Embed Size (px)
Citation preview

www.mghcme.org
Skin Signs of Rheumatic DiseaseGideon P. Smith MD PhD MPH
Vice Chair for Clinical Affairs Director of Rheumatology-Dermatology ProgramDirector of Connective Tissue Diseases Fellowship
Associate Director of Clinical Trials Department of Dermatology
Massachusetts General HospitalHarvard University

www.mghcme.org
Disclosures
“Neither I nor my spouse/partner has a relevant financial relationship with a
commercial interest to disclose.”

www.mghcme.org
CONNECTIVE TISSUE DISEASES CLINIC
•Schnitzlers
•Eosinophilic Fasciitis
•Silicone granulomas
•AML arthritis with
granulomatous papules
•Follicular mucinosis in
JRA post-infliximab
•Calcinosis, small and
exophytic
•NSF, Morphea
•EED, PAN, DLE
•Interstitial
Granulomatous
Dermatitis with
Arthritis
•Cutaneous Crohn’s
with arthritis
•Acral Anetoderma
Lupus
•TNF-alpha induced
sarcoid
•Multicentric Reticul
ohistiocytosis
•Chondrosarcoma
induced
Dermatomyositis
•Scleroderma
•Lyme arthritis with
papular mucinosis
•Celiac
•Granulomatous
Mastitis
•IgG4 Disease

www.mghcme.org
Common consults• Primary skin disease recalcitrant to therapy
• Hair loss• Nail dystrophy• Photosensitivity• Cosmetic concerns – post-
inflammatory pigmentation, scarring, volume loss, premature photo-aging
• Erythromelalgia• Dry Eyes• Dry Mouth• Oral Ulcerations• Burning Mouth Syndrome• Urticaria• Itch• Raynaud’s• Digital Ulceration• Calcinosis cutis

www.mghcme.org
Todays Agenda
Clinical Presentations
Rashes(Cutaneous Lupus vs Dermatomyositis vs ?)
Hard Skin(Scleroderma vs Other sclerosing disorders)
www.mghcme.org
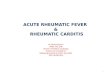
Case 1: Is this Lupus?

www.mghcme.org
Common Mimickers

www.mghcme.org
Common Mimickers

www.mghcme.org
ContactDermatitis

www.mghcme.org
ContactDermatitis
exudativegeometricID reaction

www.mghcme.org
Common Mimickers

www.mghcme.org
Seborrheic Dermatitis
• Greasy scale, often nasolabial fold prominence
• Sternum, under arms, inguinal folds

www.mghcme.org
Common Mimickers

www.mghcme.org
Rosacea

www.mghcme.org
Common Mimickers

www.mghcme.org
Dermatomyositis

www.mghcme.org
Dermatomyositis vs Lupus
• A lot of similarities
– Photosensitive
– Often Facial involvement
– +/- ANA
– +/- systemic symptoms

www.mghcme.org
Dermatomyositis: A Clinicopathological Study of 40 PatientsSmith, Edward S MD*; Hallman, James R MD†; DeLuca, Amena M BS‡; Goldenberg, Gary MD§; Jorizzo, Joseph L MD*; Sangueza, Omar P MD†American Journal of Dermatopathology: February 2009 - Volume 31 -
Issue 1 - pp 61-67
• Ten biopsy specimens each of DM and SLE (matched for anatomical site and lesion morphology) were randomized.
• Blinded histopathologic diagnosis (DM versus SLE) by expert academic dermatopathologists
• The correct histopathologic diagnosis of DM or SLE was made in 11 of the 20 skin biopsies without clinical information.

