Embed Size (px)
Citation preview
223©Elsevier & CTSUM. All rights reserved. J Med Ultrasound 2008 • Vol 16 • No 3
O R I G I N A L
A R T I C L E
Soft Tissue Hemangiomas: High-resolutionGrayscale and Color Doppler Ultrasonographic
Features in 43 Patients
Chia-Yu Keng1,2, Howard Haw-Chang Lan1,2,3*, Clayton Chi-Chang Chen1,2,3, Mein-Kai Gueng1,2, Yeou-Gie Su1, San-Kan Lee4
Background: High-resolution ultrasonography (HRUS) is the first-line imaging modality forthe assessment of soft tissue tumors. The reported HRUS features of soft tissue heman-giomas vary greatly. We reviewed 43 histologically proven soft tissue hemangiomas anddescribe the HRUS and color Doppler ultrasound (CDUS) features, and propose a convenientCDUS sign for diagnosis.Materials and Methods: HRUS data of 43 proven soft tissue hemangiomas were includedin this study. Data assessment included tumor margin, tumor echogenicity and echotexture,presence of phleboliths, fluid–fluid level in the masses, and CDUS features. In masses withweak or no color Doppler signal, color Doppler enhancing maneuver (CDEM) was applied,which was carried out using light compression on the masses or on the soft tissues adja-cent to the masses. CDEM was considered positive when the color Doppler signal in amass was more prominent and/or extensive.Results: Twenty-three hemangiomas were ill-defined and 20 were well-defined. Twenty-sixhemangiomas were hypoechoic and 17 were hyperechoic. Thirty-seven masses were het-erogeneous in echotexture. Phleboliths were found in only nine hemangiomas. Thirty-sevenhemangiomas had multiple cystic spaces and fluid–fluid levels were noted in 12. ColorDoppler signals were detected in 37 hemangiomas, i.e. 33 masses had weak signals and four masses had strong signals. CDEM was positive in all 33 hemangiomas with weakcolor Doppler signals and was positive in four of six hemangiomas with no detectable colorDoppler signal.Conclusion: Typical HRUS features of a soft tissue hemangioma were an ill-defined orwell-defined hypoechoic mass of heterogeneous echotexture with multiple cystic spaces.On CDUS, there may be no detectable or only weak color Doppler signals. CDEM washelpful in the diagnosis of soft tissue hemangiomas, especially in masses with no detectablecolor Doppler signal.
Received: January 14, 2008 Accepted: February 20, 20081Department of Radiology, Taichung Veterans General Hospital, 2Department of Radiological Technology,Central Taiwan University of Science and Technology, 3School of Physical Therapy, Hungkuang University,Taichung, and 4Department of Radiology, Chia-Yi Veterans Hospital, Chia-Yi, Taiwan.
*Address correspondence to: Dr. Howard Haw-Chang Lan, Department of Radiology, Taichung VeteransGeneral Hospital, 160 Taichung-Kang Road, Section 3, Taichung 407, Taiwan.
E-mail: [email protected]

Introduction
Hemangioma is one of the most common soft tissuetumors, constituting 7% of all benign tumors [1–4].It is also the most frequent tumor of infancy andchildhood [1–3]. These tumors may be superficialor deep, with the latter lesions most frequentlybeing intramuscular [3]. Superficial lesions are eas-ily diagnosed, appearing as a slightly raised, bluish-red subcutaneous mass. Deeper lesions, however,are a diagnostic dilemma because of normal skincolor [3] and lead to imaging assessment.
Plain radiography, xeroradiography, computedtomography, magnetic resonance imaging, high-resolution ultrasonography (HRUS), scintigraphy,and angiography have been used in the diagnosisof soft tissue hemangiomas [5]. For its real-timeassessment, excellent imaging resolution and colorDoppler evaluation, HRUS had been recommendedas the first-line imaging modality for soft tissuetumors [5–9]. The reported HRUS features of softtissue hemangiomas, however, are very variable[10,11]. In this study, we describe the HRUS andcolor Doppler ultrasound (CDUS) features of softtissue hemangiomas in 43 patients, and propose a convenient CDUS sign for diagnosis.
