Embed Size (px)
Citation preview

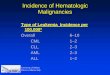
Slackers Guide to Hematologic Cancers
Mike Ori

Disclaimer
• These represent my understanding of the subject and have not been vetted or reviewed by faculty. Use at your own peril.
• I can’t type so below are common missing letters you may need to supply
• e r l• I didn’t use greek letters because they are a
pain to cut and paste in.

• What are the six hallmarks of cancer

• Evasion of apoptosis• Insensitivity to anti-growth signals• Self sufficiency of growth signals• Limitless replication potential• Sustained Angiogenesis• Tissue invasion and metastasis
• What is the Warburg effect

• It is the observation that cancer cells rely more heavily on glycolysis than on oxidative phosphorylation even in the presence of adequate oxygen supplies. Thus it is believed that the glycolysis is better suited to meet the metabolic demands of cancer cells.

• What is epigenetics • List a few epigenetic mechanisms in the cell

• Epigenetics refers to reversible but inheritable changes in gene expression that occur without mutations. Examples include– Methylation– Histone acetylation
• Both examples limit the access of promoter regions to their respective promoters.

• What is the function of micro RNA

• miRNA are small (~22bp) RNA strands that function at the post transcriptional level to silence specific genes. Each miRNA may interact with multiple genes and thus can serve as an off switch post transcriptionally.
• Some oncogenes control the expression of miRNA.

• What is mismatch repair?

• DNA replications “spell checker”. It makes sure A-T and G-C go together.

• What is Nucleotide excision repair

• Removal of pyrimidine dimers caused by UV radiation

• What is the function of p53

• P53 is a tumor suppressor gene.• It activates DNA repair genes• It can arrest the cell cycle at G1/S checkpoint• It can initiate apoptosis

• What is the function of ATM

• ATM is a tumor suppressor protein

• What is the function of Her2/neu/erb-b2

• An epithelial growth factor receptor whose gene is amplified in 25% of breast cancers.
• Self-sufficiency in growth signals

• What drug targets her2 and what is its mechanism

• Trastuzumab is a monoclonal antibody directed against her2/neu/Erb b2.
• It functions by binding to and disrupting erb b2

• What is BCR-ABL and how does it result in cancer
• BCR-ABL is a unique protein that from t(9:22) translocation that results in the fusion of the BCR promoter to the ABL tyrosine kinase in such a way that the kinase no longer requires a ligand for activation.
• ABL is a proliferative kinase that is active in hematopoietic cells
• Describe the role of B-catenin and APC in cancer

• B-catenin is a cell proliferation enzyme that is sequestered by APC.
• The deletion of one APC allele causes familial adenomatous polyposis, an autosomal dominant condition that predisposes to colon cancer in early adulthood
• Mutations in APC can lead to attenuated colon cancer forms

• What are the three benign types of lymphadenopathy

• Follicular– Expansion of B cells
• Paracortical– Expansion of T cells
• Sinus histiocytes– Surgical drainage
• What is the common gene involved with lymphoma translocation

• The heavy chain gene on CR14

• Why are immune cells susceptible to translocations?

• DNA cleavage is an important part of maturation of immune cells. This presents opportunity for abnormal joining.
• What is the etiologic classifications of lymphoma

• Translocations• Inherited– Downs, neurofibromatosis
• Viruses– HTLV, EBV, HHV-8
• Environmental agents• Iatrogenic– Radiation

• Describe the relationship of lymphoma and leukemia

• Lymphocytic leukemias evolve to lymphomas late. Similarly, lymphomas may transform into lymphocytic leukemias.
• Describe follicular lymphoma

• Common indolent lyphoma• Back to back follicles• T(14:18) BCL-2– Anti-apoptotic
• May transform into diffuse large cell lymphoma

• Describe diffuse large cell lymphoma

• Large round lymphocytes• Alterations in BCL-6– Germinal center formation disrupted

• Describe Burkitts Lymphoma

• Rapidly aggressive lymphoma• T(8:14) c-myc oncogene• Association with EBV• Starry sky pattern due to histiocytes

• Describe marginal zone lymphomas

• Associated with MALT in gut• Chronically inflamed tissue– H. pylori
• Indolent but may transform to diffuse B-cell

