Embed Size (px)
Citation preview

Oral Oncology (2007) 43, 187–192
ava i lab le a t www.sc iencedi rec t . com
journal homepage: ht tp : / / in t l .e lsevierheal th .com/ journals /oron/
Smoking has a negative impact upon healthrelated quality of life after treatmentfor head and neck cancer
Kenneth Jensen *, Anders Bonde Jensen, Cai Grau
Department of Oncology, Aarhus University Hospital, Noerrebrogade 44, 8000 Aarhus C., Denmark
Received 23 January 2006; received in revised form 10 February 2006; accepted 13 February 2006Available online 24 July 2006
Summary To examine the influence of smoking on observer based morbidity scores andpatient assessed health related quality of life after treatment for head and neck cancer. Theresults of EORTC C30 and H&N35 questionnaires and DAHANCA morbidity scores were studiedaccording to smoking status in 114 recurrence free head and neck cancer patients. In contrastto observer based toxicity scoring, smoking had a significantly negative influence on 20 of the 33quality of life scales. Previous smokers had quality of life scores in between never smokers andcontinuous smokers. Smoking after treatment of head and neck cancer adversely influenced awide range of quality of life endpoints. Quitters had better quality of life than patients whocontinued to smoke after treatment, suggesting that smoking cessation may improve qualityof life in addition to reducing the risk of new cancer.
�c 2006 Elsevier Ltd. All rights reserved.
KEYWORDSMorbidity;Toxicity;Head and neck neoplasm;Smoking;Tobacco;Quality of life;Radiotherapy;Surgery
1d
0
Introduction
Smoking is a prevalent addictive behaviour with majorimplications on mortality and morbidity in all countries.It is the second major cause of death worldwide and isresponsible for the death of 1 in 10 adults worldwide[www.who.int]. Tobacco is an important risk factor in thedevelopment of squamous cell head and neck cancer. Addi-tionally, smoking decreases the effect of radiotherapy1,2
and increases the rate of second primaries.3
368-8375/$ - see front matter �c 2006 Elsevier Ltd. All rights reservedoi:10.1016/j.oraloncology.2006.02.006
* Corresponding author. Tel.: +45 89 49 26 51; fax: +45 89 19 716.E-mail address: [email protected] (K. Jensen).
The influence of smoking on radiotherapy side effects hasonly been sparsely studied. Smoking has been reported tolead to excess duration of mucositis in radiotherapy usingthe CHART schedule4 and increased severity of mucositisand acute skin reaction also in a more heterogeneous popula-tion of head and neck cancer patients.5 However, in anotherstudy, including 115 head and neck cancer patients receivingradiotherapy with or without chemotherapy, no influencewas found of smoking on acute radiotherapy side effects.1
Smoking has been associated with late radiation induced tox-icity of the lung,6 small bowel, rectum and bladder.7
A significant number of patients continue to smoke afterdiagnosis and definitive therapy. Smokers associate theirhabit with pleasure and relaxation. A few studies have
.

Table 1 Patient characteristics of 114 recurrence freehead and neck cancer patients
Mean age (years) (range) 63 (36–92)
GenderWomen 41 (36%)Men 73 (64%)
Tumour site
188 K. Jensen et al.
suggested, however, that smoking is associated with de-creased quality of life (QoL) in a general population,8 in sur-vivors of lung cancer9 and head and neck cancer patientswith non-terminal disease.10 The aim of the present studywas to estimate the influence of continued smoking andsmoking cessation, respectively, on observer-assessed mor-bidity and self-reported overall and tumour site specific QoLin a population of recurrence free head and neck cancerpatients.
