Embed Size (px)
Citation preview

Sleep Medicine for the Non-Sleep Specialists
Q. Afifa Shamim-Uzzaman, MDChandra Gera, MD
Christopher Morgan, MDMASM Fall Conference
10/13/17

Agenda
6:30 – 6:35pm - Welcome
6:35 – 7:15pm - Sleep Disordered Breathing (SDB)
6:35 – 6:45 - Identifying the patient with SDB (Afifa Uzzaman)
6:45 – 7:00 - Testing for sleep disordered breathing (Chandra Gera)
7:00 – 7:15 – Treating the patient with SDB (Chris Morgan)
7:15 – 7:20pm: Break
7:20 – 7:40pm: Restless Legs Syndrome (Chris Morgan)
7:40 – 8:10pm: Insomnia
7:40 – 7:50pm - Approach to the Patient with Insomnia (Afifa Uzzaman)
7:50 – 8:10pm – Treating Insomnia (Chandra Gera)
8:10 – 8:30pm: Questions

OBJECTIVES
At the end of the session, participants should be able to:
• Identify patients needing to undergo testing for sleep
disordered breathing and select the appropriate sleep test
• Interpret the results of a sleep study report and order
appropriate therapy
• Identify Restless Legs Syndrome as a cause of insomnia
• Plan initial management of insomnia in the primary care
setting
• Determine when to send the patient to a sleep specialist vs.
treat in primary care

SLEEP DISORDERED BREATHING
Identifying the Patient with SDB - Afifa Shamim-Uzzaman, MD
Testing for Sleep Apnea - Chandra Gera, MD
Treating the Patient with Sleep Apnea - Chris Morgan, MD

Case 1
• 65 year old obese Caucasian male with a history of HTN, DM,
and CAD presents with fatigue. He sleeps 8 hours a night and
still wakes up in the morning feeling as tired as if he ran a
marathon. He is a truck driver, hauling loads between Detroit
and Toledo. He denies snoring or daytime sleepiness—he
does not get drowsy behind the wheel.
• His wife reports that he snores and makes some gurgling and
choking sounds that wake her up. She sometimes stays awake
watching him sleep and she often has to nudge him to start
breathing again. Although he reports that he has no problems
staying awake to complete his tasks, his wife mentions that he
falls asleep every time he watches TV.

OSA➢A disorder of sleep
➢ Recurrent episodes of narrowing or collapse of pharyngeal airway despite ongoing efforts to breathe.
➢ Leads to
➢Acute derangements in blood gas
➢ Surges of sympathetic activation
➢ Periodic arousal from sleep (fragmented sleep)

Pathophysiology of OSA
No airway obstructionObstruction at palate,
tongue, epiglottis
O2 and CO2 flow in and out of the airways easily
Neither O2 can enter below the obstruction nor CO2 escape.
http://en.wikipedia.org/wiki/Sleep_apnea

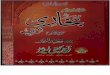
Midsagittal magnetic resonance image (MRI) demonstrating the upper airway regions: retropalatal (RP)—from the level of the hard palate to the caudal margin of the soft palate; and retroglossal (RG)—from the caudal margin of the soft palate to the base of the epiglottis. Soft palate, tongue, airway, mandible, and subcutaneous fat are denoted with arrows. Fat is bright (white) on an MRI.
Schwab RJ, et al. Identification of Upper Airway Anatomic Risk Factors for Obstructive Sleep Apnea with Volumetric Magnetic Resonance Imaging. Am J Resp Crit Care Med. 2003; 168(5): 522-530.

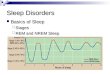
2000
Obesity Trends* Among U.S. AdultsBRFSS, 1990, 2000, 2010
(*BMI ≥30, or about 30 lbs. overweight for 5’4” person)
20101990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
www.cdc.gov
The incidence of OSA in the US is increasing with
the average BMI of the population

RISK FACTORS for OSA
• Obesity
• Age
• Sex
• Race
• Craniofacial anatomy
• Smoking
• Alcohol consumption

Risk factor: OBESITY
• Alters upper airway mechanics during sleepIncreased parapharyngeal fat deposition with
subsequent:
→ smaller upper airway
→ increased collapsibility of the pharyngeal airway
neck circumference: > 17” males
> 16” females

Risk Factor: AGE%
wit
h A
HI
>5
Adapted from Young T, et al. N Engl J Med 1993; 328.

Risk Factor: SMOKING
Adjusted Odds Ratio for Sleep Apnea (AHI > 15) in Former & Current Smokers vs Nonsmokers
Adapted from Wetter DW, et al. Arch Intern Med 1994:154
Former CurrentSmokers Smokers
(Ad
just
ed
fo
r a
ge
, ra
ce,
sex
, B
MI)
Od
ds
Ra
tio

Diagnosing OSA
Symptoms
+
Clinical features
+
PSG

Common Nocturnal Symptoms of OSA

Symptoms of OSA: Nighttime

Common Daytime Symptoms of OSA

Symptoms of OSA: Daytime

Clinical Signs of OSA

Physical Characteristics of OSA
Obesity & Large neck Retrognathia & Micrognathia



Clinical Signs of OSA

Mallampati SR, et al. A clinical sign to predict difficult intubation: a prospective study. Can Anaesth Soc J. 1985; 32(4): 429-34.

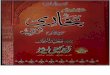
Clinical Consequences of OSA

Treated with CPAP
No CPAP
• Long-term risk for cardiovascular events according to the presence of OSA and treatment with CPAP
• 12 year follow-up
• All Men
• N=1651
• Those who were treated with CPAP had the same risk as controls
Marin et al. Lancet 2005; 365:1046
CPAP Reduces CV risk to that of Controls

Who to test?Screening for Sleep Apnea

Validated Screening Tools
• Berlin questionnaire
• Epworth Sleepiness Scale
• STOP
• STOP-BANG (greatest sensitivity, but lower specificity than ESS)

STOP-BANG QUESTIONNAIRE
Question Yes No
Snoring? (heroic)
Tired, Fatigued, or Sleepy?
Observed Apneas or choking/gasping?
High Blood Pressure?
BMI > 35 kg/m2
Age older than 50?
Neck size large? (measured around Adams apple)
Males – 17 inches (43 cm)Females – 16 inches (41 cm)`
Gender male?
> 3 = 90% sensitivity in sleep clinic population
In the sleep clinic population, the sensitivity was 90%, 94% and 96% to detect any OSA (AHI ≥ 5), moderate-to-severe OSA (AHI ≥15), and severe OSA (AHI ≥30) respectively.

