Embed Size (px)
Citation preview
RESEARCH ARTICLE Open Access
Social participation and mental health:moderating effects of gender, social role andruralityDaisuke Takagi1*, Katsunori Kondo2 and Ichiro Kawachi3
Abstract
Background: Previous studies have reported that older people’s social participation has positive effects on theirhealth. However, some studies showed that the impacts of social participation on health differ by gender. We soughtto examine whether the effects of social participation on mental health differ for men and women in a Japanesepopulation. We also examined the moderating influence of social position within the organization as well as urban/rural locality.
Methods: We used two waves of the Aichi Gerontological Evaluation Study’s longitudinal survey, which targetedresidents with aged 65 years or over (n = 2,728) in a central part of Japan. The first wave survey was conducted in 2003,and the second wave in 2006. Depressive symptoms of the study participants were assessed using the short version ofthe Geriatric Depression Scale (GDS-15). A multilevel logistic regression model was used with individual-level as level 1and the school district-level as level 2.
Results: We found that higher social participation and performing key roles in the organization had protective effectson depressive symptoms for women. However, there were no main effects of these variables for the mental health ofmen. We found an interaction between social participation, organizational position, and rural residence among menonly. That is, men who occupied leadership positions in organizations reported better mental health, but only in ruralareas.
Conclusions: Our findings support the notion that increasing the opportunities for social participation improves olderpeople’s heath, especially for women. However, in the rural Japanese context, offering men meaningful roles withinorganizations may be important.
Keywords: Japan, Social participation, Older people, Gender difference, Depressive symptoms, Key roles, Rural areas,Multilevel analysis
BackgroundStudies from the field of gerontology have reported thatolder people’s social participation is associated with higherlife satisfaction, higher self-esteem, lower rates of admis-sion to a nursing homes, as well as lower mortality [1-3].Generally, it is thought that social participation contrib-utes to health by providing a sense of meaning in people’slives as well as increasing access to social support [4]. Forexample, volunteer activities improve mental health by
increasing the participants’ range of social networks, aswell as their social prestige, access to resources and emo-tional gratification [5]. People’s social relationships formedby social participation lead to fulfillment of attachment,esteem, social approval, belongingness, social identity andsecurity. Antonucci & Jackson [6] and Bandura [7] statedthat such social relationships are useful because they arehelpful to develop self-efficacy.Some studies have reported that the effects of social par-
ticipation vary depending on people’s background socialcharacteristics. For example, previous reports found thatsocial participation produces bigger benefits for the healthof women than for men. Kavanagh et al. [8], for example,
* Correspondence: [email protected] School of Medicine, The University of Tokyo, 7-3-1 Hongo,Bunkyo-ku, Tokyo 113-0033, JapanFull list of author information is available at the end of the article
© 2013 Takagi et al.; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the CreativeCommons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, andreproduction in any medium, provided the original work is properly cited.
Takagi et al. BMC Public Health 2013, 13:701http://www.biomedcentral.com/1471-2458/13/701

examined whether the effect of neighborhood-level polit-ical participation on self rated health differs according ongender. They found that neighborhood-level political par-ticipation enhanced women’s self rated health, but had nosignificant effect on men’s health. Spanish research onolder people also showed that friendship connections areassociated with a protective effect on cognitive impair-ment for women, but not for men [9]. A gender differencein the health effects of religious participation has also beenreported. Norton et al. [10] reported that frequent attend-ance at church is associated with low prevalence of de-pressive symptoms among women, but it is associated inthe opposite direction (i.e. with higher prevalence of de-pression) among men.In contrast to the foregoing studies, some findings in-
dicate that women can be negatively affected by socialparticipation. Under certain circumstances, high socialparticipation can contribute to higher psychological dis-tress for women because of “role strain” associated withthe duty of providing support to others [4]. Strazdins &Broom [11] refer to the gendered norms regarding theduty to provide “emotional labor” within social relations.Based on the concept of role strain, Morrow-Howell et al.
[12] examined the interaction effects of gender and partici-pation in volunteer activities on self rated health, functionaldependency and depressive symptoms, using panel datafrom three time points in the U.S. Although their resultssuggested that participation in volunteer activities positivelyaffects the three health outcomes, none of the interactioneffects between gender and participation were statisticallysignificant. It is possible that there is a socially optimal levelof social participation. Musick et al. [13] pointed out thatboth too little participation and too frequent participationin volunteer activities are more likely to be associated withnegative impacts on the health of older people.In the present study, we sought to address the question
of whether the health effects of social participation vary bygender in a Japanese population. In addition, we sought toexamine whether the gender difference in the effect of so-cial participation has further interaction effects with otherfactors. First, the effect of social participation on healthmay vary according to the position occupied by the indi-vidual within the organization in which she/he partici-pates. The theory of role strain suggests that it is moreemotionally taxing when people assume positions of re-sponsibility over others in the organization. Generally, be-cause the role strain and emotional labor tend to be aburden for women [4,11], we predict that the interactioneffect of social participation and performing key roles isstronger for women’s mental health than for men’s.A second possible factor relevant for the health effects
of social participation is urban/rural location. Personalnetworks in rural areas are more exclusive and closerthan those in urban areas. In Japanese rural areas, the
predominantly agricultural mode of production (i.e. ricefarming) ensures that social bonds are tightly knit. For cen-turies, rice farmers in rural communities have developednorms of cooperation regarding water allocation (for irriga-tion of rice paddies) and mutual assistance during times ofplanting/harvesting. While highly functional in the sphereof production, these closely-knit communities may alsocramp people’s freedom by producing sanctions againstnon-conformists. In places where such bonding networksexist, negative externalities such as intolerance are likely tobe produced. Portes [14] pointed out the “excess claims ongroup members” as one of the downsides of social capital.Under such circumstances, over-involvement in the com-munity (via social participation) may actually be a burdenon people’s mental health. In Japan, the proportion of olderpeople is much higher in rural areas than in urban areas,and tight bonding capital is also more likely to be observedin such areas. Thus, we were interested in examining theinteraction effects between social participation and rurallocation in the Japanese context.To our knowledge, there is little research that examines
the interaction effect of older people’s social participation,role in organizations, and the urban/rural context of com-munity on their mental health. Thus, the present studycontributes to theoretical aspect of this field by reveal-ing the complex interaction effect and develops prac-tical aspect by suggesting the different manner of olderpeople’s social participation according to sex and com-munity characteristics.
