Embed Size (px)
Citation preview

QLIANCEYour Primary Care Medical Home
Erika Bliss, MD, FAAFPFamily Physician, Qliance Medical Group of Washington & Vice President of Medical Care and Quality,Qliance Medical Management Inc. Office: (206) 913-4711Email: [email protected]
The Impact ofDirect Primary CareMedical Homes

Strong Primary Care is Essential toa High-Functioning Health Care System• Primary care is sufficient to address 90% of all
medical conditions.1
• Those receiving care from a primary care physician (rather than a specialist) experience 33% lower annual health care costs and 19% lower mortality2
• An increase of one primary care physician per 10,000 people in a population was associated with a 6% decrease in all cause mortality3
• A 53% reduction in cost for acute illness conditions is achieved when patients’ initial contact is with a primary care provider4
• Medical home model participants saved the Boeing Company 20% in total health care costs compared to propensity matched control group5
1American Academy of Family Physicians, 2004. 2 MDVIP, Hospitalization rates compared to top performing health plans by state, 20052Journal of Family Practice, August 1998, 47(2):103-4. 3Health Affairs, March 20054Journal of Family Practice, July 1996, 43(1):30-33 5Health Affairs, Are Higher-value Care Models Replicable?, Arnold Milstein and Pranany P. Kothari, October 29, 2009

Primary Care in the United States is Broken
1. Primary care asphyxiated by undervaluation and low reimbursements by the insurance-based system
2. Fee-for-service payment model rewards doctors to do more rather than spend time on prevention and management
3. Role of the primary care physician has changed from a care provider to a referral engine for large clinics and hospitals
4. Resource Based Relative Value Scale (RBRVS) rewards doctors to perform complicated and expensive procedures without consideration of outcomes
5. Health care consumer has lost power to control quality, service and access to health care

The Effect on Doctors and Patients
Practice• High overhead• Low reimbursement• Unsustainable business model
Providers• 2,500 to 3,500 patient panels, 25 to 35
appointments per day• Production based compensation incentives• Unsatisfying patient - provider relationship
Patients
• Long appointment lead times, impersonal service, rushed visits
• Unnecessary specialist referrals, tests, procedures
• High co-pays, deductibles, coinsurance

5 5
Should Insurance Cover Primary Care?
• Insurance works well for events that are:
raredifficult to predictextremely expensive
to be avoided
But Primary care is:
frequenthighly predictablereadily affordable to be encouraged
Insurance is a critical element in the health care of Americans – for catastrophic, unpredictable events. It creates significant problems when used as a payment system for primary care.
What would happen if car insurance covered new tires, batteries and oil changes?

Nature of Transaction
Provider
Patient
Insurance Admin
Getting paid for a possible case of pneumonia… Red equals overhead for provider and payer
High FFS Primary Care Admin CostPromotes Visit Volume vs. Time with
Patient

PrimaryCare
SpecialistCare($$$)
Hospital Care($$$)
EmergencyCare($$$)
End ofLife Care
($$$)
An ineffective primary care system pushes patients to expensive downstream care
The result is an increase in overall
health care costs for payers and patients
FFS Primary Care Drives Up Healthcare Costs

8
The Qliance Direct Primary Care Practice Model
1. Take payment directly from patients in a predictable way to cover primary care, reserve insurance for unpredictable, undesirable, expensive healthcare events
2. Provide care based on a monthly membership fee, eliminate fee for service with its counterproductive and misaligned incentives
3. Provide exceptional access, eliminate much of the need for patients to access the rest of the healthcare system

Efficient Direct Primary Care Medical Homes Promote Time with Patients vs. Visit Volume
Provider
Patient
Ins. Admin
KEY
Schedule Appointment
Sees patientDiagnoses Illness
Take X-ray Onsite
Run CBC Onsite
Patient goes to pharmacy
Dispense Rx Patient recovers
Patient has fever and
cough
Pays cash for Rx
Same Day Appointment
Patient has fever and
cough
Flat monthly fee enables smaller panels, better access, and exceptional patient care & service at very affordable prices ($44-84/month)

The Qliance Direct Primary Care Medical Home
Preventive Care
Wellness Care
Chronic Disease Management
Specialist Care Coordination
Urgent Care
A renewed emphasis on patient access, patient care and coordination
Provided in an independent, monthly
fee practice environment
Unrestricted office visits
Same and next day appointments
Unhurried office visits
No co-payments
Extended weekday hours
Weekend office hours
Phone and email access
Flat monthly fee

