Embed Size (px)
Citation preview

- 75 -
Skeletal Muscle Pathology after Spinal Cord Injury: Our 20 YearExperience and Results on Skeletal Muscle Changes in Paraple-gics, Related to Functional Rehabilitation
Roberto Scelsi
Department of Human and Hereditary Pathology, University of Pavia, Pavia, Italy
AbstractThe present review on 20-year-experience on paralyzed skeletal muscle in paraplegics aftertraumatic spinal cord injury (SCI), reports changes in muscle fibres and microvasculatureseen after morphological, morphometric and ultrastructural studies on open and needlebiopsies. The changes were correlated with the time elapsed from SCI (1-17 months). Hi-stopathological and enzyme-histochemical changes in muscle fibres were seen first after 1month and increased thereafter. In all stages post SCI, paraplegics showed myopathic alte-rations, increase in the sarcoplasmic lipid contents and incidental denervation patterns. Themain ultrastructural changes regard the myofibrillar apparatus and mitochondria. Probably afibre type shifting to type 2 fibres occurs precociously, but only 7-8 months after SCI it iswell manifested. The blood vessel qualitative and quantitative changes in paraplegics re-gard small vessels and capillaries and they may be important causes of the myopathic alte-rations in paraplegics. The influence of disuse and spasticity on morphological fibre andcapillary modifications in paraplegics is reviewed and discussed. The knowledge of themuscle condition and of plastic capacities for fibre type shifting in paraplegics is importantto oppose complications of SCI and to choice of an appropriate rehabilitative program di-rected to prevention of changes associated to disuse, spasticity and vascular damage.Key words: fiber types, microvasculature, mitochondria, MHC, pathology, skeletal muscle,spinal cord injury.
Basic Appl Myol 11 (2): 75-85, 2001
Following spinal cord injury (SCI), upper motor neu-ron paralyzed muscles show widespread disuse atrophyand spasticity. In setting out a rehabilitation program ofpatients with motor disease it is necessary to evaluatethe condition of the kinetic units, i.e. of the osteo-articular segments and of the related skeletal musclegroups. Experimental and clinical studies, and strategiesrelated to rehabilitation of paraplegics as the muscularelectric stimulation (FES) and the application of the me-chanic orthoses, are directed toward the recovery of themuscle contractile properties and of the standing posi-tion or walking. These conditions are important in thepreservation of the blood circulation in the paralyzedlimb, of the Ca content in bones, of the renal functionand for the reduction of spasticity and contractions inparaplegic patients.
However, the results of the functional and morphologi-cal changes of the muscle following SCI may conditionthe choice of the rehabilitative program in paraplegics.
In the last decades, many important experimental andapplied studies were performed on the skeletal musclein paraplegics following SCI, indicating markedchanges in the muscle morphology and in their meta-bolic and contractile properties, and details on the plas-ticity of the muscle in the present condition. These al-terations are well documented in animals, after experi-mental cord lesion [18, 32], and in humans, generally aftertraumatic cord lesions [3, 14, 15, 23, 31, 33, 50].
Our study group, in association with the Centre ofFunctional Recovery of paraplegics of Villanova sul-l’Arda (Pc), widely contribute to the morphologicaldocumentation of changes in different skeletal musclesand of related pathologies in paraplegics, as the micro-circulatory alterations and the heterotopic ossifications[19-22, 38, 40, 42, 45, 46].
Currently, the main mechanism responsible for theskeletal muscle atrophy in paraplegics is tought to bedisuse, but muscle fibres following SCI begin to changetheir functional properties early post injury.
Paraplegia and muscle
It is evident that other co-factors as spasticity and mi-crovascular damage, contribute to the induction of themarked morphological and enzyme histochemicalchanges seen in the paralyzed skeletal muscle.
The present review reports the results of our 20 yearexperience on skeletal muscle morphology, on musclehistochemical and metabolic profile and on muscle mi-crocirculation from paraplegics with SCI.
Skeletal Muscle Studies
Muscle fibre morphology and morphometry
Morphological and morphometric studies were per-formed on different paralyzed muscles. Morphologicalstudies were performed on muscle transverse sections inparaffine-embedded material with routine stains ashematoxylin and eosin and Van Gieson. Quantitativeanalysis of muscle fibre diameter was performed using anautomatic interactive image analysis system (IBAS I-II.Kontron, Bilanalyse, Munich). In the first study we ana-lyzed open biopsies of the rectus femoris muscle in 22paraplegic patients aged 16-66 years in subsequent stages(1-17 months) starting from the occurrence of SCI [38].
Next, our morphometric studies regarded open biopsiesfrom the gastrocnemius and soleus muscle (composedpredominantly of type 2 slow fibres) of 10 paraplegicsaged 16-54 years, grouped on the basis to the timeelapsed from SCI (1 to 10 months) [20, 21], and biopsiesfrom rectus femoris muscle in 10 young paraplegics aged16-28 years, divided in 2 groups, 1-5 months and 6-14months post SCI, respectively [45]. More recently, amorphometric analysis on needle biopsies of quadricepsfemoris muscle was performed in 15 male paraplegicsaged 20-30 years, 7-14 months post SCI [41].
Skeletal muscle from healthy subjects is composed bytrophic fibres with multiple subsarcolemmal nuclei. Thehistographic analysis of the normal vastus lateralis mus-cle indicate a mean fibre diameter of 67.2 µm [37]. Fibresare surrounded by a thin endomysium composed by re-
ticular connective tissue and by 4-8 capillaries. In Table1, a summary of quantitative findings on rectus femorisand quadriceps femoris fibres and capillaries (the fibreatrophy grade, the fibre type percentage and the capillarydensity and percentage) in different patient groups arereported. Particularly, in a study on rectus femoris musclein paraplegics [38], in the early times post SCI (1-2months) muscle fibre atrophy was evident with mean fi-bre diameter 26 µm. The fibre diameter decreased pro-gressively after SCI and, at least in the first year after in-jury, was directly proportional to the age of the cord le-sion. In this period denervation atrophy patterns withsmall groups of angulated atrophic or targetoid fibreswere observed. 7-9 months post SCI the mean fibre di-ameter was 20 µm, and at 10-17 months 16.5 µm.
