Embed Size (px)
DESCRIPTION
anak
Citation preview

11
feb04feb04
PEDIATRIC CARDIOLOGYPEDIATRIC CARDIOLOGY
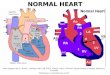
Normal HeartNormal Heart
RA
RV
LV
LA
ICV
SCV
PA
AO

22
GENERAL PRINCIPLESGENERAL PRINCIPLES
Pediatric Cardiology :Pediatric Cardiology :
1. Congenital Heart Disease (CHD, PJB)1. Congenital Heart Disease (CHD, PJB)
Occurs since organogenesisOccurs since organogenesis
2. Acquired Heart Disease (AHD, PJD)2. Acquired Heart Disease (AHD, PJD)
Disturbance of normal heart Disturbance of normal heart

33
INCIDENCEINCIDENCE
CHDCHD : : 6-8/1000 live births6-8/1000 live births8 types of CHD (85%) : 8 types of CHD (85%) :
VSD, ASD, PDA, PS, AS, TF, TGAVSD, ASD, PDA, PS, AS, TF, TGA
AHD :AHD :Neonatus : virus (Echo, Influenzae)Neonatus : virus (Echo, Influenzae)5 - 15 yrs : RF5 - 15 yrs : RF

44
ETIOLOGYETIOLOGYCHD :CHD : 90% genetic – environmental factors90% genetic – environmental factors
Environment : Environment :
11stst trimester pregnancy trimester pregnancy organogenesis of the organogenesis of the heart : heart : radiation, smoking, drugs (thalidomide), radiation, smoking, drugs (thalidomide), maternal infection (rubella), mother age (young / maternal infection (rubella), mother age (young / old), high geografic location (less O2 ), metabolic old), high geografic location (less O2 ), metabolic disorders (DM)disorders (DM)
AHDAHD : : -- infection (RF, diphtheriae)infection (RF, diphtheriae)
- neonatus (Coxsackie B virus)- neonatus (Coxsackie B virus)

55
FETAL CIRCULATIONFETAL CIRCULATION

66
FETAL CIRCULATIONFETAL CIRCULATION
Signs :Signs :Parallel systemic and pulmonary circulationsParallel systemic and pulmonary circulations
Foramen ovale, ductus Botalli, ductusForamen ovale, ductus Botalli, ductus
venosus : still openvenosus : still open
RA : enlargement, cross circulationRA : enlargement, cross circulation
Head, heart and upper extremities are Head, heart and upper extremities are supplied by high O2 content supplied by high O2 content
Minimal pulmonary circulation Minimal pulmonary circulation

77
CIRCULATION AFTER BIRTH CIRCULATION AFTER BIRTH
After birth : After birth : Expansion of lung Expansion of lung Placenta circulation endedPlacenta circulation ended
Systemic and pulmonary circulation Systemic and pulmonary circulation serial typeserial type
No cross circulation in RANo cross circulation in RA
Foramen ovale, d. Botalli & d. Venosus Foramen ovale, d. Botalli & d. Venosus closedclosed

88
CyanosisCyanosis
Reduced Hb > 5 gr% (N=2,25 gr%)Reduced Hb > 5 gr% (N=2,25 gr%)
2 types :2 types :a.a. Central C :Central C :
arterial unsaturationarterial unsaturation generalized and severegeneralized and severe
b.b. Peripheral C :Peripheral C : without arterial unsaturationwithout arterial unsaturation localized and milderlocalized and milder
Distinction between a and b : Distinction between a and b :
measurement of arterial O2 content (N=95%).measurement of arterial O2 content (N=95%).

99
Influence of Hb levels on C: Influence of Hb levels on C:
1.1. Hb. 20 gr %, 70% saturationHb. 20 gr %, 70% saturation
Reduced Hb = 30 % x 20 gr % = 6 gr % Reduced Hb = 30 % x 20 gr % = 6 gr %
(C +)(C +)
2.2. Hb 6 gr %, 70% saturationHb 6 gr %, 70% saturation
Reduced HB = 30 % x 6 gr% = 1.8 gr % (C -)Reduced HB = 30 % x 6 gr% = 1.8 gr % (C -)

1010
a.a. Central CCentral C : :
Pulmonary C :Pulmonary C :
Lung disorders (diffusion, ventilation, Lung disorders (diffusion, ventilation,
perfusion)perfusion)
Cerebral C:Cerebral C:
Brain disorders Brain disorders center of respiration center of respiration
Cardial C: Cardial C:
R – L shuntR – L shunt