PrimaryCare
SpecialistCare($$$)
HospitalCare($$$)
EmergencyCare($$$)
End ofLife Care
($$$)
An effective primary care system pulls patients back to high quality, affordableprimary care…
The result is a decrease in overall
health care costs for payers and patients
and considers not only when but also where patients are referred (w/focus on quality and cost)
The DPCMH Effect on System-wide Costs

The Effect on Doctors and Patients
Practice• Low overhead• No reimbursements• Sustainable business model
Provider• 500 to 800 patient panels, 10 to 12
appointments per day• Performance based compensation incentives• Satisfying patient - provider relationship
Patient
• Same and next day appointments, personal service, unhurried visits
• Only necessary specialist referrals, tests, procedures
• No co-pays, deductibles or coinsurance

DPCMH YieldsHigh Patient Satisfaction
• “People, it's a miracle. I pay about $45/month for all my primary care needs (their fee is based on age). They can do lab tests on-site for free, or a small fee if it's unusual, and they even have a pharmacy on-site that provides most basic prescriptions for much, much cheaper than you'll get through your insurance. The doctors are all lovely people, and can take the time to get to know you, and - most importantly - LISTEN. They don't have to funnel patients through their office just to make a buck, so they can actually pay attention to what you're saying, which, believe it or not, is mother-flipping crucial for an accurate diagnosis.”
• “I've had chronic kidney problems since I was 14, and at the time desperately needed a doctor but couldn't afford to go. When I read about Qliance's revolutionary way of approaching medicine I was in complete blissful shock! …the doctors actually listen to the patient and provide feedback and suggestions. Because appointments are 30 minutes to 1 hour long (or longer if needed) the doctors at Qliance can focus on patient education and pay attention to the whole-patient, aiming to solve the problem, not just the immediate symptoms.”
• “The level of care, the amount of compassion, and the concept of having a voice in my healthcare is priceless to me. I've sent friends to Qliance when they had complicated issues that other doctors brushed aside (and they got answers!); I've sent friends who didn't have insurance and otherwise couldn't afford care, and I'd suggest to anyone who wants a truly unique and amazing healthcare experience to go to Qliance.”
• “Qliance is redefining what good healthcare looks like, and honestly, you have to experience it to believe it...”
1 Yelp Online Reviews, 2008-2010
yelp
Net Promoter Score=79%, better than Apple, Google & Amazon

Qliance DPCMHDecreases Non-Primary Care Utilization
Per 1000 members per year
Type of Referral
Qliance # per
year/1000
RegionalBenchmar
k*Difference
**
ER Visits 60 158 -62%
Hospitalizations (in days) 136 184 -26%
Specialist Referrals 909 2000 -55%
Advanced Radiology 414 800 -48%
Surgeries (#/1000/year) 33 124 -73%
Surgeries (# days/1000/year) 83 168 -51%
*Based on regional benchmarks from Ingenix and other sources.**Based on best available internal data, may not capture all non-primary care claims
Source: Qliance Medical Group non-Medicare patients, 2009 (n=2,316)

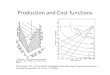
DPCMH Delivers System-wide Savings
$268 billion annual savings($864/person-yr. x 310 million people)
Sources: FFS cost data from seven large self-funded groups. Includes both employer and employee payments. Payer transaction cost estimated based on TPA discussions. Qliance DPMH monthly fee based on average age for self-funded groups. Qliance DPMH non-primary care cost based on self-funded pilot impact 2010 which is consistent with Qliance 2009 Impact Study. Excludes cost of prescriptions.
Per C
apita
Mon
thly
Hea
lth C
are
Cost

Small & Medium-Sized Employers are Catching On
Employers are hit year after year with double-digit premium increases – they are looking for solutions
• Qliance provides care for employees at over 90 Seattle-area companies
• One company is projecting savings of $1million over 5 years by switching to a DPCMH + higher deductible plan + HRA for their employees
• A small pilot with a local union has shown 35% projected savings on non-primary care costs (22% overall) in the first 6 months
• Qliance’s 7 day per week access is reducing need for employees to miss work for medical appointments or use expensive alternatives for care after hours