www.mghcme.org
So what are the Differences?
Lupus Dermatomyositis

www.mghcme.org
Acute Cutaneous Lupus

www.mghcme.org
Malar Rash

www.mghcme.org
Malar Rash

www.mghcme.org

www.mghcme.org
Malar Rash

www.mghcme.org

www.mghcme.org

www.mghcme.org
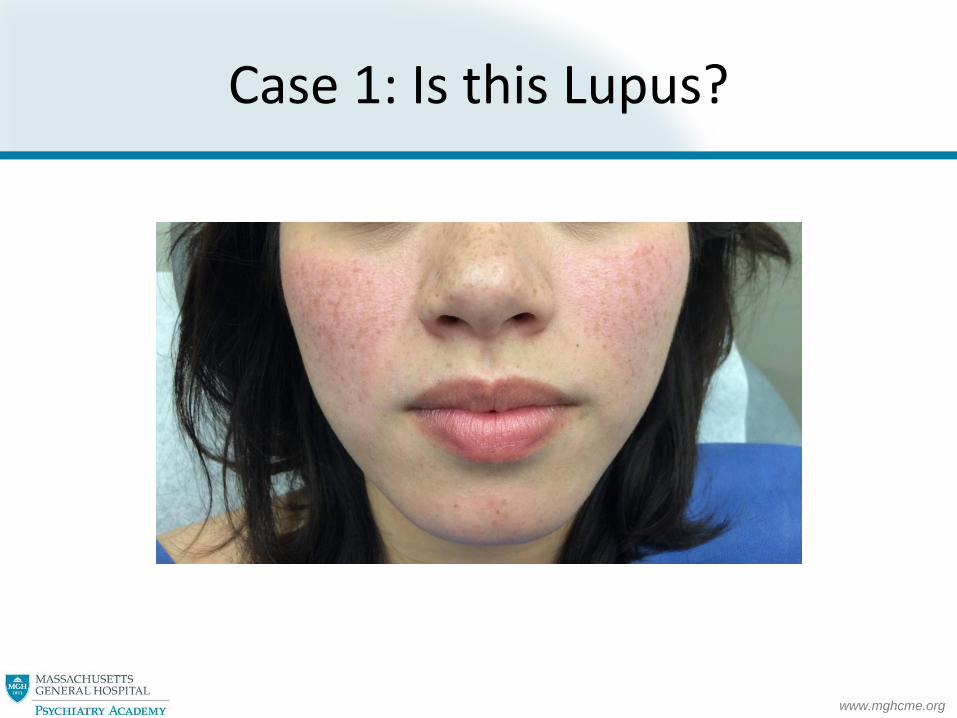
Any other cutaneous clues?

www.mghcme.org

www.mghcme.org

www.mghcme.org

www.mghcme.org

www.mghcme.org
www.mghcme.org

www.mghcme.org
Nailfold Capillaroscopy

www.mghcme.org
Nailfold Capillaroscopy

www.mghcme.org
Nailfold Capillaroscopy

www.mghcme.org
Nailfold Capillaroscopy

www.mghcme.org
Lupus Dermatomyositis
Malar rash spares nasolabial folds Facial Rash enters nasolabial folds
Rare calcinosis Microcalcifications actually common
Nailfolds largely normal Capillaries often chaotic re-angiogenesis

www.mghcme.org
CASE 2

www.mghcme.org
SCLE
• Annular
• Psoriasiform

www.mghcme.org
SCLE

www.mghcme.org
Dermatomyositis

www.mghcme.org
Not much scale; Ruddy; Telangiectasias

www.mghcme.org
Dermatomyositis

www.mghcme.org
Dermatomyositis

www.mghcme.org
Lupus Dermatomyositis
Malar rash spares nasolabial folds Facial Rash enters nasolabial folds
Rare calcinosis Microcalcifications actually common
Nailfolds largely normal Capillaries often chaotic re-angiogenesis
Hand rash between joints Hand rash joints
Rash light pink Rash darker due to capillary component
Malar and photodistributed Scalp, eyelids, hips, back

www.mghcme.org
Photosensitivity SLE vs DM
Goreshi R, Chock M, Foering K, Feng R, Okawa J, Rose M, et al. Quality of life in dermatomyositis. J Am Acad Dermatol. 2011;65(6):1107-16.

