Embed Size (px)
Citation preview
Social & Behaviour Change Communication
Insights and Strategy Case Study:Open Defecation in India
Author: Amina Tarraf Editors: Kalyani Rajan, Laura Citron
Introduction
Improving public health in developing countries requires both demand and supply. In addition to building public health infrastructure and services, individual and social behaviour must change to ensure that there is demand for public health services. There is an important role for social and behaviour change communications to address these demand-side barriers to public health.
Open defecation in India is an important case study. It demonstrates the importance of linking research-led insights with communications strategy. The supply-led approach of building latrines has failed to significantly reduce the harmful practice of open defecation, two-thirds of households with a government-supplied latrine still have a family member who defecates in the open1. In October 2014, the Prime Minister of India launched a new Clean India Mission (‘Swachh Bharat’) that focuses on large-scale social and behaviour change to increase demand for and use of latrines, alongside improving sanitation infrastructure.
This report is based upon field work and qualitative research as well as desk research. In it, we illustrate how behaviour change communications approaches can be used to tackle an ingrained public health challenge. Taking open defecation in India as a case study, we follow a four-step process to develop an effective social and behaviour change strategy. The process is based on UNICEF guidelines and Thompson Social | J. Walter Thompson’s proprietary tools. In our experience, a rigorous and evidence-based approach to communications strategy development produces campaigns with the greatest impact.
1 15 Coffey, Diane, Aashish Gupta, Payal Hathi, Nidhi Khurana, Dean Spears, Nikhil Srivastav, and Sangita Vyas. SQUAT Survey – Revealed Preference for Open Defecation: Evidence from a New Survey in Rural North India.
2

Problem Analysis
• What is happening? • What is the impact?• What needs to change?
Behavioural Drivers and Barriers
• Why are people and communities behaving this way?• What are the social trends, values and beliefs driving behaviour?• How do these differ across audience segments?
Communications Objective
• What is the role for communications to achieve the policy goal?• What are the communications levers that could change behaviour?
Communications Strategy
• Which target audiences need to be reached to achieve the change?• Which messages will drive the change?• What is the most effective way to reach the target audiences?• How should the messages be delivered?• How will impact be evaluated?
We found that the key to eliminating open defecation is to make young children develop the habit of using latrines or toilets. This will break the inter-generational cycle of open defecation.
Communication can support this by changing the social norms around open defecation in communities. At the moment, the social norm is that open defecation is acceptable and sometimes even healthier than latrine use. There is low awareness that it leads to health problems. The strategy is to use communications to create a new social norm that open defecation is dirty, disgusting and bad for children’s health.
This strategic process is supported by primary and secondary research. Once the strategy is completed, we would then move into content development, testing, implementation, optimisation and evaluation.
3
Executive SummaryThis report offers analysis of rural India’s open defecation problem and proposes recommendations for a communications strategy to address the issue through tools and channels of Behaviour Change Communication (BCC). The structure of the report is inspired by both UNICEF’s guidelines on writing a communications strategy for development programmes and the proprietary tools used by Thompson Social | J. Walter Thompson for strategy development. The report addresses the issue through:
Section IAn analysis of Open Defecation (OD) in rural India; the primary factors that lead people to indulge in it and the consequences of the practice on health, gender equality, and the economy.
Section IIAn analysis of the Swachh Bharat Mission (Gramin)2 (SBM- G); the challenges that the programme faces in enabling sustainable rural sanitation, a detailed analysis of the key stakeholders and beneficiaries, and the roles of key players in the communications process.
Section IIIRecommendations on a behaviour change communications (BCC) strategy to help implement the objectives of SBM-G through effective behaviour and attitude change channels and tools.
2 The Prime Minister of India, Narendra Modi, launched the Swachh Bharat Mission (The Clean India Mission) in October 2014. The Mission includes two sub-missions: the Swachh Bharat Gramin Mission (The Clean India Rural Mission) and the Swachh Bharat Urban Mission. The Ministry of Drinking Water and Sanitation is responsible for the Mission in rural areas and the Ministry of Urban Development is responsible for the Mission in urban areas. Through the Mission, the government aims to achieve ODF (Open Defecation Free) status for India by 2019.
A Behaviour Change Communication Strategy to Combat Open Defecation in Rural India
4
Global Situation“Open defecation refers to the practice whereby people go out in fields, bushes, forests, open bodies of water, or other open spaces rather than using the toilet to defecate.”3 Two and a half billion people live without access to improved sanitation and hygiene facilities resulting in 1 billion (15%) of the world population defecating in the open. Open defecation (OD) perpetuates a vicious cycle of disease and poverty making sanitation and hygiene among the most important drivers of health, social and economic environments4.
Many countries have accomplished great progress in tackling the issue. Vietnam and Bangladesh “where more than one in three people relieved themselves in the open in 1990 – virtually stamped out the practice entirely by 2012”.5 This led to a decrease in the global number from 1.3 billion in 1990 to 1 billion today. 90% of people who live in rural areas still defecate in the open. The practice is on the rise in 26 countries in Sub-Saharan Africa, with Nigeria the least compliant. Open defecation has risen in the Sub-Saharan region from 23 million in 1990 to 39 million in 2012.
National SituationIndia is the capital of open defecation (OD), accounting for 59% of the practice in the world. Almost 638 million people defecate in the open, leaving 65 million kilograms of faeces on streets, rail tracks and fields every day.6 The 2011 census showed that out of the 246.6 households surveyed, only 46.9% have toilets and 3.2% use public toilets, leaving the remaining 49.8% simply defecating in the open.7 The practice has been widely accepted for generations, becoming a well-established tradition deeply ingrained from early childhood and is almost an accepted part of the Indian landscape. OD is rampant in rural India where it is practiced by nearly 70% of the rural population, compared to 13% in urban areas.
I. Situation Analysis
3 “Eliminate Open Defecation | UNICEF.” UNICEF India. UNICEF, n.d. Web. 03 Aug. 2015.4 “International Decade for Action ‘Water for Life’ 2005-2015.” United Nations Department of Economic and Social Affairs
(UNDESA). UN Water, n.d. Web. 03 Aug. 2015.
5 Miles, Tom. “One Billion People Still Defecate in Public Despite Health Risks-UN.” Reuters, 8 May 2014. Web. 11 Aug. 2015.6 J Walter Thompson Social-India. UNICEF Take Poo to the Loo-AMES 2015-Asian Marketing Effectiveness and Strategy Awards.
N.p.: n.p., 2015. Print.7 Sunderarajan, P. “Half of India’s Homes Have Cellphones, but Not Toilets.” The Hindu. The Hindu, 13 Mar. 2012. Web. 03 Aug. 2015.
5
Consequences of Open Defecation (OD)• Health
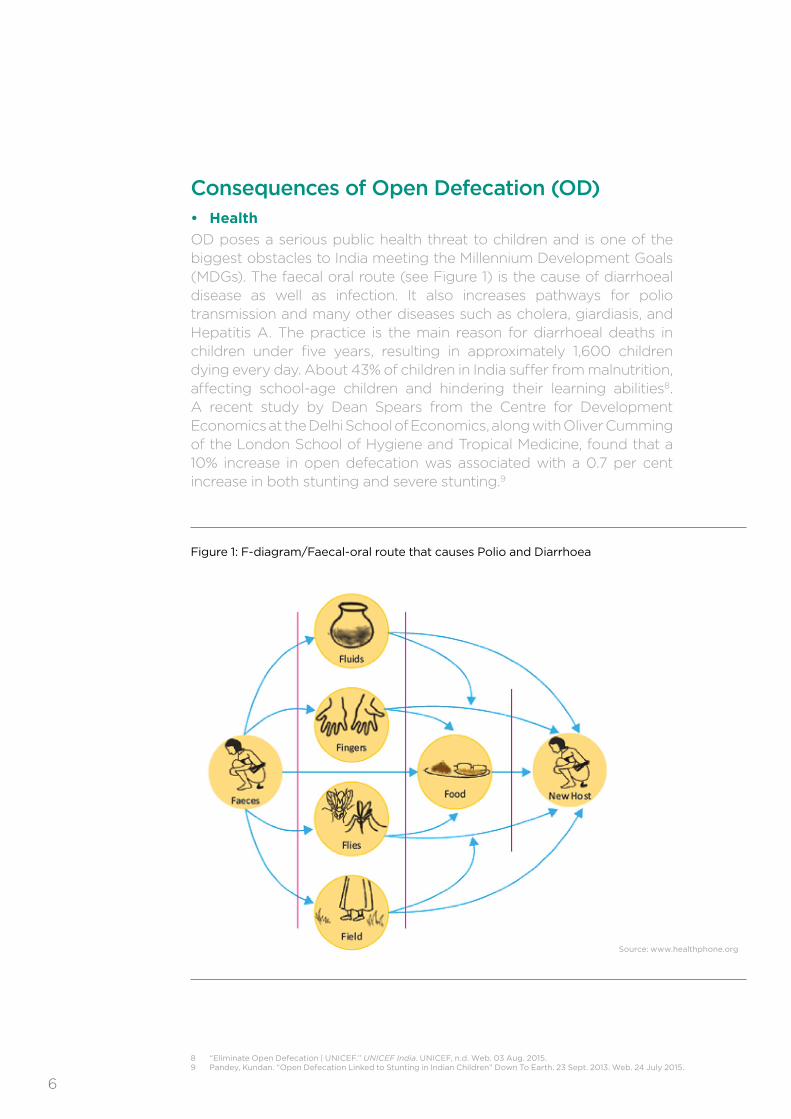
OD poses a serious public health threat to children and is one of the biggest obstacles to India meeting the Millennium Development Goals (MDGs). The faecal oral route (see Figure 1) is the cause of diarrhoeal disease as well as infection. It also increases pathways for polio transmission and many other diseases such as cholera, giardiasis, and Hepatitis A. The practice is the main reason for diarrhoeal deaths in children under five years, resulting in approximately 1,600 children dying every day. About 43% of children in India suffer from malnutrition, affecting school-age children and hindering their learning abilities8. A recent study by Dean Spears from the Centre for Development Economics at the Delhi School of Economics, along with Oliver Cumming of the London School of Hygiene and Tropical Medicine, found that a 10% increase in open defecation was associated with a 0.7 per cent increase in both stunting and severe stunting.9
8 “Eliminate Open Defecation | UNICEF.” UNICEF India. UNICEF, n.d. Web. 03 Aug. 2015.9 Pandey, Kundan. “Open Defecation Linked to Stunting in Indian Children” Down To Earth. 23 Sept. 2013. Web. 24 July 2015.
