Embed Size (px)
Citation preview

Chapter 10
Excision Techniques, Staples, and Sutures
Mollie A. MacCormack
Excisions are one of the most commonly performed
dermatologic procedures. It is estimated that more
than 650,000 excisions are performed each year in
the United States, with dermatologists accounting
for about 58% of this number.1 Excisions are per-
formed for a variety of reasons including diagnosis,
the therapeutic removal of malignant and benign
growths, as well as simply for improved appearance.
While the vast majority of excisions are straightfor-
ward in nature, close attention to a few basic tenets
will enhance both the efficiency of the procedure as
well as overall cosmesis. This chapter will review the
basic materials required for a successful excision as
well as the most common excision and closure
techniques.
Patient Preparation
Patient preparation is of great importance in assur-
ing a successful outcome to any surgical procedure.
Early identification of any potential complicating
factors can greatly reduce the incidence of adverse
events (Table 10.1). Preoperative evaluation should
begin with the assessment of patient comorbidities
that may prevent them from providing informed
consent, lessen their ability to tolerate the proce-
dure, place them at increased risk of infection, or
interfere with appropriate wound healing. All
women of childbearing age should be asked about
potential pregnancy. A complete list of medications
is required, with close attention paid to those med-
ications that may affect the ability to obtain
hemostasis (antiplatelet therapy, anticoagulants)
or potentially complicate wound healing (systemic
corticosteroids or isotretinoin use within the last 6–
12 months). It should be noted that many food
items and herbal supplements can also alter platelet
function.2–4 While in the past it was common prac-
tice to discontinue those medications that can make
hemostasis more difficult, a number of studies have
shown that the actual negative impact of such med-
ications is quite small, while the potential ramifica-
tions of discontinuation on overall health (stroke,
myocardial infarction, pulmonary embolus, etc.)
are devastating.5–9 For this reason, while patients
may be advised to discontinue herbal supplements,
nonsteroidal anti-inflammatory drugs (NSAIDs),
or aspirin taken for primary prevention, it is
strongly recommended that they be maintained on
all medically necessary anticoagulation.
Any existing drug allergies should be recorded
and avoided. Patients should be evaluated for any
electrical devices such as pacemakers, internal car-
diac defibrillators, and nerve stimulators that may
receive interference from electrocautery. In addi-
tion, needle/surgical phobias or simply patient anxi-
ety are not uncommon in the surgical setting and
should be addressed. Often a complete explanation
of the procedure is all that is required to put such a
patient at rest.
Simple nonpharmacologic interventions such as a
peaceful office setting, soothing music, the use of
drapes to minimize visualization of surgical
instruments and the surgical field, as well as dis-
tracting conversation are often quite beneficial.
D.F. MacFarlane (ed.), Skin Cancer Management, DOI 10.1007/978-0-387-88495-0_10,� Springer ScienceþBusiness Media, LLC 2010
125

In the extreme case, premedication with low-dose
anxiolytics such as lorazepam given orally 1 h prior
to the procedure can be helpful (after first ensuring
that the patient will not be driving).
Antibiotic Prophylaxis
The vast majority of dermatologic excisions do not
require pre- or postoperative antibiotics. Updated
guidelines for endocarditis prophylaxis were pub-
lished by the American Heart Association in 2007.
Based upon these recommendations, routine pro-
phylaxis is rarely required and is deemed appropri-
ate only for procedures (including biopsies and
suture removal) involving perforation of the
respiratory tract/oral mucosa or performed in
actively infected tissue in a small subgroup of
patients at highest risk of adverse outcome.10 For
those patients who require prophylaxis, antibiotic
choice should be directed toward the eradication of
viridans group streptococci for procedures invol-
ving perforation of oral/respiratory mucosa and
staphylococci and B-hemolytic streptococci if the
procedure involves infected skin. Should methicil-
lin-resistant Staphylococcus aureus (MRSA) be sus-
pected, clindamycin or vancomycin would be the
drug of choice.
While no official guidelines exist addressing the
issue of cutaneous surgery and prophylaxis of arti-
ficial joints, a joint advisory statement from the
American Dental Association and the American
Academy of Orthopedic Surgeons recommended
against the use of prophylaxis for routine dental
work in patients with artificial joints more than 2
years old—procedures that carry a significantly
higher risk of inducing bacteremia than clean cuta-
neous incisions.11 Tooth brushing alone induces
bacteremia rates of 25%,12,13 while the rate of bac-
teremia induced by cutaneous surgery is less than
3%.14,15 The guidelines are less clear for patients
whose artificial joints are less than 2 years old, as
these joints are noted to be more susceptible to
infection.11 At the current time, there is no evidence
to suggest that prophylaxis is required for the vast
majority of prosthetic joint recipients with clean
cutaneous wounds. However, given the higher risk
of bacteremia associated with procedures involving
mucosal surfaces, adopting the endocarditis pro-
phylaxis guidelines is often recommended for
patients with clean-contaminated wounds.16 As
treatment guidelines for patients who have received
their transplants within the past 2 years are unclear,
many practitioners have also adopted the endocar-
ditis recommendations for this patient subset.17
Please see Chapter 8 for further discussion.
Site Preparation and Anesthesia
Preoperative Antisepsis
The ideal cutaneous antiseptic would provide com-
plete, long-lasting sterilization of the operative field
with no tissue toxicity. A number of choices are
available for antiseptic preparation of the cuta-
neous surface (Table 10.2). The most commonly
Table 10.1 Preoperative patient evaluation
MedicalComorbidities
AnxietyArthritis/Severe musculoskeletaldisease
Artificial heart valves or recentprostheses
Cardiovascular disease/heart valveanomalies
Clotting disordersDementiaDiabetesHistory of endocarditisHistory of poor wound healing/keloid formation
HypertensionMalnutritionPeripheral vascular diseasePregnancy
Medications/Herbalsupplements
AnticoagulantsAntiplatelet agentsAccutane use within the past 6–12months
CorticosteroidsHerbal supplementsImmunosuppressants
Drug allergies
Electrical devices PacemakersImplantable cardiac defibrillatorsBrain stimulators
SocialEnvironment
Patient ability to care for wound/obtain assistance in wound care
126 M.A. MacCormack