Larynx 42 (37%)Pharynx 34 (30%)Oral cavity 38 (33%)
StageI 39 (34%)II 31 (27%)III 25 (22%)IV 19 (17%)
TreatmentSurgery 33 (29%)Radiotherapy 81 (71%)
Mean time since therapy (months) (range) 19 (1–65)
Patients and methods
Patients in follow-up after radical radiotherapy or surgeryfor larynx, pharynx and oral cavity cancer were candidatesfor the study. The study set-up has been described in detailpreviously.11 In brief, consecutive eligible patients wereasked to fill out the EORTC quality of life questionnaires(QLQ) C30 and H&N35, which have recently been validatedin Danish.11 Exclusion criteria’s, applied before askingthe patient to participate, were previously determinedrecurrences (57 patients) and dementia (three patients) orreferral for further examination because of suspectedrecurrences (27 patients). At the follow-up visit, informa-tion regarding tumour status, morbidity and smoking statuswere gathered on standard forms issued by the Danish Headand Neck Cancer Study Group DAHANCA (www.dahanca.dk).The DAHANCA endpoints are recorded on identical scalesirrespective of time after therapy. They have not been for-mally validated but has proved themselves of value in largerandomised trials12 and are correlated with clinical parame-ters as expected.13 The WHO performance status (PS) wasalso recorded. Baseline information regarding patient, tu-mour, treatment and smoking status was available fromthe DAHANCA database. The local ethics committee ap-proved the study, and a returned questionnaire was consid-ered as informed consent.
In the following, the morbidity endpoints from the DAH-ANCA forms will be written with capital letters, e.g. DYS-PHAGIA, in order to distinguish them from the EORTC QLQendpoints, which will be written as e.g. Pain (C30) or HNPain (H&N35).
All but one of the 120 patients asked for participationagreed to enter the study and was given a questionnaire.One hundred and sixteen (96%) patients returned a validquestionnaire. Compliance to the instruction given to thepatients was excellent, except for the questions concerningsexuality where answers were missing from 21% of the pa-tients. The registration of toxicity was almost completewith 97% of data present. Pre-treatment smoking status(‘smoker’, ‘previous smoker’ or ‘never smoker’) and atthe time of this study (‘smoker’ or ‘non-smoker’) wereavailable for 114 patients, and this cohort forms the basisof this report. Clinical data on the 114 patients are shownin Table 1.
Statistics
The toxicity scores and QoL data were ordinal data andnon-normal distributed. Non-parametric tests were there-fore used: Kruskal–Wallis/Wilcoxon–Mann–Whitney when
comparing categorical data and Spearmans rho test wasused when testing for correlations. In order to adjust forcovariates a univariate general linear model with no inter-action among the independent parameters was constructedand the results were represented as adjusted means for thechosen endpoints dependent on smoking status. All men-tioned parameters were included in the models irrespectiveof the significance of the influence on specific endpoints. Ap-value < 0.05 was regarded as significant and all tests weretwo tailed. When comparing multiple unadjusted values,endpoints significantly different with a p-value < 0.005 willalso be mentioned. SPSS 11.0 for Windows was used forthe statistical analysis.
Results
At the time of follow-up there were 62 non-smokers and 52smokers. Smoking status was independent of all registeredclinical parameters as: age (at study time), PS, gender,stage, site, treatment modality or time since treatment. Pa-tients who were smokers at follow-up invariably had thelowest function scores and the highest symptoms scores inboth DAHANCA and EORTC QLQ except for FIBROSIS andHN Weight gain. The difference between smokers and non-smokers were significant (p < 0.05) in 20 of the 33 QoL scalesof the EORTC QLQ. Cognitive function, nausea/vomiting,dyspnoea, appetite loss, diarrhoea and HN weight loss wasstatistical significant different with p < 0.005. In contrast,smoking status did not significantly influence any of theDAHANCA morbidity scores.
In order test for a causative correlation between smokingand the quality of life endpoints, we examined whetherthere was an effect of smoking cessation. Non-smokers atfollow-up were divided in to ‘Quitters’ (n = 48) and ‘Neversmokers’ (n = 8) according to previous smoking statusaccording to the information gathered at their first visit tothe hospital. The distribution of patients according to

Table 2 Distribution of patients according to smoking status
Non-smoker at follow-up (n = 62) Smoker at follow-up (n = 52)
‘Never smoker’ at diagnosis 14 (12%)a 0 (0%)c
‘Former smoker’ at diagnosis 27 (24%)b 8 (7%)c
‘Present smoker’ at diagnosis 21 (18%)b 44 (39%)c
a ‘Never smokers’.b ‘Quitters’.c ‘Present smokers’.
