Embed Size (px)
Citation preview
1
Sleep Disorders: A Case-based Approach
LeRoy Essig, MDRami Khayat, MD
Case• 47 y/o male presents to primary doctor
for annual examination
• Recently started on citalopram
• History of hypertension
• Family history of CAD
• ROS: 30 Lbs wt gain/1year
Fatigue
Heart burn
Nasal congestion, dry mouth
Reduced concentration/memory
Case
• Social history: School bus driver, 30 p/year
• Wife complains of husband snoring
• Meds: Lisinopril, atorvastatin, hydrochlorothiazide
Case
2
Sleep History• Struggling to stay awake during
daytime• 6 hours of sleep per night with a 1
hour nap in the early afternoon, 2-3 beers/night
• Watches TV in bed before sleep
Sleep History• Awakens 3-4 times at night to use rest
room• Persistent loud snoring• Leg jerks and kicks, restless sleep• Wife “gradually” sleeping in another
room
Physical Examination• Exam: Weight 212, BMI 35, BP 147/87• Big uvula, nasal passages narrow,
“thick neck”• Lungs clear• Heart regular, no gallop, clear lungs• No peripheral edema• Intact sensation and strength in LE’s
What problems did you identify in this patient?
3
• General:Poorly controlled HTNCardiovascular risk factorsHeartburn
Problems
• SleepFatigue, depressionSnoring, sleepinessRestless sleep/legsDissatisfied spouse
Problems
Arrange problems in order of Importance
• SleepinessProfessional driver
• Poorly controlled hypertension• Smoking• Obesity• Depression• Restless legs
Problems in Order of Importance
4
• Inadequate sleep time• Poor sleep hygiene• Obstructive Sleep Apnea• Periodic Limb Movement of
