Embed Size (px)
Citation preview

JANUARY/FEBRUARY 2011
www.sportsmed.org
N E W S L E T T E R O F T H E A M E R I C A N O R T H O P A E D I C S O C I E T Y F O R S P O R T S M E D I C I N E
STOP SportsInjuries UpdateHousing for2011 AnnualMeeting AvailableAOSSM CommitteeVolunteersWanted
SLAPTEARS
CO-EDITORS
EDITOR William N. Levine MD
EDITOR Daniel J. Solomon MD
MANAGING EDITOR Lisa Weisenberger
ISSUE EDITOR Kristi Overgaard
PUBLICATIONS COMMITTEE
Daniel J. Solomon MD, Chair
Kenneth M. Fine MD
Robert A. Gallo MD
Richard Y. Hinton MD
David M. Hunter MD
Grant L. Jones MD
John D. Kelly IV MD
William N. Levine MD
Brett D. Owens MD
Kevin G. Shea MD
Brian R. Wolf MD, MS
BOARD OF DIRECTORS
PRESIDENT Robert A. Stanton MD
PRESIDENT-ELECT Peter A. Indelicato MD
VICE PRESIDENT Christopher R. Harner MD
SECRETARY Jo A. Hannafin MD, PhD
SECRETARY-ELECT James P. Bradley MD
TREASURER Robert A. Arciero MD
TREASURER-ELECT Annunziato Amendola MD
UNDER 45 MEMBER-AT-LARGE David R. McAllister MD
UNDER 45 MEMBER-AT-LARGE Mininder S. Kocher MD
OVER 45 MEMBER-AT-LARGE Mark E. Steiner MD
PAST PRESIDENT James R. Andrews MD
PAST PRESIDENT Freddie H. Fu MD
COUNCIL OF EDUCATION Andrew J. Cosgarea MD
COUNCIL OF RESEARCH Constance R. Chu MD
COUNCIL OF COMMUNICATIONS Daniel J. Solomon MD
EX OFFICIO COUNCIL OF DELEGATES Patricia A. Kolowich MD
JOURNAL EDITOR, MEMBER EX OFFICIO Bruce Reider MD
AOSSM STAFF
EXECUTIVE DIRECTOR Irv Bomberger
MANAGING DIRECTOR Camille Petrick
EXECUTIVE ASSISTANT Sue Serpico
ADMINISTRATIVE ASSISTANT Mary Mucciante
DIRECTOR OF CORPORATE RELATIONS Debbie Cohen
DIRECTOR OF FINANCE Ken Hoffman
DIRECTOR OF RESEARCH Bart Mann
DIRECTOR OF COMMUNICATIONS Lisa Weisenberger
COMMUNICATIONS ASSISTANT Joe Siebelts
STOP SPORTS INJURIES CAMPAIGN DIRECTOR Michael Konstant
DIRECTOR OF EDUCATION Susan Brown Zahn
SENIOR ADVISOR FOR CME PROGRAMS Jan Selan
EDUCATION & FELLOWSHIP COORDINATOR Heather Heller
EDUCATION & MEETINGS COORDINATOR Pat Kovach
MANAGER, MEMBER SERVICES & PROGRAMS Debbie Turkowski
EXHIB ITS & ADMIN COORDINATOR Michelle Schaffer
AOSSM MEDICAL PUBLISHING GROUP
MPG EXECUTIVE EDITOR AND AJSM EDITOR Bruce Reider MD
AJSM SENIOR EDITORIAL/PROD MANAGER Donna Tilton
SPORTS HEALTH EDITORIAL/PROD MANAGER Kristi Overgaard
SPORTS MEDICINE UPDATE is a bimonthly publication of the American Orthopaedic Society for Sports Medicine (AOSSM). The AmericanOrthopaedic Society for Sports Medicine—a world leader in sports medicine education, research, communication, and fellowship—is a nationalorganization of orthopaedic sports medicine specialists, including national and international sports medicine leaders. AOSSM works closely withmany other sports medicine specialists and clinicians, including family physicians, emergency physicians, pediatricians, athletic trainers, andphysical therapists, to improve the identification, prevention, treatment, and rehabilitation of sports injuries.
This newsletter is also available on the Society’s Web site at www.sportsmed.org.
TO CONTACT THE SOCIETY: American Orthopaedic Society for Sports Medicine, 6300 North River Road, Suite 500, Rosemont, IL 60018,Phone: 847/292-4900, Fax: 847/292-4905.
1 From the President
7 Career DevelopmentAward Winner
8 STOP Sports InjuriesCampaign
10 Annual MeetingHousing Available
12 Society News
14 Membership News
15 Fellowship News
15 Names in the News
16 Upcoming Meetingsand Courses
2 Team Physician’s CornerSLAP Tears: Pearls and Pitfalls in Diagnosisand Management
JANUARY/FEBRUARY 2010
HOME
HOME

January/February 2011 SPORTS MEDICINE UPDATE 1
FROM THE PRESIDENT
2010 WAS AN EXCEPTIONAL YEAR FOR AOSSM, and it closed on a high pointon multiple fronts related to research, education, and public outreach.
Robert A. Stanton, MD
In early December, the Society collaborated with the NIH andthe National Arthritis Foundation, hosting the Post-Joint InjuryOsteoarthritis Conference II. The workshop, co-chaired byConstance Chu, MD, and Scott Rodeo, MD, brought togetherthe leading osteoarthritis (OA) researchers throughout the worldwith the goal of identifying research strategies for preventingor delaying the progression of post-joint trauma OA. It was aprivilege for me to be able to participate with this illustriousgroup. As a clinician who treats patients with post-traumaticOA daily, I am acutely aware of the impact of this disease. Ifwe can discover ways to modify the progression of OA, I trulybelieve that this effort may be the most significant undertakingever performed by the AOSSM. The breadth and depth ofindividual expertise that Connie and Scott assembled, alongwith the credibility and support of our institutional partners,provided a superb starting point. The challenge is not a smallone, but the intellectual and financial resources committedto this endeavor will make for an exciting next chapter.Also in December, the Society sponsored the highly successful
Advanced Team Physician Course (ATPC) in Washington, DC.The meeting is a joint endeavor between the AOSSM, theAmerican College of Sports Medicine, and the American MedicalSociety for Sports Medicine. The meeting is planned by repre-sentatives from each organization. A special note of appreciationand congratulations are in order to Augustus Mazzocca, MD, MS,not only for his service as program chair, but also for the strongprogram and faculty he assembled, and the record attendance itattracted—more than 347 orthopaedic surgeons, primary carephysicians, athletic trainers, physical therapists, and other sportsmedicine professionals. The orthopaedic surgeons who participatedas faculty noted that the meeting was especially valuable fororthopaedic sports medicine fellows because of its breadth anddepth of primary care and team coverage topics. I encourage
program directors that are looking for quality educationalresources in these areas to consider sending their fellows to thiscourse next year. It is an educational bargain that is hard toreplicate in a program setting.Finally, December marked the arrival of Michael Konstant
as Campaign Director for the STOP Sports Injuries campaign.Mike’s background and responsibilities are covered in this issueof Sports Medicine Update. I want to note the significance ofhis joining AOSSM because it reflects the Board’s commitmentto bring in senior level staff support to allow the STOP SportsInjuries program to build upon its many successes since its launcheight months ago. Mike already has been on the road, meetingwith our key partners, and will be working with our leadershipand members as we expand the STOP Sports Injuries initiativesat the national and local levels. I had the pleasure of meetingwith Mike soon after he joined our staff, and I am confidentthat his expertise, enthusiasm, and commitment will help theSociety achieve its vision for this program.During my tenure on the AOSSM Board, I’ve come to realize
that the Society’s past successes are but a prologue to its futuredirection for the organization and our profession. With that inmind, the Society should have a sense of pride and satisfactionthat 2010 finished on such a high note, and a sense of anticipationfor all that awaits us in the new year. The program committeemet in Chicago just before Christmas. Marlene DeMaio, MD,is organizing an educational Specialty Day and a superbAnnual Meeting.I hope all had a wonderful holiday season. You should be
proud of your organization and I encourage each of you toparticipate in its activities.