Source: www.healthphone.org
Figure 1: F-diagram/Faecal-oral route that causes Polio and Diarrhoea
6

• Gender
OD puts women’s dignity and safety at risk. Many women feel constrained to relieve themselves in the dark for reasons of privacy, thus exposing them to rape and sexual assault. 30% of marginalised women are violently assaulted every year as the lack of basic sanitation forces them to travel long distances to meet their needs. 24% of girls drop out of school, as many facilities do not have toilets – this problem is exacerbated when they reach menarche.10 Furthermore, recent research has established a statistically significant association between open defecation and pregnancy outcomes. According to Pinaki Panigrahi, a professor of epidemiology at the University of Nebraska Medical Centre, open defecation could have an effect on women’s genito- urinary tract due to the proximity of the vagina and the anus, which resulted in a correlation between high numbers of stillborn, preterm births and spontaneous abortions.11
• Poverty
Improper sanitation and open defecation indirectly contribute to poverty as they lead to contaminated water sources, soil and land. Once blighted by disease, children are unable to complete their formal education, and are later hindered in their capacities to work, provide for themselves and educate their children. Illness within the community’s senior population represents a significant drain on family budgets and healthcare resources. These factors only perpetuate the poverty cycle.12
• TheEconomy
Poor sanitation practices have negative effects on the economy and national development as they cripple workers’ productivity, their longevity, and their ability to invest and save. The economic impact of inadequate sanitation is about INR 2.4 trillion ($38.4 million), or 6.4 % of India’s gross domestic product.13
10 Boyd, Seren. “Snakebites, Diarrhoea and Violence: Why India’s Rural Women Need Toilets.” The Guardian. N.p., 19 Nov. 2014. Web. 15 July 2015.11 Mukunth, Vasudevan. “Open Defecation Affects Pregnancy Outcomes Too, New Study Finds.” The Wire. N.p., 9 July 2015. Web. 12 Aug. 2015.12 Arvizo, Cambria. “Open Defecation: India’s Health Hazard of the Poor-BORGEN.” BORGEN. N.p., 23 May 2014. Web. 03 Aug. 2015.13 Shivakumar, Girija. “Half of India’s Population Still Defecates in the Open.” The Hindu. N.p., 21 Nov. 2013. Web. 19 July 2015
7
Explaining Open Defecation in Rural IndiaIndia is considered an outlier with regards to open defecation, as common development indicators do not explain the widespread phenomenon.
• NotPoverty/GDP
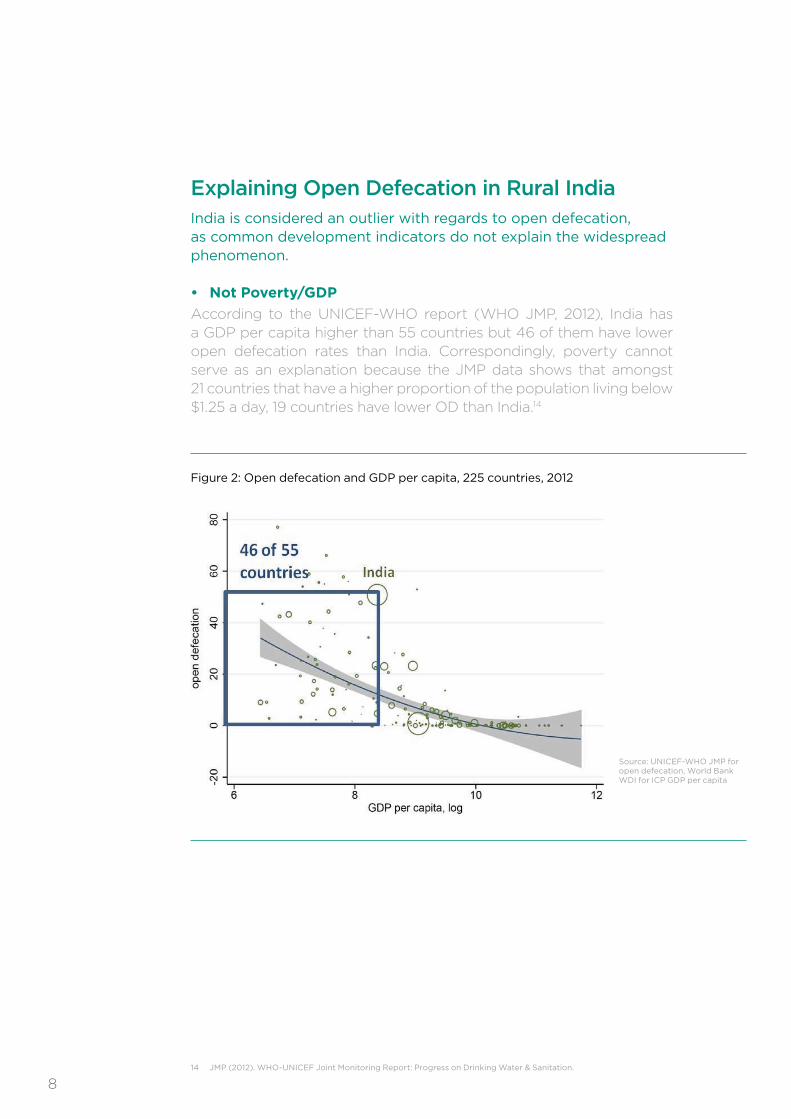
According to the UNICEF-WHO report (WHO JMP, 2012), India has a GDP per capita higher than 55 countries but 46 of them have lower open defecation rates than India. Correspondingly, poverty cannot serve as an explanation because the JMP data shows that amongst 21 countries that have a higher proportion of the population living below $1.25 a day, 19 countries have lower OD than India.14
14 JMP (2012). WHO-UNICEF Joint Monitoring Report: Progress on Drinking Water & Sanitation.
Source: UNICEF-WHO JMP for open defecation, World Bank WDI for ICP GDP per capita
Figure 2: Open defecation and GDP per capita, 225 countries, 2012
8
• NotIlliteracy
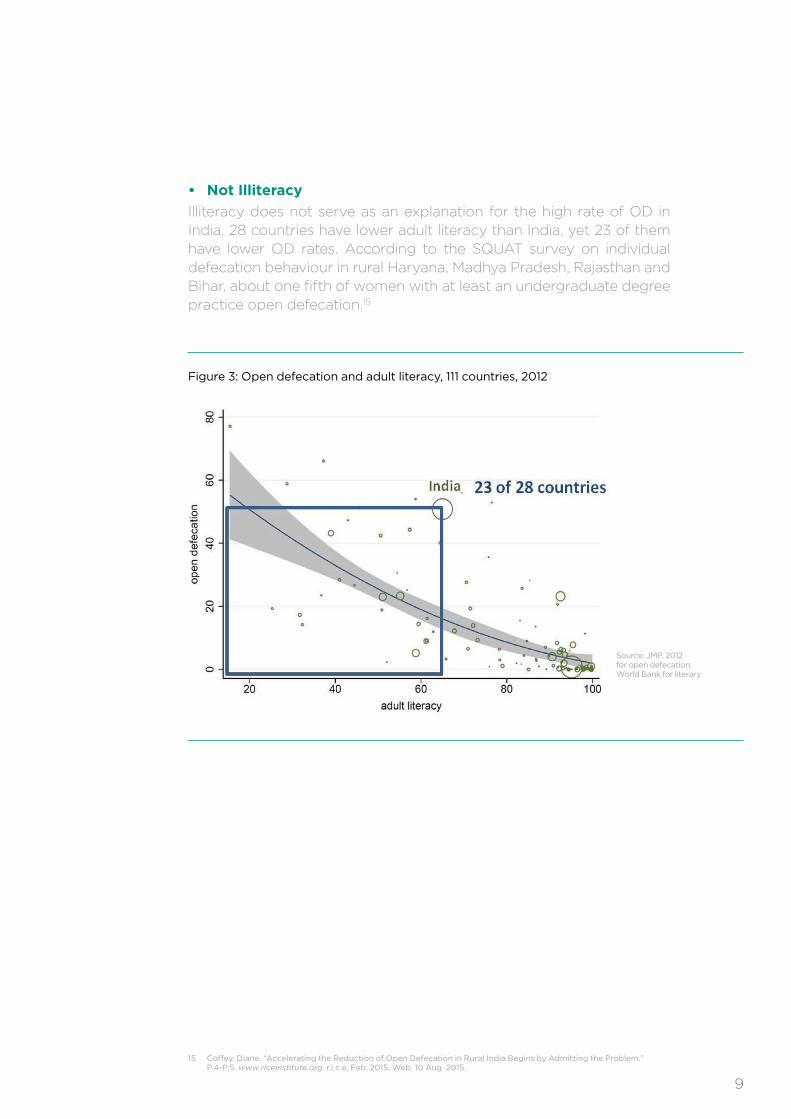
Illiteracy does not serve as an explanation for the high rate of OD in India. 28 countries have lower adult literacy than India, yet 23 of them have lower OD rates. According to the SQUAT survey on individual defecation behaviour in rural Haryana, Madhya Pradesh, Rajasthan and Bihar, about one fifth of women with at least an undergraduate degree practice open defecation.15
15 Coffey, Diane. “Accelerating the Reduction of Open Defecation in Rural India Begins by Admitting the Problem.” P.4-P.5. www.riceinstitute.org. r.i.c.e, Feb. 2015. Web. 10 Aug. 2015.
