Embed Size (px)
Citation preview
So Simple & Easy, Anyone Can Do It, Right!?So Simple & Easy, Anyone Can Do It, Right!?
Provider Enrollment Data, Data, and more Data Billing Collecting and Applying Payments Denials?
C li Compliance Website links
God made physicians to heal all of his people. A d it dAnd it was good.
On the second day he noticed providersenjoyed medicine so he created Providerenjoyed medicine, so he created Provider
Enrollment with lengthy applications and bureaucracy to rule over providers.
O h i f h 3 d d G d h On the morning of the 3rd day, God saw the challenge of paper provider applications so he created PECOS. Now instead of paperhe created PECOS. Now instead of paper applications being misplaced, they are lost in cyberspace. And it was good?
Key to getting paid correctly. Medicare = Provider Enrollment, Chain and
Ownership System (PECOS), or paper.855 i ll i i f 855 in all its various forms.
Just give them what they want! Allow plenty of time for processing! Allow plenty of time for processing! Once enrolled, make sure billing software is
setup to matchsetup to match.
Patient calls to schedule an appointment – or just shows up.
Patient provides demographics and insuranceinsurance.
Patient is seen by the provider.
Insurance is billed electronically for services. Insurance pays for all services at 100% of
amount billed, right?
Does it ever seem like: Medicare & other insurers have focused
armies of people using high end computers with sophisticated software on their side ofwith sophisticated software on their side of medical billing?
This vast array of resources is solely focused This vast array of resources is solely focused on not paying providers?
Aside from accurate medical records, it is all b t t & l t billi d tabout accurate & complete billing data.
Whose definition of “accurate & complete?” Who is typically responsible for collecting the Who is typically responsible for collecting the
data – the receptionist – who also greets each patient, answers phones, copies insurance
d h k th ti t t ft t t tcards, checks the patient out after treatment, etc.
Typically held in an EHR or billing software – Typically held in an EHR or billing software or both – which facilitate accurate and efficient billing.
Patients Demographics Insurance Referrals & Authorizations Billing codes
P t Payments
Details details details Does it all have to be Details, details, details. Does it all have to be entered correctly?
Patient’s
Name must match the Health Insurance Card (HIC) l(HIC) exactly.
Richard C. Papperman vs. Rich Papperman
Address DOB DOB Insurance policy(s) & group numbers
Providers Provider names Individual & Group #’s National Provider Identifier (NPI) numbers Office & facility addresses – Zip + 4
CPT HCPCS & ICD 9 d CPT, HCPCS, & ICD-9 codes Linking CPT & HCPCS codes with ICD-9
How do we report the data in order to get paid? CMS-1500 form Using CPT, HCPCS & ICD-9 codes Maybe some day – ICD-10 codes?
CPT = Current Procedural Terminology
Used to bill: Services of Physicians (MD, DO, DPM) & Allied Services of Physicians (MD, DO, DPM) & Allied
Health Professionals (PA, NP, APN, Midwife, etc.) for Evaluation and Management, Surgery, Radiology Lab services etcRadiology, Lab services, etc.
Some codes are composed of Professional and T h i l L b P h l &Technical components: Lab, Pathology & Radiology. Professional is what the physician did. Technical is what the facility provided.
Used to communicate information to insurers.
Example -59 separate and distinct procedure. Example: Excision of 2 separate lesions
C difi 22 24 25 50 51 52 Common modifiers: 22, 24, 25, 50, 51, 52, 57, 59, 62, 76, 78, 79, 80, 82, AS, AT, GO, GP GV GW LT RT Q5 Q6 QW TC 26GP, GV, GW, LT, RT, Q5, Q6, QW, TC, 26.