HOME
HOME

2 SPORTS MEDICINE UPDATE January/February 2011
First described by Andrews1 and later characterizedby Snyder et al.2 superior labrum anterior and posterior (SLAP)lesions are injuries to the labral cartilage of the shoulder jointat the superior aspect of the glenoid fossa in the region of theorigin of the long head of the biceps tendon. SLAP lesions area significant source of shoulder pain and instability and havebeen identified in 6–26 percent of shoulder arthroscopiesperformed for various injuries in the general populationand up to 38 percent in the military population.3-6
SLAP TEARS: PEARLS AND PITFALLS INDIAGNOSIS AND MANAGEMENT
T E A M P H Y S I C I A N ’ S C O R N E R
DANIEL J. SOLOMON, MDMarin Orthopedics and Sports MedicineNovato, California
WILLIAM N. LEVINE, MDThe Center for Shoulder, Elbow and Sports MedicineThe New York Orthopaedic HospitalColumbia University College of Physiciansand SurgeonsNew York, New York
HOME
HOME
Continued on page 3
Our purpose is to review superior labralfunction, anatomy, and mechanisms ofinjury and to provide useful tips in thetreatment of SLAP tears.
SLAP Function andRole in the ShoulderThe superior labrum augments the effectiveshape and diameter of the glenoid surface.It aids in cavity-compression, creating a sealaround the humeral head, and augmentsglenohumeral stability. A SLAP tear allowsincreased inferior and superior translationof the humeral head on the glenoid.7
Mechanism of InjurySeveral different mechanisms are postulatedto be responsible for SLAP lesions andthey are likely the result of acute orrepetitive traumatic events.8-9
One of the critical factors in determiningappropriate treatment is understanding whythe superior labrum failed. Restorationof anatomy and correcting the conditionsleading to an attritional posterior-superiorSLAP in an overhead athlete or throweris critical to success. Failure to correctthe additional pathology may be oneof the reasons that repairs of attritionaltears have less success than repairs oftraumatic SLAP tears.Burkhart et al. described pathology
leading to SLAP tears in a throwerbeginning with scapular dyskinesis ordysfunction, leading to a hypertrophyand tightness in the posterior inferiorglenohumeral ligament and glenohumeralinternal rotational deficit (GIRD).This causes the center of rotation ofthe glenohumeral joint to shift superiorand posterior on the glenoid leading tooverload and attrition of the posteriorsuperior labral region.9
Similarly, large and massive rotatorcuff tears tend to have superior migrationof the humeral head and attrition andfraying of the superior labrum.Traumatic injuries leading to SLAP
tears include falls with the arm elevatedor forceful elevation and abduction ofthe arm in the overhead position. In some
instances, recurrent shoulder instabilityepisodes can propagate anterior or evenposterior labral tears around the glenoidsuperiorly leading to the type V throughIX SLAP tears (Table 1). Traumatic tearstypically occur slightly more anterior inthe superior labrum whereas tears causedby repetitive forces and attrition aremore posterior.
ClassificationSLAP lesions were originally classifiedinto four categories by Snyder et al.2
Maffet et al. added to Snyder’s originalclassification, including types V–IX whichdescribe tears extending anterior, posterioror circumferential around the glenoid.6
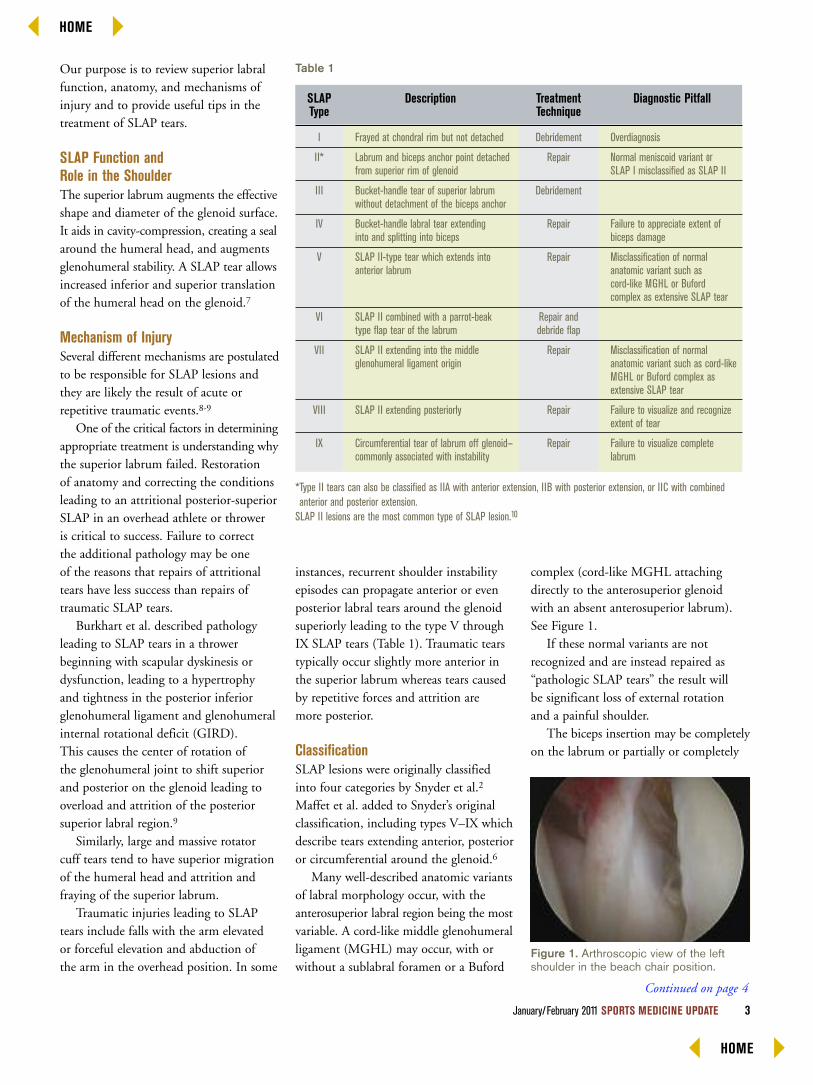
Many well-described anatomic variantsof labral morphology occur, with theanterosuperior labral region being the mostvariable. A cord-like middle glenohumeralligament (MGHL) may occur, with orwithout a sublabral foramen or a Buford
complex (cord-like MGHL attachingdirectly to the anterosuperior glenoidwith an absent anterosuperior labrum).See Figure 1.If these normal variants are not
recognized and are instead repaired as“pathologic SLAP tears” the result willbe significant loss of external rotationand a painful shoulder.The biceps insertion may be completely
on the labrum or partially or completely
January/February 2011 SPORTS MEDICINE UPDATE 3
Figure 1. Arthroscopic view of the leftshoulder in the beach chair position.
