Embed Size (px)
Citation preview

SKELETAL MUSCLE INTERSTITIUM AND BLOOD PH AT REST AND DURING EXERCISE
IN HUMANS
A thesis submitted for the degree of
Doctor of Philosophy
to
Queensland University of Technology
School of Human Movement Studies
Darrin Street
B.App.Sci. Hons.
2003


Preface
III
PREFACE
The present thesis is divided into three major parts corresponding to the three
experimental studies undertaken: Chapter 3, measurement of dialysate pH
representative of interstitial pH at rest and during dynamic leg exercise,
Chapter 4, effect of alkali ingestion rate on plasma acid-base [H+] and ionic
[K+] status, and Chapter 5, effect of sodium citrate on interstitial pH in human
skeletal muscle. These studies individually look at establishing a new method
for the detection of interstitial pH in humans at rest and during exercise,
developing an optimal ingestion regime of sodium citrate to manipulate blood
pH at rest and finally, by combining these two techniques, ascertaining the
degree to which the interstitial space is alkalised after ingesting sodium
citrate. Chapter 3 further details the in vitro experiments used to evaluate
the accuracy and reliability of the fluorometric method established for
measuring interstitial pH.
Such manipulation of a system can provide valuable information as to how the
system operates and thereby lead to a greater understanding of human
exercise physiology, which is the main concern of this thesis. Specifically,
since the measurement of interstitial pH in human skeletal muscle has never
been performed before, these studies will represent a collective approach to
gaining further knowledge about the movement of H+ between the blood and
interstitial space within skeletal muscle.
Other major sections of this thesis include the literature review, general
discussion, conclusion and future research. Collectively, these sections set
the context for the thesis, provide background for the support and
identification of the three experimental studies, analyses and interpretations
of results collected from all three studies, main findings and future directions
inspired from this work. In the literature review, my aim is to provide
information about the specific physiology pertaining to sodium citrate
ingestion and pH regulation. Consequently, I have divided it into four main
sections: gastro-intestinal absorption and sodium citrate, renal regulation, H+
and K+ regulation at rest and during exercise, and alkalosis at rest and during
exercise. Each of these sections, in turn, discusses the existing research
relevant to the experimental studies and identifies the need for further

Preface
IV
research. The general discussion mainly addresses the key findings as a
whole from Chapters 3, 4 and 5, while the conclusion adds to this information
with the inclusion of future research directions.

Keywords
V
KEYWORDS
Alkali ingestion rate
Alkalosis
Bicarbonate perfusate
Blood pH
Dialysate pH
Ergogenesis
Interstitial pH
Knee-extensor exercise
Microdialysis
pH
Proton
Skeletal muscle
Sodium citrate
Urine pH


Abstract
VII
ABSTRACT
The aims of this thesis were to: 1) develop a new method for the
determination of interstitial pH at rest and during exercise in vivo, 2)
systematically explore the effects of different ingestion regimes of 300 mg.kg-
1 sodium citrate on blood and urine pH at rest, and 3) to combine the new
interstitial pH technique with the findings of the second investigation in an
attempt to provide a greater understanding of H+ movement between the
extracellular compartments.
The purpose of the first study was to develop a method for the continuous
measurement of interstitial pH in vastus lateralis was successfully developed
using microdialysis and 2,7-bis-(2-carboxyethyl)-5-(and-6)-
carboxyfluorescein (BCECF). To avoid the presence of an artificial alkalosis
during exercise, it was necessary to add 25 mM HCO3- to the perfusate. The
outlet of the probe was cut <10 mm from the skin and connected to a
stainless steel tube completing the circuit to a microflow-through cuvette (8
µl) within a fluorescence spectrophotometer. This prevented the loss of
carbon dioxide from the dialysate and any subsequent pH artefact. Interstitial
pH was collected from six subjects before, during and after five minutes of
knee-extensor exercise at three intensities 30, 50, and 70 W. Mean±SEM
interstitial pH at rest was 7.38±0.02. Exercise reduced interstitial pH in an
almost linear fashion. The nadir value for interstitial pH at 30, 50 and 70 W
exercise was 7.27, 7.16 and 7.04, respectively. The lowest pH was obtained
1 min after exercise, irrespective of workload, after which the interstitial pH
recovered in a nearly exponential manner. The mean half time of interstitial
recovery was 5.2 min. The changes in interstitial pH exceeded the changes in
venous blood pH. This study demonstrated that interstitial pH can be
measured using microdialysis and that it is continuously decreased during
muscle activity.
The purpose of the second study was to establish an optimal ingestion regime
for the ingestion of 300 mg.kg-1 of sodium citrate and maximise the alkalotic
effect while minimising any side effects. Increasing the effectiveness of alkali
ingestion may lead to further increases in muscle performance. Ingesting 300
mg.kg-1 sodium citrate at a rate of 300 mg.min-1 was identified as the optimal

Abstract
VIII
ingestion regime to maximise alkalosis at rest, which occurred 3.5 h post-
ingestion. This was determined by monitoring eight human subjects ingesting
300 mg.kg-1 sodium citrate at five different rates, control (no ingestant),
bolus, 300, 600 and 900 mg.kg.min-1 on five days separated by at least 48
hours. Sodium citrate was ingested in capsule form with water ad libitum,
with the exception of bolus, which was combined with 400 ml <25 percent
orange juice and consumed in <1 min. Arterialised blood (mean 71.3±3.5
mmHg) acid-base and electrolyte status was assessed via the withdrawal of
~5 ml of blood every 30 min across an eight hour duration, placed on ice and
analysed within five minutes. No alkalotic difference was found between
ingestion rates (mean 7.445±0.004, 7.438±0.004 and 7.442±0.004 for 300,
600 and 900 mg.min-1, respectively). All experimental ingestion regimes
were associated with elevations in [HCO3-] (29.6, 29.7, 29.8, 29.9 and 26.3
mmol.l-1 for bolus, 300, 600, 900 and control, respectively). The 300
ingestion regime had the greatest impact on [H+], a 0.66 meq.l-1×10-8 change.
Bolus ingestion (3.93±0.08 mmol.l-1) of sodium citrate had no effect on
control (4.06±0.08 mmol.l-1) blood [K+], however, 300 mg.min-1 decreased
blood [K+] (p<0.05). There was no effect of sodium citrate on blood [Cl-], but
after 2.5 h blood [Cl-] was lower than pre-ingestion values (p<0.05). All
ingestion rates of sodium citrate increased (p<0.05) urine pH above control.
This is the first study to investigate the effect of varying ingestion rates on
acid-base status at rest in humans. The results suggest that ingesting sodium
citrate in small doses in quick succession induce a greater blood alkalosis than
the commonly practised bolus protocol.
Using the interstitial pH technique described above and the optimal ingestion
regime (300 mg.min-1) identified above, the final experiment was designed to
assess the influence of sodium citrate ingestion on interstitial pH at both rest
and during exercise. Five subjects ingested 300 mg.kg-1 sodium citrate at
300 mg.min-1 again in capsule form with water ad libitum. Prior to ingestion,
each subject had a cannula placed into their cephalic vein and one
microdialysis probe (CMA-60) inserted into their left thigh, orientated along
the fibres of vastus lateralus. This probe was used for the measurement of
pH as described above. At the end of this period, an exercise protocol
required five subjects to perform light exercise (10 W) for 10 min, before
starting an intense exercise period (~90-95% leg VO2peak) to exhaustion
followed by a 15 min recovery period. Dialysate and blood samples were

Abstract
IX
collected across all periods. Mean±SEM interstitial pH for placebo and
alkalosis were 7.38±0.12 and 7.24±0.16, respectively. Sodium citrate
ingestion was not associated with an interstitial alkalosis. An exercise induced
acidosis was observed in the interstitium during placebo but not during
alkalosis (p<0.05). Mean±SEM venous pH were 7.362±0.003 and
7.398±0.003 for placebo and alkalosis, respectively. Sodium citrate ingestion
was not associated with a venous alkalosis. Sodium citrate ingestion was
associated with an increase in mean±SEM venous [HCO3-] (placebo 25.5±0.2,
alkalosis 28.1±0.2). This increase in the blood bicarbonate buffer system was
not associated with an increase in time to exhaustion (placebo 352±71,
alkalosis 415±171). This was the first study to investigate the effects of
sodium citrate ingestion on interstitial pH. The results of this study
demonstrated that an interstitial alkalosis does not ensue after alkali
ingestion, however, it was associated with the lack of an exercise induced
acidosis suggesting an improved pH regulation during exercise.


Table of Contents
XI
TABLE OF CONTENTS
SKELETAL MUSCLE INTERSTITIUM AND BLOOD PH AT REST AND DURING EXERCISE IN HUMANS ..........................................................................................................................................................I
PREFACE ......................................................................................................................................III KEYWORDS ...................................................................................................................................V ABSTRACT ................................................................................................................................. VII TABLE OF CONTENTS ...................................................................................................................XI LIST OF FIGURES ........................................................................................................................ XV LIST OF TABLES ...................................................................................................................... XVII LIST OF EQUATIONS ..................................................................................................................XIX ABBREVIATIONS .......................................................................................................................XXI
Chemical Formulas:..............................................................................................................XXI Units of Measurement: ........................................................................................................ XXII
STATEMENT OF ORIGINAL AUTHORSHIP .................................................................................. XXV ACKNOWLEDGEMENTS..........................................................................................................XXVII
CHAPTER 1 INTRODUCTION ............................................................................................................ 1
CHAPTER 2 LITERATURE REVIEW................................................................................................. 5 Introduction...............................................................................................................................5 Gastro-Intestinal Absorption and Sodium Citrate.....................................................................5 Renal Regulation.......................................................................................................................8 H+ and K+ regulation at rest and during exercise...................................................................12
Proton - H+ ..........................................................................................................................12 Potassium - K+.....................................................................................................................15
Alkalosis at rest and during exercise ......................................................................................21 CHAPTER 3 MEASUREMENT OF DIALYSATE PH, REPRESENTATIVE OF INTERSTITIAL PH, AT REST AND DURING DYNAMIC LEG EXERCISE ................................................................... 27
Preface ....................................................................................................................................27 Introduction.............................................................................................................................28
PART I – IN VITRO VALIDATION OF MEASURING INTERSTITIAL PH USING MICRODIALYSIS AND BCECF ..........................................................................................................................................29
In vitro microdialysis components and system........................................................................29 Day to day stability of 2,7-bis-(2-carboxyethyl)-5-(and-6)-carboxyfluorescein (BCECF) dye.................................................................................................................................................32 Effect of albumin and stir rate on fluorescence using BCECF dye .........................................33 Influence of 1 cm polyurethane outlet tubing exposed to air...................................................34 Effect of HCl, La- and CO2 titrations on pH calibration curves..............................................35 Effect of dye concentration on pH calibration ........................................................................36 Effect of HCO3
- perfusate on pH calibration...........................................................................37 PART II – EFFECT OF PERFUSATE [HCO3
-] ON INTERSTITIAL PH IN VIVO......................................39 Methods...................................................................................................................................39
Subjects ...............................................................................................................................39 Exercise protocol.................................................................................................................39 Probe insertion and perfusate ..............................................................................................39 Fluorometric measurements and determination of pH ........................................................40
Results .....................................................................................................................................41 Discussion ...............................................................................................................................42
PART III – INTERSTITIAL PH AT REST AND DURING DYNAMIC LEG EXERCISE ...............................43 Methods...................................................................................................................................43
Subjects ...............................................................................................................................43 Exercise protocol.................................................................................................................43

Table of Contents
XII
Probe insertion and perfusate ..............................................................................................43 Fluorometric measurements and determination of pH.........................................................43
Results .....................................................................................................................................44 Interstitial pH at rest and during muscle activity .................................................................44 Recovery from exercise .......................................................................................................44
Discussion ...............................................................................................................................46 Changes in muscle interstitial pH during and after exercise................................................46 Recovery of interstitial pH ..................................................................................................48 Comparison between pH changes in muscle interstitium and blood ...................................48 Comparison between cellular and interstitial pH changes...................................................49 Physiological implications of changes in interstitial pH......................................................50
Conclusion...............................................................................................................................51 CHAPTER 4 EFFECT OF ALKALI INGESTION RATE ON PLASMA ACID-BASE, [H+], AND IONIC, [K+], STATUS...................................................................................................................................53
Introduction .............................................................................................................................53 Methods ...................................................................................................................................54
Subjects ...............................................................................................................................54 Experimental Protocol .........................................................................................................55 Blood collection...................................................................................................................55 Ingestion ..............................................................................................................................55 Measurement and Analysis..................................................................................................56 Statistics...............................................................................................................................56
Results .....................................................................................................................................57 Acid-base.............................................................................................................................57 Strong Ions ..........................................................................................................................62 pO2.......................................................................................................................................71 Urine....................................................................................................................................71
Discussion ...............................................................................................................................72 pO2 status.............................................................................................................................72 Sodium citrate and GI absorption ........................................................................................73 Sodium citrate and acid-base balance..................................................................................75 Ingestion time and [H+] .......................................................................................................76 Sodium citrate and [K+] .......................................................................................................76 Sodium citrate and urinary alkalosis....................................................................................77
Conclusion...............................................................................................................................78 CHAPTER 5 EFFECT OF SODIUM CITRATE ON INTERSTITIAL PH IN HUMAN SKELETAL MUSCLE ..................................................................................................................................79
Introduction .............................................................................................................................79 Methods ...................................................................................................................................81
Subjects ...............................................................................................................................81 Exercise protocol .................................................................................................................81 Experimental exercise intensity...........................................................................................82 Probe insertion.....................................................................................................................82 Perfusate ..............................................................................................................................82 Fluorometric measurements and determination of pH.........................................................83 Blood collection and analysis ..............................................................................................83 Ingestion ..............................................................................................................................84
Results .....................................................................................................................................84 Interstitial pH.......................................................................................................................84 Venous pH and HCO3
-.........................................................................................................87 Venous blood gases pO2 and pCO2 .....................................................................................90 Time to exhaustion ..............................................................................................................91
Discussion ...............................................................................................................................93 Conclusion...............................................................................................................................97
CHAPTER 6 GENERAL DISCUSSION..............................................................................................99

Table of Contents
XIII
Introduction.............................................................................................................................99 The importance of effective pH manipulation .........................................................................99 The importance of interstitial pH ..........................................................................................100 Limitations.............................................................................................................................102
CHAPTER 7 CONCLUSIONS AND FUTURE RESEARCH ......................................................... 103 Conclusions ...........................................................................................................................103 Future Research ....................................................................................................................104
REFERENCES ............................................................................................................................................ 107


List of Figures
XV
LIST OF FIGURES
Figure 1 Primary active transport of H+ into the renal tubule .........................................................9 Figure 2 Secondary active secretion of H+ into the renal tubule ....................................................11 Figure 3 Modified CMA60 microdialysis probe .............................................................................30 Figure 4 The complete fluorometric microdialysis system for the measurement of H+ in vitro......31 Figure 5 Day to day variability of 2,7-bis-(2- carboxyethyl)-5-(and-6)-carboxyfluorescein .........33 Figure 6 Effect of magnetic stir rate and albumin on [H+] measured with BCECF in vitro ..........34 Figure 7 Influence of 1 cm polyurethane tubing exposed to air on [H+] determination in vitro ....35 Figure 8 Titration curves for HCl-CO2 and HCl-La- ......................................................................36 Figure 9 Effect of BCECF dye concentration on pH calibration curves.........................................37 Figure 10 Effect of perfusate [HCO3
-] on pH calibration curves in vitro......................................38 Figure 11 Influence of [HCO3
-] on the estimation of interstitial pH during 10 W dynamic leg exercise............................................................................................................................................41 Figure 12 Interstitial acidification during exercise ........................................................................45 Figure 13 Peak interstitial pH during exercise at different power outputs.....................................46 Figure 14 Intracellular, interstitial and venous pH during knee-extensor exercise........................50 Figure 15 Blood pH 8-h temporal response....................................................................................57 Figure 16 Mean blood pH response pre- and post-ingestion..........................................................58 Figure 17 Blood pH relative change between PRE and 2 h post-ingestion ....................................58 Figure 18 Mean post-ingestion blood [HCO3
-] for all IR ...............................................................59 Figure 19 Mean blood [HCO3
-] temporal responses across 8 h for all IR .....................................60 Figure 20 Mean post-ingestion blood [pCO2] for each IR..............................................................61 Figure 21 Temporal response for blood [pCO2] for each IR..........................................................61 Figure 22 Individual IR temporal responses in blood [H+] for all conditions................................63 Figure 23 Mean (± SEM) blood [H+] for each IR at 3 time points .................................................64 Figure 24 Relative percent changes in blood [H+] .........................................................................64 Figure 25 Mean Blood K+ temporal profiles for all conditions ......................................................66 Figure 26 Mean (± SEM) blood [K+] for each condition at 3 time points ......................................67 Figure 27 Relative percent changes in blood [K+] .........................................................................67 Figure 28 Mean (±SEM) blood [Cl-] response for each condition .................................................68 Figure 29 Mean Cl- temporal response for each condition.............................................................69 Figure 30 Mean (±SEM) blood [Cl-] response at 3 time points......................................................69 Figure 31 Mean (±SEM) blood [Na+] response for all conditions .................................................70 Figure 32 Mean blood [Na+] temporal response for all conditions ...............................................70 Figure 33 Mean (±SEM) blood PO2 response for all conditions ....................................................71 Figure 34 Mean (±SEM) urine pH temporal response for each condition .....................................72 Figure 35 Interstitial pH temporal response..................................................................................85 Figure 36 Overall effect of sodium citrate ingestion on venous pH...............................................87 Figure 37 Venous pH temporal response.......................................................................................88 Figure 38 Overall effect of sodium citrate ingestion on venous [HCO3
-] ......................................89 Figure 39 Venous HCO3
- temporal response .................................................................................89 Figure 40 Venous pO2 status for both conditions placebo and alkalosis .......................................90 Figure 41 Venous pO2 temporal response.......................................................................................90 Figure 42 Venous pCO2 temporal response...................................................................................91 Figure 43 Time to exhaustion for both placebo and alkalosis conditions......................................92


List of Tables
XVII
LIST OF TABLES
Table 1 Ion concentration within plasma, interstitium and muscle.................................................13 Table 2 Blood acid-base and interstitial pH values with ingestion of CaCO3 (placebo) and Na3C8H5O7 (alkalosis).....................................................................................................................86 Table 3 Individual exhaustion times for intense knee-extensor exercise........................................92


List of Equations
XIX
LIST OF EQUATIONS
Equation 1 Calculation of pH .........................................................................................................21 Equation 2 Calculation for electrical neutrality .............................................................................24 Equation 3 Calculation of strong ion difference (SID) ...................................................................24


Abbreviations
XXI
ABBREVIATIONS
ATP – Adenosine Tri-phosphate
ATPase - Adenosine Tri-phosphatase
a-v difference – arterio-venous difference
BCECF – 2,7–bis–(2-carboxyethyl)-5-(and-6-)-carboxyfluorescein
BMI – Body Mass Index
EDL – Extensor Digitorum Longus
Ex - Exercise
Exh - Exhaustion
GI – Gastro-intestinal
Ing - Ingestion
IOC – International Olympic Committee
IR – Ingestion Rate
MVC – Maximum Voluntary Contraction
NAE – Net Acid Excretion
NMR – Magnetic Resonance Spectroscopy
NVA – Non-Volatile Acid
PFK – Phosphofructokinase
RBC – Red Blood Cells
Rec - Recovery
SB – Sodium Bicarbonate
SC – Sodium Citrate
SE – Standard Error
SEM - Standard Error of Mean
SID – Strong Ion Difference
TA – Titratable Acid
VO2peak – Peak Oxygen Consumption per minute
Chemical Formulas: Ca2+ - Calcium
CaCO3 – Calcium Carbonate
Cl- - Chloride
CO2 – Carbon Dioxide
H+ - Hydrogen Ion/Proton
H2CO3 – Carbonic Acid

Abbreviations
XXII
Hb – Haemoglobin
HCl – Hydrogen Chloride
HCO3- - Bicarbonate
K+ - Potassium
KOH – Potassium Hydroxide
La- - Lactate
Mg2+ - Magnesium
Na+ - Sodium
Na3C8H5O7 – Sodium Citrate
NaHCO3- - Sodium Bicarbonate
NaOH – Sodium Hydroxide
NH4 – Ammonia
pCO2 - Partial Pressure of Carbon Dioxide
PCr2- - Phosphocreatine
pH – “Pouvoir Hydrogene” (Hydrogen Concentration)
pO2 - Partial Pressure of Oxygen
PO4 - Phosphate
SO42- - Sulfate
Units of Measurement: µl – microlitre
da – Daltons
g – grams
g.l-1 – grams per litre
h – hour
Hz - Hertz
Kg – Kilograms
M – Molar
m.mol.l-1 - millimoles per litre
meq.h-1 – milli-equivalents per hour
meq.l-1 – milli-equivalents per litre
mg.kg-1 – milligrams per kilogram
mg.min-1 – milligrams per minute
min – minutes
ml – millilitre
mM – millimolar
mmHg – millimetres of mercury

Abbreviations
XXIII
mOsm.l-1 – milliosmolar per litre
mOsmol.kg-1 – milliosmolar per kilogram
mV – millivolt
N – Nolar
neq.l-1 – nano-equivalents per litre
nM - nanomolar
s - seconds
W – Watt


Statement of Original Authorship
XXV
STATEMENT OF ORIGINAL AUTHORSHIP
The work contained in this thesis has not previously been submitted for a
degree or diploma at any other higher education institution. To the best of my
knowledge, this thesis does not contain any material previously published or
written by any other person, except where due reference is made.
_______________________
Candidates Signature
8/8/2003


Acknowledgements
XXVII
ACKNOWLEDGEMENTS
This thesis would not have made it to completion without the assistance of
some great people. I would like to take this opportunity to express my
sincere gratitude to them.
Dr Simon Green I would like to thank my principle supervisor, Dr Simon Green for inspiring me
to embark on a journey that has provided me with many rewards. His
continual encouragement and support throughout my candidature is greatly
appreciated.
Associate Professor Carsten Juel The opportunity to perform the Danish experiments would not have been
possible without the efforts of Associate Professor Carsten Juel. My sincere
appreciation is extended to him for this and his kind hospitality. Tusind tak.
Associate Professor Andrew Hills To my associate supervisor, Associate Professor Andrew Hills, thank you for
your thoughtful comments on the final preparation of this thesis.
Ms Connie Wishart Thank you to Connie for her genuine willing, friendly and caring nature that
made the long days in the laboratory seem so much shorter and all the years
easier to pass.
Volunteers A sincere thank you to all the subjects that volunteered from the exercise
physiology class of Semester 1, 1997. Your efforts were outstanding over an
arduous 10 h day. Also, an earnest thank you for the efforts of my Danish
friends and colleagues who volunteered their time and body’s for my
experiments in Copenhagen.

Acknowledgements
XXVIII
Team AKI A special thank you to the team at the August Krogh Institute that made my
time in Copenhagen so productive and enjoyable. In particular, I would like
to especially thank Associate Professor Jens Bangsbo for his unique
combination of professionalism and comic relief in the laboratory and Mr Jens
Jung Nielsen for his great depth of talent with microdialysis and always
cheerful demeanour.
Institutions Thank you to the institutions that have provided the financial, administrative
and infrastructural support necessary to enable the production of this thesis;
the Copenhagen Muscle Research Centre, August Krogh Institute, Danish
Research Agency and Queensland University of Technology.
Comrades To all my fellow comrades I gratefully thank you for the mateship you have
provided over the years. In particular, to Glenn, Chris, Jarrod, Nuala and
Kate thank you for helping me through the ‘downs’ and being there for the
‘ups’.

Chapter 1 - Introduction
1
CH A P T E R 1 IN T R O D U C T I O N
Before detailing the physiology relating to sodium citrate ingestion and
skeletal muscle function in the literature review, it will be useful to outline in
brief the importance of pH regulation at rest and during exercise. At rest,
muscle pH is slightly alkaline and constantly regulated around 7.10 (Juel,
1998a) to maintain optimal cell functioning. The alkaline pH value at rest
helps to buffer the small amounts of acid produced via basal metabolism,
however, during intense exercise cellular metabolism produces large amounts
of H+ that are released within the cell, thus rapidly decreasing intracellular
pH. Decreased intracellular pH has negative effects on several important
mechanisms within the cell. Low intracellular pH inhibits the rate limiting
enzyme of glycolysis, phosphofructokinase (PFK) (Hermansen, 1981) and
interacts with the contractile proteins during contraction (Mainwood &
Renaud, 1985). Free H+, concomitant with low pH, compete with Ca2+ at the
binding site of troponin, thereby interfering with myofilament cross-bridge
cycling (Donaldson & Hermansen, 1978). In contrast, pyruvate
dehydrogenase activity (Hollidge-Horvat et al., 1999) and La- transport from
within the intracellular compartment are all increased at low pH. These
examples are not definitive or causative links to fatigue, but rather used to
demonstrate the extent to which low pH can effect metabolism within the
muscle cell. Collectively, the above effects of low pH during intense exercise
reduce the cells’ ability to maintain force development by both energetic
and/or chemical/mechanical interference.
To combat the interference of the cellular metabolism H+ load, skeletal muscle
possess a triad of defence systems, physicochemical buffering, consumption
or production of non-volatile acids and transmembrane fluxes of H+ and HCO3-
. When blood flow is occluded from muscle, such as during isometric exercise
at >20 percent MVC, and intracellular PCO2 is constant the physicochemical
system buffers more H+ (Sahlin, 1978a). The physicochemical buffering
system can also be sub-divided into three categories involving phosphates,
proteins, and bicarbonate buffer systems. The combined efforts of all of the
above systems attempt to buffer excess metabolically produced H+ and thus
maintain intracellular [H+] and pH.

Chapter 1 - Introduction
2
The muscle cell is separated from the capillary blood supply by the interstitial
space or interstitium. When substances leave the intracellular space they first
pass into the interstitium before entering the blood. Therefore, metabolite
concentration within the interstitium will influence ionic movements between
the intra and extracellular compartments. In addition, circulating interstitium
substances have been identified as potential mediators in important
processes, such as blood flow (Quayle et al., 1997) and sympathetic nerve
activity (Victor et al., 1988). Approximately a decade ago, the first in vivo
measurements of interstitial metabolites within skeletal muscle using the
microdialysis technique were being attempted. Recently, this method has
been successful in measuring a number of interstitial metabolites including,
lactate (Rosdahl et al., 1998), insulin (Sjostrand et al., 1999), glucose
(Maclean et al., 1999) and potassium (Green et al., 1999) at rest and during
exercise. Although it is possible to measure [H+] in muscle and blood, a
method has not been established to measure interstitial pH. One reason for
this has been due to the difficulty in controlling the movement of both HCO3-
and CO2 within the PVC tubing used in Microdialysis. As a result, no
investigations have been performed on pH regulation within skeletal muscle
interstitium in vivo. For this reason, the movement of H+ within the
interstitium is not well understood, the movement of H+ out of skeletal muscle
and into the capillary network, however, has been well documented (Bangsbo
et al., 1993a; Lindinger & Heigenhauser, 1991; Juel et al., 1990).
Efflux of H+ from muscle into the blood decreases blood pH. To maintain a
positive gradient required for continual efflux from the muscle, the additional
H+ must be buffered and removed from the contracting muscle. The same
buffer systems present in muscle are located within the blood, except that the
bicarbonate system is now the most heavily relied upon. This system consists
of two key elements, HCO3- and CO2, which can be regulated by the kidneys
and lungs. The ability to regulate these compounds enables blood pH to be
adjusted in both directions and greatly increases its capacity. Although the
capacity of the blood system is far greater, it remains finite. If high rates of
metabolically produced H+ continue, the electrochemical balance between
intra and extracellular compartments will be disturbed, compromising the
cell’s ability to move H+, resulting in both decreasing blood and muscle pH.
Consequently, the blood buffering systems will only delay increasing [H+]

Chapter 1 - Introduction
3
effects on intracellular metabolic processes that reduce the muscle’s ability to
produce force, i.e., muscle performance.
Increasing one or all of the buffer systems’ capacities, either intracellularly or
in the blood, has the potential to further delay the onset of a critical pH level,
thereby increasing the time for muscle to maintain force production. The
ingestion of sodium bicarbonate or sodium citrate results in an increase in the
capacity of the blood bicarbonate system (Kowalchuk et al., 1989; Costill et
al., 1984). In addition, the ingestion of either of these compounds disturbs
the blood acid-base balance causing a decrease in [H+] or increase in pH (Ball
& Maughan, 1997; Jones et al., 1977b), referred to as being in a state of
alkalosis. Theoretically, manipulating blood [H+] and [HCO3-] via inducing
alkalosis will improve muscle function or muscle performance. Numerous
investigations of ingesting sodium bicarbonate or sodium citrate prior to
exercise have led to increases in swimming (Gao et al., 1988), running
(Shave et al., 2001), cycling (Potteiger et al., 1996a) and rowing
(McNaughton & Cedaro, 1991) performances. Even so, there is evidence to
demonstrate the contrary across each of these modes, respectively (Schabort
et al., 2000; Robinson, 1997; Ibanez et al., 1995; Pierce et al., 1992).
As is often the case with orally induced drugs, there exists a dose-response
relationship. That is, there is a minimum quantity of the drug that must be
consumed to manipulate the system to a high enough degree to enable the
observation of a significant effect. Although this work has been performed
(Horswill et al., 1988) (McNaughton, 1992a; McNaughton, 1990) and a
minimum dose identified, 300 mg.kg-1 for both sodium bicarbonate and
sodium citrate, it was tested across one ingestion regime only, namely bolus.
It may be possible that other ingestion regimes have differing effects.
Investigations that have followed similar dosing strategies have not found
positive effects of sodium bicarbonate (Tiryaki & Atterbom, 1995) or sodium
citrate ingestion (van Someren et al., 1998). Further, some studies have
shown gastro-intestinal side effects when ingesting sodium bicarbonate
(Webster et al., 1993), and sodium citrate (Shave et al., 2001) to a lesser
extent, in bolus form. Systematic exploration of ingestion regime has yet to
be performed on either of these alkalis. Such investigations are important as
they might reveal that lower doses ingested more slowly invoke similar
physiological effects, but with reduced side effects.