Influence of smoking on health related QoC after treatment for head and neck cancer 189
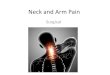
smoking status is presented in Table 2. Quitters consisted of21 patients admitting to smoke at diagnosis and 27 formersmokers who became nicotine abstinent before first visitto the centre. The influence of this classification on the dis-tribution of morbidity scores and QoL endpoints are pre-sented in Table 3 and condensed in Figure 1. These figuresgives a clear indication that ‘Quitters’ have QoL scores inbetween those of ‘Never smokers’ and continuous smokersfor most QLQ endpoints, thus indicating a ‘‘dose depen-dent’’ effect. The same relationship could not be demon-strated concerning the DAHANCA morbidity data.
Clinical factors could still influence the observed resultseven though smoking status was not directly correlated withany clinical parameter registered. In order to adjust for thisa linear model was constructed with the following clinicalvariables as dichotomous parameters: Smoking at follow-up, age (below versus above median = 62.6 years), stage(St I + II versus III + IV), gender, site (larynx, pharynx, oralcavity), time since therapy (below versus above med-ian = 16.6 months) and treatment modality (surgery versusradiotherapy). Adjusted mean values of the 19 endpointssignificantly dependent on smoking status in this modelare presented in Table 4. These endpoints hardly differedfrom the unadjusted endpoints, suggesting that smoking istruly independent of the clinical parameters available.The second most common significant parameter in the mod-el was performance status, which was a significant parame-ter for 10 endpoints of the QLQ’s.
Because smoking is associatedwith socio-economic status,we tried to adjust for this factor too. There was, however, noaccess to objective socio-economic data in the current study,butHN35 contains five questions regarding social contact (theHN Social contact scale).When the dichotomised score of thisscale (above or belowmedian = 0)was entered into the afore-mentionedmodel, as a proxy for social contact, a reducedbutstill significant independent effect of smoking on quality oflife remained in nine of the 19 endpoints of Table 4 (cognitivefunction, gastrointestinal symptoms, pulmonary symptoms,social eating (trouble eating and enjoying meals in a socialcontext) and loss of appetite and weight).
Continuous smoking has repeatedly been associated withdepression10,14 and this might also explain some of thecorrelation with quality of life endpoints. The emotionalfunction scale of the EORTC C30 questionnaire containsquestions on feeling tense, worried, irritable and de-pressed. It has been shown to correlate closely with moreelaborate anxiety and depression scales as HADS (hospitalanxiety and depression scale).15 If the dichotomised emo-tional function score and dichotomised answer of the ques-tion regarding feeling depressive (above or below median)
was entered into the model, as done above with the socialfunction scale, smoking remained significant for 13 of the19 endpoints of Table 4.