The higher the STOP-BANG Score, the higher the odds of having severe OSA

Case 1
• 65 year old obese Caucasian male with a history of HTN, DM,
and CAD presents with fatigue. He sleeps 8 hours a night and
still wakes up in the morning feeling as tired as if he ran a
marathon. He is a truck driver, hauling loads between Detroit
and Toledo. He denies snoring or daytime sleepiness—he
does not get drowsy behind the wheel.
• His wife reports that he snores and makes some gurgling and
choking sounds that wake her up. She sometimes stays awake
watching him sleep and she often has to nudge him to start
breathing again. Although he reports that he has no problems
staying awake to complete his tasks, his wife mentions that he
falls asleep every time he watches TV.

Case 1
• 65 year old obese Caucasian male with a history of HTN, DM,
and CAD presents with fatigue. He sleeps 8 hours a night and
still wakes up in the morning feeling as tired as if he ran a
marathon. He is a truck driver, hauling loads between Detroit
and Toledo. He denies snoring or daytime sleepiness—he
does not get drowsy behind the wheel.
• His wife reports that he snores and makes some gurgling and
choking sounds that wake her up. She sometimes stays awake
watching him sleep and she often has to nudge him to start
breathing again. Although he reports that he has no problems
staying awake to complete his tasks, his wife mentions that he
falls asleep every time he watches TV.
STOP BANG SCORE = 8

Sleep apnea can only by diagnosed by a
sleep study

Testing for sleep disordered breathing
Based on clinical practice guidelines by the American Academy of Sleep
Medicine, 2017Dr. C. M. Gera, MD, FCCP, ABIM (Sleep), D-ABSM
(Sleep)Medical Director at:
Mid-West Center for Sleep Disorders and Hayes Green Beach Hospital Sleep Station
Associate Clinical ProfessorCollege of Human Medicine, Michigan State University

Testing for SLEEP Disordered Breathing
Parameters Monitored
HSAT In-Lab NPSG
EEG (Sleep) No Yes
EKG No Yes
Pulse Oximetry Yes Yes
Heart Rate Yes Yes
Airflow Yes Yes
Respiratory Effort Yes Yes
Muscle Movements
No Yes

Home Sleep Apnea Test (HSAT)
oApnea Hypopnea Index (AHI) –
o Is defined as number of apneas plus
hypopneas per hour.

Home Sleep Apnea Test (HSAT)
➢Apnea Hypopnea Index Less than PSG AHI
• Not sensitive enough
• Can not be used to rule out mild sleep apnea
➢Apnea Hypopnea Index more than PSG AHI
• Not specific enough
• Can not be used to rule in mild sleep apnea

Home Sleep Apnea Test (HSAT)
➢Only recommended to test for Sleep Apnea
➢Recommended for patients with high pre-test probability for moderate to severe sleep apnea.
➢High pretest probability is determined by history, examination, questionnaires and prediction scores

Home Sleep Apnea Test
➢ Which of the following is an appropriate use of a home sleep apnea test?
A. Diagnose central sleep apnea
B. Evaluate degree of hypoxemia
C. Rule out obstructive sleep apnea
D. Evaluate degree of hypoventilation

Home Sleep Apnea Test
➢ Which of the following is an appropriate use of a home sleep apnea test?
A. Diagnose central sleep apnea
B. Evaluate degree of hypoxemia
C. Rule out obstructive sleep apnea
D. Evaluate degree of hypoventilation

Home Sleep Apnea Test
In-Lab Sleep Study➢If a single HSAT is
• Negative
• Inconclusive
• Technically inadequate
➢Central Apneas

Home Sleep Apnea Test Contraindicated
➢If sleep study is being done for any sleep disorder other than sleep apnea
➢If they have any of the following comorbid conditions
• CHF
• COPD
• Obesity Hypoventilation
• Neuromuscular Disorders
• Chronic opioid use
• Stroke
• ? Truck Driver
• Physical impairment that will not allow the patient to use the equipment at home

How to Interpret Sleep Study
Reports

H
S
A
T
I
N
T
E
R
P
R
A
T
A
T
I
O
N

H
S
A
T
I
N
T
E
R
P
R
A
T
A
T
I
O
N

H
S
A
T
I
N
T
E
R
P
R
A
T
A
T
I
O
N

N
P
S
G
I
N
T
E
R
P
R
A
T
A
T
I
O
N

N
P
S
G
I
N
T
E
R
P
R
A
T
A
T
I
O
N

N
P
S
G
I
N
T
E
R
P
R
A
T
A
T
I
O
N

C
P
A
P
I
N
T
E
R
P
R
A
T
A
T
I
O
N

C
P
A
P
I
N
T
E
R
P
R
A
T
A
T
I
O
N

C
P
A
P
I
N
T
E
R
P
R
A
T
A
T
I
O
N

Case 1
• 65 year old obese Caucasian male with a history of HTN, DM,
and CAD presents with fatigue. He sleeps 8 hours a night and
still wakes up in the morning feeling as tired as if he ran a
marathon. He is a truck driver, hauling loads between Detroit
and Toledo. He denies snoring or daytime sleepiness—he
does not get drowsy behind the wheel.
• His wife reports that he snores and makes some gurgling and
choking sounds that wake her up. She sometimes stays awake
watching him sleep and she often has to nudge him to start
breathing again. Although he reports that he has no problems
staying awake to complete his tasks, his wife mentions that he
falls asleep every time he watches TV.
HSAT

Treating patients with sleep disordered breathing (SDB)
Christopher Morgan, MD
Medical Director, Mercy Health St. Mary’s Sleep Center
Program Director, GRMEP MHSM Neurology Residency
Grand Rapids, MI
MASM Fall 2017 Meeting
October 14, 2017

Treatment: Overview
• PAP Therapy
• Oral Appliances
• Surgical Treatments• Posterior Airway Surgery – Eg. UP3• Bimaxillary Advancement • Hypoglossal Nerve Stimulation

Treatment: Continuous Positive Airway Pressure (CPAP)
•Improves HTN
•Prevents complications of sleep apnea
•Improves quality of sleep
•Auto-CPAP•Variable pressure range (5-20)
•Algorithms increase pressure for snoring, flow limitation, apneas
•Not always accurate
•May worsen central sleep apnea
•Some patients have trouble tolerating pressure variability.

What is CPAP?