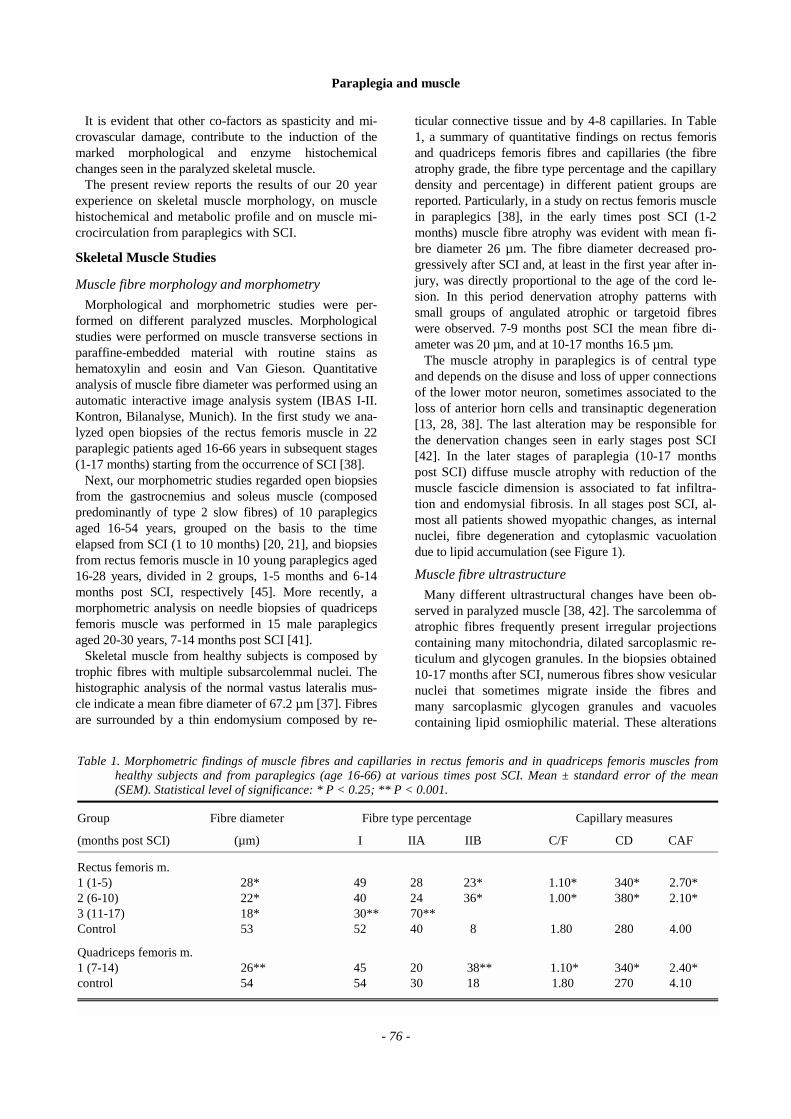
The muscle atrophy in paraplegics is of central typeand depends on the disuse and loss of upper connectionsof the lower motor neuron, sometimes associated to theloss of anterior horn cells and transinaptic degeneration[13, 28, 38]. The last alteration may be responsible forthe denervation changes seen in early stages post SCI[42]. In the later stages of paraplegia (10-17 monthspost SCI) diffuse muscle atrophy with reduction of themuscle fascicle dimension is associated to fat infiltra-tion and endomysial fibrosis. In all stages post SCI, al-most all patients showed myopathic changes, as internalnuclei, fibre degeneration and cytoplasmic vacuolationdue to lipid accumulation (see Figure 1).
Muscle fibre ultrastructure
Many different ultrastructural changes have been ob-served in paralyzed muscle [38, 42]. The sarcolemma ofatrophic fibres frequently present irregular projectionscontaining many mitochondria, dilated sarcoplasmic re-ticulum and glycogen granules. In the biopsies obtained10-17 months after SCI, numerous fibres show vesicularnuclei that sometimes migrate inside the fibres andmany sarcoplasmic glycogen granules and vacuolescontaining lipid osmiophilic material. These alterations
Table 1. Morphometric findings of muscle fibres and capillaries in rectus femoris and in quadriceps femoris muscles fromhealthy subjects and from paraplegics (age 16-66) at various times post SCI. Mean ± standard error of the mean(SEM). Statistical level of significance: * P < 0.25; ** P < 0.001.
Group Fibre diameter Fibre type percentage Capillary measures
(months post SCI) (µm) I IIA IIB C/F CD CAF
Rectus femoris m.1 (1-5) 28* 49 28 23* 1.10* 340* 2.70*2 (6-10) 22* 40 24 36* 1.00* 380* 2.10*3 (11-17) 18* 30** 70**Control 53 52 40 8 1.80 280 4.00
Quadriceps femoris m.1 (7-14) 26** 45 20 38** 1.10* 340* 2.40*control 54 54 30 18 1.80 270 4.10
- 76 -
Paraplegia and muscle
are limited tmyopathic cmuscle. Thegics regard the sarcopla
In Table mitochondrichondria peper fibre are
Myofibrillar
Remarkabhave been fstage of thefilaments, aing and strThese alterquence of m
Mitochondr
The mitosometimes s
The mitocdecrease inmuscle [38]disuse in oldthe lipid enand atrophialterations achondrial osome authoof mitochon
Figure 1. Sp
DISUSE SPASTICITY
MUSCLE FIBRE ATROPHYCAPILLARY DECREASE
FIBRE TYPE TRANSFORMATION
S
MYOPATHIC CHANGEoh
ths2ar a
ler lbeau
ia
chh . ecrxrsd
s FAST TYPE 2 FIBRE PREDOMINANCE
Satellite cells, myotubethe degenerating fibres and are consideredanges in the immobilized and hypoxiemicmain ultrastructural alterations in paraple-e myofibrillar apparatus, mitochondria and
mic lipid content of the muscle fibres., morphometric results of the analysis of (mean mitochondrial size and % of mito-fibre area) and of lipid droplet percentage are also reported.
apparatus
alterations in the myofibrillar apparatusequently observed in the medium and oldesion, with loss and disruption of the myo-normalities of the Z line, including smear-aming, and frequent formation of rods.tions are generally considered as conse-scle fibre degeneration.
hondria are generally small in size andow swelling and intracristal inclusions.ondrial size and percentage significantlyparaplegics in comparison with normal
Similar changes were observed in muscleaged subjects as result of low utilisation ofrgy sources [30, 37]. In the immobilized muscle, the morphological mitochondriale accompanied by impairment of the mito-idative enzyme activities [51]. Whereas described diffuse morphological damageria in disuse atrophy of skeletal muscle
[51], in our studies these changes are confined to rareinterspersed fibres.
Lipid content
Interspersed round vacuoles either empty or filled withosmiophylic lipid material, are seen in normal skeletalmuscle fibres. Lipids are normally utilized by mitochon-dria to release energy for metabolism and muscle con-traction. They increase in the muscle with aging and areexpression of disuse and of abnormal mitochondrialfunction [26, 37]. In paraplegics, the lipid droplets werewidely distributed in the cytoplasm, mainly in atrophicfibres, and their percentage per fibre area significantlyincreased (Table 3) [38]. This phenomenon may be re-lated to decrease in mitochondrial percentage and to theless efficient utilisation of the lipid energy sources fol-lowing muscle inactivity [26, 38].
