-
Small boweltransplantation e the latestdevelopmentsAlan
Wiles
Simon Gabe
Stephen Middleton
agents such as alemtuzumab (Campath-1H) in the 1990s,11,12
and
as reported by the international registry,10 (which receives
details of >90% of all cases world wide) is lower (Table 1)
but
this survival gap is continuing to close. In the better
performing
centres,17,18 survival figures approximate to those on HPN,
particularly for patients given lymphocyte-depleting
induction
therapy, whose survival at 1 and 5 years has been reported to
be
as high as 90% and 70% respectively.17 Patient survival at
the
largest UK adult transplantation centre in Cambridge has
also
improved, with 2-year non-oncological survival pre- and
post-
2007 of 50% and 100% respectively, associated with a 10-fold
increase in procedures undertaken per year. The larger of the
UK
paediatric transplantation centres, in Birmingham, also has
improved results, reporting 69% 3-year survival since 1998
and
31% before this.19 If these improved survival rates are
repro-
duced in other centres and prove a match for those of HPN at
10 years, intestinal transplantation may become the
preferred
primary treatment for irreversible intestinal failure, rather
than
being largely reserved for those who respond poorly to HPN.
It
TRANSPLANTATIONAlan Wiles BA DPhil BMBCh MRCP is a Senior
Transplantation Fellow at
Addenbrookes Hospital, Cambridge University NHS Trust and
has
recently been appointed as a Consultant Gastroenterologist at
Queen
Elizabeth Hospital, Kings Lynn, UK. Competing interests: none
declared.
Simon Gabe BSc MD MSc FRCP is a Consultant Gastroenterologist at
St
Marks Hospital in Harrow, UK. Competing interests: none
declared.
Stephen Middleton MA MD FRCP FAHE is a Consultant Physician
and
Gastroenterologist at Addenbrookes NHS Trust, Cambridge
University
Teaching Hospital, UK. Competing interests: none
declared.AbstractIntestinal transplantation has become a routine
clinical procedure for
selected patients. Over the last 10 years patient survival
figures have
improved considerably and are now approaching those receiving
organs
such as liver, lungandheart. Patient selectionhas improvedand
immunosup-
pression has been enhanced by the introduction of lymphocyte
modulating
antibody therapy combined with less potent maintenance
immunosuppres-
sion. The indications for intestinal transplantation remain
conservative at
present and largely reserve this procedure for patients who have
life threat-
ening complications of parenteral nutrition or require surgical
procedures
that make simultaneous or subsequent transplantation
advantageous.
However, as survival figures improve the indications are
beginning to
broaden to include consideration of quality of life. Survival
after transplanta-
tion is approaching that associated with uncomplicated
parenteral nutrition
and if this trend continues it may replace parenteral nutrition
as the treat-
ment of choice for patients with irreversible intestinal
failure. This article
describes the current indications for intestinal transplantation
and the
current results of the procedure. Guidelines for referring
patients for trans-
plantationassessment and for themanagementof the sick transplant
patient
are given. The need to consider referral of patients at an early
stage to allow
timely assessment for transplantation is also discussed.
Keywords infections; intestinal; multivisceral; NASIT;
nutrition;
transplantation
A brief history of intestinal transplantation
The earliest significant innovations in the technical aspects
of
intestinal transplantation are considered to be the canine
models
developed by Richard Lillehei in the 1950s1 and 60s,2 and
the
vascular anastomotic techniques ofCarrel.3Graft rejection
impededMEDICINE 39:3 183the appreciation that thorough preoperative
preparation, patient
selection and scrupulous postoperativemanagement are of
critical
importance (Figure 1).13 Now, intestinal transplantation can
be
considered as a routine component of the management of adult
and paediatric patients with intestinal failure, and is
beginning to
replace parenteral nutrition in the long-termmanagement
strategy
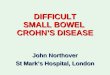
for many of these patients. Currently, children tend to have
better
survival than adults after 5 years (Figure 2).
The current role of transplantation in the management of
intestinal failure
The survival rates of patients requiring home parenteral
nutrition
(HPN) range between 86e97% at 1 year, 57e83% at 5 years and
43e71% at 10 years.14e16 Survival following intestinal
trans-
plantation (any combination of organs including small
intestine),progress but following the introduction of a series of
powerful anti-
rejection agents in the late 1980s,4,5 a cluster of reports
appeared
describing transplantation of part or all the intestine both
in
combination with other organs and as isolated grafts.6e9
However, long-term survival remained modest at best10 until
the introduction of lymphocyte-depleting induction therapy
with
Whats new?