Sleep/Restless Leg Syndrome• Inadequately treated depression• Medication side effects
Differential Diagnosis
Daytime Sleepiness• 16% of adults experience excessive
sleepiness that impairs daily functioning (Young, 2004).
• More than 100,000 automobile accidents each year are due to drivers falling asleep (National Highway Traffic Safety Administration).
71,000 non-fatal injuries1500 fatalities12.5 billion dollars in annual all-cause monetary loss
Daytime Sleepiness• Sleep deprivation for 1 day or sleeping 2
hours less/day for a week resulted in the same driving impairment as a blood alcohol level of 0.089 g/dL (Powell, 2001).
• 2002 NHTSA survey of 4010 adult drivers• Of the 11% who admitted to nodding
off while driving in the previous year, 2/3 stated they had ≤ 6 hours of sleep the previous night
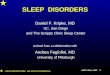
Assessment of SleepinessThe Epworth Sleepiness Scale
SITUATION CHANCE OF DOZING
1-Sitting and reading2-Watching TV3-Sitting inactive in a public place (I.e. a theater or a meeting)4- As a passenger in a carfor an hour without break5- Lying down to rest in the afternoon when circumstances permit6-Sitting and talking to someone7-Sitting quietly after lunch without alcohol 8 -In a car, while stopping for a few minutes in traffic
0 = Would never doze 1 = Slight chance of dozing2 = Moderate chance of dozing 3 = High chance of dozing
5
What is the most effective next intervention?