Materials and Methods
Forty-three cases of histologically proven soft tis-sue hemangiomas were found following a retro-spective search of our ultrasonographic files fromJanuary 2000 to July 2007. The patients consistedof 24 females and 19 males, with an age range of 1–51 years (mean, 12 years). HRUS was carriedout using an Acuson 128XP/10 (Mountain View,CA, USA), GE Logiq 700 Expert Series scanner(Milwaukee, WI, USA) or a GE Logiq 9 Series scanner
(Milwaukee, WI, USA), and 10–13 MHz linear arraytransducers.
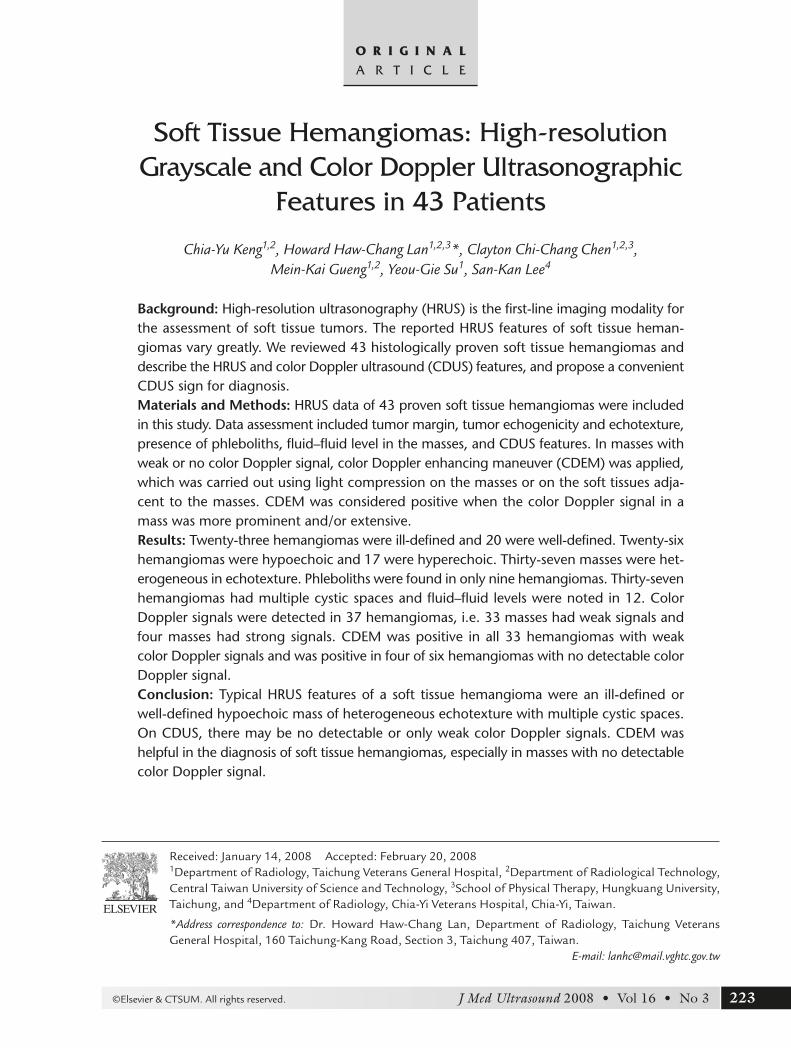
Data evaluation included tumor margin, tumorechogenicity and echotexture, presence of phle-boliths, and fluid–fluid level in the cystic spaces ofmasses. CDUS was performed on all masses. Withoptimal color scale as low as possible to detectweak flow, the color Doppler signal of a mass wasconsidered to be absent if there was no detectablecolor Doppler signal (Fig. 1A), and to be weak ifthere were a few spots of color Doppler signals(Fig. 1B). The signal was considered to be strong if there were clusters of color Doppler signals in a mass, even with the color flow dynamic rangewider than −5 to 5 cm/s (Fig. 1C). In those masseswith weak or no color Doppler signal, color Dopplerenhancing maneuver (CDEM) was applied. Thismaneuver was carried out with direct light com-pression on the masses using the transducer or withcompression on the soft tissues adjacent to themasses. CDEM was considered positive when thecolor Doppler signals in a mass were more prom-inent and/or extensive following the maneuver(Fig. 2). Spectral analysis of blood flow signal wasperformed only in the masses with strong colorDoppler signals.
