-
8/13/2019 SJS12002-34
1/7
34 S. Moeng, K. BoffardScandinavian Journal of Surgery 91: 3440,
2002
PENETRATING NECK INJURIES
S. Moeng, K. Boffard
Johannesburg Hospital Trauma Unit, and Department of Surgery,
University of the Witwatersrand,Johannesburg, South Africa.
Key words: Neck trauma; cervical trauma; penetrating trauma;
vascular injuries; carotid trauma
INTRODUCTION
Management of penetrating neck injuries is compli-
cated by the anatomic high-density relationship be-tween
vascular, upper respiratory, digestive and neu-rological
structures. Up to 30 % of the injuries involvemultiple structures
(1). Expeditious systematic as-sessment, decision-making and
appropriate treat-ment is required to minimise catastrophic
complica-tions.
Before World War II non-operative managementresulted in
mortality rates as high as 16 %, whichprompted subsequent
exploration of injuries pene-trating the platysma. It was further
shown that mor-tality associated with mandatory exploration couldbe
improved from 35 % to 6 % if patients were oper-ated on earlier
(2). Numerous centres have chal-
lenged the principle of mandatory exploration in therecent
years. Currently civilian mortality figures areexpected at 26 % and
can be as high as 11 % (3).Most of these cases are associated with
vascular in-juries (carotid arteries, subclavian vessels) and
spi-nal injuries.
ANATOMY
Basic knowledge of the anatomy of the neck is es-sential in
appreciating the complex nature of theseinjuries and serves as a
landmark in the managementof these injuries. The platysma is a thin
muscle that
originates from upper thorax extending into the neckand finally
blending with muscles of the face. It iscovered by superficial
fascia that lies just beneath the
skin. Injuries that penetrate this muscle define pene-trating
neck injuries. The deep fascia underlies thismuscle and is divided
into three portions (investing,
pretracheal and prevertebral layers). Investing fasciacovers the
trapezius, omohyoid and sternocleidomas-toid muscles. The
pretracheal fascia covers the thy-roid and cricoid cartilage
extending and blendingwith mediastinal tissues. The prevertebral
fascia cov-ers the vertebra and deep muscles close to it. Allthree
fascial divisions contribute to form carotidsheath that covers the
carotid vessels, internal jugu-lar and the vagus nerves. The
recurrent laryngealnerve lies in the groove between trachea and
theoesophagus.
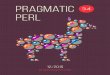
The neck is divided into three anatomic zones. Thishelps in the
categorisation and management of neckwounds. (See Fig. 1)
Zone I extends from the bottom of the cricoid car-tilage to the
clavicles and thoracic outlet. Within thiszone lie the trachea, the
great vessels, the oesopha-gus, the upper mediastinum, the lung
apices and thethoracic duct. Mortality in this zone is the highest
ofthe three zones.
Zone II includes the area between the cricoid car-tilage and the
angle of the mandible. Enclosed with-in its region are the carotid
and vertebral arteries,jugular veins, pharynx, larynx, oesophagus,
and tra-chea.
Zone III involves the area above the angle of themandible up to
the base of the skull, and includesthe distal extracranial carotid
and vertebral arteries
as well as segments of the jugular veins.Injuries in Zone II are
readily evaluated and easilyexposed operatively. Adequate exposure
of Zone Ior Zone III injuries can be difficult, thus, the
diag-nostic work-up may be more extensive than forZone II injuries.
Trauma to the neck is not necessarilylimited to a specific
zone.
The neck is also anatomically divided into the an-terior and the
posterior triangles.