Discussion
In the present study we compared morbidity and quality oflife between smokers and non-smokers in a population of114 recurrence free head and neck cancer patients. Theanalysis clearly demonstrated that patients who continuedsmoking after diagnosis and treatment had poorer qualityof life compared to quitters and never smokers. Smokingnegatively influenced much wider range of QOL endpointsthan well-known clinical parameters like performance sta-tus, stage, treatment etc. The statistically significant dif-ferences in quality of life scores between smoking groupswere larger than what is perceived to be clinically signifi-cant (P10 point difference).16
In our study, smoking did not seem to have a significant ef-fect on late morbidity, measured with the DAHANCA scoringsystem. A relationship between smoking and an increased riskof both acute5,4 and late7 side effects after radiotherapy hasbeen suggested as well as questioned1 in previous studies.The late effect study by Eifel et al.7 reported major rectal,small bowel and bladder complications after radiotherapyfor stage I carcinoma of the cervix in 3489 patients. Theyfound strong and significant correlation between smoking sta-tus and especially small bowel complications. Bladder andrectal complication risks were also higher in heavy smokers.We found less toxicity in five of six available morbidity end-points amongnon-smokers but none reached statistical signif-icance. This negative finding regarding morbidity could beexplained by the smaller sample size or by the low sensitivityof the observer based scoring systems. In a previous study, wedemonstrated that the DAHANCA morbidity scoring systemwas inferior to the EORTC quality of life questionnaires whenmeasuring subjective side effects.13
Smoking influenced a large number of quality of life end-points in this cohort of recurrence free head and neck can-cer patients. This was true for endpoints related to theupper aero-digestive tract and lungs but also endpointswithout obvious correlation with exposure to tobaccofumes. The effect of smoking was also evident concerningfew of the more overall endpoints like physical functionand fatigue. On the other hand overall QoL endpoints,e.g. general health status/QoL and HN felt ill were not sig-nificantly dependent on smoking status. This is could be ex-plained by response shift: The fact that patients with long

Table 3 QoL and morbidity dependent on smoking status among 114 recurrence free head and neck cancer patients
Never smokers (n = 14) Quitters (n = 48) Present smokers(n = 52)
Mean Median Mean Median Mean Median
Global health status/QoL 79 83 68 71 62 67Physical function* 98 100 83 93 78 87Role function 88 100 80 100 68 67Emotional function 86 96 76 83 70 75Cognitive function* 94 100 88 100 73 83Social function 90 100 83 100 76 83Fatigue* 17 11 28 22 37 33Nausea/vomiting* 0 0 3 0 14 0Pain 18 17 16 8 29 17Dyspnoea 0 0 9 0 22 0Insomnia 19 0 21 0 28 33Appetite loss* 7 0 13 0 38 33Constipation* 0 0 12 0 21 0Diarrhoea* 7 0 8 0 23 0Financial problems* 7 0 10 0 24 0HN pain* 18 13 15 8 27 25HN swallowing* 4 0 17 8 26 25HN senses* 12 0 23 17 34 33HN speech 10 0 22 11 28 11HN social eating* 7 0 15 8 31 22HN social contact* 6 0 9 0 17 7HN sexuality 18 0 38 33 37 33HN teeth 21 0 27 0 35 0HN opening mouth 26 0 19 0 24 0HN dry mouth* 45 50 43 33 61 67HN sticky saliva 24 17 39 33 47 33HN coughed* 15 0 22 0 39 33HN felt ill 12 0 11 0 21 0HN pain killers 36 0 34 0 47 0HN nutritional supp.* 21 0 13 0 35 0HN feeding tube* 0 0 4 0 18 0HN weight loss* 0 0 10 0 37 0HN weight gain 21 0 30 0 24 0DYSPHAGIA 0.07 0.00 0.50 0.00 0.75 0.00DRY MOUTH 0.86 1.00 0.86 1.00 0.90 1.00HOARSENESS 0.21 0.00 0.92 1.00 0.84 0.00OEDEMA 0.14 0.00 0.67 0.00 0.65 0.00ATROPHY 0.21 0.00 0.64 1.00 0.66 1.00FIBROSIS 0.36 0.00 0.89 1.00 0.72 0.00
*p < 0.05 Kruskal–Wallis test.