Results
Of the 43 hemangiomas, 16 were situated on thelower extremities, 15 on the upper extremities, 10on the trunk, and two on the head and neck. Thetumors were intramuscular in 26 cases and subcu-taneous in 17 cases. The histologic subtypes of thehemangiomas were cavernous (25 cases), venous(nine cases), arteriovenous (five cases), capillary(two cases), and mixed venous and capillary (twocases).
C.Y. Keng, H.H.C. Lan, C.C.C. Chen, et al
224 J Med Ultrasound 2008 • Vol 16 • No 3
KEY WORDS — color Doppler, hemangioma, musculoskeletal, soft tissue tumor,ultrasound
■ J Med Ultrasound 2008;16(3):223–230 ■
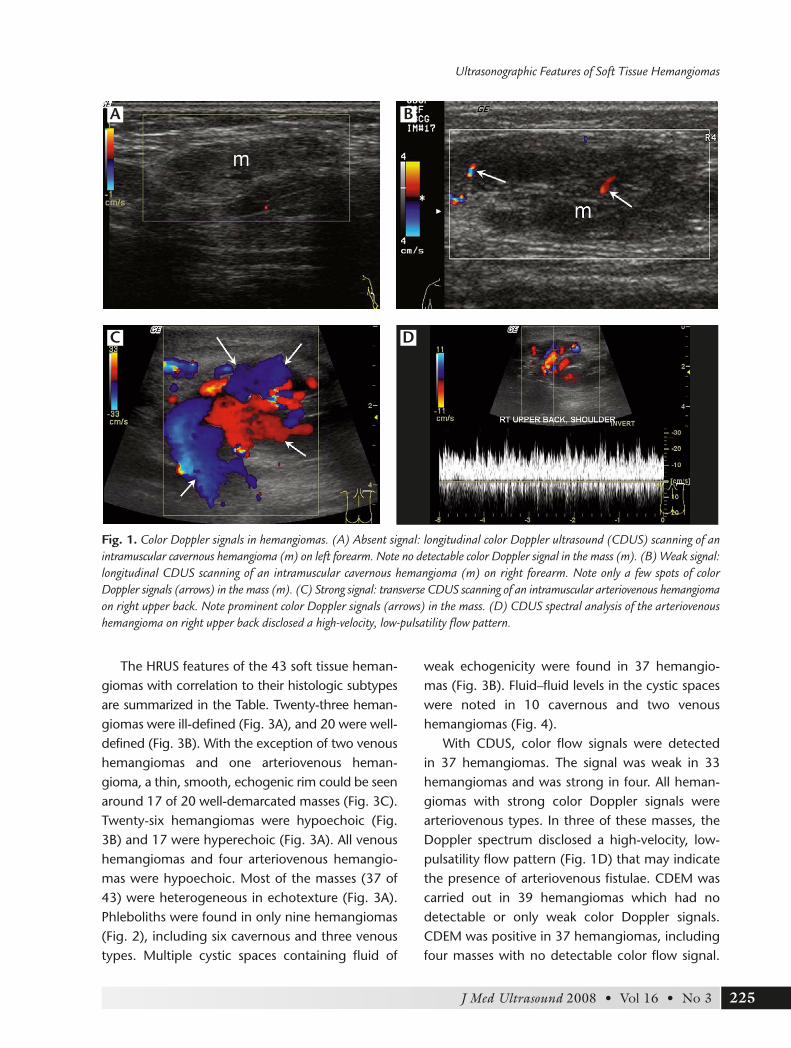
The HRUS features of the 43 soft tissue heman-giomas with correlation to their histologic subtypesare summarized in the Table. Twenty-three heman-giomas were ill-defined (Fig. 3A), and 20 were well-defined (Fig. 3B). With the exception of two venoushemangiomas and one arteriovenous heman-gioma, a thin, smooth, echogenic rim could be seenaround 17 of 20 well-demarcated masses (Fig. 3C).Twenty-six hemangiomas were hypoechoic (Fig.3B) and 17 were hyperechoic (Fig. 3A). All venoushemangiomas and four arteriovenous hemangio-mas were hypoechoic. Most of the masses (37 of43) were heterogeneous in echotexture (Fig. 3A).Phleboliths were found in only nine hemangiomas(Fig. 2), including six cavernous and three venoustypes. Multiple cystic spaces containing fluid of
weak echogenicity were found in 37 hemangio-mas (Fig. 3B). Fluid–fluid levels in the cystic spaceswere noted in 10 cavernous and two venoushemangiomas (Fig. 4).