Most of injuries involve Zone II in many studies,yet mortality
is the highest in Zone I (4). The mostcommon cause of death is
exsanguination. Vascularinjuries account for up to 25 % of
structural injurieswith carotid and internal jugular most
frequently in-
Correspondence:K. D. Boffard, M.D.Department of
SurgeryUniversity of the Witwatersrand Facultyof Health Sciences,7,
York Road,Parktown,Johannesburg, 2193Republic of South AfricaEmail:
[email protected]
-
8/13/2019 SJS12002-34
2/7
35Penetrating neck injuries
volved. The vertebral artery is less commonly in-volved due to
its protected anatomic position. Therespiratory tract is involved
in 10 % of the cases andproper airway management is essential to
avoid res-piratory embarrassment. Though the oesophagus isless
involved, missed injuries are associated withhigh morbidity and
mortality. Neurological injuriesand other injuries should be borne
in mind.
MECHANISM
Penetrating wounds can be broadly categorised intothose caused
by missiles (gunshot wounds/ blastfragments/ pellets) and those by
stabs and lacera-tions (knives/ axes/ swords/ tree branches).
The severity of injuries seen with missiles (e.g. bul-lets) is
related to a number of factors, which includethe kinetic energy
impacted by the missile on the tis-sues, the properties of the
missile and the density ofthe tissues damaged.
Energy transferred to the tissues is related to the
Kinetic Energy (5) expressed as
KE = m (VenVex)2
Where KE is Kinetic energyM is the mass of the objectVenis the
velocity on entryVexis the velocity on exit
High velocity (and therefore high energy) missilesas seen with
military, rifle and short distance shot-gun wounds cause more
damage than low velocitymissiles. The mass of the missile is
proportional tothe energy transferred.
Missiles do not necessarily enter or even travel in
the tissues perpendicular to their long axis. This abil-ity to
yaw and tumble increases the surface area thathas direct tissue
contact thus increasing the damage.They also have the ability to
form temporary cavita-tion in the tissues which relates to the
amount ofenergy transmitted. By creating several waves of
con-traction and expansion within the tissues they resultin damage
of tissues remote from direct area of con-tact. This phenomenon is
worst in tissues of greatestresistance. During initial debridement
it is very easyto underestimate the degree of tissue damage
awayfrom the path followed by the missile.
Some missiles are specially designed to cause moretissue damage
by increasing the amount of energy
transferred to the tissues. They may do so by explod-ing on
impact, fragmenting or even flattening on con-tact to cause rapid
deceleration.
More damage is caused in the tissues that havegreater resistance
mainly due to their absorption ofmost of the energy.
MANAGEMENT
Prompt initial assessment and institution of manage-ment should
be carried out according to the ATLS
principles, prioritising the life-threatening
conditionsfirst.
AIRWAY
Initial concern is to establish and maintain a patentairway,
which may be compromised by direct airwayinjury, bleeding into the
oral cavity, compressionfrom haematomas in the neck or even severe
surgi-cal emphysema around the neck. Some patients mayhave impaired
neurology from associated head in-
Fig. 1. Zones of the neck.
-
8/13/2019 SJS12002-34
3/7
36 S. Moeng, K. Boffard
jury or severe shock with impaired ability to main-
tain the airway. Sudden deterioration of initial air-way status
may occur. The need for proper assess-ment and constant monitoring
of the airway cannotbe overemphasised.
Different methods can be instituted (6) to achievethis depending
on several factors, including the skillof the attending physician,
availability of the re-sources and presenting features. Oxygen
supplemen-tation, basic airway maintenance technique and
mon-itoring should be instituted as soon as possible whilepreparing
equipment for definitive airway. A highindex of suspicion for
possible spinal injury shouldbe maintained and the neck immobilized
until radi-ological or clinical clearance has been obtained.
Orotracheal intubation is recommended for pa-tients that are
moribund, apnoeic or have associatedbleeding into the airway. Most
emergency physiciansand departments are equipped for this technique
butit may be challenging under emergency situations.Bleeding,
collapsed airway and associated spinal in-jury complicate this
technique and one should al-ways be ready to perform a surgical
airway. The air-way cannot be clearly assessed below the cords
withthis method. Therefore intubation may complicate analready
existing injury below the cords. The use ofneuromuscular blocking
agents should be avoided ifpossible because of the possible
disaster that may fol-low collapse of the airway due to relaxation
of mus-
cles which help to maintain some patency of the air-way
especially when one fails to intubate successful-ly. The patient
should not cough or strain during thisprocedure because of a
potential risk of increasingbleeding in the presence of vascular
injuries.