Treatment: CPAP

PAP Masks

PAP Machines
•Very quiet
•Easy to use
•Lots of data
•Many Different
Machines (e.g. Bilevel PAP)
609/26/2017

Clinical Sleep Medicine-Sleep Apnea
•CPAP is now more portable than ever before. •Ideal for travel
•Not paid by insurance.
•AirMini CPAP
•Z1 CPAP

Clinical Sleep Medicine-Sleep Apnea
•Airing •Crowdfunding and Facebook popularity
•Waiting FDA approval
•Not on the market
*Supposed to work as a Micro CPAP device
•Single use
•Lasts 8 hours

It’s Not Just CPAP Anymore
•Bilevel PAP (BiPAP, VPAP)•2 pressures, Inspiratory and Expiratory•Used to provide pressure support for patients with hypoventilation (morbid obesity, neuromuscular patients, COPD)•Easier to breath – used for patients with CPAP intolerance
•Servoventilation (ASV, AdaptSV)•Used for Central Sleep Apnea of various types•Varying pressure support helps to stabilize breathing
•AVAPS/iVAPS or Trilogy non-invasive ventilator•Volume support for severe hypoventilation

Central Sleep Apnea
•Higher risk in CHF, Atrial Fibrillation, opioid use
•Treatment Emergent Central Sleep Apnea (Complex sleep apnea)
•Central apnea emerges when treated with CPAP
•Treatments•ASV
•Hypnotics •Positional therapy
•Nocturnal oxygen
•? Diamox
•New study SERVE-HF – higher risk of CV mortality in patients with severe CHF on ASV (EF <30-45%)
SLEEP, Vol. 35, No. 1, 2012

Cheyne-Stokes, 5 minute slide

Oral Appliance
•May be effective for mild to moderate OSA as first line or CPAP alternative
•Can consider in severe OSA if CPAP intolerance
•More effective in positional sleep apnea
•Relative Contraindications •TMJ pain•Bruxism•Edentulous•Seizures•Risk of aspiration•Central Sleep Apnea - absolute

Oral Appliance

Tongue Retaining DevicesNon-Adjustable Mandibular
Repositioning Devices
Adjustable Mandibular
Repositioning Appliances Combined Mandibular Repositioners and
CPAP Attachment
Oral device therapy for sleep apnea

Anti-snore devices
•Not evaluated by FDA
•Marketed for snoring only
•Target mandibular advancement
or nasal obstruction
•Temporary devices, less durable, cheap
Snore Rx

Surgical Treatments – often combination
•Bariatric Surgery
•Adenotonsillectomy – mainly in children
•Uvulopalatopharyngoplasty (UPPP/UP3)
•Tongue advancement/reduction
•Nasal surgery
•Hyoid suspension
•BiMaxillary advancement• higher success rate, more invasive
Even combination surgery often only 2/3 success rate and may not cure OSA

New Stuff
•Oral Pressure Therapy (Winx)
•Nasal EPAP – Provent
•Hypoglossal Nerve Stimulation (Inspire)

INSPIRE – Hypoglossal Nerve Stimulation
•Indications:•Age 22 or older
•Moderate to severe OSA (AHI 15-65)
•BMI less than 32 (can refer if BMI <35)
•Unable to use CPAP/BiPAP
•Contraindications•CSA greater than 25% of their sleep apnea
•Concentric collapse of their soft palate
•Neurological condition affecting the upper airway
•Inability to use the device
•Overall is a long process, insurance auth can take a while, a couple months before device is adjusted well
•STAR trial – AHI <20 in 66% of participants
Woodson et. al, Otolaryngology-Head and Neck Surgery, Vol 151, Issue 5, pp. 880 – 887
Strollo, et al, N Engl J Med 2014; 370:139-149

Clinical Sleep Medicine-Sleep Apnea

OSA Long Term Follow Up for PCPs
•Check for recurrent symptoms, such as snoring through mask, return of daytime sleepiness
•Make sure patient is replacing equipment regularly•Mask cushion every few months•Mask, hose, and filters every 6-12 months
•No need to repeat study if stable
•Continued follow up every 1-2 years with sleep specialist for compliance and response

When Do I Refer?
•Suspected uncomplicated OSA and not comfortable prescribing CPAP therapy
•Complicated sleep apnea – many comorbidities (COPD, CHF, A-fib), morbid obesity (may have obesity-hypoventilation)
•High risk for central sleep apnea – significant CHF, A-fib, opioids

PCP treatment of OSA – Case 2
•45 year old complains of snoring (actually his wife complains)
•Witnessed apneas, early morning awakenings with light sleep, some daytime dozing with ESS 11
•PMHx HTN, DM, depression
•Social history: drinks caffeine until 7pm every night, alcohol 2 per week, no smoking
•Medications: 50mg Benadryl every night, Wellbutrin 100mg for depression he takes at bedtime. Metformin. Amlodipine.
•Sleep schedule 11pm to 7am
•Next Steps??•Stop caffeine in evening
•Move wellbutrin to the morning
•Home Sleep Apnea Test shows moderate OSA with AHI 23, and O2 min 79%

Case 2 Cont.
•Next Steps??•Order Auto-CPAP therapy from 5-15cm of water
•Patient needs to choose DME company which can help setup and acclimate mask – typically favor nasal type mask initially
•Obtain compliance download in 2-4 weeks.
•If patient compliant and AHI reasonable ( <5 ) without high leak, then set CPAP to 95% pressure
•Follow up clinic appointment in 31-90 days (required by most insurances)
•Discuss mask fit, CPAP pressure tolerance, dry mouth, sleep quality, daytime sleepiness
•Evaluate if can discontinue OTC sleep aids once sleep apnea treated

RESTLESS LEGS SYNDROME
Christopher Morgan, MD
Medical Director, Mercy Health St. Mary’s Sleep Center
Program Director, GRMEP MHSM Neurology Residency
Grand Rapids, MI

Case 3
•34-year-old nurse who was comes to see you for insomnia, non-restorative sleep, and a feeling of malaise throughout the day.
•Patient History and Examination: sleep problems began during late adolescence and started with difficulty falling asleep. She also developed frequent awakenings throughout the night. As a child, she suffered from “growing pains.” The sleep disturbance had initially been ascribed to stress (especially during nursing school) and to her shiftwork. She has tried melatonin, which has not helped. She tried tylenol PM, which made her feel drowsy, but for some reason still had difficulty falling asleep. She was prescribed temazepam and is current taking 30mg, which has some effectiveness, but still has difficulty falling asleep. Some nights she falls asleep easier than others. She typically goes to bed at 11pm and can take 2-3 hours to fall asleep on her bad nights, but a few days a week it only takes 20-30 minutes. She sometimes gets up to walk around when she cannot fall asleep. She wakes up 3-5 times per night.
•Social History: Darlene drinks 5 cups of strong coffee throughout the day to stay awake. She feels too exhausted to exercise. She has been happily married for 10 years.
•Family History: mother had similar problem of falling asleep throughout her life and she would often see her mother walking the house at night.