Podiatry modifiers: TA, T1, T2, T3, T4, T5, T6, T7, T8, T9, Q7, Q8, Q9., , , , Q , Q , Q
HCPCS = Healthcare Common Procedure Coding SystemSystem
Used to bill:M di ti (d th C l t B12 Medications (dexamethasone, Celestone, B12, Kenalog)
Durable Medical Equipment (DME) equipment and supplies (Wheelchairs walkers canes hospitalsupplies (Wheelchairs, walkers, canes, hospital beds)
Orthotics and Prosthetics (Therapeutic shoes & inserts)inserts)
Surgical Supplies (gauze, ointment, tape) Numerous other medical items & services
Often strict coverage policies. For DME and routine ambulance transports –
requirements for Certificates of Medical Necessity (CMN) signed by a physician orNecessity (CMN) signed by a physician or AHP.
Common Modifiers:Common Modifiers: Wound dressings: A1 – A9 DME: KX, KA, KH, KI, KJ, MS, NU, UE DME: KX, KA, KH, KI, KJ, MS, NU, UE Ambulance: GM, QL, RH, SH, PH, SI, etc.
ICD-9 is used for diagnosis codes. Must be linked to the proper CPT or HCPCS
code.
ICD-10 set for October 1, 2015.
Pairs of CPT or HCPCS Level II codes that are not separately payable except under certain circumstances.
Edits are applied to services billed by the: Edits are applied to services billed by the:- Same provider for the
Same beneficiary on the- Same beneficiary on the - Same date of service.
All claims are processed against the CCI All claims are processed against the CCI tables.
Example: 14000 (Adjacent tissue transfer, trunk) d 11402 (E i i b i l i k) O land 11402 (Excision benign lesion, trunk). Only
the 14000 will be paid if the 14000 was the result of the 11402. The 11402 should not beresult of the 11402. The 11402 should not be billed.
Common Software Edits: Age range Sex Units