MethodsDataData from the Aichi Gerontological Evaluation Study(AGES) project [15] were used for this study. The presentstudy used longitudinal data from two time points. First,in 2003, investigators for the AGES project mailed a postalsurvey to 23,152 residents over the age of 65 years residingin 5 municipalities in Aichi Prefecture, Japan (The prefec-tures of Japan are the country’s 47 subnational jurisdic-tions. Prefectures are government bodies larger than cities,towns and villages – comparable of the states in the U.S.).In one of the five municipalities, simple random sampling(n = 5,000) was carried out from the Census of all individ-ual aged over 65 years. In the remaining four municipal-ities, all residents aged 65 or older were sampled (i.e. acensus was taken). The participation rate across the fivesites was 52.0%, which is comparable to community-basedsurveys of this type.In 2006, the investigators conducted the second wave
survey based on the baseline respondents. In the sec-ond wave survey, the investigators mailed a postal sur-vey to 11,991 residents who responded to the firstsurvey. The response rate was 65.5% (n = 7,855). Ourstudy protocol and informed consent procedure were
Takagi et al. BMC Public Health 2013, 13:701 Page 2 of 8http://www.biomedcentral.com/1471-2458/13/701
approved by the Ethics Committee of Nihon FukushiUniversity.In the analysis, respondents with missing values in sex,
age, annual household income, the number of family mem-bers, years of education, marital status, social participation,roles in the organizations, and the Geriatric DepressionScale were omitted. 3,477 respondents were omitted be-cause they were missing values for the above variables. Inaddition, in order to analyze the incidence (i.e. new occur-rence) of depressive symptoms from 2003 to 2006, respon-dents who already had depressive symptoms in 2003 wereomitted (i.e. 1,650 respondents were excluded due to de-pressive symptoms at baseline). As a result, the number ofindividual observations used in the analysis was 2,728(Men = 1,541, Women = 1,187).We conducted a multilevel regression analysis to take
account of neighborhood-level contexts. The spatial unitin our multilevel analysis was elementary school district,of which there were 31 in our dataset. The school district-level data of this project was prepared by Hanibuchi [16].For Japan as a whole, there are 19,672 school districts,and the average area of each school district is 16.86 km2
(SD = 38.59). In our dataset each district has an averagearea of 6.34 km2 (SD = 3.86). In Japan, a school districtis defined as the primary residential spatial unit ofpeople because local residents’ communities, senior citi-zens clubs, sports clubs etc. are organized within eachdistrict. Generally, a school district represents a geo-graphical scale in which the elderly can travel easily byfoot or bicycle. Thus, the present study used the schooldistrict as a proxy for the neighborhoods of people inour sample. The average number of respondents used inanalysis per school district was 88.
MeasurementsDemographic variablesSex of respondents, age, annual household income, thenumber of family members, years of education, andmarital status were included as sociodemographic co-variates. For annual household income, respondentswere asked to identify their income level from the 14predetermined categories (1 = less than 500 thousandyen, 2 = 500 thousand - 1 million yen, 3 = 1–1.5 millionyen, 4 = 1.5 - 2 million yen, 5 = 2–2.5 million yen, 6 =2.5 - 3 million yen, 7 = 3–4 million yen, 8 = 4–5 millionyen, 9 = 5–6 million yen, 10 = 6–7 million yen, 11 = 7–8million yen, 12 = 8–9 million yen, 13 = 9–10 millionyen, 14 = more than 10 million yen). Using the annualhousehold income and the number of family members,we created a variable of equivalised annual income, div-iding the household income by the square root of thenumber of family members.Years of education was obtained from responses to the
question asking them to mark one response out from 4
categories (1 = less than 6 years, 2 = 6–9 years, 3 = 10–12 years, 4 =more than 13 years).For marital status, respondents who were married and
their spouse was alive at the time of survey were codedas 1 otherwise coded as 0.All of these variables used in the analysis were re-
sponses from the first wave survey.
Social participation and key rolesSocial participation was assessed by asking whether the re-spondents participated in the following 8 types of group intheir neighborhood: Political group, Industry group / Tradeassociation, Volunteer group, Civic / Consumer movementgroup, Religious group, Sport group, Neighborhood associ-ation / Senior citizens’ club, and Hobby group. Responsesto each item was binarized (i.e., respondents who partici-pated in the group was coded as 1 otherwise coded as 0 foreach item). We chose not to create an index of participationby summing the groups because the alpha coefficient of thecombined items was low (0.521 for Kuder-Richardson’sKR20). Thus, the present study used the 1st principal com-ponent score of these items as the social participation indexvariable. Table 1 shows a summary of the principal compo-nent analysis. We used the tetrachoric correlation matrix inthis analysis because these items were binary.After asking the social participation question, we asked
respondents whether they have occupied key roles withinthe organization such as president, facilitator or treasurer.Respondents responded in the affirmative were coded as 1otherwise coded as 0.For the variables of social participation and key role, we
used the measurements from the baseline wave survey.
