Embed Size (px)
Citation preview
Skin Tears
A Simplified Approach
By Joy Boyd RN BN
2013-01-26

Housekeeping
� Please mute your cellphones
� No financial input from industry sources

Skin Tears� This is a category llB tear (>25% flap lost)
ObjectivesBy the end of this session I hope you will be able: � To understand who is at risk, and why
� To know how to predict and prevent skin tears
� To do your own literature searches within the
educational databases to gain more knowledge
http://hinc.ucalgary.ca
� To identify, clean, classify, and dress skin tears
� To educate your colleagues (doctors too)
What? Skin Tear- Definition
� A traumatic wound occurring principally on the extremities of older adults as a result of friction alone, or shearing and friction forces which separate the epidermis from the dermis, or the epidermis/dermis from the underlying structures.[1]
Data� Skin tears occur more frequently than
pressure ulcers
� 1.5 million skin tears/year in U.S. in the institutionalized elderly
� 80% occur on arms, hands and anterior lower leg
[2,3]
Reporting Flaws
� True numbers of skin tears are unknown due to� Incorrect identification of skin tear [4]� Inadequate or non-existent classification tool,
system or documentation [4]� ER/UCC go unreported� Fault-based financial penalties
Who?� Premature neonates
� Elderly
� Any age with immunocompromised condition, skin diseases or taking steroids

Preemie Skin Tears
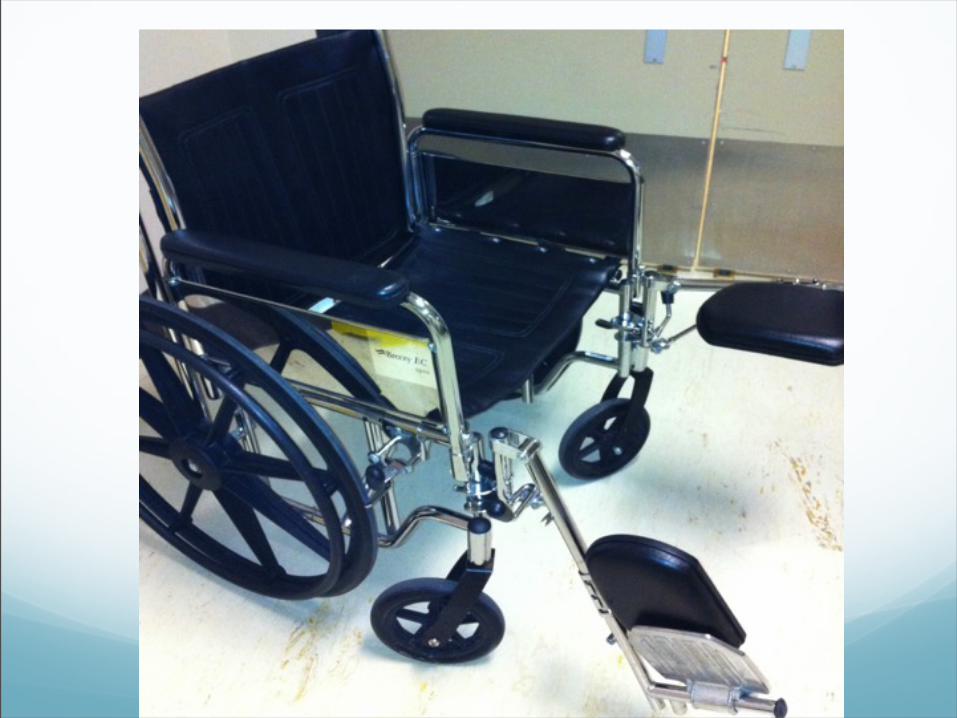
How?� 25% are wheelchair/walker injuries
� 25% are caused by bumping into objects
� 18% happen in transfers
� 12.4 from falls and stumbles
� Remainder from iatrogenic sources (rough handling, inappropriate tapes, fracture reductions, use of drying skin products etc) and violence/elder abuse [5]
WHY?� Intrinsic factors that predispose/predict
� Elderly > 75: fat, collagen atrophy, loss in skin infrastructure
� Female > male
� Caucasian
� Malnourishment
� Immunocompromised- steroids, cancer
� Cognitive impairment, mental disorders, agitative states
� Altered sensation (neuropathy, spinal cord)
� Polypharmacy- anticoagulants etc
� Comorbidities: cardiopulmonary, vascular conditions, edema
� Visual, hearing impairment
� Inability to reposition independently, immobility
� Ecchymosis or purpura; previous skin tears, skin lesions
� Limb/joint stiffness, paralysis or hemiparesis
