoop-ing crane (Grus americana). J ZooWildl Med 22(3):359-363, 1991.
20.Hunter RB, Taylor M: Lung biopsy as adiagnostic technique in avian medi-cine. Proc Assoc Avian Vet, 1992, pp207-211.
21.Ingram I: Proventricular foreign bodymimicking proventricular dilatationin an umbrella cockatoo. Proc AssocAvian Vet, 1990, pp 314-315.
22.Jacobson ER, et al: Ventriculostomyfor removal of multiple foreign bodiesin an ostrich. J Am Vet Med Assoc189(9):1117-1119, 1986.
23.Jenkins JR: Avian soft tissue surgery:Part I. Proc American College of Vet-erinary Surgeons, 1992, pp 631-633.
24.Jenkins JR: Avian soft tissue surgery:Part II. Proc American College of Vet-erinary Surgeons, 1992, pp 634-636.
25.Joyner KL: Pediatric therapies. ProcAssoc Avian Vet, 1991, pp 188-198.
26.Kenny D, Cambre RC: Indications andtechnique for the surgical removal ofthe avian yolk sac. J Zoo Wildl Med23(1):55-61, 1992.
27.Kern TJ, et al: Lens extraction by pha-coemulsification in two raptors. J AmVet Med Assoc 185(11):1403-1406,1984.
28.Kosloske AM: The Fogarty balloontechnique for removal of foreign bod-ies from the tracheobronchial tree.Surg Gyn Obs 55:72-73, 1982.
29.Lloyd M: Heavy metal ingestion:Medical management and gastro-scopic foreign body removal. J AssocAvian Vet 6(1):25-29, 1992.
30. Lumeij JT: A new instrument for re-moving gastric foreign bodies inbirds. Proc Europ Assoc Avian Vet,Utrecht, 1993, pp 91-98.
31.MacCoy DM, Campbell TW: Excisionof impacted and ruptured uropygialglands in three Gentoo penguins.Proc Am Assoc Zoo Vet, 1991, pp 259-260.
32.Martin HD: Abdominal hernia withformation of a urate concretion in acockatiel. J Am Vet Med Assoc189(10):1332-1333, 1986.
33.Martin HD: Avian reproductive emer-gencies: Surgical management. VetMed Rep 2(3):250-253, 1990.
34.McCluggage D: Hysterectomy: A re-view of selected cases. Proc AssocAvian Vet, 1992, pp 201-206.
35.McCluggage D: Proventiculotomy: Astudy of selected cases. Proc AssocAvian Vet, 1992, pp 195-198.
36.McDonald SE: Successful treatmentof mycotic tracheitis in a raven. ProcAssoc Avian Vet, 1984, pp 154-163.
37.McLelland J: A Color Atlas of AvianAnatomy. Philadelphia, WB Saun-ders Co, 1991.
38.Moore CP, et al: Extracapsular extrac-tion of senile cataract in an Andeancondor. J Am Vet Med Assoc187(11):1211-1212, 1985.
39.Mullen JL, et al: Amputation of thewing in a whooping crane. J Am VetMed Assoc 185(11):1402-1403, 1984.
40.Nickel R, et al: Respiratory system.In Anatomy of the Domestic Birds,New York, Springer-Verlag, 1977, pp62-69.
41.Quesenberry KE, et al: Nutritionalsupport of the avian patient. Proc As-soc Avian Vet, 1989, pp 11-19.
42.Reece RL: Reproductive diseases. InBurr EW (ed): Companion Bird Medi-cine. Ames, Iowa State UniversityPress, 1987, pp 89-100.
43.Ringer RK: Selected physiology forthe avian practitioner. In HarrisonGJ, Harrison LR (eds): Clinical AvianMedicine and Surgery. Philadelphia,WB Saunders Co, 1986, pp 78-80.
44.Rosskopf WJ: Surgery of the avianrespiratory system. Proc 12th An-nual Vet Surg Forum, 1984, pp 47-56.
45.Rosskopf WJ, et al: Pet avian emer-gency care. Proc Assoc Avian Vet,1991, pp 349.
46.Rosskopf WJ, et al: Sinus trephina-tion of the supraorbital sinuses inpsittacine birds: An aid in the treat-ment of chronic sinus infections. ProcAssoc Avian Vet, 1986, pp 295-301.
47.Rosskopf WJ, Woerpel RW: Cloacalconditions in pet birds with a cloaca-pexy update. Proc Assoc Avian Vet,1989, pp 156-163.
48.Rosskopf WJ, Woerpel RW: Pet avianobstetrics. Proc 1st Int Conf Zoo &Avian Med, 1987, pp 213-231.
49.Sikarski JG: Ostrich castration for be-havioral control. Proc 1st Int ConfZoo & Avian Med, 1987, pp 416.
50.Slatter DM, et al: Hereditary cata-racts in canaries. J Am Vet Med As-soc 183:872-874, 1983.
51.Smith RE: Hysterectomy to relieve re-productive disorders in birds. AvianExotic Pract 2:40-43, 1985.
52.Steinbach MJ, et al: Torsional eyemovements in the owl. Vision Res14:745-746, 1974.
53.Swartout MS, Wyman M: Pancreaticcarcinoma in a cockatiel. J Am VetMed Assoc 191(4):451-452, 1987.
54.Turrel JM, et al: Diagnosis and treat-ment of tumors of companion birds.AAV Today 1(3):109-116, 1987.
55.Van Zant F: Resolution of a cloacaladhesion in a blue-fronted Amazon.Proc Assoc Avian Vet, 1992, pp 162-164.
56.Van Zant F: Resolution of an esopha-geal stricture in a hyacinth macaw.Proc Assoc Avian Vet, 1992, pp 177-179.
57.Wissman MA: Unusual c-section andhysterectomy in the Isle of PinesAmazon. Proc Assoc Avian Vet, 1991,pp 265-266.
SECTION SIX SURGERY
1136