Embed Size (px)
Citation preview
Sjogren’s Syndrome:An Unmet Therapeutic Need
Robert I. Fox, M.D., Ph.D.
Scripps Memorial Hospital
Scripps/XiMED Medical Center
La Jolla, California

All slides are available on my website
robertfoxmd.com
2
A new Approach to Therapy is Necessary
in Sjogren’s Syndrome – Why?• At present, we have unhappy patients and
frustrated physicians.
• The symptoms of ocular/oral pain and fatigue rarely correlate with either our objective exam or our acute phase reactants.
• After years of failure of trials of biologics, it is time for a new approach.
Goals-1What are current issues
in diagnosis?
1. Is it SS or is it SLE?
1. Do we use traditional criteria (American-European) or the new SICCA criteria?
1. How does SS overlap with the newly described IgG4-related disease?
Specific Goals-2
• How can we convey information about treatment of dry eyes/dry mouth to our patients in the limited time allowed in a patient revisit?
• This is a practical limitation that is very important aspect of patient care.
• Will deal with this problem in afternoon session.
Goals-3Update on Pathogenesisincluding Genetics and
Cytokines1. Acquired immune system: HLA-DR and autoantibody
2. Innate immune system: type 1 IFN signature and IFN-g/IL-17
But we are still missing how the immune process influences the midbrain, cortical and hypothalamic axis aspects of SS.
Goals-4
1. Why have trials at systemic therapies (i.e., rituximab, belimumab) and other biologic agents failed?
They have not improved fatigue!
1. New targets must include the immune-neural targets, including the influence of cytokines on micro-glial cells and their transmitters.
Background-1
SS has “benign” and “systemic”manifestations.
FDA licensing will require improvement in both
manifestations.
Background-2
Benign manifestations include:
• Dry and painful eyes• Dry and painful mouth• Myalgias, fatigue • Impaired cognition (executive function)— trying to distinguish “fibromyalgia” from “depression”
Patients would:
• Equate SS with impact similar to moderate angina.
• Trade 2 years of “life expectancy” to not have SS symptoms.
SS Related Health Care Costs-1:
• Dry or painful eyes are now most common cause of visits to Ophthalmologists in Japan.
• Lost productivity (over $160 billion/year just for dry eyes (especially in computer users where decreased blink rate is 90%.
• Direct healthcare costs in Great Britain (NHS) are second only to RA, and exceed SLE.
• RA £2693 (not including TNFs)
• pSS £2188 (not including OTC cost of artificial tears or dental costs)
• Age Matched NHS Controls £849
SS-Related Health Care Costs-2:
SS-Related Health Care Costs-3:
Despite these costs of health care, patient and physician
dissatisfaction with clinical outcomes is higher in pSS than
in SLE or RA.
Classification-1Is Sjogren’s just SLE
with 4/5 Criteria?
• Different antibody profile (anti-SSA/B)
are not criteria for SLE;
• SS is more organ specific –
(salivary/lacrimal gland)
and more lymphoproliferative.
Classification-2Why is Sjogren’s not just SLE
with 4/5 Criteria?
1. Interstitial pneumonitis (not pleurisy), interstitial nephritis (not glomerulonephritis)
2. Higher frequency of lymphoma
3. Genome Screens support this with Homing receptors found in SS but not SLE (CXCR5)
Classification-3What is the relationship
of IgG4-related Disease and SS?
• 1892- Mikulicz described salivary gland swelling and lymphoid infiltrate.
• Initial reports by Mikulicz were TBC or lymphoma.
• Today, pathology of Mikulicz Disease is most frequently part of IgG4-related disease.
• Female-Male incidence (9:1 in SS)
Mikulicz (part of IgG4 RD)
• For many years, Mikulicz was considered the characteristic biopsy of SS.
• Now, we recognize that they are different processes.
• Confusion still exists in salivary gland and in extraglandular tissues (i.e., AIP, interstitial pneumonitis).
IgG4-Related Disease
• Different pattern on biopsy from SS.
• IgG4 plasma cells plus “storiform” fibrosis.
• Think of IgG4 RD as a plasma cell
dyscrasia where B-cells release particular
cytokines.
• The overlap of cytokines with SS may be
confusing.
History and Classification-3
Old vs. New SS Criteria•1984: San Diego Classification (Fox) to include objective criteria for clinical trials
•1998: American/European Consensus Criteria (Vitali et al.) included ocular and oral symptoms (validated in Europe) and lab studies (minor salivary gland biopsy or SS-A)
Most important “child” of AECC was the ESSDAI
(European Sjogren’s Syndrome Activity Index)
which includes 16 domains of activity score including glandular and extraglandular
activity• The ESSDAI ranges from 1-130• Practically the range is 1-41• A clinically meaningful change is 3.5 units
• Constitutional• Skin• Lung, Renal• Neurologic
ESSDAI- European SS Activity Index
• Weighted domains to give a total score— the Sjogren’s equivalent to ACR-50 for RA.
• The validated ESSDAI activity score has been the accepted outcome measure of
FDA clinical trials.
