Embed Size (px)
Citation preview

Skeletal Muscle RelaxantsSkeletal Muscle Relaxants
1
Dr. Rene AnandReference: Bertram Katzung et al, "Basic and Clinical Pharmacology", 12th edition, McGraw-Hill Lange, Chapter 27

Learning Objectives
Describe the pharmacological properties of drugs classified as relaxants
Describe the transmission process at the skeletal neuromuscular end plate and the points at which drugs modify this process
Identify the major non-depolarizing neuromuscular blockers and one depolarizing neuromuscular blocker, compare their pharmacokinetics
Describe the differences between depolarizing and non-depolarizing blockers from the standpoint of tetanic and post-tetanic twitch strength
Describe the reversal of non-depolarizing blockade List drugs for treatment of skeletal muscle spasticity and identify
their sites of action and adverse effects

Skeletal Muscle Relaxants
Skeletal muscle relaxants interfere with the contraction of skeletal muscles:
1. Neuromuscular blockers are used to completely paralyze skeletal muscle during surgical and orthopedic procedures in the controlled environment of a hospital.
2. Spasmolytics are used to elicit a more modulatory effect on muscle contraction and do not completely block the activity of the skeletal musculature. These agents are used to reduce muscle spasms and are commonly used in ambulatory patients.
3

Classification of Skeletal Muscle RelaxantsClassification of Skeletal Muscle Relaxants
Peripherally acting drugs Neuromuscular blocking drugs. Direct acting spasmolytic.
Centrally acting spasmolytics.
4

I Summary of Neuromuscular TransmissionI Summary of Neuromuscular Transmission
An action potential depolarizes the nerve
terminal and Ca2+ enters. ACh-containing vesicles
fuse with the prejunctional membrane releasing the
ACh by exocytosis into the junctional space.
The released ACh diffuses across the synaptic gap and
binds to nicotinic (Nm) receptors leading to
depolarization of the muscle end-plate region. The nicotinic receptor is a complex of 5 protein
subunits. There are 2 a subunits, and one each of b,
g and d subunits in embryonic muscle. In the adult d is replaced by an e
subunit. When one molecule of ACh binds to each of the
a subunits there is an increase of the fluxes of
Na+ in, Ca2+ in, and K+ out.
5
II Summary of Neuromuscular TransmissionII Summary of Neuromuscular Transmission
There is propagation of a muscle action potential through the conducting
system of the myofibrils, with release of Ca2+ from the
sarcoplasmic reticulum. This triggers off the troponin-
actin-myosin interaction and muscle contraction.
Relaxation is associated with restorage of Ca2+ in the
sarcoplasmic reticulum which is driven by energy supplied
by an ATPase. There is a refractory period until
repolarization of the muscle end-plate.
ACh is inactivated by ACh esterase (AChE).
6

Quick Review: Model of Nicotinic ReceptorQuick Review: Model of Nicotinic Receptor
7
Quick Review

Quick Review Quick Review

Curare
Curare is a generic term that refers to a mixture of naturally occurring alkaloids found in various South American plants and is used to make arrow poison by some South American Indians. The most important alkaloid is d-tubocurarine. First used in surgery in 1942.
9
http://waynesword.palomar.edu/ecoph23.htm

Peripherally acting drugsPeripherally acting drugs
Neuromuscular Blocking DrugsChemically most are bisquaternary ammonium compounds
Interaction with the acetylcholine (ACh) receptor appears to be one to one but the exact nature is unknown. It is speculated that the charged compounds span and bind to the nicotinic (Nm) receptor and prevent ACh from reaching it.
-N+______________N+-
+
- -
- -Pancuronium

Characteristics of quaternary compoundsconsidering their positive charge Characteristics of quaternary compoundsconsidering their positive charge
Poorly absorbed from the gut and generally rapidly
excreted
Will not cross the
blood-brain barrier
Will not cross the placenta
Administered IV
11
Indications for Neuromuscular Blocking DrugsIndications for Neuromuscular Blocking Drugs
Adjunct for surgery to
reduce muscle tone and
fasciculation at the site of
surgery (permit tracheal
intubation).
Electroshock therapy for psychiatric disorders
(prevent bone breakage).
Control convulsive
disorders (status epilepticus,
tetanus, eclampsia and
toxic reactions to local
anesthetics).
Control respiration when
the patient is unable to
ventilate.
12

Classification of Neuromuscular Blocking DrugsClassification of Neuromuscular Blocking Drugs
Nondepolarizing Blocking Drugs
(competitive, stabilizing, or
antidepolarizing drugs).
Depolarizing Blocking Drugs.
13

