Embed Size (px)
Citation preview

Socioeconomic and Lifestyle Factors and the10-year Incidence of Age-related Cataracts
BARBARA E. K. KLEIN, MD, MPH, RONALD KLEIN, MD, MPH, KRISTINE E. LEE, MS,AND STACY M. MEUER, BS
● PURPOSE: To investigate the association of socioeco-nomic and lifestyle factors with incidence of age-relatedcataracts.● DESIGN: Population-based longitudinal epidemiologicstudy.● METHODS: Persons aged 43 to 86 years (n � 4,926)living in Beaver Dam, Wisconsin, were examined in1988 to 1990, 1993 to 1995, and 1998 to 2000. Medicalhistories were obtained, and photographs of the lenseswere taken at each visit. Photographs were graded ac-cording to standard protocols.● RESULTS: Socioeconomic and lifestyle factors consid-ered were income, education, occupation, smoking, alco-hol, caffeine, and multivitamin use. After adjustment forage and sex, income (or education) was inversely andsmoking was directly related to the 10-year cumulativeincidence of nuclear cataract. None of the factors weresignificantly associated with incident cortical or posteriorsubcapsular cataract. We found no evidence in theseanalyses to suggest that history of multivitamin usealtered the relationships of smoking to the incidence ofcataracts. In models adjusting for all other significant riskfactors, the individual significance values for each indi-vidual factor differed little from the models adjustingonly for age and sex.● CONCLUSIONS: Incident nuclear cataract was associ-ated with income and smoking 10 years earlier. Therewere no significant lifestyle exposures associated withincident cortical and posterior subcapsular cataract.(Am J Ophthalmol 2003;136:506–512. © 2003 byElsevier Inc. All rights reserved.)
W HILE THE DEVELOPMENT OF CATARACTS IS
largely an age-related phenomenon, socioeco-nomic and lifestyle factors may influence their
development.1–8 Lower income and less education are alsorelated to increased morbidity and mortality.9 The causalpaths of these associations are not clear but may be relatedto health care, noxious environments, and high-risk be-haviors.
Impaired vision and cataracts have been found to beassociated with education and income.10–13 In prevalencedata from the Beaver Dam Eye Study, education wassignificantly inversely associated with risk of nuclear andcortical cataract and income was significantly inverselyassociated with risk of cortical and posterior subcapsularcataracts.14 Smoking and drinking in particular have beenfound to be directly related to at least one type ofage-related cataract (ARC) in many studies, both cross-sectionally1–7 and longitudinally.8 Caffeine has been foundto have no effect.8 When the cataract endpoint is uncom-mon (posterior subcapsular cataract), when the exposurelevels are low, or when the relationship is not strong,longer follow-up may be necessary to fully explore thepossibility of an effect. There may also be instances whentwo exposures act in concert but where the joint effectsrequire a substantial number of jointly exposed persons tobe detectable. This may be the case when examining arelative effect of vitamin supplements in smokers. Forthese reasons, we investigated the relationships of socio-economic and lifestyle factors to incidence of cataractsover a 10-year interval.
METHODS
● POPULATION: Methods used to identify the populationand descriptions of the population have appeared inprevious reports.15,16 In brief, 4,926 persons participated ina baseline examination from March 1988 to September1990. Of the 3,334 surviving persons who participated in a5-year follow-up examination17 2,764 (82.9%) participatedin the 10-year follow-up examination. The mean time
Accepted for publication March 7, 2003.From the Department of Ophthalmology and Visual Sciences, Univer-
sity of Wisconsin Medical School, Madison, Wisconsin.This research is supported by Grant EY06594 from the National
Institutes of Health, Bethesda, Maryland.Inquires to Barbara E. K. Klein, MD, MPH, Department of Ophthal-
mology and Visual Sciences, University of Wisconsin—Madison, 610North Walnut St., 4th Floor WARF, Madison, WI 53726-2397; fax (608)263-0279; e-mail: [email protected]
© 2003 BY ELSEVIER INC. ALL RIGHTS RESERVED.506 0002-9394/03/$30.00doi:10.1016/S0002-9394(03)00290-3