� Gait and balance issues [6]

Bullous pemphigoid
Why? Continued
� Extrinsic factors that predispose/predict
� Using assistive devices (mechanical trauma)
� The hospital bed
� Self-propulsion
� Having blood drawn
� Dependence for activities (turning, applying stockings, bathing, clothing, transfers etc)
� Improper tape, EKG electrode, Tegaderm removal
� Hazards (footstools, rugs, pets, furniture crowding)
� Prosthetic devices (straps, belts, connectors, wear spots)
� Soap, skin and washing preparations that dry out the skin [7]
� Iatrogenic sources (HCW holding down demented pt), hurrying, and impatience
Pro-action and Prevention� Do risk assessment to identify the vulnerable
� Multi-disciplinary staff education on gentle handling
� Provide a safe environment
� Adequate lighting, esp at night
� Arm/leg sleeves
� Padded bedrails and projections on wheelchairs
� Arm/shin guards
� Space to walk or propel
� Remove hazards

Skin Tear Prevention Sleeve
Pro-action and Prevention continued
� Adequate nutrition and hydration
� Emollient soap and lotion
� Caution when handling, transferring, transporting, and repositioning
� Don’t wear high-profile rings or watches, keep your nails short
� Use lift sheets to prevent friction and shear
� Use pillows, wedges and other positioning devices
� Use non-adherent dressings
� Use new-generation tapes (3M silicone) and cover dressings
� Use skin prep with any paper tape, adhesive tape or film dressing [8]
Tape Choices
Skin Tear Treatment � Assess the wound and the patient
� Wound Cleansing- NO TOXIC CHEMICALS!
� Approximate the flap, then classify
� Best-Practice dressings [9]
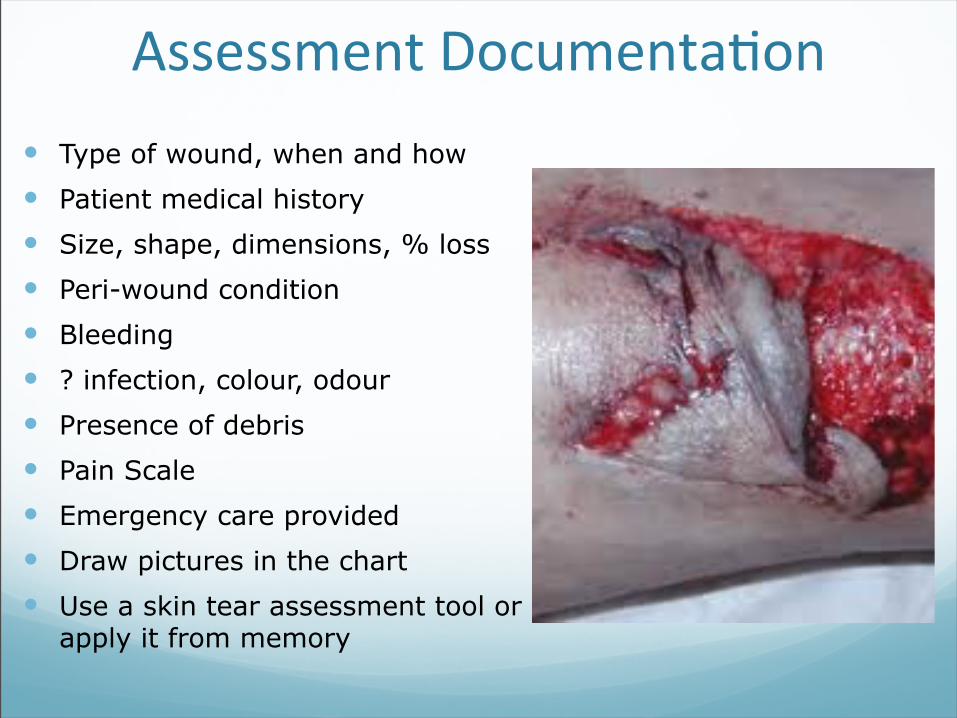
Assessment Documenta2on� Type of wound, when and how� Patient medical history� Size, shape, dimensions, % loss� Peri-wound condition � Bleeding� ? infection, colour, odour� Presence of debris� Pain Scale� Emergency care provided� Draw pictures in the chart� Use a skin tear assessment tool or
apply it from memory
Payne-Martin scale [10]
� Category lA- Linear type tear, epidermis and dermis pulled apart: no tissue loss
� Category lB- Flap completely covers the dermis to 1 mm of the wound margin
� Category llA- <25% loss of flap
� Category llB- >25% loss of flap
� Category lll- Epidermal flap is absent
Ini2al Dressings at Triage
� No dry gauze directly on wound!