Outcome variableWe used depressive symptoms as our health outcome. Thisvariable was measured both at the baseline survey in 2003and the second wave survey in 2006. Depressive symptoms
Table 1 Summary of the principal component analysis
Factor loadingCommunality1st principal
component
Political group .641 .410
Industry group/ Trade association .480 .231
Volunteer group .760 .578
Civic/Consumer movement group .803 .644
Religious group .368 .135
Sport group .556 .309
Neighborhood associaiton/Seniorcitizens’club
.582 .338
Hobby group .602 .363
Eigenvalue 3.001
Contribution 37.600
Takagi et al. BMC Public Health 2013, 13:701 Page 3 of 8http://www.biomedcentral.com/1471-2458/13/701
were measured by the short version of the Geriatric De-pression Scale (GDS-15), using simple yes/no format, suit-able for self-administration [17]. We used a cut-off pointof 5 or above to indicate crassness of depressive symp-toms. Previous validation studies of the short form GDShave reported that the sensitivity for clinical depressionusing a cut-off point of 5 ranges from 80% to 100%, whilethe specificity ranges from 56% to 90.5%. Therefore, thestudies have concluded that a cut-off point of 5 was ap-propriate for the use of GDS as a screening tool for de-pression among community-dwelling elderly in the U.S.and Japan [17-20].The present study used responses from respondents
who did not report depressive symptoms at the first wavesurvey. That is, respondents who reported newly devel-oped depressive symptoms from 2003 to 2006 were codedas 1, and respondents who remained symptom-free werecoded as 0.
Neighborhood-level urban/rural locationWe predicted that neighborhood rural location affects theeffect of social participation on health. Thus, in order tocreate a cross-level interaction term, we used the schooldistrict-level proportion of workers engaged in primary in-dustry (agriculture), following Hanibuchi [16] who usedthe primary industrial workers rate as one of indicators ofrurality.
Statistical analysisOn average, 88 respondents were nested within 31 neigh-borhoods (school district). A multilevel logistic regressionmodel was used with individual-level as level 1 and theschool district-level as level 2. The software used wasHLM6.To examine whether there were gender differences in
the relationship between social participation and depres-sive symptoms, we stratified the analyses by gender. In theanalysis, we included the interaction term of social partici-pation (centered on the mean) and key role in order toexamine how social participation with key roles affectsmental health. In addition, to test whether neighborhoodrural location moderates the association between socialparticipation and health, we included a third-order cross-level interaction term, individual-level social participationx key roles x neighborhood rural location.
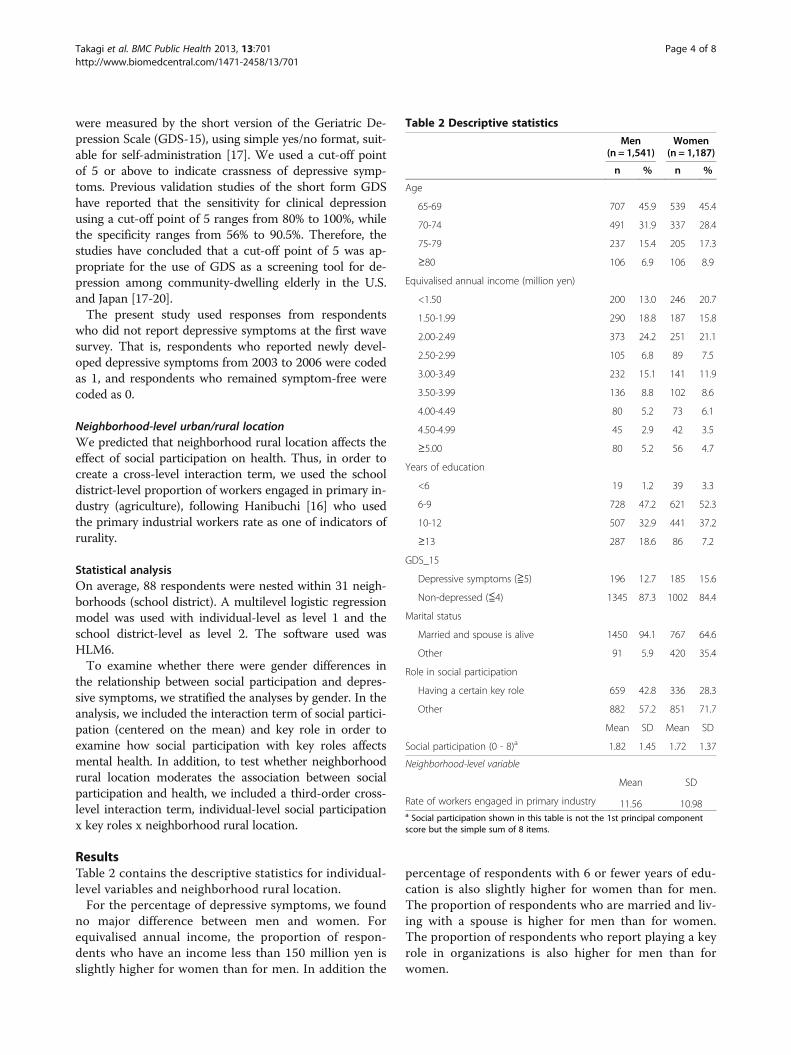
ResultsTable 2 contains the descriptive statistics for individual-level variables and neighborhood rural location.For the percentage of depressive symptoms, we found
no major difference between men and women. Forequivalised annual income, the proportion of respon-dents who have an income less than 150 million yen isslightly higher for women than for men. In addition the
percentage of respondents with 6 or fewer years of edu-cation is also slightly higher for women than for men.The proportion of respondents who are married and liv-ing with a spouse is higher for men than for women.The proportion of respondents who report playing a keyrole in organizations is also higher for men than forwomen.