With CDUS, color flow signals were detected in 37 hemangiomas. The signal was weak in 33hemangiomas and was strong in four. All heman-giomas with strong color Doppler signals werearteriovenous types. In three of these masses, theDoppler spectrum disclosed a high-velocity, low-pulsatility flow pattern (Fig. 1D) that may indicatethe presence of arteriovenous fistulae. CDEM wascarried out in 39 hemangiomas which had nodetectable or only weak color Doppler signals.CDEM was positive in 37 hemangiomas, includingfour masses with no detectable color flow signal.
Ultrasonographic Features of Soft Tissue Hemangiomas
225J Med Ultrasound 2008 • Vol 16 • No 3
B
C D
A
Fig. 1. Color Doppler signals in hemangiomas. (A) Absent signal: longitudinal color Doppler ultrasound (CDUS) scanning of anintramuscular cavernous hemangioma (m) on left forearm. Note no detectable color Doppler signal in the mass (m). (B) Weak signal:longitudinal CDUS scanning of an intramuscular cavernous hemangioma (m) on right forearm. Note only a few spots of colorDoppler signals (arrows) in the mass (m). (C) Strong signal: transverse CDUS scanning of an intramuscular arteriovenous hemangiomaon right upper back. Note prominent color Doppler signals (arrows) in the mass. (D) CDUS spectral analysis of the arteriovenoushemangioma on right upper back disclosed a high-velocity, low-pulsatility flow pattern.

C.Y. Keng, H.H.C. Lan, C.C.C. Chen, et al
226 J Med Ultrasound 2008 • Vol 16 • No 3
BA
Fig. 2. Longitudinal color Doppler ultrasound scan of an intramuscular cavernous hemangioma with color Doppler enhancingmaneuver (CDEM). (A) Before CDEM: no detectable color Doppler signal in the mass (m). (B) After CDEM: presence of irregularcolor Doppler signals (open arrows) in the mass (m). A phlebolith (arrow) was also noted in the mass. The acoustic show wasobscure owing to hypoechogenicity of the mass.