SLAP Description Treatment Diagnostic PitfallType Technique
Table 1
*Type II tears can also be classified as IIA with anterior extension, IIB with posterior extension, or IIC with combinedanterior and posterior extension.SLAP II lesions are the most common type of SLAP lesion.10
I
II*
III
IV
V
VI
VII
VIII
IX
Frayed at chondral rim but not detached
Labrum and biceps anchor point detachedfrom superior rim of glenoid
Bucket-handle tear of superior labrumwithout detachment of the biceps anchor
Bucket-handle labral tear extendinginto and splitting into biceps
SLAP II-type tear which extends intoanterior labrum
SLAP II combined with a parrot-beaktype flap tear of the labrum
SLAP II extending into the middleglenohumeral ligament origin
SLAP II extending posteriorly
Circumferential tear of labrum off glenoid—commonly associated with instability
Debridement
Repair
Debridement
Repair
Repair
Repair anddebride flap
Repair
Repair
Repair
Overdiagnosis
Normal meniscoid variant orSLAP I misclassified as SLAP II
Failure to appreciate extent ofbiceps damage
Misclassification of normalanatomic variant such ascord-like MGHL or Bufordcomplex as extensive SLAP tear
Misclassification of normalanatomic variant such as cord-likeMGHL or Buford complex asextensive SLAP tear
Failure to visualize and recognizeextent of tear
Failure to visualize completelabrum
HOME
HOME
Continued on page 4
attached on the supraglenoid tuberclerather than superior labrum.11
DiagnosisThe surgeon must correlate the patient’shistory with the physical examination andadvanced imaging for optimal diagnosticaccuracy. Based on the mechanism leadingto the SLAP tear, various examinationfindings may be present. The examinationmust allow complete visualization ofthe scapula through an arc of motion.One must critically evaluate the patients’scapular motion while viewing posteriorly.Ruling out acromioclavicular joint (ACJ)pathology should be done with palpationof the ACJ and evaluating cross-bodyadduction. Range of motion should beevaluated with the patient standing orseated but additionally the patients’shoulders should be examined in thesupine position to allow access to bothshoulders for evaluation of abducted
rotation. Specific examination tests suchas the active compression test, describedby O’Brien et al. should also be used.12
Imaging studies (MRI with or withoutintra-articular gadolinium) can helpconfirm the clinical impression. It canbe challenging to differentiate a normalvariant with pathology in some patients.Finally, intra-operative diagnosis relies onthe surgeon’s ability to differentiate a trueSLAP tear from the many normal variants.
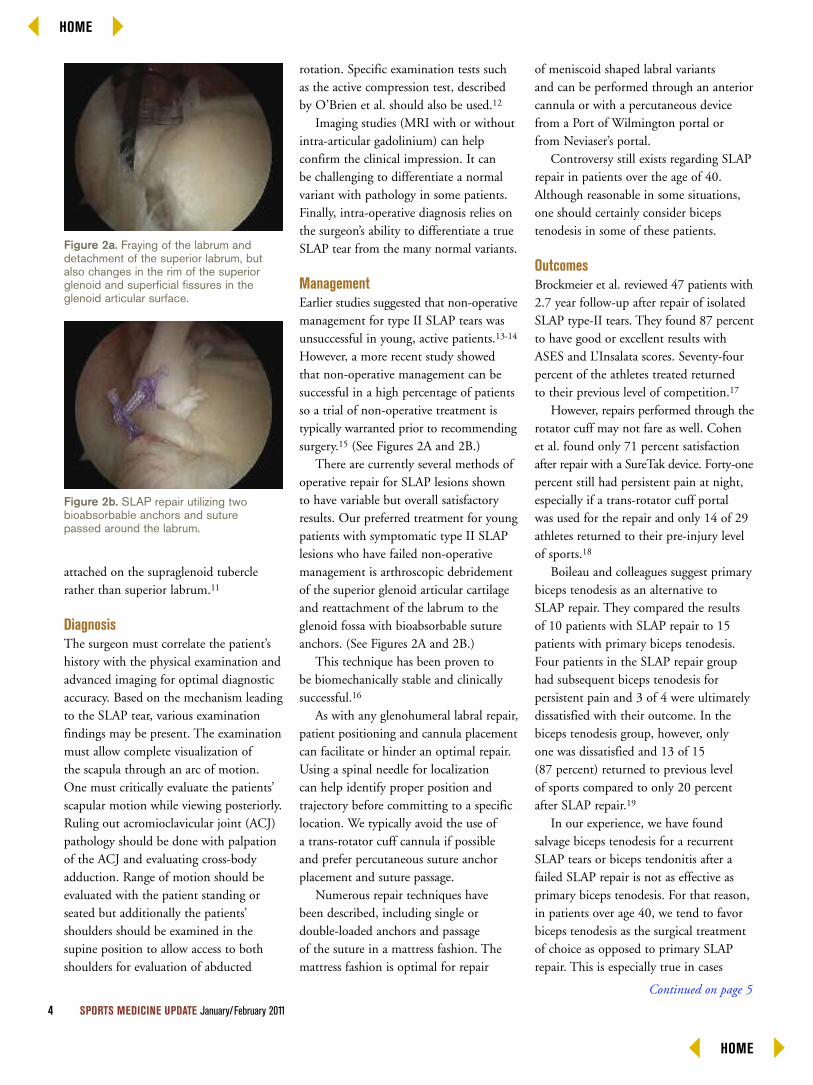
ManagementEarlier studies suggested that non-operativemanagement for type II SLAP tears wasunsuccessful in young, active patients.13-14
However, a more recent study showedthat non-operative management can besuccessful in a high percentage of patientsso a trial of non-operative treatment istypically warranted prior to recommendingsurgery.15 (See Figures 2A and 2B.)There are currently several methods of
operative repair for SLAP lesions shownto have variable but overall satisfactoryresults. Our preferred treatment for youngpatients with symptomatic type II SLAPlesions who have failed non-operativemanagement is arthroscopic debridementof the superior glenoid articular cartilageand reattachment of the labrum to theglenoid fossa with bioabsorbable sutureanchors. (See Figures 2A and 2B.)This technique has been proven to
be biomechanically stable and clinicallysuccessful.16
As with any glenohumeral labral repair,patient positioning and cannula placementcan facilitate or hinder an optimal repair.Using a spinal needle for localizationcan help identify proper position andtrajectory before committing to a specificlocation. We typically avoid the use ofa trans-rotator cuff cannula if possibleand prefer percutaneous suture anchorplacement and suture passage.Numerous repair techniques have
been described, including single ordouble-loaded anchors and passageof the suture in a mattress fashion. Themattress fashion is optimal for repair
of meniscoid shaped labral variantsand can be performed through an anteriorcannula or with a percutaneous devicefrom a Port of Wilmington portal orfrom Neviaser’s portal.Controversy still exists regarding SLAP
repair in patients over the age of 40.Although reasonable in some situations,one should certainly consider bicepstenodesis in some of these patients.