Table 2 Descriptive statistics
Men(n = 1,541)
Women(n = 1,187)
n % n %
Age
65-69 707 45.9 539 45.4
70-74 491 31.9 337 28.4
75-79 237 15.4 205 17.3
≥80 106 6.9 106 8.9
Equivalised annual income (million yen)
<1.50 200 13.0 246 20.7
1.50-1.99 290 18.8 187 15.8
2.00-2.49 373 24.2 251 21.1
2.50-2.99 105 6.8 89 7.5
3.00-3.49 232 15.1 141 11.9
3.50-3.99 136 8.8 102 8.6
4.00-4.49 80 5.2 73 6.1
4.50-4.99 45 2.9 42 3.5
≥5.00 80 5.2 56 4.7
Years of education
<6 19 1.2 39 3.3
6-9 728 47.2 621 52.3
10-12 507 32.9 441 37.2
≥13 287 18.6 86 7.2
GDS_15
Depressive symptoms (≧5) 196 12.7 185 15.6
Non-depressed (≦4) 1345 87.3 1002 84.4
Marital status
Married and spouse is alive 1450 94.1 767 64.6
Other 91 5.9 420 35.4
Role in social participation
Having a certain key role 659 42.8 336 28.3
Other 882 57.2 851 71.7
Mean SD Mean SD
Social participation (0 - 8)a 1.82 1.45 1.72 1.37
Neighborhood-level variable
Mean SD
Rate of workers engaged in primary industry 11.56 10.98a Social participation shown in this table is not the 1st principal componentscore but the simple sum of 8 items.
Takagi et al. BMC Public Health 2013, 13:701 Page 4 of 8http://www.biomedcentral.com/1471-2458/13/701
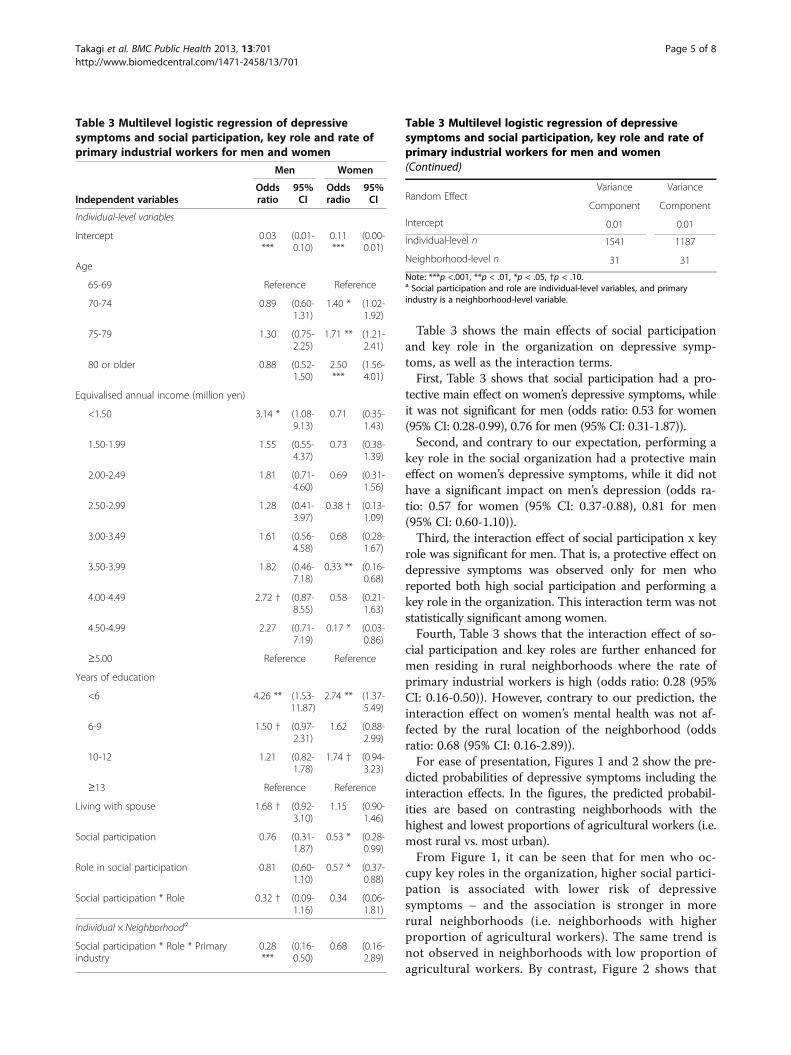
Table 3 shows the main effects of social participationand key role in the organization on depressive symp-toms, as well as the interaction terms.First, Table 3 shows that social participation had a pro-
tective main effect on women’s depressive symptoms, whileit was not significant for men (odds ratio: 0.53 for women(95% CI: 0.28-0.99), 0.76 for men (95% CI: 0.31-1.87)).Second, and contrary to our expectation, performing a
key role in the social organization had a protective maineffect on women’s depressive symptoms, while it did nothave a significant impact on men’s depression (odds ra-tio: 0.57 for women (95% CI: 0.37-0.88), 0.81 for men(95% CI: 0.60-1.10)).Third, the interaction effect of social participation x key
role was significant for men. That is, a protective effect ondepressive symptoms was observed only for men whoreported both high social participation and performing akey role in the organization. This interaction term was notstatistically significant among women.Fourth, Table 3 shows that the interaction effect of so-