Table. Correlation of ultrasonographic features and histologic subtypes of 43 soft tissue hemangiomas
Cavernous Venous Capillary Arteriovenous Mixed Total (n = 25) (n = 9) (n = 2) (n = 5) (n = 2) (n = 43)
Margin
Ill-defined 13 5 2 2 1 23
Echogenic rim (+)* 0 0 0 0 0 0
Well-defined 12 4 0 3 1 20
Echogenic rim (+)* 12 2 0 2 1 17
Echogenicity
Hypoechoic 11 9 1 4 1 26
Hyperechoic 14 0 1 1 1 17
Echotexture
Heterogeneous 22 7 2 4 2 37
Homogeneous 3 2 0 1 0 6
Cystic spaces 24 8 1 2 2 37
Fluid–fluid levels 10 2 0 0 0 12
Phleboliths 6 3 0 0 0 9
Color flow signal
No 5 1 0 0 0 6
CDEM positive 4 0 0 0 0 4
Weak 20 8 2 1 2 33
CDEM positive 20 8 2 1 2 33
Strong 0 0 0 4 0 4
*Presence of echogenic rim. CDEM = color Doppler enhancing maneuver.
In one hemangioma which had large cystic spacesand no detectable color flow signal on CDUS,mimicking lymphangioma, the CDEM was positive(Fig. 5). Both hemangiomas, one cavernous andone venous, with negative CDEM were located inthe subcutaneous layer, and had no detectablecolor Doppler signal prior to CDEM.
Discussion
Soft tissue hemangiomas represent a broad spec-trum of benign neoplasms, which histologically re-semble normal blood vessels. They are usually first
discovered before the third decade and have apredilection for female patients [3]. Pathologically,they are classified by the predominant type of vascu-lar channel identified within the lesion, i.e. capillary,cavernous, arteriovenous or venous [3]. Capillaryhemangiomas have been reported to be the mostcommon type [1,3,11]. However, only two capillaryhemangiomas were found in our series. This discrep-ancy might be due to patient selection bias. Clinically,capillary hemangiomas are usually superficial andcharacteristic, so radiologic evaluation is requiredinfrequently [3]. Pain and a palpable mass are themost common clinical presentations associatedwith soft tissue hemangiomas [3]. Intramuscular
Ultrasonographic Features of Soft Tissue Hemangiomas
227J Med Ultrasound 2008 • Vol 16 • No 3
B
A C
Fig. 3. High-resolution ultrasonography (HRUS) features of soft tissue hemangiomas. (A) Transverse HRUS scanning of an intra-muscular cavernous hemangioma (H) on the biceps brachii muscle of left upper arm. Note the mass had an ill-defined margin(arrows), with hyperechogenicity and heterogeneous echotexture. hu = humerus. (B) Longitudinal HRUS scanning of an intramuscularvenous hemangioma on the triceps brachii muscle of right upper arm. Note the mass had a well-defined margin (arrows) with hypo-echogenicity and heterogeneous echotexture. Multiple cystic spaces (c) were also noted in the mass. hu=humerus. (C) Transverse HRUSscanning of an intramuscular cavernous hemangioma (m) on calf muscle. Note the echogenic rim (open arrows) around the mass.

hemangiomas are usually asymptomatic or havevague pain after exercise [3].
Histologically, soft tissue hemangiomas usuallyhave no true capsule [3]. The demarcation of hem-angiomas on HRUS might depend upon the echo-genicity differences between the tumor and thesurrounding normal tissue. Our series showed thatthe tumor margin of soft tissue hemangiomas mightbe either ill-defined or well-defined with similarincidence. That was also true for each histologic
type except capillary hemangiomas. Although bothcapillary hemangiomas were ill-defined, the casenumber was too small to make a conclusion. Theseresults are inconsistent with previous reports thatfive of seven hemangiomas in the series of Derchiet al [10] and 14 of 23 hemangiomas in the seriesof Yang et al [11] had well-defined margins. Thisdiscrepancy might be attributed to the histologiccharacteristics as well as the anatomic location ofthe hemangiomas. Soft tissue hemangiomas consistof vascular channels of various sizes and differentnonvascular elements, including fat, muscle, fibroustissue etc. [3], accounting for the multifariousechogenicity and heterogeneous echotexture of themasses. Hemangiomas in those two series were con-fined to specific tissues (skeletal muscles in theseries of Derchi et al [10]) and anatomic locations(head and neck in the series of Yang et al [11]), sothat the masses might be delineated by normalanatomic boundaries, i.e. muscle fasciae, anatomicwalls, etc. Similar to hepatic hemangiomas whichmay have an echogenic rim as described by Moodyand Wilson [12], a well-defined soft tissue heman-gioma might be surrounded by a thin echogenicmargin. Farrell et al reported that the thin echogenicrim surrounding hepatic hemangiomas was due to a higher concentration of acoustic interfacescompared with the center of the mass [13].