• Evaluate for OSA!Improved sleep hygiene and expanded sleep alone are unlikely to reduce sleepiness if OSA is untreatedOSA is linked to hypertension, cardiovascular disease, periodic limb movement and depression
• OSA- why should I care?
• If I have to care, what should I do about it?
• Treatment of OSA and CSA in patients with heart disease is a waste of time !
Obstructive Sleep Apnea
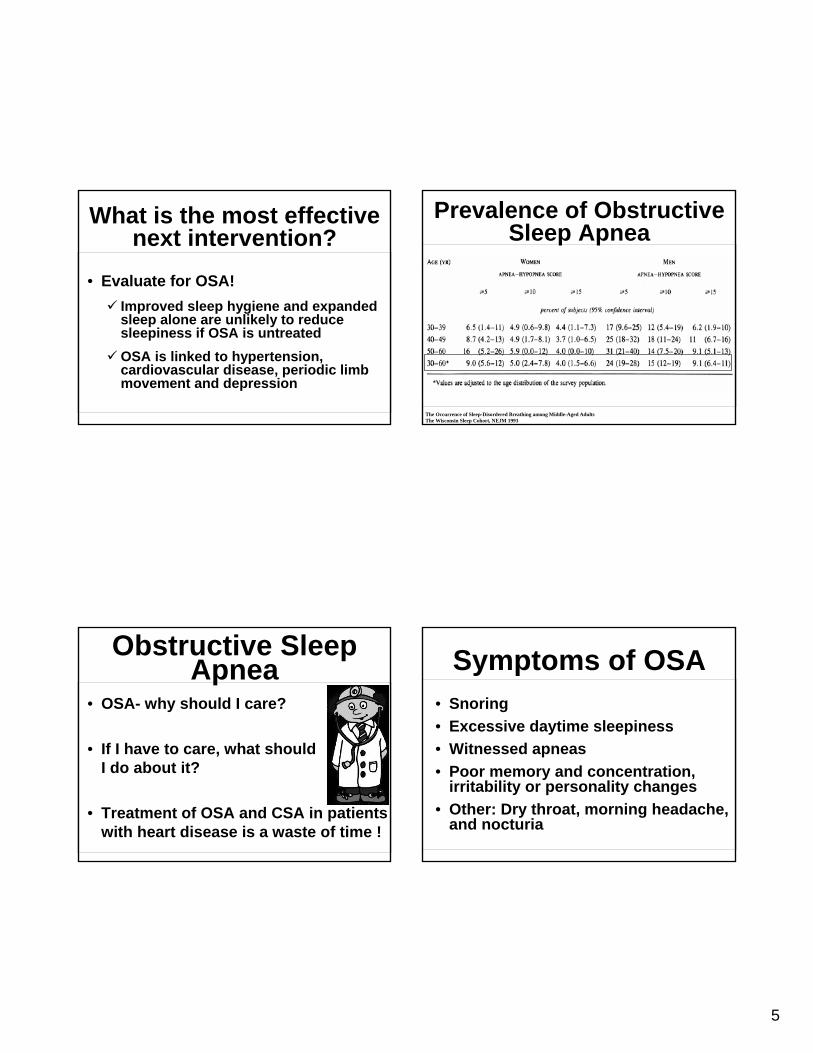
Prevalence of Obstructive Sleep Apnea
The Occurrence of Sleep-Disordered Breathing among Middle-Aged AdultsThe Wisconsin Sleep Cohort, NEJM 1993
Symptoms of OSA• Snoring• Excessive daytime sleepiness• Witnessed apneas• Poor memory and concentration,
irritability or personality changes• Other: Dry throat, morning headache,
and nocturia
6
Diagnosis• History and physical examination• Questionnaires• Pulse oximetry• Portable sleep studies• Polysomnography
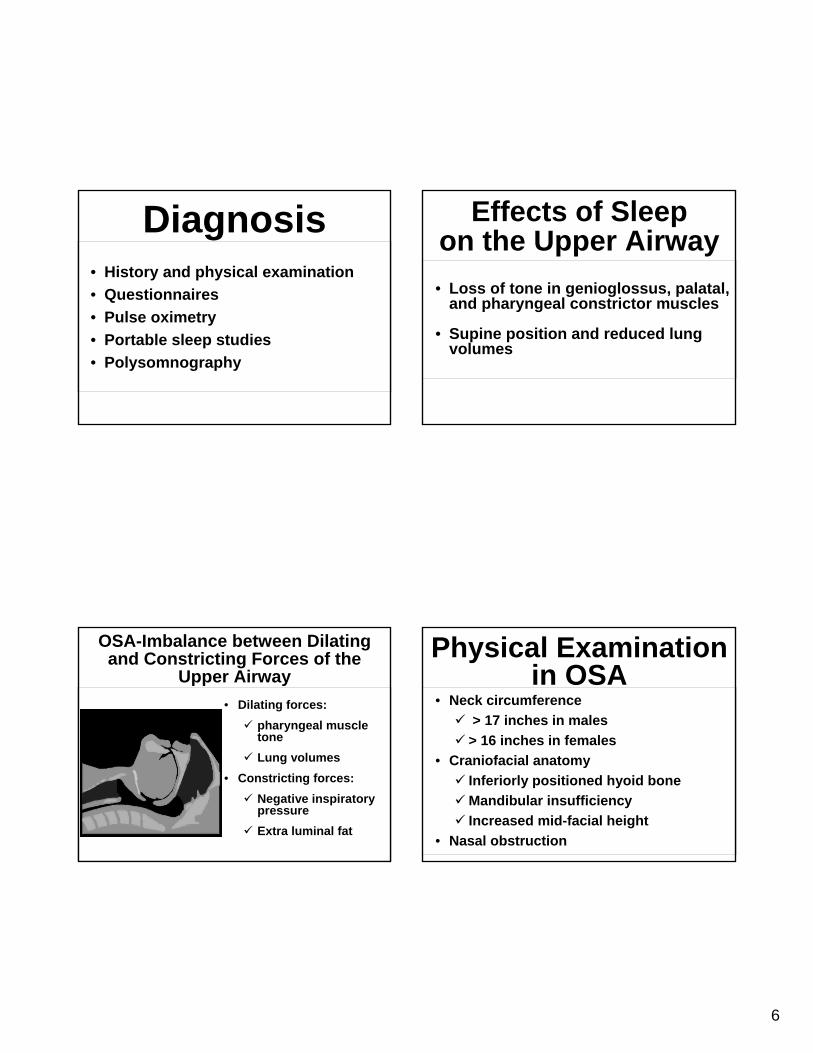
OSA-Imbalance between Dilating and Constricting Forces of the
Upper Airway• Dilating forces:
pharyngeal muscle toneLung volumes
• Constricting forces:Negative inspiratory pressureExtra luminal fat
Effects of Sleep on the Upper Airway• Loss of tone in genioglossus, palatal,
and pharyngeal constrictor muscles
• Supine position and reduced lung volumes
Physical Examination in OSA
• Neck circumference> 17 inches in males
> 16 inches in females• Craniofacial anatomy
Inferiorly positioned hyoid boneMandibular insufficiency Increased mid-facial height
• Nasal obstruction
7
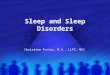
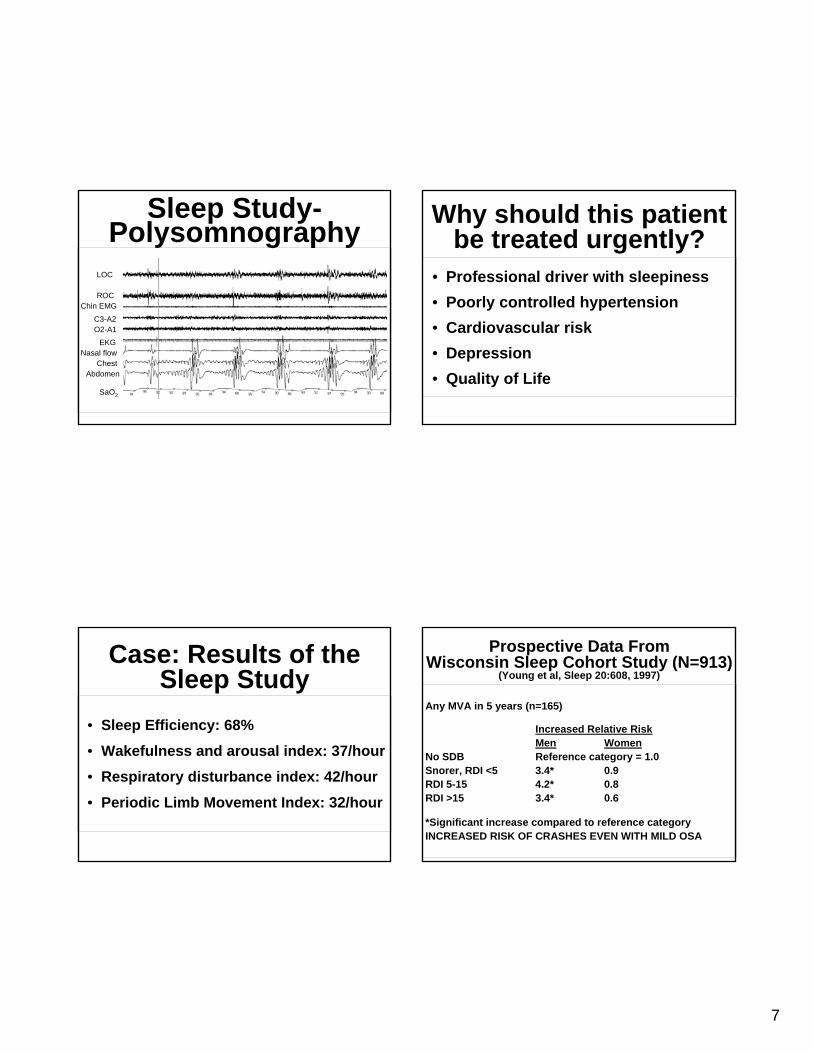
LOC
ROCChin EMG