Restless Legs Syndrome (RLS)
•Seen in 10-15% of the population
•Only 2.5% affect quality of life
•Worse in pregnancy, iron deficiency, neuropathy, ESRD
•80% have Periodic Limb Movements during sleep (PLMS)
•Pathophysiology – central/brain iron deficiency•Leads to increase dopamine, downregulation of D2 receptors
80


RLS Diagnostic Criteria - URGES
•Urge to move the limbs (legs/arms/other parts) with or without dysesthesias
•Possible descriptive words: crawling, creeping, bugs, worms, electricity, energy, burning, pain, ache, or nervous
•Rest-induced (or inactivity), sitting, lying (esp. in bed), planes, cars•Onset or exacerbation of motor/sensory symptoms with both decreased motor activity and mental activation
•Gyration or movement improves/relieves urge (Gets better)•eg. shaking, walking, stretching, rubbing, vibration•High mental activation such as computer games may also reduce the urge
•Evening or night worsening (esp. bedtime). Minimal Sx in morning•Circadian pattern
•Sole explanation for urge to move, not explained by another illness

Supportive features of RLS
When it may be difficult to obtain accurate clinical history•Positive family history
•May be as much as 50-80% genetic, often autosomal dominant in many pedigrees•Those with family history have earlier age of onset (typically in 30s or earlier)
•Positive response to dopaminergic therapy, such as brief dopamine agonist trial•Presence of periodic limb movements of on polysomnography (both sleep and wakefulness)
Associated features•Clinical course is generally chronic and progressive•Sleep disturbance, particularly in first half of the night•Normal neurologic examination in primary RLS, unless a comorbid condition exists

84 9/26/2017

Case 3 (cont.)
•Further questioning about her insomnia revealed she had an urgency to move her legs when she was trying to fall asleep in order to alleviate discomfort. Moving her legs provides partial and temporary relief of the discomfort. The sensations are worse when she is at rest (i.e., lying or sitting down), and later in the day; they occur mainly during the evening and during the nighttime. When she takes a nap during the day, she is rarely bothered by these sensations.

Diagnostic Workup
•Clinical diagnosis, neuro exam to r/o secondary diagnosis
•Check Iron levels•Ferritin <75 – iron supplementation
•Ferritin <15 – Iron repletion, other workup
•Consider PSG if symptoms of EDS, apnea or severe PLMS
•Consider EMG if symptoms or neuropathy or abnormal neuro exam
•Consider MRI brain if suspicion for neurological disease
•Other labs tests for secondary causes•B12, folate, glucose tolerance test/Hgb A1C, BUN/Cr

Case 3 (cont.)
•Evaluation and Diagnosis: A polysomnographic exam documented the existence of periodic limb movements during sleep (PLMS) and ruled out other sleep disorders, including Obstructive Sleep Apnea Syndrome (OSAS). In approximately 70% of Darlene’s PLMS, she experienced short arousals from sleep. On the basis of her history, Darlene was diagnosed with Restless Legs Syndrome.

RLS Treatment – non-pharmacologic
•Mentally Alerting Acitvities – reading, card games, etc.
•Eliminate/decrease meds that make it worse
•Yoga – has some evidence to improve RLS
•Good Sleep hygiene, including adequate sleep
•Consider slight delayed sleep schedule
•Moderate exercise during day and stretching in evening
•Relaxis Pad – timed vibratory counterstimulation – FDA approved
•Restiffic pressure pad on feet
•Iron supplementation

90 9/26/2017

Drugs That Worsen RLS
•Dopamine Antagonists – Reglan, Compazine
•Neuroleptics
•Antihistamines – benadryl, hydroxyzine, meclizine
•Anti-depressants especially SSRI, SNRI (Effexor), Cymbalta•Mirtazapine, lexapro , Prozac worst for RLS
•Best agent may be Wellbutrin (Buproprion) – works well!!
•For anxiety, try Buspirone
•Trazodone also OK for depression and insomnia
•Caffeine, Alcohol, Nicotine (alcohol most)
•Decrease dose or stop medication if able
•If not able, at least move to morning schedule

Tips for Iron Replacement
•Need to check FERRITIN and TIBC/Iron sat as well as iron•Replace Iron if Ferritin <75 or if ferritin borderline, but iron saturation is <20%
•Ferritin need to check FASTING and no high iron meal the night before. Also is acute phase reactant!
•Vitamin C helps absorption of Non-heme iron
•Calcium, bran, teas, antacids, soy protein, can block absorption
•Better absorption on an empty stomach
•Enteric coated/slow release not recommended
•Complications: constipation, iron overload•Take with Miralax and stool softener if constipation
•If intolerant, can try other iron formulations

Case 3 (cont.)
•Treatment: Sleep health measures were started: A gradual but almost total decrease in caffeine intake was requested, along with a leg exercise regime to be completed almost daily. The bedroom clock was removed. These measures did little to decrease Darlene’s RLS symptoms, however.
•her serum ferritin level was measured and found to be 24 ng/mL. Upon inquiry, no organic reason for her iron deficiency was found except for her frequent blood donations. She was advised to stop the donations and to take iron supplements. When her ferritin levels rose above 75 ng/mL, Darlene’s RLS symptoms improved
Case from the National Sleep Foundation: The Sleep Disorders, Chapter 7

Pharmacological Therapy With a Single Agent Can Be Tried By PCP If Comfortable
•Key is TIMING! – want to give 30-60 minutes before patient experiences symptoms
• Alpha-2 Ligands are now considered first line by many experts!
•Gabapentin – 100-1200mg in afternoon/evening
•Lyrica – 50-300mg/day as effective as Mirapex in recent study
•Helpful in concurrent pain syndromes as well
• Dopamine agonist is still first line•Mirapex (pramipexole) – start 0.125mg, titrated up to 0.75mg max
•Requip (ropinirole) – start at 0.25mg, up to 2-3mg max
•Titrate up slowly and split doses into 2 evening/bedtime doses
•Opioids: Tramadol – 50-100mg•Methadone 2.5 - 10mg great for RLS in refractory cases
•Oxycodone 2.5 – 15mg
•Risk of dependence almost non-existent in RLS treatment!!
•Klonopin – 0.5mg – less effective, must not have OSA
•Hypnotics – can try Ambien

Dopamine Agonist Side Effects
•Nausea (19%)
•Somnolence (10%)•This is more prominent at higher doses, such as those used in Parkinson's disease
•Epworth Sleepiness often not increased despite somnolence
•Dizziness
•Decrease Blood pressure
•Impulse Control Disorders •Excessive gambling
•Increased sexual desire
•Shopping
•Augmentation
•Punding: •characterized by excessive handling of the same object repeatedly, such as manipulation of technical equipment such as radios or engines, repetitive cleaning of a room or object, and excessive attention to personal hygiene.