• Describe hodgkins lymphoma

• Common cancer of young adults• Orderly progression from local nodes to
spleen to liver to bone marrow• Reed-sternberg cells

• Describe Mycosis Fungoides

• T cell lymphoma– CD4+– Band like infiltrates in dermis
• Flat erythematous rash -> plaques -> tumor nodules• TX with local control early• Sezary syndrome– Widespread rash– Blood and lymph node involvement– Poor prognosis

• List the myeloid cells

• Granulocytes– Neutrophils– Eosinophils– Basophils
• Monocytes• Erythrocytes• Megakaryocytes

• Differentiate myeloproliferative neoplasms, myelodysplastic syndromes, and myelogenous leukemias

• MPN– Clonal proliferation of a myeloid precursor – Retains ability to mature– Effective hematopoiesis– Expansion of one or more related cell lines– Normal blast levels
• MDS– Clonal proliferation of myeloid precursors– Retains ability to mature– Ineffective hematopoiesis– Peripheral cytopenia– Elevated blasts account for < 20% of marrow
• Leukemia– Malignant neoplasms of the hematopoietic precursors– Blasts account for more than 20% of the marrow– Classified as acute or chronic depending on maturity of cells

• Describe the blood counts of leukemic patients

• In some instances there may be elevated counts and in some instances cytopenia may result.

• If a sample shows clonal origin, what does this imply?

• This strongly implies a dysplastic/neoplastic process. Excess growth hormones would affect all members of a lineage sensitive to the hormone.

• Why is BCR-ABL a favorable indicator in CML but not in AML

• The fusion products are similar but are not the same.
• Are auer rods present in ALL

• No. Auer rods are an AML finding.
• What are the two categories of acute lymphoblastic leukemia

• B cell• T cell

• What are the classic populations for ALL

• B cell – children• T cell – adolescent males as lymphoma

• What are the prognostic indicators for ALL

Favorable Unfavorable
Hyperdiploidy hypodiploidy
1-10 yo <1 or > 10 yo
WBC < 50x109 /L WBC > 50x109 /L
TEL-AML1 MLL, BCR-ABL, E2A-PBX1
Trisomy 4,10, or 17
Induction failure
CNS disease

• Describe the treatment terms for leukemia

• Induction– Therapy intended to reduce cancer cells to below
cytologic detection levels• Consolidation– Therapy intended to further reduce tumor cells
• Continuation– Maintenance therapy intended to insure
continued remission

• When would a stem cell transplant be considered in ALL

• 1st remission if poor prognostic factors• 2nd remission if < 1 year

• What is the cell of origin for chronic lymphocytic leukemia?
• 95% are B-cell• 5% are T cell

• What is the initial treatment for CLL

• Watchful waiting• 10% yearly transform to diffuse B-cell

• When would it be prudent to institute TX in CLL?

• Conversion to prolymphocytic or diffuse B cell lymphoma
• Worsening B symptoms• Progressive adenopathy or hepatosplenomegaly• Peripheral blood cytopenias• Recurring infections• Immune mediated complications such as hemolytic
anemia• Short doubling time of peripheral lymphocyte count
• List the myeloproliferative disorders

• Chronic Myelogenous Leukemia• Polycythemia Rubra Vera• Essential thrombocytosis• Primary myelofibrosis

• List several attractions of CML’s favorite city

• Philadelphia– Cheese steaks– Liberty bell– Independence hall– Eagles– http://www.phillyfunguide.com for more…who
knew ( I just realized knew is a funny word)

• What are the common clinical and lab findings in CML?

• WBC – count > 50k/ul– All forms increases
• RBC– Decreased
• Thrombocytosis• Splenomegaly

• What is the common genetic pathway altered in other myeloproliferative disorders

• JAK2

• Describe polycythemia vera

• Absolute increase in RBC’s but other lines may also be affected
• Platelets often 500,000/ul• Issues related to blood viscosity

• What is the most likely outcome of increased blood viscosity

• Thrombosis
• What is the treatment course for PV

• Watchful waiting• Blood letting– phlebotomy– Leeches– Cage matches • 16 references were cited on the Blood Letting wikipedia
page vs 93 references on the Professional Wrestling Match types page so I guess cage matches have more evidence. No chochrane reviews though.