C3-A2O2-A1
EKGNasal flow
ChestAbdomen
SaO2
Sleep Study-Polysomnography
Case: Results of the Sleep Study
• Sleep Efficiency: 68%
• Wakefulness and arousal index: 37/hour
• Respiratory disturbance index: 42/hour
• Periodic Limb Movement Index: 32/hour
Why should this patient be treated urgently?
• Professional driver with sleepiness• Poorly controlled hypertension• Cardiovascular risk• Depression• Quality of Life
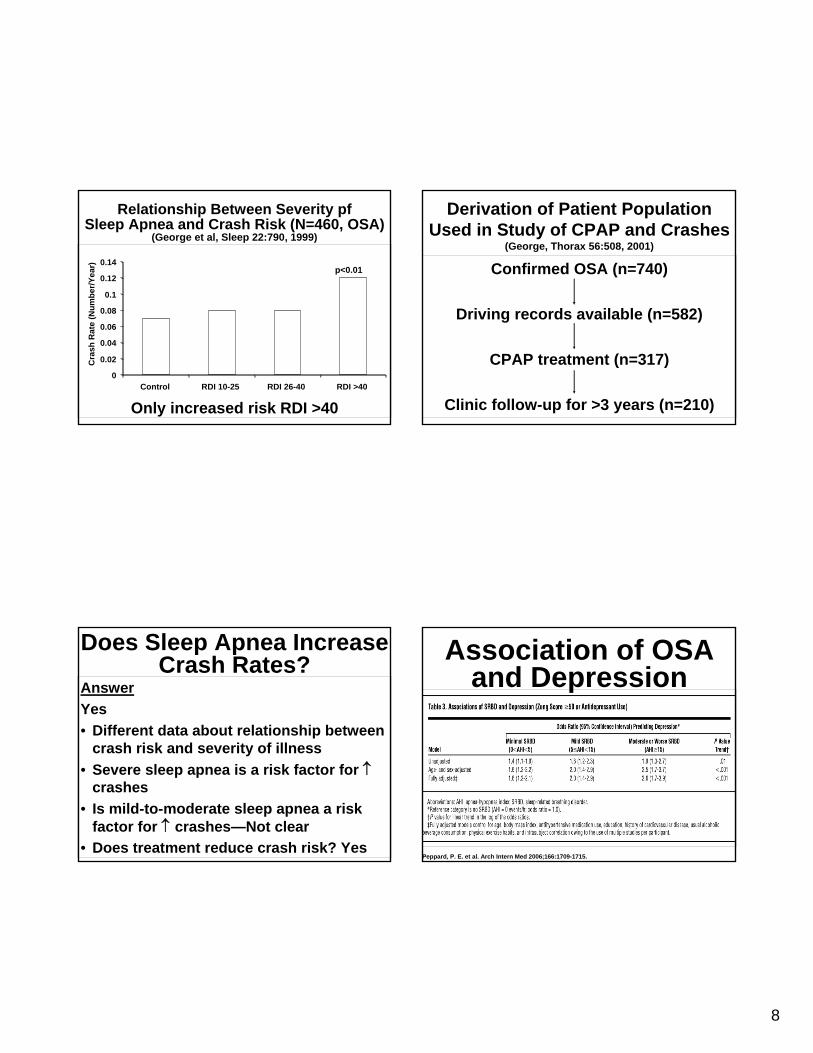
Prospective Data FromWisconsin Sleep Cohort Study (N=913)
(Young et al, Sleep 20:608, 1997)
Any MVA in 5 years (n=165)
Increased Relative RiskMen Women
No SDB Reference category = 1.0Snorer, RDI <5 3.4* 0.9RDI 5-15 4.2* 0.8RDI >15 3.4* 0.6
*Significant increase compared to reference categoryINCREASED RISK OF CRASHES EVEN WITH MILD OSA
8
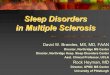
Relationship Between Severity pfSleep Apnea and Crash Risk (N=460, OSA)
(George et al, Sleep 22:790, 1999)
p<0.01
Only increased risk RDI >40
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
Control RDI 10-25 RDI 26-40 RDI >40
Cra
sh R
ate
(Num
ber/Y
ear)
Does Sleep Apnea IncreaseCrash Rates?
AnswerYes• Different data about relationship between
crash risk and severity of illness• Severe sleep apnea is a risk factor for ↑
crashes• Is mild-to-moderate sleep apnea a risk
factor for ↑ crashes—Not clear• Does treatment reduce crash risk? Yes
Derivation of Patient Population Used in Study of CPAP and Crashes
(George, Thorax 56:508, 2001)
Confirmed OSA (n=740)
Driving records available (n=582)