C.Y. Keng, H.H.C. Lan, C.C.C. Chen, et al
228 J Med Ultrasound 2008 • Vol 16 • No 3
Fig. 4. Fluid–fluid levels in hemangioma. Longitudinal high-resolution ultrasonography scanning of a subcutaneous cavern-ous hemangioma over right forearm. The mass was ill-definedand consisted of multiple cystic spaces (c). A fluid–fluid level(arrows) was noted in one of the cystic spaces.
A B
Fig. 5. Subcutaneous cavernous hemangioma mimicking lymphangioma. The mass consisted of dilated cystic spaces with septa con-taining echogenic fluid. (A) Before color Doppler enhancing maneuver: no detectable color Doppler signal in the cystic spaces (c).(B) After color Doppler enhancing maneuver: irregular color Doppler signals (open arrows) were noted in the cystic spaces (c).c = cyst; clv = clavicle.

The HRUS features of soft tissue hemangiomasare protean on grayscale imaging [11]. The pres-ence of focal soft tissue masses consisting of solidparts of heterogeneous echotexture, hypoecho-genicity, and cystic parts of multiple cystic spacescontaining fluid of weak echogenicity might raisethe diagnosis of hemangiomas. In our series, 86%(37/43) of hemangiomas were heterogeneous inechotexture, and 60.5% (26/43) of hemangiomaswere hypoechoic. These results are consistent withrecent reports [11,14,15] but were different fromthe series of Derchi et al [10]. This variation has beenattributed to the histologic characteristics of thehemangioma itself and to the background echoge-nicity [11]. Hemangiomas confined to the subcu-taneous layer (hyperechoic background) tend tobe hypoechoic. On the other hand, intramuscularhemangiomas (hypoechoic background) tend tobe hyperechoic. In our series, 70.6% (12/17) ofhemangiomas confined to subcutaneous tissuewere hypoechoic. However, the echogenicity ofintramuscular hemangiomas was variable with46.2% (12/26) being hyperechoic. Occasionally,in the masses with characteristic HRUS features,the presence of fluid–fluid levels in cystic spacesand/or phleboliths might enhance the diagnosticconfidence. Cavernous and venous hemangiomastypically have larger vascular spaces and slow bloodflow [3], accounting for the presence of phlebolithsand fluid–fluid levels in the cystic spaces. In ourseries, all 12 masses with fluid–fluid levels in the cys-tic spaces were cavernous hemangiomas, and innine masses with phleboliths, six were cavernoushemangiomas and three were venous lesions.
Soft tissue hemangiomas are widely believed tohave no detectable color Doppler signals on CDUSbecause of slow blood flow [11]. With recent ad-vances in the sensitivity of color Doppler ultrasoundscanners, the detectable color Doppler signals inhemangiomas have increased. Color Doppler signalswere detectable in only 52% (12/23) of heman-giomas in the series of Yang et al [11], whereas88% (44/49) were detectable in the series of Paltielet al [15] and 86% (37/43) were detectable in ourseries. Arteriovenous hemangiomas are composed
of abnormal communications between arteriesand veins [3]. Histologically, two forms of arteriove-nous hemangioma exist: superficial lesions withoutarteriovenous shunting, and deep lesions with arte-riovenous shunting. The deep lesions are usuallysymptomatic and characterized by high blood flow.These lesions are more likely to have strong colorDoppler signals on CDUS. All four hemangiomaswith strong color Doppler signals in our study werearteriovenous lesions. In three of the lesions, theDoppler spectrum disclosed a high-velocity, low-pulsatility flow pattern implying the presence ofarteriovenous fistulae.