OutcomesBrockmeier et al. reviewed 47 patients with2.7 year follow-up after repair of isolatedSLAP type-II tears. They found 87 percentto have good or excellent results withASES and L’Insalata scores. Seventy-fourpercent of the athletes treated returnedto their previous level of competition.17
However, repairs performed through therotator cuff may not fare as well. Cohenet al. found only 71 percent satisfactionafter repair with a SureTak device. Forty-onepercent still had persistent pain at night,especially if a trans-rotator cuff portalwas used for the repair and only 14 of 29athletes returned to their pre-injury levelof sports.18
Boileau and colleagues suggest primarybiceps tenodesis as an alternative toSLAP repair. They compared the resultsof 10 patients with SLAP repair to 15patients with primary biceps tenodesis.Four patients in the SLAP repair grouphad subsequent biceps tenodesis forpersistent pain and 3 of 4 were ultimatelydissatisfied with their outcome. In thebiceps tenodesis group, however, onlyone was dissatisfied and 13 of 15(87 percent) returned to previous levelof sports compared to only 20 percentafter SLAP repair.19
In our experience, we have foundsalvage biceps tenodesis for a recurrentSLAP tears or biceps tendonitis after afailed SLAP repair is not as effective asprimary biceps tenodesis. For that reason,in patients over age 40, we tend to favorbiceps tenodesis as the surgical treatmentof choice as opposed to primary SLAPrepair. This is especially true in cases
4 SPORTS MEDICINE UPDATE January/February 2011
Figure 2a. Fraying of the labrum anddetachment of the superior labrum, butalso changes in the rim of the superiorglenoid and superficial fissures in theglenoid articular surface.
Figure 2b. SLAP repair utilizing twobioabsorbable anchors and suturepassed around the labrum.
HOME
HOME
Continued on page 5

with concurrent rotator cuff pathologywhere post-operative stiffness has beena clinical problem.
Concomitant PathologyWhen selecting operative treatmenttechniques, one must always return tothe basic tenet of restoring the anatomyby correcting the pathology. As discussedpreviously, the SLAP lesion may besecondary to other problems, such asGIRD, rotator cuff tears, or instability.Treatment of SLAP pathology in thesepatients must occur in conjunctionwith treatment of the primary problemas well. SLAP lesions commonly occurin association with other shoulderpathology. Snyder et al. found that only28 percent of SLAP tears were isolated.Twenty-nine percent had partial thicknessrotator cuff tears, 11 percent hadfull-thickness rotator cuff tears, 22 percenthad Bankart lesions, 16 percent hadacromioclavicular degeneration and10 percent had glenohumeral arthritis.10
Voos et al. evaluated 30 patients withcombined labral and rotator cuff repairs.Despite an average age over 47, 90 percenthad good or excellent outcome scoreswith ASES and L’Insalata and 77 percentreturned to a pre-injury athletic level.Two patients were limited by recurrentrotator cuff tears.20
In a small retrospective study, Ozbaydaret al. reviewed their results of combinedSLAP and Bankart (Maffet type V SLAPtears) repairs. Eight patients with an averageage of 31.8 (range 23–50) had follow-upaveraging just over three years. UCLA andRowe scores respectively improved from15 and 25 pre-operatively to 30 and 81 atfinal follow-up. Five of the eight patientsrated themselves as good or excellent.21
In a slightly larger study, Seroyer et al.evaluated 13 patients (average age 27.8years) with combined SLAP and posteriorlabral repairs (Maffet type VIII SLAPtears). Eight of the 13 patients werecontact athletes, however none requiredrevision or sustained recurrent instability.ASES scores improved from 51.4 to
90.0 and 69 percent returned to theirprevious level of sports.22
Two studies have reviewed results afterrepair of circumferential labral lesions.Lo and Burkart treated seven patientswith traumatic triple labral injuries. Nopatients sustained recurrent instabilityafter repair and six of seven were satisfied.23
Tokish et al. recently reviewed their
experience treating 39 shoulders withpost-traumatic circumferential labraltears. While six shoulders required revisionsurgery for recurrent instability (2), adhesivecapsulitis (2), biceps tendonitis (1), orrecurrent SLAP tear (1); all remained onactive duty in the military and returnedto their pre-injury level of activity.24
The Failed SLAP RepairKatz et al. retrospectively reviewedunsuccessful outcomes in 39 patients(40 shoulders) with a mean age of 43years at the time of SLAP repair. Thirtyshoulders (75 percent) had pain anddecreased range of motion (ROM); nine(22.5 percent) had pain but full ROM,
and one (2.5 percent) had pain andmechanical symptoms but full ROM.The Simple Shoulder Test score followinga painful SLAP repair was 3 out of apossible 12. Only 13 of 21 patients(62 percent) were satisfied after anothersurgical procedure which included onerevision repair, five biceps tenodeses,and 14 arthroscopic debridements.25
SummaryTrue unstable SLAP tears are stillrelatively uncommon and the increasein diagnosis and surgical treatment needsto be carefully evaluated in the future.Unnecessary surgical treatment of SLAPtears can lead to painful, stiff shouldersthat are not easily remedied with revisionsurgery or other measures. However,when appropriately indicated (failednon-operative management, clinicaland radiographic confirmation of aSLAP tear) surgical treatment can besuccessful in a high percentage of patients.Adherence to narrow indications andappropriate surgical techniques are criticalto the ultimate success of treatment.