CPAP treatment (n=317)
Clinic follow-up for >3 years (n=210)
Peppard, P. E. et al. Arch Intern Med 2006;166:1709-1715.
Association of OSA and Depression
9
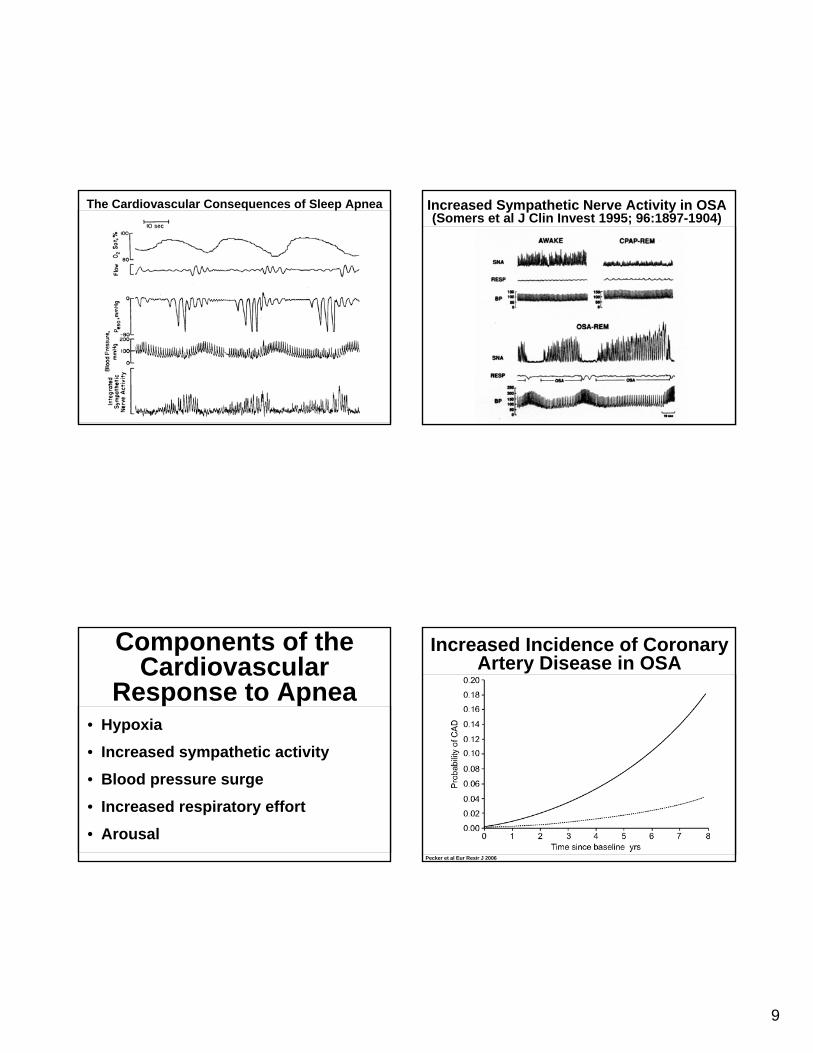
The Cardiovascular Consequences of Sleep Apnea
Components of the Cardiovascular
Response to Apnea• Hypoxia
• Increased sympathetic activity
• Blood pressure surge
• Increased respiratory effort
• Arousal
Increased Sympathetic Nerve Activity in OSA(Somers et al J Clin Invest 1995; 96:1897-1904)
Increased Incidence of Coronary Artery Disease in OSA
Pecker et al Eur Resir J 2006
10
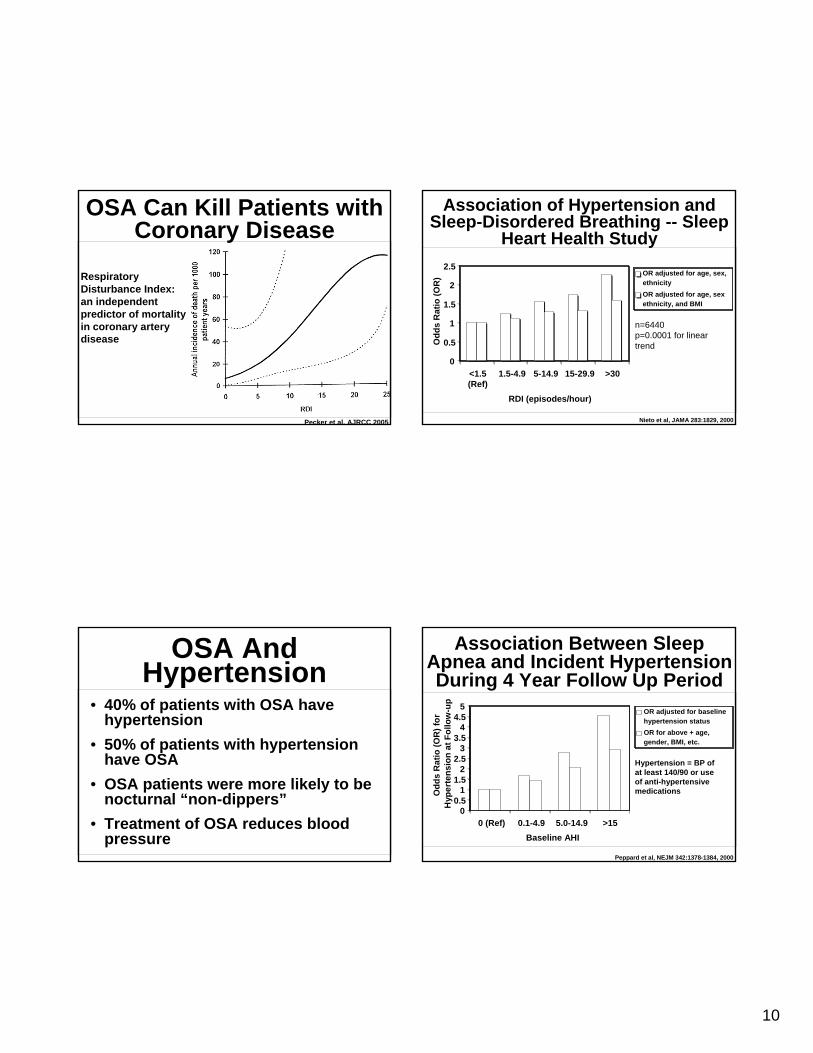
OSA Can Kill Patients with Coronary Disease
Pecker et al. AJRCC 2005
Respiratory Disturbance Index: an independent predictor of mortality in coronary artery disease
OSA And Hypertension
• 40% of patients with OSA have hypertension
• 50% of patients with hypertension have OSA
• OSA patients were more likely to be nocturnal “non-dippers”
• Treatment of OSA reduces blood pressure
0
0.5
1
1.5
2
2.5
<1.5(Ref)
1.5-4.9 5-14.9 15-29.9 >30
RDI (episodes/hour)
Odd
s R
atio
(OR
) OR adjusted for age, sex,ethnicityOR adjusted for age, sexethnicity, and BMI
Association of Hypertension and Sleep-Disordered Breathing -- Sleep
Heart Health Study
n=6440p=0.0001 for lineartrend
Nieto et al, JAMA 283:1829, 2000
00.5
11.5
22.5
33.5
44.5
5
0 (Ref) 0.1-4.9 5.0-14.9 >15Baseline AHI
Odd
s R
atio
(OR
) for
H
yper
tens
ion
at F
ollo
w-u
p
OR adjusted for baselinehypertension statusOR for above + age,gender, BMI, etc.