Dubois et al suggested that high vessel densityand high peak arterial Doppler shift, more than2 kHz, differentiated hemangiomas from other softtissue masses [14]. However, in hemangiomas withno detectable or only weak color Doppler signals,the differential diagnosis between hemangioma andother soft tissue masses based on grayscale US andCDUS might be challenging, especially in lymph-angiomas. Chou et al recommended the adminis-tration of intravenous contrast agents to overcomethe difficulties in the differential diagnosis of large-vessel hemangiomas from lymphangiomas [16].CDEM provided a simpler and more convenientmethod to achieve this diagnosis. CDEM enhancedblood flow rate artificially by compressing tissueadjacent to vascular or cystic spaces, hence produc-ing color Doppler signals. Theoretically, the vascularchannels both in hemangiomas and lymphangio-mas are open spaces with many communications, sothat the fluid can be pushed forward and produceartificial color Doppler signals. Lymphatic fluid inlymphangiomas, in fact, contain too few cells toproduce echo [16,17], leading to a negative CDEM.Using CDEM, we successfully made the correctdiagnosis before surgery in four of six hemangio-mas, which had no detectable color Doppler signals,including the mass mimicking a lymphangioma.Nevertheless, in our series, there were approximately5% false-negative results for CDEM. The reasonsfor these false-negative results might be related totechnical errors and/or structural variations in thehemangiomas. In addition, positive CDEM was not
Ultrasonographic Features of Soft Tissue Hemangiomas
229J Med Ultrasound 2008 • Vol 16 • No 3

a specific diagnostic sign for hemangiomas. Softtissue masses containing echogenic fluid in openspaces might produce color Doppler enhancingphenomenon as well. The sensitivity and specificityof CDEM in the diagnosis of hemangiomas andthe role of CDEM in the differential diagnosis be-tween hemangiomas and other soft tissue tumorsneeds further study with a larger series.
In conclusion, HRUS provided a useful first-lineimaging modality for the diagnosis of soft tissuehemangiomas. A soft tissue hemangioma might beill-defined or well-defined. A thin echogenic rimmay demarcate the mass from adjacent tissue.Typical HRUS features of soft tissue hemangiomasincluded a focal mass of heterogeneous echogenic-ity with multiple cystic spaces containing fluid ofweak echoes, and occasionally, fluid–fluid levels inthe cystic spaces or the presence of phleboliths.Hemangiomas might show no or only weak colorDoppler signals on CDUS. CDEM was a helpfulcomplementary method for the diagnosis of softtissue hemangiomas which had no detectable colorDoppler signals.
References
1. Allen PW, Enzinger FM. Hemangioma of skeletal mus-cles: an analysis of 89 cases. Cancer 1972;29:8–22.
2. Murphey MD, Fairbairn KJ, Parman LM, et al. Muscu-loskeletal angiomatous lesions: radiologic-pathologiccorrelation. Radiographics 1995;15:893–917.
3. Kransdorf MJ, Murphey MD. Vascular and lymphatictumors. In: Kransdorf MJ, Murphey MD, eds. Imagingof Soft Tissue Tumors. Philadelphia: WB Saunders,1997:103–41.
4. Chiou HJ, Chou YH, Chiou SY, et al. High-resolutionultrasonography in superficial soft tissue tumors. J Med Ultrasound 2007;15:152–74.
5. Greenspan A, McGahan JP, Vogelsang P, et al.Imaging strategies in the evaluation of soft-tissuehemangiomas of the extremities: correlation of the
findings of plain radiography, angiography, CT, MRI,and ultrasonography in 12 histologically provencases. Skeletal Radiol 1992;21:11–8.