Chapter 1 - Introduction
4
Therefore, the aims of this thesis are to: a) develop a new method for
determination in vivo of interstitial pH at rest and during exercise, b)
systematically explore the effects of different ingestion regimes of 300 mg.kg-
1 sodium citrate on blood and urine pH at rest, and c) to combine the new
interstitial pH technique with the findings of the second investigation, in an
attempt to provide a greater understanding of pH within the extracellular
compartment.

Chapter 2 – Literature Review
5
CH A P T E R 2 LI T E R A T U R E RE V I E W
Introduction As outlined in the preface, the objective of this literature review is to provide
information about the specific physiology pertaining to sodium citrate
ingestion and pH regulation in skeletal muscle. The four main sections,
gastro-intestinal absorption and sodium citrate, renal regulation, H+ and K+
regulation at rest and during exercise, and alkalosis at rest and during
exercise, in turn, discuss the existing research relevant to the experimental
studies and identify the need for further research.
Gastro-Intestinal Absorption and Sodium Citrate A potentially large factor that influences the degree to which induced alkalosis
affects the muscle cell is the gastro-intestinal (GI) system. That is, how the
alkali will be introduced to the body will play a role in how it will eventually
affect the muscle cell. The two main ways of introducing an alkali to the body
are orally and intravenously. The most common method used in research of
skeletal muscle function is orally, probably due to the ease of use in the
applied setting. Since this is the case, the rate at which the alkali is
introduced to the GI system will directly affect the time it takes to manipulate
blood pH. Although there has been an abundance of research investigating
sodium bicarbonate metabolism through the GI system (Kuu et al., 1998;
Belangero & Collares, 1992; Busse et al., 1989), little has been performed
with sodium citrate (SC). Therefore, it is not completely understood how SC
is metabolised within the GI system, although it seems logical that when
introduced it dissociates into its constituent ions, sodium and citrate. The GI
metabolism of these ions is very well understood and is considered hereafter.
At a given dose of 0.4 ml.kg-1, SC increases gastric pH from 2.5 to 6.11
(Hauptfleisch & Payne, 1996). The direct mechanism for this process is not
known and further GI investigation is required to ascertain this. It is,
however, known that the level of acidity within the GI system has a direct
effect on the rate of digestion (Guyton, 1991). It is possible that the increase
in pH associated with the ingestion of SC may in itself have a direct effect on
absorption through the GI system. If SC dissociates into its constituent ions,

Chapter 2 – Literature Review
6
then the mechanisms and factors that contribute to its absorption may differ
from the absorption of the molecule as a whole.
The absorption of Na+ from the GI system takes place in the small intestine.
The active process to transport Na+ out of the small intestine involves two
steps (Schultz, 1984). The first is to move the Na+ into the intestine epithelia
and the second is to move it out into the interstitial space. Although the
objective is to move Na+ from the small intestine lumen, the process begins
by actively transporting Na+ out of the epithelia across the basolateral
membrane and into the interstitial space. In doing so, the epithelia
intracellular [Na+] is reduced to ~50 meq.l-1 and thus creates a steep
electrochemical gradient for Na+ to move out of the chyme (~140 meq.l-1)
and into the epithelia cell (Wright & Loo, 2000). In effect, it replaces the
actively transported Na+.
There are two positive side effects of this process. The first being a
concurrent movement of Cl- and the second a constant movement (in effect,
absorption) of water from the small intestine to the interstitial space (Binder
et al., 2000). Since there is a large electrochemical attraction between Na+
and Cl-, the movement of Na+ in itself, draws Cl- to follow out of the epithelia
and into the interstitium (Liedtke, 1989). Chloride within the small intestine
then has two forces acting upon it to move into the epithelia, a concentration
gradient and the strong electrical attraction of Na+ moving into the cell. The
large increase in ions present in the interstitium creates an osmotic pressure
forcing water to move from within the epithelia cell into the interstitial space,
continuing to the capillary supply of the villi (Schultz & Dubinsky, 2001). The
reduction of water within the epithelia cell creates another gradient between
the lumen of the small intestine, which draws water from the chyme into the
cell. These processes combined create an almost constant flow of Na+, Cl-
and water between the lumen of the small intestine and the capillary blood
supply of the villi (Schultz, 1984).
The second dissociated constituent to be considered is citrate. Absorption
through the GI tract can be influenced by many different factors. The volume
of secreted gastric acid and bile can alter the breakdown of foodstuffs into its
constituents and thus delay the start of absorption processes through the
duodenal wall. These factors do not appear to severely limit the digestion of

Chapter 2 – Literature Review
7
citrate as Erskine and Hunt (1981) showed that approximately half the
quantity of SC when orally ingested reached the duodenum within three
minutes. Others have suggested that the caloric content of a meal is not an
important limiting factor (Hattner, 1991), however Moore et al. (1981) have
shown a positive relationship between the caloric content of a meal and its
emptying rate from the GI tract. The caloric value of SC is very low, almost
negligible, which would tend to rule out any effect this factor might have on
its absorption. The form of a meal, liquid or solid, appears to have a
significant impact on the emptying rate from the GI tract. Notivol et al.
(1984) demonstrated a liquid meal empties from the duodenum ~35 percent
faster than a solid meal.
Some investigators have attempted to look for relationships between
individual physical characteristics and GI function. However, their
investigations showed that no relationship exists between anthropometric
data and GI function in humans (Notivol et al., 1984; Moore et al., 1981).
Notivol et al. (1984) did find differences between male and female GI
function. In addition to a slower GI function, females also exhibit variance in
gastric emptying corresponding to the phase of their menstrual cycle.
MacDonald (1957) showed an increase in gastric emptying on day 14 that
gradually decreased as the cycle continued. Further, gastric pH increased
during days one to fourteen of the menstrual cycle, but reversed during days
fifteen to twenty-eight.
Vist and Maughan (1995) tested two concentrations of carbohydrate in liquid
form, high (188 g.l-1) and low (40 g.l-1), and found the high concentration
emptied slower from the duodenum. Further, they found that by increasing
liquid osmolality, gastric empting was diminished, although not to the same
extent. The work of Erskine and Hunt (1981), demonstrating that glucose
enters the duodenum at 5%.min-1 compared with 15%.min-1 for citrate,
supported these findings. Citrate entered the duodenum three-fold faster
than glucose. This may have important implications for the commonly
practised administration of citrate in bolus form (Schabort et al., 2000),
whereby the citrate is added to a glucose/carbohydrate solution. By ingesting
citrate in this manner, it may decrease the uptake and any corresponding
effect in the blood. Other factors that alter gastric emptying include circadian
rhythm (Goo et al., 1987) and smoking (Notivol et al., 1984). Although

Chapter 2 – Literature Review
8
ingesting foodstuffs at 20.00 hrs decreases gastric emptying half time by ~30
percent, circadian rhythm has no effect on the digestion of liquids. In
contrast, people who smoke have an increased gastric emptying rate
compared to those who do not smoke (Notivol et al., 1984).
Renal Regulation Systemic pH is tightly regulated due to large effects of relatively small
disturbances. A key organ involved in the regulation of systemic pH is the
kidney (Tannen, 1980). The kidney controls the amount of acid and base
excreted or reabsorbed to maintain systemic pH stability. Specifically, this is
performed by balancing the amount of HCO3- and H+ secreted into the tubule
for excretion (Hopfer & Liedtke, 1987). When more HCO3- is removed from
the blood and extracellular compartments and secreted via the glomerular
filtrate, more HCO3- will be present in the urine increasing its alkalinity while
reducing the alkalinity of systemic pH. Conversely, an increase in the removal
of H+ from the blood and extracellular compartments and followed by
secretion from the tubular epithelia will result in an increase in the acidity of
the urine while reducing the acidity of systemic pH (Maren, 1988). Thus by
manipulating these two pathways the kidney has the ability to tightly regulate
systemic pH. At normal extracellular pH, 7.4, HCO3- and H+ are secreted at
3.46 and 3.50 mmol.l-1, respectively. Therefore, at rest, slightly more acid is
excreted to accommodate the small amount (0.8 meq.kg.day-1) of acid
continually produced via metabolism, thereby reducing normal resting urine
pH to ~6.0 (Cogan et al., 1990; Oster et al., 1988; Kachadorian & Johnson,
1970).
The regulation of H+ via the kidneys is the result of two mechanisms, primary
active transport and secondary counter transport (Eiam-Ong & Sabatini,
1996). Primary active transport relies on the diffusion of CO2 from the
extracellular compartment into the tubular epithelia (Ilundain, 1992). The
CO2 combines with water to form carbonic acid (H2CO3), which quickly
dissociates into HCO3- and H+. The H+ is then actively moved across the
tubular membrane via an ATP driven process. Once the H+ is in the tubule it
is excreted in the urine. The remaining HCO3- within the epithelia is
reabsorbed into the extracellular space via an HCO3-/Cl- exchanger with the
Cl- passively lost to the urine (Pajor, 1999). The net result being for each H+

Chapter 2 – Literature Review
9
secreted to the urine, there is a loss of one Cl- and reabsorption of one HCO3-
(Boyarsky et al., 1988) This process is normally responsible for less than 5
percent of the regulation of H+ due to its location in the distal part of the
tubule and a large (up to 900-fold) concentration gradient (see Figure 1)
(Tanner, 1980).
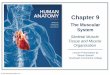
Figure 1 Primary active transport of H+ into the renal tubule
The diffussion of CO2 into the epithelial cell results in the formation of H+, which is transported into the tubule via an ATP-driven process. Associated with this process is the passive movement of Cl- into the tubule. Figure adapted from Guyton (1991).
Secondary active transport again relies on the simple diffusion of CO2 from
the extracellular fluid into the tubular cell and follows the same steps to
dissociate into both HCO3- and H+ (Dunn & Walley, 1991). However, the H+
takes an alternative path and is moved into the tubular lumen via the positive
gradient of Na+ in counter transport (Krapf, 1989). In effect, for each H+
TUBULE EXTRACELLULAR
CI-
H+
CI-
ATP
ADP
CI-
HCO-3 HCO-
3 + H+
H2CO3
H2O +
CO2 CO2

Chapter 2 – Literature Review
10
removed there is a net reabsorption of Na+. The H+ then combines with
tubular HCO3- to reform H2CO3, which again dissociates into CO2 and water to
be excreted in the urine (Guyton, 1991). Although most segments of the
nephron participate in acid-base balance, regulation of HCO3- occurs mainly
(70-90 percent) via the glomerular filtrate in the proximal tubule of the
kidney (Eiam-Ong & Sabatini, 1996). When the HCO3-:CO2 increases, CO2
movement into the tubular cell is decreased, which in turn leads to a lower
H2CO3 concentration available to dissociate into HCO3- and H+. This reduces
the amount of H+ available to actively transport into the tubular lumen and be
excreted in the urine. Concurrently, in the glomerular filtrate, the excess
HCO3- is being transported into the proximal tubule at a much higher rate,
resulting in an increased concentration of HCO3- in the urine (Pajor, 1999).
The net result is alkaline urine due to both a low [H+] and high [HCO3-]. The
removal of HCO3- decreases the buffer concentration within the extracellular
space and shifts pH in the acid direction, cf. the Henderson Hasselbach
equation. This is further enhanced by the isohydric principle that states, ‘all
buffer systems will move in the acid direction in an attempt to correct
alkalosis’ (see Figure 2)(Guyton, 1991).
Ingestion of 2 mmol.kg-1 NaHCO3- increases plasma HCO3
- by 4 meq and
blood pH by 0.02 units (Cogan et al., 1990). In an attempt to restore this
disturbance to acid-base balance the two mechanisms previously mentioned
result in the following observations. As aforementioned, normal urinary pH is
approximately 6.0, however, under conditions of alkali ingestion the urinary
pH can climb to values as high as 8.0 while attempting to rid the body of
excess base (author’s unpublished observation). Oster et al. (1988) found
that renal net acid production was reduced by 70 percent in an attempt to
reverse the effects of SC ingestion. The process to rectify such imbalances
via the renal system is not fast. In fact, the system is only capable of
excreting about 500 mmol of excess acid or base each day (Dunn & Walley,
1991). Amounts greater than this will result in disturbances that the renal
system will be unable to cope with and major disturbances to extracellular
normality will result. If left untreated, the ensuring alkalosis will cause over
excitability of the neural system resulting in tetany and could be fatal in the
form of tetany of the respiratory muscles (Tanner, 1980).

Chapter 2 – Literature Review
11
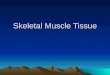
Figure 2 Secondary active secretion of H+ into the renal tubule
Sodium reabsorption in exchange for proton ions secreted, proton and bicarbonate ions combine in the tubule to form carbon dioxide and water. Figure adapted from Guyton (1991).
To further aid the bicarbonate buffer system in combating acid-base
disturbances, the renal system can reabsorb ‘new’ bicarbonate (Maren, 1988).
The mechanism occurs largely in conjunction with the removal of excess H+.
When H+ is finally transported to the tubular lumen it will combine with HCO3-,
collected in the proximal tubule, to again form H2CO3, which then dissociates
into water and CO2. This CO2 rapidly diffuses back into the tubular epithelia,
and under the influence of the enzyme carbonic anhydrase combines with
water to form H2CO3 once again. Dissociation again occurs leaving the two
original components HCO3- and H+. Proton is then moved back into the lumen
via the processes mentioned above, while decreased K+ levels stimulate the
enzyme H,K-ATPase to transport HCO3- out of the cell and back into the
extracellular compartment (Eiam-Ong & Sabatini, 1996). In effect, this
Na+ + HCO-3
Tubule Extracellular Fluid
Na+
H+
H2CO3
CO2 + H2O
(Carbonic anhydrase)
Na+ Na+ - H+Active transport
K+ K+
HCO-3 + H+
Na+
+
HCO3 Counter transport
H2CO3
H2O +
CO2 CO2

Chapter 2 – Literature Review
12
process re-introduces newly generated HCO3- back into the circulation, thus
helping to maintain the HCO3- buffer system’s integrity.
H+ and K+ regulation at rest and during exercise
Proton - H+ It has been well documented in both animal and human skeletal muscle
investigations that muscle acidity increases with high intensity exercise
(Hermansen, 1979; Sahlin et al., 1978b) (Juel & Pilegaard, 1998; Bangsbo et
al., 1996; Thompson et al., 1992). Many experiments have demonstrated
that muscle acidity has major regulatory effects on numerous mechanisms,
including key energetic pathways (Spriet et al., 1987; Sutton et al., 1981),
membrane transport systems (Juel, 1998b; Juel et al., 1994; Davies, 1990;
Inesi & Hill, 1983), excitation-contraction coupling (Donaldson & Hermansen,
1978; Fabatio & Fabatio, 1978), and blood flow (Aalkjaer & Peng, 1997). In
contrast, there exists some controversy as to whether or not [H+] per se is
responsible for these effects (Spriet, 1991a; Ren & Hultman, 1989). As it
appears that the results are not yet conclusive, it is therefore important to
continue to develop new techniques that will assist in providing a greater
understanding of the intricate regulation of H+.
Approximately 45-75 percent of the body is comprised of fluid. The fluid
within the body can be divided into intracellular and extracellular
compartments. Approximately 55 percent of the total body fluid is contained
within the intracellular compartment. The extracellular space can be
subdivided to consist of blood and interstitial fluid. Each of these
compartments contains approximately 4 and 16 percent of the total body
fluid, respectively. Therefore, the regulation of intracellular [H+] is firstly
influenced by the cytosol and interstitial fluid that are separated by the
sarcolemma. Although, muscle, interstitium and plasma are osmotically and
electrically neutral at rest, selective permeability between these
compartments maintains a unique ionic composition (Table 1) (Kowalchuk &
Scheuermann, 1995). The exact composition of these compartments will be
influenced by the hydration status of the individual as evidenced by disparity
in the literature (Kowalchuk & Scheuermann, 1995).

Chapter 2 – Literature Review
13
This table is not available on line. Please consult the hardcopy thesis available
at the QUT Library.
Table 1 Ion concentration within plasma, interstitium and muscle
This table shows the ionic concentrations of the major anions and cations within each respective compartment (Aickin & Thomas, 1977)
Intracellular pH at rest is kept slightly alkaline to offset small amounts of acid
produced via basal cellular metabolism (Bangsbo et al., 1993a; Costill et al.,
1983). In addition, H+ continually passively fluxes across the sarcolemma
due to electrochemical forces (Juel, 1998a). Thus to prevent the
accumulation of intracellular H+ at rest, it is necessary for skeletal muscle to
possess mechanisms through which H+ can be transported out of the cell.
Transporters that envelop this ability include the Na+/H+ exchanger (Juel,
1998b) and HCO3- exchangers (Putnam, 1990).
The contribution of these exchangers at rest is not well defined. Several
investigators have attempted to describe the contribution of the Na+/H+
transporter by inhibiting its function with amiloride (Juel, 1995; Kemp et al.,
1994; Grossie et al., 1988). However, the results of these investigations
showed only modest intracellular acidification without the Na+/H+ pathway.
Evidence from animal studies would suggest that up to 20 percent of pH
regulation in mouse slow twitch fibres is managed by a bicarbonate transport
system (Aickin & Thomas, 1977), while more recent investigations using
vesicles from homogenised rat skeletal muscle suggest a capacity similar to
that of the Na+/H+ transporter (Juel, 1995).
During exercise, metabolism is increased. It has been well documented that
this is associated with an increase in intracellular [H+] (Sullivan et al., 1994;

Chapter 2 – Literature Review
14
Spriet et al., 1989; Greenhaff et al., 1988; Costill et al., 1983). To maintain
optimal cell functioning and relocate the additional H+, there is a high demand
for the transport systems to increase their rate. To assist with the increased
demand additional transporters are involved during exercise. Furthermore,
H+ can passively diffuse across the sarcolemma in the form of undissociated
lactic acid (Juel, 1996). In both animals (Juel & Pilegaard, 1998; Lindinger &
Heigenhauser, 1991; Seabury et al., 1977) and humans (Bangsbo et al.,
1997) the function and capacity of the La-/H+ transporter has been
investigated. The study by Juel (1995) demonstrated the functional
capacities of the three H+ transporters in rat hind limb muscle using giant
sarcolemmal vesicles. His data showed that the La-/H+ system capacity was
approximately eight- and five-fold larger than the Na+/H+ and HCO3- systems,
respectively. This is further supported by the findings of Westerblad and Allen
(1992) that demonstrated no effect on force production and intracellular pH
when the Na+/H+ transport system is blocked with amiloride in mouse skeletal
muscle. Therefore, the La-/H+ co-transporter is of major importance in
exporting H+ out of the cell during exercise. However, there are additional
mechanisms at play including; passive movement, Na+/H+ exchange, HCO3-
systems and diffusion of undissociated lactic acid. Together, these systems
assist in the maintenance of an optimum intracellular pH environment.
At the cessation of intense exercise, intracellular [La-] is high and pH can
decrease to values as low as ~6.56 (range 6.4 – 6.7) (Bangsbo et al., 1996;
Spriet et al., 1987; Costill et al., 1983; Hermansen, 1981; Sahlin et al.,
1978b). While the intracellular [La-] remains high, there exists a large
positive gradient from muscle to interstitium and plasma. The La-/H+ co-
transport system is largely regulated by increases in intracellular [La-] and
relatively insensitive to the increased [H+] (Juel, 1996). However, later in
recovery when the La- gradient is low and the [H+] is approximating resting
values, the Na+/H+ transport system’s sensitivity to these [H+] re-activates it
to finely tune the intracellular [H+] to resting levels (Juel, 1996). Further, it
has been suggested that the HCO3- systems may also contribute to this fine-
tuning process (Putnam & Roos, 1986a).
It should be noted that the regulation of H+ within the interstitium is
remarkably unexplored and as such poorly understood. The importance of
this sub-compartment of the extracellular space has been identified by others

Chapter 2 – Literature Review
15
that have suggested that interstitial [H+] can influence H+ efflux from the
muscle cell (Roth & Brooks, 1990). Recently, interstitial [H+] has been
measured in humans using microdialysis and pH sensitive electrodes placed in
the dialysate (outflow) (Maclean et al., 2000). The data reported in this study
does not immediately concur with previous investigations of muscle and blood
pH. As mentioned above, there is sound support for the regulation of
intracellular H+ via exchangers and passive diffusion. Further, the same
investigators and others (Lindinger et al., 1992) report increases in blood [H+]
associated with intense exercise. Therefore, it seems reasonable to assume
that the H+ removed from the muscle cell will inevitably end up in the
interstitium and then further to the blood. If this is the case, the interstitium
[H+] would increase (decrease pH). However, this is in direct contrast to the
findings reported by Maclean et al. (2000). They report a mean±SEM resting
interstitial pH of 7.162±0.023 and almost immediately after the initiation of
exercise, a decrease in interstitial [H+]. This exercise-induced interstitial
alkalosis is observed for the full duration of exercise and very sharply returns
to pre-exercise levels at the cessation of exercise. It seems peculiar that
muscle H+ efflux to the blood via the interstitial space during intense exercise
would result in a decline in interstitial [H+]. Further investigations are
required to validate the microdialysis method and clarify H+ regulation within
this extracellular compartment.
Potassium - K+ Arterial K+ is an important factor in many mechanisms of control, including
ventilation (McCoy & Hargreaves, 1992; Busse et al., 1992), circulation
(Fallentin et al., 1992), cardiac arrhythmias (Kjeldsen, 1991) and has been
suggested as a regulator of muscle function (Juel, 1986). It is this last role
that is most interesting and pertinent to this thesis.
The propagation of an action potential is required for the activation of both
neural and skeletal tissue (Fitts & Balog, 1996). In skeletal muscle, the action
potential is initiated by a negative electrical imbalance created across the
sarcolemma. Constantly shifting three Na+ ions out of and two K+ ions into
the muscle cell creates high and low intracellular concentrations of K+ and
Na+, respectively (Fitts & Balog, 1996). Concurrently, a negative electrical
imbalance or membrane potential between intra and extracellular

Chapter 2 – Literature Review
16
compartments is generated. This active process is mediated by a pump
mechanism driven by ATP hydrolysis and is commonly referred to as the Na-K
pump or Na-K ATPase (Brody & Akera, 1977). To increase the complexity of
the process, specialised K+ channels within the sarcolemma constantly allow
K+ to leak out of the cell, thereby decreasing intracellular [K+] and thus the
membrane potential (Sakobe et al., 1991). In order to maintain the
membrane potential, the Na-K pump must replenish the intracellular [K+] at a
rate equal to the K+ lost through the channels.
Two factors that aid in this process are the total number and location of the
Na-K pumps within a cell. The pump numbers are far in excess of that
required to maintain K+ concentrations. Only 2-6 percent of the pumps need
to be activated to maintain [K+] within the cell (Clausen et al., 1987; Clausen,
1986). The location of the pumps are restricted to certain parts of the
interstitium, decreasing K+ travelling distance, thereby reducing repeated
depolarisation-repolarisation time (Wasserman et al., 1997). The capability of
the Na-K pump has recently been theoretically described using a
mathematical approach (Lindinger et al., 1995). By removing Na-K pump
activity from the K+ regulatory process and using K+ kinetic data from
previous experiments, they calculated the subsequent rise in arterial plasma
[K+] as a result of continual loss through K+ channels. The calculations
demonstrate that cycling at 400 percent VO2peak for 30 s without the use of
the Na-K pump, arterial plasma [K+] would increase from 6.3 (recorded) to 27
mmol.l-1. Such an increase in arterial plasma [K+] would result in
disturbances to the cells’ ability to maintain the membrane potential and
generate action potentials, which would compromise muscle cell contraction
and force production. Further experimental work has demonstrated that
hyperkalemia is due to a failure of the Na-K pump to keep pace with K+ loss
from the muscle cell during contraction (Wasserman et al., 1997; Lindinger et
al., 1995).
Prior to the onset of exercise, the Na-K pump ensures K+ is the main ion
intracellularly and Na+ extracellularly. However, at the onset of exercise, the
intracellular environment is perturbed. Specifically, other non-diffusible anion
concentration is altered and due to the physicochemical laws of ions in
solution, K+ is released from the cell via K+ channels. The increased K+ efflux
via these K+ channels decreases intracellular [K+] thus signalling the pumps to

Chapter 2 – Literature Review
17
increase activity in an attempt to restore intracellular [K+] (Wasserman et al.,
1997).
Continual muscle activity results in K+ loss from the cell with the majority of
efflux occurring during the repolarisation phase of the muscle action potential
(Marcos & Ribas, 1995). Studies using mice (Juel, 1986) have shown
intracellular K+ loss during stimulation only accounts for half of the associated
depolarisation, suggesting K+ leaked out through the channels and into the
interstitium. Further interstitial measurements showed a concurrent two-fold
increase in [K+]. It has been demonstrated (Clausen, 1986) that intracellular
K+ and interstitial K+ concentrations are regulated by the Na-K pump and K+
channels, and that the amount of efflux into the interstitium is proportional to
the frequency of muscle action potentials (Marcos & Ribas, 1995).
Blood flow into the muscle (arterial) and blood draining the muscle bed
(venous) are both influenced by the release of K+ from the muscle via the
interstitium. Venous blood is the first compartment to be affected due to the
collection of metabolites from the active muscle. Release from muscle is very
rapid and increases femoral vein [K+] during the first 3 minutes of both high
and low intensity exercise (Wasserman et al., 1997). It appears that trained
status has no bearing on the peak venous values obtained during intense
exercise. During cycling to exhaustion in two groups, cyclists and controls
exercising at the same relative intensity but exhibiting markedly different
absolute values (400 and 250 W respectively) elicited indifferent venous K+
changes of 35 and 31 percent, respectively (Marcos & Ribas, 1995). In
contrast, arterial K+ efflux of cyclists was greater compared with control
subjects. A possible explanation for this was an up regulation of the Na-K
pump numbers with training, thereby increasing the amount of K+ reabsorbed
into the muscle cell and reducing the concentration with the plasma (Marcos &
Ribas, 1995). Resting arterial blood [K+] is approximately 4.0 mmol.l-1,
however, during intense exercise this can increase as high as 6.3 mmol.l-1,
which can be influenced by fluid shifts in and out of the plasma. Even so, in
some cases the fluid changes that can occur are too small (~10%) to account
for these large changes (~50%) in plasma [K+] (Wasserman et al., 1997;
Marcos & Ribas, 1995).

Chapter 2 – Literature Review
18
At the cessation of exercise, the stimulated Na-K pump continues to return K+
into the intracellular space while removing excess Na+ from within the
contracting cell. The Na-K pump is highly effective at performing this as
demonstrated by Juel (1986) in mice and (Lindinger et al., 1995) in humans
where, within 2-3 minutes post exercise intracellular [K+] was only slightly
lower than control, and after 30 s supra-VO2peak exercise approximately 50
percent of lost K+ was returned bringing it to within 90 percent of pre-exercise
values, respectively. The rate of return influx could be modulated by
extracellular [K+] or K+ activated diffusion, intracellular Na+ or circulating
hormones, such as epinephrine (Marcos & Ribas, 1995; Juel et al., 1990).
Nonetheless, it appears K+ clearance post-exercise is more dependent on Na-
K pump activity rather than an increase in blood flow (Marcos & Ribas, 1995).
In evidence of this was a faster clearance of venous K+ in trained cyclists
compared with control subjects (Marcos & Ribas, 1995), since trained muscle
has been shown to have an up regulated number of Na-K pumps (Green et
al., 1999; Green et al., 1993).
Normal function and optimal force production of a muscle cell requires a
membrane electrical potential of approximately –90 mV (Guyton, 1991). As
explained above, the Na-K pump creates this electrical potential by actively
restoring and removing K+ and Na+ within and from the cell. If the Na-K
pump function is compromised, cell contractile function will be impaired
inevitably resulting in a decline in force production. Theoretically, assuming
all other ions remain constant, a decrease in intracellular [K+] from 146 to
117 mmol.l-1 and an increase in interstitial [K+] from 4.5 to 7.0 mmol.l-1
would result in a loss of membrane potential from –92 mV to –75 mV
(Lindinger et al., 1995). Not only does this demonstrate the contribution both
intracellular and interstitial K+ play, 70 and 30 percent respectively, in
maintaining the electrical potential, but also the magnitude of change that is
required to elicit such an effect on the membrane potential. Studies in mice
have demonstrated this relationship whereby a force reduction of 29 and 10
percent in soleus and extensor digitorum longus (EDL) muscle, respectively,
was associated with a measured intracellular K+ loss of 14 and 22 percent,
respectively (Juel, 1986).
There are two ways of determining Na-K pump activity, by measuring arterial-
venous K+ difference at exhaustion and by measuring increases in intracellular

Chapter 2 – Literature Review
19
[K+] during the first minutes of exercise (Lindinger et al., 1995). Later,
Fraser and McKenna (1998) modified the K+ stimulated method yielding
significant improvements in the reliability of measuring Na-K pump activity.
In vitro work has provided evidence that ouabain is a specific blocker of the
Na-K pump. By simply adding ouabain to a bath, in vitro, intracellular K+ loss
was reduced from 32 to 25 mmol.l-1 (Juel, 1986). Using these techniques to
examine the functional significance of the Na-K pump has demonstrated that,
at the onset of exercise, the Na-K pump is operating but not optimally
(Lindinger et al., 1995; Juel, 1986). Although it has been demonstrated that
only 2-6 percent of the Na-K pump capacity is required to maintain
intracellular [K+] even during intense exercise, a down regulation is possible
but probably unlikely. Even so, Juel et al. (1990) have provided evidence to
support this hypothesis, in that K+ efflux was reduced late in a 3-minute
intense exercise bout. They proposed two explanations for this finding: that
the reduced K+ efflux was mediated by the progressively lowering intracellular
pH, which (based on work by Blatz, 1980) alters the permeability of K+
channels; and/or that the increased Na-K pump efficiency late in exercise was
mediated by an increased plasma [K+], intracellular [Na+] or catecholamines.
Unfortunately, this increased pump efficiency late in exercise is insufficient to
restore intracellular [K+] during exercise to the level required to maintain the
optimal membrane potential.
During high intensity exercise, large quantities of La- are produced, massive
effluxes of K+ and small influxes of Na+, Cl- and water occur (Hebestreit et al.,
1996). The large efflux of K+ may be to control intracellular osmolality and
cell volume (Lauf, 1987) or be important in maintaining intracellular
concentrations of ATP (Castle & Haylett, 1987; Spruce et al., 1985). The
increase in extracellular:intracellular concentration of K+ may inhibit
excitation-contraction coupling and reduce the muscles’ ability to produce
tension (Heigenhauser et al., 1990). In addition, this will also reduce the
velocity of the propagation of the action potential to the transverse tubule
(Bigland-Ritchie et al., 1981). Together, these two effects will result in a
slower release of Ca2+ from the sarcoplasmic reticulum (Heigenhauser et al.,
1990).
Under alkalotic conditions, efflux of K+ is smaller while La- and non-volatile
acid (NVA) efflux is greater (Lindinger et al., 1990). The precise mechanism

Chapter 2 – Literature Review
20
for this reduced K+ loss is not known (Lindinger et al., 1990). A possible
mechanism may be due to an increase in the Na-K pump activity and/or a
decrease in sarcolemmal permeability to K+ per action potential (Juel et al.,
1990; Lindinger et al., 1990). The loss of K+ during muscular contraction is
very closely linked to the accumulation of intracellular La- (Lindinger et al.,
1990).
Potassium shifts may play a role as a limiting factor for muscle function (Juel
et al., 1990). As K+ is reaccumulating in the muscle, La- is continually
released from the muscle during the recovery period (Juel, 1997). The small
shrinkage of erythrocytes found during high intensity exercise is a function of
both the increased plasma [La-], [K+] and water movement into the active
muscles (Sjogaard et al., 1985). Haemoglobin (Hb) concentration is increased
during high intensity exercise and then returns to normal values during
recovery. This is closely related to the changes in [K+] and the change in
K+/Hb ratio is due entirely to volume changes (Juel et al., 1990). This
suggests that red blood cells (RBC) shrink during exercise and return to
normal size during recovery, thereby allowing the potassium content of the
RBC to remain unaltered during the exercise and recovery period. More
support for this is provided by the K+/Hb ratio remaining relatively constant
thus suggesting no net movement of K+ across the cell membrane.
During exercise, 70 percent of gross K+ efflux is immediately reaccumulated,
30 percent is lost to the blood, and one-third of the 30 percent lost to the
blood is accumulated in the other tissues. The presence of a K+ a-v difference
suggests K+ must have moved out of other tissue and into the blood. Since
approximately 10 percent of K+ accumulates in the interstitial space during
intense exercise, it should be considered a possible agent of fatigue (Juel et
al., 1990).
Both respiratory and metabolic acidoses increase muscle La- and K+ efflux,
and reduce the intracellular muscle water volume in the hind limb of the rat
(Lindinger et al., 1990). By increasing K+ efflux from exercising muscle, the
ionic environment created augments the effects on extracellular [H+] and the
ability of the muscle to maintain homeostasis (Heigenhauser et al., 1990).