Association Between Sleep Apnea and Incident Hypertension During 4 Year Follow Up Period
Hypertension = BP of at least 140/90 or use of anti-hypertensive medications
Peppard et al, NEJM 342:1378-1384, 2000
11
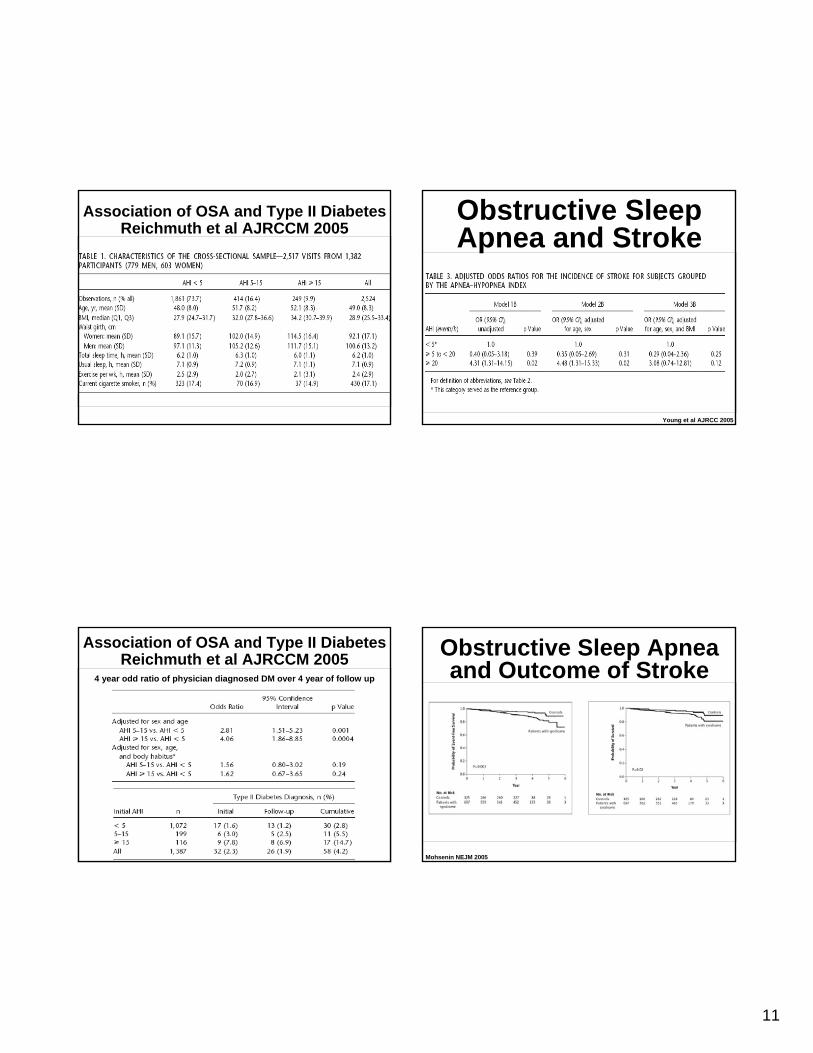
Association of OSA and Type II DiabetesReichmuth et al AJRCCM 2005
Association of OSA and Type II DiabetesReichmuth et al AJRCCM 2005
4 year odd ratio of physician diagnosed DM over 4 year of follow up
Obstructive Sleep Apnea and Stroke
Young et al AJRCC 2005
Obstructive Sleep Apnea and Outcome of Stroke
Mohsenin NEJM 2005
12
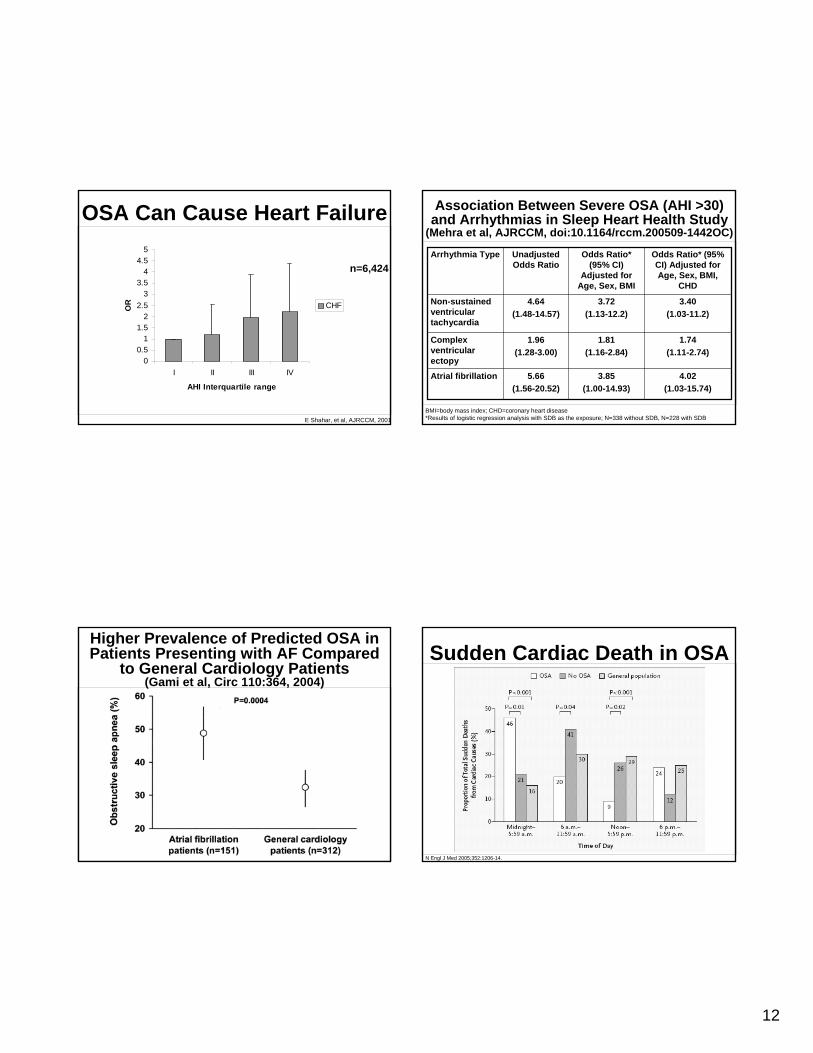
OSA Can Cause Heart Failure
E Shahar, et al, AJRCCM, 2001
00.5
11.5
22.5
33.5
44.5
5
I II III IV
AHI Interquartile range
OR CHF
n=6,424
Higher Prevalence of Predicted OSA in Patients Presenting with AF Compared
to General Cardiology Patients(Gami et al, Circ 110:364, 2004)
Association Between Severe OSA (AHI >30) and Arrhythmias in Sleep Heart Health Study
(Mehra et al, AJRCCM, doi:10.1164/rccm.200509-1442OC)
4.02(1.03-15.74)
3.85(1.00-14.93)
5.66(1.56-20.52)
Atrial fibrillation
1.74(1.11-2.74)
1.81(1.16-2.84)
1.96(1.28-3.00)
Complex ventricular ectopy
3.40(1.03-11.2)
3.72(1.13-12.2)
4.64(1.48-14.57)
Non-sustained ventricular tachycardia
Odds Ratio* (95% CI) Adjusted for Age, Sex, BMI,
CHD
Odds Ratio* (95% CI)
Adjusted for Age, Sex, BMI
Unadjusted Odds Ratio
Arrhythmia Type
BMI=body mass index; CHD=coronary heart disease*Results of logistic regression analysis with SDB as the exposure; N=338 without SDB, N=228 with SDB