1111
Hyperoxic (100% O2) test / Crying :Hyperoxic (100% O2) test / Crying :
pulmonary C pulmonary C less/no C less/no C
cardial C cardial C C still persist C still persist
b.b. Peripheral CPeripheral C
Decreased cardiac outputDecreased cardiac output

1212
CONGENITAL HEART DISEASE (CHD)CONGENITAL HEART DISEASE (CHD)
Early signs of CHDEarly signs of CHD
CyanosisCyanosis
Inadequate intakeInadequate intake
Heart murmurHeart murmur
Unpalpable femoral and brachial pulse Unpalpable femoral and brachial pulse
Circulation collapsCirculation collaps
ArrhythmiaArrhythmia

1313
ASD
RA
LA
RVLV
ATRIAL SEPTAL DEFECT (ASD)ATRIAL SEPTAL DEFECT (ASD)

1414
Any opening (defect) in the atrial septum Any opening (defect) in the atrial septum shunt shunt
Ostium Secundum (50-70%)Ostium Secundum (50-70%)
Hemodynamic : depends on the size, compliance Hemodynamic : depends on the size, compliance
of V and resistance of Pulm. and Syst. circulationof V and resistance of Pulm. and Syst. circulation
ATRIAL SEPTAL DEFECT (ASD)ATRIAL SEPTAL DEFECT (ASD)

1515
Signs/Symptoms :Signs/Symptoms :
Usually asymptomatic, mmr is found by chanceUsually asymptomatic, mmr is found by chance
Fatigue, dyspnea, recurrent respiratory infection.Fatigue, dyspnea, recurrent respiratory infection.
Ausc. : ( mmr may be absent in infants)Ausc. : ( mmr may be absent in infants)
widely split and fixed S2widely split and fixed S2

1616
X ray : increased PBF X ray : increased PBF
ECG : RAD, RVHECG : RAD, RVH
Echo : position and size of the defectEcho : position and size of the defect
Catheterization : OCatheterization : O22 in RA > CV in RA > CV

1717
ManagementManagement
To favour the spontaneous closure of ASD To favour the spontaneous closure of ASD (87%)(87%)
Transcatheter closure (Transcatheter closure (Amplatzer Septal Amplatzer Septal OccluderOccluder))
Surgical closure :Surgical closure :
Indication : P / S ratio Indication : P / S ratio ≥ 1.5 : 1≥ 1.5 : 1

1818
VENTRICULAR SEPTAL DEFECT VENTRICULAR SEPTAL DEFECT (VSD)(VSD)
VSD
RA LV
LA
RV

1919
VENTRICULAR SEPTAL DEFECT VENTRICULAR SEPTAL DEFECT (VSD)(VSD)
Defect in the ventricular septumDefect in the ventricular septum
Prevalence : CHD no.1 (25%)Prevalence : CHD no.1 (25%)
Hemodynamic :Hemodynamic :
– Depends on the size and pressure between Depends on the size and pressure between RV and LVRV and LV
– Pressure LV > RV Pressure LV > RV L-R shunt L-R shunt
– R-L, L-R, R-L (R-L, L-R, R-L (Eisenmenger SEisenmenger S) )

2020
SIMPLE VSDSIMPLE VSD
20 % of CHD, 25 % of VSD20 % of CHD, 25 % of VSD
Small 1-5 mm, Moderate 5-10 mmSmall 1-5 mm, Moderate 5-10 mm
Asymptomatic : Asymptomatic : Roger’s diseaseRoger’s disease
Normal G-D, mmr heard at Week 1Normal G-D, mmr heard at Week 1

2121
MODERATE VSDMODERATE VSD
Fatigue, intol.activity, dyspnea, recurrent Fatigue, intol.activity, dyspnea, recurrent
resp.tr infectionresp.tr infection
Pansystolic (holosystolic) 3-4/6, pm LSB Pansystolic (holosystolic) 3-4/6, pm LSB
3-53-5

2222
X-ray : - increased PBF
ECG : Small VSD normal
Moderate VSD LVH (+LAE)
Catheterization : O2 in RV > RA
ECHO : nr, size, location

2323
Management Management : :
Nonsurgical closureNonsurgical closure : :
Amplatzer septal occluderAmplatzer septal occluder
SurgicalSurgical : infant with large VSD + CHF : infant with large VSD + CHF
PrognosisPrognosis : :
Perimembranous Perimembranous : surgical intervention: surgical intervention
Muscular defectMuscular defect : spontaneous closure : spontaneous closure