� If medics have applied dry gauze, remove it and replace with a wet saline gauze or pour normal saline on the existing dressing. [12]
Pause Before You Use Gauze![11]
Wound Cleansing: What to use?� Normal saline (best)� Commercial Wound Cleanser� Tap water� Sterile water [13]
Gentle wound cleanser
Contains a non-ionic surfactant
Non-toxic, non-irritating
Currently on AHS contract
Non-‐chemicalized spongebrush
Avoid these products on/in wounds(Can be toxic locally and systemically) [14,15,16,17,18,19,20,21]
� Iodine as liquid, ung., gauze, is cytotoxic, thyrotoxic, nephrotoxic
� Chlorhexidine in 2% and 4% is cytotoxic, impedes healing
� Alcohol burns open tissues� Hydrogen peroxide is cytolytic, can cause oxygen emboli� Bleach solutions (Dakin’s) - cytotoxic� Vinegar is acetic acid - cytotoxic� Or any other toxic agents� Chlorhexidine and iodine are for intact skin only
Iodine � Is irritating to tissues and skin
� Is painful in open wounds
� Is deactivated by exudate (bioburden)
� Is inhibitive to healing
� Can cause allergic reaction
� Fumes are harmful
� Embolizes in bleeding wounds, thyrotoxic and nephrotoxic [22,23]
Recent Literature on Chlorhexidine� More research is needed to determine safe %.
Product in even very low concentrations (.02%) has been found to be effective in killing microbes [24]
� Impedes granulation tissue
� Decreases tensile strength of healing tissue [18]
� The topical antiseptic 2% containing alcohol should not be used on open wounds (intact skin only)
� If the physician insists on using Chlorhexidine, rinse the wound with sterile water, NOT NORMAL SALINE
Chlorhexidine
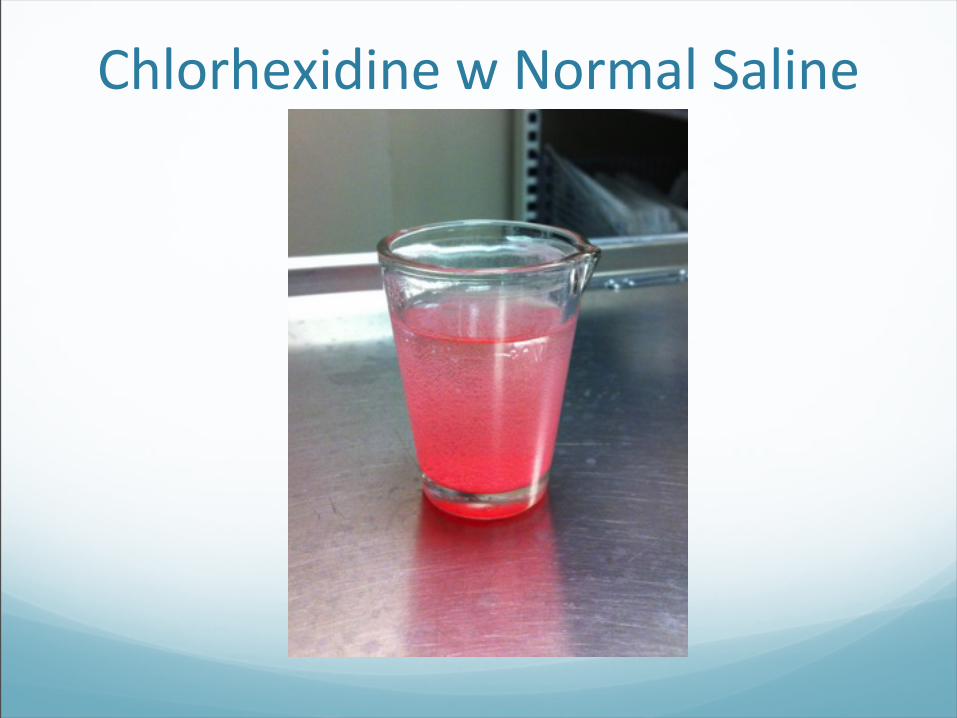
Chlorhexidine w Normal Saline
Precipitate
Dressings � Tegaderm Absorbent (Cavilon prep)
� Mepitel/Tegaderm (Cavilon prep)
� Aquacel/Aquacel Ag/ Tegaderm (Cavilon prep)
� Mepilex foam
� Dermabond skin glue
� Steri-strips
� Surgicel

‘Gauzed’ Skin Tear
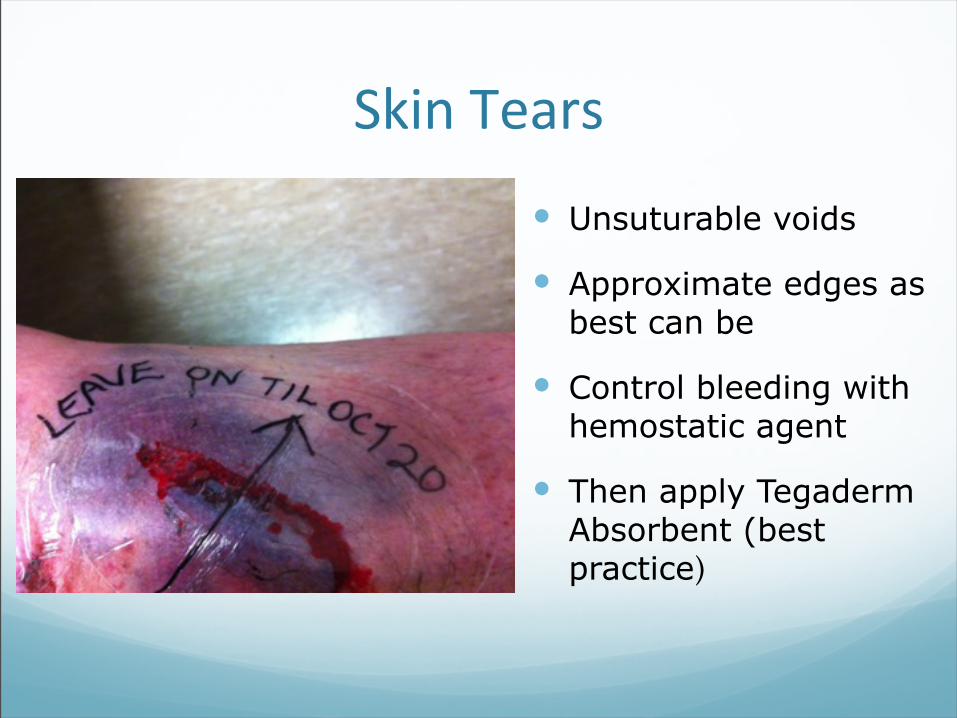
Skin Tears
� Unsuturable voids
� Approximate edges as best can be
� Control bleeding with hemostatic agent
� Then apply Tegaderm Absorbent (best practice)
