Embed Size (px)
Citation preview

The patient was a 25-year-old man who was serving in the military. He was re-
ferred to a physical therapist by his primary care physician for a progressively worsening painful snap-ping sensation in the posteromedial left knee region, which began 8 months prior and now limited his ability to perform re-quired military activities. The symptoms were insidious in onset, and there was no prior history of left knee pain or trauma. Prior magnetic resonance imaging for the left knee was interpreted as normal, ex-cept for a mild fluid signal about the left pes anserine bursa.
At the time of the physical thera-pist’s initial evaluation, the patient had
a nonantalgic gait and there was normal strength of the lower ex-tremity musculature. Active and passive range-of-motion assess-ment of the left knee from flexion
to extension revealed an audible pop and a palpable painful snapping sensation along the posteromedial aspect of the left knee at approximately 30° of knee flexion. The patient was diagnosed with snapping pes anserine syndrome.1,2 How-ever, despite 6 weeks of physical therapist intervention, the patient did not improve.
A dynamic real-time ultrasound ex-amination was then ordered, which demonstrated that the pes anserine ten-dons changed position as the knee moved from flexion to extension, sliding across a
[ musculoskeletal imaging ]
CHARLES E. RAINEY, PT, DSc, DPT, OCS, FAAOMPT, Naval Special Warfare Group ONE, San Diego, CA.DANIELLE A. TAYSOM, MD, Department of Radiology, Naval Medical Center, San Diego, CA.
MICHAEL D. ROSENTHAL, PT, DSc, SCS, ECS, ATC, Department of Physical/Occupational Therapy, Naval Medical Center, San Diego, CA.
Snapping Pes Anserine Syndrome
heterogeneous rounded mass in the pos-teromedial knee (FIGURE 1, video available at www.jospt.org), which was thought to represent focal scarring/thickening of the joint capsule when correlated with the prior magnetic resonance image (FIGURE 2, available at www.jospt.org). The patient was referred to an orthopaedic surgeon and subsequently underwent harvest-ing of the semitendinosus and gracilis tendons.1,2 At 6 weeks following surgery, the patient had no complaints of left knee pain and had successfully returned to all required military activities. t J Orthop Sports Phys Ther 2014;44(1):41. doi:10.2519/jospt.2014.0402
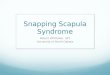
FIGURE 1. Longitudinal ultrasound images of the left pes anserine tendons (orange arrows) with the knee in 90° (left) and 30° of flexion (right). As the knee moved from a flexed (left) to a more extended position (right), the pes anserine tendons changed position (note that the semitendinosus tendon is no longer in view for the image on the right), sliding across a heterogeneous rounded mass at the proximal medial tibia (white arrows), which was thought to represent focal scarring/thickening of the joint capsule when correlated with the prior magnetic resonance image (FIGURE 2, available at www.jospt.org). The change in position of the pes anserine tendons was also accompanied by an audible pop and palpable snapping sensation that was painful. Patient positioning during the ultrasound examination is seen in the bottom right-hand corner of the images.
References 1. Bollen SR, Arvinte D. Snapping pes syndrome: a report of four cases. J Bone Joint Surg Br. 2008;90:334-335. http://dx.doi.org/10.1302/0301-620X.90B3.20369. 2. Geeslin AG, LaPrade RF. Surgical treatment of snapping medial hamstring tendons. Knee Surg Sports Traumatol Arthrosc. 2010;18:1294-1296. http://dx.doi.org/10.1007/
s00167-010-1174-5
The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the views of the Department of the Navy or Department of Defense.
journal of orthopaedic & sports physical therapy | volume 44 | number 1 | january 2014 | 41
SUPPLEMENTAL VIDEO ONLINE
44-01 Imaging-Rainey.indd 1 12/17/2013 5:22:56 PM
Jour
nal o
f O
rtho
paed
ic &
Spo
rts
Phys
ical
The
rapy
®
Dow
nloa
ded
from
ww
w.jo
spt.o
rg a
t Otte
rbei
n U
nive
rsity
on
June
2, 2
014.
For
per
sona
l use
onl
y. N
o ot
her
uses
with
out p
erm
issi
on.
Cop
yrig
ht ©
201
4 Jo
urna
l of
Ort
hopa
edic
& S
port
s Ph
ysic
al T
hera
py®
. All
righ
ts r
eser
ved.