between the baseline and 10-year follow-up examinationswas 10.1 years (standard deviation [SD] � 0.4 years) andthe median was 10.0. Comparisons between participantsand nonparticipants at 10-year follow-up revealed that the418 nonparticipants who were alive at the 10-year fol-low-up were more likely to be older than the 2,764participants. While controlling for age, these nonpartici-pants were more likely (at baseline) to have completedfewer years of education, be retired, have lower income,poorer visual acuity, hypertension, more pack-years ofcigarettes smoked, higher serum cholesterol, higher systolicblood pressure, and to have a higher frequency of age-related maculopathy than persons who participated. Therewere no statistically significant differences in sex, thepresence of cataract, cardiovascular disease history, cancerhistory, diabetes, or heavy alcohol consumption at base-line.18 There were also no statistically significant differ-ences while controlling for age, in baseline visual acuity,age-related maculopathy, or cataract between those whoparticipated at the 10-year follow-up and those who haddied (n � 152).18 Those included in the analyses consistedof the 2,764 people examined at all three visits and 920people who were examined at baseline and at the 5-yearfollow-up only. Ninety-nine percent of the population waswhite. Comparisons between participants and nonpartici-pants at the baseline and at the 5-year follow-up appearelsewhere.16,17
● PROCEDURES: Approval was granted by the HumanSubjects Committee at the University of Wisconsin, andinformed consent was obtained from each participant atthe beginning of each examination. The parts of theexamination pertinent to this report consisted of a stan-dardized questionnaire including questions about date ofbirth, household income, education, occupation, activitylevel, cigarette smoking history, intake of alcohol, caf-feine-containing beverages, and current and past use ofmultivitamins. Photographs were taken of the lens of eacheye after pupillary dilation. Photographs were graded inmasked fashion.19
● DEFINITIONS: Individuals were asked to categorizetheir household income and education according to thecategories in Table 1. Occupation was classified as whitecollar, blue collar, or farm. Activity level was characterizedas active or sedentary, based on a report of engaging inregular activity long enough to work up a sweat three timesper week.
Subjects were asked whether they had ever smoked(�100 cigarettes/lifetime); if so, they were asked thenumber of cigarettes smoked per day and the number ofmonths they smoked, current smoking status, and the dateof stopping. Pack-years was computed based on cigarettessmoked per day / 20 � years smoked. Each participant wasasked about his or her consumption of beer, wine, andliquor in the last year. From responses, subjects wereclassified as current drinkers or nondrinkers of the specific
alcohol type. We asked the number of each beverage typethey consumed each week. The response was converted tograms of alcohol according to the following estimates ofethanol per serving: 12 ounces of beer contained 13 g, 4ounces of wine contained 11.5 g, and 1.5 ounces of liquorcontained 14 g. Current nondrinkers were asked if theyhad ever consumed alcohol. Those answering no wereclassified as lifetime abstainers. We asked whether partic-ipants drank beverages with caffeine in them once a day ormore often. For those who answered no, we asked whetherthey had done so in the past. For past and current users, weasked them to name the beverage, to tell us how many cups(or cans) per day they usually consumed, and whether suchuse occurred in the present or in the past only. Usingestimates of amount of caffeine per serving, we tallied theamount ingested per day for current and past intake. Theestimated amounts of caffeine per serving were as follows:103 mg for brewed coffee, 57 mg for instant coffee, 37 mgfor “balanced” coffee (a combination of brewed and breweddecaffeinated coffee), 36 mg for tea, 6 mg for hot choco-late, 46 mg for soda with caffeine, and 57 mg for coffeewith acid removed. To compute amount of caffeine, wetook coffee as the standard (103 mg/cup). The approxi-mate number of cups per day was calculated. Participantswere asked to bring all medications (prescription andover-the-counter) that they were regularly taking to thestudy examination. The examiner also asked whether therewere other medications being taken that were not brought.In addition, participants were asked if they had usedspecific classes of drugs in the past. Information on dura-tion of use and dose was not obtained. Multivitamins wereclassified as such if their composition conformed to theclassification of the American Hospital Formulary Service.If a participant reported using a multivitamin at the timeof the examination, her or she was considered to be acurrent user.
Grading procedures for the lens photographs were basedon detailed codified decision rules.19 Graders were maskedas to subject identity. Scores for nuclear sclerosis werebased on comparisons with standard photographs, whichresulted in a five-step scale of severity based on opacity ofthe nucleus. Severities greater than standard three wereconsidered to be nuclear cataract. Scores for cortical andposterior subcapsular cataracts were based on weightedestimates of degree of opacity of lens area as defined by acircular grid, divided into eight “pie-wedged” peripheralareas and a central circular area overlaid on the photo-graph. Cortical cataract was defined as 5% or more of thelens area. Posterior subcapsular cataract was defined as 5%or more of any grid segment.