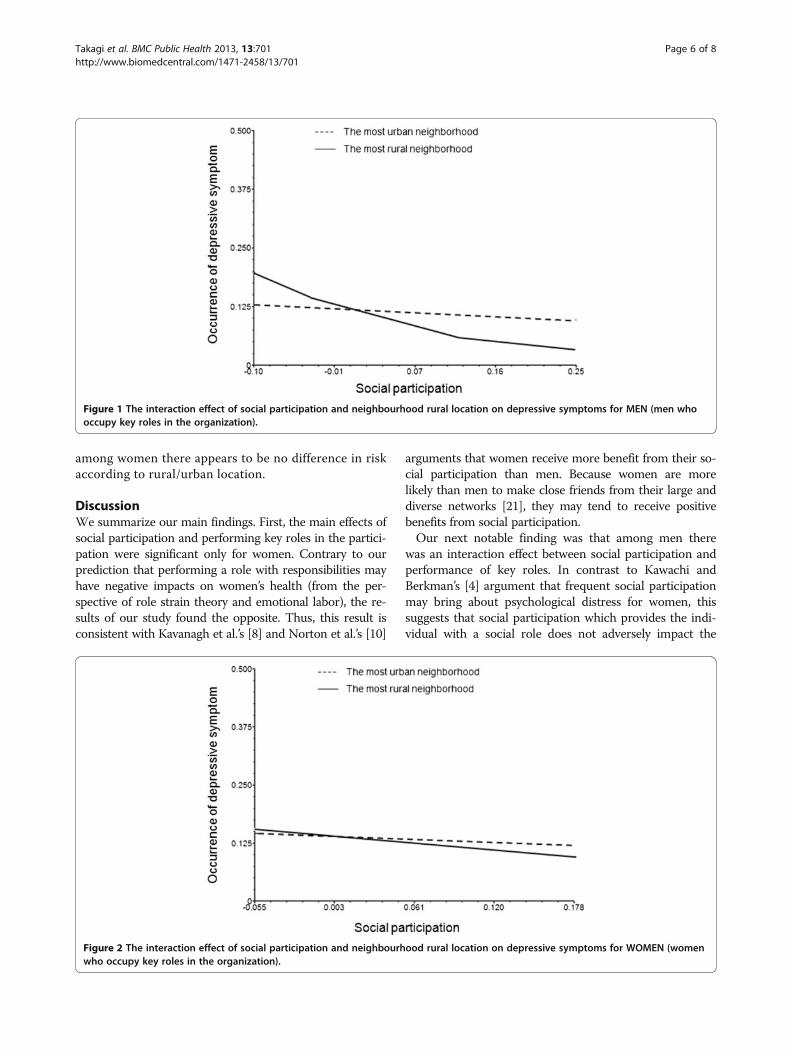
cial participation and key roles are further enhanced formen residing in rural neighborhoods where the rate ofprimary industrial workers is high (odds ratio: 0.28 (95%CI: 0.16-0.50)). However, contrary to our prediction, theinteraction effect on women’s mental health was not af-fected by the rural location of the neighborhood (oddsratio: 0.68 (95% CI: 0.16-2.89)).For ease of presentation, Figures 1 and 2 show the pre-
dicted probabilities of depressive symptoms including theinteraction effects. In the figures, the predicted probabil-ities are based on contrasting neighborhoods with thehighest and lowest proportions of agricultural workers (i.e.most rural vs. most urban).From Figure 1, it can be seen that for men who oc-
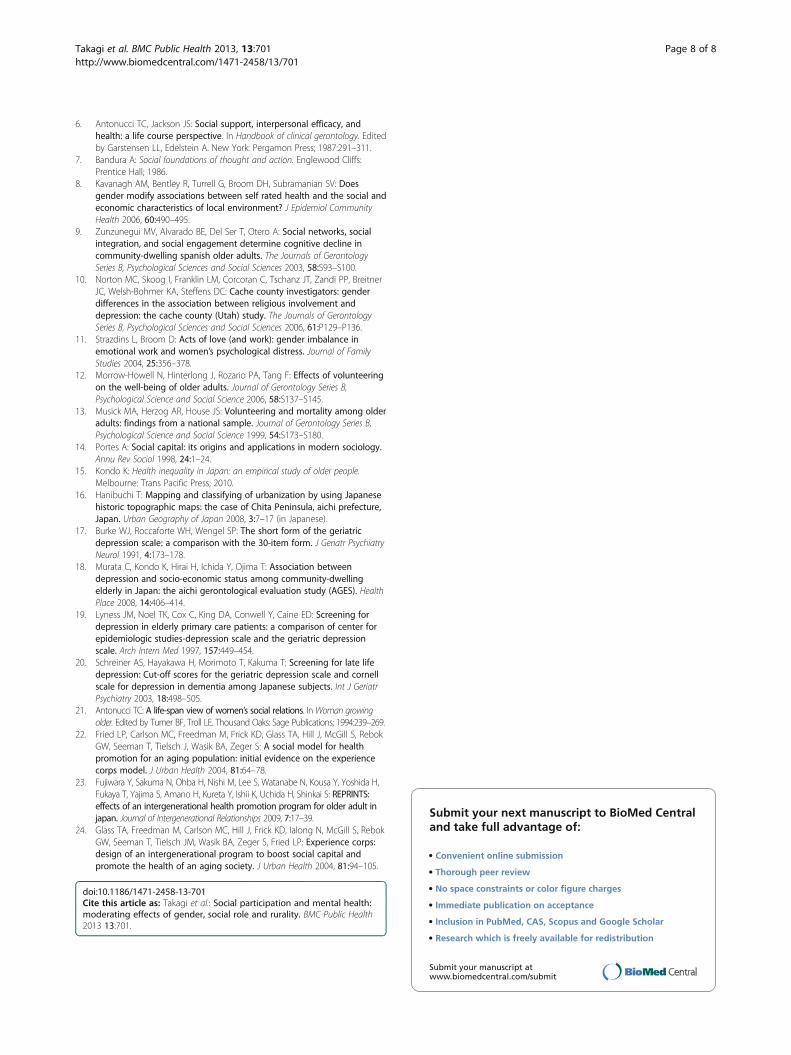
cupy key roles in the organization, higher social partici-pation is associated with lower risk of depressivesymptoms – and the association is stronger in morerural neighborhoods (i.e. neighborhoods with higherproportion of agricultural workers). The same trend isnot observed in neighborhoods with low proportion ofagricultural workers. By contrast, Figure 2 shows that
Table 3 Multilevel logistic regression of depressivesymptoms and social participation, key role and rate ofprimary industrial workers for men and women
Independent variables
Men Women
Oddsratio
95%CI
Oddsradio
95%CI
Individual-level variables
Intercept 0.03***
(0.01-0.10)
0.11***
(0.00-0.01)
Age
65-69 Reference Reference
70-74 0.89 (0.60-1.31)
1.40 * (1.02-1.92)
75-79 1.30 (0.75-2.25)
1.71 ** (1.21-2.41)
80 or older 0.88 (0.52-1.50)
2.50***
(1.56-4.01)
Equivalised annual income (million yen)
<1.50 3.14 * (1.08-9.13)
0.71 (0.35-1.43)
1.50-1.99 1.55 (0.55-4.37)
0.73 (0.38-1.39)
2.00-2.49 1.81 (0.71-4.60)
0.69 (0.31-1.56)
2.50-2.99 1.28 (0.41-3.97)
0.38 † (0.13-1.09)
3.00-3.49 1.61 (0.56-4.58)
0.68 (0.28-1.67)
3.50-3.99 1.82 (0.46-7.18)
0.33 ** (0.16-0.68)
4.00-4.49 2.72 † (0.87-8.55)
0.58 (0.21-1.63)
4.50-4.99 2.27 (0.71-7.19)
0.17 * (0.03-0.86)
≥5.00 Reference Reference
Years of education
<6 4.26 ** (1.53-11.87)
2.74 ** (1.37-5.49)
6-9 1.50 † (0.97-2.31)
1.62 (0.88-2.99)
10-12 1.21 (0.82-1.78)
1.74 † (0.94-3.23)
≥13 Reference Reference
Living with spouse 1.68 † (0.92-3.10)