Beware of Augmentation
•Further down-regulation of dopamine receptors due to higher doses of DA
•If symptoms worse after being on higher doses of short acting dopamine agonist and doses are escalating – likely augmentation
•Symptoms moving up the body – into arms
•Symptoms earlier in the day – at least 2 hours•Quicker onset of symptoms•Duration of relief from symptoms is shorter•Intensity greater (or more PLMS)
•Need to wean off dopamine agonist and start alternative agent if severe –alpha-2 ligand
•Splitting up dose of DA or switching to long acting can help

Augmentation

98 9/26/2017

Periodic Limb Movements
•Not the same as RLS, although about 80% of people with RLS have PLMS
•Diagnosed by sleep study - Need at least 4 consecutive leg jerks separated by 5-90 seconds
•Debatable clinical significance – do they contribute to arousals?
•Periodic Limb Movement Disorder (PLMD)•Can only be diagnosed in the absence of RLS
•Must have daytime symptoms + PLMS (>15/hr) without other sleep disorders
•Tx with similar meds as RLS•Mirapex/Requip seems to be most potent, but klonopin may also work well, some effect with gabapentin/lyrica

When Do I Refer?
• RLS not responsive to iron therapy or first line agents, or having to titrate up medication to higher doses
• Any signs of Augmentation

101 9/26/2017

Case 4
•65 y/o female with RLS symptoms since she was 16 y/o
•Has progressively worsened over her life
•Diagnosed with OSA in 2009 and prescribed CPAP 11cm, but could not tolerate therapy due to mask and pressure issues.
•Currently taking Mirapex 1.5mg TID (morning, afternoon, bedtime).
•Symptoms are earlier into the day, close to noon, sometimes gets symptoms in her arms
•Has some compulsive behaviors as well such as excessive shopping, buying things online when she does not have the money
•She had trialed multiple medications in the past including Klonopin, Sinemet, gabapentin, tramadol, Requip – patient does not remember side effects or why she stopped these.
•At one point she was on Klonopin, Sinemet, and Mirapex
•She had iron infusions in 2009 for very low ferritin of 7.

Case 4 (cont)
•PMHx: HTN, GERD, Migraines, Depression, COPD
•Soc Hx: no caffeine or alcohol, former smoker
•Fam Hx: RLS in mother
•Meds: Lexapro 20mg, Mirapex, Nuvigil 250mg, inhalers, triamterene/HCTZ
What would you do?

Case 4 f/u
•Did CPAP titration, started CPAP of 12cm, but not compliant still. Did BiPAP titration, but still not compliant, but pt had hypoxia and given O2
•PSG showed frequent leg movements when awake or in transitional sleep, but not significant PLMS
•Told her to STOP morning dose of mirapex.
•Make sure to take lexapro in morning and take lowest effective dose
•Later, we weaned slowly off mirapex and then onto lyrica 300mg.
•Patient UNABLE to stop mirapex, did not have willpower, so continue on 1-3mg even with lyrica, felt lyrica did not help much
•What is another option for her RLS? Any other ideas?

Case 4 f/u
•Started patient on oxycodone 2.5mg at bedtime and taper mirapex
•Sleeping better with oxycodone, but still taking mirapex afternoon dose at 1.5mg.
•Recommended add extra dose of oxycodone 2.5mg in afternoon and d/c mirapex
•Still not complaint on BiPAP
•Had long appointment with her and finally agreed to stop Mirapex. She weaned off in 2 weeks
•Patient had worst sleep of her life and was miserable for 2 weeks following being off mirapex. Called me every day.
•At f/u, her RLS symptoms have significantly improved and are still present, but much milder. We are starting gabapentin at low doses to see if we get adequate response. Could not afford lyrica
•I reordered her BiPAP to get her on therapy now that RLS is better

References
•Review of Sleep Medicine – Alon Avidan 2012
•Kryger Sleep Medicine Review: A problem based approach: Kryger 2011
•Fundamentals of Sleep Medicine: Richard Berry 2012
•CONTINUUM. 19(1, Sleep Disorders): February 2013
•Sleep Medicine Clinics – issue 10, entire issue
•Neurotherapeutics (2012) 9:776–790
•Sleep Medicine 17 (2016) 99–105
•Sleep Medicine 8 (2007) 520–530
•Sleep Medicine 5 (2004) 279–283
•Journal of Family Practice. 61.5 (May 2012): p296.

INSOMNIA
Approach to the Patient with Insomnia - Q. Afifa Shamim-Uzzaman, MD
Treating the Patient with Insomnia - Chandra Gera, MD

Case 5
• 45 year old Caucasian female with known depression and fibromyalgia presents with fatigue and sleep disturbances.
• She complains that she never sleeps, and is very tired because of it. She sleeps in on the weekends but is only able to do so for an extra hour. She tries to nap during her days off, but even though she is tired, she is unable to fall asleep.
• It takes her 2 hours to fall asleep, regardless of what time she goes to bed. So she has started going to bed at 8pm, in order to get as much sleep as she can.
• When she eventually does fall asleep, she awakens spontaneously at 3am and is awake for another 2 hours before she falls back to sleep. However, she is only able to sleep another hour before her alarm rings at 6am.
• She is a nurse working 7am to 7pm, and is frustrated that her lack of sleep is affecting her ability to concentrate and slowing her down at work.

InsomniaDifficulty Falling Asleep
Early Morning AwakeningsDifficulty Staying Asleep
+ Daytime Impairment
Chronic if lasts 3 or more months
Occurs at least 3x/week
Given adequate opportunity to sleep

Epidemiology
• Insomnia is the most common sleep disorder in the US
~1/3 of adults experience insomnia at some point
in their lives
• Persistent problem in 10% of US adults
• Women > men (2:1)
• Increases with Age

National Sleep Foundation Survey (1991)
Insomnia: Complex Symptom or Syndrome? , Presented by Sonia Ancoli-Israel, PhD. Medscape. Downloaded 10/1/17

Occurrence of Insomnia Symptoms
Ancoli-Israel S1, Roth T. Characteristics of insomnia in the United States: results of the 1991 National SleepFoundation Survey. I.Sleep. 1999 May 1;22 Suppl 2:S347-53.