For this reason most people may use benzodi-azepines such as
midazolam (with or without opi-oids) or anaesthetic inducing agents
like etomidateor ketamine to facilitate intubation. Obviously a
mor-ibund unstable patient might not even require anysedation or
paralysis.
The need for a surgical airway should be antici-pated and
instituted promptly should the need arise.Cricothyroidotomy in
failed endotracheal intubation
or in cases associated with severe facial or laryngealfractures
may be life saving. This procedure is tech-nically easier but may
be challenging in the presenceof neck swelling due to extensive
surgical emphyse-ma or haematoma. It is usually avoided in
childrenand in patients with injuries below the
cricothyroidmembrane. Tracheostomy may be done in the emer-gency
department or in the operating theatre in lessurgent cases. Not all
upper airway injuries requiretracheostomy for definitive
management. Either anopen or percutaneous route may be chosen.
Awake fibreoptic intubation with the use of localspray
anaesthesia, bronchoscopy and endotrachealtube can be attempted if
facilities and expertise areavailable. This technique has become
useful in therecent years though not necessarily universally
avail-able. The advantage is that the airway can be visual-ised,
with placement of the intubation tube beyondthe injury, and it can
be confirmed that the balloonis distal to the injury to minimise
further damage tothe airway and massive air leak. This can be
achievedwith the patient awake and breathing spontaneo-
usly. Some centres use a visual monitor that allowsother members
of the resuscitation team to assess theairway and plan
appropriately. Rapid sequencefiberoptic induction has also been
tried but it is morechallenging in emergency situations, especially
thoseassociated with bleeding in the area.
Other methods include intubation via the injuryitself,
especially in stabs where there is an obviousdirect airway injury
in the midline. This is only usedtemporarily until a more
definitive airway can be es-tablished.
Blind nasal intubation is discouraged since it mayconvert a
partial airway injury into a complete oneand there is a possibility
of creating a false tract.
BREATHING
After securing the airway, ventilation should also beassessed to
ensure good oxygenation. Tension pneu-mothorax, haemothorax and
pneumothorax shouldbe dealt with. Persistent pneumothoraces despite
in-tercostal decompression should alert one to a possi-ble major
airway injury that may require surgical re-pair.
CIRCULATION
Vascular assessment and management will include
assessing for haemodynamic stability, checking forsigns of
injury (expanding haematoma, bruit, shock,severe bleeding, unequal
upper limb pulses, hemi-plegia etc), and control of active bleeders
either bydirect pressure or balloon tamponade (7). Avoidprobing
neck wounds because this may dislodge aclot resulting in bleeding
or air embolism. Vascularaccess should be established and fluid
administeredaccordingly. At this stage one would have an idea ofthe
patients stability, in order to decide whether fur-ther
investigation was helpful, or whether urgentsurgery in the unstable
patient was necessary.
The key is where possible to obtain vascular con-trol. Ideally
this should be by direct pressure, or dig-
Fig. 2. Stab wound of the neck showing the use of a Foleys
cathe-ter for haemostasis.
-
8/13/2019 SJS12002-34
4/7
37Penetrating neck injuries
ital pressure, however in difficult access situations,a Foley
catheter can be used.
The patient should never be allowed to sit up be-cause of the
danger of air embolism.
DISABILITY
Neurological assessment includes checking level ofconsciousness
and Glasgow Coma Scale (GCS), pres-ence of hemiplegia, Horners
Syndrome, spinal cordlesion, brachial plexus injuries and injury to
cranialnerves (especially VII/IX/ X/ XI/ XII). Hoarsenessshould
alert one to possible recurrent laryngeal nerveinjury and further
assessment of mobility of the vo-cal cords.