Source: JMP, 2012 for open defecation; World Bank for literary
Figure 3: Open defecation and adult literacy, 111 countries, 2012
9
16 Ibid.P.5
• NotLackofWater
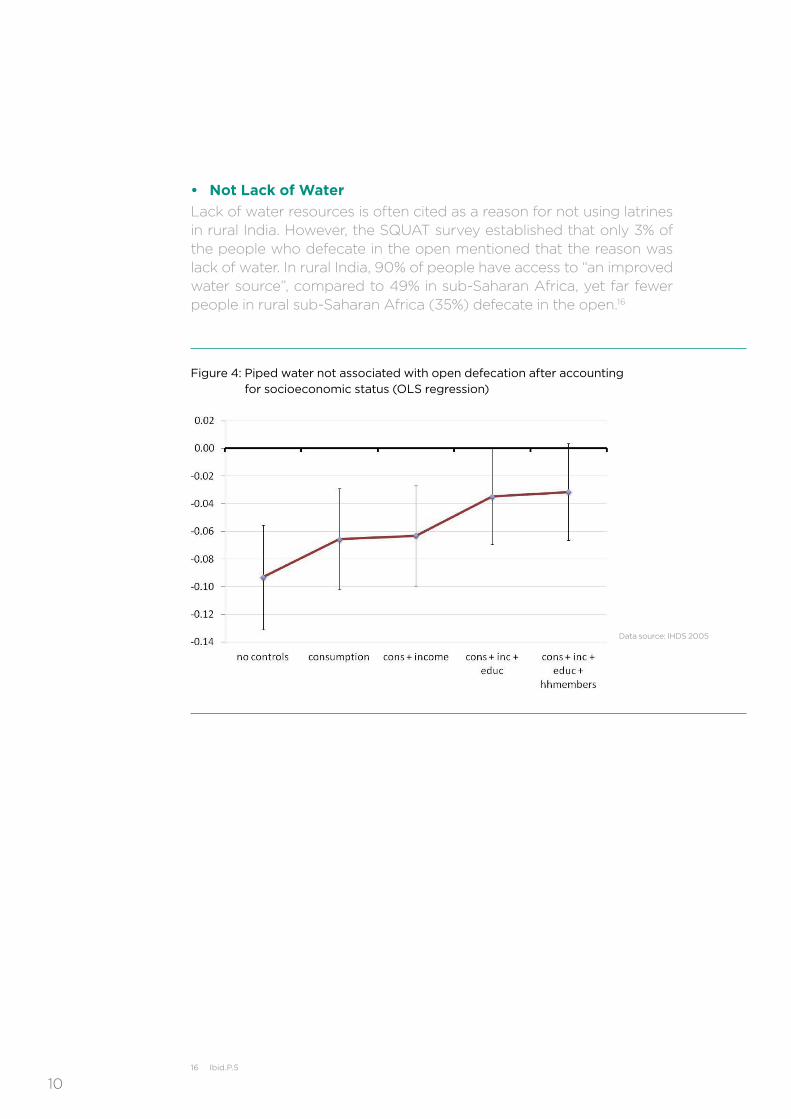
Lack of water resources is often cited as a reason for not using latrines in rural India. However, the SQUAT survey established that only 3% of the people who defecate in the open mentioned that the reason was lack of water. In rural India, 90% of people have access to “an improved water source”, compared to 49% in sub-Saharan Africa, yet far fewer people in rural sub-Saharan Africa (35%) defecate in the open.16
Data source: IHDS 2005
Figure 4: Piped water not associated with open defecation after accounting for socioeconomic status (OLS regression)
10
So Why do Indians Defecate in the Open?There are many factors affecting rural sanitation behaviours, the most salient of which are social norms, customs and traditions around open defection. Other important factors include perceptions of latrine affordability, access and availability of functioning latrines, sanitation products and services.
The SQUAT survey highlights three key insights to explain OD in rural India:
1. LackofDemandforSimple,AffordableLatrines:• Households in India rarely build the types of inexpensive latrines that
are commonly used by poor households to save lives and reduce disease in Bangladesh, South East Asia and Sub-Saharan Africa. One possible explanation is what people in rural India consider to be the requirements of an acceptable latrine. Respondents to the SQUAT survey had a very expensive concept of what makes a latrine. The latrines that the respondents described cost on average more than INR 21,000. This contributes to the view that building toilets is an unaffordable luxury. On the contrary, latrines that safely contain faeces could be built in a much less expensive manner for around INR 2,500 at purchasing power parity. The figures estimated by Indians are much higher than those of Bangladeshis and Indonesians, who allocated a figure between INR 2500-5000.17 Such perceptions can be seen as a contributing barrier to latrine construction and use in India.
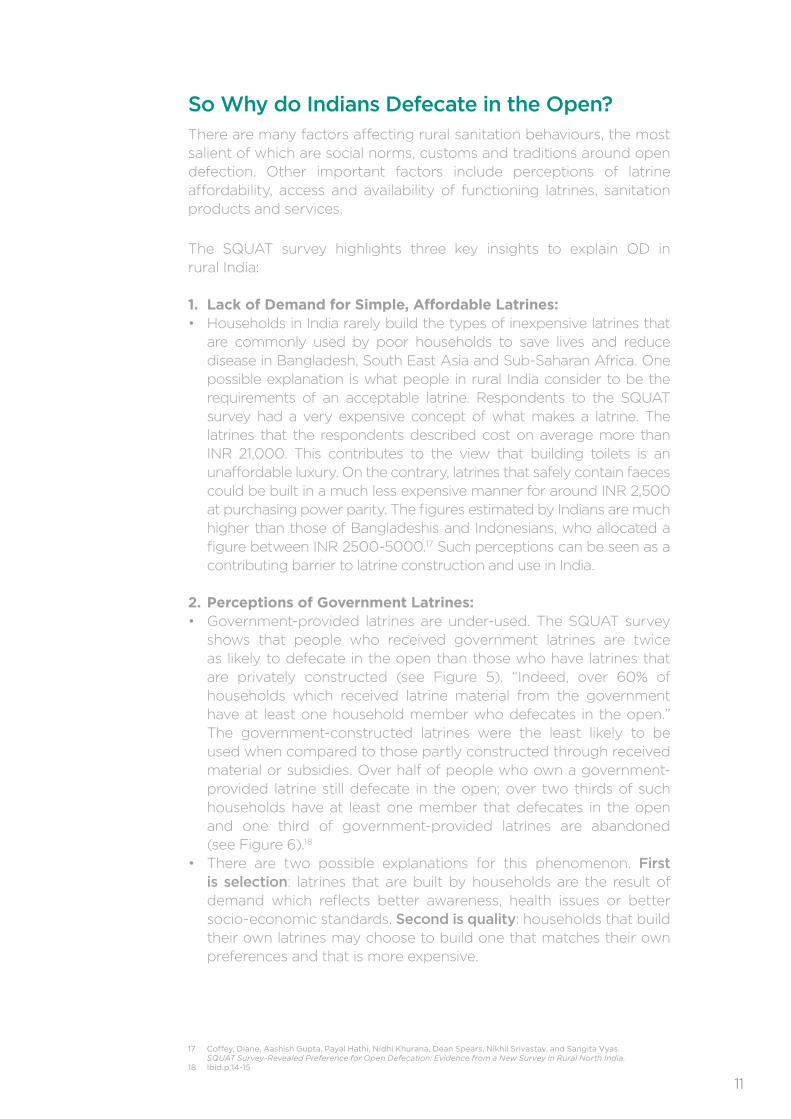
2.PerceptionsofGovernmentLatrines:• Government-provided latrines are under-used. The SQUAT survey
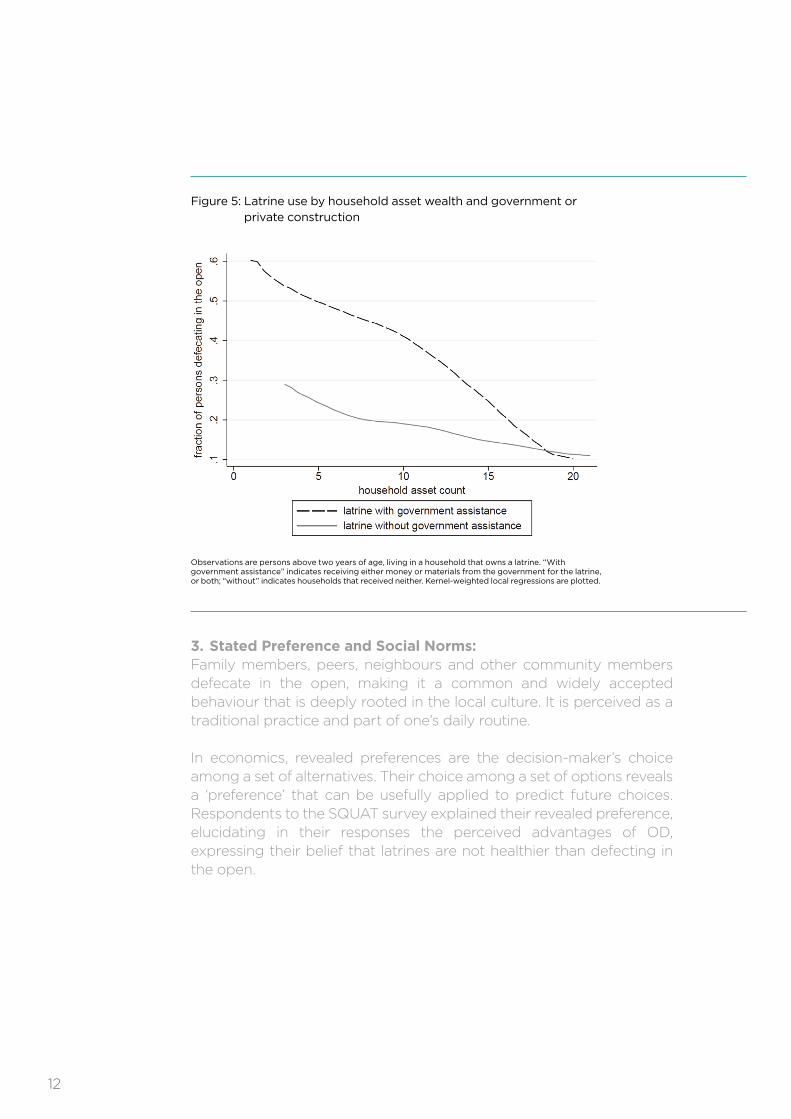
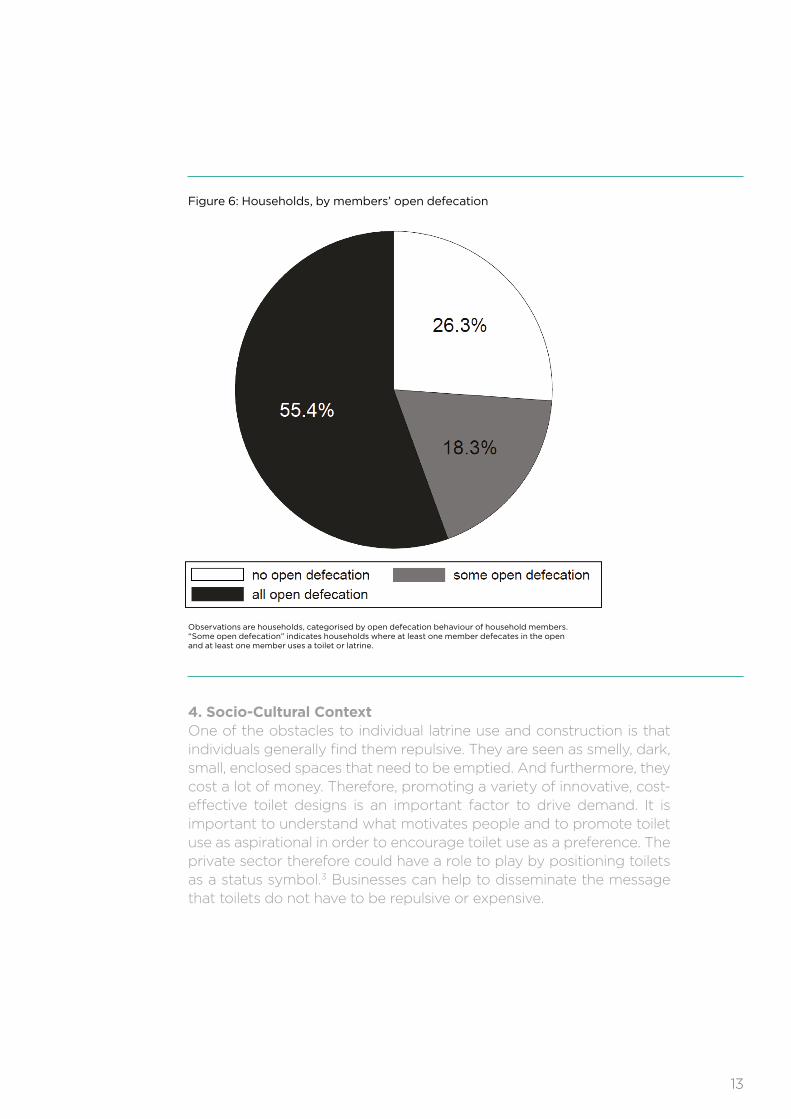
shows that people who received government latrines are twice as likely to defecate in the open than those who have latrines that are privately constructed (see Figure 5). “Indeed, over 60% of households which received latrine material from the government have at least one household member who defecates in the open.” The government-constructed latrines were the least likely to be used when compared to those partly constructed through received material or subsidies. Over half of people who own a government-provided latrine still defecate in the open; over two thirds of such households have at least one member that defecates in the open and one third of government-provided latrines are abandoned (see Figure 6).18
• There are two possible explanations for this phenomenon. First is selection: latrines that are built by households are the result of demand which reflects better awareness, health issues or better socio-economic standards. Second is quality: households that build their own latrines may choose to build one that matches their own preferences and that is more expensive.