Moisture Retention
Facilitating Wound Healing� We need to help the body heal itself
� Body likes moisture, skin holds moisture in� Moisture helps decrease pain, facilitates cell
reproduction and migration
� We can help with temperature control and moisture retention by using dressings with these characteristics to provide a “second skin”, and avoiding gauze on the wound bed
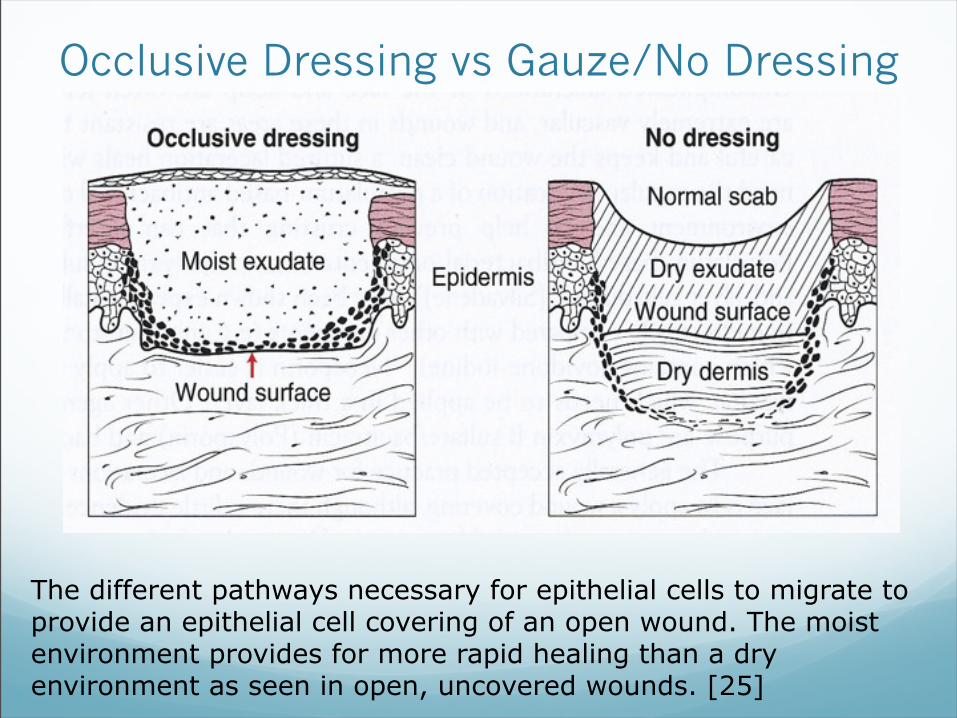
Occlusive Dressing vs Gauze/No Dressing
The different pathways necessary for epithelial cells to migrate to provide an epithelial cell covering of an open wound. The moist environment provides for more rapid healing than a dry environment as seen in open, uncovered wounds. [25]
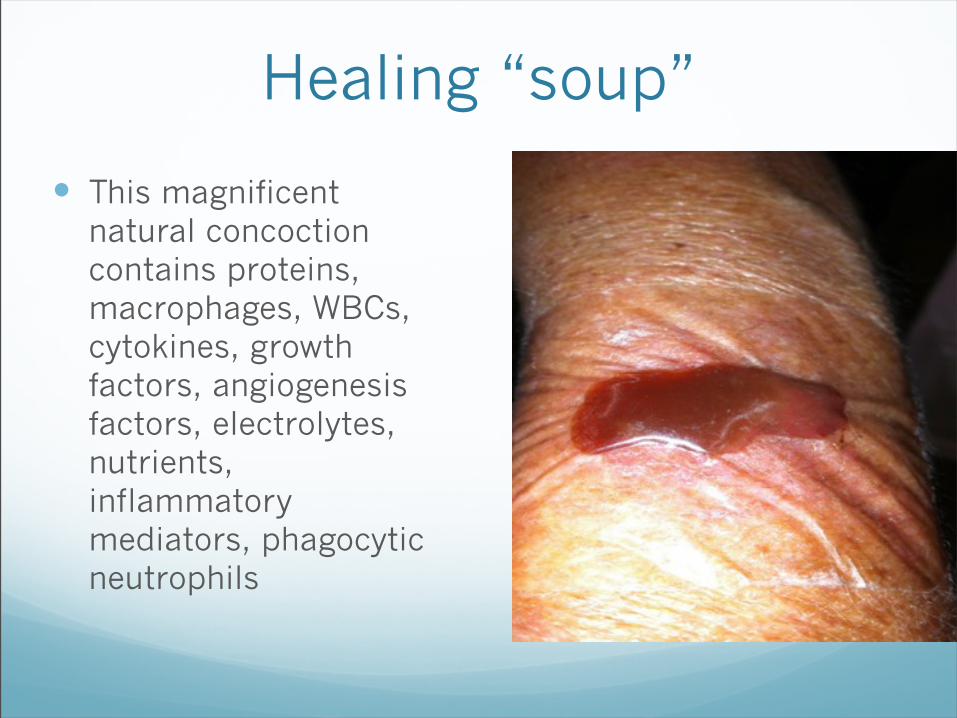
Healing “soup”
� This magnificent natural concoction contains proteins, macrophages, WBCs, cytokines, growth factors, angiogenesis factors, electrolytes, nutrients, inflammatory mediators, phagocytic neutrophils

After shot
� Eight days after immersion in the fluid matrix, the wound is fully re-epithelialized.