● STATISTICAL METHODS: Cumulative 10-year rateswere calculated from the product-limit method.21 Theassumption we have made in our analyses is that once acataract endpoint is reached, regression of that lesion doesnot occur. Multivariable analyses and age-adjusted and
SOCIOECONOMIC AND LIFESTYLE FACTORS AND CATARACTSVOL. 136, NO. 3 507
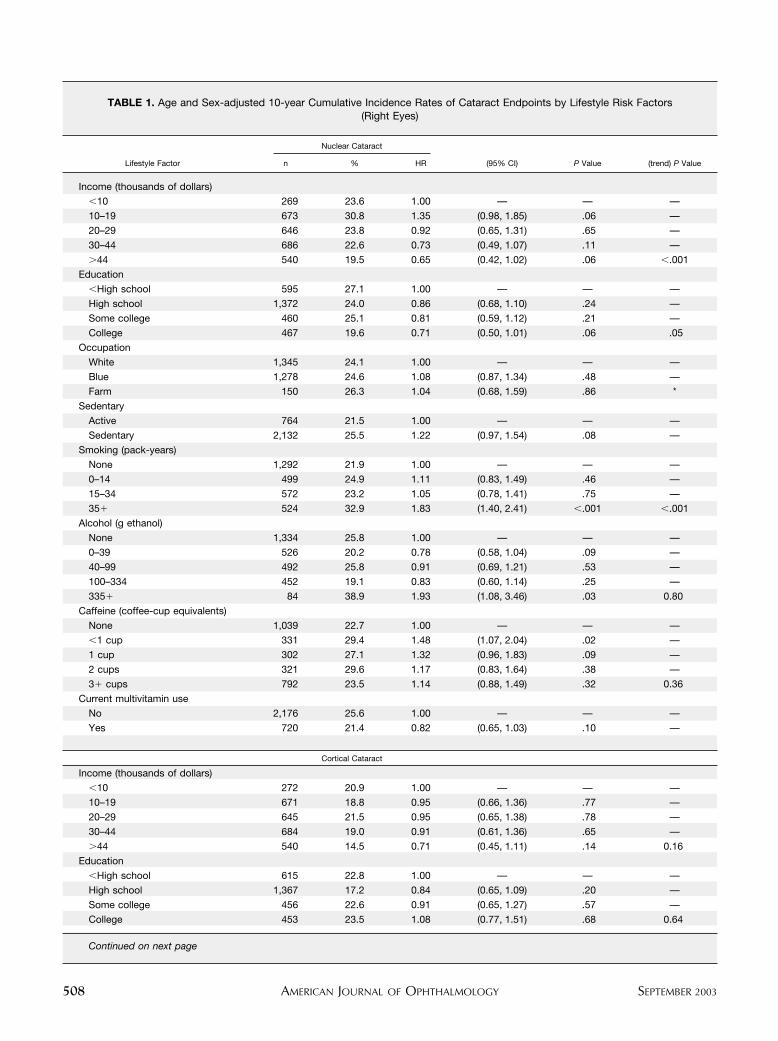
TABLE 1. Age and Sex-adjusted 10-year Cumulative Incidence Rates of Cataract Endpoints by Lifestyle Risk Factors(Right Eyes)
Lifestyle Factor
Nuclear Cataract
(95% CI) P Value (trend) P Valuen % HR
Income (thousands of dollars)
�10 269 23.6 1.00 — — —
10–19 673 30.8 1.35 (0.98, 1.85) .06 —
20–29 646 23.8 0.92 (0.65, 1.31) .65 —
30–44 686 22.6 0.73 (0.49, 1.07) .11 —
�44 540 19.5 0.65 (0.42, 1.02) .06 �.001
Education
�High school 595 27.1 1.00 — — —
High school 1,372 24.0 0.86 (0.68, 1.10) .24 —
Some college 460 25.1 0.81 (0.59, 1.12) .21 —
College 467 19.6 0.71 (0.50, 1.01) .06 .05
Occupation
White 1,345 24.1 1.00 — — —
Blue 1,278 24.6 1.08 (0.87, 1.34) .48 —
Farm 150 26.3 1.04 (0.68, 1.59) .86 *
Sedentary
Active 764 21.5 1.00 — — —
Sedentary 2,132 25.5 1.22 (0.97, 1.54) .08 —
Smoking (pack-years)
None 1,292 21.9 1.00 — — —
0–14 499 24.9 1.11 (0.83, 1.49) .46 —
15–34 572 23.2 1.05 (0.78, 1.41) .75 —
35� 524 32.9 1.83 (1.40, 2.41) �.001 �.001
Alcohol (g ethanol)
None 1,334 25.8 1.00 — — —
0–39 526 20.2 0.78 (0.58, 1.04) .09 —
40–99 492 25.8 0.91 (0.69, 1.21) .53 —
100–334 452 19.1 0.83 (0.60, 1.14) .25 —
335� 84 38.9 1.93 (1.08, 3.46) .03 0.80
Caffeine (coffee-cup equivalents)
None 1,039 22.7 1.00 — — —
�1 cup 331 29.4 1.48 (1.07, 2.04) .02 —
1 cup 302 27.1 1.32 (0.96, 1.83) .09 —
2 cups 321 29.6 1.17 (0.83, 1.64) .38 —
3� cups 792 23.5 1.14 (0.88, 1.49) .32 0.36
Current multivitamin use
No 2,176 25.6 1.00 — — —
Yes 720 21.4 0.82 (0.65, 1.03) .10 —
Cortical Cataract
Income (thousands of dollars)
�10 272 20.9 1.00 — — —
10–19 671 18.8 0.95 (0.66, 1.36) .77 —
20–29 645 21.5 0.95 (0.65, 1.38) .78 —
30–44 684 19.0 0.91 (0.61, 1.36) .65 —
�44 540 14.5 0.71 (0.45, 1.11) .14 0.16
Education
�High school 615 22.8 1.00 — — —
High school 1,367 17.2 0.84 (0.65, 1.09) .20 —
Some college 456 22.6 0.91 (0.65, 1.27) .57 —