Examples of mismatch edits: Prostatectomy on a female Hysterectomy on a male 99385 Well exam, age 18-39. Invalid for
anyone outside that age range. 69210 Removal of impacted cerumen (ear 69210 – Removal of impacted cerumen (ear
wax), unilateral. Maximum units is 2.
Standard coverage throughout the nation –well, almost!
Fairly clear policiesN h R il d M di Not the same as Railroad Medicare
For Railroad Retirement beneficiaries Palmetto GBA is the Railroad Specialty
Medicare Administrative Contractor (RRB SMAC) and processes Part B claimsSMAC) and processes Part B claims
Part C Covers both Part A (Hospital) & B (Medical) Offered by Private Companies – Blue Shield,
A CIGNA UHC HAetna, CIGNA, UHC, Humana, etc. Cover all Medicare services Medicare pays a fixed sum of money to the Medicare pays a fixed sum of money to the
HMO per enrollee Can charge different out-of-pocket costs & Can charge different out of pocket costs &
have different rules (referrals, authorizations)
Part D Pharmacy Usually offered thru a Medicare Advantage
PlPlan If not offered thru Part C, you can join a
Medicare Prescription Drug PlanMedicare Prescription Drug Plan
By definition are 2’ to Traditional Medicare and only cover Medicare approved charges and services.
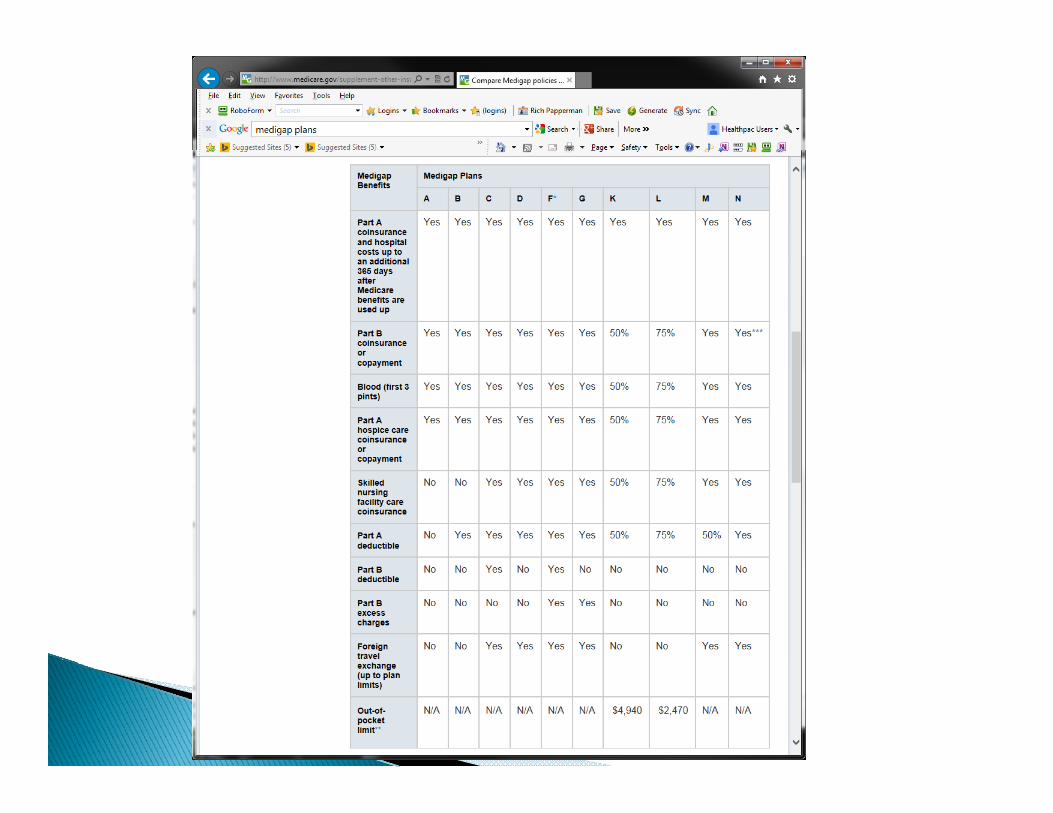
Standard plans with the same coverage Standard plans with the same coverage regardless of the insurer – AARP, Blue Shield, etc.etc.
Cannot be used to pay Medicare Advantage Plans copayments, deductibles, or premiums.
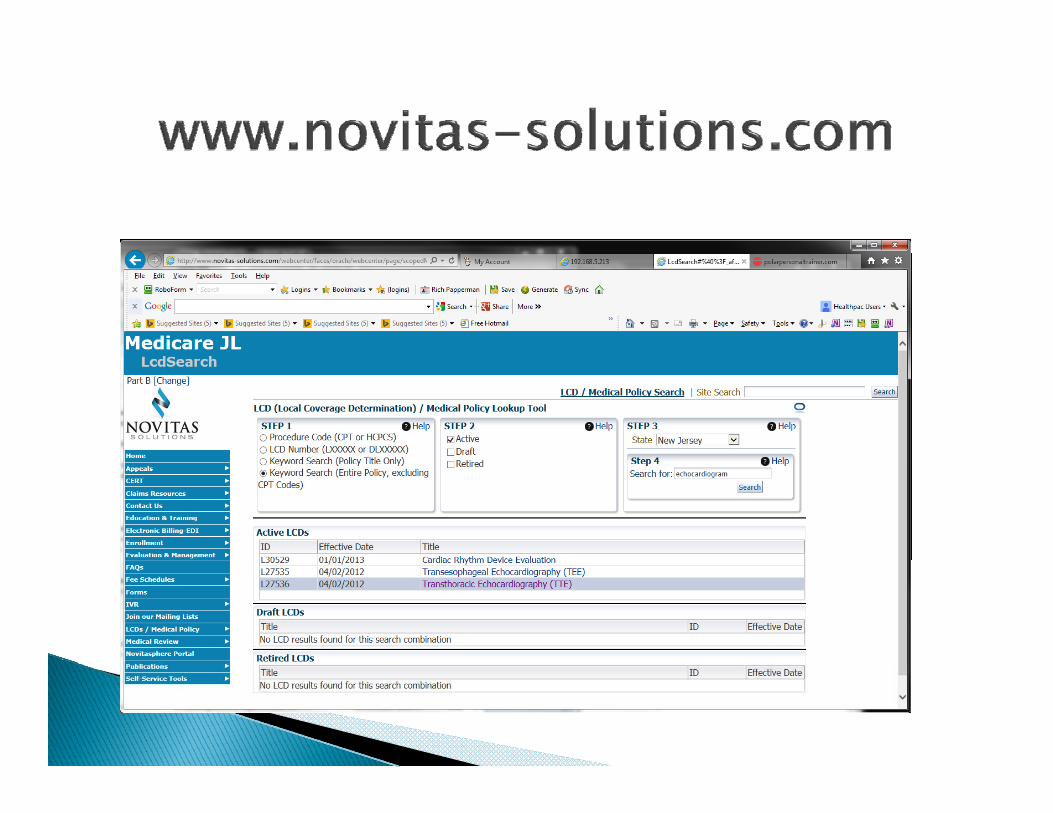
LCD = Local Coverage DeterminationsC l C NCD = National Coverage Determinations
Indicate what an insurer considers acceptable Indicate what an insurer considers acceptable reasons to pay specific CPT & HCPCS codes –often diagnosis code specific.