17 Coffey, Diane, Aashish Gupta, Payal Hathi, Nidhi Khurana, Dean Spears, Nikhil Srivastav, and Sangita Vyas. SQUAT Survey-Revealed Preference for Open Defecation: Evidence from a New Survey in Rural North India.
18 Ibid.p.14-15
11
3.StatedPreferenceandSocialNorms:Family members, peers, neighbours and other community members defecate in the open, making it a common and widely accepted behaviour that is deeply rooted in the local culture. It is perceived as a traditional practice and part of one’s daily routine.
In economics, revealed preferences are the decision-maker’s choice among a set of alternatives. Their choice among a set of options reveals a ‘preference’ that can be usefully applied to predict future choices. Respondents to the SQUAT survey explained their revealed preference, elucidating in their responses the perceived advantages of OD, expressing their belief that latrines are not healthier than defecting in the open.
Observations are persons above two years of age, living in a household that owns a latrine. “With government assistance” indicates receiving either money or materials from the government for the latrine, or both; “without” indicates households that received neither. Kernel-weighted local regressions are plotted.
Figure 5: Latrine use by household asset wealth and government or private construction
12
4.Socio-CulturalContextOne of the obstacles to individual latrine use and construction is that individuals generally find them repulsive. They are seen as smelly, dark, small, enclosed spaces that need to be emptied. And furthermore, they cost a lot of money. Therefore, promoting a variety of innovative, cost-effective toilet designs is an important factor to drive demand. It is important to understand what motivates people and to promote toilet use as aspirational in order to encourage toilet use as a preference. The private sector therefore could have a role to play by positioning toilets as a status symbol.3 Businesses can help to disseminate the message that toilets do not have to be repulsive or expensive.
Observations are households, categorised by open defecation behaviour of household members.“Some open defecation” indicates households where at least one member defecates in the open and at least one member uses a toilet or latrine.
Figure 6: Households, by members’ open defecation
13
PerceivedAdvantagesofOpenDefecation
• It is associated with pleasure and comfort. 47% of respondents explain the habit by attributing it to comfort and pleasure, and 74% of those who defecate in the open despite having latrine access cite the same reason.19
• It is associated with rising up early as well as being industrious and healthy. Many respondents indicated that it gives them the opportunity to breathe some fresh air and take morning walks. 14% highlight that there are problems with using a latrine, while 12% say it is a habit.20
• Among rural Indians open defecation is not widely recognised as a health threat. 43% of respondents reported that latrines are not better for child health. Among those who practice OD 51% report that OD would be as good as latrine use for child health. The survey also highlights that women are more likely than men to cite OD as healthy for their children. The survey further emphasises the lack of health awareness; when asked, 89% of respondents said that they built latrines for reasons of comfort and convenience and only 26% mention perceived health benefits.21
• It is associated with the concept of purity in Hinduism. It is believed that one cannot eat and defecate under the same roof and must defecate as far as possible from the household.
ChallengestoRuralSanitation
To summarise, there are a set of interlinked issues for sanitation policy in rural India:
1. The widespread scale of the problem – nearly 70% of rural Indians defecate in the open.
2. High population density makes open defecation costly in India. It imposes high costs on human capital and healthcare expenditure.
3. Low demand for latrine use hinders what latrine construction can achieve in terms of solving the problem.
19 Ibid.P.2020 Ibid.P20 21 Ibid.P.21
14
22 India. Ministry of Drinking Water and Sanitation. “Swachh Bharat Mission (Gramin) Guidelines”. The Principal Secretary/Secretary I/C Sanitation. N.p., Dec. 2014. Web. Aug. 2015.
23 Gram Panchayat or Gram Panchayat(village council) is a Village Based Self Government in India.24 Ibid
• PreviousGovernmentEfforts
The government has been working consistently to respond to the rural sanitation problem since 1954. However, the 1981 Census revealed that rural sanitation coverage was only 1%. The first national programme to increase access to rural sanitation on a large scale was the Central Rural Sanitation Programme, launched in 1986. Despite considerable efforts, the approach failed to motivate and sustain sanitation efforts as it was based on the assumption that providing sanitary facilities would lead to coverage and usage.
As a result of the limitations of this approach, the Total Sanitation Campaign was launched in 1999 under the umbrella of a “demand-driven” methodology. The campaign moved away from a focus on infrastructure provision to promoting behaviour change. To add dynamism to the campaign, an incentive-based scheme was initiated for fully sanitised and open defecation free Gram Panchayats, Blocks, and Districts called the ‘Nirmal Gram Puraskar’ (NGP). “While the award gained popularity in bringing about a desire in the community for attaining Nirmal status, there have been issues of sustainability in some awardees.”22
A successor programme was launched, the “Nirmal Bharat Abhiyan” (NBA) in 2012. Its objective was to accelerate sanitation coverage in rural areas through renewed strategies. Despite the efforts there were implementation difficulties as funding from different resources caused delays.
• CurrentProgramme
SwachhBharatMissionanditsObjectives:In order to accelerate progress towards universal rural sanitation coverage, the Prime Minister of India launched the “Swachh Bharat Mission” (Clean India Mission) in October 2014. The Mission includes two sub-missions: the Swachh Bharat Mission (Gramin) and the Swachh Bharat Mission (Urban), which aims to achieve Swachh Bharat (Clean India) by 2019. The focus of this strategy will be on the Swachh Bharat Gramin, which aims at “improving the levels of cleanliness in rural areas through solid and liquid waste management activities and making Gram Panchayats23 open defecation free, clean and sanitised.24”
II. Programme Analysis
15
Mission Objectives of Swachh Bharat Mission (Gramin)
Bring about an improvement in the general quality of life in rural areas by promoting cleanliness, hygiene and eliminating open defecation.
Accelerate sanitation coverage in rural areas to achieve the vision of Swachh Bharat by 2nd October 2019.
Motivate communities and Panchayati Raj Institutions to adopt sustainable sanitation practices and facilities through awareness-creation and health education.
Encourage cost effective and appropriate technologies for ecologically safe and sustainable sanitation.
Develop wherever required, community-managed sanitation systems focusing on scientific solid and liquid waste management systems for overall cleanliness in the rural areas.
Part of the objectives include changing key behaviours. According to the joint framework developed by the Ministry and UNICEF, there are four key behaviours that need to be promoted:
1. Building, using and maintaining toilets.2. Safe disposal of child faeces.3. Hand washing with soap at critical times.4. Safe storage and handling of drinking water.
StakeholderAnalysis
In order to change hygiene practices and behaviour in rural India, a multitude of stakeholders will need to intervene on a massive scale. In terms of government bodies, the responsibility for implementation is shared between the Ministry of Urban Development (MoUD) for implementation in urban areas and the Ministry of Drinking Water and Sanitation (MDWS) for rural implementation.
The stakeholders can be categorised into five broad groups according to Thompson Social | J. Walter Thompson’s 3-tier communications model:
1. BeneficiariesBeneficiaries are at the core of any initiative, as those who are directly affected by the issue and its consequences. In the case of rural sanitation, the beneficiaries are the families affected by the high risk of infectious diseases. The main target groups are:
• Men in OD households: Men tend to see open defecation as an acceptable practice that is entrenched in their habits from early childhood. This group often choose open defecation even if there is easy access to toilets.
• Women in OD households: Women face a great deal of inconvenience due to lack of privacy and therefore they have to travel long distances to defecate in secluded areas, which makes them vulnerable to violence, assault and rape.