C Improved survival figures: 1 year 85%; 5 years 70%
C Survival gap between home parenteral nutrition (HPN) and
transplantation is closing
C Quality of life on home parenteral nutrition HPN can be
improved by transplantation
C National Adult Intestinal Transplantation (NASIT) Forum e
UK
forum to discuss all patients before transplantation
C CaMi (Cambridge-Miami) score: first preoperative scoring
system to estimate postoperative survival following
intestinal
transplantation
C It is now a requirement that all suitable patients should
be
referred (or discussed) for assessment at an appropriate
stage
before they lose the opportunity of transplantation 2010
Elsevier Ltd. All rights reserved.
-
Su
rviv
al
pro
ba
bil
ity
Years
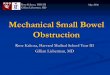
Logrank p < 0.001 1: 19851989
2: 19901994
3: 19952000
4: 20002004
5: 20052009
0.0 1
2
3
4
5
23
131
409
757
856
4
39
146
196
0
1
25
68
0
1
10
0
0
0
0 20
0.6
0.8
1.0
0.4
0.2
5 10 15
Patient survival following intestinal transplantation in
different eras
between 1985 and 2009
Figure 1
Su
rviv
al
pro
ba
bil
ity
Years
Logrank p < 0.584 1: 02
2: 36
3: 717
4: 18-50
5: 51+
0.0 1
2
3
4
5
360
123
116
392
125
100
39
35
100
34
0
0
0
0
0
0 6
0.6
0.8
1.0
0.4
0.2
2 1 3
21
14
8
18
4
4 5
Patient survival following intestinal transplantation according
to age
of patient
Figure 2
TRANSPLANTATION
MEDICINE 39:3 184 2010 Elsevier Ltd. All rights reserved.
-
C Severe liver disease or progressive disease despite all
reme-
dial actions.
(b) Recurrent septic episodes
C IF patients who have severe septic complications (i.e.
life-
threatening line infection needing admission to ITU, or
recurrent yeast or candidal infections).
(c) Lack of central venous access
C For isolated intestine: venous access limited to three
major
sites.
C For intestine as part of a cluster graft: venous access
limited to
four major sites.
2. Very poor quality of life thought to be correctable by
transplantation.
3. Patients with indications for extensive surgery involving
partial
or complete evisceration:
Adults
(a) Surgery to remove a large proportion of the abdominal
viscera
that is considered untenable without associated
multi-visceral
transplantation (e.g. extensive desmoid disease, extensive
severe mesenteric arterial disease requiring intervention).
(b) Localized malignancy considered to be amenable to
curative
resection that would necessitate extensive evisceration
(e.g.
localized neuroendocrine tumours and cholangiocarcinoma e
particular caution should be exercised with this group).
Children
(a) Surgery that will lead to:
C Terminal gastrostomy
C Terminal duodenostomy
C Ultra short bowel: In children
-
isolated intestine liver and intestine multivisceral (liver,
intestine, stomach, pancreas) modified multi-visceral (intestine,
stomach, pancreas).In addition, patients may undergo renal
transplantation and some
centres favour splenic transplantation for immunological
reasons.
Patients invariably have an ileostomy, at least initially, to
provide
access for ileoscopic surveillance biopsies to detect rejection.
A
few centres transplant the large intestine and abdominal
wall.
Following surgery it is usual for an ITU stay of 2 or 3
days,
then HDU for 2 or 3 weeks, and finally a less intensive ward
stay
for a further 4e6 weeks to establish full enteral nutrition,
satis-
factory immunosuppression and resolution of any
postoperative
problems such as infection.
Infection is the commonest postoperative complication (Table
3). Rejection is now less of a problem since the introduction
of
lymphocyte-depleting agents, but early detection and
treatment
remain a pivotal part of the process and surveillance biopsies
via
the stoma are undertaken at least three times a week in the
first
month. Fluid and electrolyte balance are also frequently
chal-
lenging but of critical importance, to prevent the downward
spiral triggered by a confluence of salt and water
imbalance,
impaired renal function and sepsis, which may result in
multi-
organ failure. At this point, other pre-existing co-morbidities
and
the lack of venous access for treatments such as dialysis
can
result in inexorable deterioration. The postoperative
manage-
ment of these patients is complex and requires a fully
integrated
team of consultants from a broad range of specialties who
are
well motivated and able to provide prompt consultant-led
expertise. The combination of inducing profound immunosup-
pression and transplanting an organ with very high
antigenicity
that also contains a host of potential pathogens produces
Common infections following intestinal transplantation (in the
UK)
Location Likely pathogens Clinica l features Diagnosis
Treatment
Bacterial Central line related
Superficial
surgical site:
Pneumonia
Abdominal collection/
peritonitis
Staphylococcus aureus
(incl. MRSA)
Escherichia coli
Klebsiella,
Pseudomonas.