•
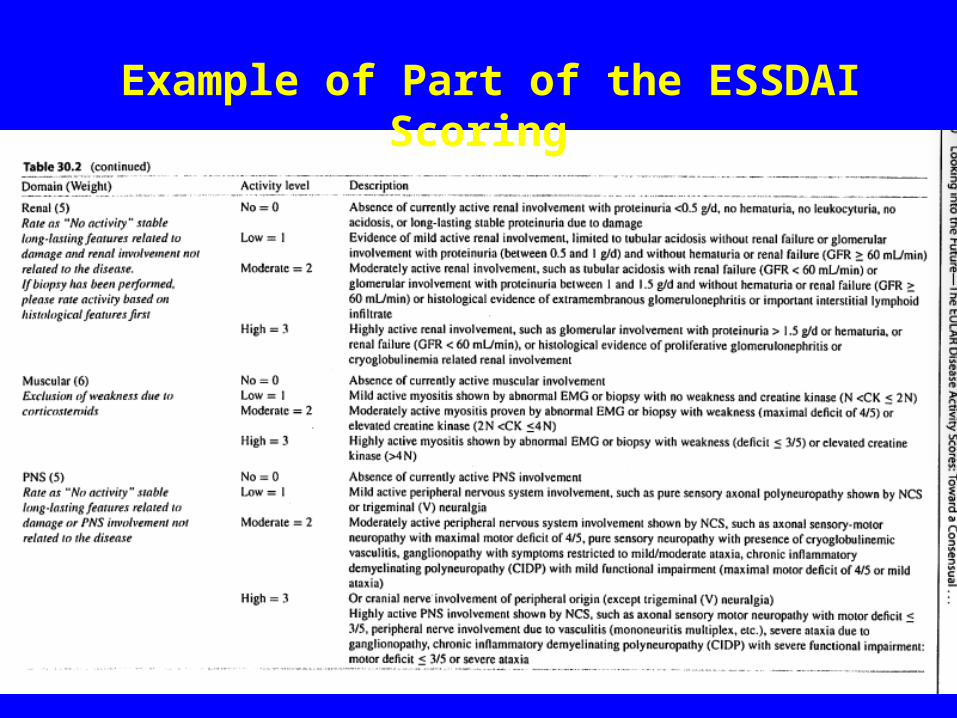
Example of Part of the ESSDAI Scoring
Although the Consensus AECCwas used for over over 20 years in over 1300 publications and
50 clinical trials approved by FDA and EMA …
the AECC were never “formally” submitted to ACR for US validation and formal ACR
acceptancesince everyone seemed comfortable using
these criteria.
Further, formal ACR validation would require an additional study in a US cohort.
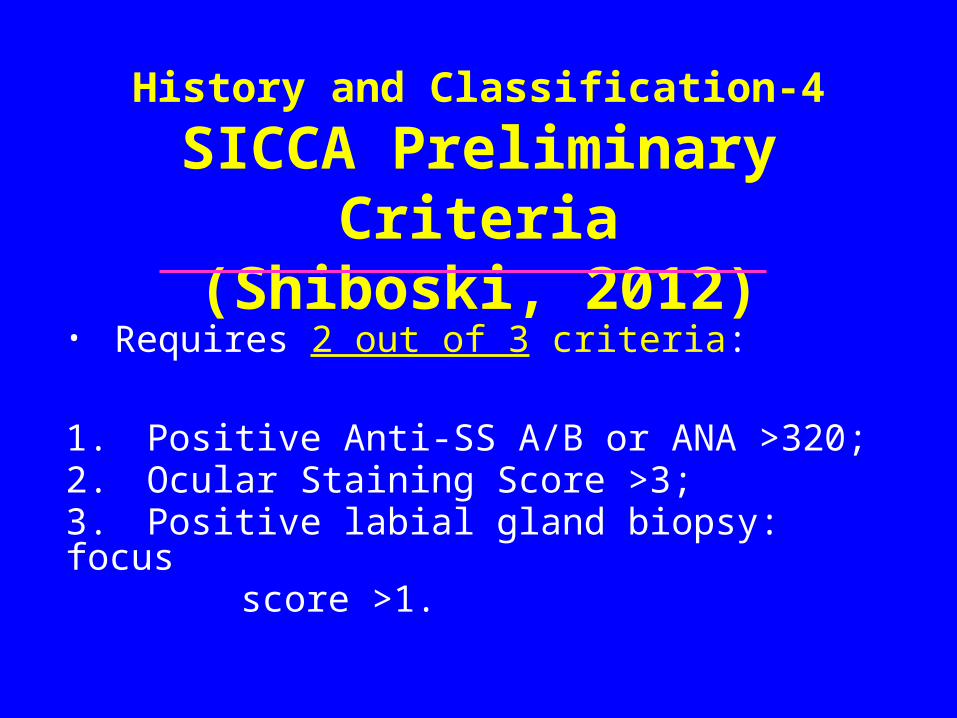
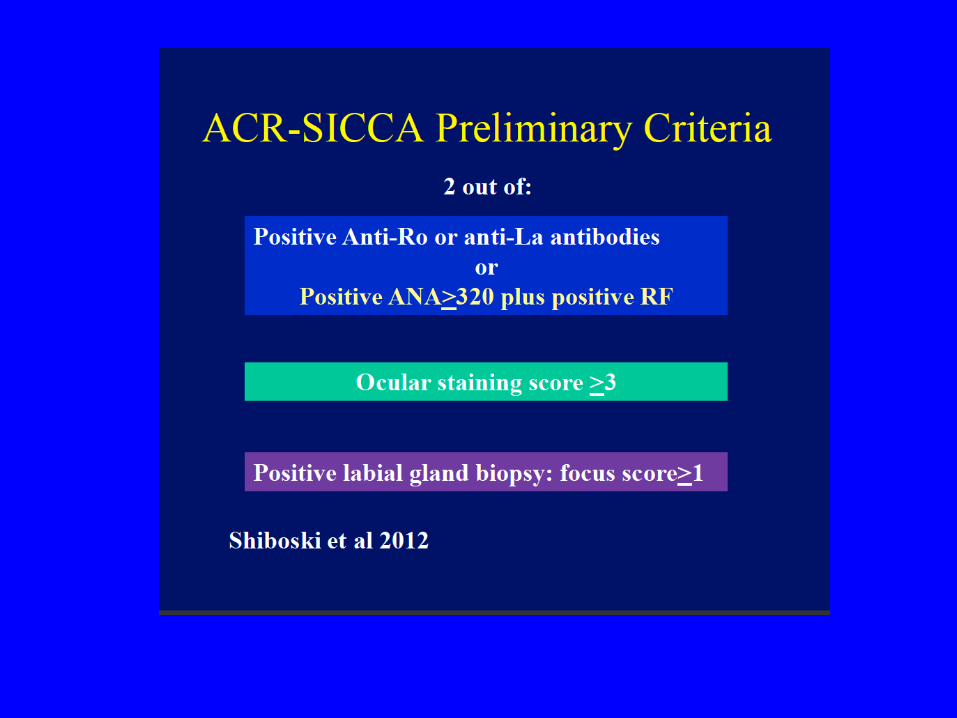
History and Classification-4
SICCA Preliminary Criteria
(Shiboski, 2012)• Requires 2 out of 3 criteria:
1. Positive Anti-SS A/B or ANA >320;2. Ocular Staining Score >3;3. Positive labial gland biopsy: focus score >1.
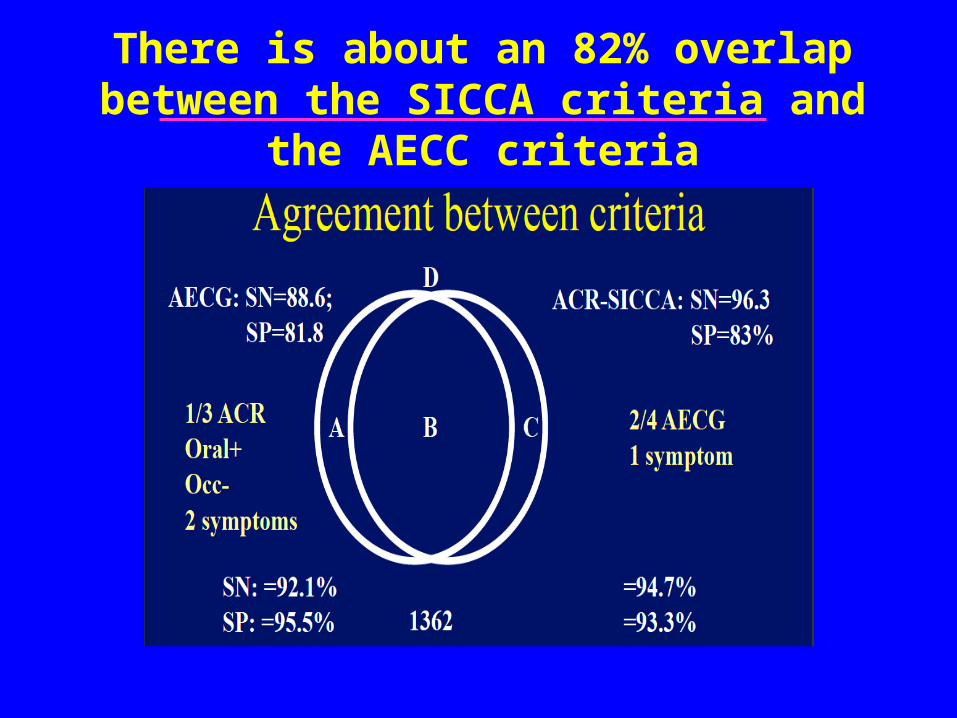
There is about an 82% overlap between the SICCA criteria and the AECC criteria
Does it matter?
• Our outcome measures ESSDAI may not be true in new SICCA system, so there is no way to judge study outcomes.
• Literature search and prognosis are all based on old AECC criteria.
• The 5 published studies comparing both systems indicate IT DOES make a difference.
Problems with New SICCA Classification-1
• ACR tentatively accepting these, pending “validation” on independent cohort.
• Independent validation has not been performed and the grant denied.
• At least 5 published studies have shown important differences in the patients identified by AECC and SICCA.
• Although 82% similar, the discordant group greatly affect the outcome in clinical trials.
Other Problems with new SICCA Classification
• Few Rheumatologists do SG biopsies.
• Few Ophthalmologists perform the ocular exam as specified by SICCA (because it is time-consuming and much harder than a simple Lissamine green).
• Committees in process of a new “combined” criteria.
Pathogenesis-1
• Concordance of SS among identical twins only about 20%
• Thus, genetic sequence is not enough and over 80% is epigenetic— environmental factor or gene regulation.
• Distinct histone acetylation pattern upstream of key genes.
Pathogenesis-2
• Large sequences of untranslated mRNA.
• Novel miRNA, some with sequence similar to EBV fragments.
• Genetics in GWAS recently published and only SS (not SLE) has homing receptor (CXCR5) as a strong “hit.”
To briefly summarize PATHOGENESIS …
Acquired Immune System--
•HLA DR and Associated T-cell directed B-cell antibodies;
•IFN-g and IL-17 pathways
Innate immune system—
• Type I IFN signature
•NK like cells link acquired and innate
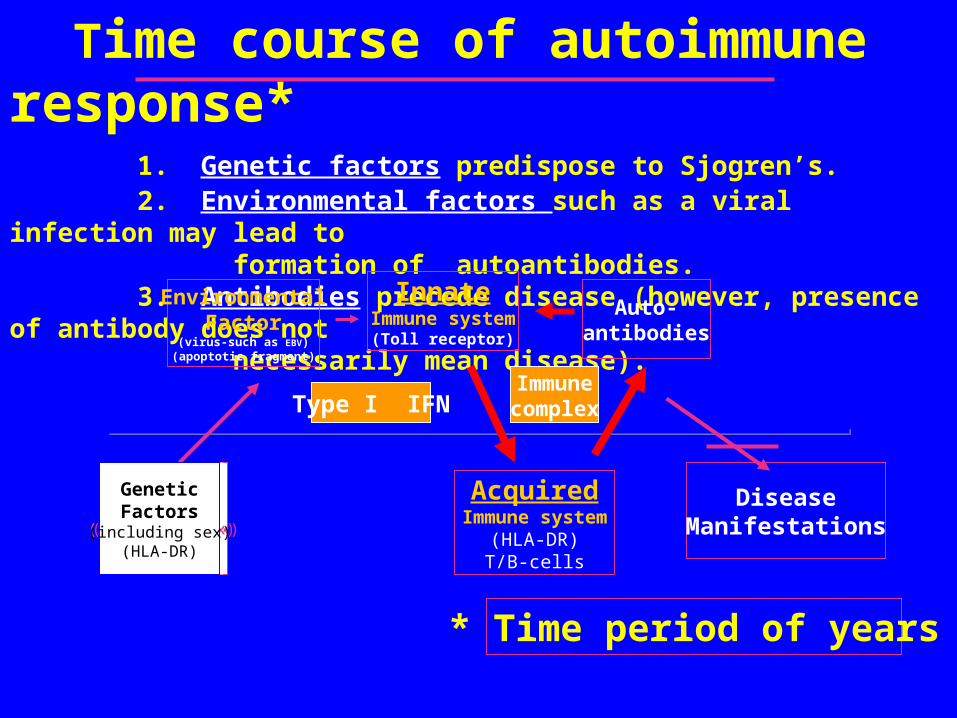
Time course of autoimmune response* 1. Genetic factors predispose to Sjogren’s. 2. Environmental factors such as a viral infection may lead to formation of autoantibodies. 3. Antibodies precede disease (however, presence of antibody does not necessarily mean disease).