• Describe essential thrombocytosis

• ET is an increase in thrombocytes that cannot be explained by any other cause
• Megakaryocytes have decreased need to growth factors and thus are increased in the marrow
• Platelet function may be poor.
• What is the primary risk with ET

• Abduction and probing
• Really, if you didn’t know it was thrombotic events, you are a slacker.

• Describe myelofibrosis

• Fibrous marrow • Primary– If no other reason established
• Secondary– Arises due to “burned out” marrow from CML or
PV• Extramedullary hematopoieis – Massive splenomegaly

• What drug is useful in decreasing WBC count in CML

• Hydroxyurea

• What is the most common pediatric leukemia and what is its survival rate

• ALL• 80% survival

• List the genetic changes in lymphoma
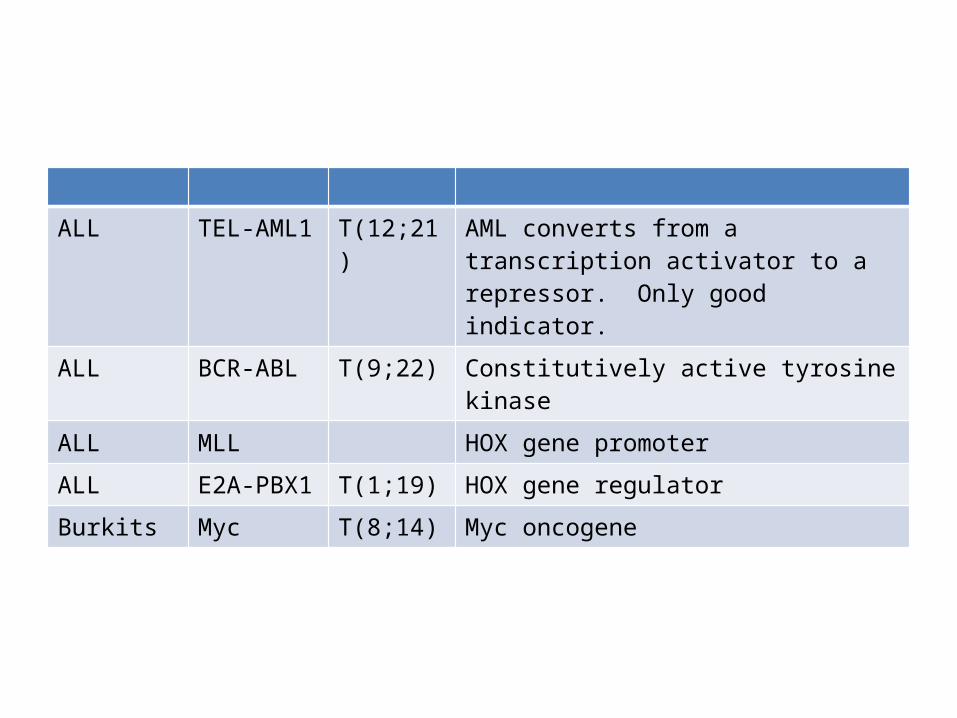
ALL TEL-AML1 T(12;21) AML converts from a transcription activator to a repressor. Only good indicator.
ALL BCR-ABL T(9;22) Constitutively active tyrosine kinase
ALL MLL HOX gene promoter
ALL E2A-PBX1 T(1;19) HOX gene regulator
Burkits Myc T(8;14) Myc oncogene

• What is the typical age of presentation for hodgkins vs non-hodgkins lymphoma

• Hodgkins = late 20’s• NHL = 60’s

• List the major risk factors for lymphoma

• Immunodeficiency– Acquired
• HIV, organ transplant
– Inherited• Autoimmune disease– RA, SLE, Sjogrens, Celiac
• Infection– Viruses
• HIV, EBV, HTLV, HEP C, HHV 8
– Bacteria• H pylori

• What are the B symptoms

• Drenching night sweats• FUO• Unexplained weight loss > 10%

• Describe the biopsy technique for suspected lymphoma
• Preferable is excisional biopsy of the suspected node. Otherwise need a core needle biopsy. Fine needle is insufficient