used are 10% povidone-iodine, 4% chlorhexidine
gluconate, 70% isopropyl alcohol, and 2% chlor-
hexidine gluconate combined with 70% isopropyl
alcohol. Povidone-iodine has broad-spectrum
activity against bacteria and some viruses; how-
ever, it is easily inactivated as it is only effective
when dry. Chlorhexidine is slower in onset, how-
ever, its overall effect is of longer duration and it
has been demonstrated to be superior to povi-
done-iodine in decreasing bacterial load.18 Com-
parative studies suggest that the 70% isopropyl
alcohol and 2% chlorhexidine gluconate combina-
tion, as well as a combined isopropyl alcohol/
povidone-iodine scrub, provide the best immedi-
ate and persistent antimicrobial effect.19–21 While
generally well tolerated, caution must be taken
when using cutaneous antiseptics. Prolonged,
direct contact with chlorhexidine can lead to ker-
atitis and ototoxicity, while iodine preparations
are often irritating to the skin and can be toxic in
newborns.
Anesthesia
Most cutaneous excisions can be performed
under local anesthesia. The most commonly
used anesthetic is 0.5–1% lidocaine due to its
rapid onset of action and intermediate duration
of effect. The addition of epinephrine not only
provides increased hemostasis but also extends
efficacy. Maximum recommended dose is
4.5 mg/kg for the plain formulation and 7 mg/
kg for lidocaine plus epinephrine.22 While it was
once thought that only plain lidocaine could be
used in anatomic areas such as the nose, ear, or
penis, this is not the case and there are no
absolute anatomic contraindications to epinephr-
ine use.23–25 The use of epinephrine should be
avoided in patients taking propanolol, a nonse-
lective beta blocker, as it could potentially lead
to malignant hypertension.26 True allergy to
anesthetics is rare. It is important to obtain a
complete history of reported allergic reactions
because what many patients interpret as an aller-
gic response is actually a vasovagal episode or
symptoms due to epinephrine effect (palpita-
tions, shaking, sweating, light-headedness). In
the uncommon case of actual allergy, the offend-
ing agent is often the preservative present in
multi-dose vials or a sodium metabolite found
in epinephrine-containing products.27 Should a
true lidocaine allergy exist, an ester anesthetic
such as procaine can be substituted.
The discomfort associated with anesthesia injec-
tion is multi-factorial, in part due to tissue disten-
sion and in part due to the acidity of the anesthetic
(especially in epinephrine-containing formula-
tions). Simply buffering the anesthetic with sodium
bicarbonate in a 9:1 formulation, initiating the
injection in the more distensible subcutaneous tis-
sue, and decreasing the speed of infiltration can
increase patient comfort substantially.28 An
in-depth review of cutaneous anesthesia is provided
in Chapter 9.
Excision Margins
Surgical margins vary based on such factors as
tumor type, intent of procedure (diagnostic ver-
sus therapeutic), and tumor size/depth. For basal
cell carcinomas less than 2 cm in diameter
located in low-risk anatomic areas (trunk,
Table 10.2 Antiseptic solutions
Antisepticagent
Advantages Disadvantages
Povidone-iodine Broad spectrum,including fungi
Quickly neutralized by blood, serum proteins, or sputum; irritant; potentialsystemic toxicity with large body surface area
Chlorhexidinegluconate
Prolonged effect Keratitis and otitis
Hexachlorophene Neurotoxicity in infants
Isopropyl alcohol Inexpensive Flammable, must allow it to dry
10 Excision Techniques, Staples, and Sutures 127

extremities), a margin of 4 mm provides a 98%
initial cure rate.29 Larger basal cell carcinomas,
as well as tumors with more aggressive histologic
growth patterns—such as morpheaform and
micronodular tumors—have been shown to
have a much greater degree of subclinical exten-
sion, and thus should be excised with either
greater margins or treated with Mohs micro-
graphic surgery.29–31 Recurrence rates for pri-
marily excised basal cell carcinomas range from
approximately 5–10% at 5 years.32,33 Well-differ-
entiated squamous cell carcinomas less than
2 cm in diameter and located in low-risk ana-
tomic areas excised with a 4-mm margin have a
95% initial clearance rate; however, moderately/
poorly differentiated tumors or tumors greater
than 2 cm in diameter require a 6-mm margin.34
Recurrence is about 8% at 5 years.35 For tumors
in high-risk locations (H-zone of the face, geni-
talia, hand/feet, ears) or very large tumors,
Mohs micrographic surgery may be a better
treatment option due to its higher cure rate.36
Recommendations for the surgical treatment
of melanoma have been made by the National
Comprehensive Cancer Network and are out-
lined in Table 10.337 and further discussed in
Chapter 15.
Specimen Handling
Handling of tissue specimens should be performed
in accordance with the overseeing institution’s poli-
cies. Most specimens should be immediately placed
in formalin to await transport to the lab. To avoid
confusion, it is highly recommended that appropri-
ately labeled containers be prepared prior to the
start of the procedure and that all specimens are
transported directly from patient to jar.
Hemostasis
Obtaining good wound hemostasis is essential for
appropriate field visualization as well as avoidance
of adverse postoperative events. For very small pro-
cedures, simple pressure and suturing may be all that
is needed. However, in general, most excisions pro-
ceedmore smoothlywith the use of an external device
such as a heat cautery unit, hyfrecator, or electrocau-
tery. Heat cautery can be provided either via dispo-
sable handheld units or by a free-standing unit with
sterilizable tips and is a good choice for patients with
pacemakers, implantable cardiac defibrillators, brain
stimulators, or other internal electronic devices as
there is no current that could cause potential inter-
ference. Hyfrecators work via the emission of mono-
terminal, high-voltage, low-amperage current, while
electrocautery units use high-amperage, lower vol-
tage AC electricity to achieve effect (Table 10.4).
Most electrocautery units have ‘‘cut’’ and ‘‘coagula-
tion’’ settings. The ‘‘cut’’ current is a continuous,
lower voltage current producing high levels of heat
that rapidly vaporizes tissue, while the ‘‘coagulation’’
current is a pulsed, higher voltage current that pro-
duces heatmore slowly, leading to blood coagulation
Table 10.3 Recommended surgical margins for melanomaexcision3,7
Melanomadepth
Clinical margin
In situ 5 mm (larger may be required forlentigo maligna)
<1.01–2 mm 1 cm (consider sentinel node)
2.01–4 mm 1–2 cm (consider sentinel node)
>4 mm 2 cm
Table 10.4 Electrosurgical devices
Device Circuit Tissue contact Voltage Amperage
Electrofulguration Monoterminal No High Low
Electrodesiccation Monoterminal Yes High Low
Electrocoagulation Biterminal Yes Low High
Electrosection Biterminal Yes Low High
Electrocautery None Yes Low High
128 M.A. MacCormack

