Embed Size (px)
Citation preview
13
Skin Graft Preservation
Liangpeng Ge1, Zhenggen Huang2 and Hong Wei3
1Chongqing Academy of Animal Sciences 2Northern Hospital
3Third Military Medical University China
1. Introduction
Skin transplants have long been of interest to plastic surgeons for the treatment of burns and
other wounds. Skin transplants provide a better micro-enviromental for wound healing and
provide physiological barrier which greatly decreases water, electrolyte, protein and heat
loss through the wound. However, skin grafts are not always available in adequate
quantities for the complete duration of treatment, making skin graft preservation important
in meeting the need for skin transplantation.
This chapter highlights progress in the field of skin graft preservation including basic
knowledge of skin preservation, harvesting, processing and preservation, and quality
control methods and is intended to provide a reference for skin preservation techniques for
doctors and researchers.
2. Thermal physics of skin low-temperature preservation
The low-temperature preservation with viable cells and tissues is a complicated procedure,
which needs to undergo multiple processes including pretreatment, freezing, preservation
under low temperature and thawing in proper order. In these processes, there is
unavoidably evident change in the functions and morphology of the tissues. An ideal
preservation procedure should be that viable cells and tissues can restore to the original
functions and morphology prior to preservation after undergoing all of these processes and
then be used for grafting and other purposes like fresh cells and tissue. So far, the effect of
low-temperature preservation does not meet the above ideal conditions. Also, doctors and
researchers are not fully aware of the change in viable tissue in the preservation processes,
especially in the processes of freezing and thawing.
Water occupies a considerable proportion ofviable cells and tissues. The moisture content of
skin is about 70%. The quality of skin is closely related to the phase transition of water
during low-temperature preservation, which including the solidification in freezing,
ebullition in freezing of viable tissue using liquid nitrogen, thawing during freezing and so
on.
Water or water vapor can generate more than 10 kinds of solid phase structure,
nevertheless, most of them need to be formed under high pressure environment (at least 200
million Pascal′Mpa″), and only hexagonal ice, cube ice or amorphous ice can be
www.intechopen.com
Skin Grafts – Indications, Applications and Current Research
160
generated under low pressure. Water vapor deposits on a cold surface within the
temperature range from 0襖 slightly below to about -80襖, or forms a hexagonal symmetric
ice crystal in a suspended state in the air, snow is a typical case in point, and cubic crystal
with diamond structure will be generated under lower temperature (about -80襖~-130襖)
and amorphous solid (also called glassy, vitrification) will be formed below -140襖. Liquid
water usually only forms a hexagonal symmetric ice crystal upon freezing, however,
solutes-bearing water solution more easily realizes vitrification upon freezing compared
with pure water. Therefore, some components shall be added before freezing, in order to
promote the suspension of cells or tissues to more easily reach vitrification (Zhu et al.,
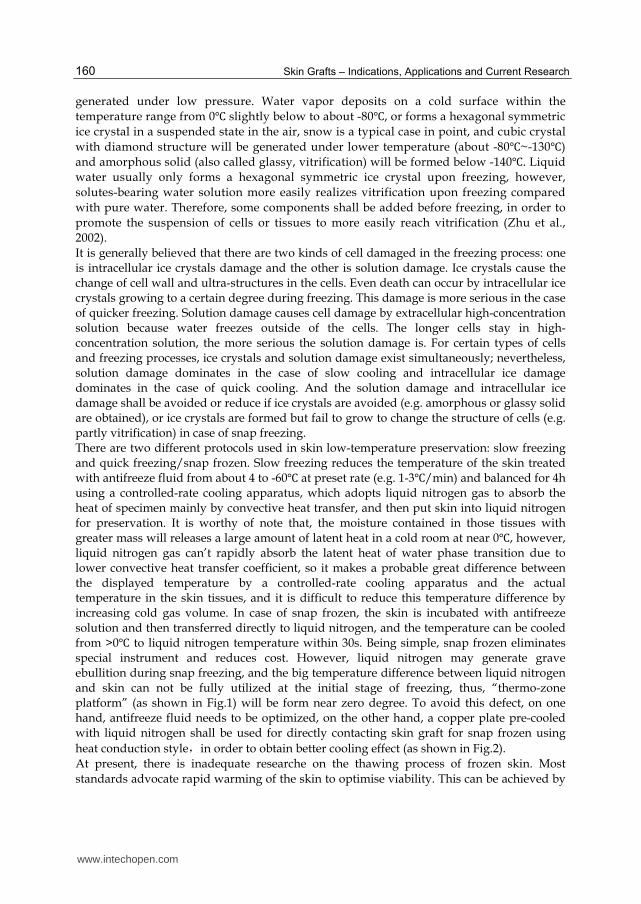
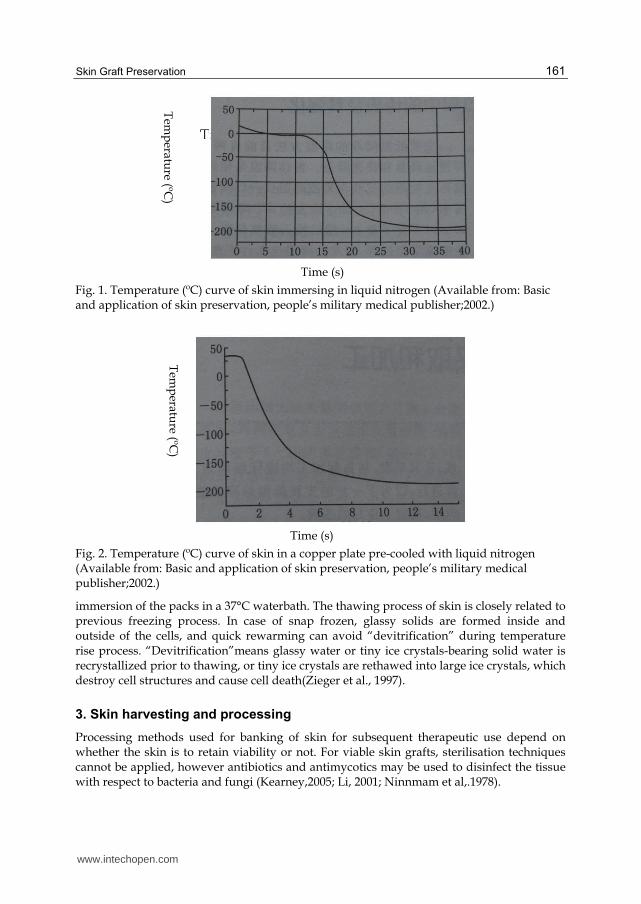
2002). It is generally believed that there are two kinds of cell damaged in the freezing process: one is intracellular ice crystals damage and the other is solution damage. Ice crystals cause the change of cell wall and ultra-structures in the cells. Even death can occur by intracellular ice crystals growing to a certain degree during freezing. This damage is more serious in the case of quicker freezing. Solution damage causes cell damage by extracellular high-concentration solution because water freezes outside of the cells. The longer cells stay in high-concentration solution, the more serious the solution damage is. For certain types of cells and freezing processes, ice crystals and solution damage exist simultaneously; nevertheless, solution damage dominates in the case of slow cooling and intracellular ice damage dominates in the case of quick cooling. And the solution damage and intracellular ice damage shall be avoided or reduce if ice crystals are avoided (e.g. amorphous or glassy solid are obtained), or ice crystals are formed but fail to grow to change the structure of cells (e.g. partly vitrification) in case of snap freezing. There are two different protocols used in skin low-temperature preservation: slow freezing and quick freezing/snap frozen. Slow freezing reduces the temperature of the skin treated with antifreeze fluid from about 4 to -60襖 at preset rate (e.g. 1-3襖/min) and balanced for 4h using a controlled-rate cooling apparatus, which adopts liquid nitrogen gas to absorb the heat of specimen mainly by convective heat transfer, and then put skin into liquid nitrogen for preservation. It is worthy of note that, the moisture contained in those tissues with greater mass will releases a large amount of latent heat in a cold room at near 0襖, however, liquid nitrogen gas can’t rapidly absorb the latent heat of water phase transition due to lower convective heat transfer coefficient, so it makes a probable great difference between the displayed temperature by a controlled-rate cooling apparatus and the actual temperature in the skin tissues, and it is difficult to reduce this temperature difference by increasing cold gas volume. In case of snap frozen, the skin is incubated with antifreeze solution and then transferred directly to liquid nitrogen, and the temperature can be cooled from >0襖 to liquid nitrogen temperature within 30s. Being simple, snap frozen eliminates special instrument and reduces cost. However, liquid nitrogen may generate grave ebullition during snap freezing, and the big temperature difference between liquid nitrogen and skin can not be fully utilized at the initial stage of freezing, thus, “thermo-zone platform” (as shown in Fig.1) will be form near zero degree. To avoid this defect, on one hand, antifreeze fluid needs to be optimized, on the other hand, a copper plate pre-cooled with liquid nitrogen shall be used for directly contacting skin graft for snap frozen using
heat conduction style,in order to obtain better cooling effect (as shown in Fig.2).