Chapter 2 – Literature Review
21
Alkalosis at rest and during exercise It has been well documented that ingestion of an alkali at rest, such as
sodium citrate or sodium bicarbonate, decreases the blood [H+] as
represented by an increased blood pH and further alkalises the blood
(Linossier et al., 1997; Hausswirth et al., 1995; Lambert et al., 1993; Iwaoka
et al., 1989; Brien & McKenzie, 1989). The presence of a blood alkalosis prior
to exercise has been associated with improvements in human performance
(ergogenesis) across a variety of modalilities (Shave et al., 2001; Potteiger et
al., 1996a; McNaughton & Cedaro, 1991; Gao et al., 1988). The precise
mechanism/s of alkalosis on exercise performance, however, has not been
conclusively established. As such, there is evidence to suggest both positive
(McNaughton et al., 1999; McNaughton et al., 1991), neutral (Pierce et al.,
1992; Gaitanos et al., 1991) and negative (Goldfinch et al., 1988; Wilkes et
al., 1983) effects of pre-exercise induced alkalosis on performance. The
negative effects refer to side-effects of alkali ingestion that inhibit a subject to
perform the exercise task. Before detailing the specifics of these
investigations, it is important to briefly clarify the relationship between [H+]
and pH.
The Brønsted-Lowry theory describes an acid as any molecule or ion that can
act as a proton donor. Conversely, any molecule or ion that can act as a
proton acceptor is identified as a base. The expression pH can be defined as
the negative logarithm of the hydrogen ion concentration (Equation 1) and
was invented to provide a more convenient method of expressing
concentration better given in scientific notation.
[ ] [ ]++ =−=
HHpH 1loglog
Equation 1 Calculation of pH
For dilute solutions this value will usually fall between 1 and 14. It is
important to understand that the pH scale is logarithmic and not linear. For
example, a decrease in muscle pH as observed during intense exercise (Allsop
et al., 1990) from 7.1 to 6.5 equates to approximately a five-fold increase in
[H+]. Normal resting plasma, skeletal interstitial and intracellular pH are
approximately 7.4 (Cogan et al., 1990), 7.2 (Maclean et al., 2000) and 7.1

Chapter 2 – Literature Review
22
(Greenhaff et al., 1987), respectively. At rest all of the body’s fluid
compartments are therefore slightly alkalised.
Since early in the 20th century, it has been hypothesised that a state of
alkalosis would positively influence physical work capacity (Denning et al.,
1931). A number of studies to investigate the effects of alkalosis have
followed (Cox & Jenkins, 1994; Costill et al., 1984; Jones et al., 1977a; Jones
et al., 1977b). Approximately 50 percent show a positive improvement in
performance with alkali loading. The ergogenic effect of alkalosis appears to
be independent of mode of exercise as improvements have been
demonstrated in cycling (Potteiger et al., 1996a), running (Shave et al.,
2001), swimming (Gao et al., 1988) and rowing (McNaughton & Cedaro,
1991). From these studies the most common mode (~60%) investigated was
cycling.
Although there has been no formal investigation into the effect of trained-
status on alkalosis ergogenesis, there is room for limited speculation between
investigations. It would appear there is no effect of trained status as
supported by the observations of performance improvements in sprint trained
(Pierce et al., 1992; Goldfinch et al., 1988), endurance trained (Bird et al.,
1995), active healthy (Iwaoka et al., 1989) and sedentary (Hausswirth et al.,
1995) populations. These statements should be interpreted cautiously, as
there may be other factors mediating the ergogenic effect of alkalosis
independent of trained status.
It has been suggested that to observe an ergogenic effect of alkalosis, the
exercise intensity needs to be highly anaerobic in nature (Heigenhauser &
Jones, 1991). However, recent investigations by McNaughton et al. (1999)
and Potteiger et al. (1996a) have demonstrated improvements in aerobic
cycling exercise performance lasting up to one hour in duration. In contrast,
other investigations have found no such improvements over long durations
(Potteiger et al., 1996b; Kowalchuk et al., 1984). It has been adequately
demonstrated that below 120 seconds exercise duration there is no
improvement in performance with either sodium bicarbonate (McNaughton,
1992b) or sodium citrate (McNaughton & Cedaro, 1992). This has been
further supported by the work of Parry-Billings and MacLaren (1986)
demonstrating that alkalosis had no performance effect on 30 second Wingate

Chapter 2 – Literature Review
23
tests. Therefore, there is considerable evidence to suggest that duration of
exercise should not be less than 120 seconds, an upper limit, however, is still
under some conjecture.
There exists a positive dose-response relationship for both sodium citrate
(McNaughton, 1990) and sodium bicarbonate (McNaughton, 1992a). Both
these investigations identified a minimum dose (300 mg.kg-1) required to
observe an ergogenic effect of alkalosis on cycling performance. Work by
Horswill et al. (1988) further supported this finding by demonstrating no
effect of 100 or 200 mg.kg-1 sodium bicarbonate on exercise performance.
Increasing the dose of sodium citrate to 400 and 500 mg.kg-1 resulted in a
corresponding increase in performance (McNaughton, 1990). The same
cannot be said for sodium bicarbonate. Further dose increases to 400 and
500 mg.kg-1 led to increases in gastro-intestinal complications in the subjects,
thereby preventing the task being performed (McNaughton, 1992a).
As identified above, there has been much research identifying many factors
that are associated with the ergogenic potential of orally induced alkalosis.
However, investigations into the mechanisms underpinning this phenomenon
have been less prolific. Before discussing these studies in detail, it will be
beneficial to briefly introduce a theoretical concept introduced by Stewart
(1983) in the early 1980’s. The Stewart approach uses physicochemical
principles to describe the behaviour of H+ in physiological aqueous solutions.
These relate to three fundamental laws that govern [H+] in solutions such as
plasma and muscle: conservation of mass, maintenance of electrical
neutrality (Equation 2) and the equilibrium state of weak electrolytes and
water. Specifically, [H+] becomes a dependent variable determined by
independent variables: strong and weak electrolytes and pCO2.. Therefore,
the regulation of intracellular [H+] is a result of the exchange of strong ions
(Na+, K+, Cl-, SO42-, Mg2+, Ca2+, La-, PCr, NH4, ketones) between muscle and
extracellular fluid and intracellular pCO2 regulation (down its concentration
gradient). Strong ions exert their influence on [H+] through the difference
between the sum of strong cations and the sum of strong anions, termed the
strong ion difference (SID) (Equation 3).

Chapter 2 – Literature Review
24
[ ] [ ] [ ] [ ] [ ] [ ] 0233 =−−−−+ −−−−+ OHCOAHCOHSID
Equation 2 Calculation for electrical neutrality
[ ] [ ] [ ]∑ ∑−= anionsstrongcationsstrongSID
Equation 3 Calculation of strong ion difference (SID)
Two proposed sequential mechanisms through which alkalosis improves
muscle function are 1) an enhanced CO2-HCO3
- blood system to buffer H+
released from muscle during exercise and 2) an attenuated rate and decrease
in intracellular [H+] (Matson & Tran, 1993; Heigenhauser & Jones, 1991).
This theory does not discriminate between the different types of alkalis
ingested, such as sodium citrate, sodium bicarbonate or potassium
bicarbonate. Therefore, it can be deduced that the way in which alkalosis is
induced is not of primary concern, the end result of an increase in [HCO3-]
and [H+], however, is. Although this seems logical, recently, it was
demonstrated that sodium and potassium bicarbonate bring about alkalosis in
distinctly unique ways (Lindinger et al., 1999). An increase in [SID] was the
key determinant of alkalosis using both alkalis, however, the ions that
contributed to the increase in [SID] were different between the alkalis.
Specifically, an increase in plasma [Na+] and an increase in plasma [K+] both
combined with decreases in plasma [Cl-] to invoke plasma alkalosis.
Still, there seems to be some disagreement regarding the metabolism of
sodium citrate and the mechanisms involved that ensue alkalosis (Linossier et
al., 1997). It has been suggested that tri-sodium citrate dissociates into its
constituent ions, sodium and citrate, and is rapidly absorbed into the blood
(Kowalchuk et al., 1989). There are conflicting theories as to how citrate
manipulates plasma [HCO3-] and [H+]. Halperin (1982) suggested plasma
[HCO3-] is increased via the hepatic oxidation of citrate, while in contrast,
Kowalchuk et al. (1989) suggested that as the citrate anion is removed from
the plasma the SID is increased (via the remaining Na+) requiring a decrease
in [H+] and increase in [HCO3-] to maintain electrical neutrality. It is, of
course, possible that a combination of both of these theories contributes to
the increased [HCO3-] associated with alkalosis.

Chapter 2 – Literature Review
25
In summary, there is good evidence to suggest that ingestion of sodium
bicarbonate, potassium bicarbonate and sodium citrate increase both plasma
[HCO3-] and [H+] in humans. Further, there is considerable evidence to
support the contention that ingestion of 300 mg.kg-1 of an alkali can improve
human performance greater than 120 s and up to one hour in duration.
However, the exact physiological mechanisms mediating the ergogenic effect
of alkalosis, especially when ingesting sodium citrate, remain elusive. Further
research into these mechanisms is thus required.


Chapter 3 – Interstitial pH
27
CH A P T E R 3 ME A S U R E M E N T O F D I A L Y S A T E PH,
R E P R E S E N T A T I V E O F I N T E R S T I T I A L PH, A T R E S T
A N D D U R I N G D Y N A M I C L E G E X E R C I S E
Preface This chapter is centred round the paper authored by Darrin Street1, Jens
Bangsbo2 & Carsten Juel2, “Interstitial pH in human skeletal muscle during
and after dynamic graded exercise”, published in Journal of Physiology
(2001), 537.3, pp. 993-998. 1Department of Human Movement Studies, Queensland
University of Technology, 2August Krogh Institute, University of Copenhagen.
Statement of Joint Authorship This chapter is in part a result of a cooperative effort between myself and the
stated authors. The following outlines the relative contribution/s of each
author:
Darrin Street (Candidate) in vitro validation of method Part I (Duration:11 months) Experimental design Parts I, II and II Recruitment of subjects Parts II and III Equipment and subject preparation Parts II and III Data collection Parts I, II and III Data management Parts I, II and III Data analysis Parts I, II and III (90%) Data presentation Parts I, II and III (90%) Data interpretation Parts I, II and III (75%) Chapter preparation (75%)
Carsten Juel (Associate Professor) Experimental design Part III Supervised in vitro validation of method Assisted in experiment preparation Parts II and III Assisted in data collection Parts II and III Data analysis (10%) Data presentation (10%) Data interpretation (25%) Chapter preparation (20%)
Jens Bangsbo (Associate Professor) Subject preparation Part II and III Assisted in data collection Part III Chapter preparation (5%)

Chapter 3 – Interstitial pH
28
Introduction This chapter consists of three parts; Part I details the in vitro experiments
undertaken to test the validity and reliability of measuring pH using
microdialysis and a pH-sensitive dye, Part II details the in vivo experiment
performed to ascertain the effect of perfusate [HCO3-] on interstitial pH
measurement at rest and during exercise, Part III details the culmination of
these previous methodological studies in an in vivo experiment undertaken to
determine interstitial pH in humans at rest, during exercise and recovery
using microdialysis.
During muscle activity, accumulation of lactic acid and CO2 reduces cellular pH
and subsequently interstitial pH due to acid efflux from the muscle cells. It
has been proposed that the changes in interstitial pH during muscle activity
may be an important signal in the regulation of blood flow (Street et al.,
2001). In accordance with this idea, acidosis is probably mediated by
reduced extracellular pH and a subsequent lowering of the intracellular
calcium concentration (Aalkjaer & Peng, 1997). Furthermore, it has been
suggested that changes in pH may modulate vascular K+ channels (Davies,
1990) and thereby influence blood flow (Quayle et al., 1997), and that
acidosis may activate sensory nerve endings located in the muscle
interstitium (Victor et al., 1988). In order to evaluate such modulatory
effects, it is important to describe and quantify the exercise-induced
interstitial pH changes in human muscle.
The exercise-induced changes in muscle pH have, so far, mainly been
described from changes in venous blood pH (Bangsbo et al., 1993a; Juel et
al., 1990; Sjogaard et al., 1985), but the relationship between interstitial pH
and blood pH cannot be easily predicted because venous blood is mixed with
blood draining from active tissue (Radegran & Saltin, 1998). Furthermore,
studies using microdialysis in active muscle have demonstrated that during
muscle activity interstitial concentrations of lactate are higher than venous
lactate concentrations (Maclean et al., 1999), suggesting that the
equilibration across the capillary wall is restricted. It may therefore also be
expected that interstitial to venous pH gradients exist during exercise. In
addition, there is no protein present in the interstitium thereby reducing the
buffer capacity in comparison to blood (Aukland & Reed, 1993). For these

Chapter 3 – Interstitial pH
29
reasons, it can be hypothesised that the exercise-induced changes in
interstitial and venous blood pH are different and that the changes in venous
blood pH underestimate the local interstitial pH changes. Although electrodes
have previously been used in an attempt to measure pH directly (Allsop et al.,
1990), this was only performed at rest after exercise and showed an
artificially slow recovery from muscle pH after muscle activity. Thus, it has
not previously been possible to record interstitial pH during exercise in
humans.
Consequently, the objective of the present studies was to develop a method
to determine the changes in interstitial pH in human skeletal muscle during
and after exercise at different intensities. For that purpose, a microdialysis
technique was combined with the use of pH-sensitive fluorescent dye BCECF,
making it possible to perform continuous measurements of interstitial pH both
during and after muscle activity. Further, the first experiment was conducted
in an attempt to clarify some methodological considerations, specifically the
effect of a HCO3- perfusate on [H+] at rest and during exercise in humans.
PART I – IN VITRO VALIDATION OF MEASURING
INTERSTITIAL PH USING MICRODIALYSIS AND BCECF
In vitro microdialysis components and system Figure 3 shows a schematic of a microdialysis probe (CMA-60, CMA
Microdialysis AB, Sweden) that was used for all in vitro experiments.
The major difference between the probe set-up for measuring [H+] and other
metabolites was the removal of the polyurethane outlet tubing and its
replacement with 350 mm of 0.16 mm internal diameter (∅) stainless steel
tubing. The use of stainless steel on the outlet prevented the equilibration of
CO2 with the atmosphere and subsequent loss of CO2 from the dialysate,
which has the potential to influence dialysate [H+]. The total internal volume
of the modified CMA60 probe (H+ probe) was 35.7 µl, although only 3 µl was
exposed to the polyamide membrane where diffusion can occur. It is
important to note that the total volume from the microdialysis membrane to

Chapter 3 – Interstitial pH
30
the outlet was 15 µl and, at a perfusion rate of 5 µl.min-1, will result in a 3 min
delay.
The H+ probe was then placed within the following set-up for the
measurement of [H+] in vitro (Figure 4). The H+ probe itself was attached to
a 100 ml glass beaker using slick tape. The probe was orientated
perpendicularly within the centre of the beaker. In addition, a pH meter
(Radiometer ABL505, Copenhagen) probe was placed within the beaker for
reference monitoring of the solution. On the inlet side of the H+ probe, a 1 ml
syringe was attached and placed within a CMA 100 microdialysis pump set at
a flow rate of 5 µl.min-1.
Figure 3 Modified CMA60 microdialysis probe
A microdialysis probe (CMA60, Sweden) is modified for the measurement of [H+] in vitro by the removal of the polyurethane outlet tubing and replaced by 350 mm of stainless steel tubing to prevent CO2 loss.
The stainless steel outlet of the H+ probe was secured and sealed within a
micro flow-through cuvette (Sterna 73-1-FQ1, Great Britain) so that the end
of the tube would be as close as physically possible to the measuring window
Polyurethane Tubing (400 mm)
Stainless Steel Tubing (350 mm)
Polyamide Membrane
Polyurethane ShaftTubing

Chapter 3 – Interstitial pH
31
of the cuvette, thereby reducing lag time to analysis. The outlet of the
cuvette was placed into a waste beaker. The cuvette was placed in a
fluorescence spectrophotometer (Hitachi F2000, Japan), which completed the
continuous flow through system for the measurement of H+ in solution.
With the emission wavelength constant at 530 nm, the fluorescence
spectrophotometer continuously switched between the excitation wavelengths
of 440 and 500 nm with a bandpass of 10 nm. The excitation intensity at 440
nm was insensitive to pH, while the excitation intensity at 500 nm was
sensitive to pH. The two excitation intensities created an excitation intensity
ratio of 500/440. The intensity ratio was proportional to pH and insensitive to
any water movements from or into the probe. The temperature in the
fluorescence spectrophotometer was kept constant by circulating
thermostatically controlled water.
Figure 4 The complete fluorometric microdialysis system for the measurement of H+ in vitro
The modified microdialysis probe is immersed in a 100 ml beaker containing a solution of Na+ (154 mM), Cl- (154 mM) and HCO3
- (25 mM). The probe is perfused via micro-pump (CMA100, Sweden) set at 5 µl.min-1 and connected to fluorescent spectrophotometer. A laboratory pH meter (Radiometer ABL505, Copenhagen) is placed within the beaker solution for reference measurement.
Stainless Steel
CMA60 Microdialysis Probe
pH Meter
Fluorescence Spectrophotometer
7.35 Cl-
H+
Na+
HCO3-
Microdialysis Syringe Pump

Chapter 3 – Interstitial pH
32
Day to day stability of 2,7-bis-(2-carboxyethyl)-5-(and-6)-carboxyfluorescein (BCECF) dye Since many microdialysis investigations occur across several hours, it was
important to assess the stability of the dye across long durations. On two
occasions separated by 24 hrs, [H+] was measured in a beaker solution (Na+
154 mmol.l-1, Cl- 154 mmol.l-1, HEPES 5 mmol.l-1, NaHCO3- 20 mmol.l-1) by
perfusing a H+ probe with sterile saline and 0.1 mg.ml.l-1 of the pH sensitive
dye, BCECF. The pH of the beaker solution was manipulated from 6.8 to 7.2
and back to the initial setting by the addition of small amounts of 5 M HCl or 6
N KOH. Since the molecular cut-off of the polyamide membrane is 20000
daltons (da), the BCECF was coupled to dextran (molecular mass 70000 da),
thereby preventing any loss of the dye from the perfusate. The perfusate was
placed into a 1 ml syringe, mounted in a microdialysis pump and connected to
the inlet of the H+ probe. Figure 5 shows the results of this in vitro
experiment. Two trials of each experiment were performed each day for a
duration of 10 min with pH initiating at ~6.82, increasing it to ~7.23 after 3
min and decreasing it back to ~6.78 for the remainder of sampling.
Fluorescence was recorded at a frequency of 10 Hz for the full duration of the
test.
There was no difference between the H+ fluorescent signals obtained when
measuring pH on the 2 separate days. Closer inspection of the data revealed
minor fluorescent differences between the days but this was due to different
pH values (~0.04) at the time of sampling, which further demonstrated the
sensitivity of the system. The upward drift in signal on both days was
explained by the open nature of the system and the continual loss of CO2 to
the environment. These results would thus indicate that BCECF is stable in
detecting pH changes across a 24-hour period. Therefore, it was concluded
that H+ measurement using BCECF is not influenced by experiments of long
durations up to 24 hours.

Chapter 3 – Interstitial pH
33
Time (min)
Fluo
resc
ent R
atio
0.0
3.0
3.5
4.0
4.5
5.0
5.5
6.0
Figure 5 Day to day variability of 2,7-bis-(2- carboxyethyl)-5-(and-6)-carboxyfluorescein The small drift upwards is explained by the open nature of the system and the continual loss of CO2 to the environment.
Effect of albumin and stir rate on fluorescence using BCECF dye In an attempt to simulate the in vivo effects of proteins surrounding the
polyamide membrane and muscle cells contracting in close proximity to the
membrane, the probe was subjected to a series of high magnetic stirring rates
with the solution saturated with albumin. The high stirring rates resulted in a
large amount of turbulence created within the beaker and, as a result, the
membrane moved vigorously. [H+] was measured under three conditions;
magnetic stirring at 100 rpm and no albumin (100 control), magnetic stirring
at 500 rpm and albumin (500 albumin) and, pulsing the spin rate between
100 and 500 rpm in 30 s intervals and albumin (100/500 albumin). Each
condition was performed for a duration of 10 min with pH initiating at ~6.82,
3 min later increasing to ~7.23 and decreasing it back to ~6.78 for the
remainder of measurement. Fluorescence was recorded at a frequency of 10
Hz for the full duration of the test.
Figure 6 displays the fluorescent data collected during this experiment. Both
stir rate and albumin failed to affect the H+ fluorescent data. The differences
observed were again due to the nature of the in vitro system and subsequent
Day 1
Day 2

Chapter 3 – Interstitial pH
34
CO2 loss resulting in an upward drift in pH that was coincident with a
corresponding drift in
Time (min)
Fluo
resc
ent R
atio
0.0
3.0
3.5
4.0
4.5
5.0
5.5
6.0
12 13
Figure 6 Effect of magnetic stir rate and albumin on [H+] measured with BCECF in vitro
fluorescence, and small pH manipulations between experiments. Therefore, it
was concluded that an abundance of protein and dynamic movement of the
membrane was unlikely to interfere with the measurement of H+ using 2,7-
bis-(2- carboxyethyl)-5-(and-6)-carboxyfluorescein in vivo.
Influence of 1 cm polyurethane outlet tubing exposed to air During in vivo H+ measurement using microdialysis, approximately 1 cm of
the probe outlet would emerge from the skin of the thigh and thus be exposed
to the air. Stainless steel tubing was attached to the 1 cm of outlet to
transport the dialysate to the fluorometric spectrophotometer without the loss
of CO2. The internal volume of the outlet was ~0.35 µl, which allowed ~4
seconds for the diffusion of CO2 from the dialysate (assuming a flow rate of 5
µl.min-1). Given the steep CO2 gradient from dialysate to air, the aim of this
experiment was to establish whether there was a significant loss of CO2 from
the exposed polyurethane tubing. Two probes were used, one with a 1 cm
piece of tubing and the other with no tubing emerging from the solution in the
beaker. Then, across a wide pH range (6.8-8.0) four duplicate measurements
were made using both types of tubing. The fluorometric ratios were plotted
100 Control
500 Albumin
100/500 Albumin

Chapter 3 – Interstitial pH
35
against the corresponding pH values at the time of measurement with
subsequent linear regression analysis. As shown in Figure 7, 1 cm of exposed
polyurethane tubing had no effect on the [H+] regression curves suggesting
that CO2 loss under these conditions is not a concern.
Fluorescence Ratio
0.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0
Beak
er p
H
0.0
6.0
6.5
7.0
7.5
8.0
8.5
9.0
1 cm y = 5.232+0.5048x0 cm y = 5.384+0.4624x
Figure 7 Influence of 1 cm polyurethane tubing exposed to air on [H+] determination in vitro
Effect of HCl, La- and CO2 titrations on pH calibration curves All acid-base manipulations in vitro were performed via the addition of HCl,
however this acid is not physiological within skeletal muscle. Alterations in
acid-base status during muscular contraction are largely influenced by
metabolically produced La- and CO2, therefore the microdialysis probe was
tested to examine if it performed similarly titrating with both La- and CO2 to
manipulate pH in vitro. The same probe was used for each titration, then
across a wide range of physiological pH values the [H+] was manipulated with
each of the chosen acids. The fluorometric ratios were plotted against the
corresponding pH values at the time of measurement with subsequent linear
regression analysis. Figure 8 shows the titration curves for HCl-La- and HCl-
CO2 comparisons. No difference was found between any of the regression
curves for all titrations. These findings suggest two things; that in vitro
titrations with HCl were applicable to the in vivo model and, since the probe

Chapter 3 – Interstitial pH
36
performed similarly with all titrations, its performance in vivo should be
adequate.
Fluorometer Ratio
0 2 3 4 5 6 7 8
Beak
er p
H
0.0
6.0
6.5
7.0
7.5
8.0
8.5
HCl y = 5.371+0.3588xCO2 y = 5.525+0.3291x
Fluorometer Ratio
0 2 3 4 5 6 7
Beak
er p
H
0.0
6.0
6.5
7.0
7.5
8.0
8.5
HCl y = 5.426+0.4244xLa- y = 5.421+0.4326x
Figure 8 Titration curves for HCl-CO2 and HCl-La-
Effect of dye concentration on pH calibration Previously, the effect varied dye concentration would have on pH calibration
was unknown. To examine this question, three concentrations of dye were

Chapter 3 – Interstitial pH
37
assessed, low (0.1 mg.ml-1), medium (0.2 mg.ml-1) and high (0.4 mg.ml-1).
Across a wide pH range (6.8-8.0), four duplicate measurements were made
using each dye concentration. The fluorometric ratios were plotted against
the corresponding pH values at the time of measurement with subsequent
linear regression analysis (Figure 9). Interestingly, there was not a
systematic increase or decrease in the calibration curves generated during
this experiment. Although the y-intercepts were similar between
concentrations, the positive slopes were not 0.37, 0.46 and 0.41 for low,
middle and high, respectively. When using the above functions to calculate
pH, the results obtained varied greatly, 6.01 for low to 7.60 for high. This has
obvious implications for the amount of dye used and for establishing which is
the correct or most accurate concentration for in vivo pH determination.
Currently, there is no explanation for these results and further investigation is
required to elucidate possible reasons.
Fluorometer Ratio
0 2 3 4 5 6 7 8
Beak
er p
H
0.0
6.0
6.5
7.0
7.5
8.0
8.5
LowMiddleHigh
Figure 9 Effect of BCECF dye concentration on pH calibration curves
Effect of HCO3- perfusate on pH calibration
Blood consists of approximately 25 mmol.l-1 HCO3-, and evidence suggests
that a similar concentration may exist within the interstitium (Geers & Gros,
2000). Any concentration of HCO3- within the perfusate would alter the
equilibration between the interstitial space and probe membrane. To test the

Chapter 3 – Interstitial pH
38
effect of perfusate [HCO3-] on the recovery of H+ in vitro, two HCO3
-
concentrations were used, 0 and 25 mmol.l-1. These two concentrations were
chosen for the following reasons, 0 mmol.l-1 had been used in a recent paper
by Maclean et al. (2000) and 25 mmol.l-1 being similar to the interstitial
concentration would reduce the fractional uptake or loss of HCO3- from the
microdialysis probe, which would in turn reduce concurrent HCO3- effects on
[H+] within the probe. Several measurements were made using each
perfusate [HCO3-] across a wide range of beaker pH values (6.5–7.5). Figure
10 shows the resultant calibration curves for each perfusate and the beaker
pH for reference. The data clearly shows that perfusing a probe without
HCO3- alkalises the pH calibration curve, while 25 mmol.l-1 HCO3
- acidified the
calibration curve. However, further in vivo testing is required to ascertain
what effects this may have at rest and during exercise.
Beaker pH
0.0 6.6 6.8 7.0 7.2 7.4 7.6
Fluo
rom
eter
Rat
io
0
2
3
4
5
6
7
8
Beaker pHNo HCO3-
25mM HCO3-
Figure 10 Effect of perfusate [HCO3-] on pH
calibration curves in vitro