and more diffuse tissue damage.38 Monopolar elec-
trocauteryunits require the use of a ground and entail
passage of electrical current through the patient;
whereas in bipolar electrocautery units the current
should pass only through the tissue placed between
the forceps probe, making it a safer choice for
patients with internal electrical devices.39,40
To obtain hemostasis the wound should first be
blotted with gauze or similar material so that active
sites of bleeding can be identified. The offending
blood vessels can then be treated directly or grasped
with a forceps to which the cautery tip is then
placed. The desired endpoint is a bloodless field,
yet it is important to remember that excessive cau-
tery can delay wound healing and increase risk of
infection. On occasion, some vessels are too large to
be treated with electrocautery and need to be tied
off with suture. As cautery is by its very nature a
destructive process, excessive cautery and treatment
of the skin edge should be avoided.
Suture Materials
Sutures are classified into two major categories:
absorbable and nonabsorbable. Traditionally,
absorbable sutures are used for deep closure and
nonabsorbable sutures are used for epidermal repair;
however, many exceptions to this rule apply. For
example, in situations where suture removal is incon-
venient, absorbable suture such as 6.0 fast absorbing
gut is often used for epidermal closure. The choice of
suture material is largely a matter of physician
preference; the major characteristics of the most
commonly used suture materials are outlined in
Table 10.5.41 As a general rule, the smallest suture
providing adequate tensile strength is preferred.
Wounds closed under significant tension will benefit
from suture that maintains its tensile strength,
whereas in low-tension wounds sited in rapidly heal-
ing areas this is much less of a concern. Overly tight
epidermal sutures, as well as failure to remove epider-
mal sutures in a timely fashion, may lead to the for-
mation of suture marks resulting from epidermal
ingrowth/scarring along the suture line. As a general
rule of thumb, facial sutures should come out within
5–7 days, while sutures on the trunk and extremities
should be removed between days 10 and 14.
Staples
Staples provide a rapid, secure means of wound
closure. While sutures typically allow for more pre-
cise alignment of wound edges, in certain areas such
as the scalp, staples can provide an equivalent or even
slightly improved overall cosmetic outcome.42,43
Staples may provide an alternative for poten-
tially contaminated wounds where delayed pri-
mary closure is not elected.44
A variety of disposable stapler sizes are available.
To place a staple, the stapler tip is firmly placed
perpendicular to the wound edge and the handle
depressed. Staplers typically provide excellent wound
edge eversion; however, if additional eversion is
required an assistant can manually evert the wound
edge using two-toothed Adson forceps prior to staple
discharge. Specialized staple removers enable easy
extraction.
Skin Adhesive
Although typicallymore expensive than suturemate-
rial, skin adhesive (2-Octyl cyanoacrylate) can be an
acceptable choice for closure in low-tension wounds.
When used in conjunction with appropriately placed
subcutaneous sutures, cosmetic outcome has been
shown to be excellent in low-tension repairs.45–49
However, in areas of high mobility or tension, epi-
dermal sutures may be a better choice.50
For proper application of skin adhesive, thewound
should first be completely reapproximated with
subcutaneous sutures. The skin surface is cleaned,
the ampoule crushed, the wound edges manually
everted with forceps, and the adhesive is applied
extending at least 1/2 cm beyond the wound edge,
gradually building up to 3 or 4 layers.
As skin adhesive forms its own dressing, minimal
postoperative care is required. Patients should be
instructed to avoid washing the area too vigor-
ously, as this can result in rapid breakdown of the
adhesive.
10 Excision Techniques, Staples, and Sutures 129

Skin Tape
Various types of skin tapes are available, typically
composed of nonocclusive, microporous material.
While simple tapes such as Steri-Strip1 closures
(3 M, St. Paul, MN) are more often used to pro-
vide additional support to an already closed
wound, more complex products such as ClozeX1
tape (Clozex Medical LLC, Wellesley, MA), an
adhesive film with multiple interlocking filaments
that allow for wound edge approximation, have
been shown to have good effect.51 To obtain best
adhesive results, the skin should be degreased with
alcohol or acetone and Mastisol1 (Ferndale
Laboratories, Ferndale, MI) or tincture of ben-
zoin applied prior to application.
Table 10.5 Suture materials4,1
Suture Filament
type
Tensile strength Inflammatory
response
Absorption Notes
Absorbable
Surgical gut (Plain) Mono 7–10 days ++ 70 days Collagen from sheep/beef
intestine
Surgical gut (Fast
absorbing)
Mono 5–7 days ++ Treated with heat to speed
absorption
Good for low-tension facial
closures, full thickness skin
grafts
Surgical gut
(Chromic)
Mono 10–14 days ++ 90 days Chromium salts slow absorption
and decrease reactivity
Polyglactin 910
(Vicryl)
Braided
Multi
65–75% at
14 days
20–50% at
21 days
10% at
35 days
– Minimal for
45 days,
complete
by 70
days
Rapid absorption once tensile
strength is lost
Poliglecaprone 25
(Monocryl)
Mono 50–60% at
7 days
20–30% at 14
days
0% at 21 days
– 120 days Very pliable, good for
subcuticular closure
Polydioxanone
(PDS II)
Mono 70% at 14 days
50% at 28
days
25% at 42
days
+ 6 months Lower initial tensile strength,
but longer retention providing
extended wound support
Non
absorbable
Silk Braided
Multi
0% by 1 year +++ +/– 2 years Handles well, high reactivity
Good for mucosal areas (soft)
Nylon
(Ethilon)
Mono 81% at 1 year – Slowly
hydrolyzed
Good elasticity, high memory
Polypropylene
(Prolene)
Mono 2 years – – Does not stick to tissue, good for
subcuticular or other
‘‘pullout’’ closures
130 M.A. MacCormack