At present, there is inadequate researche on the thawing process of frozen skin. Most
standards advocate rapid warming of the skin to optimise viability. This can be achieved by
www.intechopen.com
Skin Graft Preservation
161
Fig. 1. Temperature (ºC) curve of skin immersing in liquid nitrogen (Available from: Basic and application of skin preservation, people’s military medical publisher;2002.)
Fig. 2. Temperature (ºC) curve of skin in a copper plate pre-cooled with liquid nitrogen (Available from: Basic and application of skin preservation, people’s military medical publisher;2002.)
immersion of the packs in a 37°C waterbath. The thawing process of skin is closely related to previous freezing process. In case of snap frozen, glassy solids are formed inside and outside of the cells, and quick rewarming can avoid “devitrification” during temperature rise process. “Devitrification”means glassy water or tiny ice crystals-bearing solid water is recrystallized prior to thawing, or tiny ice crystals are rethawed into large ice crystals, which destroy cell structures and cause cell death(Zieger et al., 1997).
3. Skin harvesting and processing
Processing methods used for banking of skin for subsequent therapeutic use depend on whether the skin is to retain viability or not. For viable skin grafts, sterilisation techniques cannot be applied, however antibiotics and antimycotics may be used to disinfect the tissue with respect to bacteria and fungi (Kearney,2005; Li, 2001; Ninnmam et al,.1978).
Tem
peratu
re (ºC)
Tem
peratu
re (ºC)
Time (s)
Time (s)
www.intechopen.com

Skin Grafts – Indications, Applications and Current Research
162
3.1 Screening of donor
One of the major concerns with the use of skin grafts from donors is the risk of disease transmission. A case involving the transmission of HIV from a skin donor to a recipient has been reported(Clark, 1987). To reduce the risk of disease transmission, skin donors should be screened before skin harvesting. If skin grafts obtained from cadaveric donors,medical
records held by hospitals, family doctors, and others must be screened for conditions that would exclude donation(Delmonico,1998). This may include current systemic infection, diseases of unknown etiology, and previous infections with the possibility of current carrier status (hepatitis, malaria, HIV, syphilis antibodies etc). It may also be prudent to exclude a history of malignant disease particularly if the skin might be used on immunosuppressed patients, for example, those suffering massive burn injuries. Behavioral history may also be grounds for rejection of the donor owing to the high correlations between activities such as intravenous drug abuse and viral infections such as HIV and hepatitis.
3.2 Reducing the population of microorganism
Skin tissue possesses a mixed commensal population of bacteria and fungi that lives primarily in or around the hair and sebaceous follicles (Kearney et al.,1984). Even the commensal bacteria may damage the skin if subsequently allowed to grow during the skin storage period to reach massive population densities. Therefore, it is important to try to eliminate or minimize the microbial population of skin before retrieval. For viable skin allografts, it is not possible to apply a sterilization technique because sterilization methods tend to inactivate cells at an equal or greater rate than for the bacterial cells. The best that can be achieved is a combination of serology screening for viruses and bacterial disinfection using antibiotic cocktails (Holder et al., 1998). This is generally achieved using skin prepping techniques similar to those used on the skin of patients undergoing operations in hospital. When banking skin in a viable state, it is important to validate that the prepping agents have been adequately removed before harvesting the skin, and that any residuals are not toxic to the skin cells. Although effective in reducing the bioburden, skin prepping is unlikely to totally eliminate bacteria (Lomas et al., 2003). It is therefore essential to prevent proliferation of any residual bacteria after retrieval, during transportation, and during subsequent processing. Maintaining the skin in a refrigerator or at wet ice temperatures prevents the proliferation of most bacteria. To eliminate residual bacteria and fungi in viable skin, an antibiotic/antimycotic cocktail may be used. If used at reduced temperatures (4襖), the skin may be incubated for up to 24 hours in the cocktail; however, only antibiotics that are effective at this temperature should be included. At normothermic temperature (37襖), most antibiotics can be considered; however, the exposure period should be minimized. For nonviable grafts, a range of sterilization techniques can be considered. Dry heat and autoclaving damage the structure of the skin tissue, including denaturation of collagen, and hence are not suitable. Techniques that have been successfully used include ethylene oxide gas and γ irradiation; however, concerns and limitations of these methods are beginning to appear. Ethylene oxide gas and its reaction product with chloride—ethylene chlorohydrin—are very toxic. Although acceptable levels for these compounds had been proposed, more recent data suggest that there is no safe level of ethylene oxide with respect to genotoxicity. Questions have also been raised about the effectiveness of γ irradiation. Many small viruses and spore-forming bacteria are fairly resistant to γ irradiation. The high doses that would be required to inactivate HIV in a window-period donor (more than 80 kGy) would cause
www.intechopen.com
Skin Graft Preservation
163
extensive damage to the tissue matrix including collagen denaturation. Therefore, a current consideration is whether “sterilization” can be achieved instead by using combinations of
microbial inactivation procedures (Kearney, 1989,2005; Prolo et al.,1980).
3.3 Time control
Viable skin grafts may be obtained from living donors or, more frequently, from cadaveric donors. In the latter case, the skin becomes ischemic immediately after circulatory arrest. This leads to progressive cell death over a period of days, which is accelerated at higher temperatures. Even if the cadaver is immediately placed into a refrigerator, the body cools at a slow rate, leading to at least some warm ischemia time. Nevertheless, viable skin can still be retrieved up to circa 24 hours after death. If the body is not quickly refrigerated, the skin will be subjected to a much longer warm ischemia period resulting in an accelerated deterioration in viability. Once the skin is removed from the body, it can be cooled rapidly by immersion into a refrigerated solution, thus immediately reducing the rate of cell death. In the other hand, tissue banking standards generally set limits on the maximum warm and cold ischemia times permitted after the death of the donor, because it is known that bacteria from the gut can be released into the vascular system postmortem and migrate to the internal organs and tissues(Kearney, 2005).