Previous reports on skeletal muscle fibre morphologyand composition have been performed on patients at dif-ferent times post SCI, using standard qualitative en-zymehistochemical methods. All authors reported in-crease in the relative proportion of the fast type II fibresin longstanding paralyzed muscles, if compared to nor-mal healthy control subjects. In some patients, this fibretype transformation appears to be important, with rare-faction of slow type I fibre in the biopsies [14, 15, 23,31, 33, 50]. Morphological and morphometric analysisof paralyzed muscle post SCI indicates a progressivemuscle fibre atrophy, with important structural altera-tions. A 50% decrease in the fibre diameter was presentin the early stages of paraplegia. The disuse may be the
inal cord injury.
Table 2. Morphometric results of mitochondrial and lipid droplet content in quadriceps femoris muscle from young paraple-gics 7-12 months post SCI and control healthy subjects (mean age: 25). Mean ± standard error of the mean (SEM).Statistical level of significance: * P < 0.25; ** P < 0.001.
Mean mitochondrial size % mitochondria % lipid dropletssize (µm) per fibre area per fibre area
Controls 0.14 ± 0.09 2.53 ± 0.3 0.48 ± 0.20Paraplegics 0.008 ± 00.4** 1.70 ± 0.5* 3.20 ± 1.00**
- 77 -

Paraplegia and muscle
mcdlcmwmbprlpeisnct
M
mcattoattatrnrnSsa
-
Table 3. Mean muscle fibre type diameter in soleus and gastrocnemius muscles of paraplegics (age 16-54) and healthy control subjects.Group Soleus muscle Gastrocnemius muscle(months post SCI)
Fibre type Fibre typeI IIA IIB I IIA IIB
1 (1-2) 30 24 26 28 22 242 (3-4) 28 22 24 28 24 243 (5-6) 28 24 22 26 24 224 (7-8) 26 24 24 24 22 20
5 (9-10) 16 21 20 14 20 18
Control 50 48 44 48 46 46
- 78 -
ain cause of muscle atrophy in paraplegics. In the re-ent cord lesion, the degree of muscle atrophy was evi-ent and denervation changes were also seen. In theater stages of paraplegia the muscle atrophy degree in-reased and myopathic changes with focal necrosis andore extensive fibre degeneration in about 4% of fibresere observed. The degenerative changes in paralyzeduscle may be due to the vascular changes reported
elow, and the denervation patterns might reflect theresence of some coincidental alterations of the pe-ipheral nerve or trans-synaptic degeneration in theower motor neuron [13, 28, 38]. In advanced stagesost SCI, muscle atrophy and increase in the interstitialndomysial connective tissues and perifascicular fattynfiltration were evident. The significance of the ultra-tructural changes, particularly of the decrease in theumber of muscle mitochondria and of the increase inytoplasmic lipid vacuoles, are related to muscle inac-ivity and degeneration.
uscle fibre type composition
Normal quadriceps femoris muscle is composed of twoajor types of fibre characterized by enzymehistochemi-
al methods (myofibrillar ATPase pH 9.6 and 4.6): type 1nd type 2 fibres, and numerous sub-types. In our studieshe normal type 1 fibre diameter measures 52.2 µm andhe type 2 fibre diameter 48.2 µm [20]. Type 1 fibres areften of smaller diameter, contain many mitochondriand do not stain histochemically for myosin ATP-ase ac-ivity. Type 2 fibres are often broad and possess few mi-ochondria but they stain intensely for myosin ATP-asectivity [8]. In Table 1 and 3, morphometric findings onhe fibre diameter and on the fibre type percentage inectus femoris, quadriceps femoris, soleus and gastroc-emius muscle biopsies from paraplegic patients at timesanging over 1-17 months post SCI are reported. In sig-ificantly early time periods post injury (1-4 months postCI) evident preferential atrophy of type 2 fibres was ob-erved, but no changes in the relative percentage of type 1nd 2 fibres were remarked.
Biopsies performed 4-9 months post SCI showed at-rophy of both fibre types with a reduction in the relativepercentage of type 1 fibres. Following long term SCI(10-17 months post SCI), upper motor neuron paralysedmuscles lose the normal type 1 and 2 type mosaic pat-tern and become predominantly composed of type 2 fi-bres. Interesting results have been obtained from thestudy of the paretic soleus muscle, that normally is pre-dominantly composed by slow type 1 fibres. A signifi-cant shift of type 1 fibres to type 2B was observed in the7-10 months post SCI patient group [20, 21, 38, 42].
The above described results support the presence ofprogressive changes in paralyzed muscles probably oc-curring early after cord injury, but most evident 4 monthspost SCI. The main interesting change in the contractileproperties of paralyzed muscle after SCI is the fibre typetransformation phoenomenon, with type 1 fibre change totype 2, representing down-regulation of the slow MHCisoform and upper-regulation of the fast isoform in thosefibres. The shift to type II fibres was more evident inquadriceps and rectus femoris, and in soleus muscle,while in the gastrocnemius muscle the fibre type conver-sion was less remarkable. Moreover, the plastic modifi-cations of the fibre types was more evident in youngparaplegics than in older subjects. This result is probablyrelated to modifications in muscle morphology and intheir contractile properties described in the normal sed-entary aging man [30, 37]. The fast type II predominancein longstanding paraplegia may explain the problem ofmuscle fatigability encountered during rehabilitation ex-ercise using FES. Studies on experimental spinal cordtransaction showed changes in the rat and cat skeletalmuscle, with almost complete type I to type II fibre trans-formation [18, 52]. These changes are different fromthose seen in immobilisation in which large increase inthe ratio for fast resistant and slow units are seen [24]. Itmay be suggested that in long term paraplegia the loss ofthe upper motor neuron control and the spasticity mayinduce phoenomena of fibre type transformation. The de-scribed muscular changes in paraplegics are reversible
Paraplegia and muscle
- 79 -
after FES and electrically induced training, with partialrecovery of the muscle atrophy and with modification inthe fibre type transformation [25].
Myosin heavy chain isoform profileStudies on myosin heavy chain (MHC) content in
muscle fibres from parapegic patients are very scarce.
The adult normal skeletal muscle fibres express onlyone MHC isoform. Type 1 fibres have the slow MHCisoform, type 2 fibres have the fast MHC isoform andtype C fibres co-express both MHC isoforms. In ourstudies, the expression in MHC isoform content of thewhole biopsy was analyzed with an electrophoretic sepa-ration technique [6] on medial gastrocnemius and soleusmuscles in paraplegics 1-10 months post SCI.