January/February 2011 SPORTS MEDICINE UPDATE 5
Controversy still exists regarding SLAP repairin patients over 40. One should considerbiceps tenodesis in some patients.
HOME
HOME
1. Andrews JR, Carson Jr. SG, McLeod WD. Glenoid labrum tearsrelated to the long head of the biceps. Am J Sports Med. 1985.13(5): p. 337-41.
2. Snyder SJ, et al. SLAP lesions of the shoulder. Arthroscopy. 1990.6(4): p. 274-9.
3. Handelberg F, et al. SLAP lesions: a retrospective multicenterstudy. Arthroscopy. 1998. 14(8): p. 856-62.
4. Kampa RJ, Clasper J. Incidence of SLAP lesions in a militarypopulation. J R Army Med Corps. 2005. 151(3): p. 171-5.
5. Kim TK, et al. Clinical features of the different types of SLAPlesions: an analysis of one hundred and thirty-nine cases.J Bone Joint Surg Am. 2003. 85-A(1): p. 66-71.
6. Maffet MW, Gartsman GM, Moseley B. Superior labrum-bicepstendon complex lesions of the shoulder. Am J Sports Med. 1995.23(1): p. 93-8.
7. Pagnani MJ, et al. Effect of lesions of the superior portion of theglenoid labrum on glenohumeral translation. J Bone Joint SurgAm. 1995. 77(7): p. 1003-10.
8. Burkhart SS, Morgan CD. The peel-back mechanism: its role inproducing and extending posterior type II SLAP lesions and itseffect on SLAP repair rehabilitation. Arthroscopy. 1998. 14(6):p. 637-40.
9. Burkhart SS, Morgan CD, Kibler WB. The disabled throwingshoulder: spectrum of pathology Part I: pathoanatomy andbiomechanics. Arthroscopy. 2003. 19(4): p. 404-20.
10. Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuriesto the superior glenoid labrum. J Shoulder Elbow Surg. 1995.4(4): p. 243-8.
11. Tuoheti Y, et al. Attachment types of the long head of the bicepstendon to the glenoid labrum and their relationships with theglenohumeral ligaments. Arthroscopy. 2005. 21(10): p. 1242-9.
12. O’Brien SJ, et al. The active compression test: a new and effectivetest for diagnosing labral tears and acromioclavicular jointabnormality. Am J Sports Med. 1998. 26(5): p. 610-3.
13. Mileski RA, Snyder SJ. Superior labral lesions in the shoulder:pathoanatomy and surgical management. J Am Acad Orthop Surg.1998. 6(2): p. 121-31.
14. Nam EK, Snyder SJ. The diagnosis and treatment of superiorlabrum, anterior and posterior (SLAP) lesions. Am J Sports Med.2003. 31(5): p. 798-810.
15. Edwards SL, et al. Nonoperative treatment of superior labrumanterior posterior tears: improvements in pain, function, andquality of life. Am J Sports Med. 2010. 38(7): p. 1456-61.
16. DiRaimondo CA, et al. A biomechanical comparison of repairtechniques for type II SLAP lesions. Am J Sports Med. 2004.32(3): p. 727-33.
17. Brockmeier SF, et al. Outcomes after arthroscopic repair of type-IISLAP lesions. J Bone Joint Surg Am. 2009. 91(7): p. 1595-603.
18. Cohen DB, et al. Outcomes of isolated type II SLAP lesionstreated with arthroscopic fixation using a bioabsorbable tack.Arthroscopy. 2006. 22(2): p. 136-42.
19. Boileau P, et al. Arthroscopic treatment of isolated type II SLAPlesions: biceps tenodesis as an alternative to reinsertion. Am JSports Med. 2009. 37(5): p. 929-36.
20. Voos JE, et al. Outcomes of combined arthroscopic rotator cuffand labral repair. Am J Sports Med. 2007. 35(7): p. 1174-9.
21. Ozbaydar MU, et al. [Arthroscopic repair of combined superiorlabrum anterior posterior and Bankart lesions]. Acta OrthopTraumatol Turc. 2006. 40(2): p. 134-9.
22. Seroyer S, Tejwani SG, and Bradley JP. Arthroscopic capsulolabralreconstruction of the type VIII superior labrum anterior posteriorlesion: mean 2-year follow-up on 13 shoulders. Am J Sports Med.2007. 35(9): p. 1477-83.
23. Lo IK and Burkhart SS. Triple labral lesions: pathology andsurgical repair technique-report of seven cases. Arthroscopy. 2005.21(2): p. 186-93.
24. Tokish JM, et al. Arthroscopic repair of circumferential lesionsof the glenoid labrum. J Bone Joint Surg Am. 2009. 91(12):p. 2795-802.
25. Katz LM, et al. Poor outcomes after SLAP repair: descriptiveanalysis and prognosis. Arthroscopy. 2009. 25(8): p. 849-55.
References
6 SPORTS MEDICINE UPDATE January/February 2011
HOME
HOME
January/February 2011 SPORTS MEDICINE UPDATE 7
Dr. Cristin M. Ferguson has been selectedas the recipient of this year’s AOSSM-MTFCareer Development Award Supplement. Thisaward program provides $50,000 per year insalary supplementation to sports medicineorthopaedic surgeons who receive a CareerDevelopment Award (K Award) from NIH.The purpose of this program is to encouragemore sports medicine orthopaedic surgeonsto apply for K Awards by providing an offsetto the loss of clinical revenue due to dedicatedresearch time. Prior winners have includedDr. Bruce Miller of the University of Michiganand Dr. Warren Dunn of Vanderbilt University.Dr. Ferguson is currently an assistant professor
in the Department of Orthopaedic Surgery atthe Wake Forest University School of Medicineand is a team physician for Wake ForestUniversity Athletics. Her research interests
include the molecular biology of cartilage,meniscus, ligament repair and regeneration;tissue engineering; growth factors; and cellsignaling, with a focus on sports medicine.During her Career Development Award, she
will complete a study in which she has implantedan initial meniscus scaffold construct (seededand unseeded) in a large animal sheep surgicalmodel. Ultimately, she hopes to translate thistissue engineering approach when successfuland mature, to human clinical trials. She alsoplans to conduct studies of the role of hypoxia,HIF-1α, HIF-2α, F-2α, NFκ-b, and Sox-9signaling in fibrochondrocyte differentiation forboth tissue engineering applications, as well astheir role in regulating the process of meniscusdegeneration as it relates to osteoarthritis.To learn more about the NIH K Awards visit
http://grants.nih.gov/training/kawardhp.htm.