3.4 Sample of preparation skin graft from cadaveric donors 3.4.1 Donor selection Donor skin procurement must comply with local legislation. To ensure skin grafts quality, donors were aged between 8–60 years. The exclusion criteria for harvesting skin are basically the same as for donors of parenchymatous organs. Further exclusion criteria comprise skin diseases, injuries in the areas from which skin may be harvested, and blood samples were tested for HIV, HbA, HbB, HbC and syphilis antibodies.
3.4.2 Skin harvesting
Skin is cleaned with povidone-iodine 10% solution and skin with adipose layer harvested with a knife. Areas from which skin is harvested are limited to the following regions: ventral and dorsal trunk, left and right upper arm, and left and right thigh. Immediately after the removal, grafts were placed in saline, refrigerated and transferred to the processing room. The hair was removed and skin was soaked in 0.1% benzalkonium bromide for 15 min to sterilize. Split skin of 0.2–0.3mm was harvested under sterile conditions by a dermatome. Thereafter split skin was washed extensively and soaked for 10 min 3 times in saline with Penicillin /Streptomycin; then in Neomycin–saline (0.5%) for 10 min, 3 times. All the following procedures are carried out under sterile conditions.
3.5 Sample of preparation skin graft from porcine Domestic pigs were sacrificed and the skin was washed extensively with soap and water. The hair was removed by razor and the carcass was cleaned with povidone-iodine 10% solution. After cleaning, 0.3 mm to 0.6 mm partial-thickness skin from the pig`s back was harvested with a dermatome. Immediately after the removal, the harvested skins were placed into sterile boxes in normal saline supplemented with penicillin/streptomycin and sent to the laboratory, then soaked in 0.1% benzalkonium bromide for 15 min to sterilise and rinsed thrice in normal saline supplemented with penicillin/streptomycin in a laminar flow hood (Chiu&Burd, 2005).
www.intechopen.com
Skin Grafts – Indications, Applications and Current Research
164
4. Viable skin grafts preservation
Fresh cadaver allograft is still considered the ‘gold standard’ biologic dressing for closure of
burns. Unfortunately, the use of fresh allografts is severely impeded by their inadequate
availability. Skin graft preservation for the purpose of delayed application is still a basic tool
in burn treatment and plastic and reconstructive surgery. Even if the skin is placed into an
oxygenated nutrientrich medium, ischemic necrosis of the tissue still occurs because the
diffusion path from the tissue periphery to the central cells is extensive, oxygen and
nutrients cannot diffuse fast enough to supply the cells, and toxic metabolites cannot be
removed quickly enough. Therefore, method for the viable storage of skin is to reduce the
temperature hence reduces the metabolic rate of the cells and the nutritional demands and
metabolite production (Bravo et al,. 2000; Ge et al., 2010; Robb et al., 2001; Sterne et al., 2000).
4.1 Storage in 4°C
As early as 1903, Wentscher reported the successful storage and grafting of skin autografts
at temperatures near 0襖 for 14 days (Wentscher, 1903). Further studies by Carrel using
normothermic and hypothermic storage conditions confirmed the utility of the latter (Carrel,
1912). Eventually, refrigerator storage for skin autografts became the norm in burn units.
The simplest technique was to fold the skin so that the cut surfaces were in apposition and
then wrap the skin sandwich in tulle gras and/or saline gauze to prevent desiccation. Using
this method, autologous skin can be used after around 2 weeks of storage, although cell
viability is very low at this point. Unlike autograft, allograft has already lost some viability
by the time it is retrieved; therefore, maximum storage times using this method are reduced
to 7 or 8 days. Many attempts have been made to extend the refrigerator storage period for
skin. The addition of homologous serum at 10% to 33% was found to be beneficial because it
provided nutrients and diluted and buffered acids produced as byproducts of metabolism
(Allgower & Blocker, 1952). Alternatively, tissue culture media as a source of nutrients and
various buffering systems have been evaluated. The buffering systems, however, only
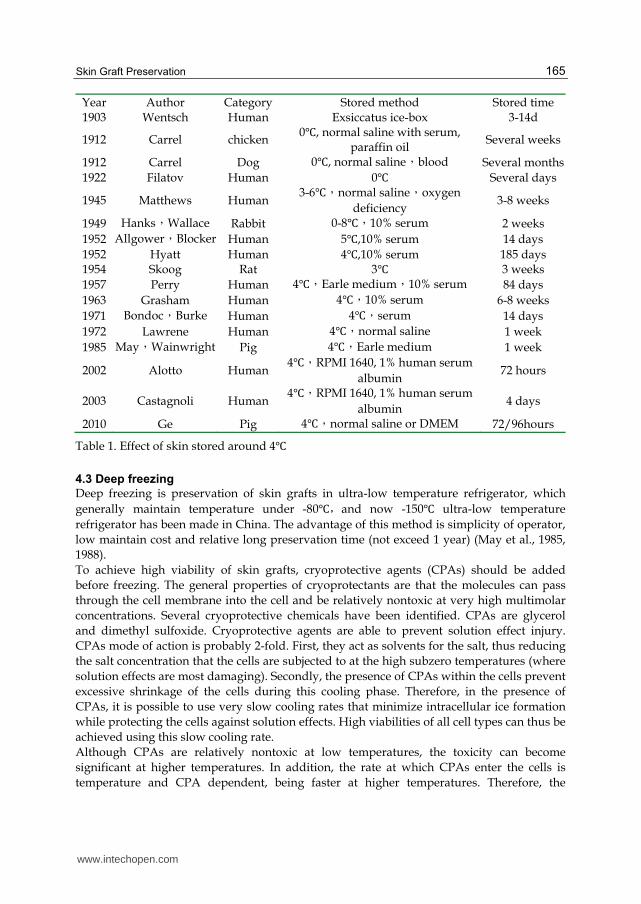
extend slightly the period of useful storage. Different methods for storing skin grafts around
4襖 are shown in Table 1 and show a large variance in storage time although the storage
methods are similar. The main reason for this variance may be criteria incompatible and the
absence of reliable detection methods of early research especially before 1970. The storage of
skin grafts in a 4襖 refrigerator is a simple and practicable technique; however, the skin
showed a very slow viability decrease with time stored at 4襖 (Chang et al., 1998; DeBono et
al., 1998; DeLW, 1980; Matsuka et al., 1993; May & Wainwright, 1985). The preservation time
of fresh skin should not exceed 3 days when stored in normal saline and must be used
within two weeks even when stored in tissue culture media with 10% serum.
4.2 Storage in -20°C
Wang has success develop non-freeze complex cryoprotectants( 10% DMSO, 10% propylene
glycol,10% PEG,10% glycerin) to avoid ice crystal formation when skin stored in -
20襖,the skin remain 76% activity in 14th day, higher than that of stored at liquid
nitrogen′60-70%″, then skin activity lower than that of stored at liquid nitrogen in the following time, but still remain 50% viability(the ultimate rate to survival post-transplantation) in 60 days, so skin grafts stored at -20襖 should be first consider if skin will be used within 2 weeks.(Wang et al., 2002).
www.intechopen.com
Skin Graft Preservation
165
Year Author Category Stored method Stored time 1903 Wentsch Human Exsiccatus ice-box 3-14d
1912 Carrel chicken 0襖, normal saline with serum,
paraffin oil Several weeks
1912 Carrel Dog 0襖, normal saline,blood Several months
1922 Filatov Human 0襖 Several days
1945 Matthews Human 3-6襖,normal saline,oxygen
deficiency 3-8 weeks
1949 Hanks,Wallace Rabbit 0-8襖,10% serum 2 weeks
1952 Allgower,Blocker Human 5襖,10% serum 14 days
1952 Hyatt Human 4襖,10% serum 185 days 1954 Skoog Rat 3襖 3 weeks
1957 Perry Human 4襖,Earle medium,10% serum 84 days
1963 Grasham Human 4襖,10% serum 6-8 weeks
1971 Bondoc,Burke Human 4襖,serum 14 days
1972 Lawrene Human 4襖,normal saline 1 week
1985 May,Wainwright Pig 4襖,Earle medium 1 week
2002 Alotto Human 4襖,RPMI 1640, 1% human serum
albumin 72 hours
2003 Castagnoli Human 4襖,RPMI 1640, 1% human serum
albumin 4 days
2010 Ge Pig 4襖,normal saline or DMEM 72/96hours
Table 1. Effect of skin stored around 4襖
4.3 Deep freezing
Deep freezing is preservation of skin grafts in ultra-low temperature refrigerator, which
generally maintain temperature under -80襖,and now -150襖 ultra-low temperature
refrigerator has been made in China. The advantage of this method is simplicity of operator,
low maintain cost and relative long preservation time (not exceed 1 year) (May et al., 1985,
1988).