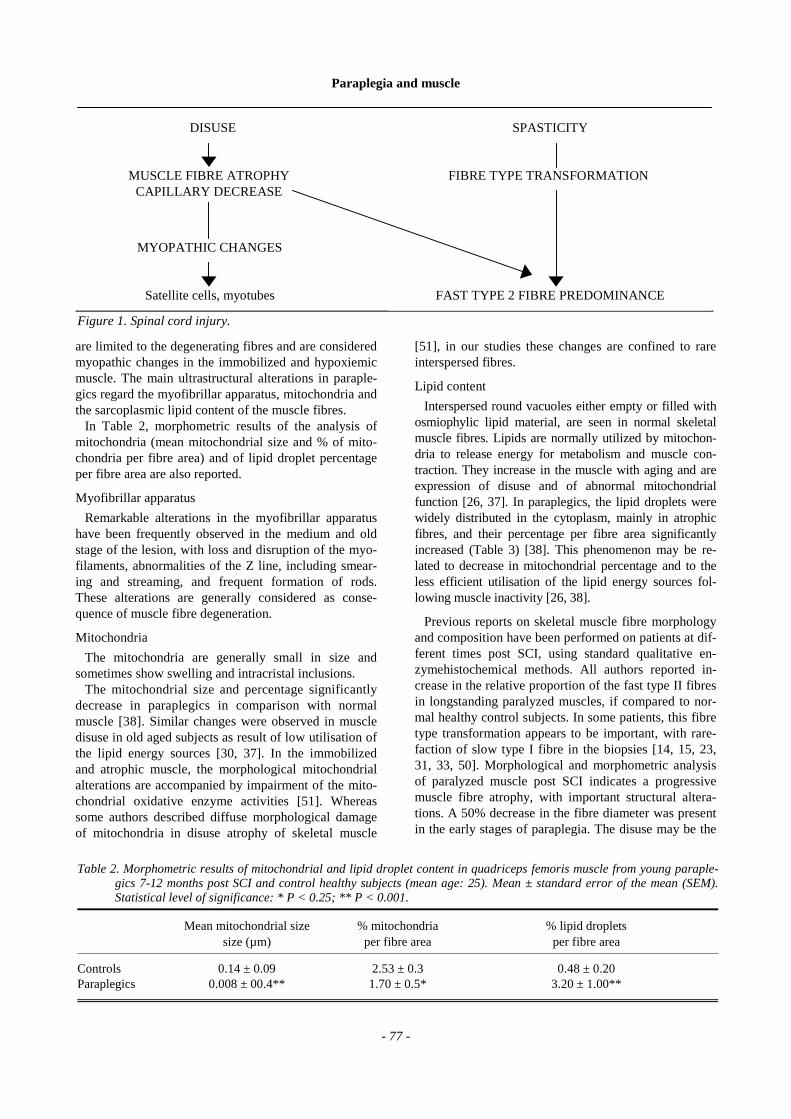
Figure 2. A. Fascicular atrophy with increase of perimysial fatty tissue in the rectus femoris muscle. 15 months postSCI. Giemsa. X 60. B. Pattern of denervation in groups of angulated atrophic fibres in the rectus femoris muscle.1 month post SCI. DPNH diaphorase. X 250. C. Numerous lipid vacuoles in the muscle fibre cytoplasm. 6months post SCI. H & E. X 250 D. Normal type I and type II (dark) fibre distribution in the quadriceps femorismuscle. 18 days post SCI. Myosin ATPase pH 9.4. X 150. E. Some areas of type 2 fibre predominance in therectus femoris muscle. 9 months post SCI. Myosin ATPase pH 9.4. X 150. F. Diffuse type II fibre predominancein the soleus muscle. 17 months after SCI. Myosin ATPase pH 9.4. X 150.
Paraplegia and muscle
- 80 -
The results indicated in the early period post SCI (1-6months) a predominant type 2 muscle fibre atrophy,without changes in the relative percentage of fibre typesand MHC content. Eight months post injury, we re-marked atrophy of both fibre types with increase in therelative percentage of type 2 fibres and fast MHC con-tent. However, the shift of the type 1 to type 2 fibres wasevident 7-8 months post SCI [42]. Fibre type transforma-tion of type 1 to type 2 fibres goes through a transitionalphase where they co-express slow and fast myosin iso-forms. Data presented by Burnham et al [3], by means ofimmunofluorescence determination of single fibre MCHisoform, suggest that the onset of fibre shifting to type 2fibres in paraplegics may to be earlier than previously de-scribed, probably occurring about 1 month post SCI. Thisstudy was performed on vastus lateralis muscle biopsiesfrom 12 paraplegics with SCI over a period of 1-219months after SCI. Thus, following long term SCI inducedparalysis, fibres in the quadriceps femoris and vastus lat-eralis muscle take on a new state profile defined by a shiftin the MHC expression to the fast isoform.
FES and electrically induced training determine in theparalyzed muscle expressing a majority of MHC iso-form II B fibres, a fibre type transformation towards themore fatigue resistant MHC isoform II A [25].