College 453 23.5 1.08 (0.77, 1.51) .68 0.64
Continued on next page
AMERICAN JOURNAL OF OPHTHALMOLOGY508 SEPTEMBER 2003
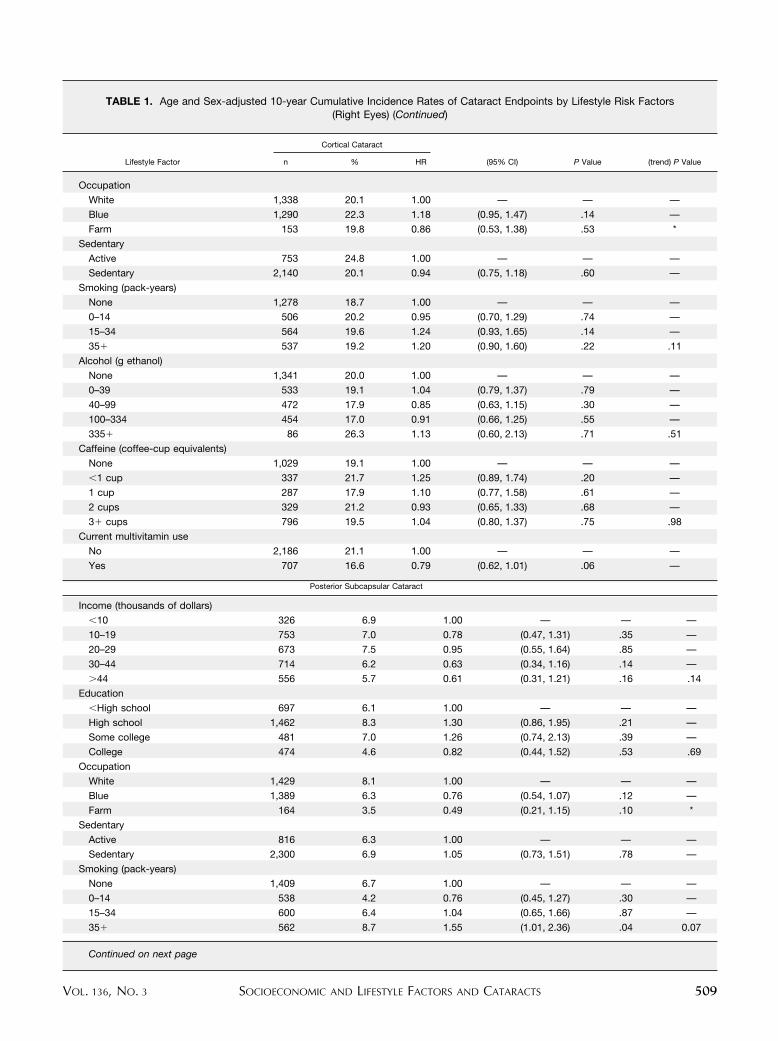
TABLE 1. Age and Sex-adjusted 10-year Cumulative Incidence Rates of Cataract Endpoints by Lifestyle Risk Factors(Right Eyes) (Continued)
Lifestyle Factor
Cortical Cataract
(95% CI) P Value (trend) P Valuen % HR
Occupation
White 1,338 20.1 1.00 — — —
Blue 1,290 22.3 1.18 (0.95, 1.47) .14 —
Farm 153 19.8 0.86 (0.53, 1.38) .53 *
Sedentary
Active 753 24.8 1.00 — — —
Sedentary 2,140 20.1 0.94 (0.75, 1.18) .60 —
Smoking (pack-years)
None 1,278 18.7 1.00 — — —
0–14 506 20.2 0.95 (0.70, 1.29) .74 —
15–34 564 19.6 1.24 (0.93, 1.65) .14 —
35� 537 19.2 1.20 (0.90, 1.60) .22 .11
Alcohol (g ethanol)
None 1,341 20.0 1.00 — — —
0–39 533 19.1 1.04 (0.79, 1.37) .79 —
40–99 472 17.9 0.85 (0.63, 1.15) .30 —
100–334 454 17.0 0.91 (0.66, 1.25) .55 —
335� 86 26.3 1.13 (0.60, 2.13) .71 .51
Caffeine (coffee-cup equivalents)
None 1,029 19.1 1.00 — — —
�1 cup 337 21.7 1.25 (0.89, 1.74) .20 —
1 cup 287 17.9 1.10 (0.77, 1.58) .61 —
2 cups 329 21.2 0.93 (0.65, 1.33) .68 —
3� cups 796 19.5 1.04 (0.80, 1.37) .75 .98
Current multivitamin use
No 2,186 21.1 1.00 — — —
Yes 707 16.6 0.79 (0.62, 1.01) .06 —
Posterior Subcapsular Cataract
Income (thousands of dollars)
�10 326 6.9 1.00 — — —
10–19 753 7.0 0.78 (0.47, 1.31) .35 —
20–29 673 7.5 0.95 (0.55, 1.64) .85 —
30–44 714 6.2 0.63 (0.34, 1.16) .14 —
�44 556 5.7 0.61 (0.31, 1.21) .16 .14
Education
�High school 697 6.1 1.00 — — —
High school 1,462 8.3 1.30 (0.86, 1.95) .21 —
Some college 481 7.0 1.26 (0.74, 2.13) .39 —
College 474 4.6 0.82 (0.44, 1.52) .53 .69
Occupation
White 1,429 8.1 1.00 — — —
Blue 1,389 6.3 0.76 (0.54, 1.07) .12 —
Farm 164 3.5 0.49 (0.21, 1.15) .10 *
Sedentary
Active 816 6.3 1.00 — — —
Sedentary 2,300 6.9 1.05 (0.73, 1.51) .78 —
Smoking (pack-years)
None 1,409 6.7 1.00 — — —
0–14 538 4.2 0.76 (0.45, 1.27) .30 —
15–34 600 6.4 1.04 (0.65, 1.66) .87 —
35� 562 8.7 1.55 (1.01, 2.36) .04 0.07
Continued on next page
SOCIOECONOMIC AND LIFESTYLE FACTORS AND CATARACTSVOL. 136, NO. 3 509
sex-adjusted risk estimates were based on the discretelinear logistic model. SAS was used for all analyses.22 Thegeneral estimating equation approach was used to evaluatethe potential effect of common household on the lifestyle–cataract relationships.23