To achieve high viability of skin grafts, cryoprotective agents (CPAs) should be added
before freezing. The general properties of cryoprotectants are that the molecules can pass
through the cell membrane into the cell and be relatively nontoxic at very high multimolar
concentrations. Several cryoprotective chemicals have been identified. CPAs are glycerol
and dimethyl sulfoxide. Cryoprotective agents are able to prevent solution effect injury.
CPAs mode of action is probably 2-fold. First, they act as solvents for the salt, thus reducing
the salt concentration that the cells are subjected to at the high subzero temperatures (where
solution effects are most damaging). Secondly, the presence of CPAs within the cells prevent
excessive shrinkage of the cells during this cooling phase. Therefore, in the presence of
CPAs, it is possible to use very slow cooling rates that minimize intracellular ice formation
while protecting the cells against solution effects. High viabilities of all cell types can thus be
achieved using this slow cooling rate.
Although CPAs are relatively nontoxic at low temperatures, the toxicity can become
significant at higher temperatures. In addition, the rate at which CPAs enter the cells is
temperature and CPA dependent, being faster at higher temperatures. Therefore, the
www.intechopen.com
Skin Grafts – Indications, Applications and Current Research
166
optimum temperature and the exposure time need to be validated. The basal medium into
which the CPA is dissolved for incubation of the skin tissue should be a balanced salt
solution, in which the zwitterionic buffers hydroxyethyl piperazine ethanesulfonic acid
(HEPES) and trimethylamino-ethanesulfonic acid (TES) have been shown to work well
(Basaran et al., 2006). To avoid osmotic lysis of the cells, either the saline can be added
gradually or an impermeant solute such as sucrose can be added to the saline to reduce the
difference in osmolarity.
4.4 Cryopreservation
A better method for the long-term preservation of skin grafts is cryopreservation. The
cryopreservation technique facilitates the cooling of the tissues to ultralow temperatures
while protecting the viability of the cells (Aggarwal et al., 1985; Bondox & Burke, 1971; Cui
et al., 2007; Fujita et al., 2000; Marrel et al., 1986). Once the skin is at a temperature lower
than -130襖, no further loss of cell viability is incurred. The boiling point of nitrogen gas is -
196襖, so skins immersed into liquid nitrogen should be able to keep viabily indefinitely in
abstracto.
There are two different cryopreservation protocols used in skin preservation: slow freezing
and quick freezing/snap frozen. Slow freezing can be achieved using a controlled-rate
cooling apparatus (Blondet et al., 1982). There is an optimum cooling rate for any cell type
that produces maximum cell survival. On either side of this optimum, the survival rate falls.
In the presence of CPA, a cooling rate of -1 ºC per minute will ensure survival of most of the
cells within skin tissue. As the cooling rate is increased,cell populations are sequentially
and adversely affected. Many cells in the body derived from leukocytes or closely related
lineages are known to be exquisitely sensitive to cryogenic injury. The depletion of
immunostimulatory “passenger leukocytes” was demonstrated by increasing the cooling
rate for pancreatic islets of Langerhans while maintaining the viability of the insulin-
producing islet cells (Ingham et al., 1993). This concept of cooling rate–dependent
immunomodulation was evaluated for skin tissue. A cooling rate of -30襖/min was shown
to maintain the viability of keratinocytes and fibroblasts while reducing the immunogenicity
(as assessed by the mixed epidermal cell/lymphocyte response assay) of murine allografts
by 95%. This was assumed to be due to an effect of the faster cooling rate on the major
immunostimulatory cell in the skin—the Langerhans cell.
Quick freezing/snap frozen is skin vitrification technique. Vitrification is defined as “the
instant solidification of a solution brought about by an extreme elevation in viscosity during
cooling, without ice crystal formation”. In other words, vitrification is faster and lacks some
of the typical disadvantages seen in traditional slow freezing (Mukaida, 2003). It bypasses
the ice-crystal formation phase and instantaneously solidifies into a glass-like structure,
moves the water directly into a glass-like phase. In a glass, the molecules do not rearrange
themselves into grainy ice crystals as the solution cools, but instead become locked together
while still randomly arranged as in a fluid, forming a “solid liquid” as the temperature falls
below the glass transition temperature (Silvestre et al., 2002). This technique was simple,
and no expensive equipment was needed. Initially, this method needed a 2-step procedure
because the cryoprotective agent was toxic. Kasai et al., (1990) modified this impractical to a
1-step method and incubated the skin with vitrification solution at room temperature and
was transferred directly into liquid nitrogen.
www.intechopen.com
Skin Graft Preservation
167
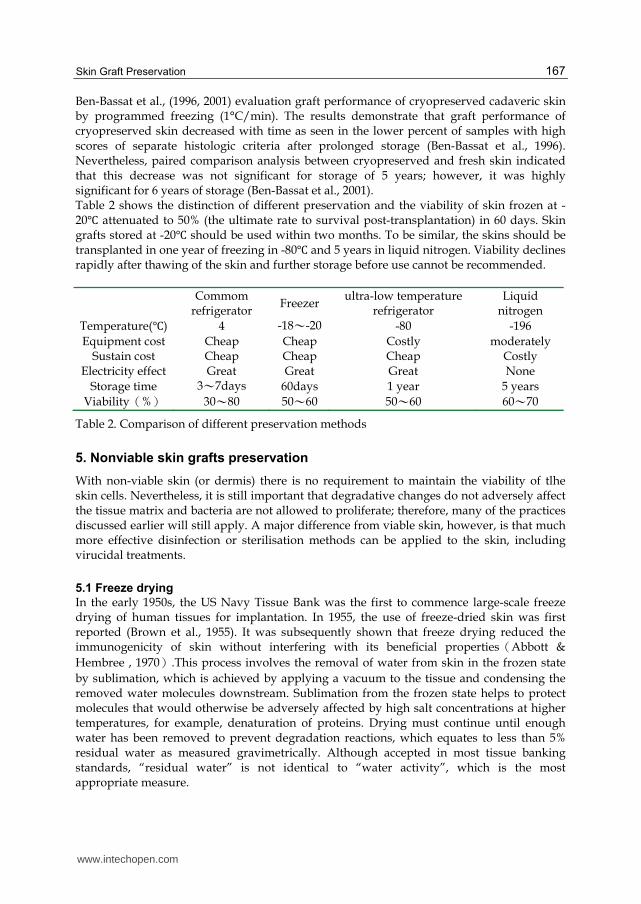
Ben-Bassat et al., (1996, 2001) evaluation graft performance of cryopreserved cadaveric skin by programmed freezing (1°C/min). The results demonstrate that graft performance of cryopreserved skin decreased with time as seen in the lower percent of samples with high scores of separate histologic criteria after prolonged storage (Ben-Bassat et al., 1996). Nevertheless, paired comparison analysis between cryopreserved and fresh skin indicated that this decrease was not significant for storage of 5 years; however, it was highly significant for 6 years of storage (Ben-Bassat et al., 2001). Table 2 shows the distinction of different preservation and the viability of skin frozen at -20襖 attenuated to 50% (the ultimate rate to survival post-transplantation) in 60 days. Skin grafts stored at -20襖 should be used within two months. To be similar, the skins should be transplanted in one year of freezing in -80襖 and 5 years in liquid nitrogen. Viability declines rapidly after thawing of the skin and further storage before use cannot be recommended.