1. Nondepolarizing Blocking Drugs1. Nondepolarizing Blocking Drugs
Block neuromuscular
junction nicotinic receptors
competitively. They compete for the receptor with
ACh.
14
I Classification of some neuromuscular blocking agents based on duration of actionI Classification of some neuromuscular blocking agents based on duration of action
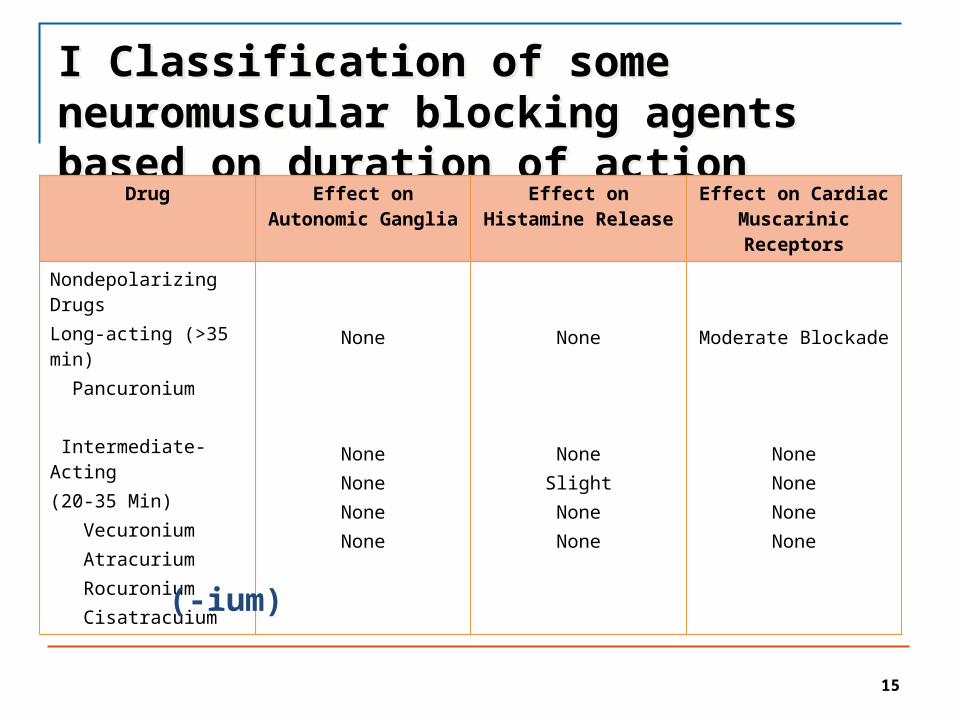
Drug Effect on Autonomic Ganglia
Effect on Histamine Release
Effect on Cardiac Muscarinic Receptors
Nondepolarizing DrugsLong-acting (>35 min) Pancuronium Intermediate-Acting (20-35 Min) Vecuronium Atracurium Rocuronium Cisatracuium
None
NoneNoneNoneNone
None
NoneSlightNoneNone
Moderate Blockade
NoneNoneNoneNone
15
(-ium)

Nondepolarizing Blocking DrugsNondepolarizing Blocking Drugs
Because they are competitive
blockers their action can be reversed by
increasing the concentration of
endogenous ACh at the NMJ.
Use ChE inhibitors such as
neostigmine, physostigmine, edrophonium together with
atropine to protect muscarinic
receptors against excessive
stimulation by increased levels of
ACh.
16

II Classification of some neuromuscular blocking agents based on duration of actionII Classification of some neuromuscular blocking agents based on duration of action
Drug Effect on Autonomic
Ganglia
Effect on Histamine Release
Effect on Cardiac
Muscarinic Receptors
Depolarizing DrugsShort-Acting (5-15 min) Succinylcholine
Stimulation Slight Stimulation
17
Succinylcholine (Anectine®) structurally looks like two molecules of ACh end-to-end. It is a relatively short duration (5-15 min) ACh-like agonist at nicotinic receptors.
Progression of pharmacological response to succinylcholineProgression of pharmacological response to succinylcholine
• Initial depolarization of the end-plate region. Transient muscle fasciculation followed by relaxation.
Phase 1
Block.
• Desensitization of the receptor to ACh. End-plate repolarization possibly do to conformational change of the receptor molecule.
Phase 2
Block.
18
Note. Cholinesterase inhibitors will intensify the response to succinylcholine during Phase 1 block. They may reinitiate muscle contraction if administered during late Phase 2 block.

Metabolism of succinylcholineMetabolism of succinylcholine
19
ACh
(CH3)3-N-CH2-CH2-O-OC-CH3
Succinylcholine
(CH3)3-N-CH2-CH2-O-OC-CH2-CH2-CO-O-CH2-CH2-N-(CH3)3
plasma ChE
succinylmonocholine 1/2 activity
plasma ChE
succinic acid + choline
Note. ACh metabolism takes place primarily in the NMJ, while succinylcholine metabolism takes place in the plasma
+
+ +
Plasma ChE
Plasma ChE is synthesized in the liver and therefore patients with liver dysfunction, decreased hepatic blood flow or genetic abnormalities would show prolonged responses to succinylcholine. Neonates have low plasma ChE. A clinical dose of 1-2 mg/kg usually lasts <15 min while an atypical patient may respond for >2 hr. • About 1:3000 patients have a genetic related decrease of
plasma ChE.• Treatment- mechanical respiration
20