RESULTS
THE SOCIOECONOMIC AND LIFESTYLE FACTORS WE CON-
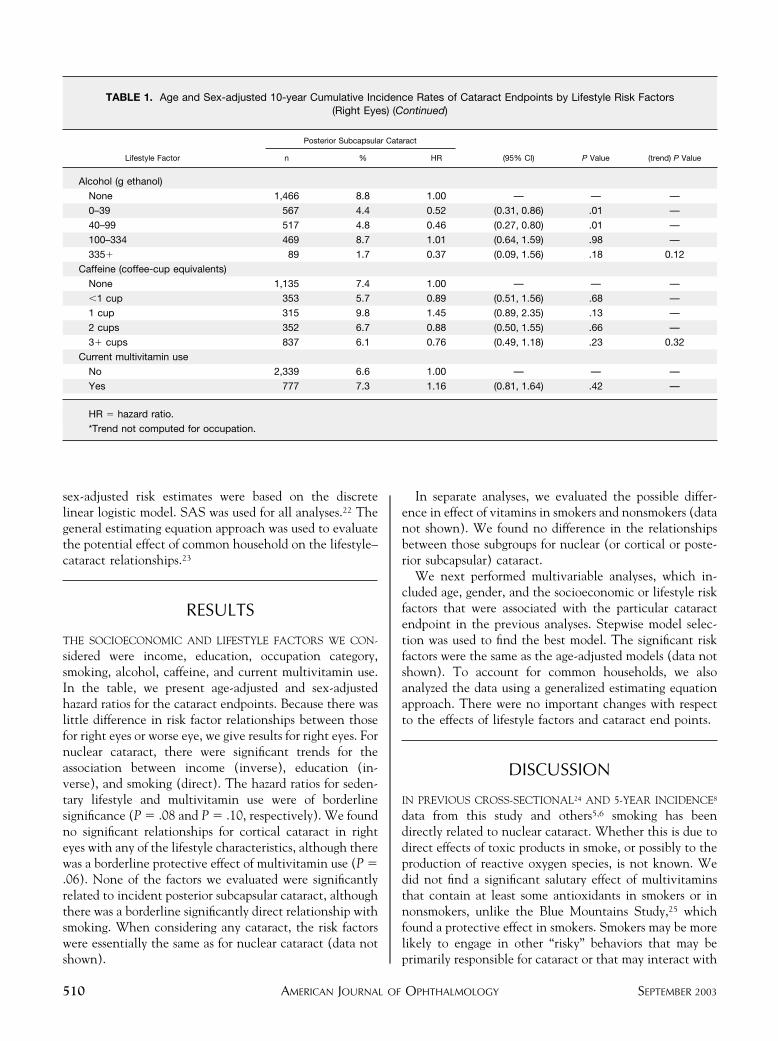
sidered were income, education, occupation category,smoking, alcohol, caffeine, and current multivitamin use.In the table, we present age-adjusted and sex-adjustedhazard ratios for the cataract endpoints. Because there waslittle difference in risk factor relationships between thosefor right eyes or worse eye, we give results for right eyes. Fornuclear cataract, there were significant trends for theassociation between income (inverse), education (in-verse), and smoking (direct). The hazard ratios for seden-tary lifestyle and multivitamin use were of borderlinesignificance (P � .08 and P � .10, respectively). We foundno significant relationships for cortical cataract in righteyes with any of the lifestyle characteristics, although therewas a borderline protective effect of multivitamin use (P �.06). None of the factors we evaluated were significantlyrelated to incident posterior subcapsular cataract, althoughthere was a borderline significantly direct relationship withsmoking. When considering any cataract, the risk factorswere essentially the same as for nuclear cataract (data notshown).
In separate analyses, we evaluated the possible differ-ence in effect of vitamins in smokers and nonsmokers (datanot shown). We found no difference in the relationshipsbetween those subgroups for nuclear (or cortical or poste-rior subcapsular) cataract.
We next performed multivariable analyses, which in-cluded age, gender, and the socioeconomic or lifestyle riskfactors that were associated with the particular cataractendpoint in the previous analyses. Stepwise model selec-tion was used to find the best model. The significant riskfactors were the same as the age-adjusted models (data notshown). To account for common households, we alsoanalyzed the data using a generalized estimating equationapproach. There were no important changes with respectto the effects of lifestyle factors and cataract end points.
DISCUSSION
IN PREVIOUS CROSS-SECTIONAL24 AND 5-YEAR INCIDENCE8