Closure Techniques
Second Intention
After an excision has been performed it can be left
to heal on its own (second intention healing), which,
while slow, can be an appropriate choice for defects
in areas where primary closure is prohibited due to
lack of tissue mobility and/or concerns regarding
graft take. In certain instances—for example, con-
cavities such as the medial canthus, nasal alar crease
or conchal bowl, as well as for many mucosal sur-
faces—second intention healing can be the closure
of choice providing excellent cosmesis52 (Figs. 10.1
and 10.2). As second intention wounds contract as
they heal, this type of healing should be undertaken
with caution in areas adjacent to free margins such
as the eyelid, nasal alar rim, and lip, as unwanted
tissue distortion may result.
Layered Closures
The vast majority of excisions are closed primarily
and there are a number of techniques available to
achieve closure. The simplest closure consists of
purely epidermal sutures, a type of repair appropri-
ate only for areas with negligible tension. Should
wound tension be present, a layered closure is a
more appropriate choice. Deep dermal sutures func-
tion to close dead space, approximate wound edges,
and provide wound eversion, while epidermal
sutures act to further refine edge alignment. When
placing dermal sutures, use of the ‘‘buried vertical
mattress technique’’ as described by Zitelli andMoy
provides an excellent result due to prolonged der-
mal support and edge eversion.53 While similar to a
traditional dermal suture, this technique is charac-
terized by a few key differences. To begin, the needle
should enter the base of the skin flap through the
subcutaneous fat, head up toward the superficial
dermis and then dive back down to exit the ipsilateral
skin edge at the level of the deep dermis, the opposite
pattern is repeated on the contralateral side and a
buried knot is placed. When drawn together, the
central portion of the wound is raised up forming a
tightly opposed, well-everted wound (Fig. 10.3a).
Some practitioners have found this technique so
effective that they forgo additional epidermal
sutures.54,55 In the rare situation where significant
eversion is not desired, the dermal suture can be
placed in the dermis without the lateral upward arch.
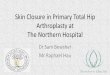
A myriad of techniques exist for epidermal clo-
sure. Simple interrupted sutures provide good
strength and excellent wound edge alignment, but
are considered time consuming by some (Fig. 10.3b).
To be properly placed, the needle should enter the
skin at 90 degrees within 1–2 mm of the wound
edge, the needle should move smoothly through the
dermis and subcutaneous fat to the contralateral side
following the curve of the needle and exiting the skin
in a similar manner. The two ends of suture are
typically tied using an instrument tie. To perform thisFig. 10.2 Healed wound by second intention, 4 weeks afterinitial surgery. Photograph courtesy of SuzanneOlbricht,M.D.
Fig. 10.1 Wound resulting from surgical removal of squa-mous cell carcinoma. Photograph courtesy of SuzanneOlbricht, M.D.
10 Excision Techniques, Staples, and Sutures 131

procedure, a double loop (to help prevent knot slip-
page) should be made around the needle driver tip
utilizing the needle end of the suture. The needle driver
then grasps the short (free) end of the suture and the
two sides are pulled tight. The procedure is then
repeated from the opposite direction to create the
next knot; however, after the first knot is placed, only
a single loop around the needle driver is required.
Depending on the type of suture used, between 3 and
6 knots should be placed to avoid untying (more for
monofilament as opposed to braided suture). Knots
should be tight, but care must be taken to avoid stran-
gulating the skin. One trick is to leave some laxity in
the first 1 or 2 knots to accommodate potential
swelling.
Running epidermal sutures are faster to place, but
sacrifice some precision, run a greater risk of being
pulled too tight leading to tissue strangulation, and are
more vulnerable should the suture break (Fig. 10.3c).
Locked running sutures are similar, allow for slightly
more precision in edge alignment, but carry an even
higher risk of vascular compromise (Fig. 10.3d). Runn-
ing subcuticular sutures are faster to place than simple
interrupted sutures, and with good technique can pro-
vide good wound edge alignment (Fig. 10.3e). Further-
more, if placedwith buried knots and absorbable suture
the need for suture removal is eliminated. Vertical mat-
tress sutures provide excellent wound edge eversion and
are useful in areas, such as the helical rim, where a
depressed scar would be quite visible; however, if not
a)
b)
e)
c)
f)
d)
g)
Fig. 10.3 Various suturetechniques for epidermalclosure (Illustration byAlice Y. Chen)
132 M.A. MacCormack

removed promptly they carry a high risk of leaving
suture marks (Fig. 10.3g). Horizontal mattress sutures
are useful for closing areas under high tension, although
if there is difficulty in edge approximation, an alterna-
tive repair may be a better choice (Fig. 10.3f). High
tension not only increases risk of vascular compromise,
tissue injury, and poor healing, but also significantly
increases risk of scar spread. Even for low-tension
wounds, when tying sutures it is important to use the
minimal amount of tension necessary to obtain edge
approximation.
Description of Procedure
Elliptical Excision
The majority of excisions are elliptical or fusiform
in design, in large part due to ease of closure. By
designing an excision with a length/width ratio of
approximately 3:1 or with apical angles of no more
than 308 (on a flat plane), the likelihood of standing
cone deformities or ‘‘dog ears’’ is markedly reduced,
resulting in a cosmetically elegant flat scar.
When performing excisions on convex areas, the
desired apical angle is often less than 308, whileon a concave surface, apical angles greater than
308 are often well tolerated.
Cosmesis can be further enhanced by orienting the
long axis of the excision parallel to existing skin tension
lines and/or the intersection of two cosmetic units.
When planning an excision, the borders of the tumor
should first be marked, the appropriate margins deli-
neated, and the incision line drawn, taking care to
place the long axis in the most desirable orientation,
as described previously (Figs. 10.4 and 10.5).
Once anesthesia has been obtained, the proce-
dure may begin. The scalpel handle should be held
firmly between the first and second fingers, similar
to a pencil, with the opposing hand used to provide
skin traction.
In general a #15 blade is used; however, in areas
of very thick skin, such as the back, a #10 blade
may be more effective.
Starting at one end of the excision site, the skin
should be scored in a single pass. This is then
repeated on the opposing side, with care being
taken to cleanly incise the tips. Utilizing firm pres-
sure, the skin should then be incised completely
down to subcutaneous tissue using theminimal num-
ber of passes possible (one to two strokes) (Figs. 10.6
and 10.7).
At all times it is important to hold the blade
perpendicular to the skin surface to allow for good
edge approximation later during closure. For most
tumors, excision to the mid to deep subcutaneous
fat is adequate; however, when excising melanoma
the excision should extend down to fascia. After the
excision edges are freed, the specimen is grasped
with forceps and separated from the wound base
by scalpel blade, scissors, or electrosection. To help
maintain an even base, it is helpful to draw the
Fig. 10.4 Elliptical excision, marking margins
Fig 10.5 Elliptical excision, planned incision line
10 Excision Techniques, Staples, and Sutures 133