www.mghcme.org
Pruritus SLE vs DM
Goreshi R, Chock M, Foering K, Feng R, Okawa J, Rose M, et al. Quality of life in dermatomyositis. J Am Acad Dermatol. 2011;65(6):1107-16.

www.mghcme.org
Pruritus SLE vs DM
Goreshi R, Chock M, Foering K, Feng R, Okawa J, Rose M, et al. Quality of life in dermatomyositis. J Am Acad Dermatol. 2011;65(6):1107-16.

www.mghcme.org
Pruritus SLE vs DM
Goreshi R, Chock M, Foering K, Feng R, Okawa J, Rose M, et al. Quality of life in dermatomyositis. J Am Acad Dermatol. 2011;65(6):1107-16.

www.mghcme.org
Lupus Dermatomyositis
Malar rash spares nasolabial folds Facial Rash enters nasolabial folds
Rare calcinosis Microcalcifications actually common
Nailfolds largely normal Capillaries often chaotic re-angiogenesis
Hand rash between joints Hand rash joints
Rash light pink Rash darker due to capillary component
Malar and photodistributed Scalp, eyelids, hips, back
Pain/burning > itch Itch > pain

www.mghcme.org
Hair

www.mghcme.org
Lupus Hairs

www.mghcme.org

www.mghcme.org
PASTE
• P – plugging
• A – Atrophy
• S – Scale
• T – Telangiectasias
• E – Erythema

www.mghcme.org

www.mghcme.org
Dermoscopy DLE

www.mghcme.org
Dermoscopy DLE

www.mghcme.org
Lupus Dermatomyositis
Malar rash spares nasolabial folds Facial Rash enters nasolabial folds
Rare calcinosis Microcalcifications actually common
Nailfolds largely normal Capillaries often chaotic re-angiogenesis
Hand rash between joints Hand rash joints
Rash light pink Rash darker due to capillary component
Malar and photodistributed Scalp, eyelids, hips, back
Pain/burning > itch Itch > pain
Hairloss patchy Hairloss diffuse

www.mghcme.org
Summary Differences
Lupus Dermatomyositis
Malar rash spares nasolabial folds Facial Rash enters nasolabial folds
Rare calcinosis Microcalcifications actually common
Nailfolds largely normal Capillaries often chaotic re-angiogenesis
Hand rash between joints Hand rash joints
Rash light pink Rash darker due to capillary component
Malar and photodistributed Scalp, eyelids, hips, back
Pain/burning > itch Itch > pain
Hairloss patchy Hairloss diffuse
www.mghcme.org
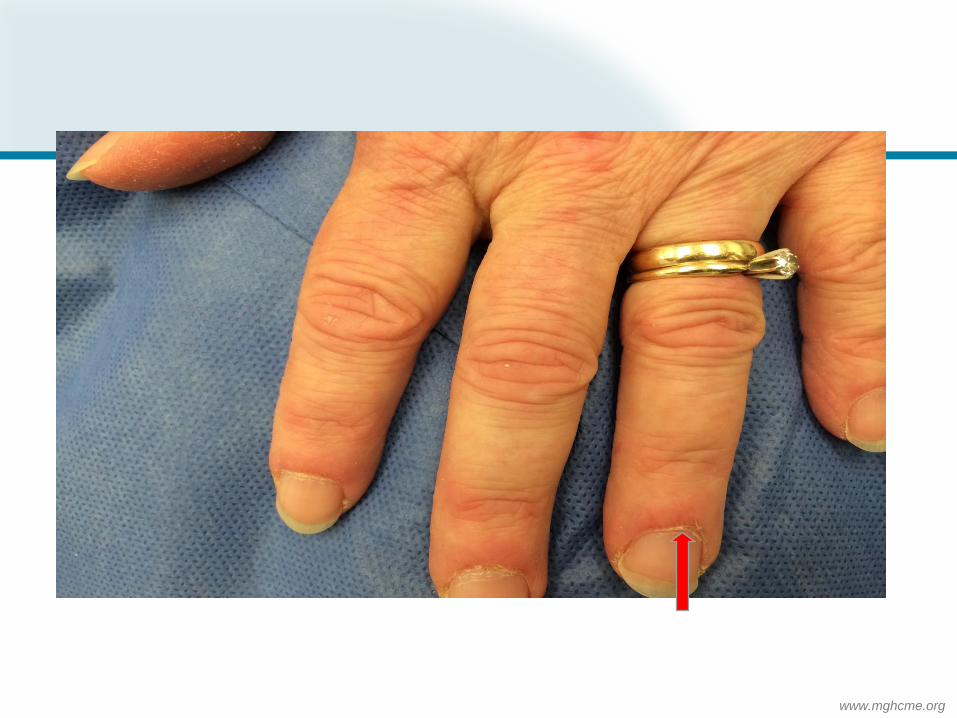
Is it scleroderma?