How does insomnia develop?

Spielman’s 3P Model of Insomnia
Predisposing factors:
Biological
• Inherited susceptibility/altered
neurotransmitter substances
Psychosocial
• Anxiety
• Hyperarousal
Precipitating factors:
• Life stressors
• Medical illness
• Psychiatric illness
• Medications/substance
Perpetuating factors:
• Wake activities in
bed/bedroom
• Sleep extension (too much
time in bed/napping)
(Poor sleep hygiene)
Spielman A, Caruso L, Glovinsky P. A behavioral perspective on insomnia treatment. Psychiatr Clin North Am 1987;10:541-
553

Clinical history is the key to treating
insomnia!You do NOT need a sleep study to diagnose insomnia

Key Components of Insomnia History
• Characterization of the complaint type
• Frequency (nights per week or number of times per night)
• Duration (months, years, lifetime)
• Course (progressive, intermittent, relentless)
• Factors which increase or decrease symptoms
• Severity of nighttime distress and associated daytime symptomatology
• Identification of past and current precipitants, perpetuating
factors, treatments, and responses.
• A complete insomnia history also includes medical, psychiatric,
medication/substance, and family/social/occupational histories.

Medical Conditions associated with Insomnia
Schutte-Rodin S et al. Clinical Guideline for the Evaluation and Management of Chronic Insomnia. Journal of Clinical Sleep Medicine, Vol. 4, No. 5, 2008

Medications Causing Insomnia
Adapted from Schutte-Rodin S et al. Clinical Guideline for the Evaluation and Management of Chronic Insomnia. Journal of Clinical Sleep Medicine, Vol. 4, No. 5, 2008
Analgesics Ibuprofen

Characterization of Sleep
• Sleep onset vs. maintenance vs. early morning awakenings
• Sleep quality
• State of mind at bedtime
• Level of sleepiness
• Relaxed vs. anxious
• Heightened arousal in bed and anxiety around bedtime,
anticipating a “bad night”
• Sensations of being more aware of environment

Is the sleep environment conducive to sleep?
• Bed vs. couch vs. recliner
• Room Temperature
• Light/dark
• Quiet/Noisy
• TV
• Bedpartner
• Environmental

Sleep hygiene
• Behaviors around sleep
• Frequently “bad” behaviors start as strategies to combat the sleep problem:
e.g., spending more time in bed in an effort to “catch up” on sleep.
Perpetuate sleep problems

What is the Patient Doing to Perpetuate the Insomnia?
• Napping
• Irregular sleep/wake schedules
• Routinely using sleep-disruptive products
• Caffeine
• Tobacco
• Alcohol
• Engaging in mentally or physically activating or emotionally upsetting
activities too close to bedtime
• Routinely using the bed/bedroom for activities other than sleep
• Failing to maintain a comfortable bedroom environment conducive to
sleep
Inadequate Sleep Hygiene

Wake Promoting Behaviors
• Some common wake promoting behaviors in bed or close to bedtime that can disrupt sleep:
• Using computer/smart phone
• Watching TV
• Talking on the telephone
• Exercising
• Eating
• Smoking
• “Clock watching”
• Doing homework

When to treat
• Treatment is recommended when the chronic insomnia has a
significant negative impact on the patient’s sleep quality, health,
comorbid conditions, or daytime function.
• It is essential to recognize and treat comorbid conditions that
commonly occur with insomnia, and to identify and modify
behaviors and medications or substances that impair sleep.

So what about our nurse? Should we treat?
• 45 year old Caucasian female with known depression and fibromyalgia presents with fatigue and sleep disturbances.
• She complains that she never sleeps, and is very tired because of it. She sleeps in on the weekends but is only able to do so for an extra hour. She tries to nap during her days off, but even though she is tired, she is unable to fall asleep.
• It takes her 2 hours to fall asleep, regardless of what time she goes to bed. So she has started going to bed at 8pm, in order to get as much sleep as she can.
• When she eventually does fall asleep, she awakens spontaneously at 3am and is awake for another 2 hours before she falls back to sleep. However, she is only able to sleep another hour before her alarm rings at 6am.
• She is a nurse working 7am to 7pm, and is frustrated that her lack of sleep is affecting her ability to concentrate and slowing her down at work.

Insomnia Treatment Modalities
➢Behavioral Therapies
➢Pharmacotherapy

Behavioral Therapies
➢Sleep hygiene rules
➢Stimulus control therapy
➢Sleep restriction therapy
➢Relaxation techniques
➢Cognitive therapy strategies

Implementation of Behavioral Therapies for
Insomnia➢By PCP
➢By Sleep Specialist
➢By Behavioral Sleep Specialist
➢Only 14 in the state of Michigan
➢Web based CBT-I Programs

Web Based CBT-I Programs
1)MySHUTi.com
2)CBTforImsomnia.com
3)CBT-i Coach
4)RESTore.CBTprogram.com
5)Sleepio.com


Insomnia Pharmacotherapy
➢Unregulated substances
• Melatonin – Used for
1. Hypnotic Effect
2. Circadian Rhythm
Disorders

Insomnia Pharmacotherapy
➢Over the counter sleep aids
• Most have antihistamines
• Potential side effects of antihistamines
(Greater risks in elderly and patients taking
anticholinergic medications).
1. Confusion and delirium
2. Urinary retention
3. Dry mouth
4. Blurred vision
5. Narrow-angle Glaucoma exacerbation

Insomnia Pharmacotherapy
➢Off label Prescription medications
• Antidepressants
• Commonly prescribed examples
1.Trazodone
2.Amitriptyline
3.Mirtazapine
4.Doxepin

Insomnia Pharmacotherapy
➢Trazodone
• Usual dosage 50 – 150mg
• Side effects
1. Dizziness
2. Sedation
3. Hypotension
4. Headache
5. Sweating
6. Arrhythmia
7. Serotonin syndrome

Insomnia Pharmacotherapy
➢Anti-psychotics
• Usually with psychiatric
comorbidity
• Examples
1. Quetiapine
2. Olanzapine

Insomnia Pharmacotherapy
➢FDA Approved Medications
• Benzodiazepines
• Examples
1. Temazepam
➢Non-Benzodiazepines
• Examples
2. Zolpidem