specimen over the blade or scissors while cutting
(Fig. 10.8). Once freed (Fig. 10.9), the specimen
should immediately be placed in a correctly labeled
container.
Hemostasis should be obtained, if needed, uti-
lizing the techniques described previously to pro-
vide a clear operative field (Fig. 10.10). If the
wound is very small, one can then progress imme-
diately to closure. However, in most cases, wounds
will benefit from undermining as it increases tissue
mobility, decreases tension, and facilitates edge
eversion. The large plate-like scar resulting from
wide undermining may even help in the resolution
of tissue redundancies/dog ear deformities.56 It is
important when undermining to always be aware
of the surrounding anatomy in order to avoid
unwanted injury to adjacent nerves, vessels, or
other structures.
Undermining can be performed via either blunt
dissection or sharp dissection. In blunt dissection,
the wound edge is stabilized in a nontraumatic
manner, such as with a skin hook. A pair of
surgical scissors is inserted with closed blade
Fig. 10.10 Elliptical excision, obtaining hemostasis
Fig. 10.6 Elliptical excision, initial incision
Fig. 10.7 Elliptical excision, incision completed
Fig. 10.8 Elliptical excision, separation from subcutaneoustissue
Fig. 10.9 Elliptical excision, specimen removed
134 M.A. MacCormack

into the wound, parallel to the skin surface. The
blades are then opened, gently separating the sub-
cutaneous tissue. Blunt dissection is a good option
for areas where nerve or vessel injury is a concern
as these structures are often pushed aside rather
than severed. However, blunt dissection can also
lead to an uneven dissection plane and is fre-
quently slower than sharp dissection. In sharp
dissection, either the scalpel blade or one blade
of an open pair of scissors is inserted into
the wound—again parallel to the skin surface—
and the tissue separated either by cutting, pushing
the scissors through the skin in a planing motion,
or blade closure (Fig. 10.11). Sharp undermining
tends to be faster and allows for more control over
the dissection plane. The depth of undermining
varies by anatomic site. In general, undermining
should be performed at the level of the wound
base in the mid to deep subcutaneous fat or
just above the fascial layer, however, exceptions
apply (Table 10.6).57 There are no hard and fast
rules governing the extent of undermining;
each wound must be considered individually with
the goal of creating a tension-free repair.
Once the wound has been completely under-
mined it should be reassessed for hemostasis.
When all active bleeding has been controlled
the wound is ready for sutures. Dermal sutures
are placed first, preferably utilizing the buried
vertical mattress technique as described pre-
viously. It is often helpful to start at the tips
(areas of lower tension), gradually moving in
toward the center (area of highest tension).
Once the dermal sutures are completed, the
wound should appear as a slightly raised ridge
with the skin edges nicely opposed. The dermal
sutures are followed by epidermal sutures, again
utilizing one of the aforementioned techniques
(Figs. 10.12, 10.13, 10.14, 10.15 and 10.16).
A common variation of the classic elliptical exci-
sion gently curves the ends of the incision resulting in
an S-shaped repair. S-plasty closure has the advan-
tage of decreasing wound tension and may often
result in a more esthetically pleasing scar; however,
the resulting scar is often longer than that created by
a traditional elliptical procedure.
Purse-String Repair
An alternative to the elliptical excision is the purse-
string closure. On occasion, high skin tension pre-
vents immediate closure following elliptical exci-
sion, or the long linear scar that would result from
elliptical excision is undesirable. In such cases a disc
excision with purse-string closure may be a more
acceptable alternative. To perform a disc excision
one begins by marking the desired surgical margin
around the excision site. The lesion is then excised in
a circular or disc-like manner leaving a round
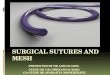
defect. The wound is gently undermined, hemosta-
sis is obtained, and the wound is ready for closure.
Various techniques exist for placing a purse-string
suture. The original publication in the dermatologicFig. 10.11 Elliptical excision, tissue undermining
Table 10.6 Recommended undermining planes
Scalp Subgaleal
Forehead : small Subcutaneous fat
: large Subgaleal
Temple Subcutaneous fat (Need to stayabove superficial temporalfascia to avoid temporal branchCN VII)
Nose Sub-nasalis
Cheek Subcutaneous fat
Jaw/Neck Superficial subcutaneous fat(Avoid marginal mandibularnerve, CN XI)
Trunk/Extremities Deep subcutaneous fat/fascia
Dorsal Hands/Feet
Subdermal
10 Excision Techniques, Staples, and Sutures 135

literature described using a nonabsorbable 3-0 or 4-
0 polypropylene subcuticular suture with an epider-
mal knot at 12 o’clock and escape loops placed at 3,
6, and 9 o’clock.58
The author’s preference for purse-string closure is
to use an absorbable suture, such as Vicryl, placed
horizontally in the mid to deep dermis. As the
suture is drawn together and tied, the wound
becomes puckered, much like the top of a draw-
string purse. Once the wound has been maximally
reapproximated, simple interrupted epidermal
sutures can be placed to further speed healing.
On occasion, it is impossible to close the wound
completely and the central area is closed with a
skin graft or is left to heal by second intention.
Another excellent alternative is to place a purse-
string suture utilizing a nonabsorbable suture,
such as polypropylene, using vertically oriented
bites placed approximately 5–10 mm from the
wound edge. The skin edges can then be further
Fig. 10.14 Elliptical excision, dermal sutures completed
Fig. 10.15 Elliptical excision, epidermal sutures
Fig. 10.16 Elliptical excision, final woundFig. 10.13 Elliptical excision, initial dermal suture tied
Fig. 10.12 Elliptical excision, initial dermal suture
136 M.A. MacCormack