data from this study and others5,6 smoking has beendirectly related to nuclear cataract. Whether this is due todirect effects of toxic products in smoke, or possibly to theproduction of reactive oxygen species, is not known. Wedid not find a significant salutary effect of multivitaminsthat contain at least some antioxidants in smokers or innonsmokers, unlike the Blue Mountains Study,25 whichfound a protective effect in smokers. Smokers may be morelikely to engage in other “risky” behaviors that may beprimarily responsible for cataract or that may interact with
TABLE 1. Age and Sex-adjusted 10-year Cumulative Incidence Rates of Cataract Endpoints by Lifestyle Risk Factors(Right Eyes) (Continued)
Lifestyle Factor
Posterior Subcapsular Cataract
(95% CI) P Value (trend) P Valuen % HR
Alcohol (g ethanol)
None 1,466 8.8 1.00 — — —
0–39 567 4.4 0.52 (0.31, 0.86) .01 —
40–99 517 4.8 0.46 (0.27, 0.80) .01 —
100–334 469 8.7 1.01 (0.64, 1.59) .98 —
335� 89 1.7 0.37 (0.09, 1.56) .18 0.12
Caffeine (coffee-cup equivalents)
None 1,135 7.4 1.00 — — —
�1 cup 353 5.7 0.89 (0.51, 1.56) .68 —
1 cup 315 9.8 1.45 (0.89, 2.35) .13 —
2 cups 352 6.7 0.88 (0.50, 1.55) .66 —
3� cups 837 6.1 0.76 (0.49, 1.18) .23 0.32
Current multivitamin use
No 2,339 6.6 1.00 — — —
Yes 777 7.3 1.16 (0.81, 1.64) .42 —
HR � hazard ratio.
*Trend not computed for occupation.
AMERICAN JOURNAL OF OPHTHALMOLOGY510 SEPTEMBER 2003

smoking to produce an effect. One such exposure might bealcohol. We did not find evidence of an independent effectof alcohol or a significant interaction of it with smoking.Caffeine intake is also related to smoking, and it was ourconcern that it might be in part responsible for therelationship of smoking to nuclear cataract. Caffeine is alsoa pharmacologically active substance that might affect thelens. However, we did not find this to be so in our analyses.Both education and income were inversely related toincident nuclear cataract. The relationship to income wasa bit stronger, and when both were included in a singlemodel, they did not add independently. Both of these aremarkers in a general way of lifestyle, but we are unable todetermine what specific risk factors are avoided or whichprotective factors are engendered by a better or moreprivileged lifestyle.