OTHER INJURIES
The presence of surgical emphysema, haemoptysis,or odynophagia
should also alert one to the possibil-ity of oesophageal injury
that may require furtherinvestigation.
Further assessment for associated injuries shouldbe carried out
appropriately.
INVESTIGATION
The choice of investigation will be influenced by thecondition
of the patient. Stable patients can be inves-tigated fully
according to the clinical findings, where-as instability may only
allow for a few emergencyroom investigations or nothing at all
before explora-tion in theatre. Investigation does not replace
goodthorough clinical examination but complements the
findings.
BASIC INVESTIGATION
As a minimum, a chest X-ray and an X-ray of the cer-vical spine
will allow assessment for haemothorax,pneumothorax, surgical
emphysema, cervical spineinjury and to check for foreign bodies.
These can beused to augment clinical findings and help in
direct-ing further management. Markers should be appliedto the
entrance and exit wounds if possible prior toradiological
examination to obtain an idea about thetract. The mediastinum
should be assessed for evi-dence of vascular injury. Blood for
cross-matching
and other tests should be organised accordingly.
SPECIFIC INVESTIGATIONS
Angiogram is considered the gold standard for ar-terial injury
investigation. It is an invasive investi-gation associated with
some complications in about1 % of the cases and false positives and
false nega-tives do occur in about 3 % of cases (8). These
com-plications include bleeding at the arteriotomy site,spasm of
the vessels (which may be of major concernif it involves the
carotids), allergic reactions, intimaltears, embolisation of
atheromatous plaques and sep-sis. Indications include evidence of
vascular injury
on examination in a stable patient, close proximitygunshot
wounds, transcervical wounds and hemi-plegia. Abnormal findings
include extravasation ofcontrast, vascular cut-off, intimal tears,
false aneu-rysm and A-V fistula.
An additional advantage of angiography in pa-tients with
proximal injury is that a balloon can beleft in place by the
radiologist, to control proximalbleeding.
Other than diagnostic value it has therapeutic uses.Vessels can
be embolised during this procedure. Themost commonly embolised
vessels in the neck are thevertebral arteries. Stenting to control
bleeding or tem-porary balloon occlusion of vessels to determine
pos-sible neurological effects of arterial ligation can beattempted
during angiography.
Recently, Colour Flow Duplex imaging has beenshown to be safe
and effective as a screening proce-dure with fewer side effects and
at a less cost (9). Thisis a non-invasive procedure using a 510
MHztrans-ducer to analyse vessels in the neck both longitudi-nally
and transversely. Carotids and vertebral ves-
sels have been assessed with this method. It has beenshown that
smaller vascular injuries may be missede.g. small intimal tears.
However, these small inju-ries can be managed conservatively.
Unfortunatelythis modality is not always available and is
operatordependant. It can also be used in follow-up of
con-servatively managed injuries. Angiography is pre-ferred in Zone
I and possibly Zone III injuries.
Oesophagography and/or oesophagoscopy may berequired in the
investigation of oesophageal injuries.Either of the studies alone
may detect 60 % of the in-juries but together they approximate 100
% (10). Wa-ter-soluble contrast is preferred to barium swallowas an
initial test in oesophagography, but if this test
is negative and there is still a high index of suspi-cion, the
latter may yield superior results. Better yieldcan be achieved with
the patient in a lateral decubi-tus position. The problem arises
with a patient whocannot swallow for the test (e.g. intubated or
uncon-scious patients). A nasogastric tube may be intro-duced under
direct visual guidance into the oesopha-gus and contrast given, but
proximal oesophageal le-sions are not well visualised this way.
Both rigid andflexible oesophagoscopy may be used.
Flexibleoesophagoscopy is associated with false negative re-sults
in proximal oesophageal injuries especiallywhen mucosal oedema is
present, and in addition,mucosal folds in the cricopharyngeal area
may hide
the pathology. Some feel that rigid oesophagoscopymay yield
closer to 100 % accuracy for proximal le-sion but general
anaesthesia is required and hyper-extension of the neck may not be
possible in unsta-ble spinal injuries.