Interesting results on paralyzed muscle derive fromthe characterization of fibre type profile with enzyme-histochemistry and from the study of the MHC isoformsover a wide range of post SCI periods. The findingssupport the concept of progressive stages of change inmuscle from paraplegics, suggesting that the earliest al-terations post SCI are confined to the morphologicalmuscle aspects (fibre atrophy, focal fibre degenerationwith changes in the ultrastructural profile and capillarydilatation). The onset of the fibre type shifting to type 2fibre probably occurs 1 month after SCI, but only 7-8months after injury the shift of the type 1 to type 2 fi-bres is well manifested. This fibre type conversion isrelated to muscle plasticity, defined as a functional fibreremodeling after different normal and pathological con-ditions, inducing important changes of the subcellular
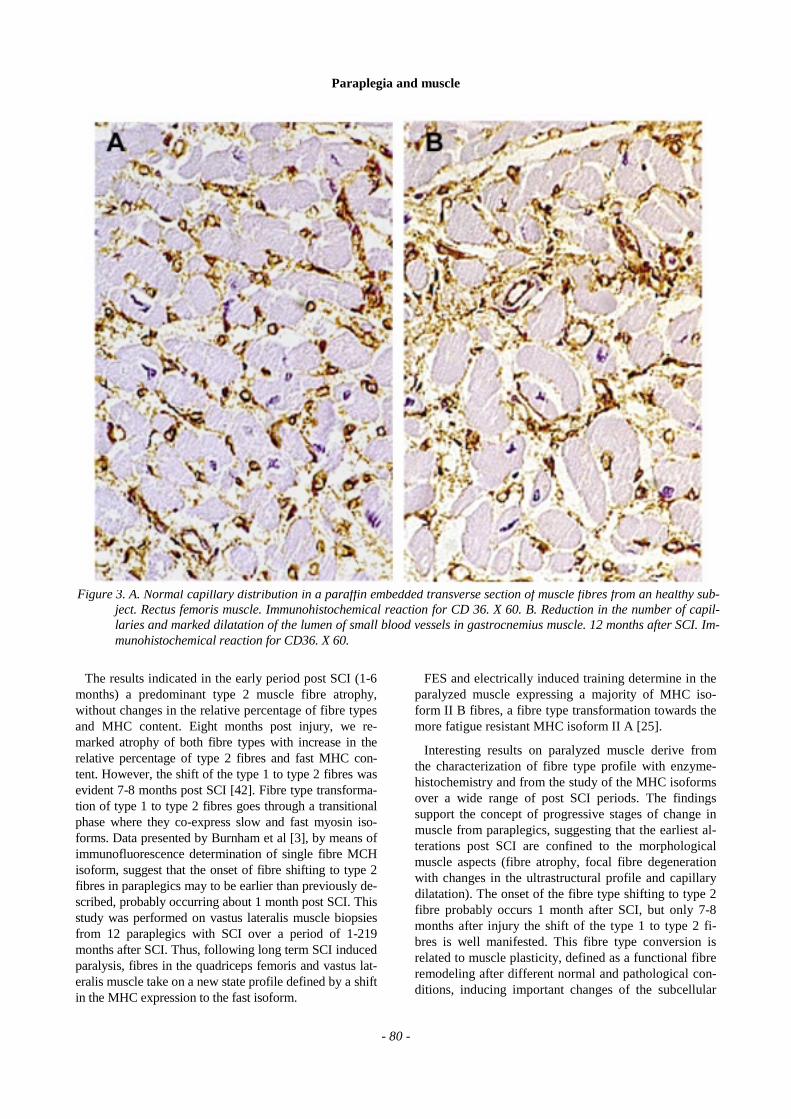
Figure 3. A. Normal capillary distribution in a paraffin embedded transverse section of muscle fibres from an healthy sub-ject. Rectus femoris muscle. Immunohistochemical reaction for CD 36. X 60. B. Reduction in the number of capil-laries and marked dilatation of the lumen of small blood vessels in gastrocnemius muscle. 12 months after SCI. Im-munohistochemical reaction for CD36. X 60.

Paraplegia and muscle
structure, of the enzyme content, of the metabolic andbiochemical characteristics, and of the contractile prop-erties of muscle fibres [10, 34]. The spasticity causespathological changes in refex function, such as loss ofreciprocal inhibition, cocontraction of agonist and an-tagonist muscles and the loss of activity in the inhibitorypathways. These alterations, together with disuse andother co-factors, are undoubtedly an appropriate opportu-nity for the development of the plastic changes in the hy-pertonic paralyzed muscle [4].
Muscle microcirculation studies
Blood vesselsThe first studies on microvasculature from human
skeletal muscle concerned normal healthy adults, athletesand normal subjects trained in endurance or strength [1,2, 7]. They demonstrated a close relationship among themuscle fibre diameter, fibre type and capillary number.The greatest number of capillaries surrounds the type 1slow fibres. Literature data on normal muscle microcir-culation concern qualitative and quantitative analysis ofcapillaries. In our studies on muscle microcirculation inparaplegics, microscopic qualitative studies were per-formed using histological and ultrastructural methods.More recently these studies utilized the immunohisto-chemical characterization of capillaries by mean of anti-bodies as endotheline and CD 36.
The quantitative evaluation of capillaries was per-formed with an automatic Interactive Image AnalysisSistem- IBAS I,II (Kontron-Bildanalyse Munich, Ger-many) on histological sections, the number of capillariesper fibre (C/F), capillaries surrounding a single fibre(CAF), and the capillary density per square millimeter(CD) were determined (Table 1). The clinical and mor-phological evidences of vascular alterations in paraple-gics, as vasomotor disturbances and decrease in the ve-nous distensibility and capacity [16] and structural altera-tions in the muscle blood vessels [45] may be importantcauses of the degenerative myopathic changes in para-lyzed muscle fibres. These alterations are similar to thoseseen in patients with chronic venous insufficiency, whodevelop microangiopathy of cutaneous blood and lym-phatic capillaries [11]. In recent SCI (1-4 months postinjury), when paralysis with profound hypotonic flaccid-ity is evident, marked capillary dilatation and interstitialvasogenic oedema were seen. In later stages of paraplegia(10-17 months post SCI), when spasticity becomes evi-dent, paraplegics showed thickening of the arteriolar wallwith reduplication of the basal lamina of capillaries and
of capillary wall associated to reduction in the capillarynumber [20, 38, 42, 45]. The above mentioned microvas-cular changes are also present in the skin of paralyzedmuscle and may be expression of a microangiopathy inparaplegics after SCI [11, 20, 42]. These alteration areimportant and similar changes, as the reduplication andthickening of the capillary basal lamina, have been de-scribed in diabetes mellitus, in dystrophia myotonica andin other different microvascular diseases [36, 48]. Humanand experimental studies on skeletal muscle inactivitywhich causes muscle atrophy, showed reduction of cap-illaries as well as the long standing denervation atrophythat cause reduction and damage of mitochondria and ofcapillaries [5, 35, 51].
On the basis of these observations, the capillaryqualitative and qualitative changes in paraplegics maybe due to interaction of different factors: disuse fibreatrophy, reduction in muscle volume, incidental over-imposed denervation, loss of type 1 fibres that are nor-mally surrounded by a great number of capillaries, andshift to the type 2 muscle fibres. Moreover they couldbe interpreted as a negative phoenomenon inducing theischemic degenerative myopathic changes described inmuscle fibres in long term paraplegia [42].
The results of a study on young paraplegics after useof gait orthoses (HGO,ORLAU Parawalker), the periodafter supply ranging from 5-6 months [41, 43] supportthe latter hypothesis.
In Table 4, overall capillary and fibre morphometry inrectus femoris muscle from untrained and Parawalkertrained paraplegics were reported. After orthotic walk-ing training there was a discrete preservation of themuscle fibre diameter and increase of the muscle capil-lary supply in comparison with untrained paraplegics.These results are in agreement with those described inexperimental spinal cord lesions in animals in whichfavourable exercise-induced changes in biochemical andcontractile properties of muscle fibres and in musclecapillarity were observed [9, 17].