1.15 (0.90-1.46)
Social participation 0.76 (0.31-1.87)
0.53 * (0.28-0.99)
Role in social participation 0.81 (0.60-1.10)
0.57 * (0.37-0.88)
Social participation * Role 0.32 † (0.09-1.16)
0.34 (0.06-1.81)
Individual × Neighborhooda
Social participation * Role * Primaryindustry
0.28***
(0.16-0.50)
0.68 (0.16-2.89)
Table 3 Multilevel logistic regression of depressivesymptoms and social participation, key role and rate ofprimary industrial workers for men and women(Continued)
Random EffectVariance Variance
Component Component
Intercept 0.01 0.01
Individual-level n 1541 1187
Neighborhood-level n 31 31
Note: ***p <.001, **p < .01, *p < .05, †p < .10.a Social participation and role are individual-level variables, and primaryindustry is a neighborhood-level variable.
Takagi et al. BMC Public Health 2013, 13:701 Page 5 of 8http://www.biomedcentral.com/1471-2458/13/701
among women there appears to be no difference in riskaccording to rural/urban location.
DiscussionWe summarize our main findings. First, the main effects ofsocial participation and performing key roles in the partici-pation were significant only for women. Contrary to ourprediction that performing a role with responsibilities mayhave negative impacts on women’s health (from the per-spective of role strain theory and emotional labor), the re-sults of our study found the opposite. Thus, this result isconsistent with Kavanagh et al.’s [8] and Norton et al.’s [10]
arguments that women receive more benefit from their so-cial participation than men. Because women are morelikely than men to make close friends from their large anddiverse networks [21], they may tend to receive positivebenefits from social participation.Our next notable finding was that among men there
was an interaction effect between social participation andperformance of key roles. In contrast to Kawachi andBerkman’s [4] argument that frequent social participationmay bring about psychological distress for women, thissuggests that social participation which provides the indi-vidual with a social role does not adversely impact the
Figure 1 The interaction effect of social participation and neighbourhood rural location on depressive symptoms for MEN (men whooccupy key roles in the organization).