Sudden Cardiac Death in OSA
N Engl J Med 2005;352:1206-14.
13
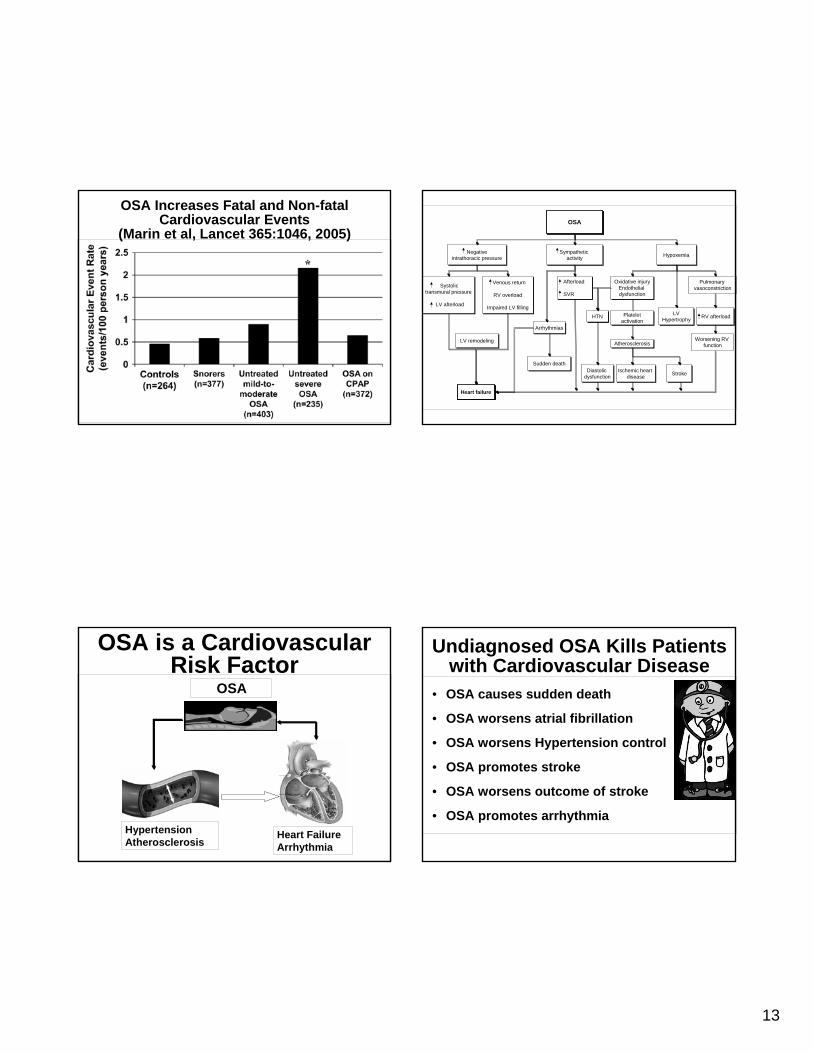
OSA Increases Fatal and Non-fatal Cardiovascular Events
(Marin et al, Lancet 365:1046, 2005)
OSA is a Cardiovascular Risk Factor
Heart FailureArrhythmia
HypertensionAtherosclerosis
OSA
Pulmonary vasoconstriction
Worsening RV function
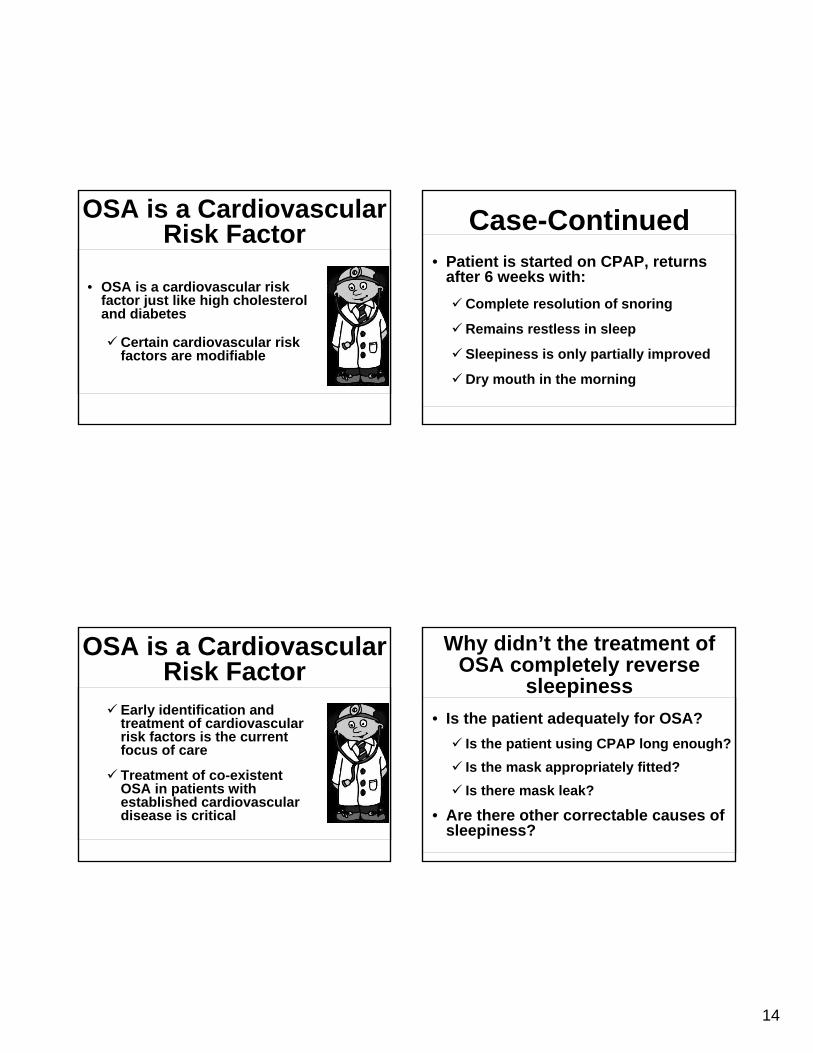
OSA
Sympathetic activity HypoxemiaNegative
intrathoracic pressure
Oxidative injuryEndothelial dysfunction
Afterload
SVR
RV afterload
Atherosclerosis
Ischemic heart disease
HTN
Arrhythmias
Diastolic dysfunction
Systolic transmural pressure
LV afterload
Venous return
RV overload
Impaired LV filling
Heart failure
Sudden death
Stroke
LVHypertrophy
LV remodeling
Plateletactivation
Undiagnosed OSA Kills Patients with Cardiovascular Disease
• OSA causes sudden death
• OSA worsens atrial fibrillation
• OSA worsens Hypertension control
• OSA promotes stroke
• OSA worsens outcome of stroke
• OSA promotes arrhythmia
14
OSA is a Cardiovascular Risk Factor
• OSA is a cardiovascular risk factor just like high cholesterol and diabetes
Certain cardiovascular risk factors are modifiable
OSA is a Cardiovascular Risk Factor
Early identification and treatment of cardiovascular risk factors is the current focus of care
Treatment of co-existent OSA in patients with established cardiovascular disease is critical
Case-Continued• Patient is started on CPAP, returns
after 6 weeks with:Complete resolution of snoring