Laryngoscopy and bronchoscopy may be used toassess the airway
injury. Confirming mucosal in-volvement, and associated possible
full thickness in-jury will assist in decision-making regarding
furthermanagement. Both flexible and rigid bronchoscopesare
available. Vocal cords may be assessed for move-ment in relevant
cases.
Other tests include magnetic resonance imaging(MRI) angiography
and helical (spiral) CT angiogra-
-
8/13/2019 SJS12002-34
5/7
38 S. Moeng, K. Boffard
phy for vascular work-up, and CT scanning of thebrain or neck
tissues.
MRI angiography is not always immediately avail-able in most
cases requiring transfer to relevant cen-tres. Furthermore
monitoring of patients with multi-ple injury or haemodynamic
instability may be com-promised. This makes this investigation
impracticalin most situations.
Helical (spiral) CT angiography has been shownto have high
specificity and sensitivity in diagnos-ing vascular injuries. It is
available in certain centresand with recent advances in technology
is rapid.Other injuries can be assessed at the same time.
Tooptimise sensitivity it is advised to scan from the topof the
arch of the aorta to the base of the skull.
In cases of hemiplegia, coma or head injury CTscan of the brain
may be essential. Infarcts may notbe evident initially. CT scan may
also be useful inassessing spinal injuries and some laryngeal
injuries.
DEFINITIVE CARE
UNSTABLE PATIENT
There is no argument about the need to operate onpatients that
are unstable or who have evidence ofsevere injury to the
aerodigestive or vascular system.The patient will be prepared for
theatre urgently, assoon as the airway and circulation have been
tem-porarily controlled. Further resuscitation and inves-tigation
may be carried out in theatre. This group in-cludes patients with
severe active bleeding, shock notresponding to resuscitation,
expanding haematomas,pulsatile haematomas, or evidence of severe
respira-
tory injury.
STABLE PATIENT
Controversy exists in patients that have no clinicalsigns of
major injury or have soft signs. Most au-thors practice selective
management (11) of these in-juries while some advocate mandatory
exploration.
Selective management
Most have adopted policy of selective managementin view of a
high rate of negative exploration andgood outcomes. Patients are
assessed clinically and
by investigation and triaged further into operative
orconservative (non-operative) management. In injuriesthat have
penetrated the platysma, a bronchoscopy,laryngoscopy,
oesophagoscopy and/or oesophago-grapy with Duplex Flow Doppler
studies or angio-graophy will be performed to assess the patient
fur-ther and manage accordingly. This is even more im-portant in
patients who cannot be clinically moni-tored to assess for change
in symptoms (for exampleundergoing other surgical procedures).
Angiographywould be advised for Zone I and III injuries.
Recently an even more selective approach has beenadopted by some
centres even for Zone I and ZoneIII injuries (12). Clinical
examination for stable pa-
tients would include cervical and chest X-rays, andwould be
carried thoroughly as described above. Ifhoarseness was present, or
minor haemoptysis orsurgical emphysema then laryngoscopy and or
bron-choscopy would be required. Pain on swallowingand emphysema
around the neck should mandateoesophagoscopy and or
oesophagography.
Minor evidence of vascular injury or injury in closeproximity to
the vessel or sometimes even for trans-cervical will require
vascular investigation. Initiallya Duplex Flow Ultrasound (when
available) will beperformed if vascular injury is suspected. If the
ul-trasound examination is equivocal or not availablethen
angiography will be required.
Patients should be assessed regularly and then canbe discharged
if no complications develop.
The major concern about this approach is possi-bility of missing
injuries on examination.