• List the Ann Arbor criteria for staging lymphomas

Stage
I Single lymph node region
II Multiple lymph node regions on same side of diaphragm
III Multiple lymph node regions across diaphragm
IV Extralymphatic non-contiguous involvement
SuffixB B sx present
A No B sx
E Extralymphatic
X Bulky
S Splenic

• What are the prognostic factors for lymphoma

• APLES• Age > 60• Performance status > 1• LDH > normal• Extra nodal sites > 1• Stage III/IV

• What are the risk factors for Non-hodkgins lymphoma
• WALSHAM• WBC > 15K• Albumin < 4 g/dl• Lymphocyte count < 600/ul• Stage IV• Hemoglobin < 10.5 g/dl• Age > 45• Male
• List the indolent, aggressive, and highly aggressive lymphomas

• Indolent– Follicular– Small lymphocytic– Marginal zone
• Aggressive– Diffuse large B-cell– Mantle cell
• Highly aggressive– Burkitts– Precursor B/T cell

• What is the treatment for indolent lymphoma

• Watchful waiting until– cytopenia– Leukemia– Marked splenomegaly, pelural effusion,
compressive symptoms– Single large node > 7cm– 3 nodes > 3cm

• What is the treatment for aggressive lymphoma

• R-CHOP• Rituximab• Cyclophosphamide• Doxorubacin• Vincristine• Prednisone

• What is the treatment regemin for non-hodgkin’s lymphoma

• ABVD• Doxorubicin• Bleomycin• Vinblastine• dacarbazine
• What is the signature side effect for doxorubicin

• CHF/cardiac toxicity• AML

• What is the principle side effect of vincristine

• Peripheral neuropathy• Constipation

• What is the principle side effect of bleomycin

• Pulmonary fibrosis

• Describe autologous stem cell transplant

• Autologous– From self– Risk of recurrence due to contamination or
continued gene defects– No graft v leukemia reaction– No graft v host reaction

• Describe syngenic stem cell transplant

• Syngenic– From an identical twin– No contamination with disease cells– Genetic defects remain– No graft v leukemia reaction– No graft v host reaction

• Describe allogenic stem cell transplant

• Allogenic– From another member of the species that is not
identical– No contamination with disease cells– Should not have similar genetic defects– Graft v leukemia reaction– Graft v host reaction

• What are the sources for stem cells

• Bone marrow aspirate• Cord blood• Peripheral blood– G-CSF– AMD3100 – allows stem cells to leave marrow

• When should SCT be considered

ALL
AML Allogenic 1st remission high risk, 2nd otherwise
CLL Allogenic or autologous
CML Allogenic After imatinib failure
NHL
Hodgkins Autologous
Myelodysplastic Syndroms
Allogenic If < 40yo and high risk
Multiple myeloma
Autotransplant
Most common reason for autotransplant

• What are the risk factors for prostate adenocarcinoma

• Age• Race• Family history• Diet• Cadmium exposure• Vasectomy (controversial)

• What are the screening tools for prostate cancer

• Digital rectal exam• PSA

• What is the staging for prostate cancer

• T1 – incidental finding• T2 – confined to prostate• T3 – outside of prostate capsule• T4 – Invading other pelvic structures

• Which patients should receive radiation therapy

Low riskT1-T2a
Radiation or radical prostatectomy
Medium riskT2b/c, PSA 10-20
Radiation if expected survival > 10 yearsHormone therapy
High riskT3, PSA > 20
RadiationHormone therapy

• Define initiation

• A mutation defect resulting in a phenotypically normal but altered cell.

• Define promotion

• The proliferation of a cell as a result of genetic changes occurring in initiation

• Define progression

• Acquisition of additional mutations in an initiated/promoted cell that confer more advanced neoplastic phenotype

• Describe tumorgenesis in skin cancer

• Cells are initiated by uv or other environmental insults. Over time promotion and progression occur until a frank tumor arises.

• What is the prevalence of basal cell carcinoma, squamous cell carcinoma, and malignant melanoma.

• BCC– #1 epithelial skin cancer– Low death rates
• Squamous cell carcinoma– #2 epithelial skin cancer– Low death rates
• Malignant melanoma– #3 skin cancer (?)– #1 in deaths (75%)

• Describe basal cell carcinoma

• Slow growing epithelial skin cancer with no known precursor lesion that is locally invasive and only rarely metastatic.
• Often translucent when stretched due to mucin (?)