R E S E A R C H N E W S
AOSSM Selects Next Career Development Award Winner
The AOSSM-MTF Career Development Award Supplement Program is underwrittenby a grant from the Musculoskeletal Transplant Foundation (MTF).
Dr. Ferguson hopesto translate hertissue engineeringresearch to humanclinical trials.
HOME
HOME

A Message from Mike Konstant, STOPSports Injuries Campaign Director
I am honored and pleasedto have recently joinedAOSSM as the CampaignDirector for the STOPSports Injuries Campaign.I excitedly took this
position as a long-time sports fan andfather of three children, ages 19, 16,and 12, who have all been involved ina variety of sports at all levels. I believe inthe campaign’s message to prevent sportstrauma and overuse injuries in children.The campaign is off to a great startthanks to the hard work of AOSSM staff,members, the STOP Steering Committee,the STOP Council of Champions, andmany others. We have signed up morethan 120 collaborating organizationsand have developed an educational andvisually thrilling Web site and materialsfor distribution.My first two weeks on the job allowed
me to travel and make some outstandingcontacts. Irv Bomberger, AOSSM’sExecutive Director, and I visited the MLBWinter Baseball Meetings in Orlando andhad a great discussion with the leadershipof the Professional Baseball AthleticTrainers Society (PBAT). They are veryinterested in working with us through
their membership. We also had a chanceto meet two of AOSSM’s leaders: currentAOSSM President, Dr. Robert Stantonin his Fairfield, Connecticut, office andDr. James Andrews, STOP Sports InjuriesCampaign Co-Chairman, at his AndrewsSports Medicine and Orthopaedic Centerin Birmingham, Alabama. We also hadthe good fortune to meet with one ofthe campaign’s major sponsors, DePuyMitek at their headquarters in Raynham,Massachusetts. We look forward to teamingup with our other sponsors Smith &Nephew and Arthrex, Inc. to bring thecampaign’s message to the grassroots level.In closing, I’d like to thank AOSSM,
its members, and other partners for
this opportunity and encourage youto get involved in the STOP SportsInjuries Campaign this year. Visitwww.stopsportsinjuries.org to find easyways to help us spread the word and givea donation, if possible. Also, if you haven’talready, please fill out the “Join OurTeam” form on the Web site to officiallybecome an advocate for child safety.If you have suggestions or thoughts
on the campaign, please e-mail me [email protected] or call me at847/292-4900. Be sure to also keep up onthe latest developments with the campaignthrough our Facebook and Twitter pages.Together we can make a difference andKeep Kids in the Game for Life.
8 SPORTS MEDICINE UPDATE January/February 2011
New Year, New Opportunities in theSTOP Sports Injuries Campaign
NEW BLOG WRITER KEEPS READERS ENGAGEDDr. David Geier, a STOP Sports Injuries supporter and active member of AOSSM, began regularly contributingarticles to the campaign’s blog site this winter. Geier serves as Director of MUSC Sports Medicine in Charleston,South Carolina, as well as the team physician for area high schools. His experience as an orthopaedic surgeonand background with young athletes proves invaluable in delivering information on topics ranging from swimming
and cheerleading injuries to the risks involved with concussions. We continue to look for new blog contributors and subjectmatter, please send your suggestions to Lisa Weisenberger at [email protected].
HOME
HOME
Continued on page 9
January/February 2011 SPORTS MEDICINE UPDATE 9
New Supporters
The Denver-based Panorama Orthopedics & Spine Center, PCrecently gave their support to the STOP Sports Injuries campaign.As part of their efforts to spread the message of keeping youngathletes safe, the group reached out to members of the media.Dr. Mitch Robinson, orthopaedic surgeon and AOSSM member,spoke to Denver-based NBC 9 and CW 2 about the increasingincidence of overuse injuries and how the campaign focuses oneducating athletes, parents, and coaches. Efforts like these areinstrumental to spreading the message within local communities.If you have hosted an event or given an interview, please forwardpictures and links and a brief description to Joe Siebeltsat [email protected].
Radio Media Tour
The Society teamed-up with the American Academy ofOrthopaedic Surgeons in late 2010 to address and helpavoid winter sports injuries in children. Drs. Robert Stanton(current AOSSM President) and Peter Millett conductedtime for interviews with radio programs nationwide,discussing some common winter sports injuries andtips for staying safe. The tour included nationalbroadcasts on USA Radio Network and theSports Byline USA Network, along with regionalbroadcasts at stations, including KWLM-AMMinneapolis and WJSS-AM Baltimore.
Injury Prevention Event
The JCC of Greater Connecticut hosted anevent to help young female athletes learnhow to decrease ACL injury risk throughpreventative screening and exercises.Physical therapist Stephania Bell,a full-time injury analyst and seniorwriter for ESPN, participated in theevent and shared the importanceof the programs of the STOP SportsInjuries campaign with attendees.
Prepare Now for April’sYouth Sports Safety Month
In mid-February, we will be sending out tipsand information on preparing your own eventsand outreach efforts for April’s Youth SportsSafety Month. Share your suggestions or whereyou will be having your events on Facebook orTwitter or submit your event to Joe Siebelts [email protected].
HOME
HOME
10 SPORTS MEDICINE UPDATE January/February 2011
This year’s Annual Meeting in San Diego, July 7–10, 2011, will bringattendees a full plate of educational, social and cultural experiences.AOSSM President Robert A. Stanton, MD, and Program ChairMarlene DeMaio, MD, have been working hard to develop a line-upwhich shouldn’t be missed. Some of the highlights include:
� New Thursday afternoon workshop with live surgical demonstrationson the shoulder and elbow
� Symposium on the Disabled Athlete: A Sport Based Discussion
� Presidential Guest Speaker, Frank Deford, celebrated sportswriterand radio presence
� The Young Sports Medicine Specialists’ Workshop: Game Plans fora Winning Sports Medicine Practice—a chance for practice solutions
� AOSSM 2011 Research Workshop: Clinical Outcomes and TrialDesign in Orthopaedic Sports Medicine
� Social events at the San Diego Children’s Museum, ManchesterGrand Hyatt and other area attractions
� San Diego Zoo, Sea World, Legoland, Gas Lamp District andthe Pacific Ocean
SAN DIEGOBRINGS MORE THAN SHAMU TO THE
Stay tuned for moredetails and thePreliminary Programcoming to your mailboxand Inbox in March. Welook forward to seeingyou there!