Coagulase-negative
Staphylococci:
(IV line infections only)
Brisk deterioration/septic
shock/and organ-specific
features
(respiratory, urinary,
intra-abdominal)
Lower-grade sepsis with
coagulase-negative
Staphylococci
Cause of death in 18%
Blood cultures/pneumococcal/
Legionella urinary antigens
Organ-specific: broncho-
alveolar lavage (BAL);
sputum, urine culture, etc.
Intra-abdominal scans
Initially broad-spectrum
antibiotics then adjust
to include sensitivities
of known organisms.
Need to cover, MRSA
and other potential
hospital-acquired
infections
Fungal Aspergillosis:
Wound, pulmonary,
disseminated,
cerebral
Aspergillus fumigatus Antibiotic-resistant
pneumonia
Aspergillosis is serious,
particularly disseminated,
and intra-cerebral
is usually fatal
Chest CT scan
BAL and trans-bronchial
biopsy PCR
Aspergillosis with
amphotericin/
AmBisome, voriconazole
or caspofungin
Candidal Candidiasis:
oropharyngeal,
genitourinary,
wound related,
line infections.
Candida albicans Antibiotic-resistant
sepsis
Blood and urine culture,
line tip culture.
AmBisome/
caspofungin
Fluconazole if
mild/known to be
sensitive.
Viral CMV looks for colitis, Influenza virus Flu-like
illness
ase
ken
um
fec
ase
ula
fec
fec
ase
Nose and throat swabs, Antivirals, depending
TRANSPLANTATIONhepatitis and retinitis.
EBV PTLD late:
>1 year
Respiratory syncytial
virus (RSV) or
parainfluenza
virus 3
Cytomegalovirus (CMV)
Varicella-zoster virus
(VZV)
Herpes simplex virus 1
or 2 (HSV-1/2)
EpsteinBarr virus (EBV)
Human herpes virus 6
(HHV-6)
Adenovirus
Pneumonia
Organ dise
Severe chic
zoster, pne
Systemic in
organ dise
From gland
to PTLD
Systemic in
fever
Systemic in
organ dise
Table 3MEDICINE 39:3 186pox or
onitis
tion,
r fever
tion,
tion,
nasopharyngeal aspirate,
broncho-pulmonary
lavage PCR
on circulating strains
Nebulized ribavirin
Ganciclovir
Acyclovir
Acyclovir
Discuss with virologist
and haematologist
Discuss with virologist
Cidofovir (discuss with
virologist) 2010 Elsevier Ltd. All rights reserved.
-
a unique clinical setting, where patients often respond in
an
unusual way to infections and treatments.
Which patients should be referred to a transplant centre for
consideration?
The management of all patients with intestinal failure should
now
include consideration of the potential role of transplantation.
It is
important to make every attempt to treat reversible disease
and
thorough intestinal rehabilitation can often restore
adequate
enteral nutrition. In the UK, this process is undertaken in
regional
or national intestinal failure (IF) centres. The regional
(medium-
volume) centres have a nutrition team and clinical staff
with
subspecialty interests in the management of intestinal
failure
patients. For themore complex patients,
especiallywheremultiple
surgical procedures are thought necessary, the UK has two
national IF centres. These centres have specialist medical
and
surgical staff that are dedicated to intestinal failure work and
have
a high enough volume of these complex patients to build up a
high
level of corporate experience. This system is very efficient as
it
allows appropriate escalation and concentrates experience of
the
less frequent, highly complex patients, who require a very
rounded team of clinicians to manage them effectively. In
most
cases, patients fulfilling the criteria for transplantation
(Table 2) or
who are approaching this situation (Table 4) should be
referred.
Particular attention should be given to those who are likely
tomiss
the window of opportunity. These patients often have
progressive
disease, which may advance to a point that contraindicates
transplantation or results in death whilst they are on the
waiting
list. Examples of this include patients who are rapidly
losing
venous access points and those bleeding fromportal
hypertension.
Special consideration should also be given to PN-dependent
patients who require transplantation of other organs. They
may
benefit from a cluster graft including intestine rather than
have
a subsequent intestinal transplantation in the setting of an
existing
graft and consequent immunosuppression.