Chapter 3 – Interstitial pH
39
PART II – EFFECT OF PERFUSATE [HCO3-] ON INTERSTITIAL
PH IN VIVO
Methods
Subjects Two human subjects were continuously monitored at rest, during 5 min of
one-legged knee extensor exercise at 10 W, and during recovery. The
subjects were aged 24 and 32 years. They were 163 and 178 cm in height
and had a mass of 58 and 85 kg, respectively. Both subjects were active
individuals with no health-related problems. Prior to the start of the
experiment, the subject were informed of any risks and discomforts related to
the experiment. Both subjects signed a written consent form prior to the
experiments. The study was approved by the local ethics committee (August
Krogh Institute, University of Copenhagen) and conformed to the Declaration
of Helsinki.
Exercise protocol Subjects performed one-legged knee-extensor exercise in a supine position
and were secured via a series of straps, two shoulder, one waist and one
thigh strap, so exercise was restricted to the quadriceps muscle (Bangsbo et
al., 1990). During exercise, the subjects had visual feedback in the form of a
digital display showing the cadence and power output. Subjects were
required to maintain a cadence of 60 rpm for the exercise duration. The 10 W
exercise period was preceded and succeeded by 5 min and 10 min of rest,
respectively. This test was performed on three occasions, corresponding to 3
perfusates without HCO3- (wHCO), 25 mmol.l-1 HCO3
- (25HCO) and 50 mmol.l-
1 HCO3- (50HCO), each separated by 7 days.
Probe insertion and perfusate Before the experiment, the subjects rested in a supine position with the legs
well supported. For each microdialysis probe to be inserted, the subject was
given approximately 1 ml of 20 g.l-1 xylocaine via a 25-gauge needle at the
insertion site. An 18-gauge cannula was first passed through the skin and
fascia to make way for the probe. A second cannula containing the

Chapter 3 – Interstitial pH
40
microdialysis probe (CMA-60, CMA Microdialysis AB, Sweden) was then
pushed through the skin and fascia and orientated along the length of the
fibres of the vastus lateralis muscle. The cannula was removed leaving the
microdialysis probe within the muscle. After insertion of the probe, it was
secured with tape and the outlet cut at a maximal length of 10 mm from the
skin. The subjects recovered for 1.5 h after probe insertion before any
measurements were performed. The pH-sensitive fluorescent dye BCECF was
coupled to dextran (molecular mass cut off at 70000 Da), which prevented
any diffusion of dye across the probe membrane (cut off at a molecular mass
of 20000 Da). The dye (0.1 mg ml.l-1) was dissolved in a sterile saline
solution (154 mM Na+). The perfusate was then placed into a sterile 1 ml
syringe equipped with a filter, mounted in a microdialysis pump and
connected to the inlet of the microdialysis probe. The outlet from the probe
was removed, replaced with a steel tube and connected to a micro flow-
through cuvette (total volume 8 µl) in a (Hitachi F-2000, Japan) fluorescence
spectrophotometer. The pump rate was 5 µl.min-1 in all experiments. The
time scales on the figures have been corrected for the delay due to the
volume of tubing and cuvette.
Fluorometric measurements and determination of pH With the emission wavelength constant at 530 nm, the fluorescence
spectrophotometer continuously switched between the excitation wavelengths
of 440 and 500 nm with a bandpass of 10 nm. The excitation intensity at 440
nm was insensitive to pH, but dependent on the amount of dye, whereas the
excitation intensity at 500 nm was also sensitive to pH. Thus, the excitation
intensity ratio 500/440 was proportional to pH and independent of changes in
dye concentration and consequently was insensitive to any water movements
from or into the probe. The temperature in the fluorescence
spectrophotometer was kept constant by circulating thermostatically
controlled water. For calibration, a microdialysis probe was placed in a beaker
with magnetic stirring and connected to a pump and the fluorometer. The
beaker contained saline and bicarbonate, and the pH was monitored with a
laboratory pH meter. The pH in the beaker was changed in a stepwise
manner by adding HCl/NaOH and the excitation ratio was recorded. This was
performed with a separate probe before the experiment (as a backup) and
then after the experiment with the probe used in vivo (if it was still intact). A

Chapter 3 – Interstitial pH
41
calibration curve was obtained by plotting the excitation intensity ratio versus
external pH. The constants obtained from a linear regression to the
calibration curve were used to convert fluorescent signals obtained in human
experiments to interstitial pH.
Results The mean pH at rest was 7.42, 7.07 and 6.77 for wHCO, 25HCO, and 50HCO,
respectively. Exercise resulted in an alkalosis of 0.24 pH units without HCO3-,
while 25HCO and 50HCO showed slight acidoses of 0.01 and 0.02 pH units,
respectively. Five minutes of 10 W leg flexion and extension resulted in an
average exercise interstitial pH of 7.66, 7.06 and 6.75 for wHCO, 25HCO and
50HCO, respectively. After 5 minutes recovery, interstitial pH had returned to
7.50, 7.05 and 6.72 for wHCO, 25HCO and 50HCO, respectively. Only 25HCO
and 50HCO had made a full recovery to pre-exercise pH values. Figure 11
shows this data, which have been time adjusted to show real time at the
muscle interstitium.
Time (min)
0 5 10 15 20 25
pH
0.00
6.50
6.75
7.00
7.25
7.50
7.75
8.00without HCO3-
25 mM HCO3-
50 mM HCO3-
Figure 11 Influence of [HCO3-] on the estimation of interstitial pH
during 10 W dynamic leg exercise
Three interstitial pH curves generated from different concentrations of HCO3-
, no HCO3- (blue), 25 mM HCO3
- (red), 50 mM HCO3- (green), before, during
and after 10 W knee-extensor exercise. Exercise started 5 min after the initial recording, marked with a black line.

Chapter 3 – Interstitial pH
42
Discussion The main finding from this experiment was that [HCO3
-] within perfusate
profoundly influences the estimated interstitial pH during dynamic leg exercise
using BCECF dye and microdialysis. Specifically, the absence of HCO3- in the
perfusate significantly alkalises the pH value at rest (7.42), during exercise
(7.66), and in recovery (7.50). In contrast, doubling the estimated interstitial
[HCO3-] to 50 mmol.l-1 resulted in an acidosis of the rest (6.77), exercise
(6.75) and recovery (6.72) pH values, respectively. These results suggest
that the total absence or presence of too much perfusate HCO3- leads to an
over or underestimation of interstitial pH, respectively. Further, the temporal
response during exercise under the wHCO condition (Figure 11) shows a
significant increase in pH or alkalosis. This has been demonstrated previously
by Maclean et al. (2000), who also used a perfusate lacking HCO3-. The 10 W
exercise intensity was specifically chosen because of its small effects on
muscle and blood pH. As such, it was expected that 10 W exercise intensity
would have very little effect on interstitial pH. This prior knowledge suggests
that the method involving no HCO3- in the perfusate causes erroneous
interstitial pH results. It is possible that the large gradient of bicarbonate
between interstitium and the probe led to bicarbonate diffusing across the
probe membrane. For most compounds, the equilibration across the probe
membrane is only partial (fractional uptake) and the rate of equilibration is
increased by movement (Juel et al., 2000; Maclean et al., 1999). Therefore,
the apparent alkalisation during exercise could be due to an increased
fractional uptake of bicarbonate induced by movement. It follows then that
since there is approximately 25 mM bicarbonate is present in blood (Bangsbo
et al., 1997) and presumably also in the interstitium (Geers & Gros, 2000) the
addition of 25 mM bicarbonate to the perfusate best reduces the bicarbonate
concentration gradient between probe and interstitial space. It thus appears
that adding bicarbonate to the perfusate is crucial and that there is no
evidence to support an interstitial alkalisation during muscle contraction.

Chapter 3 – Interstitial pH
43
PART III – INTERSTITIAL PH AT REST AND DURING
DYNAMIC LEG EXERCISE
Methods
Subjects Six male subjects with a mean age of 31 years (range 24–52 years)
participated in the study. Mean height and weight were 181 cm (175–190
cm) and 82 kg (68–97 kg), respectively. All subjects were active individuals
with no health-related problems. Prior to the start of the experiment, each
subject was informed of any risks and discomforts related to the experiment.
All subjects signed a written consent form prior to experiments. The study
was approved by the local ethics committee (August Krogh Institute,
University of Copenhagen) and conformed to the Declaration of Helsinki.
Exercise protocol The only modification to the exercise protocol that was performed in
experiment I was the addition of a third exercise intensity of 70 W.
Probe insertion and perfusate The method used for placing microdialysis probes in each subject has been
described in detail in the section on experiment I and was not altered for this
experiment. However, in accordance with the findings of experiment I, 25
mmol.l-1 HCO3- was added to the perfusate without pH adjustment.
Fluorometric measurements and determination of pH To ascertain interstitial pH values the same method was used as described
above in experiment I.

Chapter 3 – Interstitial pH
44
Results
Interstitial pH at rest and during muscle activity With the addition of 25 mmol.l-1 HCO3
- to the perfusate, mean calculated
interstitial pH at rest was 7.38±0.02. Exercise induced a reduction in muscle
interstitial pH in all six subjects and at all intensities (Figure 12).
Interstitial pH was gradually reduced during the 5 min of exercise. The
decrease in interstitial pH during exercise was nearly linearly related to the
power output. The mean value of the lowest interstitial pH at 30, 50 and 70
W exercise was 7.27 (range 7.18–7.34), 7.16 (7.05–7.24) and 7.04 (6.93–
7.12), respectively. The mean peak acidification during exercise at a power
output of 30, 50 and 70 W was 0.11 (0.06–0.20), 0.22 (0.13–0.34) and 0.34
(0.22–0.41) pH units, respectively. For each subject there was a correlation
between power output and peak acidificat-ion (Figure 13). The large inter-
individual variation in peak acidification was probably due to the large
variation in relative workload.
Recovery from exercise The peak acidification was obtained 1.0 min (0.5–2.0 min) after the cessation
of exercise. Recovery from peak acidification proceeded in an exponential
fashion (Figure 12). The mean half time for recovery of interstitial pH after
70 W exercise was 5.2 (4.1–6.1) min. For most subjects, the pH curve in
recovery after 70 W intersected the curve obtained after 50 W, indicating that
the rate of pH recovery was higher after 70 W than after 50 W exercise.

Chapter 3 – Interstitial pH
45
0 5 10 15 20 25 30
Inte
rstit
ial p
H
6.9
7.0
7.1
7.2
7.3
7.4
7.5
0 5 10 15 20 25 306.9
7.0
7.1
7.2
7.3
7.4
7.5
Time (min)
0 5 10 15 20 25 306.9
7.0
7.1
7.2
7.3
7.4
7.5
0 5 10 15 20 25 30
Inte
rstit
ial p
H
6.9
7.0
7.1
7.2
7.3
7.4
7.5
0 5 10 15 20 25 306.9
7.0
7.1
7.2
7.3
7.4
7.5
Time (min)
0 5 10 15 20 25 30
Inte
rstit
ial p
H
6.9
7.0
7.1
7.2
7.3
7.4
7.5
Figure 12 Interstitial acidification during exercise
Individual recordings of interstitial pH during 5 min knee-extensor exercise are shown. The power output was 30 W (green), 50 W (blue) and 70 W (red). Exercise was started 5 min after the onset of the recording (marked with a horizontal bar). One subject, marked *, became exhausted after 2 min of 70 W exercise. Numbers at the top-centre of each graph depict subject age.
*
52 24
26 26
27 29

Chapter 3 – Interstitial pH
46
Power output (Watts)0 10 20 30 40 50 60 70
Inte
rstit
ial p
H
0.0
6.9
7.0
7.1
7.2
7.3
7.4
Figure 13 Peak interstitial pH during exercise at different power outputs
For each subject the line connects pH at rest and pH at peak interstitial acidification obtained at a power output of 30, 50 and 70 W. One subject, marked *, became exhausted after 2 min of 70 W exercise.
Discussion This is the first study to continuously measure interstitial pH during and after
muscle activity in humans. At each intensity, interstitial pH gradually reduced
during the entire exercise period. Peak acidification was obtained
approximately 1 min after cessation of exercise, after which interstitial pH
recovered in an exponential manner. It was also demonstrated that
interstitial pH is reduced proportional to power output during muscle exercise.
Changes in muscle interstitial pH during and after exercise The rate of interstitial acidification at the onset of exercise can be evaluated
from the slope of the curves in Figure 12. In most subjects, the slope of
acidification was greater the higher the power output. This finding probably
demonstrates that the rate of acid accumulation in the muscle cells is related
to the power output and that the acid transport across the sarcolemma
membrane is dependent on the concentration gradient from muscle to
interstitium.
*

Chapter 3 – Interstitial pH
47
The present study showed that muscle activity induced an interstitial
acidification. In contrast, two studies also using the microdialysis technique
but with the probe attached to a flow-through pH microelectrode have
reported an alkalisation during muscle activity and a fast (1 min) recovery
(Maclean et al., 2000; Maclean et al., 1998). In these studies, no bicarbonate
was added to the perfusate. When bicarbonate was not added to the
perfusate, it was observed, as in previous studies (Maclean et al., 2000;
Maclean et al., 1998), that exercise induced an apparent fast alkalisation,
succeeded by a plateau and a fast recovery (see experiment I). It is likely
that the large gradient of bicarbonate between interstitium and the probe had
caused the bicarbonate to diffuse across the probe membrane. For most
compounds, the equilibration across the probe membrane is only partial
(fractional uptake) and the rate of equilibration is increased by movement
(Juel et al., 2000; Maclean et al., 1999). Therefore, the apparent alkalisation
during exercise in previous experiments could be due to an increased
fractional uptake of bicarbonate induced by movement. Approximately 25 mM
bicarbonate is present in blood (Bangsbo et al., 1997) and presumably also in
the interstitium (Geers & Gros, 2000). In the present study, 25 mM
bicarbonate was thus added to the perfusate, which resulted in a low
bicarbonate concentration gradient between probe and interstitial space. With
bicarbonate in the probe, exercise induced an interstitial acidification,
succeeded by a recovery phase with a time course similar to recovery in the
intracellular space and in blood (see Figure 12). It therefore appears that
adding bicarbonate to the perfusate is crucial and that there is no evidence to
support an interstitial alkalisation during muscle activity.
Extracellular (interstitial) muscle pH has also been measured with a needle-
protected glass pH electrode before and after exercise (Allsop et al., 1990).
With this method, pH after exercise was found to be 6.6. An apparently fast
initial recovery after activity was succeeded by a slow, nearly linear recovery,
which was only partial even after 30 min (Allsop et al., 1990). The low pH
and the slow and only partial recovery could indicate that the measurements
were influenced by fibre damage and/or the existence of a large artificial
space in the muscle created by the needle. In contrast, the present study
showed a complete recovery of interstitial pH 20 min after exercise.

Chapter 3 – Interstitial pH
48
Recovery of interstitial pH The lowest interstitial pH was obtained approximately 1 min after exercise. A
similar time course has been found for cellular pH determined by phosphorus
magnetic resonance spectroscopy (NMR) (Bangsbo et al., 1993b; Arnold et
al., 1985). A possible reason for the further acidification after cessation of
exercise is that a large fraction of phosphocreatine resynthesis, which
releases H+, occurs within the first minute after exercise (Bangsbo et al.,
1993b; Arnold et al., 1985).
The recovery of interstitial pH took place with a mean half-time of 5.2 min
calculated from the end of exercise (see Figure 12). This value is similar to
the recovery of muscle pH (intracellular pH) measured in needle biopsies
obtained at different time intervals after exercise (Juel, 1998a; Juel et al.,
1990). These studies have reported half-time values of 4.9 min for muscle
pH, approximately 4 min for H+, and 5 min for lactate (Juel, 1998a; Juel et
al., 1990). Consequently, the time course of changes in interstitial pH after
exercise closely corresponds with the changes in intracellular pH reported in
the literature. The recovery of interstitial pH after intense exercise (70 W)
was faster than after more moderate exercise (50 W) (see Figure 12). In
fact, some of the recovery curves for 70 W crossed the curves for 50 W
approximately 5 min after exercise. This observation could suggest that pH
recovery is blood flow dependent, as blood flow after intense exercise is
higher than after moderate exercise (Radegran & Saltin, 1998).
Comparison between pH changes in muscle interstitium and blood The interstitial pH at rest (7.38±0.02) fell within the range (7.37–7.43) of
femoral venous pH values reported in the literature (Bangsbo et al., 2000;
Bangsbo et al., 1993a; Juel et al., 1990; Sjogaard et al., 1985). In Figure 14,
the exercise-induced interstitial pH values at peak acidification are compared
to femoral venous pH values. The figure includes unpublished values from the
same laboratory as well as femoral venous blood pH values obtained in
comparable knee-extensor exercise studies (Bangsbo et al., 2000; Bangsbo et
al., 1993a; Sjogaard et al., 1985). This figure depicts two distinct interstitial
acidification relationships with venous blood. Low intensity exercise (10–30
W) induced an interstitial acidification similar to venous blood, whereas high

Chapter 3 – Interstitial pH
49
intensity exercise (>50 W) resulted in a larger interstitial acidification than in
venous blood. There may be several reasons for this difference. During one-
legged knee-extensor exercise, the femoral vein does not drain only the
active part of the quadriceps muscle, since a fraction of venous blood comes
from inactive tissues and inactive parts of the quadriceps muscle. At an
exercise intensity of 50 W, blood flow may be 5.3 l.min-1 (Juel et al., 1990)
(Bangsbo et al., 1990) of which 1.2 l.min-1 may be perfusing inactive muscle
(Radegran & Saltin, 1998). This results in a decrease in femoral venous blood
pH that is less than the interstitium pH decrease of the active muscle.
Another reason for the larger acidification of the interstitial space during
muscle activity is probably its lower buffer capacity compared to blood. The
lack of protein concentration within the interstitial space makes the
interstitium more exposed to pH fluctuations (Geers & Gros, 2000). A third
possibility is that the higher blood flow rate during high intensity exercise
reduces the mean transit time for the blood passing the capillaries in the
active muscle during exercise (Radegran & Saltin, 1998; Bangsbo et al.,
1990; Juel et al., 1990), which may result in only partial equilibration of H+
between interstitium and blood. The present study does not allow for
discrimination between the possibility that a pH gradient exists across the
capillary wall during exercise and that the pH difference between interstitium
and femoral venous blood is exclusively due to mixing with blood from
inactive tissues.
Comparison between cellular and interstitial pH changes One method to access intracellular pH has been to measure pH in
homogenised needle-biopsy material. This method is based on the fact that
the intracellular space makes up the main fraction of the muscle and that the
homogenate pH therefore mainly represents the intracellular pH (Sjogaard et
al., 1985). The homogenisation method reveals resting intracellular pH
values in the range of 7.04–7.17 (Bangsbo et al., 1996; Bangsbo et al.,
1993a; Juel et al., 1990; Sjogaard et al., 1985). Thus, resting muscle pH is
at least 0.2 pH units lower than interstitial pH (7.38). In Figure 14, the
intracellular pH values during exercise reported in the literature are plotted
together with the interstitial pH values obtained in the present study.

Chapter 3 – Interstitial pH
50
It can be seen that cellular pH is 0.2–0.3 pH units lower than interstitial pH
both at rest and immediately after intense exercise. However, if the data in
the figure are converted to [H+], it is evident that the H+ gradient across the
muscle membrane is larger (approximately 100 nM) after intense exercise
than at rest (30 nM). This is probably due to the large intracellular
accumulation of lactic acid during muscle activity (Juel et al., 1990).
Power output (Watts)
0 10 20 30 40 50 60 70
pH
0.0
6.7
6.8
6.9
7.0
7.1
7.2
7.3
7.4
Figure 14 Intracellular, interstitial and venous pH during knee-extensor exercise
, mean (± SEM) peak interstitial pH obtained in the present study. Data connected by a straight line. , femoral venous pH during knee-extensor exercise (authors’ unpublished data); each value represents mean from six subjects. 1, femoral venous pH during exhaustive knee-extensor exercise in three studies (Sjogaard et al., 1985) (Bangsbo et al., 1996) (Bangsbo et al., 2000). The dashed line represents a regression line for the venous data. , intracellular pH obtained with the homogenisation technique (Sjogaard et al., 1985) (Juel et al., 1990) (Bangsbo et al., 1993a) (Bangsbo et al., 1996). Data from the literature represent means of five to six subjects.
Physiological implications of changes in interstitial pH Since the relationship between exercise intensity and interstitial pH displayed
similarities with exercise-related changes in blood flow (Bangsbo et al., 1990;
Juel et al., 1990), it is reasonable to speculate that blood flow during muscle
activity is regulated by changes in interstitial pH. Supporting this hypothesis
is the finding that interstitial pH has a local modulatory effect on smooth
muscle cells inducing vasodilatation, which is probably mediated by a

Chapter 3 – Interstitial pH
51
reduction in intracellular calcium (Aalkjaer & Peng, 1997) or changes in the
activity of potassium channels (Quayle et al., 1997; Davies, 1990).
Alternatively, blood flow during knee-extensor exercise increases rapidly and
has reached a steady level after about 1.5 min (Radegran & Saltin, 1998),
whereas interstitial pH progressively decreases during exercise. In addition,
the time courses for recovery of blood flow and interstitial pH after exercise
are different (Bangsbo et al., 1990; Juel et al., 1990). Consequently, it would
seem that other factors are also involved in the regulation of blood flow
during and after exercise. The exercise induced decrease in interstitial pH
may also have other effects. The lower interstitial pH could modulate the
sensory response from the muscle, since interstitial pH has been linked to
sympathetic nerve discharge (Victor et al., 1988). In addition, interstitial pH
is probably also important in modulating transport systems and ion channels
in muscle sarcolemma as well as in vascular cells.
Conclusion The present study demonstrated that interstitial pH is continuously decreasing
during muscle activity. The exercise-induced reduction in interstitial pH was
correlated with power output and was larger at high exercise intensities than
the pH reduction of femoral venous blood.


Chapter 4 – Ingestion Regime
53
CH A P T E R 4 EF F E C T O F A L K A L I I N G E S T I O N
R A T E O N P L A S M A A C I D-B A S E , [H + ] , A N D I O N I C ,
[K + ] , S T A T U S
Introduction Increasing one or all of the buffer systems’ capacities, either intracellularly or
in the blood, has the potential to further delay the onset of a critical pH level,
thereby increasing the time for muscle to maintain force production. The
ingestion of sodium bicarbonate or sodium citrate can increase the capacity of
the blood bicarbonate system (Kowalchuk et al., 1989; Costill et al., 1984).
Associated with this increase in blood [HCO3-] is a decrease in [H+] or
increase in pH (Ball & Maughan, 1997), and is commonly referred to as a
state of alkalosis. Manipulating blood [H+] and [HCO3-] via inducing alkalosis
can improve muscle function and performance. Numerous investigations of
ingesting sodium bicarbonate or sodium citrate prior to exercise have led to
increases in swimming (Gao et al., 1988), running (Shave et al., 2001),
cycling (Potteiger et al., 1996a) and rowing (McNaughton & Cedaro, 1991)
performances. However, there is evidence to demonstrate the contrary
across each of these modes of exercise, respectively (Schabort et al., 2000;
Robinson, 1997; Ibanez et al., 1995; Pierce et al., 1992).
As is often the case with ingested substances, there exists a dose-response
relationship. That is, there is a minimum quantity of the substance that must
be consumed to manipulate the system to a high enough degree to enable the
observation of a significant effect. Although this work has been performed
(McNaughton, 1992a; McNaughton, 1990; Horswill et al., 1988) and a
minimum dose identified, 300 mg.kg-1 for both sodium bicarbonate and
sodium citrate, it was tested across one ingestion regime only, namely bolus.
The bolus regime usually involves subjects consuming the ingestant in less
than 3 min. This rapid infusion of alkali very quickly increases gastric pH from
2.5-6.11 (Hauptfleisch & Payne, 1996), thereby dramatically altering the GI
milieu. Such alterations challenge the body’s regulatory and absorptive
mechanisms. Unfortunately, sometimes the stress is too much for the system
and results in symptoms of nausea and vomiting (Goldfinch et al., 1988;
Wilkes et al., 1983). Although this is a rare occurrence in this type of

Chapter 4 – Ingestion Regime
54
research, it is a clear message of overloading the system. Under these
circumstances any potential benefits of alkali ingestion are usually negated.
Therefore, this situation needs to be avoided at all costs. Further, it may be
possible that even when these symptoms are not displayed by subjects, the
bolus method is still overloading and not optimising the absorptive
mechanisms within the GI system. The investigations of Tiryaki and Atterbom
(1995) and van Someren et al. (1998) support this view, as they reported no
side-effects but, more importantly, no ergogenic effects either.
Ingestion of an alkali at a slower rate would have the benefit of better
matching the absorption processes within the GI system. This could, in turn,
result in greater increases and decreases in pH, thereby further increasing the
protection against pH during muscular contraction. In addition, decreasing
the amount of alkali within the GI system at any one time would decrease the
likelihood of overload and the chance of subjects experiencing nausea or
vomiting. To date there has been no systematic examination of SB or SC
ingestion regime on blood acid-base status. Such investigations are
important, as they could reveal that lower doses ingested more slowly invoke
greater physiological effects but with reduced side effects.
In an attempt to identify an optimal ingestion rate for SC, four ingestion rates
(bolus, 300, 600 and 900 mg.min-1) were investigated. The first hypothesis
tested was that the bolus ingestion rate was not the optimal rate in humans
at rest, as measured by change in blood pH. In addition, since SC has
previously shown ergogenic properties and is not currently on the IOC banned
substances list, the second hypothesis tested whether SC ingestion would
induce a measurable alkalosis in urine.
Methods
Subjects Eight human subjects participated in the study. The mean age of the subjects
was 21±3 years with mean heights and weights 173.9±3.1 cm and 69.2±4.2
kg, respectively. All subjects were active individuals with no health-related
problems. Prior to the start of the experiment, each subject was informed of
any risks and discomforts related to the experiment. All subjects signed a

Chapter 4 – Ingestion Regime
55
written consent form prior to the experiments. The study was approved by
the University Research Ethics committee (Queensland University of
Technology) and conformed to the Declaration of Helsinki.
Experimental Protocol During the 24-h period prior to testing, subjects refrained from vigorous
exercise, alcohol and caffeine ingestion. Approximately 3-h prior to testing,
subjects consumed a normal meal consisting largely of carbohydrates,
minimal fats and proteins (e.g., cereal, toast and juice). The meal was
recorded and repeated prior to subsequent tests in an attempt to standardise
the effect of prior food. The total length of experimenting was approximately
9-h, 1-h preparation and 8-h data collection.
Blood collection The laboratory temperature was a constant 210 centigrade (C) and the
humidity was 55±10 percent. To prevent blood flow being compromised and
due to a drafting effect within the laboratory, all subjects were informed to
bring warm clothing to use at their own discretion. After initial weighing, each
subject rested in the supine position for a period of 10-min. Subjects’
forearm cephalic vein was then cannulated with a 23-gauge needle (Becton
Dickinson, Germany) and attached to a 3-way tap (Terumo, Belgium). Ten
millilitres (ml) of blood was removed as discard and a 1-ml sample was
subsequently obtained and immediately placed on ice. To maintain cannula
patency and plasma volume, an equivalent amount of 0.9 percent saline was
re-infused after each sample. After 15 minutes in the supine position, resting
samples were obtained prior to the start of ingestion. Subjects were in the
supine position ten minutes prior to all sampling thereafter. Immediately
after obtaining the resting sample, subjects provided approximately 50 ml of
urine. The order of the ingestion protocols was randomised and separated by
at least 48 hours.
Ingestion The initiation of ingestion followed the resting samples and subjects were
required to ingest 300 mg.kg-1 of tri-sodium citrate (sigma chemicals -
Na3C8H5O7.H2O) at one of four rates, bolus, 300, 600, 900 mg.min-1. In an

Chapter 4 – Ingestion Regime
56
attempt to disguise the taste and make the ingestion more palatable, the
bolus regime involved the respective quantity of sodium citrate added to 400
ml of low energy (approximately 6 percent orange juice) solution. The
sodium citrate for the remaining ingestion rates was consumed in ‘OO’ size
gelatine capsules with water ad libitum. Each capsule was weighed before
and after being filled with sodium citrate to determine the exact quantity
(mean 1.2 g.capsule-1). The determined quantity of sodium citrate was
divided by the ingestion rate in question to obtain the timing for ingestion of
each capsule. The control condition required the participants to remain in the
laboratory for the full testing duration and provide the same samples as on an
ingestion day. After the ingestion process was finished, the subjects were
encouraged to drink water ad libitum across the duration of testing. No solid
food was ingested by the subjects during testing.
Measurement and Analysis Arterialised blood was achieved by immersing the subject’s hand in
approximately 460 C water for five minutes prior to sampling. Samples were
collected at 30-min intervals across an 8-h duration into 1.5 ml heparinised
syringes (Terumo, Belgium). The sample was immediately analysed
(Radiometer ABL505, Copenhagen) in duplicate for acid-base status (pH,
HCO3-, pCO2) and selected plasma ions (K+, Na+, Cl-). Urine samples were
obtained hourly across 8-h and immediately analysed (Radiometer ABL505,
Copenhagen) for pH.
Statistics All reported values are means±SEM. A two-way analysis of variance with
repeated measures was used to examine differences in dependent variables
with respect to treatment and time. Significant F-values were further
subjected to a Tukey’s post-hoc test to identify differences. Statistical
significance was set at p<0.05.