GeneticFactors
(including sex)(HLA-DR)
GeneticFactors
(including sex)(HLA-DR)
GeneticFactors
(including sex)(HLA-DR)
GeneticFactors
(including sex)(HLA-DR)
Auto-antibodies
AcquiredImmune system
(HLA-DR)T/B-cells
DiseaseManifestations
* Time period of years
InnateImmune system
(Toll receptor)
GeneticFactors
(including sex)(HLA-DR)
EnvironmentalFactor
(virus-such as EBV)(apoptotic fragment)
Type I IFNImmunecomplex
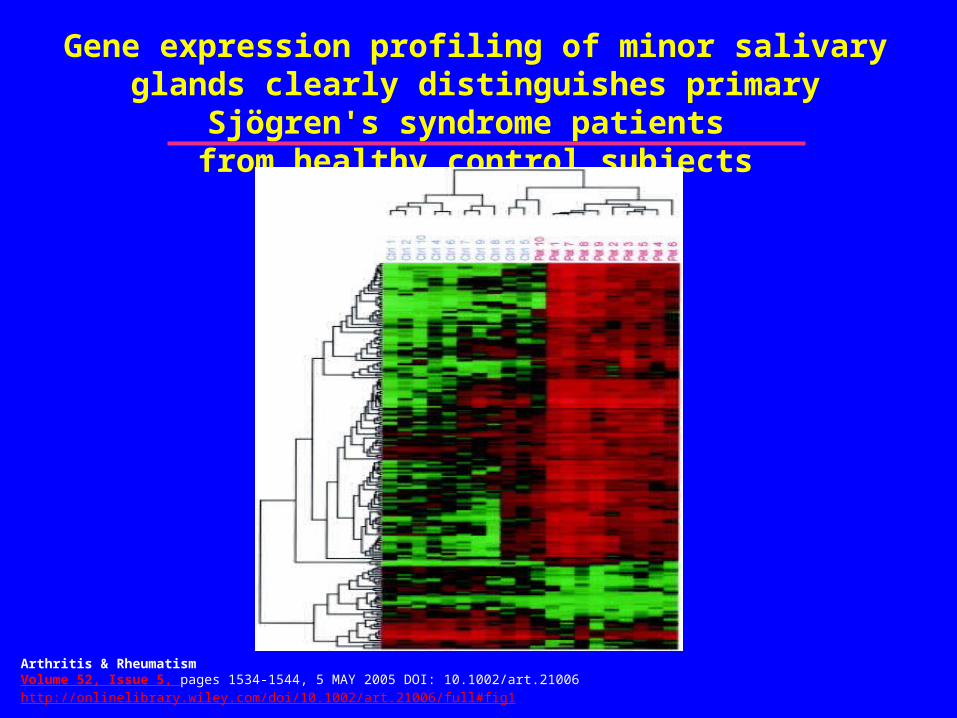
Gene expression profiling of minor salivary glands clearly distinguishes primary Sjögren's syndrome patients
from healthy control subjects
Thegene signatureis type I IFN
Arthritis & RheumatismVolume 52, Issue 5, pages 1534-1544, 5 MAY 2005 DOI: 10.1002/art.21006http://onlinelibrary.wiley.com/doi/10.1002/art.21006/full#fig1
The main cytokine targets match those identified in genome wide screens*
• HLA-DR (T-cell), CTLA and IFN-• NF-K /IkB
• Homing receptor (CXCR5)
• Type I IFN –IRF5, STAT4, TLR3/7/9 and pkR (cytoplasmic
sensor)
• B-cell activation –BLK, BAFF, IL12, and A20 (TNFAIP3)
• * Most of these targets do not map to the encoded protein but to upstream sites of RNA transcription that are not translated (presumed epigenetic sites such as methylation)
Pathogenesis-3Genome-Wide Association
Parallels-- our studies on cytokine profiles• Strongest is HLA-DR and acquired immune system
leading to T-cell/B-cell production of autoantibody.
• Next strongest are Innate Immune markers associated with Type 1 IFN production.
• As noted above, also find a homing receptor (CXCR5) which goes with the tissue-specific homing receptors.
• In SS patients with lymphoma, find A20 (member of TNF superfamily) that suppresses NFK-b and B-cell proliferation.