reapproximated using buried vertical mattress
sutures and simple interrupted epidermal
sutures59,60 (Figs. 10.17–10.24). All nonabsorbable
sutures should be removed at 5–7 days for facial
wounds and 10–14 days for nonfacial repairs. The
wound will continue to display moderate pleating at
Fig. 10.17 Purse-string closure, margin marked
Fig. 10.18 Purse-string closure, margin incised
Fig. 10.19 Purse-string closure, undermining
Fig. 10.20 Purse-string closure, purse-string suture of 4.0Prolene placed
Fig. 10.21 Purse-string closure, purse-string suture tied
Fig. 10.22 Purse-string closure, further edge approximation
10 Excision Techniques, Staples, and Sutures 137

the time of suture removal; however, as long as the
wound is in an area of moderate tension these skin
folds almost always resolve.
Standing Cones (Dog Ears)
On occasion, after elliptical excision the wound
continues to exhibit vertical elevations at the tips
or ‘‘dog ears.’’ Many factors can contribute to the
formation of tissue redundancies including initial
apical angles greater than 308, inadequate under-
mining, failure to maintain a 90-degree incision
angle, or unequal side lengths. When an excision
borders a free margin, such as the lip or ala, such
tissue redundancy presents not as a vertical eleva-
tion, but rather as a pushing distortion of that mar-
gin. Small dog ears, especially in areas of high ten-
sion/tissue mobility, such as the dorsal hand, will
often resolve on their own. Larger redundancies,
however, are often best resolved at the time of the
initial procedure. One of the easiest means of reso-
lution is simply by wound extension. While holding
the redundancy steady, an incision can be made
through the center of the standing cone to its base.
After careful undermining, the two resulting trian-
gular halves can be laid across the initial incision
line and neatly trimmed (Figs. 10.25–10.30). As one
becomes more proficient in dog ear management, it
becomes clear that by utilizing the same principles
the tissue redundancy can be removed from almost
any direction. The same technique can be applied
when performing immediate linear closure follow-
ing disc excision. In fact, this method of surgical
removal has been demonstrated to result in overall
shorter scar lengths than those seen with preplanned
ellipses.61
If a difference in wound edge lengths is appre-
ciated prior to closure it can often be dealt with via
‘‘the rule of halves.’’ The first suture is placed in the
midportion of each side and the wound bisected.
The process is repeated—continuing to divide the
unsutured areas in half until the wound is closed—
ultimately resulting in a curvilinear repair.
An excellent review of dog ear management has
been published by Weisburg, Nehal, and Zide.62
Postprocedure Care
Wound dressings serve a number of functions.
Not only do they act to keep the wound clean
and protected from unwanted exposure, they
also act to provide pressure, limiting postopera-
tive bleeding complications and can help support
and stabilize the wound. While small procedures
require little more than daily cleansing followed
by application of ointment (such as petrolatum
or topical antibiotic) covered by gauze, larger
procedures often benefit from a more substantial
dressing. Many patients prefer a ‘‘leave-on’’
Fig. 10.23 Purse-string closure, final repair
Fig. 10.24 Purse-string closure, 4-month outcome
138 M.A. MacCormack

bandage that requires no wound care on the part
of the patient. One such example is to begin by
applying a thin layer of ointment over the
wound edge. Steri-Strips held in place with
liquid adhesive are then placed perpendicular to
the wound to further enhance edge support. The
next layer is an absorptive material such as a
hydrocolloid (i.e., Cutinova-Hydro1, Smith &
Fig. 10.26 Cutaneous redundancy, initial incision
Fig. 10.27 Cutaneous redundancy, tissue overlap
Fig. 10.28 Cutaneous redundancy, second incision
Fig. 10.29 Cutaneous redundancy, dog ear removed
Fig. 10.30 Cutaneous redundancy, final wound
Fig. 10.25 Cutaneous redundancy
10 Excision Techniques, Staples, and Sutures 139

Nephew, London, UK) trimmed to fit the exci-
sion line, which is in turn covered by a breath-
able, waterproof film (i.e., Tegaderm1, 3 M)
allowing the patient to shower. On top of all of
this is a pressure dressing composed of gauze
and tape, which is removed by the patient at
24–48 h.
Complications
When properly performed, surgical excisions
have a very low complication rate. All patients
should be informed preprocedure that some sort
of scarring is inevitable and localized cutaneous
numbness is not uncommon due to transaction of
sensory nerves. With time, typically within 1
year, sensation often returns to normal, and
scar cosmesis can be enhanced via proper plan-
ning and orientation. Appropriate knowledge
of surgical anatomy can prevent inadvertent
injury to surrounding vessels and nerves as well
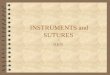
as tissue distortion. Allergic reactions to topical
antibiotics, dressing materials, or adhesive tape
(Fig. 10.31) are not uncommon and can be easily
addressed by removal of the offending agent and
application of a mild topical steroid. Wound
infection occurs in less than 2% of cases and is
often heralded by an increase in pain63,64 (Fig.
10.32). Risk can be minimized by use of good
sterile technique and appropriate wound care.
Should infection occur, the wound should be
cultured, drained if necessary, and the patient
started on a suitable antibiotic. Bleeding compli-
cations occur in about 3% of cases, but careful
attention to intraoperative hemostasis as well as
use of a good pressure dressing for the first 24–
48 h following the procedure can help to decrease
this risk64 (Fig. 10.33). Wound dehiscence can
occur as a result of excessive wound tension,
hematoma formation, or infection. In such cases
the underlying issue should be addressed and the
wound then allowed to heal by second intention.
Once healed, the scar can be revised, if necessary.
For further discussion on surgical complications
see Chapter 12.
Fig. 10.31 Allergic contact dermatitis to adhesive
Fig. 10.32 Postoperativewound infection
Fig. 10.33 Postoperative hematoma
140 M.A. MacCormack