Chapter 4 – Ingestion Regime
57
Results
Acid-base Figure 15 shows the blood pH temporal response for all conditions. The mean
pre-ingestion pH was 7.397±0.004 and was not different between conditions.
Blood pH was significantly elevated two hours post-ingestion, mean
7.44±0.004, and stayed elevated for the remaining collection time (p<0.05).
The blood pH response during this time was not different between ingestion
rates. Figure 16 compares the average blood pH response for two time
periods: PRE and 1.5–8 h post-ingestion (POST) for each condition. PRE
values were not different between conditions. Control values were also not
different. As indicated by *, ingestion rates (IR) bolus, 300, 600 and 900
increased POST pH values, 7.445±0.004, 7.438±0.004, 7.442±0.004,
respectively, higher than control, 7.415±0.004 (p<0.05, p=0.06, p<0.05,
respectively). In addition, there was a significant interaction between time
and condition for all IR (p<0.05). Figure 17 shows the relative change in pH
from PRE to two hours post-ingestion for all conditions. There was a small,
0.66 percent, but significantly greater relative change above PRE pH values
for all conditions (p<0.05). There was no difference in relative change
between ingestion rates.
Time (hr)
0 1 2 3 4 5 6 7 8
Blo
od p
H
0.00
7.36
7.38
7.40
7.42
7.44
7.46
7.48
7.50
ControlBolus300600900
Figure 15 Blood pH 8-h temporal response
Mean (±SEM) blood pH temporal responses for all conditions. All IR, indicated by *, increased pH above control from 2-8 h (p<0.05).
*

Chapter 4 – Ingestion Regime
58
Condition
control bolus 300 600 900
Blo
od p
H
0.00
7.36
7.38
7.40
7.42
7.44
7.46
7.48 PREPOST
Figure 16 Mean blood pH response pre- and post-ingestion
Mean (±SEM) blood pH values for each IR are shown. Comparison of mean blood pH pre-ingestion (PRE) and 1.5-8 h post-ingestion (POST) within condition. PRE values were not different between conditions. Control values were not different. All IR, marked *, increased pH above control POST values (p<0.05, p<0.10 and p<0.05 for 300, 600 and 900, respectively).
Condition
control bolus 300 600 900
% c
hang
e
0.0
0.2
0.4
0.6
0.8
Figure 17 Blood pH relative change between PRE and 2 h post-ingestion
Mean relative blood pH changes for each IR are shown. Each IR, indicated by *, induced a small (mean 0.66%) but significant relative change in blood pH (p<0.05).
** *
* *
*
*

Chapter 4 – Ingestion Regime
59
Figure 18 shows the average post-ingestion blood [HCO3-] for each condition.
As indicated by * bolus, 300, 600 and 900 (29.6, 29.7, 29.8 and 29.9 mmol.l-
1, respectively) conditions significantly (p<0.05) elevated blood [HCO3-] above
that for control (26.3 mmol.l-1). There were no statistical differences between
the respective increases in blood [HCO3-] for each ingestion rate of 12.5,
12.9, 13.3 and 13.7 percent. Temporal responses for each condition are
depicted in Figure 19. After 1.5 h of ingestion, all experimental IR had
elevated blood [HCO3-] higher than control (p<0.05). This observation
continued for the next 6.5 h. Interestingly, the most rapid dose, bolus, had a
faster temporal response than the three remaining ingestion rates. Under
bolus, only thirty minutes was required to elevate blood [HCO3-] above control
(p<0.05). Although the response was faster under the bolus condition, the
magnitude of change was slightly less (approximately 0.8 percent or 0.2
mmol.l-1) than the other three rates.
Condition
Control Bolus 300 600 900
HC
O3- (
mm
ol.l-1
)
0
20
22
24
26
28
30
32
34
Figure 18 Mean post-ingestion blood [HCO3-] for all IR
Mean (±SEM) blood [HCO3-] for each IR are shown. Ingestion rates, marked
*, elevated post-ingestion [HCO3-] significantly above control (p<0.05).
* ***

Chapter 4 – Ingestion Regime
60
Time (h)
0 1 2 3 4 5 6 7 8
HC
O3- (
mm
ol.l-1
)
05
24
26
28
30
32
34
36
ControlBolus300600900
Figure 19 Mean blood [HCO3
-] temporal responses across 8 h for all IR
All ingestion rates elevated blood [HCO3-] (SEM removed for clarity) above
control after 1.5 and remained elevated to 8 h, represented by * (p<0.05). Bolus, marked #, had the fastest response elevating [HCO3
-] above control in 30 min (p<0.05).
Average post-ingestion blood pCO2 response for each condition is shown in
Figure 20. Similar to the response of blood [HCO3-], bolus, 300, 600 and 900
(45.4, 43.8, 44.7 and 44.8 percent, respectively) conditions elevated blood
[pCO2] above control (41.5 percent) (p<0.05). Figure 21 shows the temporal
blood pCO2 response for each condition. The pre-ingestion values were not
significantly different from each other. Unfortunately, the between-day
variability obscured the observation of any condition effect on pCO2.
* #

Chapter 4 – Ingestion Regime
61
Condition
Control Bolus 300 600 900
PC
O2 (
mm
Hg)
0
38
40
42
44
46
48
50
Figure 20 Mean post-ingestion blood [pCO2] for each IR
Mean (±SEM) blood [pCO2] for all IR are shown. Each IR, marked *, significantly raised post-ingestion [pCO2] above control (p<0.05).
Time (h)
0 1 2 3 4 5 6 7 8
pCO
2 (m
mH
g)
0
38
40
42
44
46
48
50
52
ControlBolus300600900
Figure 21 Temporal response for blood [pCO2] for each IR
Mean blood [pCO2] (SEM removed for clarity) for each condition were not different from each other or control. This was mainly due to large between-day variability.
***
*

Chapter 4 – Ingestion Regime
62
Strong Ions Figure 22, (a) through (e), shows the mean blood H+ response for each
condition separately. The ↓ symbol identifies the time at which the nadir PRE
values occurred. The number (e.g., 0.50) above the arrow represents the
magnitude of change expressed in meq.l-1×10-8. The fastest IR, bolus,
induced the slowest peak change from PRE values at 6.0 h, whereas the
greatest magnitude of change (0.66 meq.l-1x10-8) was induced by the 300 IR.
Figure 22 (f) shows the average PRE and POST blood [H+] for each condition.
No differences were identified between the PRE values, mean 4.0x10-8 meq.l-
1. As indicated by * all IR reduced POST blood [H+], mean 3.6x10-8 meq.l-1,
lower than POST control values, 4.0×10-8 meq.l-1 (p<0.05), however the
reductions caused by each IR were not different from each other. Figure 23
shows the average blood [H+] at three time points: PRE, 1.5 h post-ingestion
(POST1) and 2.5 – 5.5 h post-ingestion (POST2). Control PRE blood [H+] was
not different between the three time points, mean 4.0×10-8 meq.l-1. Further,
PRE blood [H+] was not different between conditions, mean 3.95×10-8 meq.l-1.
As indicated by *, the 300 IR significantly lowered blood [H+] at POST1,
3.55×10-8 meq.l-1, from control, 3.87×10-8 meq.l-1 (p<0.05). IR 300, 600 and
900 POST2, marked #, [H+] (3.48, 3.58, 3.52×10-8 meq.l-1) were lower than
POST2 control [H+] (3.87×10-8 meq.l-1) (p<0.05). When compared with their
respective PRE values, all IR significantly reduced blood [H+] at both POST1
and POST2 time points (p<0.05). In Figure 24, the relative change for each
time period, POST1 and POST2, can be seen. The relative changes from PRE
values at both time points for control were less than one percent. However,
under the influence of SC ingestion this increased to approximately 10, 14, 10
and 7 percent during POST1 and a further 2, 2, 2 and 7 percent during POST2
for bolus, 300, 600, and 900 mg.min-1 IR, respectively (p<0.05). When
considering the above changes as a 100 percent change, the POST2
component measures approximately 19, 14, 17 and 43 percent of the
decrease in blood [H+] for each IR, respectively.

Chapter 4 – Ingestion Regime
63
Time (hr)
0 1 2 3 4 5 6 7 8
Bloo
d [H
+ ] (m
eq.l-1
)
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
Control
Time (hr)
0 1 2 3 4 5 6 7 8
Bloo
d [H
+ ] (m
eq.l-
1 )
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
Bolus
Time (hr)
0 1 2 3 4 5 6 7 8
Bloo
d [H
+ ] (m
eq.l-
1 )
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
300
Time (hr)
0 1 2 3 4 5 6 7 8
Bloo
d [H
+ ] (m
eq.l-
1 )
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
600
Time (hr)
0 1 2 3 4 5 6 7 8
Bloo
d [H
+ ] (m
eq.l-
1 )
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
900
Condition
Control Bolus 300 600 900
Bloo
d [H
+ ] (m
mol
.l-1)
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
PREPOST
Figure 22 Individual IR temporal responses in blood [H+] for all conditions
Mean (±SEM) blood H+ response for each condition separately (a) – (e). Time at peak change is marked with ↓. The number above ↓ represents magnitude of change in meq.l-1×10-8. Mean (±SEM) PRE and POST values are compared in (f). IR POST blood [H+] was significantly lower than POST control and marked with * (p<0.05).
*
0.50
0.50 0.66
0.45* * *
(a)
(e)
(d)
(b)
(c)
(f)

Chapter 4 – Ingestion Regime
64
Condition
Control Bolus 300 600 900
Bloo
d [H
+ ] (m
mol
.l-1 )
0.0
3.0e-8
3.2e-8
3.4e-8
3.6e-8
3.8e-8
4.0e-8
4.2e-8
4.4e-8
PREPOST1POST2
Figure 23 Mean (± SEM) blood [H+] for each IR at 3 time points
Collection time was divided into 3 periods, pre-ingestion (PRE), 1.5 h post-ingestion (POST1) and 2.5–6 h post-ingestion (POST2). Only 300 mg.min-1 POST1 [H+], marked *, was statistically lower than control POST1 (p<0.05). However, 300, 600 and 900 mg.min-1 POST2 [H+], marked #, were lower than control POST2 [H+] (p<0.05).
Condition
control bolus 300 600 900
% C
hang
e
0
2
4
6
8
10
12
14
16
18 POST1POST2
Figure 24 Relative percent changes in blood [H+]
Decrease in [H+] expressed as percent change. Total change has been proportioned into the respective changes for POST1 and POST2 periods.
*## #

Chapter 4 – Ingestion Regime
65
Figure 25, (a) through (e), shows the mean blood K+ response for each
condition separately. Again, the ↓ symbol identifies the time at which the
nadir PRE values occurred. The number (e.g., 0.29) above the arrow
represents the magnitude of change expressed in mmol.l-1. The most rapid
ingestion regime, bolus, induced what seems to be a two-step K+ response.
There was a slight decline from PRE [K+] (4.03±0.10 mmol.l-1) for the first 2.5
hours post ingestion (3.96±0.09 mmol.l-1) and then a further decline that
peaked at 6 hours post ingestion (3.74±0.09 mmol.l-1). The overall decline in
[K+] was only slight at 0.29 mmol.l-1 compared with the other IR. The
remaining IR (Figure 25 c, d and e) resulted in a steady decline in [K+] across
time peaking at 2.5, 4.5 and 5.5 hours post ingestion, respectively. The
maximum decline in [K+] for each IR (bolus, 300, 600 and 900 mg.min-1) was
0.29, 0.44, 0.54 and 0.50 mmol.l-1, respectively. Figure 25 (f) compares both
average pre-ingestion (PRE) and 1.5-8 hours post ingestion (POST) K+ values
for each condition. No differences were identified between PRE values, mean
4.06±0.04 mmol.l-1. As indicated by * 300 (3.68±0.09 mmol.l-1), 600
(3.74±0.09 mmol.l-1) and 900 (3.74±0.09 mmol.l-1) IR reduced blood POST
[K+] significantly lower than their respective PRE (4.08±0.09 mmol.l-1) values
(p<0.05). Although all three rates were lower, the 300 IR POST [K+] was
significantly lower (p=0.11) than either the 600 or 900 IR POST [K+], as
represented by #. Figure 26 shows the average blood [K+] at three time
points: PRE, 1.5 h post ingestion (POST1) and 2.5 – 5.5 h post ingestion
(POST2). At no time were control (mean 4.06±0.08 mmol.l-1) and bolus
(mean 3.93±0.08 mmol.l-1) [K+] different. As represented by *, only the 300
POST1 IR decreased [K+], (3.66±0.08 mmol.l-1), lower than all three control
time points (4.01±0.11, 4.20±0.08, 4.10±0.08 mmol.l-1) (p=0.06). In
addition, 300, 600 and 900 POST2 [K+] were lower than their respective PRE
values, as indicated by # (p<0.05).
Figure 27 shows the relative change in blood [K+] for both time periods,
POST1 and POST2. There was a larger variation, almost five percent,
between control K+ values than what was seen with H+, however, this was not
significant. With the exception of the bolus and 600 IR, a large proportion of
total change from PRE K+ values, 300–83 percent and 900–86 percent,
occurred after 1.5 hours post ingestion. Although large changes occurred
with IR 600 and 900, it would appear this has been exacerbated by PRE K+
values (4.13±0.09 and 4.09±0.09, respectively), which were approximately 3

Chapter 4 – Ingestion Regime
66
percent higher than the other IR. Even taking this into consideration, the
combination of the 600 IR and longer ingestion time induced a further 28
percent change in [K+].
Time (hr)
0 1 2 3 4 5 6 7 8
[K+ ] (
mm
ol.l-1
)
0.0
3.43.53.63.73.83.94.04.14.24.34.44.5
Control
Time (hr)
0 1 2 3 4 5 6 7 8
[K+ ] (
mm
ol.l-1
)
0.0
3.4
3.5
3.6
3.7
3.8
3.9
4.0
4.1
4.2
4.3
4.4
4.5
Bolus
Time (hr)
0 1 2 3 4 5 6 7 8
[K+ ] (
mm
ol.l-1
)
0.0
3.4
3.5
3.6
3.7
3.8
3.9
4.0
4.1
4.2
4.3
4.4
4.5
300
Time (hr)
0 1 2 3 4 5 6 7 8
[K+ ] (
mm
ol.l-1
)
0.0
3.4
3.5
3.6
3.7
3.8
3.9
4.0
4.1
4.2
4.3
4.4
4.5
600
Time (hr)
0 1 2 3 4 5 6 7 8
[K+ ] (
mm
ol.l-1
)
0.0
3.4
3.5
3.6
3.7
3.8
3.9
4.0
4.1
4.2
4.3
4.4
4.5
900
Condition
control bolus 300 600 900
[K+ ] (
mm
ol.l-1
)
0.0
3.43.53.63.73.83.94.04.14.24.34.44.5
PREPOST
Figure 25 Mean Blood K+ temporal profiles for all conditions
Mean (±SEM) blood K+ response for each condition separately (a) – (e). Time at peak change is marked with ↓. The number above ↓ represents magnitude of change in mmol.l-1. Mean (±SEM) PRE and POST values are compared in (f). IR 300, 600 and 900, marked *, reduced POST [K+] lower than their respective PRE values (p<0.05). In addition, 300 IR, marked #, [K+] was lower than both 600 and 900 IR (p=0.11).
*#* *
0.54
0.50
0.44
0.29
(a)
(e)
(d)
(b)
(c)
(f)

Chapter 4 – Ingestion Regime
67
Condition
control bolus 300 600 900
Bloo
d [K
+ ] (m
mol
.l-1)
0.03.53.63.73.83.94.04.14.24.34.44.5
PREPOST1POST2
Figure 26 Mean (± SEM) blood [K+] for each condition at 3 time points
Collection time was divided into 3 periods, pre-ingestion (PRE), 1.5 h post-ingestion (POST1) and 2.5–6 h post-ingestion (POST2). 300 mg.min-1 POST1 IR, marked *, reduced [K+] below all control values (p=0.06). 300, 600 and 900 POST2 IR, marked #, reduced [K+] lower than their respective PRE values (p<0.05).
Condition
control bolus 300 600 900
% c
hang
e
-5
0
5
10
15
20
POST1POST2
Figure 27 Relative percent changes in blood [K+]
Decrease in [K+] expressed as percent change. Total change has been proportioned into the respective changes for POST1 and POST2 periods. 83, 28 and 86 percent of the decrease in [K+] occurred during POST2 for 300, 600 and 900 IR, respectively.
*
# # #

Chapter 4 – Ingestion Regime
68
When comparing 1.5 h post-ingestion and control values (Figure 28), blood
[Cl-] was unaffected by the ingestion of sodium citrate independent of IR.
When exploring the Cl- response temporally (Figure 29) it would seem there
was a negative time effect independent of the treatment (sodium citrate
ingestion). To test this further, the data were separated into three time
periods, pre-ingestion (PRE), 2.5-5.5 h post-ingestion (POST1) and 7.0-8.0 h
post-ingestion (POST2) and then compared. It was revealed that after 2.5 h
of ingestion PRE blood [Cl-], 98.2±0.4 mmol.l-1, significantly declined to
94.9±0.4 mmol.l-1 (p<0.05), however this level was maintained (95.0±0.4
mmol.l-1) across the remaining collection period (Figure 30).
Condition
Control Bolus 300 600 900
Cl- (m
mol
.l-1)
0
90
92
94
96
98
100
Figure 28 Mean (±SEM) blood [Cl-] response for each condition
SC ingestion had no effect on mean [Cl-] response for each condition.

Chapter 4 – Ingestion Regime
69
Time (h)
0 1 2 3 4 5 6 7 8
Cl- (m
mol
.l-1)
0
90
92
94
96
98
100
ControlBolus300600900
Figure 29 Mean Cl- temporal response for each condition
No ingestion rate effect on [Cl-], however there appears to be a negative time effect.
Time
PRE POST1 POST2
Cl- (m
mol
.l-1)
0
90
92
94
96
98
100
Figure 30 Mean (±SEM) blood [Cl-] response at 3 time points
Collection time was divided into 3 periods, pre-ingestion (PRE), 2.5–5.5 h post-ingestion (POST1) and 7.0–8.0 h post-ingestion (POST2). A negative time effect is apparent by POST1, marked *, and is maintained through POST2 (p<0.05).
As shown in Figure 31, blood [Na+] was elevated above control values
(130.9±0.5 mmol.l-1) only when sodium citrate was ingested at a rate of 300
mg.min-1 (133.6±0.5 mmol.l-1) (p<0.05).
* *

Chapter 4 – Ingestion Regime
70
Figure 32 shows the temporal response for each condition. The large
variability within and between conditions greatly affected the ability to
demonstrate differences. Although there were differences between some
conditions, they appeared not to be systematic.
Condition
Control Bolus 300 600 900
Na+ (m
mol
.l-1)
0
130
132
134
136
138
140
Figure 31 Mean (±SEM) blood [Na+] response for all conditions
SC ingested at 300 mg.min-1, marked *, increased [Na+] above control values (p<0.05).
Time (h)
0 1 2 3 4 5 6 7 8
Na+ (m
mol
.l-1)
010
130
132
134
136
138
ControlBolus300600900
Figure 32 Mean blood [Na+] temporal response for all conditions
The large variability (not shown) within and between IR greatly affected the identification of any differences.
*

Chapter 4 – Ingestion Regime
71
pO2 To ensure the arterialisation status was consistent across all samples and
therefore had no confounding influence, pO2 was measured in every sample.
The mean [PO2] across all conditions was 71.3±3.5 mmHg. [PO2] was not
different between conditions as shown in Figure 33.
Condition
Control Bolus 300 600 900
pO2 (
mm
Hg)
0
50
55
60
65
70
75
80
85
90
Figure 33 Mean (±SEM) blood PO2 response for all conditions
Stable arterialisation was maintained across all conditions, no differences were observed.
Urine The urine pH response was quite marked and is depicted in Figure 34. All
sodium citrate ingestion regimes increased urine pH (p<0.05). This increase
was detectable one hour after the initiation of ingestion. Again, the bolus
regime altered urine pH to the greatest extent earliest, increasing pH by 32
percent compared with 21, 24 and 21 percent for 300, 600 and 900 mg.min-1,
respectively, within the first hour. A further 6, 19, 15 and 17 percent
increase in pH for bolus, 300, 600 and 900 mg.min-1, respectively, brought
each condition to its maximum where they remained up to seven hours post-
ingestion.

Chapter 4 – Ingestion Regime
72
Time (h)
0 1 2 3 4 5 6 7 8
Urin
e pH
0.00
5.00
6.00
7.00
8.00
9.00
Control Bolus 300600900
Figure 34 Mean (±SEM) urine pH temporal response for each condition
All IR, indicated by *, alkalised urine pH above control (p<0.05). Bolus, 300, 600 and 900 IR increased urine pH by 38, 40, 39 and 38 percent, respectively.
Discussion This is the first study to compare four ingestion rates of 300 mg.kg-1 body
mass of tri-sodium citrate on blood and urine pH in humans at rest. The
present study supports the hypothesis that consuming 300 mg.kg-1 of sodium
citrate in bolus form is not the optimal regime to perturb blood pH at rest.
The greatest blood alkalosis, 7.473 pH units, was achieved by ingesting
sodium citrate at a rate of 300 mg.min-1. Secondly, this study supports the
hypothesis that SC ingestion, independent of IR, induces a clearly measurable
urine alkalosis. The mean urine alkalosis across all experimental conditions
was approximately 40 percent (range 38–40 percent) larger than control.
pO2 status Heating of the hand, by immersing it in 460 C water, increases blood flow via
the dilation of local vasculature. In doing so, low oxygenated venous blood is
mixed with higher oxygenated arterial blood, which is reflected by a [pO2]
approximately midway between venous and arterial blood. This technique
allows the investigator to obtain close-to arterial blood values without the
complications of arterial punctures. To ensure the same level of arterial-
*

Chapter 4 – Ingestion Regime
73
venous mixing was achieved, the [pO2] was recorded for each sample. The
[pO2], mean 71.3±3.5 mmHg, was not different between any of the conditions
(Figure 33), thus confirming that any differences observed in other measured
ions were not an artefact of the pO2 status.
Sodium citrate and GI absorption In the current study, bolus ingestion was associated with a blood [H+]
decrease from 4.0×10-8 meq.l-1 to 3.57×10-8 meq.l-1 at rest. The observed
decrease in [H+] is greater than reported in the literature (Kowalchuk et al.,
1989), however this can be explained by the timing of these observations.
The lower [H+] in the present study was recorded at 6 h post-ingestion
compared with only 1 h for the above-mentioned study. The 1 h [H+] for both
studies is comparable. Of the other ingestion rates investigated, 300 mg.min-
1 was associated with the largest effect and continued to decrease [H+]
beyond that experienced during the bolus regime to 3.37×10-8 meq.l-1. This
further 45 percent change in blood [H+] may be linked to a number of
explanations.
The first of these may lie in how the alkali is introduced to the body, i.e., via
the GI tract. This method relies upon the components of the GI tract to
transport the alkali through the intestinal wall across the interstitial space and
finally into the blood via the capillary network of the villi. In the current
study, the bolus regime combined the sodium citrate with a low energy
flavoured drink of 400 ml in an attempt to disguise the taste and make
ingestion more palatable. This technique has been previously reported in the
literature (Ibanez et al., 1995; McNaughton & Cedaro, 1992). The 30 g.l-1
carbohydrate concentration contained within the solution probably slows
gastric emptying from the stomach into the duodenum in comparison to the
300 mg.min-1 regime, which has no carbohydrate content. The work of
Erskine and Hunt (1981), which demonstrated that sodium citrate given in 6
small doses entered the duodenum 200 percent faster than 100 g.l-1 of
glucose, may support this theory. Therefore, it appears that small doses of
sodium citrate taken in quick succession enter the small intestine faster than
one large dose. This is especially true when using a bolus dose in combination
with carbohydrate.

Chapter 4 – Ingestion Regime
74
Carbohydrate content and osmolality can affect absorption through the small
intestine (Vist & Maughan, 1995). Vist and Maughan (1995) demonstrated
that a higher concentration of carbohydrate slowed emptying from the small
intestine. In the present study, the carbohydrate concentration for the bolus
regime and the 300, 600 and 900 mg.min-1 regimes collectively were 30 g.l-1
and 0 g.l-1, respectively. Therefore, it is reasonable to assume that combining
sodium citrate with carbohydrate may slow its absorption through the small
intestine. Based on the assumption that 100 ml of water was consumed with
each sodium citrate capsule, the calculated osmolality for the bolus ingestion
regime and the 300, 600 and 900 mg.min-1 regimes collectively were 171.7
and 4.1 mosmol.kg-1, respectively. As suggested by Vist and Maughan
(1995), the solution osmolality may play an additional role in emptying from
the small intestine. That is, the higher the osmolality, the slower the solution
will be emptied from the intestine. Consequently, the bolus ingestion regime
seems to have two properties inhibiting its movement and uptake through the
stomach and small intestine. These inhibiting properties may mediate a loss
of sodium citrate uptake under the bolus regime resulting in a decreased
effect on blood pH. In contrast, the 300 mg.min-1 ingestion regime creates a
better environment for passage through the GI tract and into the blood, which
is supported by the increased blood pH response.
No subject in the current study exhibited GI upsets, which is consistent with
other studies using sodium citrate (Schabort et al., 2000; Linossier et al.,
1997; Hausswirth et al., 1995). The use of sodium bicarbonate, in contrast,
has often led to GI upsets (McNaughton, 1992a; Goldfinch et al., 1988;
Wilkes et al., 1983). This problem is probably a function of the mechanisms
through which the substances act. While the exact mechanism explaining
how sodium citrate increases pH is not well understood (Potteiger et al.,
1996b), studies using sodium bicarbonate may help to explain this
phenomenon, as it has similar physiological effects to sodium citrate (Spiegal,
1997; Tiryaki & Atterbom, 1995; Parry-Billings & MacLaren, 1986). Citrate is
not an alkali per se (Tiryaki & Atterbom, 1995), rather it produces sodium
bicarbonate via its hepatic oxidation (Halperin, 1982). Consequently, and in
contrast to sodium bicarbonate, the alkalising effect of citrate is not apparent
until after it has left the stomach, which most likely decreases the risk of
nausea and vomiting.

Chapter 4 – Ingestion Regime
75
Sodium citrate and acid-base balance Sodium citrate ingestion was associated with an elevated blood pH across all
conditions. This finding is consistent with other research (van Someren et al.,
1998; Ball & Maughan, 1997) that has investigated the effects of SC ingestion
at a similar dose. Analysis of the blood pH temporal response showed that all
ingestion rates had similar effects (Figure 15). The two most common
methods for ingesting sodium citrate have been diluting it in a solution of
300-500 ml (Hausswirth et al., 1995; Ibanez et al., 1995; Kowalchuk et al.,
1989) or in gelatine capsules with water ad libitum (Potteiger et al., 1996b).
Typically, the ingestion period is 90 min with only pre-ingestion and pre-
exercise pH values reported. Therefore, it appears that a) there is a lack of
understanding relating to the most beneficial ingestion regime and b) that the
general assumption is that after 90 min the alkali has had enough time to
induce a complete physiological effect and cause an ergogenic response. The
present study demonstrated that ingesting SC at 300 mg.min-1 induced a
greater alkalosis than the bolus regime commonly practiced (7.473 and 7.447
pH units, respectively). Further, at 90 min post-ingestion, pH had only
partially alkalised the blood with peak alkalosis occurring some 60 and 120
min later for bolus and 300 mg.min-1, respectively. Therefore, if the degree
of alkalosis is in part responsible for the ergogenic effect of SC, it should be
consumed at a rate of 300 mg.min-1 and the impending performance should
not be initiated less than 3.5 h post-ingestion.
The metabolic alkali load of 70.4 mmol (mean total ingestion 20.7 g sodium
citrate) was associated with increases in HCO3- and pCO2 concentrations of
3.47 mmol.l-1 and 3.15 mmHg, respectively. These values are similar to
those found in other investigations (Hausswirth et al., 1995; Tiryaki &
Atterbom, 1995; McNaughton, 1990). When comparing the four ingestion
rates, the most rapid ingestion rate, bolus, resulted in a corresponding
increase in blood [HCO3-]. Under these conditions blood [HCO3
-] was elevated
above control after 30 min. In contrast, the blood pH response was not
different from control until 2 h post-ingestion. These inconsistent findings
suggest that different mechanisms are involved in the regulation of each ion.

Chapter 4 – Ingestion Regime
76
Ingestion time and [H+] The times at which peak [H+] changes occurred were also different between
conditions. Some researchers (Potteiger et al., 1996a; Cox & Jenkins, 1994;
McNaughton, 1990) have assumed that 90 minutes post ingestion was a
sufficient waiting time to obtain the physiological benefits from alkali loading,
while others have suggested longer periods up to 3 h (Potteiger et al., 1996b;
Heigenhauser & Jones, 1991). This study demonstrated that for sodium
citrate ingested in bolus and at 300, 600 and 900 mg.min-1 only a partial
physiological response is achieved at 90 minutes post ingestion (Figure 24).
Peak changes in [H+] ranged from 3.5 h-6.0 h for 300 mg.min-1 and bolus,
respectively. These additional ingestion periods resulted in [H+] decreasing a
further 15–20 percent. The implications of a further reduction in [H+] on
exercise performance are unknown and further research is warranted to
establish this. Nevertheless, McNaughton (1990) showed a positive
relationship between sodium citrate and performance for three doses of
sodium citrate, 300, 400 and 500 mg.kg-1. Associated with these observed
performance increases was a continual decline in blood [H+]. Consequently,
the degree of decreased [H+] induced may be linked to the ergogenic
potential of sodium citrate. Numerous studies have shown no ergogenic
effect of alkalosis (Schabort et al., 2000; Tiryaki & Atterbom, 1995; Cox &
Jenkins, 1994; Kozak-Collins et al., 1994; Gaitanos et al., 1991), even with
significant decreases in blood [H+]. The current study suggests that a longer
ingestion time would have led to a greater alkalosis and possibly the
observation of an ergogenic effect.
Sodium citrate and [K+] This is the first study to examine the effect of SC ingestion on the blood K+
response in humans. An interesting observation was that SC ingestion in
bolus form had no effect on blood [K+]. In contrast, all capsule ingestion
rates (slower) were associated with decreases in blood [K+] approximating 0.5
mmol.l-1. The magnitude of these responses are similar to those recently
reported by Lindinger et al. (1999). Moreover, the ingestion regime they
employed was similar to the 300 mg.min-1 used here. Although their
investigation used sodium bicarbonate to manipulate plasma ion regulation,
other investigations have shown that the physiological effects of sodium
citrate and sodium bicarbonate are similar (Tiryaki & Atterbom, 1995) and

Chapter 4 – Ingestion Regime
77
therefore comparable. Even though the effects of SC on blood [K+] are not
fully understood, it has been suggested that the NaHCO3- alkalosis decreases
extracellular [K+] via an increased intracellular [Na+] activated Na+-K+-ATPase
activity (Clausen, 1986). Accordingly, the current venous data supports this
potential role with an increased blood [Na+] when ingesting at 300 mg.min-1
(Figure 31). Unfortunately, it is impossible to support or refute the work of
others without corresponding muscle and blood arterial data. Furthermore,
venous blood values often vary due to the rapidity of gas and ion exchange
processes in skeletal muscle (Lindinger et al., 1999) and should therefore be
interpreted carefully. To elucidate the mechanisms underpinning K+
regulation, further research incorporating the above-mentioned techniques is
thus required. Still, the present data does indicate that ingesting SC in
capsules at a rate of 300, 600 or 900 mg.min-1 can manipulate blood [K+].
Sodium citrate and urinary alkalosis The aim of collecting and analysing urine pH hourly was to establish whether
the ingestion of 300 mg.kg-1 sodium citrate was associated with a urinary
alkalosis of a sufficient magnitude to be identified. The mean urine pH at rest
was 6.45±0.65 and is consistent with the literature (Lindinger et al., 2000;
Cogan et al., 1990; Oster et al., 1988; Kachadorian & Johnson, 1970).
Sodium citrate ingestion was associated with a significant elevation in urine
pH (mean 7.68±0.26), which was evident 1 h post-ingestion and remained
elevated above resting urine pH for a further 7 h. The data collected in this
study offers no explanation for the mechanisms involved in this increase;
however, work done by Oster et al. (1988) may provide some insight. They
compared net acid excretion after chronically loading with both sodium citrate
and sodium bicarbonate for four days. The effects they demonstrated on
urine pH were quite modest in comparison with the current study, but this can
probably be explained by the dose of 2.55 mEq.h-1 (calculated based on 61.2
mEq.day-1) compared with (at least) 70.4 mEq.h-1 here. Nevertheless, they
showed that associated with an alkalotic urine pH, NH4, TA (titratable acid)
and NAE (net acid excretion) were all decreased, while HCO3- excretion was
also increased (Oster et al., 1988). An unexpected result in the current study
was the marked similarity in urine pH response between ingestion rates
despite the marked differences in the rate and magnitude of disturbances
observed in the blood.