Lymphatics
In paraplegics, immobilization, prolonged bed rest andloss of muscle contraction are main causes of venous sta-sis in the lower extremities. The venous stasis is fre-quently associated to microlymphatic changes of the skinof the paralyzed leg and it is an important cause of throm-boembolic disease in paraplegics. In the patients, the in-crease of the deep venous resistance and the venous stasisdeterminate microangiopathic alterations in the skin, in-
-
Table 4. Overall capillary and fibre morphometry in rectus femoris muscle from healthy control subjects, untrained paraplegics and Parawalker trained paraplegics. Mean ± standard error of the mean (SEM). P < 0.0001.Untrained paraplegics 26.0 ± 4.2* 47.0 ± 4.0 1.10 ± 0.12 340 ± 8 2.70 ± 0.1*Parawalker users 33.0 ± 5.4* 50.0 ± 5.6 1.46 ± 0.6* 300 ± 8 3.60 ± 0.4*Normal adults 53.3 ± 7.4* 52.0 ± 4.2 1.80 ± 0.1* 280 ± 18 4.00 ± 0.2
- 81 -
Paraplegia and muscle
- 82 -
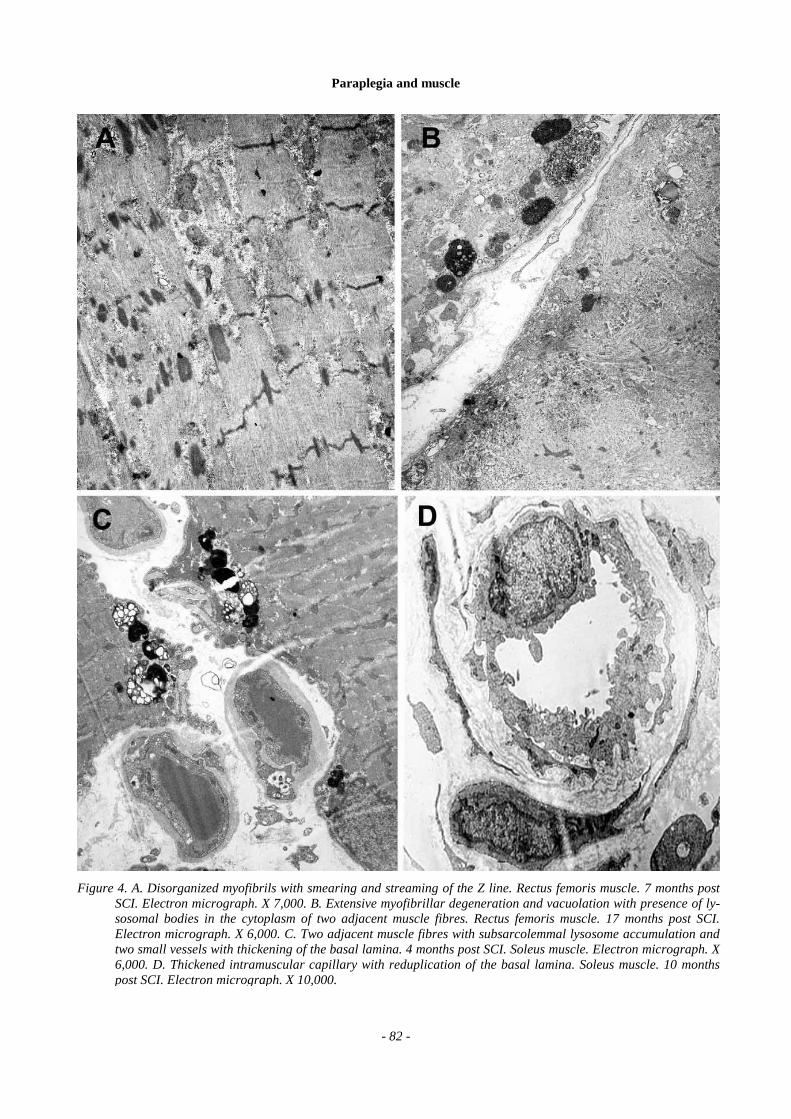
Figure 4. A. Disorganized myofibrils with smearing and streaming of the Z line. Rectus femoris muscle. 7 months postSCI. Electron micrograph. X 7,000. B. Extensive myofibrillar degeneration and vacuolation with presence of ly-sosomal bodies in the cytoplasm of two adjacent muscle fibres. Rectus femoris muscle. 17 months post SCI.Electron micrograph. X 6,000. C. Two adjacent muscle fibres with subsarcolemmal lysosome accumulation andtwo small vessels with thickening of the basal lamina. 4 months post SCI. Soleus muscle. Electron micrograph. X6,000. D. Thickened intramuscular capillary with reduplication of the basal lamina. Soleus muscle. 10 monthspost SCI. Electron micrograph. X 10,000.

Paraplegia and muscle
- 83 -
volving blood and lymphatic vessels and eventually lead-ing to skin dystrophic changes and oedema (phlegmasiaalba dolens). The morphological identification of lym-phatic vessel in the skeletal muscle is difficult. However,in a study, we analyzed lymphatic vessels in the skin ofthe lower extremities from young male paraplegic patientswith and without thromboembolic disease (TED) [44, 46].
In paraplegics with TED of deep veins, skin lymphaticvessels of paretic legs showed dilated lumen and dis-tended wall. The endothelial cells were attenuated andnumerous channels among endothelial cells were present.Perivascular collagen and elastic fibres were dissociatedby oedema and by the presence of granular material. Inparaplegics without TED similar but more rare micro-lymphatic changes are present.
These morphological changes demonstrated a lym-phatic microangiopathy in paraplegics, with lymph sta-sis and an increased transcapillary diffusion of thelymph material into perivascular dermic tissues, clini-cally resulting in oedema and reduced removal of tissuecatabolites. These leg terminal lymphatic changes andthe blood cutaneous microangiopathy probably determi-nates the extent of the trophic disturbances and the ulcerformation in paraplegics. The microangiopathy is thebasis for reduction of PO2 and of for destruction of thelymphatic capillary network, seen respectively aftertranscutaneous PO2 measurements and by fluorescentmicrolymphography in long term paraplegia and in pa-tients with chronic venous insufficiency [11, 46].