� Still fragile and remodelling for a year
� Susceptible to re-injury
The “Ideal” Dressing� Removes excess exudate & toxins� Maintains high humidity at the dressing-wound
interface� Allows for gas exchange� Provides thermal insulation� Protects against secondary infection� Is free from particulate & toxic components� Produces no trauma with removal� Obliterates dead space� Allows pt to shower� Cost effective [28]
Simple Dressing Choices for ERCombina2ons can enhance healing
� Silicone non-stick� Hydrofibre gels with and without silver� Films with and without islands� Hemostatic agents� Semi-adherents� Glue� Foams with and without silver� Skin preps� Tapes and Covers

Skin Tear with Surgicel
Surgicel in 50% void
Dermabond® Topical Skin Adhesive
Ideal for
� Wounds in areas where skin is not stretched or pulled
� Exterior, hair-free areas
� Face, but not too close to the eye
(and not the mouth!)
Steri-Strips� Used less often now
that new-technology dressings are available
� Are still effective
� Must be applied with no traction to avoid shearing
� Use with Cavilon skin prep to prolong wear time
Benefits of Extended Wear-Time Dressings
� Faster healing
� Pleasing cosmetic appearance of scar
� Decreases:� Pain and stress� Trauma to wound bed and periwound skin� Infection� Visits to MD or hospital ER/UCC� Home care visits� Wound specialist referrals� Antibiotic use� Costs of medical supplies/ dressings
How to heal a skin tear� Don’t use toxic chemicals to clean the wound. They
impede healing� Approximate the edges of the wound if possible� Use dressings that have moist technology� Use non-adherents with a waterproof outer layer� Use film dressings to enable surveillance of healing;
and in dementia pts� Use periwound prep to protect the skin� Optimize intrinsic barriers to healing � NO DRY GAUZE directly on a wound� Stop serial voyeurism (use non-disturbance long-term
regimen)

We Don’t Want This
Removing Tegaderm� Pull the membrane sideways to disengage it from
skin. Use your thumb to press along the path of removal as it teases off the skin
� Do NOT peel it back, as this causes pain.
� Remove in the direction of the skin tear flap, not against it
� Note: Use of Cavilon prep to protect the skin before application will make the removal of Tegaderm less traumatic
Outpatient Dressings
� Condition of patient� Location of wound� Access to help� Frequency of dressing change� Ease of dressing use� Condition of peri-wound area� Bathing/showering � Pain control medications� Pre-existing infections� Compliance� Costs
Final Documentation
� Treatment (cleansing, closure, etc.)
� Dressing(s) and preps used
� Meds given
� Tetanus/diphtheria prn
� Discharge teaching/sheets
� Referrals
Beware of ‘polysporin and gauze dressing’ order!Now that you are bePer informed, be an advocate for
appropriate dressing choices.
Spread the word ! [26,27]
Thank YouFor the opportunity to educate you about acute wound therapy in the 21st Century. The knowledge has been difficult to disseminate especially in those health professionals still entrenched in 19th Century thinking. We have come a long way in wound care research, in the fields of toxic cleansers, cleansing techniques, dressing products and associated technologies and treatments. So I need YOU to teach, inform, be role models and patient advocates in the practice of safe, current wound care modalities.
Questions?Thank you for attending.
Please complete the evaluation sheet, as feedback is important for improvement.
Contact:
Downloads at:
http://www.notitia.com/acutewoundcare.html
References� 1. Payne RL, Martin ML. Defining and classifying skin tears: need for a common language. Ost Wound Man.
1993:93:3, 16-20, 22-24,26.