Commom
refrigerator Freezer
ultra-low temperature refrigerator
Liquid nitrogen
Temperature(襖) 4 -18~-20 -80 -196
Equipment cost Cheap Cheap Costly moderately Sustain cost Cheap Cheap Cheap Costly
Electricity effect Great Great Great None
Storage time 3~7days 60days 1 year 5 years
Viabilityう%え 30~80 50~60 50~60 60~70
Table 2. Comparison of different preservation methods
5. Nonviable skin grafts preservation
With non-viable skin (or dermis) there is no requirement to maintain the viability of tlhe skin cells. Nevertheless, it is still important that degradative changes do not adversely affect the tissue matrix and bacteria are not allowed to proliferate; therefore, many of the practices discussed earlier will still apply. A major difference from viable skin, however, is that much more effective disinfection or sterilisation methods can be applied to the skin, including virucidal treatments.
5.1 Freeze drying
In the early 1950s, the US Navy Tissue Bank was the first to commence large-scale freeze drying of human tissues for implantation. In 1955, the use of freeze-dried skin was first reported (Brown et al., 1955). It was subsequently shown that freeze drying reduced the immunogenicity of skin without interfering with its beneficial propertiesうAbbott &
Hembree , 1970え.This process involves the removal of water from skin in the frozen state
by sublimation, which is achieved by applying a vacuum to the tissue and condensing the removed water molecules downstream. Sublimation from the frozen state helps to protect molecules that would otherwise be adversely affected by high salt concentrations at higher temperatures, for example, denaturation of proteins. Drying must continue until enough water has been removed to prevent degradation reactions, which equates to less than 5% residual water as measured gravimetrically. Although accepted in most tissue banking standards, “residual water” is not identical to “water activity”, which is the most appropriate measure.
www.intechopen.com

Skin Grafts – Indications, Applications and Current Research
168
5.2 Glycerolization preservation
In 1980s, glycerin was applied in clinical practice as skin graft preservation fluid, and had very good effect (Hermans, 1989; Huang et al., 2004; Richter et al., 1997; Van Baare et al., 1994,1998; Vuola & Pipping, 2002). EuroSkin Bank has done considerable fruitful work in the area and developed a solute preservation method using glycerol (De Backere & Mackie, 1997; Mackie, 1997). The skin was incubated in successively more concentrated glycerol solutions (50%, 70%, and 85%) and maintained long term in 85% glycerol. More recently, the glycerol and water flux kinetics have been characterized and a more efficient validated protocol was proposed. Study demonstrated that the 85% concentration originally chosen by the Euroskin Bank is optimal for minimizing degradative reactions (Ross & Kearney, 2004). It is very important that the glycerol is removed from the skin before clinical use. Failure to remove glycerol may lead to high systemic concentrations when used on open wounds. This is achieved by repeatedly washing the skin in physiological saline, and at least 30 to 60 minutes are required to remove most of the glycerol.
5.3 Glutaraldehyde preservation
As early as 1975, Schetnter reported the successful grafting of glutaraldehyde- preserved skin in clinical (Schetnter, 1975). The morphology of skin grafts has not evident change after treated with glutaraldehyde, and skin antigenicity was greatly reduced because antigen determinant site was closed by cross-linking of protein in the skin grafts. Glutaraldehyde-treated skin grafts can be used for escharectomy and tangential excision wounds and granulation wound covering, and has been shown to promote the formation of granulation tissues. However, such skin grafts have least elasticity, that is, with the extension of preservation duration, the skin becomes harder. Fresh allograft skin or lyophilized skin shall be immersed in 0.5% glutaraldehyde solution for 7-20min and be washed with normal saline for three times prior to use. There is no evident change in the elasticity and softeness of such skin, but its antignicity is decreased, which helps to extend the adhesion duration of grafted skin.
5.4 Irradiation preservation
Irradiated porcine skin is the most commonly used burn wound covering in China. Fresh porcine skin graft is sealed in a plastic bag and is irradiated with 60Co or an accelerator, then put into an ordinary refrigerator for preservation. After being irradiated, porcine skin can achieve integral asepsis, and its antignicity can be decreased. For gamma irradiation, the most resistant microorganisms are viruses, D10-values as high as 13 KGy have been reported for certain small viruses. Application of the commonest used dosage (25 KGy) to these viruses would only reduce the bioburden by 2 logs10. The high doses that would be required to inactivate HIV in a window-period donor (more than 80 kGy) would cause extensive damage to the tissue matrix including collagen denaturation. There are two possible effects on the macromolecular structure of skin matrix resulting from ionising irradiation. The first is scission which results in the breaking of bonds thus weakening the matrix. In the presence of water a second process involves crosslinking by new bond formation resulting from the generation of free radicals which may lead to stiffening of the matrix.
6. Quality control
A variety of national/international organisations have issued standards or guidelines for tissue banking, including the National Blood Service, British Association for Tissue Banking,
www.intechopen.com

Skin Graft Preservation
169
and European Association of Tissue Banks, etc (Baxter, 1985; Ben-Bassat et al., 2000; British Association for Tissue Banking, 2011; Chua et al., 2004; European Association of Tissue Banks, 2011; Freedlander et al., 1998; Janezic, 1999; Kalter, 1997; Kearney, 1998; May, 1990; Pillipp et al., 2004; Pianigiani et al., 2005). The core principle of skin banking quality control is to avoid the risk of cross infection and provide high-quality skin grafts for clinical. Therefore, donor selection, microbial/viral tests, skin viability detection and transplantation performance will be discussed in this paper.
6.1 Donor selection
With respect to medical/behavioural history screening, the regulatory and standards documents are once again very specific with a good deal of international consensus. Sources of medical/behavioural information include the next of kin (or partner/close friend) of the deceased who must be interviewed regarding medical history and any factors, practices or behaviour that may have increased the risk of exposure to HIV/Hepatitis. In addition, the family doctor, hospital records, and autopsy report should be consulted as additional sources of medical and behavioural history. Evaluation of the risk of virus exposure must be explored in detail with other aspects of medical and behavioural history. The exclusion criteria for harvesting skin are basically the same as for donors of parenchymatous organs including cancer, diseases of unknown aetiology and various viral, bacterial and parasitic diseases. Further exclusion criteria comprise other skin diseases and injuries in the areas from which skin may be harvested.
6.2 Microbial/viral tests
There is a widespread consensus on the testing of donors to preclude certain virological diseases, including HIV, Hepatitis B, Hepatitis C, syphilis antibodies ,and in general these follow the National Blood Service testing regimens for each country. Screening for CMV is important when recipients are CMV negative and will receive immunosuppressive drugs following organ transplantation. However, the natural immunosuppression associated with burns does not appear to lead to CMV related problems in skin allograft recipients. Many tissue banks do not screen for CMV. The microbial tests are generally done on allograft samples and the viral tests on blood samples.Skin samples for microbial tests are incubated in Thioglycollate and Roswell Park Memorial Institute (RPMI) 1640 without antibiotics, in a 37襖 incubator for 10 days.