HOME
HOME
Continued on page 11
January/February 2011 SPORTS MEDICINE UPDATE 11
Housing NowAvailable—Book Early
Attendee lodging for the2011 AOSSM AnnualMeeting is now open. TheManchester Grand Hyatt isthe host hotel and location forexhibits, scientific sessions,and instructional courses.
Book your housing onlineat www.sportsmed.org or bycalling 888/421-1442 or619/232-1234 and identifyyourself as an AOSSM 2011Annual Meeting attendee.Rates are $229/per night.Rooms with a view arelimited but available at anadditional premium. Ratesare guaranteed until June 4,2011, but are subject toavailability. Book early!
2011 ANNUAL MEETING
HOME
HOME
12 SPORTS MEDICINE UPDATE January/February 2011
J. MAYFIELD HARRIS, MD, a founding member of AOSSM,who served as a team doctor for several professional and amateursports organizations, died December 27, 2010, in his Los Altos,California, home. He was 86.A former high hurdler at USC, where he attended undergraduate
studies, Dr. Harris never lost his passion for sports. He served as ateam physician to the San Jose Earthquakes, Stanford University, andDeAnza and Foothill Colleges. He also counted numerous sportsroyalty among his clients, including 49ers legends John Brody andY. A. Tittle, Irish soccer star George Best, and tennis great Rod Laver.Recognizing that sports medicine soon would become a major
discipline, Dr. Harris joined a number of fellow professional teamphysicians in the early 1970s to organize AOSSM. It started withjust 18 members—all team physicians—and now comprises amembership of more than 2,500. Dr. Harris served on the AOSSMboard for many years.“When Rod came into town to play in the Transamerica
Tournament, he’d always come to see ‘Mayf ’ before his first match,”said Dr. Jeffrey Kliman, his partner. “He had a number of highprofile clients who relied on him for advice and treatment, no matterwhere they lived. He also was in demand among Silicon Valleyexecutives who beat a path to his door for consultations and surgeries.”Dr. Harris is survived by his wife, Joann, daughters Ann Brennan
of San Francisco and Martha Fuhrmann of San Antonio, Texas, andson Mike Harris of Los Altos.
Sports Health Call for Papers T. David SiskAwards for Research Excellence
Submit your manuscript today for the T. DavidSisk Award for Research Excellence in clinical,laboratory, and international research. Winnerswill be selected from the best papers submittedin each category to Sports Health: A MultidisciplinaryApproach by May 11, 2011. Winners will beannounced at the 2011 AOSSM Annual Meetingin San Diego and receive $2,500. To submit amanuscript visit http://submit.sportshealthjournal.orgor for more information, contact Kristi Overgaard,Sports Health Editorial Manager, at [email protected].
Review Annual Meeting andSpecialty Day Presentations
Did you know you can access presentationsfrom the AOSSM Annual Meeting, SpecialtyDay, and sport specific meetings by purchasinga yearly meeting subscription with your duesrenewal or you can pay for each meetingindividually? For more information visitwww.sportsmed.org/tabs/education/opportunities.aspx.
AOSSM Founding Member,J. MAYFIELD HARRIS, Passes Away
S O C I E T Y N E W S
Submit Your Hip ArthroscopyPaper to AJSM TodayThe American Journal of Sports Medicine(AJSM), with the support of Conmed Linvatec,is producing a special supplement on hiparthroscopy in the summer of 2011. BruceReider, MD, Editor-in-Chief, and guest editorsMark Safran, MD, and Mark Hutchinson, MD,are issuing a call for papers. Submissions shouldreport original clinical research or clinically-relevant laboratory research. The deadline formanuscript submission is February 28, 2011.Early submission in encouraged.Don’t miss this exciting opportunity. Visit
http://ajsm-submit.highwire.org to submit yourmanuscript. ContactDonna Tilton, AJSMeditorial manager, [email protected] withany questions.
HOME
HOME
Continued on page 13
January/February 2011 SPORTS MEDICINE UPDATE 13
Start the Year Off on the RightFoot—Send In Motion Directlyto Your PatientsAOSSM offers members the ability to addtheir practice name and logo to the electronicversion of In Motion for just $300 for all fourissues, which includes the high-resolution andlow-resolution PDFs to print the newsletteryourself, e-mail to patients, or post on yourWeb site. Personalizing In Motion gives yourpatients the resources for beginning the newyear on a positive note at a low price. Get thisexciting newsletter into your patients’ handstoday by e-mailing Lisa Weisenberger [email protected] for more information.
2010 Athletic HealthHandbook UpdatesThe 2010 Team Physician Corner articles fromSMU will be available for insertion into yourAthletic Health Handbook in early February. Login to My AOSSM page at www.sportsmed.organd click on the resources tab to download. Ifyou haven’t ordered your copy of the AthleticHealth Handbook we still have copies avail-able to members for just $10. Order this valu-able resource today!
Didn’t Get a Gift for Your ATC?Give them Sports Health.AOSSM members can provide gift subscriptionsto Sports Health: A Multidisciplinary Approachto Athletic Trainers in their institutions andcommunities. For the special rate of $45,you can give the gift of knowledge to yoursports medicine team in 2011. The amountof subscriptions you may sponsor is unlimited.To enter a gift subscription, please visitwww.sportsmed.org/shj. For more informationcontact Kristi Overgaard at [email protected].
Got NewsWe Could Use? Sports Medicine UpdateWants to Hear from You! Have you received a prestigious awardrecently? A new academic appointment? Been named a team physician? AOSSM wants to hear from you! Sports MedicineUpdate welcomes all members’ news items. Send information to Lisa Weisenberger, AOSSM Director of Communications,at [email protected], fax to 847/292-4905, or contact the Society office at 847/292-4900. High resolution (300 dpi) photosare always welcomed.
Subspecialty CertificationGrandfather OptionEnds March 31, 2011If you did not attend an ACGMEor Canadian Orthopaedic Associationaccredited orthopaedic sports medicinefellowship, you must register withthe American Board of OrthopaedicSurgery (ABOS) by March 31, 2011,to take the subspecialty certificationexam. After that deadline, individualswho did not attend an accreditedprogram will no longer be eligibleto sit for the exam. This deadline isespecially important because after 2011,a combined written recertification examwill only be offered to individualswho hold a general certificate anda subspecialty certificate.The 2011 exam will be offered on
November 3, 2011. In order to sit forthe exam, applicants must completethe application, submit their case list,provide the supplemental requireddocuments and pay the $450 fee byMarch 15, 2011. Late applications tosit for the exam will be accepted untilMarch 31, 2011, for an additional$350 late fee.The application process is detailed
and requires preparation. Anyoneinterested in sitting for the examis encouraged to get an early startin learning the requirements andcollating the materials. Details areavailable at www.abos.org, underthe Diplomates section.