Red-flag indicators for referral for transplant assessment
[In addition to the standard indications for transplantation e
Table 2]
Patients with intestinal failure and one or more of the
following:
C Abnormal LFTs Persistent elevation of hepatic enzymes may
indicate PN-associated hepatic fibrosis or
cirrhosis
Assessment of liver including biopsy, optimize
HPN and exclude other causes. Refer to or
discuss with national IF or transplant centre
C Frequent line sepsis Patients with three or more episodes of
line
sepsis in a year or one episode of life-
threatening sepsis may be candidates for
transplantation particularly if there are other
relative indications
Refer to/discuss with national IF centre
C Ultra-short bowel syndrome Less than 40 cm of jejunum to a
stoma is
associated with rapid-onset liver disease
Refer to/discuss with a National IF or
transplant centre
C Co-existing diabetes mellitus with
complication
Diabetic complications are often indications
for pancreatic transplantation and if advanced
increase the risk associated with intestinal
transplantation. Patients may benefit from
early combined transplantation
Refer to transplantation centre for
consideration of combined pancreas and small
bowel transplantation
abd
e in
ion
my
p fo
a-pe
on
nin
s. E
erab
eria
e a
TRANSPLANTATIONa The UK National Desmoid Centre is at St Marks
hospital, Harrow, London.
Table 4C Pseudo-obstruction. Complicated by
severe abdominal pain
Patients with intractable
distended small and larg
benefit from transplantat
colectomy and enterecto
a relatively high-risk grou
of intestines reduces intr
subsequent transplantati
Patients without intestinal failure
C Desmoid disease Extensive disease threate
other important structure
intervention may be pref
C Mesenteric vascular disease Extensive mesenteric art
disease involving intestin
intra-abdominal organsMEDICINE 39:3 187ominal pain from
testine may
rather than
and PN. They are
r PN and removal
ritoneal space for
Refer patient to transplant centre
g or damaging
arly surgical
le
Refer to transplantation centre for assessment
or to the national desmoid centrea
l or venous
nd other essential
Refer to transplantation centre for assessment
or to the national desmoid centre 2010 Elsevier Ltd. All rights
reserved.
-
given this opportunity at an appropriate stage.
There are certain red flag indicators for referral to a main
centre (Table 4) in addition to the standard indications for
trans-
plantation (Table 2). This is not an exhaustive list of
high-risk
factors but provides a guide to the type of situation that
should
prompt the gastroenterologist to consider referral, to
either
a national IF centre or a transplant centre, for further
consideration.
Conclusion
Considerable advances over the last 20 years have taken
intes-
tinal transplantation from the first procedures that provided
only
short-term success to its current status as a routine
therapeutic
option for selected patients. Although HPN remains the
primary
treatment for most patients with intestinal failure, we
approach
the threshold of a new era when intestinal transplantation will
be
considered to be the primary treatment for most patients.
This
promises to be cost effective and bring with it better quality
of life
for patients without reducing their longevity. A key element
of
success is appropriate timing of referral to a national IF
or
transplantation centre. All gastroenterologists should be aware
of
when and how to refer patients, and seek advice early in the
management of the more complex patients. A
REFERENCES
1 Lillehei RC, Miller FA. The physiological response of the dog
small
intestine including prolonged in vitro preservation of the bowel
with
successful replacement and survival. Ann Surg 1959; 159:
543e61.
sodium and water balance with spot urinary sodium and
TRANSPLANTATIONWhat is the likely future demand for intestinal
transplantation?
The ongoing improvement in postoperative survival brings with
it
broadening of the indications for transplantation to include
larger
numbers of patients. The point prevalences of adult patients
receiving HPN in the UK in 2007 and 2008 were 867 and 856
respectively, with estimated paediatric prevalences of 28 and
128
respectively. In the corresponding years, the incidences of
adult
HPN patients were 138 and 157 respectively and for
paediatrics,
nine and eight respectively. Themajority of adult patients are
aged
-
2 Lillehei RC, Idezuki Y, Feemster JA, et al. Transplantation of
stomach,
intestine, and pancreas: experimental and clinical
observations.
Surgery 1967; 62: 721e41.
3 Carrel A. The transplantation of organs. A preliminary
communica-
tion. JAMA 1905; 45.
4 Calne RY, White DJ, Thiru S, et al. Cyclosporin A in patients
receiving
renal allografts from cadaver donors. Lancet 1978; 2:
1323e7.
5 Calne RY. Cyclosporine and liver transplantation. Mt Sinai J
Med
1987; 54: 465e6.
6 Grant D, Wall W, Mimeault R, et al. Successful
small-bowel/liver
transplantation. Lancet 1990; 335: 181e4.
7 Starzl TE, Rowe MI, Todo S, et al. Transplantation of
multiple
abdominal viscera. JAMA 1989; 261: 1449e57.