Summary
Excision remains one of the most frequently per-
formed dermatologic procedures. As time goes on,
advances such as improved topical anesthetics or
the use of confocal microscopy to help better deline-
ate tumor margins may improve patient comfort
and treatment efficacy. However, for the foresee-
able future cutaneous excisions will remain one of
the mainstays of surgical dermatology.
References
1. Shaffer CL, Feldman SR, Fleischer AB Jr et al. Thecutaneous surgery experience of multiple specialties inthe Medicare population. J Am Acad Dermatol. 2005;52(6):1045–1048.
2. Chang LK, Whitaker DC. The impact of herbal medi-cines on dermatologic surgery. Dermatol Surg. 2001;27(8):759–763.
3. Ang-Lee MK, Moss J, Yuan CS. Herbal medicines andperioperative care. JAMA. 2001;286(2):208–216.
4. Heller J, Gabbay JS, Ghadjar K, et al. Top-10 list ofherbal and supplemental medicines used by cosmeticpatients: what the plastic surgeon needs to know.Plast Reconstr Surg. 2006;117(2):436–445; discussion446–437.
5. Lewis KG, Dufresne RG Jr. A meta-analysis of compli-cations attributed to anticoagulation among patientsfollowing cutaneous surgery. Dermatol Surg. 2008;34(2):160–164; discussion 4–5.
6. Khalifeh MR, Redett RJ. The management of patientson anticoagulants prior to cutaneous surgery: case reportof a thromboembolic complication, reviewof the literature,and evidence-based recommendations. Plast ReconstrSurg. 2006;118(5):110e–117e.
7. Syed S, Adams BB, Liao W, et al. A prospective assess-ment of bleeding and international normalized ratio inwarfarin-anticoagulated patients having cutaneous sur-gery. J Am Acad Dermatol. 2004;51(6):955–957.
8. Alam M, Goldberg LH. Serious adverse vascular eventsassociated with perioperative interruption of antiplateletand anticoagulant therapy. Dermatol Surg. 2002;28(11):992–998; discussion 8.
9. Otley CC, Fewkes JL, Frank W, et al. Complications ofcutaneous surgery in patients who are taking warfarin,aspirin, or nonsteroidal anti-inflammatory drugs. ArchDermatol. 1996;132(2):161–166.
10. Wilson W, Taubert KA, Gewitz M, et al. Prevention ofinfective endocarditis: guidelines from the American HeartAssociation: a guideline from theAmericanHeart Associa-tion Rheumatic Fever, Endocarditis, afsnd Kawasaki Dis-ease Committee, Council on Cardiovascular Disease in theYoung, and the Council on Clinical Cardiology, Councilon Cardiovascular Surgery and Anesthesia, and the
Quality of Care and Outcomes Research InterdisciplinaryWorking Group. Circulation. 2007;116(15):1736–1754.
11. Antibiotic prophylaxis for dental patients with total jointreplacements. J Am Dent Assoc. 2003;134(7):895–899.
12. Roberts GJ, Gardner P, Simmons NA. Optimum sam-pling time for detection of dental bacteraemia in chil-dren. Int J Cardiol. 1992;35(3):311–315.
13. Sakamoto H, Karakida K, Otsuru M, et al. Antibioticprevention of infective endocarditis due to oral proce-dures: myth, magic, or science? J Infect Chemother. 2007;13(4):189–195.
14. Carmichael AJ, Flanagan PG, Holt PJ, et al. The occur-rence of bacteraemia with skin surgery. Br J Dermatol.1996;134(1):120–122.
15. Sabetta JB, Zitelli JA. The incidence of bacteremia dur-ing skin surgery. Arch Dermatol. 1987;123(2):213–215.
16. Babcock MD, Grekin RC. Antibiotic use in dermatolo-gic surgery. Dermatol Clin. 2003;21(2):337–348.
17. Hurst EA, Grekin RC, Yu SS, et al. Infectious complica-tions and antibiotic use in dermatologic surgery. SeminCutan Med Surg. 2007;26(1):47–53.
18. Garland JS, Buck RK, Maloney P, et al. Comparison of10% povidone-iodine and 0.5% chlorhexidine gluconatefor the prevention of peripheral intravenous cathetercolonization in neonates: a prospective trial. PediatrInfect Dis J. 1995;14(6):510–516.
19. Hibbard JS. Analyses comparing the antimicrobial activ-ity and safety of current antiseptic agents: a review. JInfus Nurs. 2005;28(3):194–207.
20. Nishimura C. Comparison of the antimicrobial efficacyof povidone-iodine, povidone-iodine-ethanol and chlor-hexidine gluconate-ethanol surgical scrubs. Dermatol-ogy. 2006;212(Suppl 1):21–25.
21. Hibbard JS, Mulberry GK, Brady AR. A clinical studycomparing the skin antisepsis and safety of ChloraPrep,70% isopropyl alcohol, and 2% aqueous chlorhexidine.J Infus Nurs. 2002;25(4):244–249.
22. MICROMEDEX1 Healthcare Series. In: POISIN-DEX1 Managements: Thomson Micromedex; 2008.http://www.micromedex.com/products/poisindex/
23. LalondeD, BellM, Benoit P, et al. Amulticenter prospec-tive studyof3,110 consecutive cases of elective epinephrineuse in the fingers and hand: the Dalhousie Project clinicalphase. J Hand Surg [Am]. 2005;30(5): 1061–1067.
24. Denkler K. A comprehensive review of epinephrine inthe finger: to do or not to do. Plast Reconstr Surg.2001;108(1):114–124.
25. Thomson CJ, Lalonde DH, Denkler KA, et al. A criticallook at the evidence for and against elective epinephrine usein the finger. Plast Reconstr Surg. 2007;119(1):260–266.
26. Dzubow LM. Optimizing local anesthesia. The heat ison. Dermatol Surg. 1996;22(8):681.
27. Golembiewski J. Local anesthetics. J Perianesth Nurs2007;22(4):285–288.
28. Burns CA, Ferris G, Feng C, et al. Decreasing the pain oflocal anesthesia: a prospective, double-blind comparisonof buffered, premixed 1% lidocaine with epinephrineversus 1% lidocaine freshly mixed with epinephrine. JAm Acad Dermatol. 2006;54(1):128–131.
29. Wolf DJ, Zitelli JA. Surgical margins for basal cell carci-noma. Arch Dermatol. 1987;123(3):340–344.
10 Excision Techniques, Staples, and Sutures 141