Chapter 4 – Ingestion Regime
78
Conclusion The present study demonstrated that ingesting 300 mg.kg-1 of sodium citrate
at a rate of 300 mg.min-1 induced a greater degree of blood alkalosis than the
commonly practiced bolus regime. In addition, a 90 min ingestion time
resulted in only a partial blood alkalosis with the complete blood alkalosis
achieved at 3.5 and 6.0 h post-ingestion for 300 mg.min-1 and bolus ingestion
rates, respectively. Finally, the ingestion of 300 mg.kg-1 sodium citrate,
independent of ingestion rate, can be easily detected via the analysis of urine
pH.

Chapter 5 – Interstitial Alkalosis
79
CH A P T E R 5 EF F E C T O F S O D I U M C I T R A T E O N
I N T E R S T I T I A L PH I N H U M A N S K E L E T A L M U S C L E
Introduction Ingestion of sodium citrate improves exercise performance across a variety of
modalities (Shave et al., 2001; Potteiger et al., 1996a; McNaughton &
Cedaro, 1991; Gao et al., 1988). Although there has been an abundance of
research in this area, the precise mechanisms underpinning this phenomenon
are still not well understood (Hollidge-Horvat et al., 2000). These studies
have been performed on whole body exercise. There has been little research
performed on the effect of alkali ingestion on small muscle mass. Webster et
al. (1990) showed no effect of sodium bicarbonate ingestion on resistance
exercise performance. Further, there have been no investigations on single
leg quadriceps muscle performance. Due to it well controlled nature, this
latter type of exercise model may be a better model to provide new
information about the mechanisms underpinning the ergogenic properties of
orally induced alkalosis.
Currently, it is known that sodium citrate ingestion is associated with an
increase in blood pH and [HCO3-] (Schabort et al., 2000). It has been
suggested that the increased pH (or decreased [H+]) associated with alkalosis
amplifies the gradient between muscle and blood, thereby augmenting proton
efflux from the muscle (in both H-La and H+ forms) (Tiryaki & Atterbom,
1995; Lindinger et al., 1990; Mainwood & Warsley-Brown, 1975). However,
this theory does not take into account any involvement of the interstitial
compartment that protons pass through to enter the blood. Some studies
have referred to both the blood and interstitial compartments collectively as
extracellular (Brien & McKenzie, 1989; Mainwood & Warsley-Brown, 1975).
While this remains true (they are both outside the muscle cell), these
compartments possess markedly different characteristics and may thus
exhibit different reactions to alkalosis. As there has been limited research
performed on skeletal muscle interstitium during exercise, little is known
about its function and reaction to introduced substances. Recently, however,
Maclean et al. (2000) demonstrated that interstitial pH increases during
isometric exercise. This finding is somewhat difficult to explain, but

Chapter 5 – Interstitial Alkalosis
80
nonetheless demonstrated that blood and interstitium respond differently
during exercise and therefore should be considered as separate entities. In
addition, it has been shown that the buffer capacities of interstitium and blood
are different (Aukland & Reed, 1993). Although the osmolalities are similar
between blood (306 mosmol.l-1) and interstitium (308 mosmol.l-1), the ionic
composition is not. In particular, the interstitial concentrations of Cl-, HCO3-
and Na+ are all higher than blood. In contrast, there are no proteins found
within the interstitium (Geers & Gros, 2000). Since sodium citrate ingestion
has been linked to increases in blood [HCO3-] (Potteiger et al., 1996a), it may
be possible that the different initial [HCO3-] are influenced in different ways.
Similarly, since the ionic composition is different between these
compartments and alkali ingestion has been shown to influence ionic
composition within blood (Lindinger et al., 2000), it seems reasonable to
assume that induced alkalosis will affect the interstitium dissimilar to blood.
Two factors that mediate changes in pH are HCO3- and pCO2 (Lindinger et al.,
1990). It has been suggested that the sarcolemma is impermeable to HCO3-
(Robin, 1961), and as such metabolic alkalosis has no direct influence on the
intracellular buffer capacity. On the other hand, there appears to be no such
evidence for the movement of HCO3- into the interstitium. Further, pCO2 can
easily diffuse across membranes between compartments (Geers & Gros,
2000; Kowalchuk & Scheuermann, 1995). Since metabolic alkalosis is
associated with elevated blood HCO3-, and it is likely that HCO3
- is capable of
moving between the blood and interstitium, it stands that the effects of
alkalosis may be different within the two compartments. As a result, it is
possible that the suggested augmentation of intracellular H+ efflux associated
with alkalosis is part of a two-tiered process, the first between muscle and
interstitium and the second between interstitium and blood.
Of late, Maclean et al. (2000) have measured interstitial pH during static
quadriceps exercise in humans using microdialysis. However, there were
methodological limitations in their study that resulted in measurements at
minute intervals only. At the time, there was no technique available to
examine changes in interstitial pH during dynamic exercise in humans that
was capable of detailed analysis of short-term exercise. A technique to
accomplish this has been successfully developed and performed as part of this

Chapter 5 – Interstitial Alkalosis
81
thesis (see Chapter 3). Thus, it is now possible to investigate the role of
interstitial pH during exercise.
As outlined above, the aims of this study were to determine the effects of
metabolic alkalosis on human skeletal muscle interstitial pH at rest and during
intense exercise. The specific hypotheses tested were that sodium citrate
ingestion would increase knee-extensor exercise performance and increase
interstitial pH.
Methods
Subjects Five human subjects participated in this study. The mean age of the subjects
was 31±10 years with mean heights, weights and BMI’s of 180.8±5.4 cm,
81.7±11.1 kg, and 25.0±3.1, respectively. All subjects were active individuals
with no health-related problems. Prior to the start of the experiment, each
subject was informed of any risks and discomforts related to the experiment.
All subjects signed a written consent form prior to the experiments. The
study was approved by the local ethics committee (August Krogh Institute,
University of Copenhagen) and conformed to the Declaration of Helsinki.
Exercise protocol Subjects performed one-legged knee-extensor exercise in a supine position
and were secured via a series of straps, two shoulder, one waist and one
thigh strap, so exercise was restricted to the quadriceps muscle (Bangsbo et
al., 1990). During exercise the subjects had visual feedback in the form of a
digital display showing the cadence and power output. A 10 min warm-up at
an intensity of 10 W was performed prior to the experimental test. The
experimental test required subjects to maintain a cadence of 60 rpm for as
long as possible at a pre-determined exercise intensity. Subjects were given
verbal encouragement to perform, however, the test was terminated when
the cadence was below 60 rpm for more than 15 consecutive seconds.

Chapter 5 – Interstitial Alkalosis
82
Experimental exercise intensity The experimental exercise intensity was determined via an incremental test
followed by two constant load exercise tests, each separated by 48 h. All
tests were preceded by a 10 min warm-up at an intensity of 10 W followed by
a five minute rest. The incremental test was initiated at 10 W and increased
at a rate of 10 W at the end of each 5 min period until the subject could no
longer maintain a cadence of 60 rpm. Subjects were given verbal
encouragement, however, the test was terminated when the cadence was
below 60 rpm for 15 consecutive seconds. To ascertain the final intensity for
the constant load test, the last incomplete 10 W increment was proportioned
over the 5 min time period. That is, each minute of the stage was equivalent
to a two watt increase. Therefore, if the subjects completed 2 min of an
incremental period, a further 4 W was added to their previously completed
stage. Subjects then returned to the laboratory and performed a constant-
load exercise test at this calculated intensity to ensure the intensity was of a
sufficient magnitude to cause fatigue between 5 and 7 min. This was
repeated on a second occasion for reliability. A second repeat (third test) was
performed in the event that the above objectives were not achieved.
Probe insertion Prior to the experiment, subjects rested in a supine position with their legs
well supported by a chair. Each microdialysis probe was inserted after the
subject was given approximately 1 ml of 20 g.l-1 xylocaine via a 25-gauge
needle at the insertion site. An 18-gauge cannula was first passed through
the skin and fascia to make way for the probe. A second cannula containing
the microdialysis probe (CMA-60, CMA Microdialysis AB, Sweden) was then
pushed through the skin and fascia and orientated along the length of the
fibres of the vastus lateralis muscle. The cannula was removed leaving the
microdialysis probe within the muscle. After insertion of the probe, it was
secured with tape and the outlet cut at a maximal length of 10 mm from the
skin. The subjects recovered for 1.5 h after probe insertion before any
measurements were performed.
Perfusate The pH-sensitive fluorescent dye BCECF was coupled to dextran (molecular
mass cut off at 70000 Da), which prevented any diffusion of dye across the

Chapter 5 – Interstitial Alkalosis
83
probe membrane (cut off at a molecular mass of 20000 Da). The dye (0.1 mg
ml.l-1) was dissolved in a sterile saline solution (154 mmol.l-1 Na+). The
perfusate was then placed into a sterile 1 ml syringe equipped with a filter,
mounted in a microdialysis pump and connected to the inlet of the
microdialysis probe. The outlet from the probe was removed, replaced with a
stainless steel tube and connected to a micro flow-through cuvette (total
volume 8 µl) in a fluorescence spectrophotometer (Hitachi F-2000, Japan).
The pump rate was 5 µl.min-1 in all experiments. The time scales on the
figures were corrected for the delay due to the volume of tubing and cuvette.
Fluorometric measurements and determination of pH With the emission wavelength constant at 530 nm, the fluorescence
spectrophotometer continuously switched between the excitation wavelengths
of 440 and 500 nm with a bandpass of 10 nm. The excitation intensity at 440
nm was insensitive to pH, but dependent on the amount of dye, whereas the
excitation intensity at 500 nm was also sensitive to pH. Thus, the excitation
intensity ratio 500/440 was proportional to pH and independent of changes in
dye concentration and thereby insensitive to any water movements from or
into the probe. The temperature in the fluorescence spectrophotometer was
kept constant by circulating thermostatically controlled water. For calibration,
a microdialysis probe was placed in a beaker with magnetic stirring and
connected to a pump and the fluorometer. The beaker contained saline (154
mM Na-1) and bicarbonate (25 mM), and the pH was monitored with a
laboratory pH meter. The pH in the beaker was changed in a stepwise
manner by adding HCl/NaOH and the excitation ratio was recorded. A
calibration curve was obtained by plotting the excitation intensity ratio versus
external pH. The constants obtained from a linear regression to the
calibration curve were used to convert fluorescent signals obtained in human
experiments to interstitial pH.
Blood collection and analysis After initial weighing, each subject rested in a seated position for a period of
10-min. Subjects’ cephalic vein was then cannulated with a 23-gauge needle
(Becton Dickinson, Germany) and attached to a 3-way tap (Terumo,
Belgium). Five millilitres of venous blood was removed as discard and then a

Chapter 5 – Interstitial Alkalosis
84
2-ml venous sample was obtained. The sample was immediately analysed for
acid-base (pH, pCO2, HCO3-) and pO2 status. The sample remained on ice
before a duplicate measurement was performed. To maintain cannula
patency and plasma volume, an equivalent amount of 0.9 percent saline was
re-infused after each sample.
Ingestion The initiation of ingestion followed the resting measurements. The subjects
were required to ingest either 300 mg.kg-1 of tri-sodium citrate (Sigma
Chemicals - Na3C8H5O7.H2O) at a rate of 300 mg.min-1 or calcium carbonate
matched for the number of capsules. Subjects consumed the sodium citrate
in hand-filled ‘OO’ size gelatine capsules with water ad libitum. Each capsule
was weighed before and after being filled to determine the exact quantity of
sodium citrate contained within the capsule (mean 1200 mg.capsule-1). This
mass was divided by 300 to establish the timing for ingestion of each capsule.
After the ingestion process was completed, the subjects were encouraged to
drink water ad libitum across the duration of the experiment. The subjects
consumed no solid food during testing. The warm-up exercise intensity of 10
W was initiated 150 min after the start of ingestion. The order of ingestion
was randomised in a double-blind fashion.
Results Mean±SEM values for blood and interstitial pH, blood gases and bicarbonate at
rest (time 0), during (30-150 min) and after (151-196.4 min) ingestion of
placebo (CaCO3) and alkalosis (Na3C8H5O7) are shown in Table 2.
Interstitial pH Mean resting interstitial pH was 7.38±0.12 and 7.24±0.16 for placebo and
alkalosis, respectively. Sodium citrate ingestion had no alkalising effect on
interstitial pH. Intense exercise was associated with a decrease (p<0.05) in
placebo interstitial pH that commenced after 2 minutes of exercise (Figure
35). Interstitial pH continued to decline throughout the exercise bout and
peaked at three and two minutes after the cessation of exercise, for placebo
and alkalosis, respectively. The magnitude of change in interstitial pH from
rest was 0.59 and 0.29 pH units for placebo and alkalosis, respectively.

Chapter 5 – Interstitial Alkalosis
85
Placebo interstitial pH was not different from resting values within 7.5 minutes
of recovery.
Time
rest
ing
30in
g 60
ing
90in
g 12
0in
g 15
010
W 1
10 W
210
W 5
10 W
10
10 W
R 1
10 W
R 2
10 W
R 5
10 W
R 1
0ex
0.7
5ex
1.5
ex
2ex
3ex
4ex
5ex
hre
c 1
rec
2re
c 3
rec
4re
c 5
rec
7.5
rec
10re
c 15
Inte
rstit
ial p
H
0.0
6.6
6.7
6.8
6.9
7.0
7.1
7.2
7.3
7.4
7.5
7.6 Placebo Alkalosis
Figure 35 Interstitial pH temporal response
Mean±SEM interstitial pH temporal response for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O). There was no effect of alkalosis on interstitial pH. Intense exercise reduced placebo interstitial pH below (p<0.05) resting placebo values, marked *.
* * *
* * * * * *
*

Chapter 5 – Interstitial Alkalosis
86
Table 2 Blood acid-base and interstitial pH values with ingestion of CaCO3 (placebo) and Na3C8H5O7 (alkalosis)
pHb HCO3- pCO2 pO2 pHi
Time (min) Placebo
±SEM Alkalosis ±SEM
Placebo ±SEM
Alkalosis ±SEM
Placebo ±SEM
Alkalosis ±SEM
Placebo ±SEM
Alkalosis ±SEM
Placebo ±SEM
Alkalosis ±SEM
Pre-Ingestion 0.00 7.367±0.015 7.367±0.015 26.7±0.6 26.2±0.6 47.9±1.2 46.7±1.2 42.2±4.5 38.5±4.5 7.375±0.118 7.236±0.155
30.00 7.359±0.015 7.362±0.015 26.7±0.6 25.9±0.6 48.2±1.2 47.0±1.2 43.5±4.5 34.9±4.5 7.366±0.118 7.182±0.155 60.00 7.355±0.015 7.366±0.015 26.8±0.6 27.2±0.6 49.0±1.2 49.4±1.2 35.5±4.5 30.4±4.5 7.352±0.118 7.183±0.155 90.00 7.358±0.015 7.372±0.015 27.2±0.6 27.7±06 48.8±1.2 50.6±1.2 39.7±4.5 30.1±4.5 7.331±0.118 7.253±0.155 120.00 7.369±0.015 7.400±0.015 27.2±0.6 28.5±0.6 48.9±1.2 48.6±1.2 41.2±4.5 32.2±4.5 7.311±0.118 7.161±0.155
Ingestion
150.00 7.381±0.015 7.411±0.015 26.5±0.6 29.4±0.6*# 44.3±1.2 48.5±1.2 53.5±4.5 33.6±4.5 7.304±0.118 7.145±0.155
151.00 7.376±0.015 7.417±0.015 27.8±0.8 30.6±0.6*# 48.9±1.7 49.2±1.2 54.7±6.4 33.8±4.5 7.270±0.118 7.152±0.155 152.00 7.374±0.015 7.416±0.015 28.4±0.6 30.8±0.6*# 51.5±1.2 49.7±1.2 37.6±4.5 32.1±4.5 7.282±0.118 7.151±0.155 155.00 7.373±0.015 7.410±0.015 28.6±0.6 31.3±0.6*# 51.7±1.2 51.5±1.2 31.4±4.5 24.2±4.5 7.263±0.118 7.135±0.155
10 W Exercise
160.00 7.372±0.017 7.410±0.017 28.8±0.9 31.3±0.6*# 52.2±1.7 51.7±1.2 32.3±6.4 25.5±4.5 7.307±0.158 7.097±0.159
161.00 7.374±0.015 7.412±0.015 28.1±0.6 30.8±0.6*# 51.1±1.2 51.7±1.2 36.3±4.5 28.3±4.5 7.309±0.158 7.084±0.159 162.00 7.379±0.015 7.415±0.015 28.2±0.6 31.4±0.6*# 51.3±1.2 51.9±1.2 35.8±4.5 28.6±4.5 7.314±0.158 7.080±0.159 165.00 7.374±0.015 7.416±0.015 28.0±0.6 30.9±0.6*# 51.3±1.2 50.4±1.2 35.2±4.5 33.0±4.5 7.252±0.118 7.131±0.155 Recovery
170.00 7.375±0.015 7.418±0.015 28.2±0.6 31.5±0.6*# 50.8±1.2 51.1±1.2 35.9±4.5 30.9±4.5 7.250±0.118 7.124±0.155
170.75 7.379±0.015 7.417±0.015 28.5±0.6 31.1±0.6*# 50.5±1.2 50.6±1.2 40.5±4.5 31.5±4.5 7.248±0.154 7.180±0.118 171.50 7.380±0.015 7.419±0.015 28.4±0.6 31.3±0.6*# 50.3±1.2 50.7±1.2 42.6±4.5 335±4.5 7.246±0.118 7.170±0.118 172.00 7.372±0.015 7.413±0.015 28.4±0.6 31.6±0.6*# 51.1±1.2 51.8±1.2 37.2±4.5 29.6±4.5 6.955±0.118 7.154±0.118 173.00 7.365±0.015 7.406±0.015 27.9±0.6 31.2±0.6*# 50.4±1.2 52.0±1.2 36.9±4.5 29.5±4.5 6.913±0.118 7.123±0.118 174.00 7.368±0.017 7.397±0.017 28.0±0.6 31.0±0.6*# 51.6±1.2 51.6±1.2 30.7±4.5 27.1±4.5 6.875±0.118 7.091±0.118 175.00 7.355±0.017 7.399±0.017 27.5±0.6 30.5±0.6*# 52.1±1.2 51.1±1.2 30.0±4.5 29.0±4.5 6.828±0.118 7.054±0.118
Intense Exercise
181.4±0.9 7.344±0.017 7.382±0.024 25.4±0.9 28.4±0.9 50.3±1.8 49.0±1.8 35.1±6.6 24.0±6.9 6.794±0.118* 6.978±0.118*
182.40 7.341±0.015 7.394±0.015 22.0±0.6* 25.8±06*# 44.1±1.2 44.0±1.2 49.7±4.5 36.6±4.5 6.791±0.118* 6.969±0.118* 183.40 7.339±0.015 7.387±0.015 19.2±0.6* 22.6±0.6*# 38.8±1.2* 39.2±1.2* 69.6±4.5* 61.5±4.5* 6.793±0.118* 6.950±0.118* 184.40 7.334±0.015 7.380±0.017 18.3±0.6* 22.2±0.6*# 37.6±1.2* 39.0±1.2* 78.2±4.5* 64.8±4.6* 6.787±0.118* 6.956±0.118* 185.40 7.334±0.015 7.378±0.017 19.0±0.6* 22.3±0.8*# 39.4±1.2* 38.2±1.7* 61.0±4.5* 70.5±6.4* 6.800±0.118 7.016±0.155 186.40 7.339±0.015 7.377±0.017 18.6±0.6* 22.6±0.6*# 38.8±1.2* 39.9±1.2* 65.6±4.5* 62.4±4.5* 6.799±0.118* 7.007±0.118* 188.90 7.341±0.017 7.388±0.017 19.1±0.6* 23.1±0.6*# 39.1±1.2* 39.8±1.2* 62.0±4.5* 59.5±4.5* 7.023±0.154 7.074±0.118 191.40 7.350±0.017 7.404±0.017 19.6±0.6* 22.8±0.6*# 39.1±1.2* 37.3±1.2* 62.1±4.5* 73.0±4.5* 7.080±0.154 7.128±0.118
Recovery
196.40 7.368±0.017 7.409±0.017 21.2±0.6* 25.3±0.6*# 40.3±1.2* 41.4±1.2* 53.1±4.5 48.6±4.5 7.118±0.154 7.177±0.118
Blood acid-base and interstitial pH changes before (time 0), during (30–150 min) and after (170–196.4 min) ingestion of CaCO3 and Na3C8H5O7. Values are mean±SEM; n=5. HCO3
- concentrations are in mmol.l-1, pCO2 and pO2 concentrations are in mmHg. * significantly different from time 0, p<0.05; # significantly different from Na3C8H5O7, p<0.05.

Chapter 5 – Interstitial Alkalosis
87
Venous pH and HCO3-
Mean venous pH was 7.362±0.003 and 7.398±0.003 for placebo and alkalosis,
respectively. Sodium citrate ingestion (300 mg.kg-1) was not associated with
a significant elevation in venous blood pH (p=0.19) above placebo (Figure
36). Although the desired statistical power was 0.8, the mean effect size in
combination with a subject pool of five resulted in a calculated statistical
power of 0.18. Nevertheless, inspection of Figure 37 does show an upward
trend in the blood pH response after ingestion of Na3C8H5O7. An exercise-
induced decrease in venous pH was identified (p=0.07) in the placebo trial,
however, this was not evident in the alkalosis trial (Figure 37)
Conditionplacebo alkalosis
Ven
ous
pH
0.00
7.30
7.32
7.34
7.36
7.38
7.40
7.42
7.44
Figure 36 Overall effect of sodium citrate ingestion on venous pH
Mean±SEM venous pH response for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O).

Chapter 5 – Interstitial Alkalosis
88
Time
rest
ing
30in
g 60
ing
90in
g 12
0in
g 15
010
W 1
10 W
210
W 5
10 W
10
10 W
R 1
10 W
R 2
10 W
R 5
10 W
R 1
0ex
0.7
5ex
1.5
ex
2ex
3ex
4ex
5ex
hre
c 1
rec
2re
c 3
rec
4re
c 5
rec
7.5
rec
10re
c 15
Veno
us p
H
0.00
7.30
7.32
7.34
7.36
7.38
7.40
7.42
7.44Placebo Alkalosis
Figure 37 Venous pH temporal response
Mean±SEM blood pH temporal response for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O).
Mean venous [HCO3-] was 25.5±0.2 and 28.1±0.2 for placebo and alkalosis,
respectively (Figure 38). Ingestion of 300 mg.kg-1 sodium citrate elevated
(p<0.05) venous [HCO3-] above placebo after 120 min of ingestion (Figure
39). The elevated [HCO3-] continued to be present for the remainder of the
experiment. Venous [HCO3-] was reduced (p<0.05) below resting values after
5 minutes of intense exercise in both conditions where it continued to
exhaustion. A further reduction in venous [HCO3-] was observed during
recovery that peaked at the third minute in both conditions. The recovery
period (15 minutes) was of insufficient length for [HCO3-] to return to resting
values in both conditions.

Chapter 5 – Interstitial Alkalosis
89
Conditionplacebo alkalosis
Ven
ous
[HC
O3- ] (
mm
ol.l-1
)
0.0
25.0
25.5
26.0
26.5
27.0
27.5
28.0
28.5
29.0
Figure 38 Overall effect of sodium citrate ingestion on venous [HCO3-]
Mean±SEM venous [HCO3-] response for both conditions, placebo (CaCO3)
and alkalosis (Na3C8H5O7). Sodium citrate ingestion increased (p<0.05) venous [HCO3
-] above placebo, marked *.
Time
rest
ing
30in
g 60
ing
90in
g 12
0in
g 15
010
W 1
10 W
210
W 5
10 W
10
10 W
R 1
10 W
R 2
10 W
R 5
10 W
R 1
0ex
0.7
5ex
1.5
ex
2ex
3ex
4ex
5ex
hre
c 1
rec
2re
c 3
rec
4re
c 5
rec
7.5
rec
10re
c 15
Veno
us [H
CO
3- ] (m
mol
.l-1)
0
16
18
20
22
24
26
28
30
32
34Placebo Alkalosis
Figure 39 Venous HCO3- temporal response
Mean±SEM venous [HCO3-] for both conditions, placebo (CaCO3) and
alkalosis (Na3C8H5O7.H2O) across time. Sodium citrate ingestion significantly elevated (p<0.05) venous [HCO3
-] above placebo after 120 min, marked *. This observation continued for the remainder of the experiment. After 5 min of intense exercise venous [HCO3-] was significantly reduced below rest values (p<0.05), marked #, and continued during exercise and recovery.
# # # # # #
#
* * * * * *
* * * * * * * * *
*
*
* * * * * *
*
*

Chapter 5 – Interstitial Alkalosis
90
Venous blood gases pO2 and pCO2 Mean venous [pO2] was 45.2±2.3 and 38.5±2.3 for placebo and alkalosis,
respectively (Figure 40).
Condition
placebo alkalosis
Ven
ous
[pO
2] (m
mH
g)
0
10
20
30
40
50
60
70
80
90
Figure 40 Venous pO2 status for both conditions placebo and alkalosis
Mean±SEM venous [pO2] for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O). Outlier [pO2] are marked . Venous [pO2] was not different between conditions.
Time
rest
ing
30in
g 60
ing
90in
g 12
0in
g 15
010
W 1
10 W
210
W 5
10 W
10
10 W
R 1
10 W
R 2
10 W
R 5
10 W
R 1
0ex
0.7
5ex
1.5
ex
2ex
3ex
4ex
5ex
hre
c 1
rec
2re
c 3
rec
4re
c 5
rec
7.5
rec
10re
c 15
Ven
ous
[pO
2] (m
mH
g)
0
18
27
36
45
54
63
72
81
Placebo Alkalosis
Figure 41 Venous pO2 temporal response
Mean±SEM venous pO2 response for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O) across time. Sodium citrate ingestion had no effect on venous [pO2], however, recovery from intense exercise was associated with an increase (p<0.05) in [pO2] across both conditions, marked *.
*
* *
* *
*

Chapter 5 – Interstitial Alkalosis
91
There was no effect of alkalosis on venous [pO2] collected from the forearm,
but there was a significant time-effect present during recovery from intense
exercise (p<0.05). Venous [pO2] was elevated above rest, ingestion and light
exercise during intense exercise recovery from 2 to 10 minutes (Figure 41).
Mean venous [pCO2] was 47.2±0.6 and 47.3±0.6 for placebo and alkalosis,
respectively. Alkalosis had no effect on forearm venous [pCO2]. However,
there was a significant (p<0.05) time effect present during recovery (Figure
42). Intense exercise was associated with a decreased venous [pCO2] from
rest (47.3±0.9 mmHg) and peaked after 10 minutes of recovery (38.2±0.9
mmHg).
Time
rest
ing
30in
g 60
ing
90in
g 12
0in
g 15
010
W 1
10 W
210
W 5
10 W
10
10 W
R 1
10 W
R 2
10 W
R 5
10 W
R 1
0ex
0.7
5ex
1.5
ex
2ex
3ex
4ex
5ex
hre
c 1
rec
2re
c 3
rec
4re
c 5
rec
7.5
rec
10re
c 15
Veno
us [p
CO
2] (m
mH
g)
0
36
39
42
45
48
51
54Placebo Alkalosis
Figure 42 Venous pCO2 temporal response
Mean±SEM venous pCO2 response for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O) across time. The ingestion of sodium citrate (300 mg.kg-1) had no influence on [pCO2], however, recovery from intense exercise was associated with a decrease (p<0.05) in [pCO2] below rest values, marked *.
Time to exhaustion The mean time to exhaustion was 352 and 415 seconds for placebo and
alkalosis, respectively (Figure 43). Ingesting 300 mg.kg-1 of sodium citrate
was not associated with an increased time to exhaustion during knee-extensor
*
*
* * *
* * *

Chapter 5 – Interstitial Alkalosis
92
exercise. Table 3 shows the individual exhaustion times for both conditions.
The individual responses were considerably different between the subjects
ranging from a decrease of 17 percent to an improvement of 63 percent in
exercise time.
Subject Placebo Alkalosis Percent Change 1 390 394 1 2 230 190 -17 3 375 400 7 4 357 422 18 5 410 670 63
Mean±SEM 352±71 415±171 14
Table 3 Individual exhaustion times for intense knee-extensor exercise
Individual subject exhaustion times for both conditions, placebo (CaCO3) and alkalosis (Na3C8H5O7.H2O). Note the large variation in percent change, range –17 to 63 percent. Alkalosis did not improve exhaustion time.
Time to exhaustion
Condition
placebo alkalosis
Tim
e (s
ec)
0
300
325
350
375
400
425
450
475
500
Figure 43 Time to exhaustion for both placebo and alkalosis conditions
Mean±SEM exhaustion times for each condition, placebo and alkalosis. Sodium citrate ingestion (300 mg.kg-1) had no influence on exhaustion time.