The main cytokine targets match those identified in genome wide screens*
• HLA-DR (T-cell), CTLA and IFN-• NF-K /IkB
• Homing receptor (CXCR5)
• Type I IFN –IRF5, STAT4, TLR3/7/9 and pkR (cytoplasmic sensor)
• B-cell activation –BLK, BAFF, IL12, and A20 (TNFAIP3)
• * Most of these targets do not map to the encoded protein but to upstream sites of RNA transcription that are not translated (presumed epigenetic sites such as methylation)
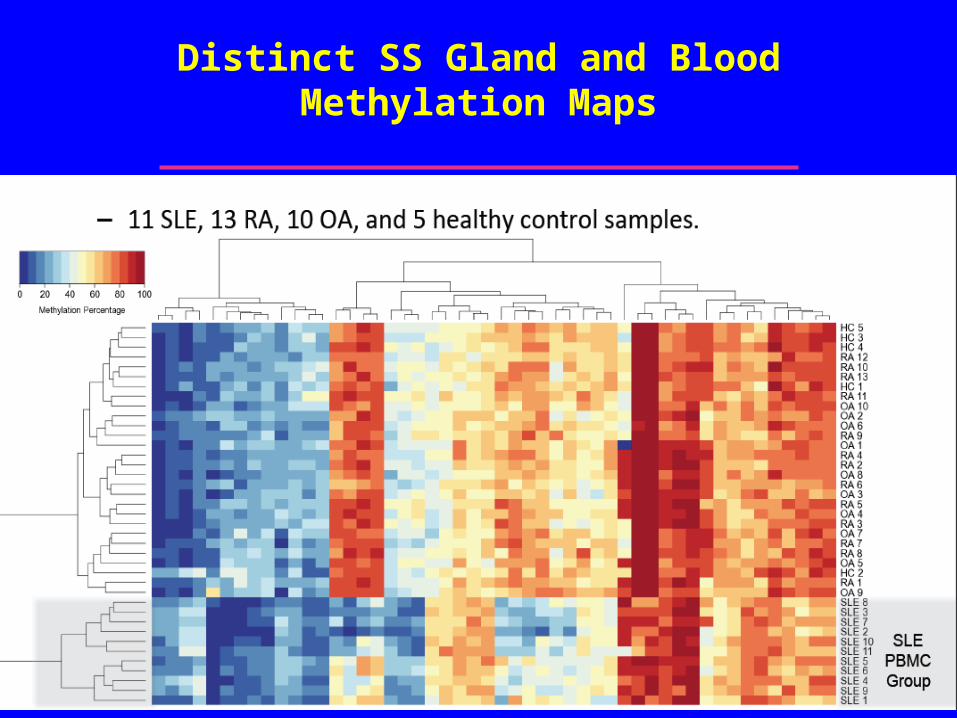
Distinct SS Gland and Blood Methylation Maps
If we know the genes and the cytokines,
why have we made so little progress with biologics in Sjogren’s Syndrome?
a) Although we can improve the extraglandular
manifestations (rash, cytopenias,
pneumonitis), none have fulfilled the
requirements where patients actually feel
better.
b) The most frequently used biologic in SS
remains rituximab—even though it failed its
randomized trials.
Previously Studied in SS
• Anti-CD20 –glandular, extraglandular and
fatigue
• BAFF (Blys)-ACR 2012 abstracts*
• Abatacept (CD40 L)-ACR 2012
• Allogeneic mesenchymal cells- ACR 2012
abstracts and article in Blood
Other Inhibitors of IFN
a. Initial trials of anti-type 1 IFN had infusion reactions and only
modest efficacy.
b. Medi 546 (type 1 IFN-R antagonists) now in phase 1 (scleroderma) and juvenile SLE phase 2 trial.
But we are still missing key targets in the
pathogenesis of fatigue and the
adrenal-hypothalmic axis.
• In both SS and SLE, we can lower the cytokine with biologics, but the patient still feels little improvement.
• This will be the focus of future direction for therapy.
The functional Circuit• To understand “benign symptoms” and develop better
therapies, we must review the concept of the functional circuit in SS.
• This “circuit” starts with unmyelinated nerves at the mucosal surface.
• These nerves travel to the “midbrain” (the salvitory and lacrimatory nuclei of cranial nerve V)
• Have reflections to the cortical surface that sense pain or dryness.
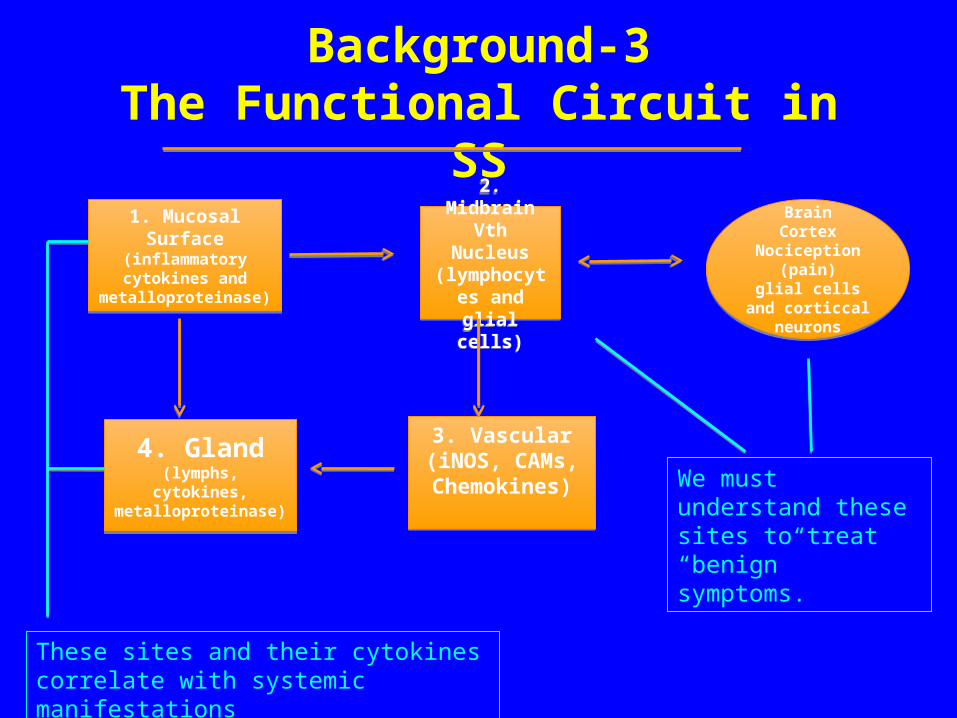
Background-3The Functional Circuit in SS
1. Mucosal Surface(inflammatory cytokines and metalloproteinase)
1. Mucosal Surface(inflammatory cytokines and metalloproteinase)
2. MidbrainVth Nucleus(lymphocytes and glial cells)
2. MidbrainVth Nucleus(lymphocytes and glial cells)
4. Gland(lymphs, cytokines, metalloproteinase)
4. Gland(lymphs, cytokines, metalloproteinase)
3. Vascular(iNOS, CAMs, Chemokines)
3. Vascular(iNOS, CAMs, Chemokines)
BrainCortex
Nociception (pain)
glial cells and corticcal neurons
BrainCortex
Nociception (pain)
glial cells and corticcal neurons
These sites and their cytokines correlate with systemic manifestations
We must understand these sites to treat “benign” symptoms.