190 K. Jensen et al.
lasting symptoms tends to adjust their expectation of overall good health.19,20 Even after controlling for a variety ofclinical parameters the influence of smoking was substanti-ated. In the study by Duffy et al. from Ann Arbor the influ-ence of smoking, alcohol and depression on quality of life in81 patients with non-terminal head and neck cancer wasmore limited. Controlling for age, tumour site and stage,eight scales of the SF-36V (Short Form 36 Veteran) but nohead and neck specific scales of HNQoL (head and neck qual-ity of life) were adversely influenced by smoking.10
In order to substantiate the connection between smokingand reduced QoL and to examine whether there was apositive effect of smoking cessation, non-smokers weredivided in quitters and never smokers. A significant benefit
on health and survival of smoking cessation have beenshown.21 We have shown a probable positive effect of ces-sation on QoL. Patients not smoking at the examinationbut admitting to have smoked previously had intermediateQoL scores compared with never smokers and persistentsmoker for most endpoints indicating an immediate effectof smoking cessation on QoL endpoints. This intermediateresult could however also be explained by a significant num-ber of reported quitters actually still smoking. This is notunlikely as reported by Hald et al.,22 where resent quitterswere the least trustworthy with respect to self-reportedsmoking status. Furthermore, we do not know the lengthof nicotine abstinence in this population. A difference be-tween quality of life in quitters and continuous smokers

Phy
sica
l Fun
ctio
nC
ogni
tive
Fun
ctio
n
Nau
sea
/ vom
iting
Dys
pnoe
aD
iarr
hoea
App
etite
loss
HN
Wei
ght l
oss
Mean S
core
0
20
40
60
80
100
Never Smokers N=14Quitters N=48Present Smokers N=52
High score = High degree of symptom
High Score = High function
Figure 1 QoL function and symptom scores among 114recurrence free head and neck cancer patients dependent onsmoking status. Symptoms presented are those statisticallydifferent between groups with p < 0.005, Kruskal–Wallis test.
Table 4 Adjusted mean score (and 95% C.I.) of QoLendpoints significantly dependent (p < 0.05) on smokingstatus in a univariate linear model with dichotomous clinicalparameters
Non-smokers Smokers
Role function 80 (71; 89) 68 (58; 78)Cognitive function 89 (82; 96) 73 (65; 81)Fatigue 23 (15; 31) 34 (25; 43)Nausea/vomiting 2 (�3; 7) 12 (7; 18)Pain 17 (10; 25) 30 (22; 39)Dyspnoea 6 (�2; 13) 20 (11; 28)Appetite loss 11 (2; 19) 36 (27; 46)Constipation 10 (3; 17) 22 (14; 30)Diarrhoea 9 (2; 16) 24 (17; 32)Financial problems 8 (�3; 15) 18 (9; 27)HN pain 16 (9; 22) 26 (19; 33)HN swallowing 14 (8; 21) 25 (18; 32)HN senses 19 (10; 28) 32 (22; 42)HN social eating 15 (8; 23) 30 (22; 38)HN dry mouth 45 (34; 55) 61 (49; 73)HN coughed 22 (12; 31) 39 (28; 49)HN nutritional supp. 15 (3; 27) 31 (18; 45)HN feeding tube 5 (�3; 13) 17 (8; 26)HN weight loss 5 (�7; 17) 30 (17; 43)
All endpoints are normalised to a scale from 0–100.
Influence of smoking on health related QoC after treatment for head and neck cancer 191
has, however, been consistently reported in lung cancer andnon-cancer populations.8,9,23
The apparent detrimental effect of smoking on QoL couldalso at least partly be explained by other factors, known to
be associated with smoking, such as socio-economic prob-lems or abuse of other substances. The causative correla-tion between socio-economic factors and health relatedendpoints are only partly known and most certainly multi-dimensional. The measures of socio-economic position (reg-istrar general social class classification, socio economicgroup, household income etc.) is associated differently withhealth related endpoints (general health, anxiety, depres-sion etc.).24 We examined the influence of social factorsby adjusting the influence of smoking for the answer ofHN Social contact. This endpoint could be closer to the defacto parameters influencing morbidity and QoL than theother proxy-variable often used e.g. marital status andnumber of friends. The endpoint would per se be expectedto be a significant explanatory variable in the model be-cause it is collected in the same context (mood, data acqui-sition time-point etc.) as the other QoL endpoints and allmulti-item scales of the questionnaires were significantlycorrelated (data not shown). Adjusting for HN Social contactexplained only a minor part of the answers to the quality oflife questionnaire.