Mandatory exploration
Those that favour mandatory exploration of all
wounds penetrating the platysma irrespective of thesigns and
symptoms (13), argue that physical signsare unreliable and that
morbidity from negative ex-ploration is preferable to complications
related tomissed injuries. Studies have shown that up to 30 %of
patients will have negative physical signs of inju-ry on
presentation thus increasing the possibility ofmissing injuries,
which increases the morbidity andmortality. The number of
investigations required isminimised thus reducing cost. Morbidity
from explo-ration is acceptable provided a thorough operationis
done. They further feel that hospital stay is not sig-nificantly
different from other methods.
Our own experience is that there is very little place
for mandatory exploration.
SPECIFIC SURGERY
Vascular injuries
General principles of good exposure, proximal anddistal control
and initial direct pressure to controlbleeding are applicable.
Zone II injuries are explored by an incision alongthe anterior
border of the sternocleidomastoid mus-cle. Zone I injuries may be
approached by sternoto-my or thoracotomy depending on the vessels
in-volved. Zone III injuries may be difficult to expose
and mandibular subluxation, vertical mandibular os-teotomy or
even intracranial control may be neces-sary.
Trap-door incisions are often difficult and we arenot in favour
of their use. Carotid arteries may in-volve internal, external or
common carotid vessels.Common carotid injuries are associated with
inter-nal jugular vein injuries and thus have higher mor-tality.
Repair is recommended for major injuries butcare should be
exercised in the presence of anaemicinfarcts because of fear of
converting them intohaemorrhagic infarcts or the worsening of
oedemaassociated with revascularisation. Presence of comahas poor
outcome irrespective of the management
-
8/13/2019 SJS12002-34
6/7
39Penetrating neck injuries
(14) although the best results can be achieved withimmediate
revascularisation.
Repairs vary from simple debridement and directanastomosis to
the use of venous and synthetic graftsfor more extensive injuries.
Shunts may be used incomplex injuries. External carotid injuries
may beligated or treated conservatively.
Minor injuries like very small intimal flaps can bemanaged
conservatively but regular follow up withDuplex ultrasound is
essential if complications areto be minimised.
Most vertebral injuries can be managed non-oper-atively or by
proximal and distal embolisation. Sur-gical approach to these
arteries is a major challengeand is reserved for patients with
failed embolisationor major bleeding.
Subclavian venous injury has a higher mortalitythan subclavian
arterial injury, probably because ofpossible air embolism and
inability of the vessel tocontract. Proximal injuries may require
sternotomywith lateral extension. Access can also be gained
bythoracotomy and transclavicular approaches. Veins
can be ligated but arteries should be repaired wherepossible.
Ligation of arteries is associated with in-creased morbidity.
Upper airway injuries
Aggressive airway management is essential to mini-mize
mortality.
Management of laryngeal injuries depends on theirseverity (15).
In minor injuries (minor lacerations,minor mucosal disruption,
airway compromise with-out laryngeal fracture) simple repair
without trache-ostomy is sufficient. Repair of major injuries
(largemucosal lacerations, displaced fractures of the larynx,
laryngeal instability, vocal cord injuries) may requirethyrotomy
with reduction of displaced fractures,stenting or tracheostomy.
Minor injuries with mobilecords have better voice results. Major
injuries tendto have worse voice results if stenting is used in
thepresence of mobile cords. Follow-up includes assess-ment for
airway patency and voice quality.
Tracheal injuries can be assessed using broncho-scopy or during
exploration. The posterior membra-nous wall should also be
inspected in anterior inju-ries. Early diagnosis and primary repair
leads to theleast complication and best long-term results.
Simple lacerations may be repaired without trache-ostomy. Larger
defects once debrided and repaired
are best managed with tracheostomy and may re-quire muscle flaps
especially if there is an associatedoesophageal injury.
Upper digestive tract
Hypopharyngeal and oesophageal injuries may beeasily missed.
Leakage of saliva and bacteria, as wellas reflux of acid, pepsin
and bile into the tissues re-sults in a severe necrotising
inflammatory response.This response is more severe if there is a
delay in ac-tive management (>1224 hours). Delayed repairs ofthe
oesophagus are associated with increased mor-bidity and
mortality.