Chapter 5 – Interstitial Alkalosis
93
Discussion This is the first study to investigate the effect of alkalosis, using sodium
citrate ingestion, on interstitial pH at rest and during exercise. The results of
the current study refute the hypothesis that sodium citrate ingestion improves
knee-extensor exercise performance in healthy individuals. The second
hypothesis that sodium citrate ingestion would increase interstitial pH was
also refuted by these findings.
Mean±SEM resting interstitial pH for all experiments was 7.37±0.01. This is
similar to that reported in the previous study in Chapter 3 (7.38±0.02 pH
units) and falls between venous pH values reported in the literature (7.37-
7.43) (Bangsbo et al., 2000; Sjogaard et al., 1985). In contrast, the
interstitial pH values from the current study are higher than those reported by
Maclean et al. (2000). In their study, dialysate pH was measured using pH
electrodes placed in the tubing on the outlet side of a microdialysis probe
during static exercise, resting dialysate pH was reported as 7.162±0.023.
Together, these studies form the collective sum of research that has
investigated interstitial pH during exercise in humans. Based on such limited
data, it is difficult to provide explanations of the differences observed between
investigations. However, there were important methodological differences
between these studies, which may provide some explanation. The first key
difference between the work of Maclean et al. (2000) was the removal of the
polyurethane outlet tubing and replacing it with stainless steel tubing. By
doing this, CO2 loss from the outlet side was prevented thereby controlling
any CO2 artefact on the measurement of dialysate pH. Secondly, and as
identified in Chapter 3, the addition of 25 mmol.l-1 HCO3- to the perfusate
without pH adjustment proved crucial in accurately determining interstitial pH
at rest and during exercise. However, to fully appreciate the relative
contributions these two factors have on the measurement of dialysate pH,
subsequent investigations need to be designed with these aims specifically in
mind.
Ingestion of sodium citrate (300 mg.kg-1) had no effect on blood pH at rest.
The mean±SEM venous blood pH response depicted in Figure 36 showed an
increase of 0.036 pH units. The magnitude of this response is lower than
previously demonstrated in Chapter 4 (0.052 pH units). The combination of
the lower response with a smaller sample size (n=5) may explain why

Chapter 5 – Interstitial Alkalosis
94
statistical significance was not achieved. Using these results the sample size
required to obtain significance at the 0.05 level was calculate at 12. The
smaller effects found in the current study are probably explained by the
method of blood collection. Venous samples were collected in the current
study while arterialised samples were obtained in the former. Resting venous
pH was 7.367±0.015 while resting arterialised pH was 7.397±0.003. These
differences can be explained by a larger [pCO2] in venous (47.3±1.2)
compared to arterialised (44.7±0.4) blood. Therefore, it is possible that the
reduced change in venous pH observed in the current study was being
partially obscured by the type of sampling and thus may be disguising the
sodium citrate effect on pH. Inspection of the data reported in the literature
revealed a large disparity of results. (McNaughton, 1990) reported mean
resting arterialised capillary venous pH values of approximately 7.15, in
contrast (Parry-Billings & MacLaren, 1986) reported mean resting capillary
venous pH values of approximately 7.41. These data in combination with the
varied ingestion rates, doses and blood sampling methods make it near
impossible to provide valid comparisons with the current data.
Sodium citrate ingestion failed to induce alkalosis within the interstitium at
rest. Mean±SEM interstitial pH was 7.304±0.118 and 7.145±0.155 for placebo
and alkalosis, respectively. The physicochemical approach to acid-base
control suggests, H+ and HCO3- are influenced by concentrations of pCO2,
weak and strong (fully dissociated) electrolytes (Stewart, 1983). Strong
electrolytes are represented by the strong ion difference (SID), which is the
difference between the sum of strong anions and cations (SID = ∑[strong
cations] - ∑[strong anions]) within the compartment. The major strong
electrolytes contributing to [SID+] in plasma are Na+, K+, Ca2+, Mg2+, Cl-,
SO42- and La-. In muscle the addition of PCr2- to the calculation is required
(Kowalchuk & Scheuermann, 1995). Presently, it is not possible to determine
all of these ion concentrations within the interstitial fluid using microdialysis or
any other techniques at rest and during exercise. Therefore, to explain the
findings of this study via this theory would be purely speculative.
Furthermore, attempting to make calculations based on this theory without all
of ion concentrations can lead to incorrect conclusions. Even ions in small
concentrations, such as Mg2+, can affect the final SID concentration and SID
has the largest effect on [H+] (Roger Fedde & Pieschl, 1995). If ions removed
from the calculation are in similar concentrations and of opposite polarity, the

Chapter 5 – Interstitial Alkalosis
95
error can be almost cancelled. Nevertheless, accuracy is compromised (Roger
Fedde & Pieschl, 1995). Therefore, it is beyond the realm of this investigation
to attempt to explain the results using the Stewart approach.
The metabolism of sodium citrate is not very well understood (Potteiger et al.,
1996b), however, it has been suggested that HCO3- is produced via its hepatic
oxidation and then added to the plasma (Halperin, 1982). Increasing plasma
[HCO3-] will reduce [H+] or increase pH via the Hendersen-Hasselbach
relationship. Therefore, it is reasonable to assume that this relationship
applies when inducing alkalosis via sodium citrate. Fluid compartments of the
body must obey the laws of electrical neutrality and conservation of mass
(Stewart, 1983). Blood and interstitial fluid are approximately osmotically
and electrically the same. However, since the interstitial fluid is protein free,
the ionic compositions differ somewhat between the two compartments
(Kowalchuk & Scheuermann, 1995). In particular, interstitial fluid has a
higher [Cl-], lower [Na+], [K+] and [SID] (Kowalchuk & Scheuermann, 1995).
The increased [HCO3-] will create a positive gradient between plasma and
interstitium, and since HCO3- can diffuse across the capillary wall, it should
theoretically lead to an increase in interstitial [HCO3-] until equilibrium is
attained. Currently, it is not possible to measure this during exercise in
humans. However, if HCO3- diffuses into the interstitium, it would decrease
[H+] and should thus be represented by a lowered pH. This was not
demonstrated in the current study. One possible explanation for this may be
linked to the HCO3- driving force between the plasma and interstitium.
Sodium citrate ingestion increased plasma [HCO3-] from 26.2 mmol.l-1 to
approximately 31.0 mmol.l-1. Since interstitial [HCO3-] is approximately 25
mmol.l-1 at rest (Geers & Gros, 2000), it may be that this gradient is
insufficient to induce movement into the interstitium. Even so, during intense
exercise (when efflux of H+ from the muscle cell to interstitium is high
(Pilegaard et al., 1999; Bangsbo et al., 1997; Bangsbo et al., 1993a) and
HCO3- is in buffering demand), both the electrical and concentration forces are
increased drawing HCO3- out of the plasma and into the interstitium. The
additional [HCO3-] could potentially buffer more H+, thereby delaying any
increase in [H+] or decrease in interstitial pH. This may explain the lack of an
exercise-induced acidosis observed during the alkalosis exercise period.

Chapter 5 – Interstitial Alkalosis
96
Another possible explanation could be related to both the Na+/H+ and HCO3-
/Cl- exchangers. These exchangers are approximately 20 percent responsible
for pH regulation at rest in skeletal muscle, but very little is known about their
degree of involvement during exercise (Juel, 1998a). One possibility, is that
under conditions of alkalosis these exchangers are upregulated due to
changes in their respective interstitial ionic components. It has been
suggested that alkalosis may be mediated via an increase in blood [Na+]
(Lindinger et al., 2000). This increased [Na+] may increase interstitial [Na+]
that may upregulate the Na+/H+ exchanger. Similarly, the increase in blood
[HCO3-] may lead to increases in interstitial [HCO3
-], which may have an
upregulatory effect on the HCO3-/Cl- exchanger. Although the data from the
current study does not indirectly support this change in interstitial [HCO3-],
via no change in interstitial pH, another electro-neutral bicarbonate exchanger
identified from animal studies may play a role (Putnam et al., 1986b).
However, very little is known about this exchangers function or importance.
New techniques need to be developed to quantify these ionic concentrations
and exchanger properties to increase the understanding of the function,
capacity and importance of these systems.
The current study did not support the hypothesis that ingestion of sodium
citrate (300 mg.kg-1) results in ergogenesis during intense knee-extensor
exercise. The mean±SEM time to exhaustion was 352±71 and 415±171
seconds for placebo and alkalosis, respectively. While this is consistent with
the findings of several others (Tiryaki & Atterbom, 1995; Ibanez et al., 1995;
Cox & Jenkins, 1994; Kowalchuk et al., 1989; Parry-Billings & MacLaren,
1986), it is worth noting the individual results as depicted in Table 3. The
mean increase in performance was 14 percent which was in contrast to the
findings of Spriet et al. (1991b), where they found only a modest 0.3 percent
mean effect. The range of percent change in performance was much larger
than anticipated (-17 to 63%). This, in itself, is probably the main reason for
the lack of statistical support for a overall ergogenic effect. To statistically
show an ergogenic effect of sodium citrate ingestion with the current
performance results a subject pool of 46 would be required. Even so, it is
difficult to overlook the large 18 and 63 percent improvement in performance
in two of the five subjects. Although it is beyond the scope of this
investigation to attempt to identify any characteristics that may separate

Chapter 5 – Interstitial Alkalosis
97
these two subjects from the rest, the next logical step would be to establish
the reasons for these individuals’ unique response.
Conclusion In conclusion, this is the first study to investigate the effects of alkalosis on
interstitial pH. The study demonstrated that sodium citrate ingestion (300
mg.kg-1) does not induce interstitial alkalosis, nor does it improve exhaustive
short-term knee-extensor performance. However, the results do suggest that
metabolic alkalosis is associated with an improved interstitial pH regulation,
as demonstrated by the lack of exercise-induced acidosis. Finally, future
research is required to investigate the mechanisms through which this
improved pH regulation may be mediated.


Chapter 6 – General Discussion
99
CH A P T E R 6 GE N E R A L D I S C U S S I O N
Introduction The previous individual discussions have focussed more or less exclusively on
the results and problems of the respective chapters. In contrast, this chapter
focuses on the experimental chapters as a whole in accordance with the
central research problem/s as defined in the preface and general introduction.
Summing up, the experiments contained in this thesis were designed to 1)
develop a new method to determine interstitial pH at rest and during exercise
in vivo, 2) discover a more effective pH-manipulating tool via the
identification of an optimal regime of sodium citrate ingestion, and finally, 3)
to combine the results of the above-mentioned experiments in an attempt to
add to the limited existing knowledge on interstitial pH. The central research
question of this thesis was thus to establish a technique for the manipulation
and detection of interstitial pH. As such, this is the focus of the discussion in
this chapter.
The importance of effective pH manipulation A key component or consideration when attempting to manipulate pH via
orally ingested substances is to prevent any negative side-effects. There
have been several studies that have reported symptoms of nausea and/or
vomiting after the ingestion of sodium bicarbonate (McNaughton & Cedaro,
1992; Goldfinch et al., 1988; Wilkes et al., 1983) or sodium citrate (Shave et
al., 2001; Potteiger et al., 1996a) in doses ranging from 300-500 mg.kg-1.
Although there have been investigations to the contrary where none of these
symptoms were evident (McNaughton, 1992a; Bouissou et al., 1988; Parry-
Billings & MacLaren, 1986), it would be logical to develop a regime that
minimises any potential risk of discomfort. Furthermore, in developing such a
regime, an important factor to obtain is the maximum benefit from the
substance introduced. Chapter 4 was designed to accommodate these two
criteria; through systematic investigation, an attempt was made to identify an
optimal ingestion regime for 300 mg.kg-1 sodium citrate.
Chapter 4 showed that ingestion of 300 mg.kg-1 SC was not associated with
nausea or vomiting independent of the four ingestion rates examined. The

Chapter 6 – General Discussion
100
maximum blood alkalosis observed was not associated with the bolus
ingestion regime most commonly used by researchers (Ibanez et al., 1995;
McNaughton & Cedaro, 1991). Of the three capsular ingestion rates
investigated, 300 mg.min-1 at the above-mentioned dose of SC was
associated with the greatest blood alkalosis. Since the method of orally
inducing alkalosis involves the GI system, it stands that to obtain maximum
absorption the ingestant should match (as closely as possible) the physical
capabilities of the GI system. This is not the case with the bolus ingestion
regime, and as such it is not surprising that the effect is less than that of the
capsular regimes. In addition to the way in which the alkali is consumed, and
important to the magnitude of effect, is the absorption time. Chapter 4 was
the first study to perform serial measurements of the effect of SC ingestion on
blood pH across 8 hours. This unique component of the study allowed for the
determination of the time it would take to reach the maximum alkalotic effect.
Some researchers have used an ingestion period of 90 minutes (Cox &
Jenkins, 1994), while others have suggested up to 3 h are required for
maximum benefits (Heigenhauser & Jones, 1991). In fact, Chapter 4 showed
that only a partial (75-80%) alkalosis was achieved 1.5 h post-ingestion, and
that a 6 h ingestion period was required to reach peak alkalosis. In contrast,
the 300 mg.min-1 rate reduced this period to 3.5 h.
The importance of interstitial pH Although little is known about the role of interstitial pH during exercise, it has
been suggested that it may be involved in the regulation of local blood flow
(Quayle et al., 1997). Furthermore, it has been suggested that interstitial pH
may affect the sensory response from muscle. This suggestion is drawn from
the findings of Victor et al. (1998), linking interstitial pH to sympathetic nerve
activity. In order to support these suggestions, it is necessary to quantify
changes within the interstitium. There are methods available to measure [H+]
in muscle and blood, however, due to technical difficulties, this had not been
the case for interstitial [H+]. Thus, until a method was successfully developed
to this end, no investigations could be performed to elucidate changes in
interstitial pH within skeletal muscle in vivo. Chapter 3 describes the
development of such a method. Furthermore, the results from this chapter
refute the suggestion that an interstitial alkalosis is present during exercise
(Maclean et al., 2000). Finally, using this method, interstitial pH was

Chapter 6 – General Discussion
101
successfully measured for the first time. The data from Chapter 3 supports
the contention that interstitial pH is involved in, but not solely responsible for,
the regulation of blood flow. The data revealed a second positive relationship
supporting interstitial pH’s involvement in the regulation of blood flow: the
first being between blood flow and power output (Radegran & Saltin, 1998),
and the second being between interstitial acidification and power output. In
addition, the data also revealed that interstitial pH is not the sole determinant
of blood flow. In support for this is the dissociation found between blood flow
and interstitial pH changes. Specifically, in chapter 3, interstitial pH
continually declined during five-minute knee-extensor exercise. In contrast,
Radegran & Saltin (1998) have shown that blood flow reaches a steady state
after approximately 1.5 minutes.
Using the method developed in Chapter 3 and the optimal ingestion regime
established in Chapter 4, Chapter 5 examined the manipulative potential of
sodium citrate on the interstitium at rest and during exercise. It was
expected that SC would be associated with an interstitial alkalosis at rest,
however the data from Chapter 5 does not support this. Two previous
investigations have postulated two distinctly different suggestions as to the
link between SC metabolism and an increase in plasma [HCO3-] (Kowalchuk et
al., 1989; Halperin, 1982). Nevertheless, the end result of increased [HCO3-]
is the same, which was further supported by the data in Chapter 5: both
plasma and interstitium are osmotically and electrically similar and therefore
the increase of a solute in plasma should result in an increased interstitial
concentration. It is reasonable to assume that if extra bicarbonate did move
into the interstitium, an increase in pH would occur similar to that found in
the blood. However, the data in Chapter 5 does once again not support this.
There appears to be no evidence to explain why the extra bicarbonate does
not equilibrate between the plasma and interstitium. One possible
explanation may lie within the equilibration driving force: SC ingestion
increased blood [HCO3-] from 26.2-31.0 mmol.l-1. In accordance, it has been
suggested that interstitial [HCO3-] is approximately 25 mmol.l-1 (Geers &
Gros, 2000), which may be insufficient to induce movement into the
interstitium.
Although there was no interstitial alkalosis induced prior to exercise, the data
from Chapter 5 suggests an improved pH regulation during exercise.

Chapter 6 – General Discussion
102
Evidence for this is the lack of an exercise-induced acidosis after the ingestion
of SC. This was an unexpected finding as alkali ingestion induces an alkalosis
(Chapter 4) followed by an exercise-induced acidosis blood response. It was
thought that a similar process would occur in the interstitium when, in fact,
there was no alkalosis followed by acidosis. This is an important finding as it
demonstrates that the two extracellular compartments perform differently.
Therefore, the data presented in Chapter 5 indicates that, where possible, the
two extracellular compartments should be treated as separate entities.
Limitations A major limitation in the measurement of interstitial pH using microdialysis
and BCECF is the demand on equipment. A fluorometer is required for each
probe within the thigh, which in a typical laboratory would limit the use to one
probe. An inherent problem with detecting interstitial pH via the use of only
one probe is the uncertainty with which it represents the whole muscle
interstitium. An additional disadvantage of using only one probe is that if is it
broken during intense contractions, it is impossible to perform accurate
determination of the calibration coefficients and thus a second separate probe
must be used. Further, to quantify the contribution of interstitial pH to
skeletal muscle function, other interstitial metabolites need to be measured.
These were omitted from the current investigations as no methods have been
established for the measurement of the interstitial ions, HCO3-, Ca2+, Mg2+,
and Cl-. When calculating the osmolalities of the different ingestion rates
(Chapter 4), the amount of water consumed with each capsule was not
measured, which may have influenced the results.

Chapter 7 – Conclusions and Future Research
103
CH A P T E R 7 CO N C L U S I O N S A N D F U T U R E
R E S E A R C H
Conclusions Through three collective original investigations, the present thesis has
demonstrated that interstitial pH can be accurately determined during
exercise in humans using microdialysis and the pH-sensitive dye BCECF. The
main advantage of this method is that data can be collected in real-time with
high resolution (10 Hz). The ability to generate data that accurately describes
short-term high intensity exercise where pH regulation is greatly challenged is
of the utmost scientific importance. When applying this newly developed
method, the examination of 5 min intense exercise revealed an exercise-
induced acidosis that was positively correlated with power output and greater
than a concomitant venous acidosis.
The second of the present investigations was designed to establish an optimal
protocol for the ingestion of an alkali (sodium citrate) to maximise the
disturbance to blood pH. This study demonstrated that consumption of an
alkali is an important factor to consider when attempting to maximise blood
alkalosis. In particular, the slowest ingestion rate examined, 300 mg.min-1,
was associated with the greatest change in blood pH from resting values.
This finding is particularly important for the applied setting, where induced
alkalosis has been shown to improve human performance. Although the exact
mechanistic link between alkalosis and ergogenesis has not been elucidated, it
appears that the ensuing alkalosis is in some way responsible. Therefore, a
maximisation of the alkalosis would probably serve to improve previously
observed effects on performance. Furthermore, inducing alkalosis can be a
powerful tool for exploring physiological phenomena potentially mediated via
acid-base changes.
The final study was designed to broaden the collective knowledge pertaining
to pH regulation by combining and applying the knowledge from the previous
two investigations. Specifically, this study explored the possibility of inducing
an interstitial alkalosis via ingestion of sodium citrate. Although this was not
achieved, it was demonstrated that sodium citrate ingestion was not

Chapter 7 – Conclusions and Future Research
104
associated with an exercise-induced acidosis during intense knee-extensor
activity. This finding suggests that pH regulation is improved during exercise.
Future Research Although there has been an abundance of research investigating the effects of
alkali ingestion on human performance (Pfefferle & Wilkinson, 1988;
Robertson et al., 1987; McKenzie et al., 1986; Katz et al., 1984; McCartney et
al., 1983), the same level of interest has not been present for the metabolism
of alkalis. In particular, the exact mechanisms underlying the movement of
SC from the GI tract through to the observation of an alkalotic effect in the
blood have not been systematically explored. Two theories have been formed
to explain the association between blood alkalosis and SC ingestion: the
hepatic oxidation of citrate (Halperin, 1982) and an increase in [SID] as a
result of increased [citrate-] (Kowalchuk et al., 1989). Recently, Lindinger et
al. (1999) investigated the plasma and muscle ionic movements associated
with the ingestion of sodium and potassium bicarbonate. Central to their
findings were the contributions of sodium and potassium movements to the
corresponding alkaloses. From the data collected in Chapter 3, SC ingestion
at a rate of 300 mg.min-1 was associated with similar increases in sodium
concentration observed by Lindinger et al. (1999) in the SB condition. Due to
the disparity of the above-mentioned investigations, any conclusions
regarding the exact mechanisms of alkalosis would be pre-emptive. It is still
unknown to what degree each of these are responsible for the effect of
alkalosis, or if there is any degree of interaction between them. Thus new
studies need to be designed to quantify the contributions of each of these
mechanisms.
It has been suggested that alkalosis induced via the ingestion of SB is
mediated by decreases in extracellular [K+]. It was further suggested that
this decrease is brought about via an increased intracellular [Na+] activated
Na+-K+-ATPase activity (Lindinger et al., 1999; Clausen, 1986). The venous
data in Chapter 3 demonstrated an increased blood [Na+] when ingesting SC
at 300 mg.min-1, which may, in turn, support a similar mechanism of action to
SB when using SC. In order to support or refute these hypotheses, however,
corresponding muscle, interstitial and blood data are required. Accordingly,
to clarify the effect of alkalosis on potassium regulation, it is necessary to

Chapter 7 – Conclusions and Future Research
105
perform complex and invasive experiments capable of obtaining the required
data.
The results of Chapter 4 have demonstrated that ingesting sodium citrate at
300 mg.min-1 has a greater effect on blood ionic status at rest. To examine if
this greater ionic effect translates to a greater effect on performance, new
studies can now be designed incorporating this ingestion regime and test its
effect on whole body performance. These studies would provide valuable
information for the coach and athlete in the applied setting by ascertaining
the value of this protocol to their needs. Further, Chapter 4 identified that the
popular bolus regime in combination with a 1.5 h ingestion time resulted in a
partial blood alkalosis. At present, it is unknown what performance effect can
be gained from the additional alkalosis obtained by an increased ingestion
time. It seems reasonable to assume that a greater alkalosis would result in
greater performance gains, requiring the longer ingestion time. Associated
with a longer ingestion time in the applied setting is the possible effect of food
ingestion during this time. It seems plausible that the ingestion of food
during ingestion may alter or interfere with the effects of induced-alkalosis.
There have been no investigations into these possibilities, such investigations
would provide further clarification on the efficacy of sodium citrate ingestion
in the applied setting.
As previously mentioned, there has been limited research performed on
skeletal muscle interstitium during exercise. This is largely due to technical
difficulties in developing reliable methods for the accurate detection of
candidates thought to be involved in regulatory processes. As a result little is
known about the role of the interstitium in muscle cell function. There is
evidence to suggest that interstitial pH may be involved in the regulation of
blood flow (Quayle et al., 1997; Davies, 1990). Data from Chapter 5
demonstrated that sodium citrate ingestion was associated with the lack of an
exercise-induced acidosis. Although there was no performance effect of
alkalosis, the data shows that a similar amount of muscular work was
performed without a significant disturbance to interstitial pH, suggesting an
improved interstitial pH regulation during exercise. It is beyond the scope of
these investigations to elaborate on the mechanisms behind this. However,
using the interstitial pH technique developed as part of this thesis in
combination with thermodilution techniques for the determination of blood

Chapter 7 – Conclusions and Future Research
106
flow, it is now possible to perform an investigation that can determine if
interstitial pH is involved in the local regulation of blood flow during exercise
in humans.

References
107
RE F E R E N C E S
1. AALKJAER, C. & PENG, H.L. (1997). pH and smooth muscle. Acta Physiol.Scand. 161, 557-566.
2. AICKIN, C.C. & THOMAS, R.C. (1977). An investigation of the ionic mechanism of intracellular pH regulation in mouse soleus muscle fibres. J.Physiol. 273, 295-316.
3. ALLSOP, P., CHEETHAM, M., BROOKS, S., HALL, G.M. & WILLIAMS, C. (1990). Continuous intramuscular pH measurement during the recovery from brief, maximal exercise in man. Eur.J.Appl.Physiol.Occup.Physiol. 59, 465-470.
4. ARNOLD, D.L., TAYLOR, D.J. & RADDA, G.K. (1985). Investigation of human mitochondrial myopathies by phosphorus magnetic resonance spectroscopy. Ann.Neurol. 18, 189-196.
5. AUKLAND, K. & REED, R.K. (1993). Interstitial-lymphatic mechanisms in the control of extracellular fluid volume. Physiol.Rev. 73, 1-78.
6. BALL, D. & MAUGHAN, R.J. (1997). The effect of sodium citrate ingestion on the metabolic response to intense exercise following diet manipulation in man. Exp.Physiol. 82, 1041-1056.
7. BANGSBO, J., GOLLNICK, P.D., GRAHAM, T.E., JUEL, C., KIENS, B., MIZUNO, M. & SALTIN, B. (1990). Anaerobic energy production and O2 deficit-debt relationship during exhaustive exercise in humans. J.Physiol. 422, 539-559.
8. BANGSBO, J., JOHANSEN, L., GRAHAM, T. & SALTIN, B. (1993a). Lactate and H+ effluxes from human skeletal muscles during intense, dynamic exercise. J.Physiol. 462, 115-133.
9. BANGSBO, J., JOHANSEN, L., QUISTORFF, B. & SALTIN, B. (1993b). NMR and analytic biochemical evaluation of CrP and nucleotides in the human calf during muscle contraction. J.Appl.Physiol. 74, 2034-2039.
10. BANGSBO, J., JUEL, C., HELLSTEN, Y. & SALTIN, B. (1997). Dissociation between lactate and proton exchange in muscle during intense exercise in man. J.Physiol. 504, 489-499.
11. BANGSBO, J., KRUSTRUP, P., GONZALEZ-ALONSO, J., BOUSHEL, R. & SALTIN, B. (2000). Muscle oxygen kinetics at onset of intense dynamic exercise in humans. Am.J.Physiol.Regul.Integr.Comp.Physiol. 279, R899-R906

References
108
12. BANGSBO, J., MADSEN, K., KIENS, B. & RICHTER, E.A. (1996). Effect of muscle acidity on muscle metabolism and fatigue during intense exercise in man. J.Physiol. 495 , 587-596.
13. BELANGERO, V.M.S. & COLLARES, E.F. (1992). Gastric emptying and metabolic acidosis. II - Gastric retention of a sodium bicarbonate solution utilizing and experimental model in rats. Arq Gastoenterol 29(1), 23-27.
14. BIGLAND-RITCHIE, B., DONOVAN, F. & ROUSSOS, C.S. (1981). Conduction velocity and EMG power spectrum changes in fatigue of sustained maximal efforts. J.Appl.Physiol 51, 1300-1305.
15. BINDER, H.J., RANJENDRAN, V.M., & GIEBEL, J.P. (2000). Cl-dependent Na-H exchange. A novel colonic crypt transport mechanism. Ann. N.Y. Acad. Sci. 915, 43-53.
16. BIRD, S.R., WILES, J. & ROBBINS, J. (1995). The effect of sodium bicarbonate ingestion on 1500-m racing time. Journal of Sports Sciences 13, 399-403.
17. BLATZ, A.L. (1980). Chemical modifiers and low internal pH block inward-rectifier K channels. Fed Proc 39, 2073
18. BOUISSOU, P., DEFER, G., GUEZENNEC, C.Y., ESTRADE, P.Y. & SERRURIER, B. (1988). Metabolic and blood catecholamine responses to exercise during alkalosis. Medicine and Science in Sports and Exercise 20(3), 228-232.
19. BOYARSKY, G., GANZ, M.B., STERZEL, R.B., & BORON, W.F. (1988). pH regulation in single glomerular mesangial cells. II. Na+-dependent and –independent Cl--HCO3
- exchangers. Am. J. Physiol. 255, C857-C869.
20. BRIEN, D.M. & MCKENZIE, D.C. (1989). The effect of induced alkalosis and acidosis on plasma lactate and work output in elite oarsmen. Eur.J.Appl.Physiol.Occup.Physiol. 58, 797-802.
21. BRODY, T.M. & AKERA, T. (1977). Relations among Na+,K+-ATPase activity, sodium pump activity, transmembrane sodium movement, and cardiac contractility. Fed. Proc. 36, 2219-2224.
22. BUSSE, M.W., MAASSEN, N. & BONING, D. (1989). The calculation of the osmotic volumes of distribution of hypertonic sodium bicarbonate and other hypertonic solutions: a theoretical approach. Journal of Medicine 20, 143-161.
23. BUSSE, M.W., SCHOLZ, J. & MAASSEN, N. (1992). Plasma potassium and ventilation during incremental exercise in humans: modulation by

References
109
sodium bicarbonate and substrate availability. Eur.J.Appl.Physiol.Occup.Physiol. 65, 340-346.
24. CASTLE, N.A. & HAYLETT, D.G. (1987). Effect of channel blockers on potassium efflux from metabolically exhausted frog skeletal muscle. J.Physiol London 383, 31-43.
25. CLAUSEN, T. (1986). Regulation of active Na+ -K+ transport in skeletal muscle. Physiological Reviews 66, 542-580.
26. CLAUSEN, T., EVERTS, M.E. & KJELDSEN, K. (1987). Quantification of the maximum capacity for active sodium-potassium transport in rat skeletal muscle. J.Physiol. 388, 163-181.
27. COGAN, M.G., CARNEIRO, A.V., TATSUNO, J., COLMAN, J., KRAPF, R., MORRIS, R.C.J. & SEBASTIAN, A. (1990). Normal diet NaCl variation can affect the renal set-point for plasma pH-(HCO3-) maintenance. J.Am.Soc.Nephrol. 1, 193-199.
28. COSTILL, D.L., BARNETT, A., SHARP, R., FINK, W.J. & KATZ, A. (1983). Leg muscle pH following sprint running. Med.Sci.Sports Exerc. 15, 325-329.
29. COSTILL, D.L., VERSTAPPEN, F., KUIPERS, H., JANSSEN, E. & FINK, W. (1984). Acid-base balance during repeated bouts of exercise: influence of HCO3. Int.J.Sports Med. 5, 228-231.
30. COX, G. & JENKINS, D.G. (1994). The physiological and ventilatory responses to repeated 60 s sprints following sodium citrate ingestion. J.Sports Sci. 12, 469-475.
31. DAVIES, N.W. (1990). Modulation of ATP-sensitive K+ channels in skeletal muscle by intracellular protons. Nature 343, 375-377.
32. DENNING, H., TALBOT, J.H., EDWARDS, H.T. & DILL, D.B. (1931). Effects of acidosis and alkalosis upon the capacity for work. Journal of Clinical Investigations 9, 601-613.
33. DONALDSON, S.K.B. & HERMANSEN, L. (1978). Differential, direct effects of H+ on Ca2+-activated force of skinned fibers from the soleus, cardiac and adductor magnus muscles of rabbits. Pflugers Archives 376, 55-65.
34. DUNN, J.F. & WALLEY, G.J. (1991). Renal regulation in hypertension. Biochem. Soc. Trans. 19, 421S.
35. EIAM-ONG, S. & SABATINI, S. (1996). Biochemical mechanisms and regulation of hydrogen transport in renal tubules. Mineral and Electrolyte Metabolism 22, 366-381.