6.3 Skin viability
The viability of graft skin is fundamental for surgical procedures involving graft taking, and
the American Association of Tissue Banks indicates that the viability of skin is an essential
prerequisite for good-quality grafts (American Association of Tissue Banks, 2011). It is a
necessity that a skin bank should certify, not only the sterility, but also the viability of the
skin allografts used and that routine quality controls be carried out to certify that grafts are
viable before transplantation. The of viability assays is two-fold: one is that of supplying an
‘‘experimental assay’’: used to optimize the various parts of a preservation procedure
during experimental development. The other offers a ‘‘predictive assay’’: used to predict the
‘‘quality’’ of an individual sample that has been stored by an established tested technique.
Various methods, both qualitative and quantitative, are currently used to determine skin
grafts viability such as cell culture, succinate dehydrogenase, trypan blue dye, skin oxygen
www.intechopen.com

Skin Grafts – Indications, Applications and Current Research
170
consumption, Tetrazolium salts (MTT/WST-1), SYTO/EB dyes and so on (Alotto et al.,
2002). The MTT method is most widely used because it is simple, quick and precise
(Castagnoli et al., 2003; Klein, 1996; Pegg, 1989; Yang et al., 2000; Zieger et al., 1993).
6.4 Transplantation performance
Skin transplantation experiment is a straightforward and reliable skin graft quality evaluation method. For any skin graft and preservation method, the final result is to identify that the skin graft can survive in the living body. For evaluation of transplantation performance of preserved skin, samples of skin were often grafted onto mice and rats and the experiment animals were sacrificed after 4 or 7 days. The grafts were then assessed by gross inspection including adherence to wound bed, color and pliability and by histologic evaluation including epidermis integrity, epidermal–dermal junction, collagen organization, the presence of fibroblasts and graft adherence (Cinamon et al., 1993).
7. Conclusions
Skin graft preservation for the purpose of delayed application is still a basic tool in burn treatment and plastic and reconstructive surgery. It is therefore important to provide a framework for selecting optimal guidelines for procurement, processing, preservation, and quality control of skin grafts for doctors and researchers, thus ensuring high levels of safety and efficacy of skin grafts.
8. References
Abbot, W.M. & Hembree, J.S.う1970え. Absence of antigenicity in freeze-dried skin
allografts. Cryobiology, Vol.6, No.5,( Mar-Apr),pp. 416-418, 0011-2240 Aggarwal, S.J.; Baxter, C.R. & Diller, KR. (1985). Cryopreservation of skin: an assessment of
current clinical applicability. J Burn Care Rehabil, Vol.6,No.6,(Nov-Dec),pp.469-476, 0273-8481
Allgower, M. & Blocker, T.G. (1952). Viability of skin in relation to various methods of storage. Tex Rep Biol Med, Vol.10, No.1, (Jan), pp.3-21, 0040-4675
Alotto, D.; Ariotti, S.; Graziano, S.; Verrua, R.; Stella, M. & Magliacani, G., et al. (2002). The role of quality control in a skin bank: tissue viability determination. Cell Tissue Bank, Vol.3, No.1, (Nov),pp.3–10. 1389-9333
American Association of Tissue Banks. Standards. Available from: www.aatb.org Basaran, O.; Ozdemir, H.; Kut, A.; Sahin, F.I.; Deniz, M.. & Sakallioglu, E.A., et al. (2006).
Effects of different preservation solutions on skin graft epidermal cell viability and graft performance in a rat model. Burns,Vol.32,No.4, (Jun),pp.423–429, 0305-4179
Baxter, C.R. (1985). Skin banking in the USA. J Burn Care Rehabil, Vol.6, No.4, (Jun-Aug), pp.322,0273-8481
Ben-Bassat, H.; Chaouat, M.; Segal, N.; Zumai, E.; Wexler, M.R. & Eldad, A. (2001).How long can cryopreserved skin be stored to maintain adequate graft performance? Burns, Vol.27,No.5,(Aug),pp.425-431. 0305-4179
Ben-Bassat, H.; Chaouat, M. ; Zumai, E. ; Segal, N. ; Cinamon, U. & Ron, M., et al.(2000). The Israel National Bank: quality assurance and graft performance of stored tissues. Cell Tissue Bank, Vol.1, No.4, pp.303–312, 1389-9333
www.intechopen.com
Skin Graft Preservation
171
Ben-Bassat, H.; Strauss, N.; Ron, M.; Chaouat, M.; Breiterman, S. & Israeli, A., et al. (1996). Transplantation performance of human skin cryopreserved by programmed or stepwise freezing and stored at −80襖 or −180襖. J Burn Care Rehabil, Vol.17, No.5, (Sep-Oct),pp.17:421-428, 0273-8481
Blome-Eberwein, S.; Jester, A.; Kuentscher, M.; Raff, T.; Germann, G. & Pelzer, M., et al. (2002). Clinical practice of glycerol preserved allograft skin coverage. Burns, Vol.28, No.Suppl.1, (Oct),pp.S10-12. 0305-4179
Blondet, R.; Gibert-Thevenin, M.A.; Pierre, C. & Ehrsam, A. (1982). Skin preservation by programmed freezing. Br J Plast Surg,Vol.35, No.4, (Oct), pp.530-536. 0007-1226
Bondox, C.C. & Burke, H.F. (1971). Clinical experience with viable frozen human skin and frozen skin bank. Ann Surg,Vol.174, No.3, (Sep), pp.371–382. 0003-4932
Bravo, D.; Rigley, T.H.; Gibran, N.; Strong, D.M. & Newman-Gage, H. (2000).Effect of storage and preservation methods on viability in transplantable human skin allografts. Burns,Vol.26, No.4, (Jun), pp.367-378, 0305-4179
British Association for Tissue Banking. General standards and technical guidelines. Available from: www.batb.org.uk/standards.htm
Brown, J.B.; Fryer, M.P. & Zaydon T.J. (1955). A skin bank for postmortem homografts. Surg Gynecol Obstet, Vol.101, No.4, (Oct), pp. 401-412, 0039-6087
Carrel A. (1912). The preservation of tissues and its application in surgery. J Am Med Assoc, Vol.59, No.7, (Jun); 523-527.0002-9955
Castagnoli, C.; Alotto, D. ; Cambieri, I. ; Casimiri, R. ; Aluffi, M. & Stella, M., et al. (2003). Evaluation of donor skin viability: fresh and cryopreserved skin using tetrazolioum salt assay. Burns,Vol.29, No.8, (Dec), pp.759–767, 0305-4179
Chiu, T. & Burd, A. (2005). "Xenograft" dressing in the treatment of burns. Clin Dermatol, Vol.23, No.4,(Oct), pp. 419–423, 1175-0561
Chang, P.; Rosenquist, M.D.; Lewis, R.W. & Kealey, G.P. (1998). A study of functional viability and metabolic degeneration of human skin stored at 4襖. J Burn Care Rehabil, Vol.19, No.1 Pt 1,(Jan-Feb),pp.25-28, 0273-8481
Chua, A.; Song, C. ; Chai, A. ; Chan, L. & Tan, K.C. (2004). The impact of banking and the use of its cadaveric skin allografts for severe burn victims in Singapore. Burns, Vol.30, No.7, (Nov), pp.696–700, 0305-4179
Cinamon, U.; Eldad, A.; Chaouat, M.; Wexler, R.M.; Israeli, A. & Zanger, U., et al. (1993). A simplified testing system to evaluate performance after transplantation of human skin preserved in glycerol or in liquid nitrogen. J Burn Care Rehabil,Vol.14, No.4, (Jul-Aug), pp.435–439, 0273-8481
Clark, J. (1987). HIV transmission and skin grafts. Lancet, Vol.329, No.8539, (Apr),pp.983. 0140-6736
Cui, X.; Gao, D.Y.; Fink, B.F.; Vasconez, H.C. & Rinker, B. (2007). Cryopreservation of composite tissues and transplantation: Preliminary studies. Cryobiology, Vol.55, No.3, (Dec), pp.295-304, 0011-2240.