16
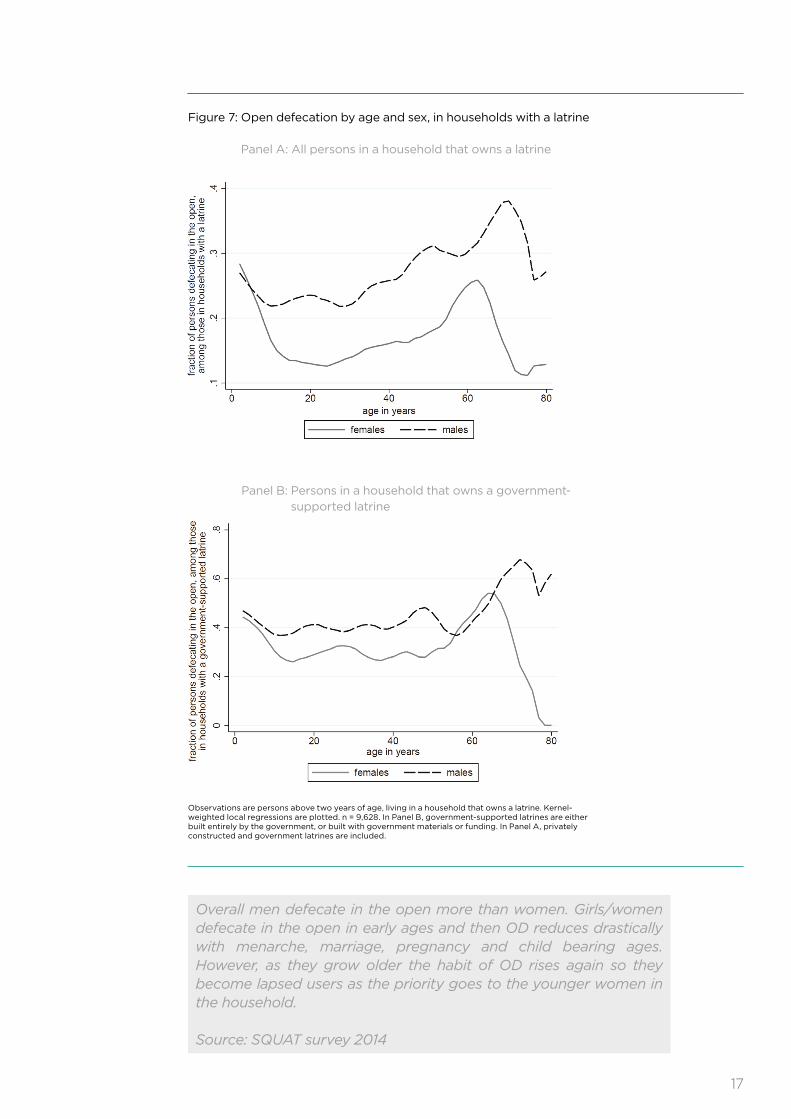
Overall men defecate in the open more than women. Girls/women defecate in the open in early ages and then OD reduces drastically with menarche, marriage, pregnancy and child bearing ages. However, as they grow older the habit of OD rises again so they become lapsed users as the priority goes to the younger women in the household.
Source: SQUAT survey 2014
Observations are persons above two years of age, living in a household that owns a latrine. Kernel-weighted local regressions are plotted. n = 9,628. In Panel B, government-supported latrines are either built entirely by the government, or built with government materials or funding. In Panel A, privately constructed and government latrines are included.
Figure 7: Open defecation by age and sex, in households with a latrine Panel A: All persons in a household that owns a latrine
Panel B: Persons in a household that owns a government-supported latrine
17
• Elders in OD households: They are comfortable with OD and they are more difficult in terms of changing behaviour. In exceptional circumstances such as illness, physical disability or lack of safety they become occasional users of toilets, but they soon go back to open defecation when circumstances change.
• Adolescent girls in OD households: This group feels the strongest need and is most in favour of toilets. Due to safety concerns, they only defecate when accompanied by older women for security. Their schools often lack toilets, which is a problem for their continuing education once they reach menarche as they have to deal with menstrual hygiene as well.
• Children in OD households: Finally, children are the most vulnerable group due to health concerns, and stand to benefit the most from using toilets.
2. Programme ImplementersThey are part of the government and are responsible for implementation; such as programme administrators at the State, District and Block level. They include the Ministry of Drinking Water and Sanitation, the Block Programme Unit (BPMU)24, the Gram Panchayat/Village Water Sanitation Committee25, the Panchayati Raj institutions26 and different government departments.
3. Service ProvidersThey are the groups that ensure the programme’s success within the community. They have a major role to play in providing services. They include the Panchayati Raj Institutions, Cooperatives, Civil Society Organisations, ANMs/AWWs/ASHAs27. Sanitary Mart Retailers, CBOs/NSS/other volunteer groups and Swachhata Doots/Swachhata Senas (Cleanliness and Sanitation Ambassadors) under the programme.
4. InfluencersThey are those who encourage change in the community and motivate community members to take action. Their role is of utmost importance as they are close to the families and the community. They can exercise influence through being role models by adopting toilets and abandoning OD themselves. In addition, they can dispel misconceptions and address the barriers. Influencers include PRI/Village Heads, religious leaders, local leaders, doctors, SHGs, Youth Groups, headmasters, school teachers and children.
24 The BPMU is the bridge between the District experts and the GPs and provides continuous support in terms of awareness generation, motivation, mobilisation, training and hand-holding of village communities, GPs and VWSCs. The BPMU serves as an extended delivery arm of the District Mission.
25 The Gram Panchayat/Village Water Sanitation Committee provides support in terms of motivation, mobilisation, implementation and supervision of the programme and manages drinking water security.
26 The Panchayati Raj functions as a system of governance in which Gram Panchayats are the basic unit of local administration.
27 ANM: Auxiliary Nurse Midwife, ASHA: Accredited Social Health Activist, AWW Anganwadi Worker (started by the Indian government in 1975 as part of the Integrated Child Development Services programme to combat child hunger and malnutrition. A typical Anganwadi centre also provides basic healthcare in Indian villages.).
18
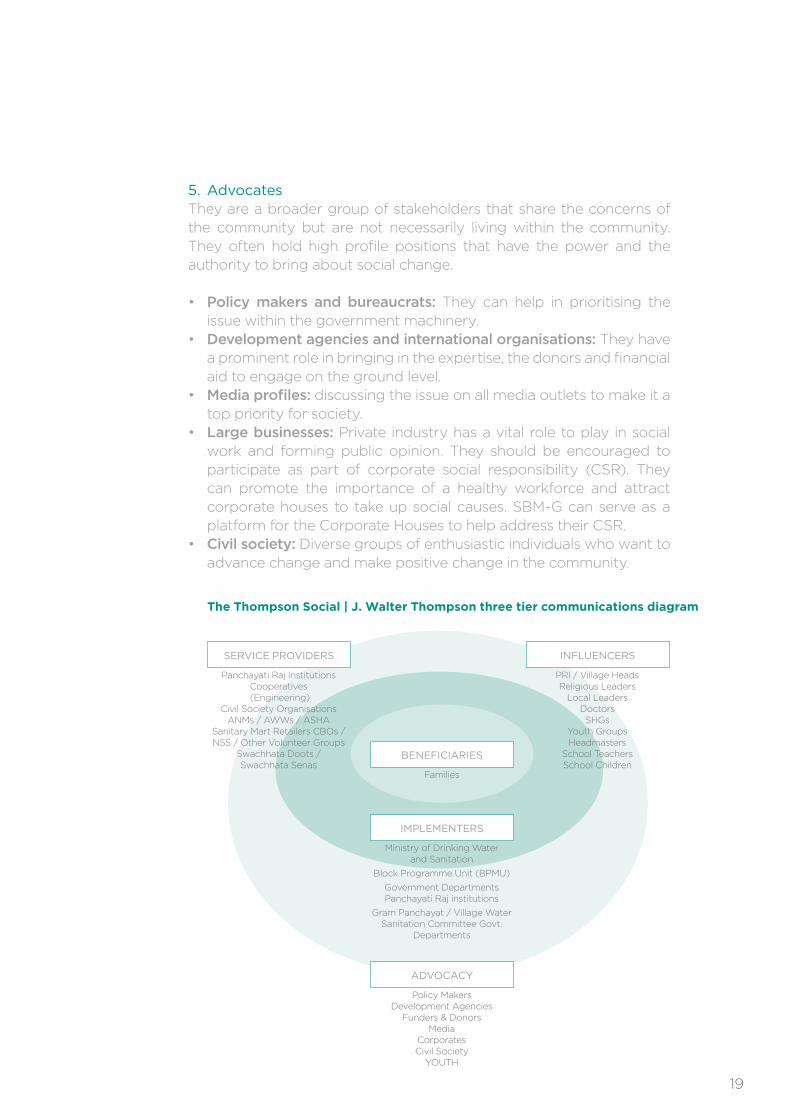
5. AdvocatesThey are a broader group of stakeholders that share the concerns of the community but are not necessarily living within the community. They often hold high profile positions that have the power and the authority to bring about social change.
• Policy makers and bureaucrats: They can help in prioritising the issue within the government machinery.
• Development agencies and international organisations: They have a prominent role in bringing in the expertise, the donors and financial aid to engage on the ground level.
• Media profiles: discussing the issue on all media outlets to make it a top priority for society.
• Large businesses: Private industry has a vital role to play in social work and forming public opinion. They should be encouraged to participate as part of corporate social responsibility (CSR). They can promote the importance of a healthy workforce and attract corporate houses to take up social causes. SBM-G can serve as a platform for the Corporate Houses to help address their CSR.
• Civil society: Diverse groups of enthusiastic individuals who want to advance change and make positive change in the community.
Panchayati Raj InstitutionsCooperatives (Engineering)
Civil Society OrganisationsANMs / AWWs / ASHA
Sanitary Mart Retailers CBOs /NSS / Other Volunteer Groups
Swachhata Doots / Swachhata Senas
SERVICE PROVIDERS
PRI / Village HeadsReligious Leaders
Local LeadersDoctorsSHGs
Youth GroupsHeadmasters
School TeachersSchool Children
INFLUENCERS
Families
BENEFICIARIES
Ministry of Drinking Water and Sanitation
Block Programme Unit (BPMU)
Government Departments Panchayati Raj institutions
Gram Panchayat / Village Water Sanitation Committee Govt.
Departments
IMPLEMENTERS
Policy Makers Development Agencies
Funders & DonorsMedia
CorporatesCivil Society
YOUTH
ADVOCACY
TheThompsonSocial|J.WalterThompsonthreetiercommunicationsdiagram
19
1. KeyProblemforCommunication
There was an increase in rural sanitation coverage in rural India from 1% in 1981 to 24.7% in 2012, according to the World Bank. However, the construction of latrines and access to sanitation have not led to regular usage by all family members. As a result, open defecation continues as a widely accepted practice with detrimental impact to health, livelihoods and the economy.