I Adverse Effects of neuromuscular blocking drugsI Adverse Effects of neuromuscular blocking drugs
Do not enter brain - CNS fully functional, pain is not dulled.
Depolarizing Drug (Succinylcholine)
Fasciculation can result in:• Post operative muscle stiffness and pain.• Increase of intraocular pressure-contraction of the extraocular
muscles.• Increased intragastric pressure – occasionally leading to emesis.• Hyperkalemia – in some patients especially with burns, nerve
damage, closed head injury, renal failure.
21

II Adverse Effects of neuromuscular blocking drugsII Adverse Effects of neuromuscular blocking drugs
Nondepolarizing Drugs
• Atracurium (occasionally succinylcholine)
Release of endogenous histamine into the circulation- bronchospasm, increased excretions, vasodilation resulting in decreased blood pressure.
• Treatment - antihistamines
Pharmacological response Potentiated by:
Some general anesthetics (methoxyflurane) and local anesthetics.
Antibiotics (aminoglycosides; neomycin and streptomycin have a tendency to inhibit Ca2+ fluxes).
Fluid and electrolyte imbalance.
22

Direct-Acting (myotropic) Spasmolytics Direct-Acting (myotropic) Spasmolytics
Dantroline
• Interferes with release of Ca2+ from the sarcoplasmic reticulum which is required for muscle contraction.
Indications
• Chronic disorders characterized by muscle spasms.• Spinal cord injury• Stroke• Cerebral palsy• Multiple sclerosis• ( Potential toxicity: Hepatotoxicity)
Malignant Hyperthermia: Genetic disorder, autosomal dominant. Triggered by halogenated anesthetic and/or succinylcholine. Sudden rise of Ca2+ in muscle fiber with increase of body temperature, rigidity.- 50% mortality.
23

I Centrally Acting Spasmolytics Antispastic action
24
Exerted mainly on the spinal cord by inhibiting mono- and poly-synaptic activation of motor neurons.
Baclofen. GABAB receptor agonist. Activates GABAB receptors on nerve endings that release excitatory neurotransmitters and prevents the release of the excitatory neurotransmitters (glutamate) onto motor neurons.
Diazepam. Belongs to the benzodiazepine class of drugs. Enhances the actions of the inhibitor neurotransmitter GABA in the spinal cord.
Indications: Chronic disorders characterized by muscle spasticity.
• spinal cord injury• stroke• cerebral palsy• multiple sclerosis
Side effects: Sedation and drowsiness

II Centrally Acting SpasmolyticsII Centrally Acting Spasmolytics
Tizanidine.
• Mechanism of action is unclear. • Derivative of clonidine and has significant α2- adrenoceptive
agonist activity. • Appears to reinforce pre- and postsynaptic inhibition in the
cord. • Also inhibits nociceptive transmission in the cord.
Indications:• Chronic disorders characterized by muscle spasticity.
Side effects: Sedation, drowsiness, hypotension, dry mouth, and asthenia.
25

26
I Drugs used for acute local muscle spasmI Drugs used for acute local muscle spasm
There are a large number of sedative
drugs that are promoted for the relief of acute
temporary muscle spasm caused by local
trauma or strain.
The drugs include: • Carisoprodol • Chlorzoxazone • Cyclobenzaprine • Metaxalone • Orphenadrine
Side effects: Most are sedative
hypnotics and some have
antimuscarininc activity.

II Drugs used for acute local muscle spasmII Drugs used for acute local muscle spasm
Botulinum Toxin • Inhibits the release of
ACh from cholinergic nerve terminals.
• Local injection is finding increasing use in the treatment of spastic disorders due to neurologic injury.
• Benefits may persist for weeks after a single injection.
Potential toxicity• May spread beyond
injection site and lead to difficulty swallowing and breathing.
27

Botulinum Toxin (Types A-G).
Botulinum Toxin (Types A-G).
The heavy chain is similar for all types,
the light chains differ.

Botox approved to treat:Botox approved to treat:
Strabismus (Cross-eyes)
Uncontrollable blinking
Cervical dystonia (a neurological disorder that
causes severe neck and shoulder
contractions)
Moderate to severe frown lines
between eyebrows
Unintended consequence: Appears to be
effective for the treatment of some forms of headache
29

Muscle Relaxants Quiz
30

Summary of Key Points to Remember
Two therapeutic groups of muscle relaxants:
A. Neuromuscular blockers (nondepolarizing and depolarizing)
- Act on nicotinic acetylcholine receptors at neuromuscular junction
- Used in surgical relaxation, endotracheal intubation, control of ventilation and treatment of convulsions
B. Spasmolytics (typically act on targets in the spinal chord)
- Used to treat spasticity associated cerebral palsy, multiple sclerosis, and stroke
31

Thank you for completing this module
Reference: Bertram Katzung et al, "Basic and Clinical Pharmacology",
12th edition, McGraw-Hill Lange, Chapter 27
Email: [email protected]

Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey





