Conclusions and PerspectivesFrom a rehabilitation perspective it is necessary to
evaluate the conditions of the motor unit and the musclefibre plastic potentialities and reversibility in paraple-gics after SCI. The results from the present studiesdemonstrated changes in the fibre morphology and intheir contractile properties, and in the muscle capillarityof paralyzed muscle fibres after SCI. There is a numberof rehabilitative programs that are able to modify muscleatrophy and to prevent some clinical complications, bymeans of physical training, FES, aerobic exercise trainersand bio-mechanic orthoses. In numerous reports, pre-vention of muscle disuse and improvement in the fibreoxidative capacities after muscle electric stimulation inparaplegics were demonstrated [12, 49]. In adult para-plegics, FES induce changes of morphological, bio-chemical and histochemical profile, and of contractileproperties of muscle fibres and improve the musclecapillarity [31], as well as the use of bio-mechanic or-thoses [27, 41, 43] and of aerobic exercise trainers [29].The muscle fibre atrophy and the fibre type transforma-tion process in paraplegics was partially normalized af-ter electrical induced cycle training [25]. These supportsfor paraplegic locomotion require high energy cost andmay be utilized in patients without cardiovascular andrespiratory diseases [27]. The knowledge of the muscle
condition and of plastic capacities for fiber type shifting isnot only important in attenuating the adverse muscle im-pact and complications of SCI, but it is also crucial in thechoice of an appropriate rehabilitative program directed topreventing the changes associated to disuse and to retraincontractile properties associated to spasticity and micro-vascular damage. In fact, it is well known that the thera-peutic exercise setting out to isotonic concentric or eccen-tric contracture determines selective recruitment of fast orslow fibres which prevents selective fibre type atrophies inparetic muscle. Finally, in an attempt to restore functionand regain motor control, many laboratories are nowfocusing a rehabilitation program based on engineeringdevices that substitute a motor controlled function (SCItranscutaneous FES walking). It is easily comprehensi-ble that these recovery techniques can be utilized onlyin well-preserved muscle after SCI. Since it is evidentthat muscle atrophy and transformation in their funda-mental properties occur precociously post SCI, reha-bilitative interventions need to be instituted as early assafetly possible.
Acknowledgements
We gratefully acknowledge for they cooperation: DrSergio Lotta, head of the Rehabilitation Center for para-plegics G Verdi of Villanova sull’Arda (Pc), Prof CarlaMarchetti and Prof Paola Poggi, professors of the His-tology and Human Anatomy of the University of Pavia,and Prof Ugo Carraro, head of the CNR Unit for MuscleBiology and Physiopathology of the Institute of GeneralPathology of the University of Padova (Italy).
Address correspondence to:
Prof. R. Scelsi, Istituto di Anatomia e Istologia Pa-tologica, via Forlanini 14, 27100 Pavia, Italy, phone +390382 528476, fax +39 0382 525866, Email [email protected].
References
[1] Anderson P: Capillary density in skeletal muscle ofman. Acta Physiol Scand 1975; 95: 203-205. [2] Brodal P, Ingjer F, Hermansen L: Capillary supplyof skeletal muscle in trained and endurance-trainedmen. Am J Physiol 1977; 232: 705-712. [3] Burke D: Spasticity as an adaptation to pyramidaltract injury. In Waxman SC (ed): Functional recov-ery in neurological diseases. Advances in Neurol-ogy. New York, Raven Press, 1988; 47: 401-423. [4] Burnham R, Martin T, Stein R, Bell G, MacLeanI, Steadward R: Skeletal muscle fibre type trans-formation following spinal cord injury. SpinalCord 1997; 35: 86-91. [5] Carpenter S, Karpati G: Necrosis of capillaries indenervation atrophy of human skeletal muscle.Muscle Nerve 1982; 5: 250-254. [6] Carraro U, Catani C: A sensitive SDS-PAGEmethod separating myosin heavy chain isoforms ofrat skeletal muscle reveals the heterogeneous nature
Paraplegia and muscle
- 84 -
of the embryonic myosin. Biochem Biophys ResCommun 1983; 116: 793-802. [7] Carry MR, Ringel SP, Starcevich JM: Distributionof capillaries in normal and diseased human skele-tal muscle. Muscle Nerve 1986; 9: 250-254. [8] Dubowitz V: Muscle biopsy. A practical approach.2nd Edn. Baillire. London. 1985. [9] Edgerton VR, Smith LA, Elred E, Mendell LM:Muscle and motor unit properties of exercised andnon-exercised chronic spinal cats. In Pette D (ed):Symposium on plasticity of muscle. New York, DeGruyter, 1980, pp 355-372. [10] Eisenberg BR, Salmons S: The reorganisation of sub-cellular structure in muscle undergoing fast to slow typetransformation. Cell Tissue Res 1981; 220: 449-471. [11] Franzeck UK, Haselbach P, Speiser D, Bollinger A:Microangiopathy of cutaneous blood and lymphaticcapillaries in chronic venous insufficiency. Yale JBiol Med 1993; 66: 37-46. [12] Gibson JNA, Smith K, Rennie MJ: Prevention ofdisuse muscle atrophy by means of electricalstimulation. Lancet 1988; Oct: 767-770. [13] Goldkamp O: Electromyographic and nerve con-duction studies in 116 patients with hemiplegia.Arch Phys Med 1987; 48: 59-63. [14] Greeve JMD: Functional electric stimulation(FES): muscle histochemical analysis. Paraplegia1993; 31: 764-770. [15] Grimby G, Broberg C, Krotkiewsky M: Muscle fi-bre composition in patients with traumatic spinalcord lesion. Scand J Rehab Med 1976; 8: 37-42. [16] Hopman MTE, Nommensen E, et al: Properties of thevenous vascular system in the lower extremities of indi-viduals with paraplegia. Paraplegia 1994; 32: 810-816. [17] Johnson DJ, Smith LA, Elred E, Edgerton VR: Ex-ercise-induced changes of biochemical, histochemi-cal and contractile properties of muscle in cordoto-mized kittens. Exp Neurol 1982; 76: 414-427. [18] Leiber R, Johansson CAB, Wahlsing HL, HargensAR, Feringa ER: Long-term effects of spinal cordtransection on fast and slow rat skeletal muscle.Exp Neurol 1986; 91: 423-434. [19] Lotta S, Lommi G, Scelsi R, Poggi P, Marchetti C,Foresti G: Composizione delle fibre muscolari stri-ate nei postumi di lesioni complete del motoneu-rone centrale. Studio morfologico in funzione ri-abilitativa. In Perfetti C, Ambrosino N (eds): Laprogrammazione della esperienza post lesionale.Atti 12° congresso Soc. It. Medicina Fisica e Ri-abilitativa. Il Ciocco, 1981, pp 353-371. [20] Lotta S, Scelsi L, Scelsi R: Microvascular changes inthe lower extremities of paraplegics with heterotopicossifications. Spinal Cord 2001; 39: 595-598. [21] Lotta S, Scelsi R, Alfonsi E, Saitta A, Nicolotti D,Epifani P,Carraro U: Morphometric and neuro-physiological analysis of skeletal muscle in para-
