Embed Size (px)
Citation preview

Slide #1
HIV Entry Inhibitors
Trip Gulick, MD, MPH
Director, Cornell HIV Clinical Trials Unit
Associate Professor of Medicine
Weill Medical College of Cornell University

Slide #2
Antiretroviral Drugs: Challenges and Needs
Challenges• Adherence• Toxicity• Activity• Resistance
Needs• Improve convenience• Improve tolerability• Reduce toxicity• Improve activity
– wild type virus– resistant virus
• Penetrate reservoirs• Exploit new targets

Slide #3
Antiretroviral Drug Approval:1987 - 2003
0
2
4
6
8
10
12
14
16
18
1987 1989 1991 1993 1995 1997 1999 2001 2003
AZTddI
ddCd4T
3TCSQV
RTVIDVNVP
NFVDLV
EFVABC APV
LPV/rTDF ENF

Slide #4
ANTIRETROVIRAL DRUGS 2003
nucleoside RTIs– zidovudine (AZT, ZDV)– didanosine (ddI)– zalcitabine (ddC)– stavudine (d4T)– lamivudine (3TC)– abacavir (ABC)
NNRTIs– nevirapine– delavirdine– efavirenz
nucleotide RTIs– tenofovir (PMPA)
protease inhibitors– saquinavir– ritonavir– indinavir– nelfinavir– amprenavir– lopinavir
entry inhibitors– enfuvirtide (T-20)

Slide #5
Life Cycle of HIV
DS dna COMPLEX
Protease

HIV Entry Mechanism
3c. FusionComplete
1. CD4Attachment
3b. coil-coilinteraction
CXCR4CCR5
HIV
HIV
gp120
3a. Anchorage
CD4
2. Co-receptorinteraction
Cell
HIV
HIV
HIV
gp41
gp41
HIV
Slide #6

Slide #7
HIV Entry Inhibitors
• attachment inhibitors: BMS-806, PRO 542, TNX-355
• chemokine receptor inhibitors:– CXCR4 inhibitors: AMD-11070– CCR5 inhibitors: AK602, PRO 140, SC-351125
(SCH-C), SCH-D, TAK-220, UK-427,857
• fusion inhibitors: enfuvirtide (T-20), T-1249
Slide #8
PRO 542: Overview
• investigational CD4 attachment inhibitor; binds to gp120• tetravalent CD4-IgG2 fusion protein
• IC90 20 µg/mL, achievable in vivo
• T1/2: 3-4 days
• Phase I (N=15): single infusion, dose escalation (0.2, 1, 5, 10 mg/kg), 0.25-0.5 log reductions in VL and viremia demonstrated Jacobson JID 2000;182:326
• Phase I/II pediatrics (PACTG 351) (N=18): 6 children received 10 mg/kg q week X 4, 4 of 6 had >0.7 log VL reductions Shearer JID 2000;182:1774

Slide #9
SC-351125 (SCH C): Overview• Investigational, small molecule CCR5 inhibitor
• HIV IC90 ~20nM (CCR5 virus)
• In vitro activity against R5, X4/R5 viral strains; resistance did not lead to co-receptor switch (mice)
• Orally bioavailable; PK supports bid dosing; not CYP450 metabolized
• Phase I/healthy volunteers/600 mg single dose: QTc prolongation >50ms (n=1)
• Phase I/HIV infected (N=12) X 10 days: 25 mg bid (-0.5 log ) and 50 mg bid (-1.0 log )
Baroudy, Barcelona AIDS Conf 2002, abstract #MoOrA138

Slide #10
Schering C: Phase IB
Reynes, 9th CROI, 2002, abst. #1

Slide #11
Inhibition of Fusion
HIV-1
gp 120gp41
gp41
gp 120 ENFENF
ENFENFCD4CD4CCR-5CCR-5