Recent studies in multiple sclerosis and animal models of “flu”
• Have led to at least 5 approved therapies;
• Have highlighted the importance of cytokines on microglial cells;
• Have identified new targets including mTor, AKT, IKDelta, and Sphingosine (the fingolimod receptor).
Does this apply to Sjogren’s syndrome?
• Patients with early SS had corneal pain that decreased completely with topical anesthesia*.
• Patients with chronic SS showed only a partial (30% decrease) in eye pain after topical anesthetic*
• Functional MRI (fMRI) showed nocioceptive pattern— called phantom pain amplification
*Rosenthal et al
Neuro-plasticity is a new concept for most rheumatologists
• A stimulus that is not painful (innocuous) in a normal model may be painful in its “autoimmune” congenic.
• Events in the CNS are not detected in the peripheral blood.
• Models such as MS model or murine flu.
0
Neuroplasticity in Pain Processing1-3
1. Woolf CJ, Salter MW. Science. 2000;288:1765-1768. 2. Basbaum AI, Jessell TM. The perception of pain. In: Kandel ER, et al, eds.
Principles of Neural Science. 4th ed. 2000:479.3. Cervero F, Laird JMA. Pain. 1996;68:13-23.
Stimulus Intensity
100
Pain state Normal
Allodynia
Hyperalgesia3
80
60
40
20
innocuous noxious
Pa
in S
en
sa
tio
n
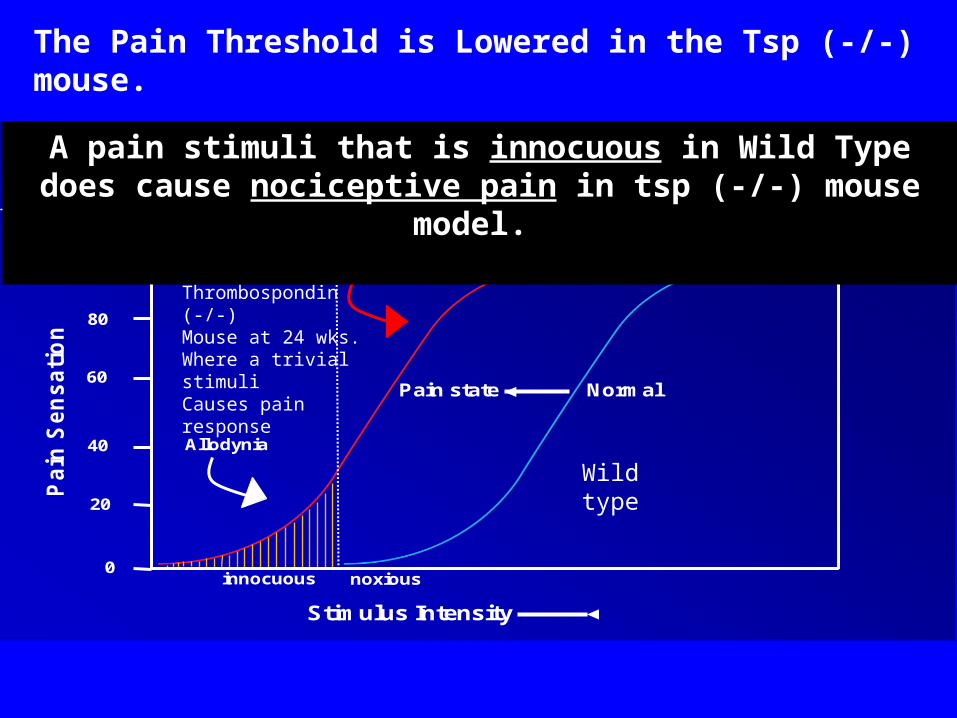
Thrombospondin (-/-)Mouse at 24 wks.Where a trivial stimuliCauses pain response
Wild type
A pain stimuli that is innocuous in Wild Typedoes cause nociceptive pain in tsp (-/-) mouse model.
The Pain Threshold is Lowered in the Tsp (-/-) mouse.
To study the mechanism of neurogenic or nociceptive pain we must use animal model-1
• The thrombospondin (-/-) mouse (TSP null) or the TGF-receptor mutation both develop SS like disease.
• The mouse develops both oral and ocular lesions.
• The mouse develops ANA and SS-A antibodies.