The QLQ endpoint financial problems could be taken as anexpression of the economic factor. But the question regard-ing financial problems only addresses problems caused bydisease and treatment. Those with jobs before the diagnosismight state the most problems caused by disease and treat-ment and patients on social welfare would not necessarilyexperience new economic problems because of disease andtreatment. Thus, we believe that financial problems fromEORTC C30 is a poor indicator of actual financial difficultiesespecially in a society with socialised medicine and socialsecurity systems as the Danish.
Depressive symptoms are correlated with poor quality oflife and with smoking10 and might therefore be a significantconfounder, explaining our findings. However, the questionsfrom EORTC QLQ C30 about emotional distress seemed toexplain even less of the impact of smoking on QoL, than so-cial contact problems.
The consistent influence on cognitive function (memoryand concentration) might be surprising, but is in agreementwith resent findings that long term tobacco exposure re-duces cognitive function even after adjustment for child-hood IQ, occupation and education.25
We have not been able to find any other explanation forour findings than an influence of smoking. We did not haveaccess to validated socio-economic data or informationregarding abuse of other substances. Together with thenon-prospective nature of our study the results needs tobe confirmed.
Nevertheless, the profound impact of continued smokingon survival and morbidity should be taken seriously by pa-tients and therapists, even though smoking intervention isvery difficult in this group of patients.26–28 Any argumentin favour of smoking cessation that the nicotine dependentpatient find relevant to his or her situation, serves to bringhim or her closer to deciding to quit and increases the prob-ability of successful smoking cessation.27 The captivatingargument that sufficient knowledge is present to ‘‘tell peo-ple that smoking is bad’’29 is too simplistic. In contrast, ourfindings stress the need for further research in the correla-tion between objective morbidity as well as quality of lifeand modifiable life style parameters.

192 K. Jensen et al.
Conclusion
Continued smoking after treatment of head and neck canceradversely influenced a wide range of quality of life end-points, of which many were apparently unrelated to the di-rect effect of smoking on the upper aero-digestive tract andlungs. Quitters had better quality of life than patients whocontinued to smoke after treatment, suggesting that smok-ing cessation may improve quality of life in addition toreducing the risk of new cancer.
Acknowledgements
The authors would like to thank the Danish Cancer SocietyGrant DP 03 112, Radiumstationens Forskningsfond, AgnesNiebuhr Anderssons Fond and William Nielsens Mindefondfor financial support.
References
1. Browman GP, Wong G, Hodson I, et al. Influence of cigarettesmoking on the efficacy of radiation therapy in head and neckcancer. N Engl J Med 1993;328:159–63.
2. Overgaard J, Grau C, Johansen LV, Overgaard M. A prospectivestudy evaluating the influence of hemoglobin and smokingduring radiotherapy for head and neck cancer. Radiother Oncol2005;73(suppl 1):S31–2.
3. Do KA, Johnson MM, Lee JJ, et al. Longitudinal study ofsmoking patterns in relation to the development of smoking-related secondary primary tumors in patients with upperaerodigestive tract malignancies. Cancer 2004;101:2837–42.
4. Rugg T, Saunders MI, Dische S. Smoking and mucosal reactionsto radiotherapy. Br J Radiol 1990;63:554–6.
5. Porock D, Nikoletti S, Cameron F. The relationship betweenfactors that impair wound healing and the severity of acuteradiation skin and mucosal toxicities in head and neck cancer.Cancer Nurs 2004;27:71–8.
6. Monson JM, Stark P, Reilly JJ, et al. Clinical radiation pneu-monitis and radiographic changes after thoracic radiationtherapy for lung carcinoma. Cancer 1998;82:842–50.
7. Eifel PJ, Jhingran A, Bodurka DC, Levenback C, Thames H.Correlation of smoking history and other patient characteristicswith major complications of pelvic radiation therapy forcervical cancer. J Clin Oncol 2002;20:3651–7.