Slide #12
Enfuvirtide (T-20) -- Overview• FDA-approved fusion inhibitor; 36 AA peptide
• HIV IC50 1.7 ng/ml
• Dose: 90 mg sq bid
• side effects: – injection site rxn (common); – hypersensitivity reactions (uncommon); – eosinophilia (10% >700; 2% >1400); – ?increased risk of pneumonia on phase III studies
• resistance: changes in gp41 (positions 36-43)
Slide #13
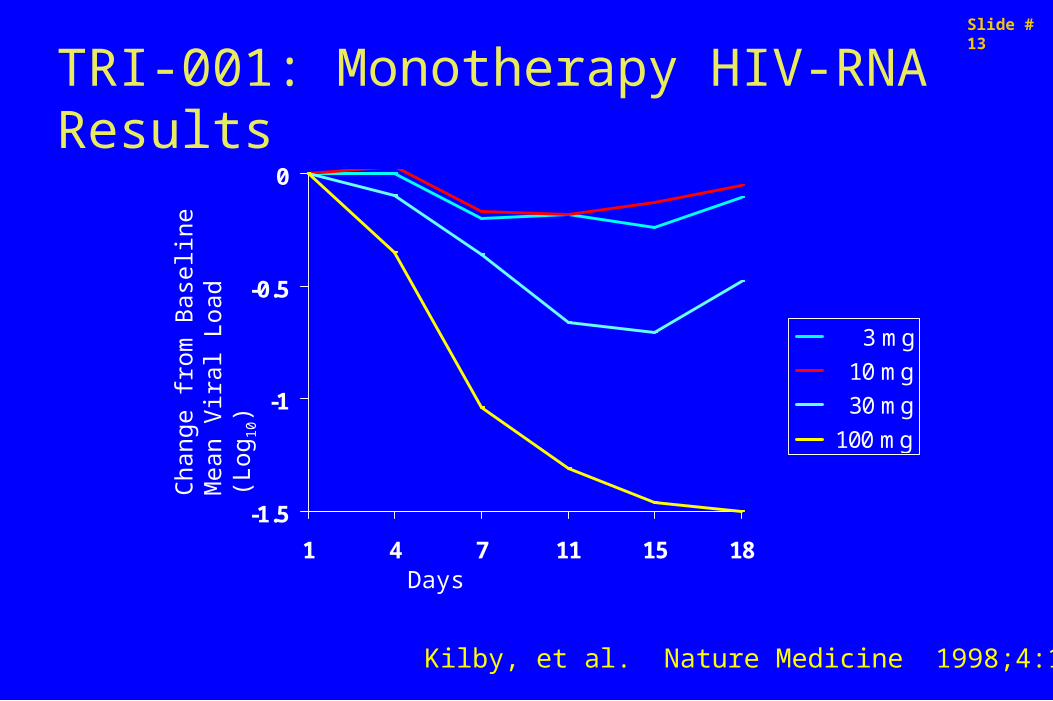
TRI-001: Monotherapy HIV-RNA Results
-1.5
-1
-0.5
0
1 4 7 11 15 18
3 mg
10 mg
30 mg
100 mg
Days
Cha
nge
from
Bas
elin
eM
ean
Vira
l Loa
d (L
og10
)
Kilby, et al. Nature Medicine 1998;4:1302-7.