For cortical cataract, we found a borderline (protective)effect of multivitamin supplements. Although cigarettesmoking did not contribute independently to the model,the influence of multivitamins on risk was strengthenedafter accounting for smoking. This small change cannot beattributed with confidence in our analyses to selectiveeffects of vitamins in smokers. Were there a definite effect,we would be unable to attribute it to specific vitamins. Wenote that Kuzniarz and associates25 found a protectiveeffect to use of folate and vitamin B12 supplements oncortical cataract. The recently completed Age-Related EyeDisease Study found no effect of antioxidant supplementsand zinc on incidence or progression of any of the threetypes of age-related cataract.26
We were unable to detect a relationship of any of thelifestyle variables to posterior subcapsular cataract. Whenwe forced alcohol use into the model, we found lower oddsratios for those drinkers who imbibed up to 99 g/wk (datanot shown). Although this may be compatible with thenotion of protective effects of small to moderate amountsof alcohol for posterior subcapsular cataracts, previousanalyses of data from this cohort suggested that heavydrinkers were at increased risk but that those with smallerintakes were not really protected. Because of the relativelysmall number of cases of posterior subcapsular cataract andthe absence of a significant effect on incidence, weconclude that this exposure is unrelated to 10-year cumu-lative incidence of posterior subcapsular cataract in BeaverDam.
Cataract surgery has not been included as an endpointin this article. Although we have not found evidence of acohort effect on cataract incidence over the three 5-yearexaminations, we have found evidence of a temporal trendfor cataract surgery.27 Because the trend is likely to beinfluenced by factors related to health care delivery andpatient demand, which may or may not be related to riskfactor status, we are persuaded that attempting to attributeor relate cataract surgery to the risk factors we are describ-ing would not be helpful in trying to understand the causalrelation of these factors to cataract risk.
The purpose of these analyses was to evaluate lifestyleexposures at baseline to cumulative incidence over a10-year follow-up. Interim changes in these factors was notconsidered in the original analyses because the values atbaseline were assumed to be reasonable estimates of usualexposure. For virtually all factors, more than 50%, and insome cases more than 70%, of persons remained in thesame category of each exposure at follow-up. Thus theinterval change in exposures in this population was un-likely to have had a great influence on incidence.
We note several limitations to our study. We may beunderestimating the effects of some risk factors to thecataract endpoints because of selective survival, for exam-ple, smokers tend to die younger, and this may haveoccurred before a cataract was detected. Interim valuesbetween baseline and follow-up visits for risk factors werenot included in our analyses. This may have led to aninaccurate estimate of the true effect of such exposures oncataracts. This could be especially important if there areages of altered vulnerability to deleterious risk factors. Wehave no specific evidence to support this possibility.Cataract surgery also may have influenced our findings inthat we may not have documented the presence of acataract before its extraction. Thus, we would have under-estimated incident cataract in general, and because riskfactors for surgery are likely to be risk factors for cataract insome cases, we may be underestimating those effects.Moreover, if cataract surgery was done for a specificcataract type, the lens was no longer at risk to developanother form of age-related cataract. Variability in photo-graphic documentation leading to misclassification of casestatus may have altered our ability to identify or accuratelyquantitate risk relationships.
As we noted in the Methods section, we assume thatonce an endpoint has been reached, improvement cannotoccur. There is some variability in grading that may lead tomisclassification, however.28 Such error is likely to lead todiminished significance of a relationship of lifestyle factorsto the endpoints. The effect of such variability in gradinghas been reported and is low.28
In conclusion, we found that incident nuclear cataractwas (inversely) associated with income (or education) andsmoking (directly) 10 years earlier. We are unable todetermine which factors specific to the more privilegedlifestyle implied by higher income and education areprotective against nuclear cataract. We found no signifi-cant lifestyle factors associated with cortical or posteriorsubcapsular cataracts.
REFERENCES
1. Harding JJ, van Heyninggen R. Beer, cigarettes, and militarywork as risk factors for cataract. Dev Ophthalmol 1989;17:13–16.
2. Munoz B, Tajchman U, Bochow T, West S. Alcohol use and
SOCIOECONOMIC AND LIFESTYLE FACTORS AND CATARACTSVOL. 136, NO. 3 511
risk of posterior subcapsular opacities. Arch Ophthalmol1993;111:110–112.
3. Hodge WG, Whitcher JP, Satariano W. Risk factors forage-related cataracts. Epidemiol Rev 1995;17:336–346.
4. Hiller R, Sperduto RO, Podgor MJ, et al. Cigarette smokingand the risk of development of lens opacities. The Framing-ham Studies. Arch Ophthalmol 1997;115:1113–1118.