Differences between MAC’s
Good coders are very valuable!
Followed by all MAC’s nationwide & covered under 1862(a)(1) of the Social Security Actunder 1862(a)(1) of the Social Security Act.
Initiated by the Centers of Medicare & Medicaid Services (CMS) if they find:Services (CMS) if they find: Inconsistent local coverage polices exist The service represents a significant medical
advance and no similar service is currentlyadvance and no similar service is currently covered by Medicare
The service is the subject of substantial controversycontroversy
The potential for rapid diffusion or overuse exists
The alphabetical index can be found at : h d http://www.cms.gov/medicare-coverage-database/indexes/ncd-alphabetical-index.aspx?bc=BAAAAAAAAAAAindex.aspx?bc BAAAAAAAAAAA
Common examples: EKG’s Blood Glucose Testing Cardiac Pacemakers Cardiac Pacemakers Colorectal Screening Tests (82270)
http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Internet-Only-Manuals-IOMs.html
Publication 100 03 Publication 100-03 Separated into Chapters
If no NCD, Medicare MAC’s may establish local policies
LCD’s are administrative and educational tools to assist providers in submitting correcttools to assist providers in submitting correct claims
Usually include specific requirements for Usually include specific requirements for providers to understand Medicare coverage of certain procedures, including specific CPT, HCPCS & covered ICD-9 codes.
Will be updated for ICD-10 ~ April 1, 2015.
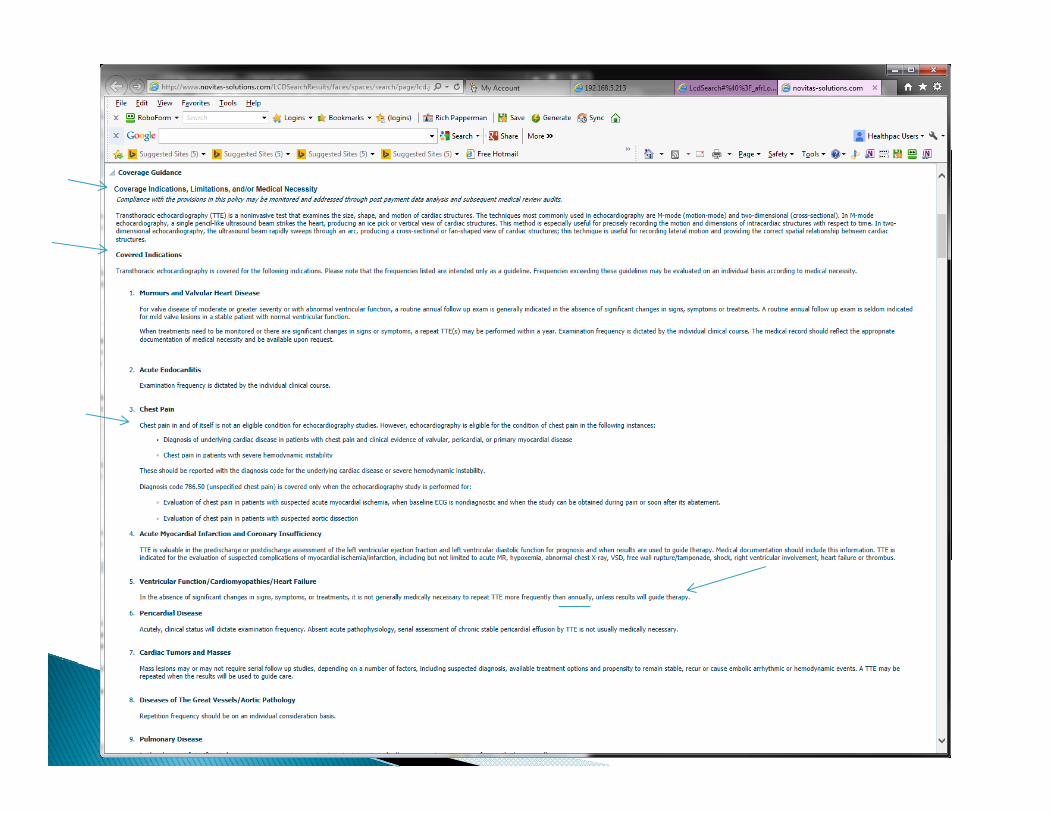
Transthoracic Echocardiography (TTE) Coverage Indications, Limitations, and/or
Medical NecessityC d I di i Covered Indications
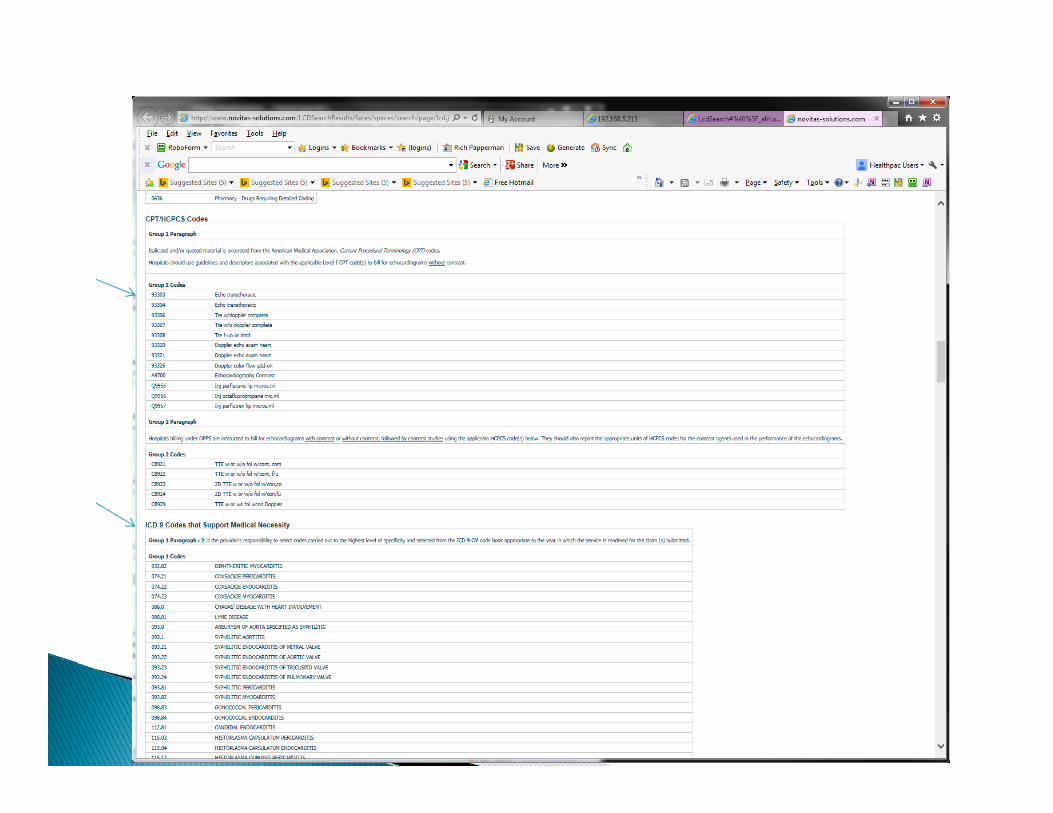
Covered CPT Codes ICD 9 Codes that Support Medical Necessity ICD-9 Codes that Support Medical Necessity
Be sure to “link” the ICD-9 code to the proper Be sure to link the ICD-9 code to the proper CPT codes.