• Where do BCC’s arise

• Keratinocytes associated with hair follicles

• What is the role of ptch1 in bcc

• Patch -----| smo ------> n-myc
• N-myc is a proliferative gene

• Describe grolin’s syndrome

• An inheritable defect in ptch1 that predisposes carriers to BCC

• What is the precursor lesion of squamous cell carcinoma

• Actinic keratosis

• Describe AK

• A rough, dry, scaly, red/brown patch on the skin.

• Describe the role of the immune system in SCC development

• The immune systems role is not well described but it plays some role as SCC increases with immune suppression and stimulation of the adaptive system is a treatment for both SCC and BCC.

• What are common genetic defects seen in SCC

• INK4a – a tumor suppressor is inactivated• P53 \/• Map kinase /\• NF-kB /\

• What is xeroderma pigmentosum

• A germline mutation in genes involved in nucleotide excision repair.
• Associated with increased levels of BCC and SCC

• Why is XP associated but not causative for BCC/SCC

• Uv is a major culprit in creating dimers that must be removed by excision repair. Therefore, if an XP patient were to limit their sunlight exposure, they limit their risk of developing SCC and BCC

• Why is malignant melanoma prone to metastasis?

• Melanoma arises from melanocytes which are of neural crest origin. These cells migrate widely in the developing embryo and its believed that this trait is re-emerges in cancer.

• What are the ABCD’s

• A tribute band to AC/DC– http://www.abcdband.com/
• Melanoma mnemonic – Asymmetry - asymmetrical– Borders - irregular– Color - uneven– Diameter - 6mm+

• What are the two phases of melanoma development and their prognosis
• Radial phase– Growth contained to the plane of the epidermis. – Curable with surgery alone
• Vertical phase– Growth perpendicular to the plane of the
epidermis resulting in invasion of the dermis and underlying tissue

• Explain the role of melanoma depth of invasion as a prognostic indicator

• Depth of invasion is inversely related to prognosis. In other words, deeper = deadlier.

• What is the role of growth factors in malanomagenesis

• Melanoma cells eventually gain self sufficiency in growth signals by producing their own fibroblast growth factor, a substance normally generated by keratinocytes.

• Once again, what is INK4

• A gene located on CR9 that is lost in 20-40% of melanomas. Hereditary melanomas are associated with loss of INK4A.
• A negative regulation of cell growth through the RB pathways

• What is the CDKN2A locus

• A critical locus on CR9 in that codes for INK4a and p14ARF. Both genes act as negative regulators of cell growth pathways.

• For no reason at all here’s Abu


• List the types of ultraviolet light

• UVA– Mildly carcinogenic– Photoaging
• Solar elastosis?
• UVB– Carcinogenic– Causes burns
• UVC– Highly carcinogenic– Blocked by ozone

• Are sunscreens protective for sundamage

• Sort of. SPF relates the amount of UVB blocked by a properly applied sunscreen. There is no current rating for blocking UVA and many sunscreens do not do so.
• Many people use sunscreens to extend the time they are in the sun thus effectively negating their benefit.

• What is the best therapy for malignant melanoma

• Early detection combined with excision.• Non-surgical interventions have poor
performance
• Proper prior planning prevents painfully poor performance.

• Make up your own sentence where every word begins with P.
• Perfectly posed purple plumed piccolo players piped prodigiously
• Pink penguins played peek-a-boo

• What are the histological hallmarks of melanoma

• Lack of maturation with descent• Single cells predominate over nests • Pagetoid appearance with migration upward
resulting in buckshot appearance
• Where would you typically expect to see superficial spreading malignant melanoma and what phase is it in

• On intermittently sunburned skin• Radial phase

• Where would you expect to see lentigo melanoma and what phase is it in

• On chronically sun damaged skin in the elderly• Radial phase

• What phase is nodular melanoma in

• Vertical• Can be rapidly fatal

• Where would you expect to find acral lentiginous melanoma and what phase is it in

• On darker skinned people on the palms, soles, and nails. Radial phase.

• What are the poor histologic factors for melanoma

• Thickness– > 1mm
• Ulceration• Vascular invasion• Microscopic satellites• Increased mitotic rate• Minimal lymphoid response• Partial regression