To study the mechanism of neurogenic or nociceptive pa2n
we must use animal model-2
• Thrombospondin is a matrix protein that plays a role in activation of latent TGF-
• Activated TGF-promotes Treg and inhibits Th-17 (IFN-
• Thus, TSP (null) has high levels of Th-17, IL-17 and IFN-
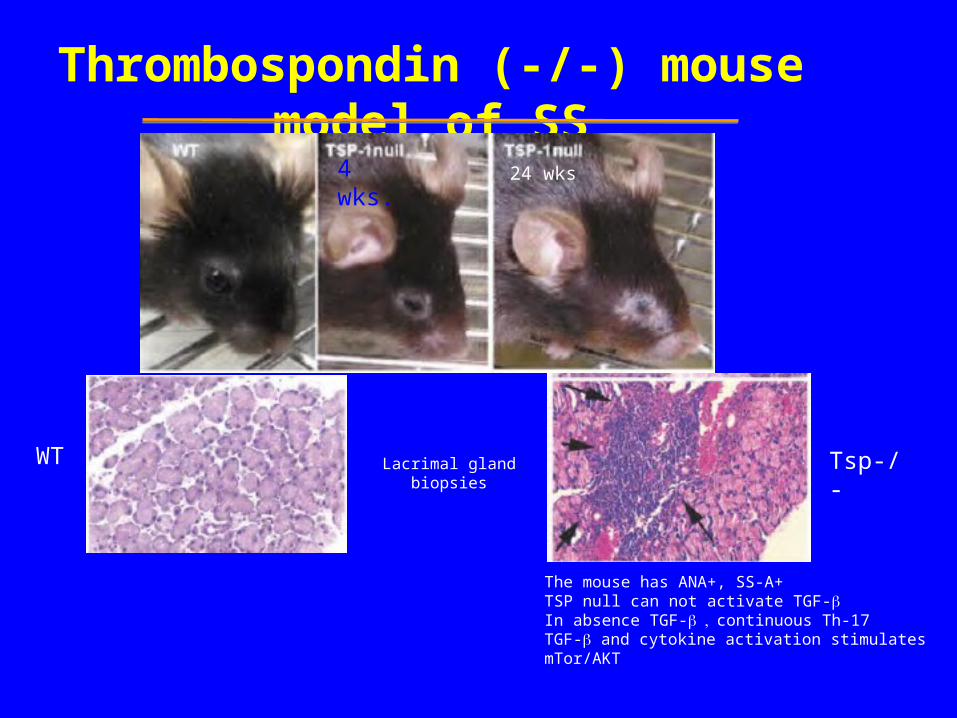
Thrombospondin (-/-) mouse model of SS
4 wks.
Lacrimal gland biopsies
The mouse has ANA+, SS-A+TSP null can not activate TGF-In absence TGF-continuous Th-17TGF- and cytokine activation stimulates mTor/AKT
WT Tsp-/-
24 wks
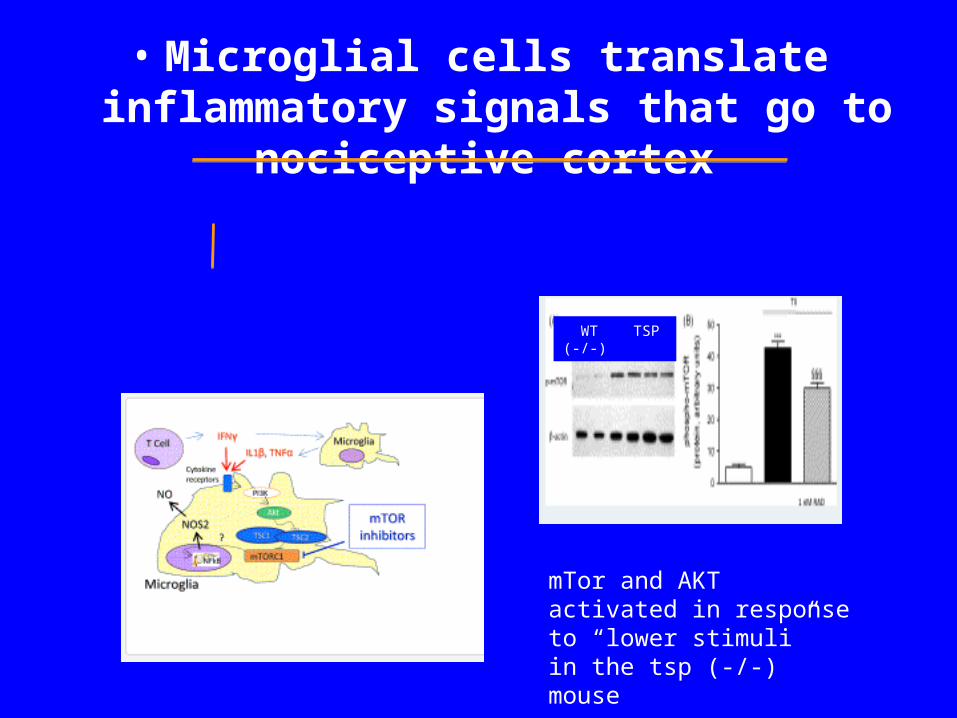
At the level of the Vth nerve(Tsp -/- mouse)
• Microglial cells translate inflammatory signals that go to nociceptive cortex
WT TSP (-/-)
mTor and AKT activated in response to “lower stimuli”in the tsp (-/-) mouse
The tsp-null mouse allows us to look at the interaction of peripheral inflammation
and microglial cells-1
• Activation of microglial cells through mTor/AKT.
• In absence of thrombospondin, constitutive activation of Th17 and IFN-activates microglial cells.
Take home lesson for Rheumatologists:
There is more to pain in SS than peripheral inflammation.
• Nociceptive (pain) pathway occurs through smad3 and non-smad pathways that involve mTor/AKT pathways in cranial nerve V.