2.RoleforCommunication
Create an environment where toilet construction and regular usage is viewed as virtuous and progressive. Ensure people appreciate the importance of latrine use, so that it ultimately becomes the norm and the habit.
Most of the discourse around tackling hygiene and sanitation is linked to health arguments, but the economic benefits may not be clear to either policy makers or beneficiaries. Therefore, highlighting the economic benefits could help to change priorities and behaviours. For example, by demonstrating how better hygiene can result in less healthcare spending in the long-run and can cut part of the 6.4% of GDP expenditure on hygiene.
3.WhoaretheTargetAudiences?
Primary Audience: Parents of children aged 0- 6 years in areas where OD is widespread, because sanitation habits are generally developed and socialised at an early age.
Beneficiaries: The primary beneficiaries are families, especially children and adolescent girls.
Secondary Audience: The wider community, including opinion leaders and influencers, religious leaders, women’s groups, teachers, school management committees, PTAs, ‘cleanliness ambassadors’ called Swachhata Doots, and suppliers of sanitation products.
Tertiary Audience: Includes service providers, programme implementers and advocacy groups.
Demographics• Average Household Size. The average rural household size was
6.2 members in the lowest monthly per capita consumer expenditure (MPCE) class (compared to 3.8 in the highest MPCE class in 2003), according to the latest round of National Sample Survey on Household Consumer Expenditure and Employment.
III. Strategy
20
• Average Household Income per Month. The Socio- Economic and Caste Census (SECC) released in 2011 shows that 92% of rural households reported their maximum income below INR 10,000 per month. Nearly three quarters of all rural households said that the income of the highest earning member was INR 5,000 or less. The average per capita income is around INR 1,400.
• Number of Children. The average number of children under 15 years of age in a rural household was 3.1 in the lowest MPCE class in 2003 (compared to 0.8 in the highest MPCE class).
• Education. The literacy rate in rural areas was 71% in 2014. In rural areas, just under 4.5% of males and 2.2% of females completed graduate-level education or above.
• Occupation. Most men work in farming and agri- businesses. Agriculture continues to be a major field for women’s employment. They are not recognised as farmers and are assigned supplementary work to that of men such as weeding, winnowing and transplanting. Women are caregivers and mostly carry out household activities.
PsychographicsIn rural India, different household members prescribe to different social roles and different ranks. Males have higher social status than females within in the household; older people of the same sex have higher status than younger people; and young women have the lowest intra-household status.
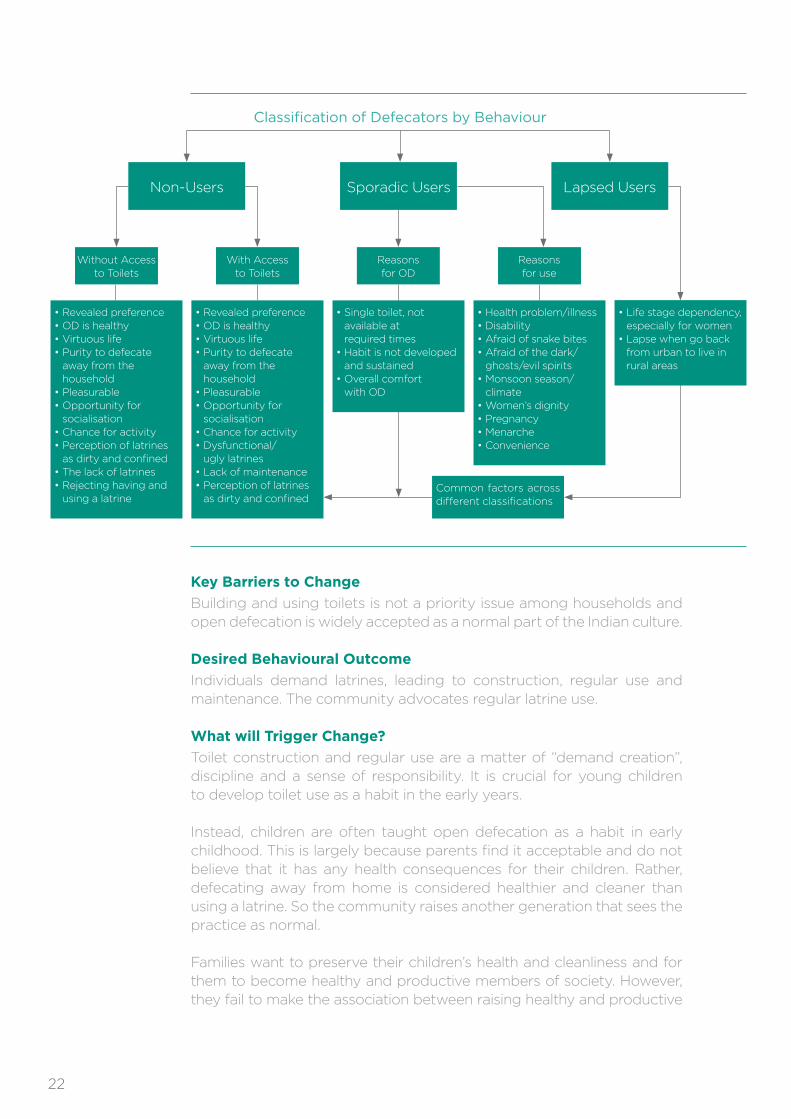
4.CurrentBehaviouralDynamics
There are three different trends with regards to open defecation and latrine use. The trends are as follows:
Non-Users. Many choose not to use toilets at all. They find it more comfortable to defecate in the open and they see it as part of their socialisation norms and habits. Furthermore, they associate open defecation with health benefits and cleanliness. Other possible reasons could be the unavailability of latrines. However, this is rarely the case as in most instances open defecation has been cited as a revealed preference.
Sporadic Users. This group are not regular latrine users although they own a latrine in the house. Sporadic latrine use could be due to illness or disability, which makes going out difficult. Some people may therefore use latrines for convenience, but as soon as the exceptional circumstances are over they lapse. Women and adolescent girls use latrines sporadically for safety, privacy and dignity. Furthermore, it is more convenient for household members to use latrines at night.
Lapsed Users. This group used toilets regularly but went back to open defecation after a while. Lapses could be age-related: for example, women who used toilets during their child rearing years and adolescence become lapsed users in their elder years. Alternatively, rural-to-urban migrants used latrines, but once they went back to living in rural areas they re- adopted the habit of open defecation.
21
Classification of Defecators by Behaviour
• Revealed preference• OD is healthy• Virtuous life• Purity to defecate
away from the household
• Pleasurable• Opportunity for
socialisation• Chance for activity• Perception of latrines
as dirty and confined• The lack of latrines• Rejecting having and
using a latrine
• Revealed preference• OD is healthy• Virtuous life• Purity to defecate
away from the household
• Pleasurable• Opportunity for
socialisation• Chance for activity• Dysfunctional/
ugly latrines• Lack of maintenance • Perception of latrines
as dirty and confined
• Single toilet, not available at required times
• Habit is not developed and sustained
• Overall comfort with OD
• Health problem/illness• Disability• Afraid of snake bites• Afraid of the dark/
ghosts/evil spirits• Monsoon season/
climate• Women’s dignity• Pregnancy• Menarche• Convenience
• Life stage dependency, especially for women
• Lapse when go back from urban to live in rural areas
Non-Users Sporadic Users Lapsed Users
Without Access to Toilets
With Access to Toilets
Reasons for OD
Reasons for use
Common factors across different classifications
KeyBarrierstoChange
Building and using toilets is not a priority issue among households and open defecation is widely accepted as a normal part of the Indian culture.
DesiredBehaviouralOutcome
Individuals demand latrines, leading to construction, regular use and maintenance. The community advocates regular latrine use.
WhatwillTriggerChange?
Toilet construction and regular use are a matter of “demand creation”, discipline and a sense of responsibility. It is crucial for young children to develop toilet use as a habit in the early years.
Instead, children are often taught open defecation as a habit in early childhood. This is largely because parents find it acceptable and do not believe that it has any health consequences for their children. Rather, defecating away from home is considered healthier and cleaner than using a latrine. So the community raises another generation that sees the practice as normal.
Families want to preserve their children’s health and cleanliness and for them to become healthy and productive members of society. However, they fail to make the association between raising healthy and productive
22
children and using latrines. The trigger of change is therefore to change the social norm around open defecation, so that parents teach their children the habit of toilet use. This will break the cycle of open defecation.
Trigger
Open defecation is a “disgusting” and “dirty” practice that affects the health of the community, especially children.
ChoiceofToolsandChannels
The choice of channels is based on detailed analysis of the most effective ways to reach and influence the target audiences. Key considerations include:
• Reach – Which channels reach the target audiences? This is based on data and insights about penetration of different media types in specific areas, as well as understanding of community structures.
• Influence – Which channels most effectively influence the target audiences? What and who do they listen to, trust, respect?
• Efficiency – With limited budgets, which channels will enable the greatest reach and influence for the least spend? This is based on careful analysis of the costs of different channels, in order to optimise the allocation of budget. The detailed analysis of this type is typically undertaken by a media planning agency.
InterpersonalCommunication
Non-media channels will be crucial for reach and influence. To use non-media channels effectively requires investment in:
• Capacity-building and training for implementers and community influencers
• High-quality interpersonal communications materials, which could include, for example, storybooks, activity kits, games, manuals.
ExecutionConsiderations
Research reveals that behaviour and attitude changes are the most challenging obstacles to achieving the desired outcomes of the Swachh Bharat Mission. Although the government emphasises the importance of BCC/IEC, the majority of the budget is allocated to toilet construction in households, whereas BCC/IEC is allocated only 15%.
Research has shown that countries like Bangladesh and Vietnam managed to yield notable success in fighting OD by singularly focusing on behaviour change. Therefore, in order to achieve the desired goal, the public outreach campaigns and BCC activities should be allocated a greater portion of the Mission’s budget.