DeBackere, A.C.J. & Mackie, D. (1997). The Euro Skin Bank: development and application of glycerol-preserved allografts. J Burn Care Rehabil, Vol.18, No.1 Pt 2,(Jan-Feb),pp.7-9, 0273-8481
DeBono, R.; Rao, G.S. & Berry, R.B. (1998). The survival of human skin stored by refrigeration at 4襖 in MacCoy’s 5A medium: does oxygenation of the medium improve storage time? Plast Reconstr Surg,Vol.102,No.1,(Jul),pp.78-83, 0032-1052
www.intechopen.com
Skin Grafts – Indications, Applications and Current Research
172
De, L.W.; De, W.F. & Penninckx, F. (1980). Metabolic changes in human skin preserved at −3襖 and at −196襖. Cryobiology, Vol.17, No.1,(Feb),pp.46-53,0011-2240
Delmonico, F. (1998). Organ donor screening for infectious diseases. Transplantation, Vol.65, No.5, (Mar),pp.603-610, 2090-0015
European Association of Tissue Banks. Standards. Available from: www.eatb.de/html/ standards.htm.
Freedlander, E.; Boyce, S.; Ghosh, M.; Ralston, D.R. & MacNeil, S. (1998). Skin banking in the UK: the need for proper organization. Burns,Vol.24, No.1,(Feb),pp.19–24, 0305-4179
Fujita, T.; Takami, Y.; Ezoe, K.; Saito, T.; Sato, A.K. & Takeda, N., et al. (2000). Successful preservation of human skin by vitrification. J Burn Care Rehabil, Vol.21, No.4, (Jul-Aug), pp.304-309, 0273-8481
Ge, L.; Sun, L.; Chen, J.; Mao, X.; Kong, Y. & Xiong, F., et al. (2010). The viability change of pigskin in vitro. Burns,Vol.36, No.4,(Jun),pp.533-538, 0305-4179
Hermans, M.H.E. (1989). Clinical experience with glycerol-preserved donor skin treatment in partial thickness burns. Burns ,Vol.15, No.1,(Feb),pp.57-59, 0305-4179
Holder, I.A.; Robb, E. & Kagan, R. (1998). Antimicrobial mixtures used by tissue banks for harvested skin: comperative in vitro activity. Burns, Vol.24, No.7, (Nov), pp.604-608, 0305-4179
Huang, Q.; Pegg, D.E. & Kearney, J.N. (2004). Banking of non-viable skin allografts using high concentrations of glycerol or propylene glycol. Cell Tissue Bank, Vol.5,No.1, pp.3-21, 1389-9333
Ingham, E.; Matthews, B.; Kearney, J.N. & Gowland, G. (1993). The effects of variation of cryopreservation protocols on the immunogenicity of allogeneic skin grafts. Cryobiology, Vol.30, No.5,(Oct), pp.443-458, 0011-2240
Janezic, T.F. (1999). Then and now: 25 years at the Ljubljana burns unit skin bank. Burns,Vol.25, No.7,(Nov),pp.599–602, 0305-4179
Kalter, E.S.; de By, T.M. (1997). Tissue banking programmes in Europe. Br Med Bull, Vol.53, No.4, pp.798-816, 0007-1420
Kasai, M.; Komi, J. H.; Takakamo, A.; Tsudera, H.; Sakurai, T. & Machida, T. (1990). A simple method for mouse embryo cryopreservation in a low toxicity vitrification solution, without appreciable loss of viability. J Reprod Fertil, Vol.89,No.1, (May), pp. 91-97, 0022-4251
Kearney, J.N. (1998). Quality issues in skin banking: a review. Burns,Vol.24, No.4, (Jun), pp.299-305. 0305-4179
Kearney, J.N. (2005). Guidelines on processing and clinical use of skin allografts. Clin Dermatol , Vol.23,No.4,(Jul-Aug),pp.357-364,1507-5516
Kearney, J.N.; Harnby, D.; Gowland, G. & Holland K.T. (1984). The follicular distribution and abundance of resident bacteria on human skin. J Gen Microbiol. Vol.130, No.4, (Apr), 130:797- 801.
Kearney, J.N.; Franklin, U.C.; Aguirregoicoa, V. & Holland, K.T. (1989). Evaluation of ethylene oxide sterilisation of tissue implants. J Hosp Infect, Vol.13, No.1, (Jan), pp.71-80, 0195-6701
Klein, M.B.; Shaw, D.; Barese, S.; Chapo, G.A. & Cuono, C.B. (1996). Reliable and cost-effective in vitro assay of skin viability for skin banks and burn centers. J Burn Care Rehabil, Vol.17, No.6 Pt 1, (Nov-Dec),pp.565–570, 0273-8481
www.intechopen.com
Skin Graft Preservation
173
Li, A. (2001).LI AO Burns, 1st ed., Shanghai Science & Technique Press, ISBN:7-5323-5910-7, Shanghai, China
Lomas, R.J.; Cruse-Sawyer, J.E.; Simpson, C.; Ingham, E.; Bojar, R. & Kearney, J.N. (2003). Assessment of the biological properties of human split skin allografts disinfected with peracetic acid and preserved in glycerol. Burns,Vol.29, No.6,(Sep),pp.515-525, 0305-4179
Mackie, D.P. (1997). The Euro skin bank: development and application of glycerol-preserved allografts. J Burn Care Rehabil, Vol.18, No.1 Pt 2,(Jan-Feb),pp.S7-9, 0273-8481
Marrel, S.W.; Shelby, J.; Saflle, J.R.; Krueger, G.G. & Navar, P.D. (1986). An invivo test of viability for cryopreserved human skin. Curr Surg,Vol.43, No.4, (Jul-Aug), pp.296–300, 0149-7944
Matsuka, K.; Hata, Y.; Yano, K.; Ito, O. & Matsuda, H. (1993). Epidermal cell viability in rat skin preserved at 4 degrees C. Ann Plast Surg, Vol.31, No.4,(Oct),pp.358–363, 1536-3708
May, S.R. (1990). The future of skin banking. J Burn Care Rehabil, Vol.11, No.5, (Sep-Oct), pp.484-486, 0273-8481
May, S.R.; Guttman, R.M. & Wainwright, J.F. (1985). Cryopreservation of skin using an insulated heat sink box stored at -70°C. Cryobiology,Vol.22,No.3,(Jun),pp.205-214, 0011-2240
May, S.R. & Roberts, D.P. (1988). Development of a passive device for freezing large amounts of transplantable skin at one time in a -70襖 mechanical refrigerator. Cryobiology, Vol.25, No.3,(Jun),pp.186-196, 0011-2240
May, S.R. & Wainwright, J.F. (1985). Integrated study of the structural and metabolic degeneration of skin during 4襖 storage in nutrient medium. Cryobiology, Vol.22, No.1, (Feb), pp.18-34, 0011-2240
Mukaida, T.; Nakamura, S.; Tomiyama, T.; Wada, S.; Oka, C.; Kasai, M. & Takahashi, K. (2003). Vitrification of human blastocysts using cryoloops: clinical outcome of 223 cycles. Hum Reprod. Vol.18,No.2, (Feb), pp.384-391, 0268-1161
Ninnmann, J.L.; Fisher, J.C. & Frank, H.A. (1978). Clinical skin banking: a simplified system for processing, storage and retrieval of human allografts. J Trauma, Vol.18, No.10, (Oct), pp.723–725. 0022-5282
Pegg, D.E. (1989). Viability assays for preserved cells, tissues, and organs. Cryobiology, Vol.26, No.3,(Jun),pp.212–231, 0011-2240