AOSSM PUBLICATIONS
HOME
HOME

14 SPORTS MEDICINE UPDATE January/February 2011
very year, AOSSM accepts new volunteers to serve on its standing committees. Thosewho join committees not only heighten their experience as an AOSSM member,but form ties of fellowship with their colleagues that can last a lifetime. Althoughrequirements and duties vary by committee, volunteers must be able to attend regular
committee meetings, typically scheduled in conjunction with Specialty Day each springand the AOSSM Annual Meeting each summer. With the range of Society programs andcorresponding committees, there is an opportunity for you!If you are interested in serving on an AOSSM committee, simply look through the
available vacancies online and fill out the volunteer form from the November/Decemberissue of SMU and fax it back to the Society office by February 1, 2011, (fax: 847/292-4905),or complete the form as posted on the AOSSM Web site at www.sportsmed.org and e-mailit to [email protected]. Volunteers will be notified if they have been selected by May 2011.
M E M B E R S H I P N E W S
Don’t Forget to MeetYour AttendanceRequirements!Just a reminder, that Active andCandidate members must attendone meeting every four yearsin order to fulfill AOSSM’smembership requirements.Meetings that count include:Annual Meeting, SurgicalSkills and Board Review. Can’tremember the last meeting youattended? This information isjust a click away by logging on towww.sportsmed.org and visitingthe My AOSSM page. You canalso call the Society office at847/292-4900 to check on yourpast meeting attendance or sendDebbie Turkowski, Manager ofMember Services an e-mail [email protected].
Get Involved: Volunteer for anAOSSM Committee
EFax volunteer form backto the Society office byFebruary 1, 2011.
HOME
HOME

January/February 2011 SPORTS MEDICINE UPDATE 15
Fellows Exam DeadlineApproachingRegister your fellows today to take the AOSSMFellows Exam. The exam is designed to helpfellows identify their strengths and weaknessesin clinical and practice management areas.This year, you can register your fellows online.After completing the online exam, each fellowwill receive their own score and comparativeinformation for all fellows. AOSSM encouragesall Fellowship Directors to have their fellowscomplete the online Fellows Exam betweenMarch 17, 2011, and May 5, 2011. The costof the exam is $145 for each fellow and theregistration deadline is March 1, 2011.For information and to register, visit
www.sportsmed.org and click the Fellows Examquick link on the left side of the screen. If youhave specific questions, please e-mail HeatherHeller at [email protected].
MSU Sports Medicine HonorsDr. David Drez, Jr.
AOSSM member Dr.David Drez, Jr., wasrecently inducted into theMcNeese State University(MSU) Hall of Fame for
his more than 37 years of service as teamphysician. In further recognition ofthe countless hours he donated to theuniversity since 1973, the rehabilitationarea of the university’s Sports MedicineCenter was also named the “David Drez,Jr., MD Rehabilitation Facility.”“This is just a small way we can show
our appreciation for the years of commit-ment Dr. Drez has given to our athletes.His dedication is and will undoubtedlybe unsurpassed,” said Jim Murphy, headathletic trainer at McNeese, which islocated in Lake Charles, Louisiana. In
addition to these honors, an MSU footballscholarship was named in for Dr. Drezand an endowed chair in Sports Medicineat the Louisiana State University Schoolof Medicine Department of Orthopaedicshas been established in his name.
Dr. John A. Bergfeld Receives 2010Lifetime Achievement Award
The Greater ClevelandSports Commissionrecently awarded Dr. JohnA. Bergfeld, Senior Surgeonand Director of Operating
Rooms for the Cleveland Clinic withits 2010 Lifetime Achievement Award.“His distinguished career has touchedthe lives of thousands of individualsfrom professional and student athletesto aspiring physicians. He continuesto be an inspirational influence to the
Cleveland sports community,” said DavidGilbert, President and CEO of theGreater Cleveland Sports Commission.The Lifetime Achievement Award
traditionally honors an individual whohas advanced sports in Cleveland throughpersonal or career dedication and achieve-ments. Former recipients of the LifetimeAchievement award include Bob Kain(senior advisor for CAA and formerchairman of the Greater Cleveland SportsCommission), Chuck Kyle (head varsityfootball coach for St. Ignatius HighSchool), Joe Tait (broadcaster for ClevelandCavaliers), Herbert J. Score (pitcher andannouncer for Cleveland Indians), RichardE. Jacobs (former owner of ClevelandIndians), Bob Feller (former player for theCleveland Indians), Mark McCormack(former owner of IMG), and Jim Brown(former player for the Cleveland Browns).
F E L L O W S H I P N E W S
Fellowship MatchProgram ContinuesSmooth OperationDecember 1 was the deadline forapplicants for the Sports MedicineFellowship Match. We received atotal of 247 registered applicants. Thisnumber is comparable to the last twoyears. Of the 247 registered applicantsthis year, 35 of them are InternationalMedical School Graduates who aredoing a residency outside of the U.S.
Upcoming Key DatesMarch 25, 2011: Rank List Due to SF MatchOffices from both programs and applicants
April 11, 2011: Programs notified if they filled.Applicants notified if they did/did not match.
April 12, 2011: Match Day
N A M E S I N T H E N E W S
HOME
HOME
16 SPORTS MEDICINE UPDATE January/February 2011
AOSSM Specialty DayFebruary 19, 2011San Diego, California
12th Annual AAOS/AOSSMSports Medicine Course:Elite Athletes to Weekend WarriorsMarch 9–13, 2011Vail, Colorado
3rd Combined Meeting of theJapanese and American OrthopaedicSocieties for Sports MedicineMarch 26–29, 2011Maui, Hawaii
AOSSM 2011 Annual MeetingJuly 7–10, 2011San Diego, California
Annual AOSSM/AAOS Review Coursefor Subspecialty Certification inOrthopaedic Sports MedicineAugust 5-7, 2011Chicago, Illinois
For more informationand to register visitwww.sportsmed.org andclick on the “Educationand Meetings” tab.
JOSSM and AOSSM Collaborate for Upcoming MeetingAOSSM is collaborating with the Japanese Orthopaedic Society for Sports Medicine (JOSSM)for the 3rd Combined Meeting of the Japanese and American Orthopaedic Societies for SportsMedicine. The meeting will be held in English from March 26–29, 2011, at the Grand Wailea inMaui, Hawaii. It will feature noted faculty and scientific papers on the overhead throwing athleteand sports medicine. Robert Stanton, MD, AOSSM President noted, “the meeting is a replicationof a similar exchange between Japan and the U.S. in the early 1990s, and it affords AOSSMmembers a unique educational and cultural exchange in an unparalleled setting.”
Upcoming Meetings and Courses
HOME
HOME
Sports Medicine UpdateAOSSM6300 North River RoadSuite 500Rosemont, IL 60018
www.sportsmed.org
HOME
HOME