23
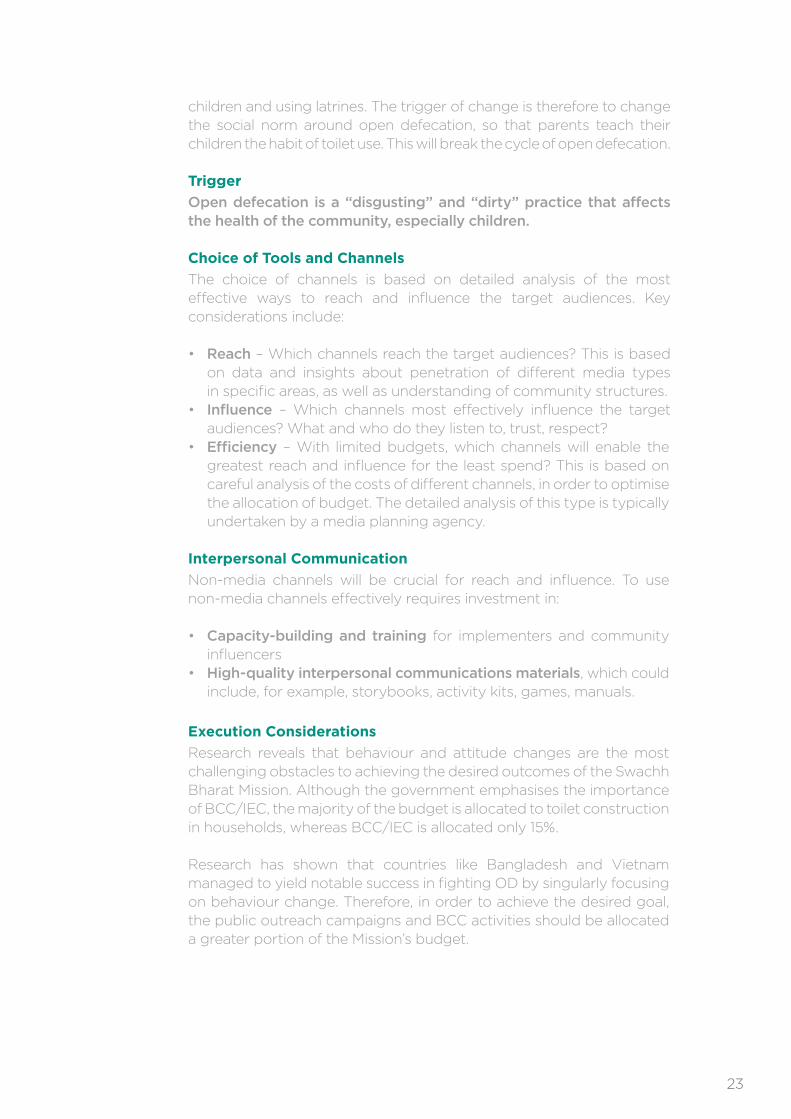
COMMUNICATION TASKS & TOOLS
Key Audience Task/Description Communication Channel Communication Tool
Thematic
All Audience GroupsPrimary Audience:• Decision Makers
• Beneficiaries
Secondary Audience:Influencers:
• PRI/Village Heads,
• Religious Leaders,
• Local Leaders,
• Doctors,
• SHGs,
• Youth Groups,
• Headmasters,
• School Teachers
• School Children
Create a vigilant environment of
no-tolerance and disgust to child
open defecation in rural villages.
To create a need and a desire
in favour of regular and consistent
use of latrines, on the platform
of disgust and better health.
Furthermore, to create a mindset
that views the practice as
disgusting and repulsive.
TV
Radio
Theatre
Street Folklore
Newspaper
Village congregation points: Panchayat Ghar,
local shop, local school,
dispensary, post office,
billboard, wall painting
• TVC
• Radio Spot
• OOH
• Posters
• Shows
• Bollywood
Movies
• TV Series
Advocacy Group:
• Government
Machinery
• Development
Agencies
• International
Organisations
• Media Profiles
• Big Corporates
and Businesses
• Civil Society
Advocacy CampaignA loud call to mobilise various
‘pressure groups’ to perform
their role in advocacy, education
and behaviour change in
influencing change with
regards to open defecation.
Direct Contact
Magazines
Workshops
Digital Based
• Website
• Posters to Create
Visibility for the
Website
• Mobile Phones
• Media Package
• Opinion Leader
Manual
• Events
Benefit Specific
Beneficiaries:
• Men
• Women
• School Aged Children
• Adolescent Girls
• Young People
• Elders
• Local Influencers
Communicating the benefit
of using latrines through
specific messages:
• Comfort
• Cleanliness
• Health
• Convenience
• Privacy
OOH Media
(out-of-home)
Radio
TV
In Print
Folk Art
• Posters
• Radio Programmes
• TVC
• Brochures, Leaflets,
Flyers
• Street Shows
24
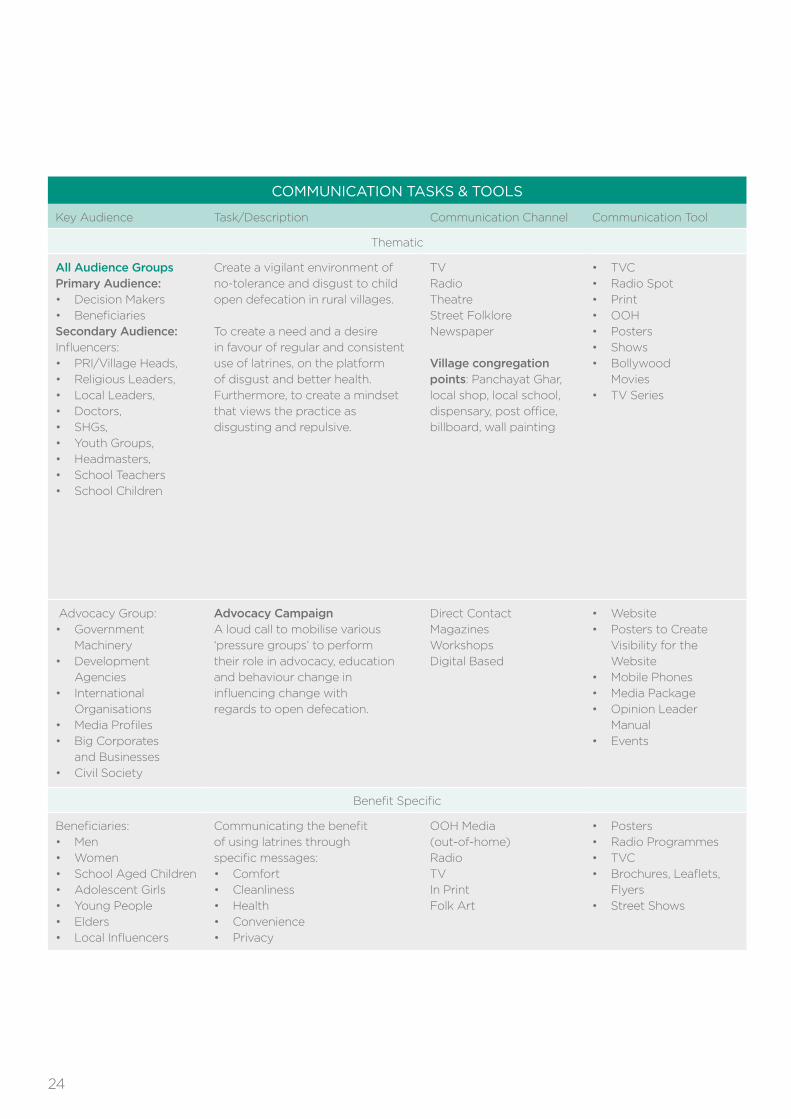
Key Audience Task/Description Communication Channel Communication Tool
Interpersonal Communication
Beneficiaries:• Men
• Women
• School Aged Children
• Adolescent Girls
• Young People
• Elders
An interactive tool with a specific
message that entails complex
intimate information exchange to
persuade adoption of regular &
consistent usage latrines Content
will include:
• Hazardous consequences
of open defecation
• Benefits of consistent use
of SLs
• Oral-faecal routes
• Information on different
latrine designs and prices
• Operation and maintenance
procedures
• Encourage dialogue-sharing
and discussions
• Encourage them to seek more
information from community
leaders and service providers
• The importance of adopting
hygiene-related practices
such as safe disposal of
child faeces, handwashing
with soap and water at
critical times and handling
drinking water.
Service Providers
• AWWs/ASHAs/ANMs
• VHN
• NGOs
• SHGs
• Swachhata Doots
• Panchayati Raj
Institutions
• Swachhata Doots
• Cooperatives
• Civil Society
• CBOs/NSS
• Sanitary Mart Retailers
• Audio-visual
• Flip book
• Information Leaflet
• Innovative Demo
Device
• Scripts for
Performances
• Guide Book
Service Providers:• AWWs/ASHAs/ANMs
• VHN
• NGOs
• SHGs
• Swachhata Doots
• Panchayati Raj
Institutions
• Swachhata Doots
• Cooperatives
• Civil Society
• CBOs/NSS
• Sanitary Mart
• Retailers
To enable service providers to hold
IPC sessions in the community and
persuade in favour of regular usage.
Construction and maintenance of
latrines/toilets
Rural Development and
Panchayat Raj Dept.
• Handbook
• Communication
Manual
• Flash Cards
25
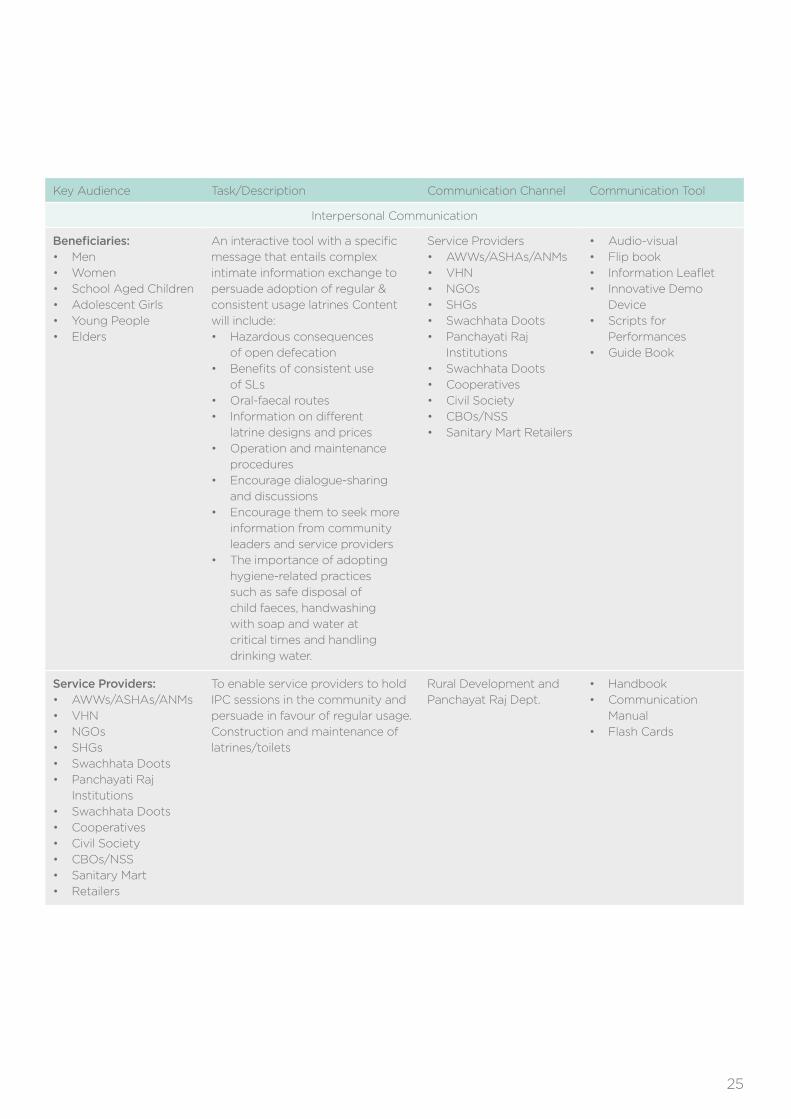
Key Audience Task/Description Communication Channel Communication Tool
School Package
School Teachers Guide teachers on their role in
children’s behaviour development
and educate them on sanitation
practices and proper hygiene. Also
orient them on how to conduct
activities that would enable children
to become channels of change and
lead the sanitation cause in their
households and community.