2424
PATENT DUCTUS ARTERIOSUS (PDA)PATENT DUCTUS ARTERIOSUS (PDA)
PDA
LV
AO
AP
LA
RVRA

2525
PATENT DUCTUS ARTERIOSUS (PDA)PATENT DUCTUS ARTERIOSUS (PDA)
Incidence : 12 % CHD (nr. 2), F > MIncidence : 12 % CHD (nr. 2), F > M
Anatomy/physiology : Anatomy/physiology : Intrauterine: AP Intrauterine: AP d. Botalli d. Botalli Aorta Aorta Extrauterine: d. Botalli 10–15 hrs still Extrauterine: d. Botalli 10–15 hrs still
openopen
L-R shunt (syst-diast) L-R shunt (syst-diast) continuous continuous mmr mmr

2626
TYPICAL PDA (SIMPLE PDA)TYPICAL PDA (SIMPLE PDA)Clin. Manifestations :Clin. Manifestations :
asymptomatic, recurrent resp. tr.infectionasymptomatic, recurrent resp. tr.infectioncontinuous mmr at LSB2continuous mmr at LSB2
Echo : direction of shunt & Ø PDAEcho : direction of shunt & Ø PDA
Prognosis : rarely closed spontaneously (1 yr),Prognosis : rarely closed spontaneously (1 yr),
except in premature babies)except in premature babies)
Management : Management :
Surgical closure (ligation)Surgical closure (ligation)
Nonsurgical closureNonsurgical closure : Amplatzer Ductal Occluder : Amplatzer Ductal Occluder

2727
PULMONARY STENOSIS (PS)PULMONARY STENOSIS (PS)
PS
RVLV
LA
RA
PA
AO

2828
PULMONARY STENOSIS (PS)PULMONARY STENOSIS (PS)
Difference of syst.pressure between RV and PA Difference of syst.pressure between RV and PA > 100 mmHg> 100 mmHg
Hemodynamic :Hemodynamic : RV activity increased RV activity increased RVH RVH PS + VSD PS + VSD R-L shunt (cardial cyanosis) R-L shunt (cardial cyanosis)
rarely CHFrarely CHF
Pulmonary ejection click (valve opening)Pulmonary ejection click (valve opening)

2929
Clin.Manif. Clin.Manif.
Eject. Syst mmr LSB2Eject. Syst mmr LSB2
X-ray : PBF <<, cardiomegaly X-ray : PBF <<, cardiomegaly
ECG : RAD , RVH ECG : RAD , RVH Echo : thick pulmonary valve, dilated PAEcho : thick pulmonary valve, dilated PA
CineangioCineangio : : a jet contrasta jet contrast Management :- Management :- Balloon valvuloplastyBalloon valvuloplastySurgery if balloon failtSurgery if balloon failt

3030
COARCTATION OF THE AORTA (CoA)COARCTATION OF THE AORTA (CoA)
Narrowing of the aorta. Turner Syndrome
Frequency : 5 – 8% CHD, M > F
Location : distal of left subclavian artery
2 types : 1. Preductal (CoA + Systemic LV/RV)
2. Postductal (CoA + Sytemic LV)
Hemodynamic :
Adequate O2 to distal of CoA :(Adaptation mechanism)
1. Increased systolic pressure at proximal of CoA
2. Increased diastolic pressure at distal of CoA
(arterioles vasoconstriction)
3. Collateral circulation (subclavian a, intercostal, etc)

3131
COARCTATION OF THE AORTA (CoA)COARCTATION OF THE AORTA (CoA)
CoA
LA
LV
RVRA
AO
PA

3232
Postductal CoAPostductal CoA
Clin.ManifestationsClin.Manifestations
Pain of calves, headaches, nose Pain of calves, headaches, nose bleeds, epistaxisbleeds, epistaxis
BP Hypertenssion (pathognomonic)BP Hypertenssion (pathognomonic)
Brachial – Femoral lagBrachial – Femoral lag
Reduced / abcent lower extremity Reduced / abcent lower extremity pulsespulses

3333
X-ray :X-ray :Rib notching (collateral vessels)Rib notching (collateral vessels)E sign on barium meals E sign on barium meals
ECHO / Doppler : ECHO / Doppler : Gradient and pattern of diastolic flowGradient and pattern of diastolic flow
Catheterization : Catheterization : Confirmation of diagnosisConfirmation of diagnosis
Management :Management :Surgery, balloon angioplastySurgery, balloon angioplasty

3434
TETRALOGI OF FALLOT (TF)TETRALOGI OF FALLOT (TF)
VSD
PS
OvA
RVH
AO
AP
LV
LA
RA

3535
TETRALOGI OF FALLOT (TF)TETRALOGI OF FALLOT (TF)
4 defects : 4 defects :
VSD, PS, RVH, Overriding of the AortaVSD, PS, RVH, Overriding of the AortaFrequency : Frequency :
10-15% CHD, cyanotic CHD no.1 (75%)10-15% CHD, cyanotic CHD no.1 (75%)
Hemodynamic :Hemodynamic : PS + VSD PS + VSD R-L shunt R-L shunt CyanosisCyanosis R-L shunt R-L shunt polycytemia & tromboemboly polycytemia & tromboemboly