www.mghcme.org
RAYNAUD’S ‘WHITE’

www.mghcme.org
RAYNAUD’S ‘BLUE’

www.mghcme.org
lSSc dSSc
NOTE DISTRIBUTION

www.mghcme.org
Puffy Fingers of dSSc

www.mghcme.org
Puffy Fingers of dSSc

www.mghcme.org
Nailfold Capillaroscopy

www.mghcme.org
Nailfold Capillaroscopy

www.mghcme.org

www.mghcme.org
Matted Telangiectasias
• More often in patients with limited disease/CREST
• Common on cheek, lips

www.mghcme.org
Matted Telangiectasias
• Common on palms

www.mghcme.org
Pterygium Inversum

www.mghcme.org
Note Distribution
Morphea LS and A

www.mghcme.org
Morphea LS and A
NOTE DISTRIBUTION

www.mghcme.org
Clinical Features: Plaque Type
• Most common variant
• peripheral violaceous ‘lilac’ ring

www.mghcme.org
Clinical Features: Plaque Type
• Central area transforms into sclerotic, shiny white tissue

www.mghcme.org
Clinical Features: Plaque Type
• Central area transforms into sclerotic, shiny white tissue

www.mghcme.org
Clinical Features: Plaque Type
• Once burnt out post-inflammatory hyperpigmentation common over sclerosis
• Hair and sweat glands frequently lost
• Pruritus from xeroderma

www.mghcme.org
Clinical Features: Plaque Type
• Once burnt out post-inflammatory hyperpigmentation common over sclerosis

www.mghcme.org
Can Koebnerize
Can koebnerize into areas of friction or other inflammatory disorders eg eczema as here

www.mghcme.org
Can koebnerize into areas of friction or other inflammatory disorders eg eczema as here
Can Koebnerize

www.mghcme.org
Variation in Appearance
• Can look very different in different skin types
• Still with loss of adnexal structures (no hair, dryer, more PIH)

www.mghcme.org
Variation in Appearance
• Can look very different in different skin types
• Still with loss of adnexal structures (no hair, dryer, more PIH)

www.mghcme.org
Scleredema Early Scleromyxedema
NOTE DISTRIBUTION

www.mghcme.org
Scleredema Scleromyxedema
NOTE DISTRIBUTION

www.mghcme.org
Eosinophilic
Fasciitis
Nephrogenic Systemic
Fibrosis
NOTE DISTRIBUTION

www.mghcme.org
Clinical Appearance

www.mghcme.org
Clinical Appearance

www.mghcme.org
Clinical Appearance
Arm

www.mghcme.org
“Groove sign”: linear depression overlying
vein

www.mghcme.org
“Groove sign”: linear depression overlying
vein

www.mghcme.org
Symmetric and spares hands, feet, face

www.mghcme.org
When Thinking Sclerosis Disorders
• LOOK AT THE HANDS
– Sclerosis or Puffiness?
– True Raynaud’s?
– Capillary Changes?
– Telangiectasias?
– Calcinosis
– Pterygium Inversa?
• LOOK AT THE DISTRIBUTION

www.mghcme.org
Thank you!