• NGOs working on the
ground with children
• Department of
Education & District
Schools
Administration
• Handbook
• Poster
• Flip Charts
School Aged Children An interactive and fun method of
learning should be used with school
children in order to educate them
on hygiene and sanitation practices
as well as enable them to develop
their behaviour and thus benefit
the whole community.
• Teachers
• NGOs
• Social Workers
• Activity sheets
with games,
puzzles, quizzes,
mobilisation activities
such as slogan-
writing exercises,
creating songs
• Colouring Books
• Plays
Community Mobilisation
All Community Members The involvement and participation
of all community members through
discussion and congregation to set
the issue as priority and build a
platform to resolve the issue and
working towards ODF villages.
• NGOs
• SHGs
• AWWs
• Outreach Activities
Community Events:
• Public Speeches
• Movie Screening
• Folk Performances
• Street Plays
Children Children should be
involved as agents
of change and leaders
for the cause of sanitation
in their communities
• Schools
• Teachers
• NGOs
• Rallies and Marches
as part of the
Community
Mobilization
• Songs
26

LimitationsandExpectations:
These recommendations demonstrate how effective behaviour change communications could fast-track the end of OD in rural India. Nevertheless, there are limitations to what communications can achieve given interdependencies with other aspects of the programme. With the current situation, reaching the stated targets by 2019 is challenging. It would require “constructing 88.4 million toilets in rural India over five years,” which translates into “constructing 48,000 toilets a day – up from the 14,000 a day that get built right now”1. Therefore, the recommended interventions could possibly help in fast-tracking progress but the targets of the Mission could be re-evaluated.
ConclusionBehavioural and attitudinal change towards OD in India is a highly complex issue that requires a holistic approach that goes beyond building toilets. Behaviour change communications is key to achieving the goals of the Swachh Bharat (Clean India) Mission. There is potential for real change, if different communications tools and channels are utilised effectively.
27
Arvizo, Cambria. “Open Defecation: India’s Health Hazard of the Poor – BORGEN.” BORGEN. N.p., 23 May 2014. Web. 03 Aug. 2015. <http://www.borgenmagazine.com/open-defecation-indias-health-hazard-poor/>.
Boyd, Seren. “Snakebites, Diarrhoea and Violence: Why India’s Rural Women Need Toilets.” The Guardian. N.p., 19 Nov. 2014. Web. 15 July 2015. <http://www.theguardian.com/global-development/poverty-matters/2014/nov/19/snakebites-diarrhoea-violence-india-rural-women-toilets>.
Coffey, Diane, Aashish Gupta, Payal Hathi, Nidhi Khurana, Dean Spears, Nikhil Srivastav, and Sangita Vyas. SQUAT Survey-Revealed Preference for Open Defecation: Evidence from a New Survey in Rural North India. Working paper no. 1. www.squatreport.in, 26 June 2014. Web. 29 July 2015. <http://squatreport.in/wp-content/uploads/2014/06/SQUAT-research-paper.pdf>.
Coffey, Diane. “Accelerating the Reduction of Open Defecation in Rural India Begins by Admitting the Problem.” (n.d.): 1-13. www.riceinstitute.org. r.i.c.e, Feb. 2015. Web. 10 Aug. 2015. <http://www.communityledtotalsanitation.org/sites/communityledtotalsanitation.org/files/Coffey_Kolkata_Group_note.pdf>.
UNICEF India. “Eliminate Open Defecation | UNICEF.” UNICEF, n.d. Web. 03 Aug. 2015. <http://unicef.in/Whatwedo/11/Eliminate-Open-Defecation>.
The Principal Secretary/Secretary I/C Sanitation. Ministry of Drinking Water and Sanitation. India. “Swachh Bharat Mission (Gramin) Guidelines”. N.p., Dec. 2014. Web. Aug. 2015. <www.and.nic.in/archives/rdpri/downloads/guidelines_Swachh_Bharat_Mission_Gramin.pdf>.
United Nations Department of Economic and Social Affairs (UNDESA). “International Decade for Action ‘Water for Life’ 2005-2015.” UN Water, n.d. Web. <http://www.un.org/waterforlifedecade/waterforlifevoices/open_defecation.shtml>.
JMP (2012). WHO-UNICEF Joint Monitoring Report: Progress on Drinking Water & Sanitation. <http://www.unicef.org/media/files/JMPreport2012.pdf>
Works cited
28
J Walter Thomson Social-India. UNICEF Take Poo to the Loo-AMES 2015-Asian Marketing Effectiveness and Strategy Awards. N.p.: n.p., 2015. Print.
Miles, Tom. “One Billion People Still Defecate in Public Despite Health Risks – UN.” Reuters, 8 May 2014. Web. 11 Aug. 2015. <http://www.scmp.com/article/1508275/un-says-1-billion-still-defecating-open>.
Mukunth, Vasudevan. “Open Defecation Affects Pregnancy Outcomes Too, New Study Finds.” The Wire. N.p., 9 July 2015. Web. 12 Aug. 2015. <http://thewire.in/2015/07/09/open-defecation-affects-pregnancy-outcomes-too-new-study-finds-5815/>.
Pandey, Kundan. “Open Defecation Linked to Stunting in Indian Children” Down To Earth. Down To Earth, 23 Sept. 2013. Web. 24 July 2015. <http://www.downtoearth.org.in/news/open-defecation-linked-to-stunting-in-indian-children-42252>.
Shivakumar, Girija. “Half of India’s Population Still Defecates in the Open.” The Hindu. N.p., 21 Nov. 2013. Web. 19 July 2015. <http://www.thehindu.com/sci-tech/health/policy-and-issues/half-of-indias-population-still-defecates-in-the-open/article5367467.ece>.
Sunderarajan, P. “Half of India’s Homes Have Cell Phones, but Not Toilets.” The Hindu. The Hindu, 13 Mar. 2012. Web. 03 Aug. 2015. <http://www.thehindu.com/news/national/half-of-indias-homes-have-cellphones-but-not-toilets/article2992061.ece>.
29
I cannot express enough thanks to my mentor Kalyani Rajan, the Executive Planning Director and India Strategic Head, Communication for Development, Thomson Social | J. Walter Thomson for her continued support and encouragement. I also cannot express enough gratitude to Laura Citron, Managing Director, Government & Public Sector Practice at WPP and Michael Chi Chen, Project Manager, Government & Public Sector Practice at WPP for giving me the opportunity to work on this project and for providing me with all the necessary support.
My completion of this project could not have been accomplished without the support of Manisha Singh, the AVP and Client Servicing Director, and Kavita Bisht the Client Servicing Director at Thomson Social| J. Walter Thomson in Delhi.
I would like to thank Dr Bindeshwar Pathack, founder of Sulabh international for facilitating my field visit to his organisation and for providing me with valuable information on the sanitation situation in India. Furthermore, I would like to acknowledge the efforts of Jeevan Sansthan (NGO) in facilitating my field trip to Gwalior. I would also like to thank Sumit Mullik the Additional Chief Secretary of the Government of Maharashtra for facilitating several meetings and interviews.
I would like to express my deepest gratitude to my Supervisor at the Blavatnik School of Government, the University of Oxford, Dr. Atif Ansar, for his excellent guidance, care and patience.
Finally, I would like to thank my parents, my elder sister, my elder brother and my friends. They were always supporting me and encouraging me with their best wishes.
Acknowledgements
30
Amina is a Master of Public Policy (MPP) graduate from the Blavatnik School of Government, University of Oxford. Her policy interests focus on gender equality and women’s empowerment, in addition to human rights with a specific emphasis on religious and ethnic minorities in Egypt. Amina previously worked as a research assistant at the Social Research Center at the American University in Cairo, where she took part in several projects focusing on Human Rights, Reproductive Health and Gender equality. She had also worked with the EU Election Observation Mission in Egypt as a gender, minorities and human rights assistant.
Amina Tarraf
31
WPPGovernment&PublicSectorPractice
WPP helps governments to achieve their public missions by communicating effectively.
The Government & Public Sector Practice brings together our best thinking and
expertise for policy makers and communicators in national and local government,
public institutions and international organisations.
ThompsonSocial,JWalterThompsonIndia
Thompson Social is the specialist Centre for Development Communication at J Walter
Thompson India, born with the recognition that communications for this sector requires
specific expertise, skills and knowledge. Through a vast spectrum of engagements
with organisations such as UNICEF, JHUCCP, Family Health International, PSI and
several government departments over a span of two decades, Thompson Social is
recognised as professional consultants for holistic communications solutions for
development issues and is the accepted pioneer in this field.
BlavatnikSchoolofGovernment,UniversityofOxford
The Blavatnik School of Government exists to inspire and support better government
and public policy around the world.
Followus
On Twitter: @WPP_Govt
Newsletter: wpp.com/govtpractice
Email: [email protected]
Copyright©2016WPP





