3636
Clin.Manifestation : Clin.Manifestation :
Clubbing fingers, scoliosis, squatting Clubbing fingers, scoliosis, squatting
positionposition
Ejection systolic mmr LSB3-4Ejection systolic mmr LSB3-4
Lab : Hb, Ht, RBC levels inreasedLab : Hb, Ht, RBC levels inreased

3737
Echo : Echo : VSD, Overriding Ao, RVOT obstructionVSD, Overriding Ao, RVOT obstruction
X-Ray : X-Ray : couer en sabotcouer en sabot, RVH, PBF , RVH, PBF
Complication : Complication :
Cerebral Infarction (age < 2 yrs)Cerebral Infarction (age < 2 yrs)
Cerebral Absces (age > 2 yrs)Cerebral Absces (age > 2 yrs)
PolycytemiaPolycytemia
Treatment : Treatment :
Surgery : palliative / total correctionSurgery : palliative / total correction

3838
TRANSPOSITION OF THE GREAT ARTERIES TRANSPOSITION OF THE GREAT ARTERIES (TGA)(TGA)
RVLV
AO
AP
LA
RA

3939
TRANSPOSITION OF THE GREAT ARTERIESTRANSPOSITION OF THE GREAT ARTERIES (TGA) (TGA)
Ventriculoarterial discordance, Ao – RV and PA - Ventriculoarterial discordance, Ao – RV and PA - LVLVCyanotic CHD no.2, M > FCyanotic CHD no.2, M > FHemodynamic :Hemodynamic :
– parallel pulmonary and systemic circulation parallel pulmonary and systemic circulation (cyanosis(cyanosis))
– prolong life : mixing of oxy- and deoxygenated blood prolong life : mixing of oxy- and deoxygenated blood
(ASD, VSD, PDA)(ASD, VSD, PDA)
– deficient O2 supply to the heart, enlargement of the deficient O2 supply to the heart, enlargement of the
heart, heart, heart failureheart failure

4040
X-ray : X-ray : like an egg on its side like an egg on its side bootshaped heart (=TF)bootshaped heart (=TF)
Echo : Echo : double circledouble circle, parallel PA & Ao , parallel PA & Ao Management :Management :– Balloon atrial septostomyBalloon atrial septostomy– Surgery palliative or arterial switch Surgery palliative or arterial switch
procedureprocedure

4141
DEXTROCARDIADEXTROCARDIA
RVLV RA
RVLV
LA
VCI
VCS
AP
AO
RA
LA
AO
AP
Normal heartIsolated Mirror Image Dextrocardia

4242
The heart is located on the right side of the chest & the The heart is located on the right side of the chest & the
apex points to the right. Dextroposition is not a Dx.apex points to the right. Dextroposition is not a Dx.
Anatomy :Anatomy :
1. 1. Visceroatrial relationship :Visceroatrial relationship :
S (solitus), I (inversus)S (solitus), I (inversus) or or A (ambiguus)A (ambiguus)
2. 2. Ventricular LoopVentricular Loop : : D (D-loop), L (L-loop)D (D-loop), L (L-loop) oror
X (uncertain or undeterminate)X (uncertain or undeterminate)
3. 3. Great arteries (conotruncal)Great arteries (conotruncal) : : S (solitus), I (inversus),S (solitus), I (inversus),
D (D-transposition) or L (L-transposition)D (D-transposition) or L (L-transposition) RA
LA
VCI
AP

4343
Isolated mirror image dextrocardia (I,L,I)Isolated mirror image dextrocardia (I,L,I)
Kartagener syndrome: Kartagener syndrome:
Dextrocardia / situs inversusDextrocardia / situs inversus
BronkhiectasisBronkhiectasis
Paranasal sinusitis Paranasal sinusitis

4444
Clin. Manifestations :Clin. Manifestations :
loudest heart sound on the right chestloudest heart sound on the right chest
IMID 50-80% without CHDIMID 50-80% without CHD
X-ray IMID: liver – left, stomach bubble- rightX-ray IMID: liver – left, stomach bubble- right
Echo : dextrocardiaEcho : dextrocardia
Prognosis : depends on the lesionsPrognosis : depends on the lesions
Treatment : overcome the associatedTreatment : overcome the associated lesionslesions