Insomnia Pharmacotherapy ➢Selective Melatonin receptor Antagonist
• Examples
1. Ramelteon (Rozerem)
➢Selective Histamine Receptor Antagonist
• Example
1. Low dose Doxepin (Silenor)
• Usually 3 – 6 mg dose
➢Duel Orexin Receptor Antagonist
• Example
1. Suvorexant (Belsomra)

Insomnia Pharmacotherapy
DEA and Pregnancy Categories Medication Class DEA Schedule Pregnancy
Category
Benzodiazepines IV X
NonBenzodiazepines• eg. Zolpidem
IV C
Melatonin Receptor
Agonist• eg. Rozerem
Non-Schedule C
Histamine Receptor
Antagonist• eg. Doxepin
Non-Schedule C
Orexin Receptor
Antagonist• eg. Belsomra
IV C

Case 5: How to Manage?
• 45 year old Caucasian female with known depression and fibromyalgia presents with fatigue and sleep disturbances.
• She complains that she never sleeps, and is very tired because of it. She sleeps in on the weekends but is only able to do so for an extra hour. She tries to nap during her days off, but even though she is tired, she is unable to fall asleep.
• It takes her 2 hours to fall asleep, regardless of what time she goes to bed. So she has started going to bed at 8pm, in order to get as much sleep as she can.
• When she eventually does fall asleep, she awakens spontaneously at 3am and is awake for another 2 hours before she falls back to sleep. However, she is only able to sleep another hour before her alarm rings at 6am.
• She is a nurse working 7am to 7pm, and is frustrated that her lack of sleep is affecting her ability to concentrate and slowing her down at work.

QUESTIONS?

Case 6
• A 47-year-old man is evaluated for difficulty falling asleep and resulting daytime
fatigue occurring at least 3 to 4 times per week for the past several months. He
denies snoring or sleepwalking, shortness of breath, and chest pain. He recently
went through a divorce, which has caused some personal and financial stress in
his life. He smokes one-half pack per day of cigarettes.
• Pulse rate is 72/min, and blood pressure is 138/85 mm Hg. BMI is 26. The
remainder of the examination is normal.
• Laboratory studies include a hematocrit of 42%, a leukocyte count of 4200/μL (4.2
x 109/L), a fasting plasma glucose of 100 mg/dL (5.55 mmol/L), and a serum
thyroid-stimulating hormone level of 2.5 μU/mL (2.5 mU/L). Results of a chest
radiograph and electrocardiogram are normal.
• Which of the following is the most appropriate next step in diagnosis?
A. Polysomnography
B. Spirometry
C. Cardiac stress testing
D. Depression screening Adapted from: Wilson J. In the Clinic: Insomnia. Annals of Internal Med; 2008.

Case 6
• A 47-year-old man is evaluated for difficulty falling asleep and resulting daytime
fatigue occurring at least 3 to 4 times per week for the past several months. He
denies snoring or sleepwalking, shortness of breath, and chest pain. He recently
went through a divorce, which has caused some personal and financial stress in
his life. He smokes one-half pack per day of cigarettes.
• Pulse rate is 72/min, and blood pressure is 138/85 mm Hg. BMI is 26. The
remainder of the examination is normal.
• Laboratory studies include a hematocrit of 42%, a leukocyte count of 4200/μL (4.2
x 109/L), a fasting plasma glucose of 100 mg/dL (5.55 mmol/L), and a serum
thyroid-stimulating hormone level of 2.5 μU/mL (2.5 mU/L). Results of a chest
radiograph and electrocardiogram are normal.
• Which of the following is the most appropriate next step in diagnosis?
A. Polysomnography
B. Spirometry
C. Cardiac stress testing
D. Depression screeningAdapted from: Wilson J. In the Clinic: Insomnia. Annals of Internal Med; 2008.

Case 7
• A 38-year-old woman is evaluated for a 4-week history of awakening in the middle
of the night, although she falls asleep without difficulty. During the day, she notes
a feeling of hyperarousal and irritability, which is interfering with her effectiveness
at work. She is in excellent health and runs competitively. She does not smoke or
drink alcohol. She has used over-the-counter antihistamines to help her sleep, but
they are no longer effective.
• Pulse rate is 60/min, and blood pressure is 120/75 mm Hg. BMI is 20. The
remainder of the examination is normal. Acute insomnia is diagnosed, and the
patient is advised to avoid strenuous exercise or alcohol within a few hours of
bedtime, develop a relaxing evening routine, and avoid afternoon caffeine. The
patient follows this advice but continues to have difficulty sleeping.
• Which of the following is the most appropriate treatment for this patient?
A. Melatonin
B. Trazodone
C. Selective serotonin reuptake inhibitor
D. Diphenhydramine
E. Triazolam Wilson J. In the Clinic: Insomnia. Annals of Internal Med; 2008.

Case 7
• A 38-year-old woman is evaluated for a 4-week history of awakening in the middle
of the night, although she falls asleep without difficulty. During the day, she notes
a feeling of hyperarousal and irritability, which is interfering with her effectiveness
at work. She is in excellent health and runs competitively. She does not smoke or
drink alcohol. She has used over-the-counter antihistamines to help her sleep, but
they are no longer effective.
• Pulse rate is 60/min, and blood pressure is 120/75 mm Hg. BMI is 20. The
remainder of the examination is normal. Acute insomnia is diagnosed, and the
patient is advised to avoid strenuous exercise or alcohol within a few hours of
bedtime, develop a relaxing evening routine, and avoid afternoon caffeine. The
patient follows this advice but continues to have difficulty sleeping.
• Which of the following is the most appropriate treatment for this patient?
A. Melatonin
B. Trazodone
C. Selective serotonin reuptake inhibitor
D. Diphenhydramine
E. Triazolam Wilson J. In the Clinic: Insomnia. Annals of Internal Med; 2008.