Figure 2 The interaction effect of social participation and neighbourhood rural location on depressive symptoms for WOMEN (womenwho occupy key roles in the organization).
Takagi et al. BMC Public Health 2013, 13:701 Page 6 of 8http://www.biomedcentral.com/1471-2458/13/701

mental health of women, and may even promote the mentalhealth of men. This also suggests that occupying a key pos-ition within an organization a necessary condition for mento receive positive effects from their social participation.The same interaction effect was not found for women’s de-pressive symptoms. In Japanese society, which is character-ized by strong patriarchal values, males seek meaning andidentity by being valued in the workplace (as opposed to inthe home). This orientation may spill over into retirement,such that men feel rewarded by seeking positions of au-thority of responsibility within the social organizations inwhich they participate. The present study’s suggestion thatit is important to have roles in social participation for re-tired men is critical for developing community-based inter-ventions to promote the health of elders.A third notable finding of our study is the cross-level
interaction effect between social participation x perform-ance of key roles x rural residence. As Figure 1 shows, thisresult suggests that the interaction effect of social partici-pation and key roles on depressive symptoms is enhanced(for men) in rural areas, while the interaction effect isnon-significant in urban areas. Although we predicted thatclosed networks are more likely to be formed in ruralareas and that such networks might be associated with ad-verse effects on mental health, our results suggested theopposite – primarily boosting the mental health of menwho perform key roles. In contrast to rural areas, openand mobile networks are more likely to be formed inurban areas, but the extent of cohesion in such networkstends to be low and the degree of members’ cooperationmay also be low. In such a setting, performing key rolesmay add to mental burden. Our results offer new insightinto health promotion among the elderly, and shed lighton the interaction between the social context and socialparticipation.In addition, because our analyses focused on only new oc-
currence of depressive symptoms (i.e. respondents whoalready had depressive symptoms at baseline were excluded),the causal interpretation of our findings is strengthened.Parallel with providing some novel insights into the the-
oretical aspects of older people’s social participation, ourresults also suggest some practical implications. In thehealth promotion literature, increasing the opportunitiesfor social participation has been suggested as a means ofimproving older people’s health [22-24]. Our findings sup-port that notion, but also suggest complexities based ongender.Some limitations of our study should be noted. The
present study used the proportion of agricultural workersas a proxy indicator of rural status. In addition, the charac-teristics of social network (tightly bonded) in Japanese ruralareas described in this paper are speculative, and requirefurther ethnographic elaboration. Ideally, instead of usingurban/rural as the indicator, a more theoretically-grounded
approach would have been to stratify the analyses basedupon network characteristics such as size, closeness, open-ness and mobility. Future studies should measure such de-tailed characteristics and incorporate them into the analyses.Second, a high number of respondents were omitted
from our analyses because of missing values. Generally,missing responses tend to be higher among older peopleand in mail surveys. The missing responses may havebiased the findings of our study.
ConclusionOur findings support the notion that increasing theopportunities for social participation improve olderpeople’s health, especially for women, but also suggestnuances based on the social context (Japanese society),sociodemographic characteristics (gender), social pos-ition (whether occupying key roles within organiza-tions), and location (rural vs. urban) – that is, in therural Japanese context, offering men meaningful roleswithin organizations may be important.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsDT performed the statistical analysis and drafted the manuscript. KK madesubstantial contributions to design and acquisition of data. IK revised thedrafted manuscript critically for important intellectual content. All authorsread and approved the final manuscript.
AcknowledgementsThis study used data from the Aichi Gerontological Evaluation Study (AGES),conducted by the Nihon Fukushi University Center for Well-being andSociety as one of their research projects. This study was supported in part bya grant of Strategic Research Foundation Grant-aided Project for PrivateUniversities from Ministry of Education, Culture, Sport, Science, andTechnology, Japan (MEXT). The authors thank Drs Toshiyuki Ojima, TatsuoYamamoto, Masayo Kojima, Naoki Kondo, Masashige Saito and YukinobuIchida for their helpful comments on this study.
Author details1Graduate School of Medicine, The University of Tokyo, 7-3-1 Hongo,Bunkyo-ku, Tokyo 113-0033, Japan. 2Center for Well-being and Society, NihonFukushi University, 5-22-35 Chiyoda, Naka-ku, Nagoya-shi, Aichi 460-0012,Japan. 3Harvard School of Public Health, Harvard University, 677 HuntingtonAvenue, Boston, MA 02115, USA.
Received: 17 March 2013 Accepted: 29 July 2013Published: 31 July 2013
References1. Glass TA, De Leon CM, Marottoli RA, Berkman LF: Population based study
of social and productive activities as predictors of survival amongelderly americans. BMJ 1999, 319:478–483.
2. Reitzes DC, Mutran EJ, Verrill LA: Activities and self-esteem: continuing thedevelopment of activity theory. Res Aging 1995, 17:260–277.
3. Unger JB, McAvay G, Bruce ML, Berkman LF, Seeman T: Validation in the impactof social network characteristics on physical functioning in elderly persons:MacArthur studies of successful aging. The Journals of Gerontology Series B,Psychological Sciences and Social Sciences 1999, 54:S245–S251.
