Embed Size (px)
Citation preview
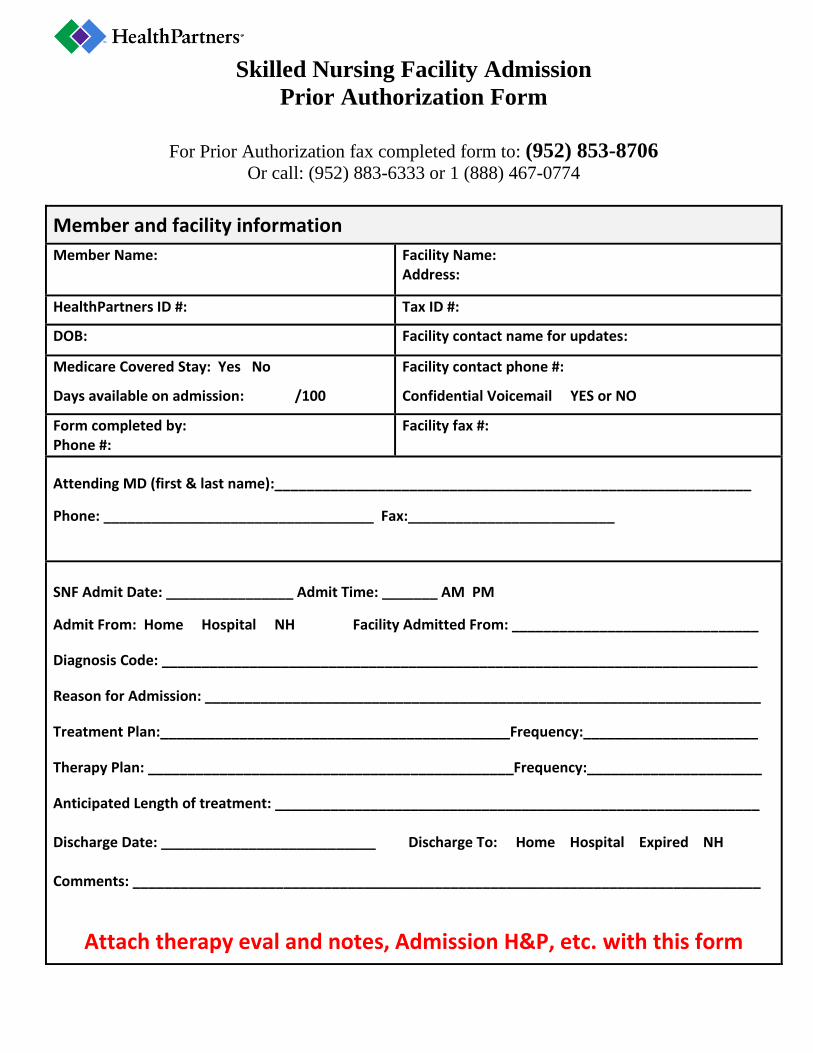
Skilled Nursing Facility Admission
Prior Authorization Form
For Prior Authorization fax completed form to: (952) 853-8706
Or call: (952) 883-6333 or 1 (888) 467-0774
Member and facility information
Member Name:
Facility Name: Address:
HealthPartners ID #: Tax ID #:
DOB: Facility contact name for updates:
Medicare Covered Stay: Yes No
Days available on admission: /100
Facility contact phone #:
Confidential Voicemail YES or NO
Form completed by: Phone #:
Facility fax #:
Attending MD (first & last name):____________________________________________________________
Phone: __________________________________ Fax:__________________________
SNF Admit Date: ________________ Admit Time: _______ AM PM
Admit From: Home Hospital NH Facility Admitted From: _______________________________
Diagnosis Code: ___________________________________________________________________________
Reason for Admission: ______________________________________________________________________
Treatment Plan:____________________________________________Frequency:______________________
Therapy Plan: ______________________________________________Frequency:______________________
Anticipated Length of treatment: _____________________________________________________________ Discharge Date: ___________________________ Discharge To: Home Hospital Expired NH Comments: _______________________________________________________________________________
Attach therapy eval and notes, Admission H&P, etc. with this form





