� 2. Carville K, Lewin G, Newall N et al. STAR: a consensus for skin tear classification. Prim Intent 2007: 15(1): 18-28
� 3. Malone et al. JAGS 1991,39 (6), 591-5.
� 4. Leblanc K, Baranoski S, Regan M. International 2010 Skin Tear Survey (unpublished data) January 2011.
� 5. Baranoski S. Skin tears: Guard against this enemy of frail skin. Nurs Management 2001;32:25-32.
� 6. Leblanc, K, Christensen D, Orsted H, Keast D. Best Practice Recommendations for the prevention and treatment of skin tears. Wound Care Canada. 2008: 6(1):14-30.
� 7. Frantz RA, Gardner S. Clinical concerns: management of dry skin. J Gerontol Nurs. 1994:20(9):15-18,45.
� 8. O’Regan A. Skin Tears: a review of the literature. World Counc Enterostomal Ther J. 2002:22(2):26-31
� 9. Sibbald G, Orsted H, Coutts P, Keast D. Best practice recommendations for preparing the wound bed: update 2006. Wound Care Canada 2006:4(1):19-29.
References continued
� 10. Payne RL, Martin ML. Defining and classifying skin tears: need for a common language. Ost Wound Man. 1993:93:3, 16-20, 22-24,26.
� 11. Convatec educational material poster 2009.
� 12. Sussman C, Bates-Jensen BM. Wound Care: A collaborative practice manual for Health Professionals. Lippincott, 2007, p. 251.
� 13. Dulecki M, Pieper B. Irrigating simple acute traumatic wounds: a review of the current literature. Jour Emergency Nursing 2005 April.
� 14. Kanakiriya S, De Chazal I, et al. Iodine toxicity treated with continuos venvenous hemodiafiltration. Am J Kidney Dis 2003: 41(3): 702-708
� 15. Naznin M Dixit. Transient hypothyroidism in a breastfed infant whose mother had a perirectal abscess packed with iodoform gauze. Sciencestage.com/d/17700179.
� 16. Brown CD, Zitelli JA. A review of topical agents for wounds and methods of cleansing. J Dermatol Surg Oncol 1993;19: 732-7.
� 17. Oberg MS, Lindsey D. Do not put hydrogen peroxide or povidone iodine on wounds. AJDC 1987: 141: 27-8.
� 18. Cooper ML, Laxer JA, Hansbrough JF. The cytotoxic effects of commonly used topical antimicrobial agents on human fobroblasts and keratinocytes. J Trauma 1991: 31(6): 715-84.
References continued
� 19. Gilchrist B. Should iodine be reconsidered in wound management? European Tissue Repair Society. J Wound Care 1997: 6(3): 148-50
� 20. Brennan SS, Foster ME, Leaper DI. Antiseptic toxicity in wounds healed by secondary intention. J Hosp Infect. 1986; 8: 263-67
� 21. Haller E, Faltin-Traub D, Faltin C, Kern C. Oxygen embolism after hydrogen peroxide irrigation of a vulvar abscess. Br Jour of Anaesthesia. 2002: 88(4): 597-599.
� 22. Aronoff GR, Friedman S, et al. Transcutaneous iodine absorption. Am J Med Sci 1980: 279(3): p. 173.
� 23. D’Auria J, Lipson S, Garfield JM. Fatal iodine toxicity following surgical debridement of a hip wound; case report. J Trauma 1990; 30(3): p. 353.
� 24. Chlorhexidine in Healthcare: Your questions Answered, by Laura Stokowski, RN, Medscape. January 2011 at http://www.medscape.com/viewarticle/726075.
� 25. Wounds and Lacerations: Emergency Care and Closure, 3rd edition. Alexander T. Trott, MD. 2005. Elsevier Mosby.
� 26. Moodabe K, Bryant, L. Topical Antibiotics-More Harm than Good? http://www.rnzcgp.org.nz/assets/documents/Publications/Archive-NZFP/Oct-2000-NZFP-Vol-27-No-5/NZFP-OCT2000-Moodabe-Topical-antibiotics.pdf
� 27. Goodnow M. The Technic of Nursing. 3rd edition. Philadelphia: Saunders, 1935 p. 337.
� 28. DermNetNZ. Dressings: the ideal dressing. www.dermnetnz.org.