8. Wilson D, Parsons J, Wakefield M. The health-related quality-of-life of never smokers, ex-smokers, and light, moderate, andheavy smokers. Prev Med 1999;29:139–44.
9. Garces YI, Yang P, Parkinson J, et al. The relationship betweencigarette smoking and quality of life after lung cancer diagno-sis. Chest 2004;126:1733–41.
10. Duffy SA, Terrell JE, Valenstein M, Ronis DL, Copeland LA,Connors M. Effect of smoking, alcohol, and depression on thequality of life of head and neck cancer patients. Gen HospPsychiatry 2002;24:140–7.
11. Jensen K, Jensen AB, Grau C. A cross sectional quality of lifestudy of 116 recurrence free head and neck cancer patients.The first use of EORTC H&N35 in Danish. Acta Oncol2006;45:28–37.
12. Overgaard J, Hansen HS, Specht L, et al. Five compared withsix fractions per week of conventional radiotherapy of squa-mous-cell carcinoma of head and neck: DAHANCA 6 and 7randomised controlled trial. Lancet 2003;362:933–40.
13. Jensen K, Jensen AB, Grau C. The relationship betweenobserver-based toxicity scoring and patient assessed symptomseverity after treatment for head and neck cancer. A correl-ative cross sectional study of the DAHANCA toxicity scoringsystem and the EORTC quality of life questionnaires. RadiotherOncol, in press.
14. Humphris GM, Rogers SN. The association of cigarette smokingand anxiety, depression and fears of recurrence in patientsfollowing treatment of oral and oropharyngeal malignancy. EurJ Cancer Care (Engl) 2004;13:328–35.
15. Mystakidou K, Tsilika E, Parpa E, Katsouda E, Galanos A, VlahosL. Assessment of anxiety and depression in advanced cancerpatients and their relationship with quality of life. Qual LifeRes 2005;14:1825–33.
16. King MT. The interpretation of scores from the EORTC quality oflife questionnaire QLQ-C30. Qual Life Res 1996;5:555–67.
19. Ringash J, Warde P, Lockwood G, O’Sullivan B, Waldron J,Cummings B. Postradiotherapy quality of life for head-and-neckcancer patients is independent of xerostomia. Int J RadiatOncol Biol Phys 2005;61:1403–7.
20. Sprangers MA, Schwartz CE. Integrating response shift intohealth-related quality of life research: a theoretical model. SocSci Med 1999;48:1507–15.
21. Edwards R. The problem of tobacco smoking. BMJ2004;328:217–9.
22. Hald J, Overgaard J, Grau C. Evaluation of objective measuresof smoking status––a prospective clinical study in a group ofhead and neck cancer patients treated with radiotherapy. ActaOncol 2003;42:154–9.
23. Tillmann M, Silcock J. A comparison of smokers’ and ex-smokers’ health-related quality of life. J Public Health Med1997;19:268–73.
24. Macintyre S, McKay L, Der G, Hiscock R. Socio-economicposition and health: what you observe depends on how youmeasure it. J Public Health Med 2003;25:288–94.
25. Whalley LJ, Fox HC, Deary IJ, Starr JM. Childhood IQ, smoking,and cognitive change from age 11 to 64 years. Addict Behav2005;30:77–88.
26. List MA, Siston A, Haraf D, et al. Quality of life and perfor-mance in advanced head and neck cancer patients on concom-itant chemoradiotherapy: a prospective examination. J ClinOncol 1999;17:1020–8.
27. Schnoll RA, Zhang B, Rue M, et al. Brief physician-initiatedquit-smoking strategies for clinical oncology settings: a trialcoordinated by the Eastern Cooperative Oncology Group. J ClinOncol 2003;21:355–65.
28. Des RC, Dische S, Saunders MI. The problem of cigarettesmoking in radiotherapy for cancer in the head and neck. ClinOncol (R Coll Radiol) 1992;4:214–6.
29. Mazzone PJ, Arroliga AC. How many ways can we say thatcigarette smoking is bad for you? Chest 2004;126:1717–8.