Slide #14TRI-003: HIV RNA Mean Change From Baseline: Intent-to-treat
-1.5
-1.2
-0.9
-0.6
-0.3
0
BASELINE DAY 7 DAY 14 DAY 21 DAY 28
12.5 mg/day CSI 25 mg/day CSI 50 mg/day CSI100 mg/day CSI 50 mg BID SQI 100 mg BID SQI
Ch a
nge
Fro
m B
asel
i ne
Pl a
sma
HIV
RN
A L
og10
(C
opie
s/m
L)
Kilby,AIDS Res Hum Retroviruses 2002;18:685-93
Slide #15
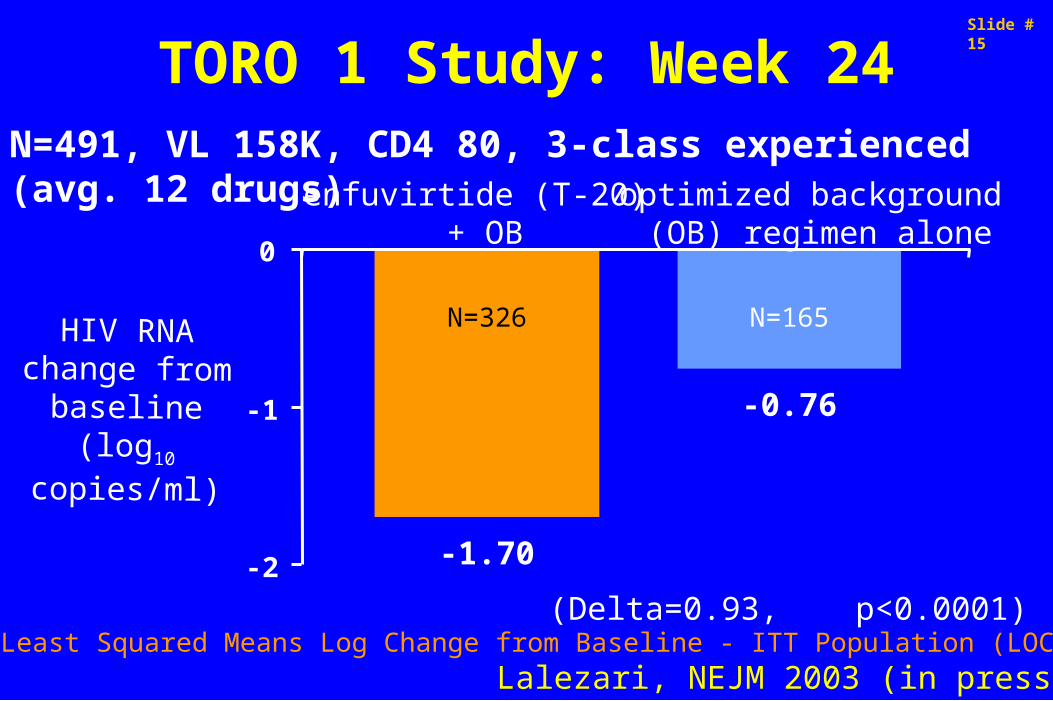
TORO 1 Study: Week 24
-1.70
-0.76
-2
-1
0
(Delta=0.93, p<0.0001)Least Squared Means Log Change from Baseline - ITT Population (LOCF)
optimized background (OB) regimen alone
enfuvirtide (T-20) + OB
N=165N=326HIV RNA change from baseline
(log10 copies/ml)
Lalezari, NEJM 2003 (in press)
N=491, VL 158K, CD4 80, 3-class experienced (avg. 12 drugs)

Slide #16
TORO 2: Week 24
-1.43
-0.65
-2
-1
0
(Delta=0.78, p<0.0001)Least Squared Means Log Change from Baseline - ITT Population (LOCF)
optimized background (OB) regimen alone
enfuvirtide (T-20) + OB
N=169N=335HIV RNA change from baseline(log10 copies/ml)
Clotet B, XIV AIDS Conf., abstract LBOr19B

Slide #17
Anti-HIV Fusion Peptides
HR1 cc HR2FPNH2 COOHtm
T-20T-1249
gp41 molecule
Slide #18
T-1249: Overview• investigational fusion inhibitor
• hybrid peptide of HIV-1, HIV-2, SIV; 39 amino acids
• PK supports qd dosing, parenteral
• 2-100 x more active in vitro than T-20
• active against many T-20- resistant-HIV variants (in vitro and in vivo)
• Resistance: gp41 substitutions (positions 35-71 of HR1)
• Stage of development: phase I/II completed; phase II planned

-2
-1.5
-1
-0.5
0
0 7 14
Study Day
Med
ian
Cha
nge
from
Bas
elin
e (H
IV R
NA
log1
0)
6.25 mg QD
6.25 mg BID
12.5 mg QD
12.5 mg BID
25 mg QD
25 mg BID
50 mg QD
100 mg QD
150 mg QD
200 mg QD
T1249-101: Virologic Response
N=115, VL 186K, CD4 57, 99% with exposure to a mean of 10 agents
Gulick, ICAAC 2002, abst. #H-1075
Slide #19

Slide #20Investigational Drugs 2002: Other Classes
• GAG processing inhibitors• budding inhibitors• DC-SIGN inhibitors• defensins• si RNAs• regulatory protein (e.g., NEF, VIF, TAT) inhibitors• uncoating inhibitors• RNAase H inhibitors• zinc finger (DNA complex) inhibitors• capsid protein polymerization inhibitors• assembly inhibitors

Slide #21
HIV Entry Inhibitors: Conclusions• Newer antiretroviral drugs are needed to improve
activity against resistant virus and exploit new targets.
• HIV entry inhibitors are promising agents with a new mechanism of action and demonstrated antiretroviral activity.
• Further basic and clinical research is needed.

Slide #22
Acknowledgments
• Joe Eron / UNC • Diego Miralles and Alex
Dusek / Trimeris• Bill Olsen / Progenics• Greg Reyes and Bahige
Baroudy / Schering-Plough

























![Presentation1 (gulick)[2]](https://img.pdfslide.us/doc/110x75/54ba3b9d4a7959d26f8b45b0/presentation1-gulick2.jpg)