5. Cumming RG, Mitchell P. Alcohol, smoking, and cataracts.The Blue Mountains Eye Study. Arch Ophthalmol 1997;115:1296–1303.
6. Delcourt C, Cristol JP, Tessier F, Leger CL, Michel F, PapozL. Risk factors for cortical, nuclear and posterior subcapsularcataracts: the POLA Study. Pathologies Oculaires Liees al’Age. Am J Epidemiol 2000;151:497–504.
7. Anonymous. Risk factors associated with age-related nuclearand cortical cataract: a case-control study in the Age-RelatedEye Disease Study, AREDS Report No. 5. Ophthalmology2001;108:1402–1408.
8. Klein BEK, Klein R, Lee KE. Incident cataract after afive-year interval and lifestyle factors: The Beaver Dam EyeStudy. Ophthal Epidemiol 1999;6:247–255.
9. Marnot MG, Kogeviras M, Elston MA. Socio/economicstatus and disease. Ann Rev Public Health 1987;8:111–135.
10. Kahn HA, Leibowitz HM, Ganley JP, et al. The FraminghamEye Study. II. Association of ophthalmic pathology withsingle variables previously measured in the FraminghamHeart Study. Am J Epidemiol 1977;106:33–41.
11. Klein BE, Klein R. Cataracts and macular degeneration inolder Americans. Arch Ophthalmol 1982;100:571–573.
12. Tielsch JM, Sommer A, Katz J, et al. Socioeconomic statusand visual impairment among urban Americans. Arch Oph-thalmol 1991;109:637–641.
13. Leske MC, Chylack LT Jr, Wu S-Y, Lens Opacities Case-Control Study Group. The Lens Opacities Case-ControlStudy. Risk factors for cataract. Arch Ophthalmol 1991;109:244–251.
14. Klein R, Klein BEK, Jensen SC, Moss SE, Cruickshanks KJ.The relation of socioeconomic factors to age-related cataract,maculopathy, and impaired vision. The Beaver Dam EyeStudy. Ophthalmology 1994;101:1969–1979.
15. Campbell JA, Palit CD. Total digit dialing for a small areacensus by phone. Presented at the 1988 conference of the
American Statistical Association. Proceedings of the SurveyResearch Methods Section, 1988:549–551.
16. Klein R, Klein BEK, Linton KLP, De Mets DL. The BeaverDam Eye Study: Visual acuity. Ophthalmology 1991;98:1310–1315.
17. Klein R, Klein BEK, Lee KE. Changes in visual acuity in apopulation. The Beaver Dam Eye Study. Ophthalmology1996;103:1169–1178.
18. Klein R, Klein BEK, Lee KE, Cruickshanks KJ, Chappell RJ.Changes in visual acuity in a population over a 10-yearperiod. The Beaver Dam Eye Study. Ophthalmology 2001;108:1757–1766.
19. Klein BEK, Klein R, Linton KLP, Magli YL, Neider MW.Assessment of cataracts from photographs in the Beaver DamEye Study. Ophthalmology 1990;97:1428–1433.
20. American Society of Health-System Pharmacists. AmericanHospital Formulary Service drug information. Bethesda, MD:American Society of Health-System Pharmacists, 2000.
21. Kaplan EL, Meier P. Nonparametric estimation from incom-plete observations. J Am Stat Assoc 1958;53:457–481.
22. SAS Institute. SAS/STAT. User’s Guide: Version 8. Volume1. 4th ed. Cary, NC: 1990.
23. Zeger SL, Liang KY. Longitudinal data analysis for discreteand continuous outcomes. Biometrics 1986;42:121–130.
24. Klein BEK, Klein R, Linton KLP, Franke T. Cigarettesmoking and lens opacities. The Beaver Dam Eye Study.Am J Preventive Med 1993;9:27–30.
25. Kuzniarz M, Mitchell P, Cumming RG, Flood VM. Use ofvitamin supplements and cataract: the Blue Mountains EyeStudy. Am J Ophthalmol 2001;132:19–26.
26. [Anonymous]. A randomized, placebo-controlled, clinicaltrial of high-dose supplementation with vitamins C and Eand beta carotene for age-related cataract and vision loss:AREDS report no. 9. Arch Ophthalmol 2001;119:1439–1452.
27. Klein BEK, Klein R, Lee KE. Incidence of age-relatedcataract over a 10-year interval. The Beaver Dam Eye Study.Ophthalmology 2002;109:2052–2057.
28. Klein BEK, Klein R, Lee KE. Incidence of age-relatedcataract. The Beaver Dam Eye Study. Arch Ophthalmol1998;116:219–225.
AMERICAN JOURNAL OF OPHTHALMOLOGY512 SEPTEMBER 2003