30. Breuninger H, Dietz K. Prediction of subclinical tumorinfiltration in basal cell carcinoma. J Dermatol SurgOncol. 1991;17(7):574–578.
31. Salasche SJ, Amonette RA. Morpheaform basal-cellepitheliomas: a study of subclinical extensions in a seriesof 51 cases. J Dermatol Surg Oncol. 1981;7(5):387–394.
32. Silverman MK, Kopf AW, Bart RS, et al. Recur-rence rates of treated basal cell carcinomas. Part3: surgical excision. J Dermatol Surg Oncol.1992;18(6):471–476.
33. Rowe DE, Carroll RJ, Day CL Jr. Long-term recurrencerates in previously untreated (primary) basal cell carci-noma: implications for patient follow-up. J DermatolSurg Oncol. 1989;15(3):315–328.
34. Brodland DG, Zitelli JA. Surgical margins for excisionof primary cutaneous squamous cell carcinoma. J AmAcad Dermatol. 1992;27(2 Pt 1):241–248.
35. Alam M, Ratner D. Cutaneous squamous-cell carci-noma. N Engl J Med 2001;344(13):975–983.
36. Leibovitch I, Huilgol SC, Selva D, et al. Cutaneoussquamous cell carcinoma treated with Mohs micro-graphic surgery in Australia I. Experience over 10years. J Am Acad Dermatol. 2005;53(2):253–260.
37. National Comprehensive Cancer Network (NCCN) clin-ical practice guidelines in oncology: melanoma. In: v.1.2008 ed. http://www.nccn.org%3F/. Accessed January19, 2009.
38. Pollack SV. Electrosurgery of the Skin. New York:Churchill Livingstone; 1991.
39. Martinelli PT, Schulze KE, Nelson BR. Mohs micro-graphic surgery in a patient with a deep brain stimulator:a review of the literature on implantable electricaldevices. Dermatol Surg. 2004;30(7):1021–1030.
40. Yu SS, Tope WD, Grekin RC. Cardiac devices andelectromagnetic interference revisited: new radiofre-quency technologies and implications for dermatologicsurgery. Dermatol Surg. 2005;31(8 Pt 1):932–940.
41. Ethicon Wound Closure Manual, Somerville, NJ, Ethi-con 2007. http://www.jnjgateway.com/public/NLDUT/Wound_Closure_Manual1.pdf. Last accessed October29, 2008.
42. Kanegaye JT, Vance CW, Chan L, et al. Comparison ofskin stapling devices and standard sutures for pediatricscalp lacerations: a randomized study of cost and timebenefits. J Pediatr. 1997;130(5):808–813.
43. Khan AN, Dayan PS, Miller S, et al. Cosmetic outcomeof scalp wound closure with staples in the pediatricemergency department: a prospective, randomized trial.Pediatr Emerg Care. 2002;18(3):171–173.
44. Stillman RM, Marino CA, Seligman SJ. Skin staples inpotentially contaminated wounds. Arch Surg. 1984;119(7):821–822.
45. Sniezek PJ, Walling HW, DeBloom JR 3rd, et al. Arandomized controlled trial of high-viscosity 2-octyl cya-noacrylate tissue adhesive versus sutures in repairingfacial wounds following Mohs micrographic surgery.Dermatol Surg. 2007;33(8):966–971.
46. Quinn J, Wells G, Sutcliffe T, et al. A randomized trialcomparing octylcyanoacrylate tissue adhesive andsutures in the management of lacerations. JAMA.1997;277(19):1527–1530.
47. Holger JS, Wandersee SC, Hale DB. Cosmetic outcomesof facial lacerations repaired with tissue-adhesive,absorbable, and nonabsorbable sutures. Am J EmergMed. 2004;22(4):254–257.
48. Toriumi DM, O’Grady K, Desai D, et al. Use of octyl-2-cyanoacrylate for skin closure in facial plastic surgery.Plast Reconstr Surg. 1998;102(6):2209–2219.
49. Coulthard P, Worthington H, Esposito M, et al. Tissueadhesives for closure of surgical incisions. CochraneDatabase Syst Rev. 2004;2:CD004287.
50. Bernard L, Doyle J, Friedlander SF, et al. A prospectivecomparison of octyl cyanoacrylate tissue adhesive (der-mabond) and suture for the closure of excisional woundsin children and adolescents. Arch Dermatol. 2001;137(9):1177–1180.
51. Kuo F, Lee D, Rogers GS. Prospective, randomized,blinded study of a new wound closure film versus cuta-neous suture for surgical wound closure. Dermatol Surg.2006;32(5):676–681.
52. Leonard AL, Hanke CW. Second intention healing forintermediate and large postsurgical defects of the lip. JAm Acad Dermatol. 2007;57(5):832–835.
53. Zitelli JA, Moy RL. Buried vertical mattress suture. JDermatol Surg Oncol 1989;15(1):17–19.
54. Sadick NS, D’Amelio DL, Weinstein C. The modifiedburied vertical mattress suture: a new technique of buriedabsorbable wound closure associated with excellentcosmesis for wounds under tension. J Dermatol SurgOncol. 1994;20(11):735–739.
55. Hohenleutner U, Egner N, Hohenleutner S, et al. Intra-dermal buried vertical mattress suture as sole skin clo-sure: evaluation of 149 cases. Acta Derm Venereol.2000;80(5):344–347.
56. Zitelli JA. TIPS for a better ellipse. J Am Acad Dermatol.1990;22(1):101–103.
57. Boyer JD, Zitelli JA, Brodland DG. Underminingin cutaneous surgery. Dermatol Surg. 2001;27(1):75–78.
58. Brady JG, Grande DJ, Katz AE. The purse-string suturein facial reconstruction. J Dermatol Surg Oncol.1992;18(9):812–816.
59. Hoffman A, Lander J, Lee PK. Modification of thepurse-string closure for large defects of the extremities.Dermatol Surg. 2008;34(2):243–245.
60. Weisberg NK, Greenbaum SS. Revisiting the purse-string closure: some new methods and modifications.Dermatol Surg. 2003;29(6):672–676.
61. Hudson-Peacock MJ, Lawrence CM. Comparison ofwound closure by means of dog ear repair and ellip-tical excision. J Am Acad Dermatol. 1995;32(4):627–630.
62. Weisberg NK, Nehal KS, Zide BM. Dog-ears: a review.Dermatol Surg. 2000;26(4):363–370.
63. Rogues AM, Lasheras A, Amici JM, et al. Infectioncontrol practices and infectious complications in der-matological surgery. J Hosp Infect. 2007;65(3):258–263.
64. Amici JM, Rogues AM, Lasheras A, et al. A prospectivestudy of the incidence of complications associatedwith dermatological surgery. Br J Dermatol.2005;153(5):967–971.
142 M.A. MacCormack