plegic patients with traumatic cord lesion. Paraple-gia 1991; 29: 247-252. [22] Lotta S, Scelsi R: Skeletal muscle atrophy after spinalcord lesion. Temporal changes in the paretic musclemorphology. In Capodaglio P, Narici MV (eds): Mus-cle atrophy. Disuse and disease. Advances in Occu-pational Medicine and Rehabilitation. 1998; 4: 83-87. [23] Martin TP, Stein RB, Hoeppner PH, Reid DC: In-fluence of electrical stimulation on the morphologicand metabolic properties of paralyzed muscle. JAppl Physiol 1992; 72: 1401-1406. [24] Mayer RF, Burke RE, Toop J, Hodgson JA: The effectof spinal cord transection on motor units in cat medialgastrocnemius muscle. Muscle Nerve 1984; 7: 21-23. [25] Mohr T, Andersen J, Biering-Sorensen F, Galbo H,Kjaer M: Long term adaptation to electrically in-duced cycle training in severe spinal cord injuredindividuals. Spinal Cord 1997; 35: 1-16. [26] Morgan-Hughes JA: The mitochondrial myopathies.In Engel AG, Ranker BSL (eds): Myology. MacGraw Hill Book Co, 1986, pp 1706-1743. [27] Nene AV, Orth D, Patrick JH: Energy cost of para-plegic locomotion with the ORLAU parawalker.Paraplegia 1989; 27: 5-18. [28] Ochs S: System of material transport in nerve fibresrelated to nerve function and trophic control. AnnNY Acad Sci 1974; 228: 202-210. [29] Petrofsky J, Chandler P, Almeida J, Briggs R:Aerobic trainer with physiological monitoring forexercise in paraplegic and quadriplegic patients. JClin Engineering 1985; 4: 307-316. [30] Poggi P, Marchetti C, Scelsi R: Automatic mor-phometric analysis of skeletal muscle fibres in theaging man. Anatomical Record 1987; 217: 30-34. [31] Rochester L, Barron MJ: Influence of electricalstimulation of the tibialis anterior muscle in para-plegic patients. Morphological and histochemicalproperties. Paraplegia 1995; 33: 514-522. [32] Round JM, Barr FMD, Moffat B, Jones DA: Fibreareas and histochemical fibre types in the quadri-ceps muscle of paraplegic subjects. J Neurol Sci1993; 116: 207-211. [33] Roy RR, Baldwin KM, Edgerton VR: The plasticityof skeletal muscle: effects on neuromuscular activity.In Hollosky J (ed): Exercise and Sport Review. Bal-timore, Williams and Wilkins, 1991; 19: 269-312. [34] Salmons S, Henriksson J: The adaptive response ofskeletal muscle to increased use. Muscle Nerve1981; 4: 94-105. [35] Sargeant AJ, Davies CTM, Edwards RHT, Maun-der C, Young A: Functional and structural changesafter disuse of human muscle. Clin Sci Mol Med1977; 52: 337-342. [36] Scelsi R, Lotta S, Lommi G, Poggi P, Marchetti C:Hemiplegic atrophy. Morphological findings in the
Paraplegia and muscle
- 85 -
anterior tibial muscle of patients with cerebral vascularaccidents. Acta Neuropathol (Berl) 1984; 62: 324-331. [37] Scelsi R, Lotta S, Poggi P, Bocchi R, Scelsi L: Mi-crolymphatic and thromboembolic disease in acutespinal cord injury. A morphological study on skinbiopsies. European J Lymphology 1994; 4: 115-119. [38] Scelsi R, Lotta S, Scelsi L: Skeletal muscle mor-phology during restoration of gait with orthoses inthoracic paraplegia. In: 9th International Conferenceon Mechanics in Medicine Biology. Ljubljana, June1996, Abstracts N 34. [39] Scelsi R, Lotta S: Morphological properties ofskeletal muscle in spastic paraplegia. Basic ApplMyol 1991; 1: 317-326. [40] Scelsi R, Marchetti C, Poggi P, Lotta S, Lommi G:Muscle fiber type morphology and distribution inparaplegic patients with traumatic cord lesion. ActaNeuropathol (Berl) 1982; 57: 243-248. [41] Scelsi R, Marchetti C, Poggi P: Histochemical andultrastructural aspects of M Vastus Lateralis in sed-entary old people (age 65-89 years). Acta Neuro-path (Berl) 1980; 51: 99-105. [42] Scelsi R, Poggi P, Nappi G, Sandrini G: Peripheralmicrocirculatory lesions in myotonic dystrophy. Alight and electron microscopic study. Acta Neurol1978; 33: 137-148. [43] Scelsi R, Poggi P, Padovani R, Lotta S, Saitta A:Skeletal muscle changes following myelotomy inparaplegic patients. Paraplegia 1986; 24: 250-259. [44] Scelsi R, Scelsi L, Bocchi R, Lotta S: Morphologi-cal changes in the skin microlymphatics in recentinjured paraplegic patients with ilio-femoral throm-bosis. Paraplegia 1995; 33: 472-475.
[45] Scelsi R, Scelsi L, Lotta S: Microvascular changesin skeletal muscle from paraplegic patients withspinal cord lesion. In Carraro U, Salmons S (eds):Basic and Applied Myology. Perspectives for the90s. Padova, Unipress, 1995, pp 163-170. [46] Scelsi R, Scelsi L, Lotta S: Skeletal muscle mor-phology in paraplegic patients after Parawalker or-thotic walking. In: Activity-induced muscle injuryand repair: International Symposium on Basic andApplied Myology. Abano Terme, May 30, 1991. [47] Scelsi R, Scelsi L, Lotta S: Skeletal muscle mor-phology in paraplegics after Parawalker orthotictraining. In: Proceedings of the 4th Vienna Interna-tional Workshop on Functional Electrostimulation.Vienna, September 24-27, 1992, pp 75-78. [48] Siperstein MD, Raskin PR, Burn H: Electron mi-croscopic quantification of diabetic microangiopa-thy. Diabetes 1973; 22: 514-524. [49] Stein RB: Optimal stimulation of paralysed muscleafter human spinal cord injury. J Appl Physiol1992; 72: 1393-1400. [50] Stilwill EW, Sahgal V: Histochemical and morphol-ogic changes in skeletal muscle following cervicalcord injury: a study of upper and lower motor neuronlesions. Arch Phys Med Rehabil 1977; 58: 201-206. [51] Weheman HJ, Max SR: Mitochondrial ultrastruc-ture in disuse atrophy of skeletal muscle. Federa-tion Proc 1972; 31: 253. [52] West SP, Roland RR, Reggie Edgerton V: Fibre typeand fibre size in cat ankle, knee and hip extensor andflexors following low thoracic spinal cord transec-tion in an early age. Exp Neurol 1986; 91: 174-182.