4. Kawachi I, Berkman LF: Social ties and mental helath. J Urban Health 2001,78:458–467.
5. Moen P, Dempster-McClain D, Williams R: Successful aging: a life-courseperspective on women’s multiple roles and health. Am J Sociol 1992,97:1612–1638.
Takagi et al. BMC Public Health 2013, 13:701 Page 7 of 8http://www.biomedcentral.com/1471-2458/13/701
6. Antonucci TC, Jackson JS: Social support, interpersonal efficacy, andhealth: a life course perspective. In Handbook of clinical gerontology. Editedby Garstensen LL, Edelstein A. New York: Pergamon Press; 1987:291–311.
7. Bandura A: Social foundations of thought and action. Englewood Cliffs:Prentice Hall; 1986.
8. Kavanagh AM, Bentley R, Turrell G, Broom DH, Subramanian SV: Doesgender modify associations between self rated health and the social andeconomic characteristics of local environment? J Epidemiol CommunityHealth 2006, 60:490–495.
9. Zunzunegui MV, Alvarado BE, Del Ser T, Otero A: Social networks, socialintegration, and social engagement determine cognitive decline incommunity-dwelling spanish older adults. The Journals of GerontologySeries B, Psychological Sciences and Social Sciences 2003, 58:S93–S100.
10. Norton MC, Skoog I, Franklin LM, Corcoran C, Tschanz JT, Zandi PP, BreitnerJC, Welsh-Bohmer KA, Steffens DC: Cache county investigators: genderdifferences in the association between religious involvement anddepression: the cache county (Utah) study. The Journals of GerontologySeries B, Psychological Sciences and Social Sciences 2006, 61:P129–P136.
11. Strazdins L, Broom D: Acts of love (and work): gender imbalance inemotional work and women’s psychological distress. Journal of FamilyStudies 2004, 25:356–378.
12. Morrow-Howell N, Hinterlong J, Rozario PA, Tang F: Effects of volunteeringon the well-being of older adults. Journal of Gerontology Series B,Psychological Science and Social Science 2006, 58:S137–S145.
13. Musick MA, Herzog AR, House JS: Volunteering and mortality among olderadults: findings from a national sample. Journal of Gerontology Series B,Psychological Science and Social Science 1999, 54:S173–S180.
14. Portes A: Social capital: its origins and applications in modern sociology.Annu Rev Sociol 1998, 24:1–24.
15. Kondo K: Health inequality in Japan: an empirical study of older people.Melbourne: Trans Pacific Press; 2010.
16. Hanibuchi T: Mapping and classifying of urbanization by using Japanesehistoric topographic maps: the case of Chita Peninsula, aichi prefecture,Japan. Urban Geography of Japan 2008, 3:7–17 (in Japanese).
17. Burke WJ, Roccaforte WH, Wengel SP: The short form of the geriatricdepression scale: a comparison with the 30-item form. J Geriatr PsychiatryNeurol 1991, 4:173–178.
18. Murata C, Kondo K, Hirai H, Ichida Y, Ojima T: Association betweendepression and socio-economic status among community-dwellingelderly in Japan: the aichi gerontological evaluation study (AGES). HealthPlace 2008, 14:406–414.
19. Lyness JM, Noel TK, Cox C, King DA, Conwell Y, Caine ED: Screening fordepression in elderly primary care patients: a comparison of center forepidemiologic studies-depression scale and the geriatric depressionscale. Arch Intern Med 1997, 157:449–454.
20. Schreiner AS, Hayakawa H, Morimoto T, Kakuma T: Screening for late lifedepression: Cut-off scores for the geriatric depression scale and cornellscale for depression in dementia among Japanese subjects. Int J GeriatrPsychiatry 2003, 18:498–505.
21. Antonucci TC: A life-span view of women’s social relations. InWoman growingolder. Edited by Turner BF, Troll LE. Thousand Oaks: Sage Publications; 1994:239–269.
22. Fried LP, Carlson MC, Freedman M, Frick KD, Glass TA, Hill J, McGill S, RebokGW, Seeman T, Tielsch J, Wasik BA, Zeger S: A social model for healthpromotion for an aging population: initial evidence on the experiencecorps model. J Urban Health 2004, 81:64–78.
23. Fujiwara Y, Sakuma N, Ohba H, Nishi M, Lee S, Watanabe N, Kousa Y, Yoshida H,Fukaya T, Yajima S, Amano H, Kureta Y, Ishii K, Uchida H, Shinkai S: REPRINTS:effects of an intergenerational health promotion program for older adult injapan. Journal of Intergenerational Relationships 2009, 7:17–39.
24. Glass TA, Freedman M, Carlson MC, Hill J, Frick KD, Ialong N, McGill S, RebokGW, Seeman T, Tielsch JM, Wasik BA, Zeger S, Fried LP: Experience corps:design of an intergenerational program to boost social capital andpromote the health of an aging society. J Urban Health 2004, 81:94–105.
doi:10.1186/1471-2458-13-701Cite this article as: Takagi et al.: Social participation and mental health:moderating effects of gender, social role and rurality. BMC Public Health2013 13:701.
Submit your next manuscript to BioMed Centraland take full advantage of:
• Convenient online submission
• Thorough peer review
• No space constraints or color figure charges
• Immediate publication on acceptance
• Inclusion in PubMed, CAS, Scopus and Google Scholar
• Research which is freely available for redistribution
Submit your manuscript at www.biomedcentral.com/submit
Takagi et al. BMC Public Health 2013, 13:701 Page 8 of 8http://www.biomedcentral.com/1471-2458/13/701