6. Lagalla R, Iovane A, Caruso G, et al. Color Dopplerultrasonography of soft-tissue masses. Acta Radiol1998;39:421–6.
7. Bodner G, Schocke MF, Rachbauer F, et al. Differ-entiation of malignant and benign musculoskeletaltumors: combined color and power Doppler US andspectral wave analysis. Radiology 2002;223:410–6.
8. Latifi HR, Siegel MJ. Color Doppler flow imaging ofpediatric soft tissue masses. J Ultrasound Med 1994;13:165–9.
9. Ozbek SS, Arkun R, Killi R, et al. Image-directedcolor Doppler ultrasonography in the evaluation ofsuperficial solid tumors. J Clin Ultrasound 1995;23:233–8.
10. Derchi LE, Balconi G, De Flaviis L, et al. Sonographicappearances of hemangiomas of skeletal muscle. J Ultrasound Med 1989;8:263–7.
11. Yang WT, Ahuja A, Metreweli C. Sonographic fea-tures of head and neck hemangiomas and vascularmalformations: review of 23 patients. J UltrasoundMed 1997;16:39–44.
12. Moody AR, Wilson SR. Atypical hepatic hemangioma:a suggestive sonographic morphology. Radiology 1993;188:413–7.
13. Farrell MA, Charboneau JW, Reading CC.Sonographic-pathologic correlation of the hyper-echoic border of an atypical hepatic hemangioma. J Ultrasound Med 2001;20:169–70.
14. Dubois J, Patriquin HB, Garel L, et al. Soft-tissuehemangiomas in infants and children: diagnosis usingDoppler sonography. AJR Am J Roentgenol 1998;171:247–52.
15. Paltiel HJ, Burrows PE, Kozakewich HPW, et al. Soft-tissue vascular anomalies: utility of US for diagnosis.Radiology 2000;214:747–54.
16. Chou YH, Tiu CM, Chiou HJ, et al. Echo-enhancingsonography of a large-vessel hemangioma of the neck.J Clin Ultrasound 1999;27:465–8.
17. Loberant N, Chernihovski A, Goldfeld M, et al. Roleof Doppler sonography in the diagnosis of cystic lymphangioma of the scrotum. J Clin Ultrasound 2002;30:384–7.
C.Y. Keng, H.H.C. Lan, C.C.C. Chen, et al
230 J Med Ultrasound 2008 • Vol 16 • No 3

![Cancer Research - Differential Inhibition of Fluid ......ICANCER RESEARCH 58. 25M4-26(X>, June 15, 1998] Differential Inhibition of Fluid Accumulation and Tumor Growth in Two Mouse](https://img.pdfslide.us/doc/110x75/614a29b312c9616cbc693cc2/cancer-research-differential-inhibition-of-fluid-icancer-research-58.jpg)


![Detection of genes mutations in cerebrospinal fluid ...plasma or CSF to monitor the tumor progression and/or treatment responses [3–5]. In patients with brain tumor, the plasma ctDNA](https://img.pdfslide.us/doc/110x75/60cb589de02f2457014cfd5e/detection-of-genes-mutations-in-cerebrospinal-fluid-plasma-or-csf-to-monitor.jpg)










![[PPT]TUMOR TRAKTUS UROGENITAL - FK UWKS 2012 C | … · Web viewTUMOR TRAKTUS UROGENITAL I. Tumor Ginjal A. Tumor Grawitz B. Tumor Wilms II. Tumor Urotel III. Tumor Testis IV. Karsinoma](https://img.pdfslide.us/doc/110x75/5ade93b87f8b9ad66b8bb718/ppttumor-traktus-urogenital-fk-uwks-2012-c-viewtumor-traktus-urogenital.jpg)