Payment for services by Medicare must be performed: In accordance with federal laws, regulations
and Medicare national payment rulesand Medicare national payment rules In accordance with Medicare coverage policies
(national and local)(national and local) By a qualified practitioner For a qualified beneficiary For a qualified beneficiary Medically reasonable and necessary Coded correctlyy
Paper EOB Paper Check Post $1,000’s in hours – hopefully accurately
ERAEFT EFT
Post $1,000’s in seconds - accurately
CMS sets values for each medical procedure (CPT) th h th f R l ti V l U it(CPT) through the use of Relative Value Units (RVUs).
An RVU for a medical procedure consists of An RVU for a medical procedure consists of three components: physician work, physician expense and malpractice expense. CMS uses a formula that combines the threea formula that combines the three components into one unit.
The RVU’s are then multiplied by a p yConversion Factor (CF) to determine how much will be paid for a medical procedure.
Types of fee schedules: physician, drug, DME, b lambulance.
Insurers pay the lower of their allowed fee or the chargecharge.
Example 1: Bill 99213 at $50.00. Insurer allows $60.00. Payment is based on $50.00 subject to co-pay, co-insurance, and/or deductibles.
Example 2: Bill 99213 at $85.00, Medicare allows $78 56 so may pay as much as $61 28allows $78.56 so may pay as much as $61.28 (78% of the Allowed). Why not 80% ?
Incentive is ?
Resource-Based Relative Value Scale. RVU’s – part of RBRVS. A system that reflects
the relative level of time, skill, training and intensity of a serviceintensity of a service.
RVUs are a method for calculating the volume of work or effort included in the codeof work or effort included in the code.
Often used to pay providers – either by insurers or employers – when multiplied by a p y p ydollar conversion factor.
Many electronic health record (EHR) programs have built-in billing software or provide HL-7 interfaces with billing software.
Provider either selects codes in the EHR or Provider either selects codes in the EHR or indicates on a paper charge form.
Some EHR programs do not yet have the Some EHR programs do not yet have the ability to output charge data.
CMS-1500 vs. UB04
Paper claims – it is how healthcare is paid for. CMS-1500 is used for Part “B” / physician /
DME billing. UB04 is Part “A” / Facility billing UB04 is Part A / Facility billing
Billing is usually now performed electronically Billing is usually now performed electronicallyvia the internet.
Hospital End-Stage Renal Disease Facility End Stage Renal Disease Facility Federally Qualified Health Center Histocompatibility Laboratory Home Health Agencyo e ea t ge cy Hospice Indian Health Services Facility Organ Procurement Organization Outpatient Facility Physical Therapy Services Outpatient Facility Occupational Therapy Services Speech Pathology Services
R li i N M di l H l h C I i i Religious Non-Medical Health Care Institution Rural Health Clinic Skilled Nursing Facility
Used to bill the following types of charges using CPT & HCPCS codes: Physician
DME DME Ambulance
All data elements are compared by insurers to ensure they are paying a valid claim only for their insured.
Code edits 9 Gender age frequency etc Code edits 9 Gender, age, frequency, etc. Data matches & passes coding edits = paid
claim!claim! Mismatch = denied claim = more work. Ugh!
PQRS = Physician Quality Reporting System Aimed at improving quality of care –
including readmissions to hospitals.U bi i f i i Uses a combination of incentive payments (carrot) and payment adjustments (stick) to promote reporting of quality information bypromote reporting of quality information by eligible professionals (EPs).
Code based. $.00 or $.01
eRx = electronic prescriptions Aimed at decreasing Rx errors which
improves the quality of care.B f 2014 d d G8443 i di h Before 2014, used code G8443 to indicate the patient’s Rx was sent electronically to a pharmacypharmacy.