Remains restless in sleep
Sleepiness is only partially improved
Dry mouth in the morning
Why didn’t the treatment of OSA completely reverse
sleepiness• Is the patient adequately for OSA?
Is the patient using CPAP long enough?Is the mask appropriately fitted?Is there mask leak?
• Are there other correctable causes of sleepiness?
15
CPAP Limitations• Interface
• Mask issues, claustrophobia• Mouth leaks• Skin abrasion
• Pressure-related• Intolerance of pressure, flow • Rhinitis, sinusitis, headaches
CPAP Limitations• Equipment related
• Noise, smell, condensation• Dryness, inadequate humidification
• Changes in optimal pressure within night/over time
• Weight gain• Nasal congestion• Positional • Sleep stage
Assessment of Adequate treatment of OSA
• Hours of use per night: >4-5 hours• Total Sleep time: 7-10 hours• Mask fitting (noise, dry eyes, aerophagia)• Number of awakening per night
Differential Diagnosis• Inadequate sleep time• Poor sleep hygiene• Obstructive Sleep Apnea• Periodic Limb Movement of Sleep/Restless
Leg Syndrome• Inadequately treated depression• Medication side effects
16
Sleep Hygiene Interventions
• Increase sleep time• Avoid Alcohol too close before
bedtime• Avoid TV in bed• Exercise 4-5 hours before bedtime
Case-Continued• Interventions:
Sleep ExpansionSleep hygieneChange Citalopram
Conclusions• Excessive Sleepiness is present in
>16% of adults
• OSA is present in 5-15% middle age adults
• OSA increases risk of vehicle accidents
• OSA is a cardiovascular risk factor