8 Deltz E, Schroeder P, Gundlach M, Hansmann ML, Leimenstoll
G.
Successful clinical small-bowel transplantation. Transplant
Proc
1990; 22: 2501.
19 Gupte GL, Beath SV, Protheroe S, et al. Improved outcome of
referrals
for intestinal transplantation in the UK. Arch Dis Child 2007;
92:
147e52.
20 Cameron EA, Binnie JA, Jamieson NV, Pollard S, Middleton SJ.
Quality
of life in adults following small bowel transplantation.
Transplant
Proc 2002; 34: 965e6.
21 DiMartini A, Rovera GM, Graham TO, et al. Quality of life
after small
intestinal transplantation and among home parenteral
nutrition
patients. JPEN J Parenter Enteral Nutr 1998; 22: 357e62.
22 Rovera GM, DiMartini A, Schoen RE, et al. Quality of life of
patients
after intestinal transplantation. Transplantation 1998; 66:
1141e5.
23 American Gastroenterological Association medical position
state-
ment: short bowel syndrome and intestinal transplantation.
Gastroenterology 2003; 124: 1105e10.
24 Middleton SJ. Is intestinal transplantation now an
alternative to
home parenteral nutrition? Proc Nutr Soc 2007; 66: 316e20.
25 BANS. Annual BANS report. Artificial nutrition support in the
UK,
www.bapen.org.uk 2009, 978-1-899467-51-8.
26 Jones BJ. Recent developments in the delivery of home
parenteral
nutrition in the UK. Proc Nutr Soc 2003; 62: 719e25.
Practice points
C The possibility of future intestinal transplantation should
be
considered in the management of all intestinal failure (IF)
patients and those with extensive benign intra-abdominal
disease.
C IF patients with significant complications of PN should be
referred for transplantation assessment (National IF or
trans-
plantation centre) or at least discussed with a centre.
C Care should be taken not to allow IF patients to
deteriorate
past the point when transplantation is possible.
C Sick transplant patients must be treated without delay and
advice should be sought from their transplantation centre
immediately on presentation.
C The early use of appropriate broad-spectrum antimicrobial
TRANSPLANTATION9 Aleksic I, Czer LS, Admon D, et al. Survival of
acute intestinal infarction
after cardiac transplantation. Thorac Cardiovasc Surg 1995; 43:
352e4.
10 Grant. Intestinal transplant registry,
www.lhsc.on.ca/itr2009; 2009.
11 Middleton SJ, Pollard S, Friend PJ, et al. Adult small
intestinal
transplantation in England and Wales. Br J Surg 2003; 90:
723e7.
12 Tzakis AG, Kato T, Nishida S, et al. Alemtuzumab
(Campath-1H)
combined with tacrolimus in intestinal and multivisceral
trans-
plantation. Transplantation 2003; 75: 1512e7.
13 Middleton SJ, Nishida S, Tzakis A, et al. Cambridge-Miami
score for
intestinal transplantation preoperative risk assessment:
initial
development and validation. Transplant Proc 2010; 42: 19e21.
14 Messing B, Crenn P, Beau P, et al. Long-term survival and
parenteral
nutrition dependence in adult patients with the short bowel
syndrome. Gastroenterology 1999; 117: 1043e50.
15 Pironi L, Paganelli F, Labate AM, et al. Safety and efficacy
of home
parenteral nutrition for chronic intestinal failure: a 16-year
experi-
ence at a single centre. Dig Liver Dis 2003; 35: 314e24.
16 Lloyd DA, Vega R, Bassett P, Forbes A, Gabe SM. Survival and
depen-
dence on home parenteral nutrition: experience over a 25-year
period
in a UK referral centre. Aliment Pharmacol Ther 2006; 24:
1231e40.
17 Abu-Elmagd KM, Costa G, Bond GJ, et al. Five hundred
intestinal and
multivisceral transplantations at a single center: major
advances with
new challenges. Ann Surg 2009. [Epub ahead of print].
18 Nishida S, Levi D, Kato T, et al. Ninety-five cases of
intestinal
transplantation at the University of Miami. J Gastrointest Surg
2002;
6: 233e9.MEDICINE 39:3 189agents in sick transplantation
patients is essential as they are
most likely to have infection. 2010 Elsevier Ltd. All rights
reserved.
Small bowel transplantation the latest developmentsA brief
history of intestinal transplantationThe current role of
transplantation in the management of intestinal failureWhat does
intestinal transplantation involve?Which patients should be
referred to a transplant centre for consideration?What is the
likely future demand for intestinal transplantation?Why do
gastroenterologists need to know about intestinal
transplantation?ConclusionReferences