In 2014 is part of Meaningful Use
835 vs. manual posting Is someone following up on denials – timely? Medicare – 1 year from DOS to bill
Yikes! What happened? Patient not covered? Service not covered?
Why? Billing error?W i i difi Wrong or missing modifiers
ICD-9 code not valid for CPT or HCPCSU f td t d d Use of outdated codes
Billing during global periods
Reason and Remit Codes convey why codes paid or denied.
MA130 – “Your claim contains incomplete and/or invalid information”and/or invalid information
M79 – “Missing / Incomplete / Invalid Charge M76 “Missing / Incomplete / Invalid M76 – Missing / Incomplete / Invalid
Diagnosis” OA22 – “This care may be covered by another OA22 This care may be covered by another
payer per COB”
Working denials: - Paper EOB - Insurance Report, or - Electronic work queue.
Watch timely filing deadlines.
Avoiding and correcting mistakes Avoiding the “F” word - Fraud
What is documented in the medical record? What is being billed?
D th t h? Do they match? Close only counts in horse shoes and hand
grenades!grenades!
Fraud – Knowingly billing for a service that was not performed.
Post-payment auditP di (d h b d l ?) Pre-payment audit (death by delay?)

Uninsured rate down from 17.1% to 13.4%. Roughly 8-11 million patients.
Approximately 1 in 4 who were not insured last Fall now have coveragelast Fall now have coverage.
Of the 5.4 million enrollees who use www HealthCare gov to enroll before mid-www.HealthCare.gov to enroll before midApril, 87% received federal subsidies.
To qualify for a subsidy, projected annual q y y, p jincome had to be 100-400% of the Federal Poverty Level (~ $11,490 - $46,000)
High Deductible Plans - $1,000 - $10,000+ The Non-Medicare Paradigm has shifted to
greater patient responsibility! M di d d ibl i $147 i 2014 Medicare deductible is $147 in 2014.
Maximizing patient payments requires strong written financial policies &strong, written financial policies & procedures.
Characteristics of best financially performing practices: Verify insurance when patient calls for the Verify insurance when patient calls for the
appointment. Use electronic eligibility verification during the call. Remind the patient to bring their co-pay Remind the patient to bring their co pay. 1-2 days prior to the appointment, re-check
eligibility. Always collect the co-pay on the DOS – when the Always collect the co pay on the DOS when the
patient arrives. Check the billing software for other unpaid patient
balances – ask the patient how they want to pay? Need a referral or authorization? Receptionists and those staff making appointments
are key people! Look for the right characteristics.
If not contractually prohibited, collect part of deductible balances on the DOS.
Create a spreadsheet of Allowables for each major insurer for the most commonmajor insurer for the most common CPT/HCPCS codes.
Don’t give them an option: “Do you want to Don t give them an option: Do you want to pay by cash, check, or credit card?”
If an overpayment occurs, p y ,promptly refund the balance.
Patient Balances
Accept and offer: Credit & debit cards, FSA, HSA, & HRA Cash & checks
P ti t t l Patient portals First born child, indentured servitude?
Secure online website 24-hour access Providers can communicate with patients Patients can pay their bills without your staff Encourages patients to be more engaged in
their care can check test results scheduletheir care - can check test results, schedule appoints, etc.
RVU’s: http://www.nhpf.org/library/the-basics/basics_rvus_02-12-09.pdf
NCCI edits: http://www cms gov/Medicare/Coding/Natiohttp://www.cms.gov/Medicare/Coding/NationalCorrectCodInitEd/NCCI-Coding-Edits.html
Medigap Policies: Medigap Policies:http://www.medicare.gov/supplement-
other-insurance/medigap/whats-/ g p/medigap.html
Railroad Medicarehttp://www.palmettogba.com/RR
Questions?


























![Billi Kay Khuwab Main Chechrey [Urdu]](https://img.pdfslide.us/doc/110x75/577ca59a1a28abea748b99dd/billi-kay-khuwab-main-chechrey-urdu.jpg)