Case 8
• A 42-year-old man is evaluated for a lifelong history of insomnia. He reports always
having had trouble sleeping, but sleep initiation and maintenance have become
more difficult over the past few years. He experiences daytime sleepiness but does
not have the opportunity to nap. He reports no depressed mood or anhedonia. His
wife has not noticed excessive snoring or abnormal or absent breathing during
sleep. He drinks one cup of coffee in the morning and drinks one alcoholic
beverage 3 to 4 nights per week. Medical history is otherwise unremarkable. He
takes no medications.
• On physical examination, the patient is afebrile, blood pressure is 142/82 mm Hg,
pulse rate is 78/min, and respiration rate is 14/min. BMI is 27. The remainder of the
physical examination is normal.
• Which of the following is the appropriate next step in management?
A. Alcohol cessation counseling
B. Sleep hygiene counseling
C. Trazodone
D. Zolpidem MKSAP-17

Case 8
• A 42-year-old man is evaluated for a lifelong history of insomnia. He reports always
having had trouble sleeping, but sleep initiation and maintenance have become
more difficult over the past few years. He experiences daytime sleepiness but does
not have the opportunity to nap. He reports no depressed mood or anhedonia. His
wife has not noticed excessive snoring or abnormal or absent breathing during
sleep. He drinks one cup of coffee in the morning and drinks one alcoholic
beverage 3 to 4 nights per week. Medical history is otherwise unremarkable. He
takes no medications.
• On physical examination, the patient is afebrile, blood pressure is 142/82 mm Hg,
pulse rate is 78/min, and respiration rate is 14/min. BMI is 27. The remainder of the
physical examination is normal.
• Which of the following is the appropriate next step in management?
A. Alcohol cessation counseling
B. Sleep hygiene counseling
C. Trazodone
D. Zolpidem MKSAP-17

Case 9• An 82-year-old woman is seen for follow-up evaluation of Alzheimer disease. Since her last visit
12 weeks ago, she has been taking rivastigmine, with a progressively titrated dosage. The
patient's only new symptoms are increasing insomnia, loss of appetite, and occasional diarrhea;
she has had no feelings of hopelessness, helplessness, sadness, or guilt. Her only other
medication is hydrochlorothiazide for hypertension.
• On physical examination, vital signs are normal. The patient has lost 6.8 kg (15.0 lb) since her
last visit. She scores 20/30 on a Mini–Mental State Examination, losing points in the recall,
orientation to time, complex commands, and attention and calculation sections; her score 12
weeks ago was 21/30. All other findings from the general physical and neurologic examinations
are normal.
• Results of laboratory studies, including a complete blood count, comprehensive metabolic profile,
and thyroid function tests, are normal.
• Which of the following is the most appropriate next step in management?
A. Add Donepezil
B. Add Memantine
C. Add mirtazapine at bedtime
D. Discontinue rivastigmine
MKSAP-17

Case 9• An 82-year-old woman is seen for follow-up evaluation of Alzheimer disease. Since her last visit
12 weeks ago, she has been taking rivastigmine, with a progressively titrated dosage. The
patient's only new symptoms are increasing insomnia, loss of appetite, and occasional diarrhea;
she has had no feelings of hopelessness, helplessness, sadness, or guilt. Her only other
medication is hydrochlorothiazide for hypertension.
• On physical examination, vital signs are normal. The patient has lost 6.8 kg (15.0 lb) since her
last visit. She scores 20/30 on a Mini–Mental State Examination, losing points in the recall,
orientation to time, complex commands, and attention and calculation sections; her score 12
weeks ago was 21/30. All other findings from the general physical and neurologic examinations
are normal.
• Results of laboratory studies, including a complete blood count, comprehensive metabolic profile,
and thyroid function tests, are normal.
• Which of the following is the most appropriate next step in management?
A. Add Donepezil
B. Add Memantine
C. Add mirtazapine at bedtime
D. Discontinue rivastigmine
MKSAP-17

Case 10
• A 73-year-old man is evaluated for sleep difficulties. He notes unrefreshing sleep that is sometimes interrupted by nocturia, and he occasionally experiences episodes of shortness of breath that awaken him. He thinks he might snore but has no regular bed partner to provide confirmation. His normal sleep schedule is 10:30 PM to 6:30 AM. Most days of the week he feels sleepy during the daytime and naps for 45 minutes. He has a history of chronic atrial fibrillation and heart failure with stable exertional dyspnea. His medications are lisinopril, atorvastatin, warfarin, and metoprolol.
• On physical examination, temperature is 36.6 °C (97.9 °F), blood pressure is 118/70 mm Hg, pulse rate is 76/min, and respiration rate is 14/min; BMI is 27. Respiratory examination shows a low-lying soft palate and clear lung fields. Cardiac examination discloses an irregularly irregular rhythm but no murmurs.
• Which of the following is the most appropriate next step in management?
A. Auto-titrating positive airway pressure (APAP)
B. In-laboratory polysomnography
C. Home sleep apnea testing
D. Overnight pulse oximetry
MKSAP-17

Case 10
• A 73-year-old man is evaluated for sleep difficulties. He notes unrefreshing sleep that is sometimes interrupted by nocturia, and he occasionally experiences episodes of shortness of breath that awaken him. He thinks he might snore but has no regular bed partner to provide confirmation. His normal sleep schedule is 10:30 PM to 6:30 AM. Most days of the week he feels sleepy during the daytime and naps for 45 minutes. He has a history of chronic atrial fibrillation and heart failure with stable exertional dyspnea. His medications are lisinopril, atorvastatin, warfarin, and metoprolol.
• On physical examination, temperature is 36.6 °C (97.9 °F), blood pressure is 118/70 mm Hg, pulse rate is 76/min, and respiration rate is 14/min; BMI is 27. Respiratory examination shows a low-lying soft palate and clear lung fields. Cardiac examination discloses an irregularly irregular rhythm but no murmurs.
• Which of the following is the most appropriate next step in management?
A. Auto-titrating positive airway pressure (APAP)
B. In-laboratory polysomnography
C. Home sleep apnea testing
D. Overnight pulse oximetry
MKSAP-17

Case 11
• A 68-year-old woman describes a 2-year history of insomnia, which she attributes to an inability to get comfortable in bed because of a “creepy-crawly” sensation in her lower limbs. The sensation is absent during the day, but it has begun to bother her in the evening and is especially troublesome in bed. Walking relieves the sensation.
• Physical examination, including neurologic examination, is normal.
• Which of the following studies should be done next?
A. Serum ceruloplasmin level
B. Serum ferritin level
C. Urine porphyrin level
D. Nerve conduction study
E. Magnetic resonance imaging of the brain
Wilson J. In the Clinic: Insomnia. Annals of Internal Med; 2008.

Case 11
• A 68-year-old woman describes a 2-year history of insomnia, which she attributes to an inability to get comfortable in bed because of a “creepy-crawly” sensation in her lower limbs. The sensation is absent during the day, but it has begun to bother her in the evening and is especially troublesome in bed. Walking relieves the sensation.
• Physical examination, including neurologic examination, is normal.
• Which of the following studies should be done next?
A. Serum ceruloplasmin level
B. Serum ferritin level
C. Urine porphyrin level
D. Nerve conduction study
E. Magnetic resonance imaging of the brain
Wilson J. In the Clinic: Insomnia. Annals of Internal Med; 2008.