Philipp, S.; Hans, L. & Hans-Ulrich, L. (2004). Five Years of Experience with the Dortmund Skin Bank. Euro J Trauma,Vol.30,No.2,(Mar),pp.116-119, 1439-0590
Pianigiani, E.; Ierardi, F.; Cherubini, D.S.F. & Andreassi, A. (2005). Skin bank organization. Clin Dermatol, Vol.23,No.4,(Jul-Aug),pp.353-356, 1175-0561
Prolo, D.J.; Pedrotti, P.W. & White DH. (1980). Ethylene oxide sterilisation of bone, dura mater and fascia lata for human transplantation. Neurosurgery, Vol.6, No.5, (May), pp.529-539, 1524-4040
Richter, C.D.; Hoekstra, M.J.; van Baare, J.; du Pont, J.S. & Kamperdijk, E.W.A. (1997). Immunogenicity of glycerol-preserved human cadaveric skin in vitro. J Burn Care Rehabil, Vol.18,No.3,(May-Jun),pp.228-233, 0273-8481
Robb, E.C.; Bechmann, N.; Plessinger, R.T.; Boyce, S.T.; Warden, G.D. & Kagan, R.J. (2001). Storage media and temperature maintain normal anatomy of cadaveric human skin
www.intechopen.com
Skin Grafts – Indications, Applications and Current Research
174
for transplantation to full-thickness skin wounds. J Burn Care Rehabil, Vol.22, No.6, (Nov-Dec),pp.393-396, 0273-8481
Ross, A. & Kearney, J.N. (2004). The measurement of water activity in allogeneic skin grafts preserved using high concentration glycerol or propylene glycol. Cell Tissue Bank, Vol.5, No.1, pp.37- 44, 1389-9333
Schechter, I. (1975). Prolonged retention of glutaraldehyde-treated skin allografts and xenografts: immunological and histological studies. Ann Surg, Vol.182, No.6, (Dec), pp.699-704, 0003-4932
Silvestre, M.A.; Saeed, A.M.; Escribá, M.J. & García-Ximénez, F. (2002). Vitrification and rapid freezing of rabbit fetal tissues and skin samples from rabbits and pigs. Theriogenology, Vol.58, No.1,(Jul),pp.69-76, 0093-691X
Sterne, G.D.; Titley, O.G. & Christie, J.L. (2000) A qualitative histological assessment of various storage conditions on short term preservation of human split skin grafts.Br J Plast Surg, Vol.53,No.4,(Jun),pp.331-336, 0007-1226
Van Baare, J.; Buitenwerf, J.; Hoekstra, M.J. & du Pont, J.S. (1994). Virucidal effect of glycerol as used in donor skin preservation. Burns, Vol.20, suppl. 1,pp.S77-S80,0305-4179
Van, Baare. J.; Cameron, P.U.; Vardaxis, N.; Pagnon, J.; Reece, J. & Middelkoop, E., et al. (1998). Comparison of glycerol preservation with cryopreservation methods on HIV-1 inactivation. J Burn Care Rehabil, Vol.19,No.6,(Nov-Dec),pp.494-500, 0273-8481
Vuola, J. & Pipping, D. (2002). Maintaining a glycerolized skin bank—a practical approach. Burns, Vol.28, Suppl. 1, (Oct), pp.S31-33,0305-4179
Wang X.H.; Wu J.; Zhang N.; Chen X.W.; Zhou L.X. & Xiao G.X. An experimental study on preservation of human split thickness skin samples with -20襖 non-freezing composite cryoprotective solution. ACTA Academiae Medicinae Militaris Tertiae . Vol.24, No.2, (Feb), pp.225-226, 1000-5404
Wentscher, J. (1903). A further contribution about the survivability of human epidermal cells. Dtsch Z Chir, Vol..70, pp.21-44, 0367-0023
Yang, H.; Jia, X.M.; Acker, J.P.; Lung, G. & McGann, L.E. (2000). Routine assessment of viability in split-thickness skin. J Burn Care Rahabil, Vol.21,No.2,(Mar-Apr), pp.99–104, 0273-8481
Zhu, Z.M.; Chai, J.K. & Jia, X.M. (2002). Basic and application of skin preservation, 1st ed., People’s military medical publisher, ISBN: 7-80157-604-7, Beijing, China
Zieger, M.A.J.; Tredget, E.E. & McGann, L.E. (1993). A simple, effective system for assessing viability in split-thickness skin with the use of oxygen consumption. J Burn Care Rehabil, Vol.14,No.3,(May-Jun),pp.310-318, 0273-8481
Zieger, M.A.J.; Tredget, E.E.; Sykes, E.D. & McGann, L.E. (1997). Injury and protection in split-thickness skin after very rapid cooling and warming. Cryobiology,Vol.35,No.1, (Aug), pp.53-69, 0011-2240
www.intechopen.com

Skin Grafts - Indications, Applications and Current ResearchEdited by Dr. Marcia Spear
ISBN 978-953-307-509-9Hard cover, 368 pagesPublisher InTechPublished online 29, August, 2011Published in print edition August, 2011
InTech EuropeUniversity Campus STeP Ri Slavka Krautzeka 83/A 51000 Rijeka, Croatia Phone: +385 (51) 770 447 Fax: +385 (51) 686 166www.intechopen.com
InTech ChinaUnit 405, Office Block, Hotel Equatorial Shanghai No.65, Yan An Road (West), Shanghai, 200040, China
Phone: +86-21-62489820 Fax: +86-21-62489821
The procedure of skin grafting has been performed since 3000BC and with the aid of modern technology hasevolved through the years. While the development of new techniques and devices has significantly improvedthe functional as well as the aesthetic results from skin grafting, the fundamentals of skin grafting haveremained the same, a healthy vascular granulating wound bed free of infection. Adherence to the recipient bedis the most important factor in skin graft survival and research continues introducing new techniques thatpromote this process. Biological and synthetic skin substitutes have also provided better treatment options aswell as HLA tissue typing and the use of growth factors. Even today, skin grafts remain the most common andleast invasive procedure for the closure of soft tissue defects but the quest for perfection continues.
How to referenceIn order to correctly reference this scholarly work, feel free to copy and paste the following:
Liangpeng Ge, Zhenggen Huang and Hong Wei (2011). Skin Graft Preservation, Skin Grafts - Indications,Applications and Current Research, Dr. Marcia Spear (Ed.), ISBN: 978-953-307-509-9, InTech, Available from:http://www.intechopen.com/books/skin-grafts-indications-applications-and-current-research/skin-graft-preservation





![Alveolar Ridge Preservation after Tooth Extraction Using ... · ridge resorption rate and bone remodelling after tooth extraction [15]. Autogenous bone as bone graft material is still](https://img.pdfslide.us/doc/110x75/5ed57c6a0bd3843450408daa/alveolar-ridge-preservation-after-tooth-extraction-using-ridge-resorption-rate.jpg)