Oesophageal perforations should be debrided,mobilised if
necessary and repaired primarily. Ade-quate drainage is essential.
A muscle flap may beused in large defects or when there is
associated tra-cheal injury. Their use may not prevent
oesophagealleaks but may prevent tracheo-oesophageal
fistulaformation. Antibiotics should be started as early
aspossible. Delayed oesophageal repairs may requiremore extensive
procedures, including diversion.
There is a place for conservative management ofupper hypophyseal
injuries (lesions above the levelof arytenoid cartilage). This area
is wrapped by mid-dle and inferior constrictor muscles and has a
lowintraluminal pressure allowing of injuries to sealspontaneously.
Early intravenous antibiotics, restric-ted oral intake and frequent
observation for septicmarkers can be sufficient for management of
theselesions.
Lower hypophyseal injuries are managed as foroesophagus because
they are more likely to leak andproduce deep neck sepsis if not
repaired anddrained.
CONCLUSION
Management of penetrating neck injuries is contro-versial but
there is a trend towards selective conserv-ative management. Rapid
assessment and promptmanagement of life threatening conditions
especi-ally airway and vascular control is essential in
earlymanagement. Unstable patients should be surgicallyexplored as
soon as possible. Thorough physical ex-amination and appropriate
investigations followedby serial examination optimise care of
stable patients.The incidence of missed injuries should be
minimised
to avoid the high morbidity and mortality associatedwith
them.
REFERENCES
01. Demetriades D, Skalkides J, Sofianos C, Melissas J, Franklin
J:Carotid artery injuries: experience with 124 cases. J
Trauma1989;29:9194
02. Fogelman MJ, Steward RD: Penetrating wounds of the neck.Am J
Surg 1956;91:581596
03. Asensio J, Valenziano CP, Falcone R, Grosh J: Management
ofpenetrating neck injuries: The controversy surrounding ZoneII
injuries. Surg Clin North Am 1991;71:267296
04. Thal ER, Meyer DM: Penetrating neck trauma. Curr Probl
Surg1992;29:1015
05. Stiernberg C, Jahrsdoerfer R, Gillenwater A, Joe S, Alcalen
S:Gunshot wounds to the head and neck. Arch
Otolaryngol1992;118:592597
06. Desjardins G, Varon AJ: Airway management for
penetratingneck injuries: the Miami experience. Resuscitation
2001;48:7175
07. Gilroy D, Lakhoo M, Charalambides D, Demetriades D: Con-trol
of life-threatening haemorrhage from neck injuries: a newindication
for balloon tamponade. J Trauma. 1992;23:557559
08. Douglas P: Emergent radiological evaluation of the
gunshotwounds. Radiol Clin North Am. 1992;30:307323
09. Corr P, Abdool Carrim A, Robbs J: Colour-flow ultrasound
inthe detection of penetrating vascular injuries of the neck. S
AfrMed J 1999;89:644646
10. Detar MJ, Stanley R:Diagnosis and management of
externalpenetrating cervical oesophageal injuries. Ann Otol
RhinolLaryngol. 1994;103:863871
-
8/13/2019 SJS12002-34
7/7
40 S. Moeng, K. Boffard
11. Demetriades D, Asensio J, Velmahos G, Thal E: Complex
prob-lems in penetrating neck trauma. Surg Clin North
Am1996;76:661683
12. Eddy VA, and the Zone I penetrating neck injury group:
Isroutine arteriography mandatory for penetrating injuries toZone I
of the neck? J Trauma. 2000;48:208214
13. Apffelstaedt J, Muller R: Results of mandatory exploration
forpenetrating neck trauma. World J Surg 1994;18:917920
14. Feliciano DV: A new look at penetrating carotid artery
injuries.Adv Trauma Crit Care. 1994;9:319345
15. Grewal H, Rao P, Mukerji S, Ivatury R: Management of
pene-trating laryngotracheal injuries. Head and neck.
1995;17:494502
Received: July 2, 2001