References
110
36. ERSKINE, L. & HUNT, J.N. (1981). The gastric emptying of small volumes given in quick succession. Journal of Physiology 313, 335-341.
37. FABATIO, A. & FABATIO, F. (1978). Effects of pH on the myofilaments and the sarcoplasmic reticulum of skinned cells from cardiac and skeletal muscles. Journal of Physiology 276, 233-235.
38. FALLENTIN, N., JENSEN, B.R., BYSTROM, S. & SJØGAARD, G. (1992). Role of potassium in the reflex regulation of blood pressure during static exercise in man. Journal of Physiology 451, 643-651.
39. FITTS, R.H. & BALOG, E.M. (1996). Effect of intracellular and extracellular ion changes on E-C coupling and skeletal muscle. Acta Physiol. Scand. 156, 169-181.
40. FRASER, S.F. & MCKENNA, M.J. (1998). Measurement of Na+, K+-ATPase activity in human skeletal muscle. Analytical Biochemistry 258, 63-67.
41. GAITANOS, G.C., NEVILL, M.E., BROOKS, S. & WILLIAMS, C. (1991). Repeated bouts of sprint running after induced alkalosis. J.Sports Sci. 9, 355-370.
42. GAO, J., COSTILL, D.L., HORSWILL, C.A. & PARK, S.H. (1988). Sodium bicarbonate ingestion improves performance in interval swimming. European Journal of Applied Physiology and Occupational Physiology 58, 171-174.
43. GEERS, C. & GROS, G. (2000). Carbon dioxide transport and carbonic anhydrase in blood and muscle. Physiol.Rev. 80, 681-715.
44. GOLDFINCH, J., MC, N.L. & DAVIES, P. (1988). Induced metabolic alkalosis and its effects on 400-m racing time. Eur.J.Appl.Physiol.Occup.Physiol. 57, 45-48.
45. GOO, R.H., MOORE, J.G., GREENBERG, E. & ALZRAKI, N.P. (1987). Circadian variation in gastric emptying of meals in man. Gastroenterology 92(5), 1408-1408.
46. GREEN, H., DAHLY, A., SHOEMAKER, K., GOREHAM, C., BOMBARDIER, E. & BALL-BURNETT, M. (1999). Serial effects of high-resistance and prolonged endurance training on Na+-K+ pump concentration and enzymatic activities in human vastus lateralis. !Lost Data 165, 177-184.
47. GREEN, H.J., CHIN, E.R., BALL-BURNETT, M. & RANNEY, D. (1993). Increases in human skeletal muscle Na(+)-K(+)-ATPase concentration with short-term training. Am.J.Physiol 264, C1538-C1541

References
111
48. GREEN, S., BULOW, J. & SALTIN, B. (1999). Microdialysis and the measurement of muscle interstitial K+ during rest and exercise in humans. J.Appl.Physiol. 87, 460-464.
49. GREENHAFF, P.L., GLEESON, M. & MAUGHAN, R.J. (1987). The effects of dietary manipulation on blood acid-base status and the performance of high intensity exercise. Eur.J.Appl.Physiol.Occup.Physiol. 56, 331-337.
50. GREENHAFF, P.L., GLEESON, M. & MAUGHAN, R.J. (1988). The effects of diet on muscle pH and metabolism during high intensity exercise. Eur.J.Appl.Physiol.Occup.Physiol. 57, 531-539.
51. GROSSIE, J., COLLINS, C. & JULIAN, M. (1988). Bicarbonate and fast-twitch muscle: evidence for a major role in pH regulation. J.Membr.Biol. 105, 265-272.
52. GUYTON, A.C. (1991). Textbook of medical physiology. Philadelphia: W.B. Saunders Company.
53. HALPERIN, M.L. (1982). Metabolism and acid-base physiology. Artifical Organs 6, 357-361.
54. HATTNER, R.S. (1991). Determining gastric emptying rate. The Journal of Nuclear Medicine 32(10), 2024-2025.
55. HAUPTFLEISCH, J.J. & PAYNE, K.A. (1996). An oral sodium citrate-citric acid non-particulate buffer in humans. British Journal of Anaesthesia 77, 642-644.
56. HAUSSWIRTH, C., BIGARD, A.X., LEPERS, R., BERTHELOT, M. & GUEZENNEC, C.Y. (1995). Sodium citrate ingestion and muscle performance in acute hypobaric hypoxia. Eur.J.Appl.Physiol.Occup.Physiol. 71, 362-368.
57. HEBESTREIT, H., MEYER, F., HTAY-HTAY, HEIGENHAUSER, G.J.F. & BAR-OR, O. (1996). Plasma metabolites, volume and electrolytes following 30-s high-intensity exercise in boys and men. European Journal of Applied Physiology and Occupational Physiology 72, 563-569.
58. HEIGENHAUSER, G.J.F. & JONES, N.L. (1991). Bicarbonate Loading. In Perspectives in exercise science and sports medicine, eds. LAMB, D.R. & WILLIAMS, M.H., pp. 183-212. Wm. C. Brown.
59. HEIGENHAUSER, G.J.F., JONES, N.L., KOWALCHUK, J.M. & LINDINGER, M.I. (1990). The role of the physicochemical systems in plasma in acid-base control in exercise. In Biochemistry of Exercise VII, Anonymouspp. 359-374. Illinois: Human Kinetics.

References
112
60. HERMANSEN, L. (1979). Effect of acidosis on skeletal muscle performance during maximal exercise in man. Bull.Eur.Physiopathol.Respir. 15, 229-241.
61. HERMANSEN, L. (1981). Effect of metabolic changes on force generation in skeletal muscle during maximal exercise. Ciba.Found.Symp. 82, 75-88.
62. HOLLIDGE-HORVAT, M.G., PAROLIN, M.L., WONG, D., JONES, N.L. & HEIGENHAUSER, G.J. (1999). Effect of induced metabolic acidosis on human skeletal muscle metabolism during exercise. Am.J.Physiol. 277, E647-E658
63. HOLLIDGE-HORVAT, M.G., PAROLIN, M.L., WONG, D., JONES, N.L. & HEIGENHAUSER, G.J. (2000). Effect of induced metabolic alkalosis on human skeletal muscle metabolism during exercise. Am.J.Physiol.Endocrinol.Metab. 278, E316-E329
64. HOPFER, U. & LIEDTKE, C.M. (1987). Proton and bicarbonate transport mechanisms in the intestine. Annu. Rev. Physiol. 49, 51-67.
65. HORSWILL, C.A., COSTILL, D.L., FINK, W.J., FLYNN, M.G., KIRWAN, J.P., MITCHELL, J.B. & HOUMARD, J.A. (1988). Influence of sodium bicarbonate on sprint performance: relationship to dosage. Med.Sci.Sports Exerc. 20, 566-569.
66. IBANEZ, J., PULLINEN, T., GOROSTIAGA, E., POSTIGO, A. & MERO, a. (1995). Blood lactate and ammonia in short-term anaerobic work following induced alkalosis. J.Sports Med.Phys.Fitness. 35, 187-193.
67. ILUNDAIN, A. (1992). Intracellular pH regulation in intestinal and renal epithelial cells. Comp. Biochem. Physiol. Comp. Physiol. 101, 413-424.
68. INESI, G. & HILL, T.L. (1983). Calcium and proton dependence of sarcoplasmic reticulum ATPase. Biophys.J. 44, 271-280.
69. IWAOKA, K., OKAGAWA, S., MUTOH, Y. & MIYASHITA, M. (1989). Effects of bicarbonate ingestion on the respiratory compensation threshold and maximal exercise performance. Jpn.J.Physiol. 39, 255-265.
70. JONES, N.L., SUTTON, J.R., TAYLOR, R. & TOEWS, C.J. (1977a). Effect of pH on cardiorespiratory and metabolic responses to exercise. J.Appl.Physiol 43, 959-964.
71. JONES, N.L., SUTTON, J.R., TAYLOR, R. & TOEWS, C.J. (1977b). Effect of pH on cardiorespiratory and metabolic responses to exercise. J.Appl.Physiol 43, 959-964.

References
113
72. JUEL, C. (1986). Potassium and sodium shifts during in vitro isometric muscle contraction, and the time course of the ion-gradient recovery. Pflugers Archives 406, 458-463.
73. JUEL, C. (1995). Regulation of cellular pH in skeletal muscle fiber types, studied with sarcolemmal giant vesicles obtained from rat muscles. Biochim.Biophys.Acta 1265, 127-132.
74. JUEL, C. (1996). Lactate/proton co-transport in skeletal muscle: regulation and importance for pH homeostasis. Acta Physiol.Scand. 156, 369-374.
75. JUEL, C. (1997). Lactate-proton cotransport in skeletal muscle. Physiol.Rev. 77, 321-358.
76. JUEL, C. (1998a). Muscle pH regulation: role of training. Acta Physiol.Scand. 162, 359-366.
77. JUEL, C. (1998b). Skeletal muscle Na+/H+ exchange in rats: pH dependency and the effect of training. Acta Physiol.Scand. 164, 135-140.
78. JUEL, C., BANGSBO, J., GRAHAM, T. & SALTIN, B. (1990). Lactate and potassium fluxes from human skeletal muscle during and after intense, dynamic, knee extensor exercise. Acta Physiol.Scand. 140, 147-159.
79. JUEL, C., KRISTIANSEN, S., PILEGAARD, H., WOJTASZEWSKI, J. & RICHTER, E.A. (1994). Kinetics of lactate transport in sarcolemmal giant vesicles obtained from human skeletal muscle. J.Appl.Physiol. 76, 1031-1036.
80. JUEL, C. & PILEGAARD, H. (1998). Lactate/H+ transport kinetics in rat skeletal muscle related to fibre type and changes in transport capacity. Pflugers Arch. 436, 560-564.
81. JUEL, C., PILEGAARD, H., NIELSEN, J.J. & BANGSBO, J. (2000). Interstitial K(+) in human skeletal muscle during and after dynamic graded exercise determined by microdialysis. Am.J.Physiol.Regul.Integr.Comp.Physiol.2000.Feb.;278.(2.):R400.-6. 278, R400-R406
82. KACHADORIAN, W.A. & JOHNSON, R.E. (1970). Renal responses to various rates of exercise. Journal of Applied Physiology 28, 748-752.
83. KATZ, A., COSTILL, D.L., KING, D.S., HARGREAVES, M. & FINK, W.J. (1984). Maximal exercise tolerance after induced alkalosis. Int.J.Sports Med. 5, 107-110.

References
114
84. KEMP, G.J., THOMPSON, C.H., SANDERSON, A.L. & RADDA, G.K. (1994). pH control in rat skeletal muscle during exercise, recovery from exercise, and acute respiratory acidosis. Magn.Reson.Med. 31, 103-109.
85. KJELDSEN, K. (1991). Muscle Na,K-pump dysfunction may expose the heart to dangerous K levels during exercise. Canadian Journal of Sport Science 16, 33-39.
86. KOWALCHUK, J.M., HEIGENHAUSER, G.J.F. & JONES, N.L. (1984). Effect of pH on metabolic and cardiorespiratory responses during progressive exercise. Journal of Applied Physiology 57(5), 1558-1563.
87. KOWALCHUK, J.M., MALTAIS, S.A., YAMAJI, K. & HUGHSON, R.L. (1989). The effect of citrate loading on exercise performance, acid-base balance and metabolism. Eur.J.Appl.Physiol.Occup.Physiol. 58, 858-864.
88. KOWALCHUK, J.M. & SCHEUERMANN, B.W. (1995). Acid-base balance: origin of plasma [H+] during exercise. Canadian Journal of Applied Physiology 20(3), 341-356.
89. KOZAK-COLLINS, K., BURKE, E.R. & SCHOENE, R.B. (1994). Sodium bicarbonate ingestion does not improve performance in women cyclists. Med.Sci.Sports Exerc. 26, 1510-1515.
90. KRAPF, R. (1989) Physiology and molecular biology of the renal Na/H antiporter. Klin. Wochenschr. 67, 847-851.
91. KUU, W.Y., CHILAMKURTI, R. & CHEN, C. (1998). Effects of relative humidity and temperature on moisture sorption and stability of sodium bicarbonate powder. International Journal of Pharmaceutics 166, 167-175.
92. LAMBERT, C.P., GREENHAFF, P.L., BALL, D. & MAUGHAN, R.J. (1993). Influence of sodium bicarbonate ingestion on plasma ammonia accumulation during incremental exercise in man. Eur.J.Appl.Physiol.Occup.Physiol. 66, 49-54.
93. LAUF, P.K. (1987). Physiology and biophysics of chloride and cation transport. Fed Proc 46, 2377-2394.
94. LIEDTKE, C.M. (1989). Regulation of chloride transport in epithelia. Annu. Rev. Physiol. 51, 143-160.
95. LINDINGER, M.I., FRANKLIN, T.W., LANDS, L.C., PEDERSEN, P.K., WELSH, D.G. & HEIGENHAUSER, G.J. (1999). Role of skeletal muscle

References
115
in plasma ion and acid-base regulation after NaHCO3 and KHCO3 loading in humans. Am.J.Physiol. 276, R32-R43
96. LINDINGER, M.I., FRANKLIN, T.W., LANDS, L.C., PEDERSEN, P.K., WELSH, D.G. & HEIGENHAUSER, G.J. (2000). NaHCO(3) and KHCO(3) ingestion rapidly increases renal electrolyte excretion in humans. J.Appl.Physiol. 88, 540-550.
97. LINDINGER, M.I. & HEIGENHAUSER, G.J. (1991). The roles of ion fluxes in skeletal muscle fatigue. Can.J.Physiol.Pharmacol. 69, 246-253.
98. LINDINGER, M.I., HEIGENHAUSER, G.J., MCKELVIE, R.S. & JONES, N.L. (1992). Blood ion regulation during repeated maximal exercise and recovery in humans. Am.J.Physiol. 262, R126-R136
99. LINDINGER, M.I., HEIGENHAUSER, G.J. & SPRIET, L.L. (1990). Effects of alkalosis on muscle ions at rest and with intense exercise. Can.J.Physiol.Pharmacol. 68, 820-829.
100. LINDINGER, M.I., MCKELVIE, R.S. & HEIGENHAUSER, G.J. (1995). K+ and Lac- distribution in humans during and after high-intensity exercise: role in muscle fatigue attenuation? J.Appl.Physiol. 78, 765-777.
101. LINOSSIER, M.T., DORMOIS, D., BREGERE, P., GEYSSANT, A. & DENIS, C. (1997). Effect of sodium citrate on performance and metabolism of human skeletal muscle during supramaximal cycling exercise. Eur.J.Appl.Physiol.Occup.Physiol. 76, 48-54.
102. MACDONALD, I. (1957) Gastric activity during the menstrual cycle. Gastroenterology 30, 602-607.
103. MACLEAN, D.A., BANGSBO, J. & SALTIN, B. (1999). Muscle interstitial glucose and lactate levels during dynamic exercise in humans determined by microdialysis. J.Appl.Physiol. 87, 1483-1490.
104. MACLEAN, D.A., IMADOJEMU, V.A. & SINOWAY, L.I. (2000). Interstitial pH, K(+), lactate, and phosphate determined with MSNA during exercise in humans. Am.J.Physiol.Regul.Integr.Comp.Physiol.2000.Mar.;278.(3.):R563.-71. 278, R563-R571
105. MACLEAN, D.A., LANOUE, K.F., GRAY, K.S. & SINOWAY, L.I. (1998). Effects of hindlimb contraction on pressor and muscle interstitial metabolite responses in the cat. J.Appl.Physiol. 85, 1583-1592.

References
116
106. MAINWOOD, G.W. & RENAUD, J.M. (1985). The effect of acid-base balance on fatigue of skeletal muscle. Can.J.Physiol.Pharmacol. 63, 403-416.
107. MAINWOOD, G.W. & WARSLEY-BROWN, P. (1975). The effects of extracellular pH and buffer concentration on the efflux of lactate from frog sartorius muscle. Journal of Physiology 250, 1-22.
108. MARCOS, E. & RIBAS, J. (1995). Kinetics of plasma potassium concentrations during exhaustive exercise in trained and untrained men. European Journal of Applied Physiology and Occupational Physiology 71, 207-214.
109. MAREN, T.H. (1988). The kinetics of HCO3- synthesis related to fluid
secretion, pH control, and CO2 elimination. Annu. Rev. Physiol. 50, 695-717.
110. MATSON, L.G. & TRAN, Z.V. (1993). Effects of sodium bicarbonate ingestion on anaerobic performance: a meta-analytic review. Int.J.Sport.Nutr. 3, 2-28.
111. MCCARTNEY, N., HEIGENHAUSER, G.J. & JONES, N.L. (1983). Effects of pH on maximal power output and fatigue during short-term dynamic exercise. J.Appl.Physiol. 55, 225-229.
112. MCCOY, M. & HARGREAVES, M. (1992). Potassium and ventilation during incremental exercise in trained and untrained men. Journal of Applied Physiology 74(4), 1287-1290.
113. MCKENZIE, D.C., COUTTS, K.D., STIRLING, D.R., HOEBEN, H.H. & KUZARA, G. (1986). Maximal work production following two levels of artificially induced metabolic alkalosis. Journal of Sports Sciences 4, 35-38.
114. MCNAUGHTON, L.R. (1990). Sodium citrate and anaerobic performance: implications of dosage. Eur.J.Appl.Physiol.Occup.Physiol. 61, 392-397.
115. MCNAUGHTON, L.R. (1992a). Bicarbonate ingestion: effects of dosage on 60 s cycle ergometry. J.Sports Sci. 10, 415-423.
116. MCNAUGHTON, L.R. (1992b). Sodium bicarbonate ingestion and its effects on anaerobic exercise of various durations. J.Sports Sci. 10, 425-435.
117. MCNAUGHTON, L.R. & CEDARO, R. (1991). The effect of sodium bicarbonate on rowing ergometer performance in elite rowers. The Australian Journal of Science and Medicine in Sport 23(3), 66-69.

References
117
118. MCNAUGHTON, L. & CEDARO, R. (1992). Sodium citrate ingestion and its effects on maximal anaerobic exercise of different durations. Eur.J.Appl.Physiol.Occup.Physiol. 64, 36-41.
119. MCNAUGHTON, L., CURTIN, R., GOODMAN, G., PERRY, D., TURNER, B. & SHOWELL, C. (1991). Anaerobic work and power output during cycle ergometer exercise: effects of bicarbonate loading. J.Sports Sci. 9, 151-160.
120. MCNAUGHTON, L., DALTON, B. & PALMER, G. (1999). Sodium bicarbonate can be used as an ergogenic aid in high-intensity, competitive cycle ergometry of 1 h duration. Eur.J.Appl.Physiol.Occup.Physiol. 80, 64-69.
121. MOORE, J.G., CHRISTIAN, P.E. & COLEMAN, R.E. (1981). Gastric emptying of varying meal weight and composition in man. Digestive Diseases and Sciences 26(1), 16-22.
122. NOTIVOL, R., CARRIO, I., CANO, L., ESTORCH, M. & VILARDELL, F. (1984). Gastric emptying of solid and liquid meals in healthy young subjects. Scandinavian Journal of Gastroenterology 19, 1107-1113.
123. OSTER, J.R., STEMMER, C.L., PEREZ, G.O. & VAAMONDE, C.A. (1988). Comparison of the effects of sodium bicarbonate versus sodium citrate on renal acid excretion. Miner.Electrolyte Metab. 14, 97-102.
124. PAJOR, A.M. (1999). Citrate transport by the kidney and intestine. Semin. Nephrol. 19, 195-200.
125. PARRY-BILLINGS, M. & MACLAREN, D.P. (1986). The effect of sodium bicarbonate and sodium citrate ingestion on anaerobic power during intermittent exercise. Eur.J.Appl.Physiol.Occup.Physiol. 55, 524-529.
126. PFEFFERLE, K.P. & WILKINSON, J.G. (1988). Induced alkalosis and supramaximal cycling in trained and untrained men. Medicine and Science in Sports and Exercise 20, S25
127. PIERCE, E.F., EASTMAN, N.W., HAMMER, W.H. & LYNN, T.D. (1992). Effect of induced alkalosis on swimming time trials. J.Sports Sci. 10, 255-259.
128. PILEGAARD, H., DOMINO, K., NOLAND, T., JUEL, C., HELLSTEN, Y., HALESTRAP, A.P. & BANGSBO, J. (1999). Effect of high-intensity exercise training on lactate/H+ transport capacity in human skeletal muscle. Am.J.Physiol 276, E255-E261
129. POTTEIGER, J.A., NICKEL, G.L., WEBSTER, M.J., HAUB, M.D. & PALMER, R.J. (1996a). Sodium citrate ingestion enhances 30 km cycling performance. Int.J.Sports Med. 17 , 7-11.

References
118
130. POTTEIGER, J.A., WEBSTER, M.J., NICKEL, G.L., HAUB, M.D. & PALMER, R.J. (1996b). The effects of buffer ingestion on metabolic factors related to distance running performance. Eur.J.Appl.Physiol.Occup.Physiol. 72, 365-371.
131. PUTNAM, R.W. (1990). pH regulatory transport systems in a smooth muscle-like cell line. Am.J.Physiol. 258, C470-C479
132. PUTNAM, R.W. & ROOS, A. (1986a). Effect of calcium and other divalent cations on intracellular pH regulation of frog skeletal muscle. J.Physiol. 381, 221-239.
133. PUTNAM, R.W., ROOS, A. & WILDING, T.J. (1986b). Properties of the intracellular pH-regulating systems of frog skeletal muscle. J.Physiol. 381, 205-219.
134. QUAYLE, J.M., NELSON, M.T. & STANDEN, N.B. (1997). ATP-sensitive and inwardly rectifying potassium channels in smooth muscle. Physiol.Rev. 77, 1165-1232.
135. RADEGRAN, G. & SALTIN, B. (1998). Muscle blood flow at onset of dynamic exercise in humans. Am.J.Physiol. 274, H314-H322
136. REN, J.M. & HULTMAN, E. (1989). Regulation of glycogenolysis in human skeletal muscle. J.Appl.Physiol 67, 2243-2248.
137. ROBERTSON, R.J., FALKEL, J.E., DRASH, A.L., SWANK, A.M., METZ, K.F., SPUNGEN, S.A. & LEBOEUF, J.R. (1987). Effect of induced alkalosis on physical work capacity during arm and leg exercise. Ergonomics 30, 19-31.
138. ROBIN, E.D. (1961). Of men and mitochondria: intracellular and sub-cellular acid-base relations. New England Journal of Medicine 265, 780-785.
139. ROGER FEDDE, M. & PIESCHL, R.L. (1995). Extreme derangements of acid-base balance in exercise: advantages and limitations of the stewart analysis. Canadian Journal of Applied Physiology 20(3), 369-379.
140. ROSDAHL, H., HAMRIN, K., UNGERSTEDT, U. & HENRIKSSON, J. (1998). Metabolite levels in human skeletal muscle and adipose tissue studied with microdialysis at low perfusion flow. Am.J.Physiol. 274, E936-E945
141. ROTH, D.A. & BROOKS, G.A. (1990). Lactate and pyruvate transport is dominated by a pH gradient-sensitive carrier in rat skeletal muscle sarcolemmal vesicles. Archives of Biochemisty and Biophysics 279(2), 386-394.

References
119
142. SAHLIN, K. (1978a). Intracellular pH and energy metabolism in skeletal muscle of man. With special reference to exercise. Acta Physiol.Scand.Suppl. 455, 1-56.
143. SAHLIN, K., ALVESTRAND, A., BRANDT, R. & HULTMAN, E. (1978b). Intracellular pH and bicarbonate concentration in human muscle during recovery from exercise. J.Appl.Physiol. 45, 474-480.
144. SCHABORT, E.J., WILSON, G. & NOAKES, T.D. (2000). Dose-related elevations in venous pH with citrate ingestion do not alter 40-km cycling time-trial performance. Eur.J.Appl.Physiol. 83, 320-327.
145. SCHULTZ, S.G. (1984). A cellular model for active sodium absorption by mammalian colon. Annu. Rev. Physiol. 46, 435-451.
146. SCHULTZ, S.G. & DUBINSKY, W.P. (2001). Sodium absorption, volume control and potassium channels: in tribute to a great biologist. J. Membr. Biol. 184, 255-261.
147. SEABURY, J.J., ADAMS, W.C. & RAMEY, M.R. (1977). Influence of pedalling rate and power output on energy expenditure during bicycle ergometry. Ergonomics 20(5), 491-498.
148. SHAVE, R., WHYTE, G., SIEMANN, A. & DOGGART, L. (2001). The effects of sodium citrate ingestion on 3,000-meter time-trial performance. J.Strength.Cond.Res. 15, 230-234.
149. SJOGAARD, G., ADAMS, R.P. & SALTIN, B. (1985). Water and ion shifts in skeletal muscle of humans with intense dynamic knee extension. Am.J.Physiol 248, R190-R196
150. SJOSTRAND, M., HOLMANG, A. & LONNROTH, P. (1999). Measurement of interstitial insulin in human muscle. Am.J.Physiol. 276, E151-E154
151. SOKABE, M., KASAI, M., NOMURA, K., & NARUSE, K. (1991). Electrophysiological analysis of structural aspects of voltage-dependent SR K+ channel. Comp. Biochem. Physiol. 98, 23-30.
152. SPRIET, L.L. (1991a). Phosphofructokinase activity and acidosis during short-term tetanic contractions. Can.J.Physiol.Pharmacol. 69, 298-304.
153. SPRIET, L.L., CAMPBELL, C.B. & DYCK, D.J. (1991b). Effect of aging on the buffering capacity of fast-twitch skeletal muscle. Mech.Ageing Dev. 59, 243-252.
154. SPRIET, L.L., LINDINGER, M.I., MCKELVIE, R.S., HEIGENHAUSER, G.J. & JONES, N.L. (1989). Muscle glycogenolysis and H+ concentration during maximal intermittent cycling. J.Appl.Physiol. 66, 8-13.

References
120
155. SPRIET, L.L., SODERLUND, K., BERGSTROM, M. & HULTMAN, E. (1987). Skeletal muscle glycogenolysis, glycolysis, and pH during electrical stimulation in men. J.Appl.Physiol. 62, 616-621.
156. SPRUCE, A.E., STANDEN, N.B. & STANFIELD, P.R. (1985). Voltage-dependent ATP-sensitive potassium channels of skeletal muscle membrane. Nature London 361, 736-738.
157. STEWART, P.A. (1983). Modern quantitative acid-base chemistry. Can.J.Physiol.Pharmacol. 61, 1444-1461.
158. SULLIVAN, M.J., SALTIN, B., NEGRO-VILAR, R., DUSCHA, B.D. & CHARLES, H.C. (1994). Skeletal muscle pH assessed by biochemical and 31P-MRS methods during exercise and recovery in men. J.Appl.Physiol. 77, 2194-2200.
159. SUTTON, J.R., JONES, N.L. & TOEWS, C.J. (1981). Effect of PH on muscle glycolysis during exercise. Clin.Sci.(Lond.) 61, 331-338.
160. TANNER, R.L. (1980). Control of acid excretion by the kidney. Annu. Rev. Med. 31, 35-49.
161. TANNER, G.A. (1984). Renal regulation of acid-base balance: ammonia excretion. Physiologist 27, 95-97.
162. THOMPSON, L.V., BALOG, E.M. & FITTS, R.H. (1992). Muscle fatigue in frog semitendinosus: role of intracellular pH. American Journal of Physiology 262 (Cell Phys 31), C1507-C1512
163. TIRYAKI, G.R. & ATTERBOM, H.A. (1995). The effects of sodium bicarbonate and sodium citrate on 600 m running time of trained females. J.Sports Med.Phys.Fitness. 35, 194-198.
164. VAN SOMEREN, K., FULCHER, K., MCCARTHY, J., MOORE, J., HORGAN, G. & LANGFORD, R. (1998). An investigation into the effects of sodium citrate ingestion on high-intensity exercise performance. Int.J.Sport.Nutr. 8, 356-363.
165. VICTOR, R.G., BERTOCCI, L.A., PRYOR, S.L. & NUNNALLY, R.L. (1988). Sympathetic nerve discharge is coupled to muscle cell pH during exercise in humans. J.Clin.Invest. 82, 1301-1305.
166. VIST, G.E. & MAUGHAN, R.J. (1995). The effect of osmolality and carbohyrate content on the rate of gastric emptying of liquids in man. Journal of Physiology 486.2 , 523-531.
167. WASSERMAN, K., STRINGER, W.W., CASABURI, R. & ZHANG, Y.Y. (1997). Mechanism of the exercise hyperkalemia: an alternate hypothesis. J.Appl.Physiol. 83, 631-643.

References
121
168. WEBSTER, M.J., WEBSTER, M.N., CRAWFORD, R.E. & GLADDEN, L.B. (1993). Effect of sodium bicarbonate ingestion on exhaustive resistance exercise performance. Med.Sci.Sports Exerc. 25, 960-965.
169. WESTERBLAD, H. & ALLEN, D.G. (1992). Changes of intracellular pH due to repetitive stimulation of single fibres from mouse skeletal muscle. J.Physiol. 449, 49-71.
170. WILKES, D., GLEDHILL, N. & SMYTH, R. (1983). Effect of acute induced metabolic alkalosis on 800-m racing time. Medicine and Science in Sports and Exercise 15, 277-280.
171. WRIGHT, E.M. & LOO, D.D (2000) Coupling between Na+, sugar, and water transport across the intestine. Ann. N.Y. Acad. Sci. 915, 54-66.