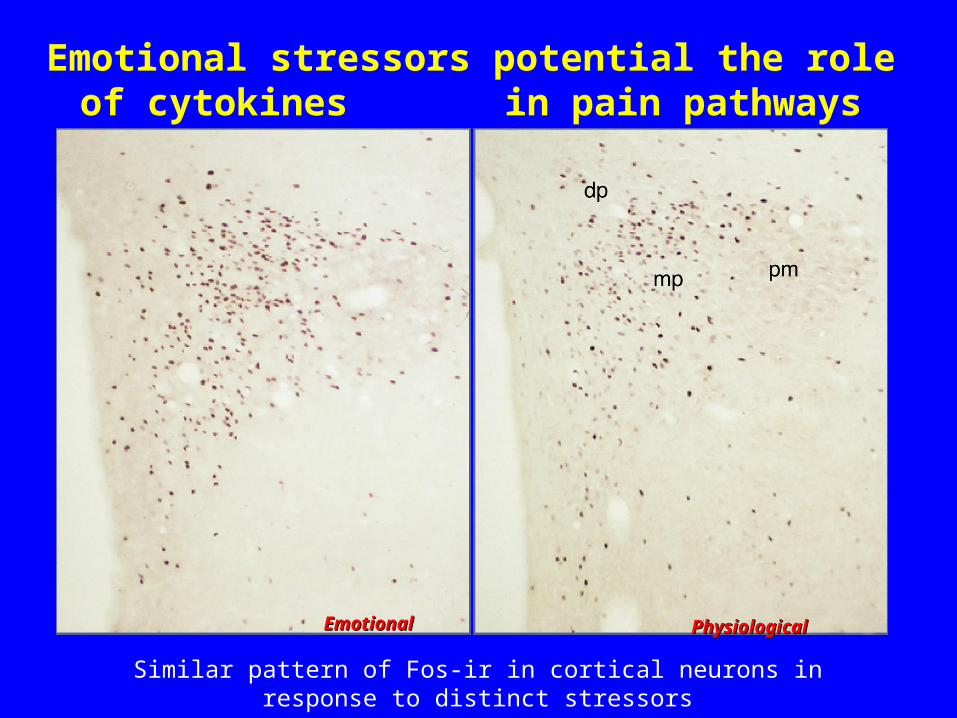
Emotional stressors potential the role of cytokines in pain pathways
EmotionalEmotional PhysiologicalPhysiological
Similar pattern of Fos-ir in cortical neurons in response to distinct stressors
Summary-1
1. Functional circuit needs to be considered when assessing “benign” symptoms of corneal or oral pain.
2. Symptoms of oral/ocular pain do not correlate with markers of systemic inflammation (ESR/CRP) because the events are contained within the brainstem and cortex.
Summary-2
3. Afferents go to midbrain regions of Cranial Vth.
4. Microglial cells are site of cytokine/neurokine interaction
5. Receptors and neurokines from microglial cells are therapeutic targets.
Summary-3
6. Novel targets include mTor and AKT pathways
7. These mTor/AKT pathways also implicated in chronic pain and depression—so we must collaborate with these neurochemists.
Summary-4
8. Cortical “memory” of nociceptive pain is well described in neurologic literature.
9. fMRI indicates that nociceptive pain is the cause of benign symptoms in SS that do not correlate with acute phase reactants
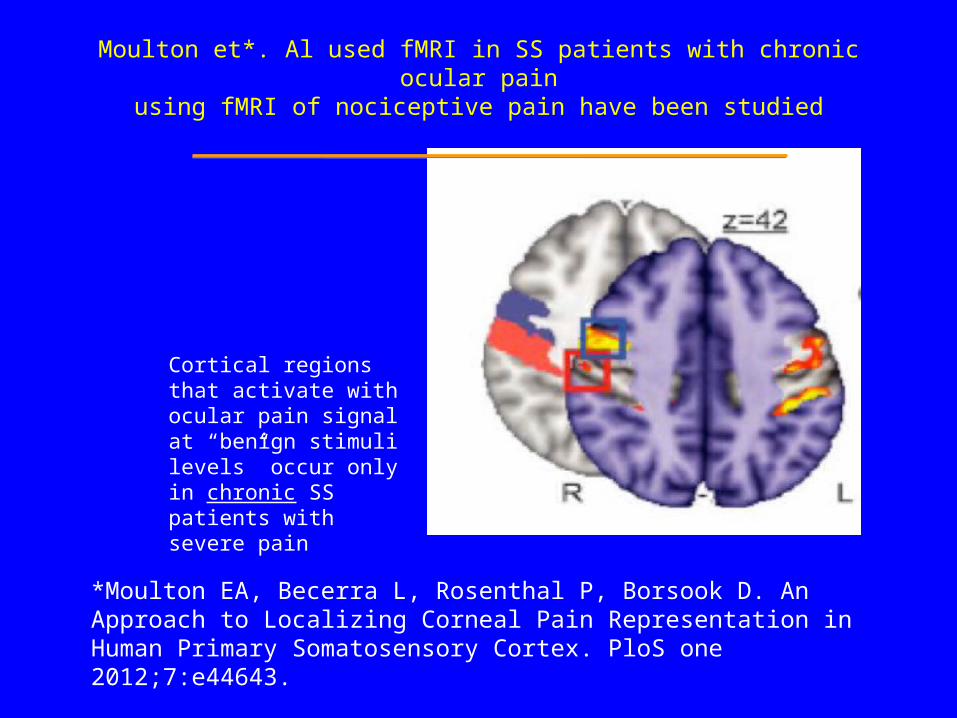
Moulton et*. Al used fMRI in SS patients with chronic ocular painusing fMRI of nociceptive pain have been studied
Cortical regions that activate with ocular pain signal at “benign stimuli levels” occur only in chronic SS patients with severe pain
*Moulton EA, Becerra L, Rosenthal P, Borsook D. An Approach to Localizing Corneal Pain Representation in Human Primary Somatosensory Cortex. PloS one 2012;7:e44643.
Summary-5
10. We have made advances in “systemic inflammation” and these are encouraging.11. For “drug licensing” we will also need to improve the patients “quality of life” symptoms of dryness, pain and fatigue12. We need for “autoimmune” divisions to
work with “neuro-chemistry” research divisions.
Thank you
for inviting me to participate in this wonderful meeting.
We will discuss treatment of dryness of eyes and mouth during afternoon session.
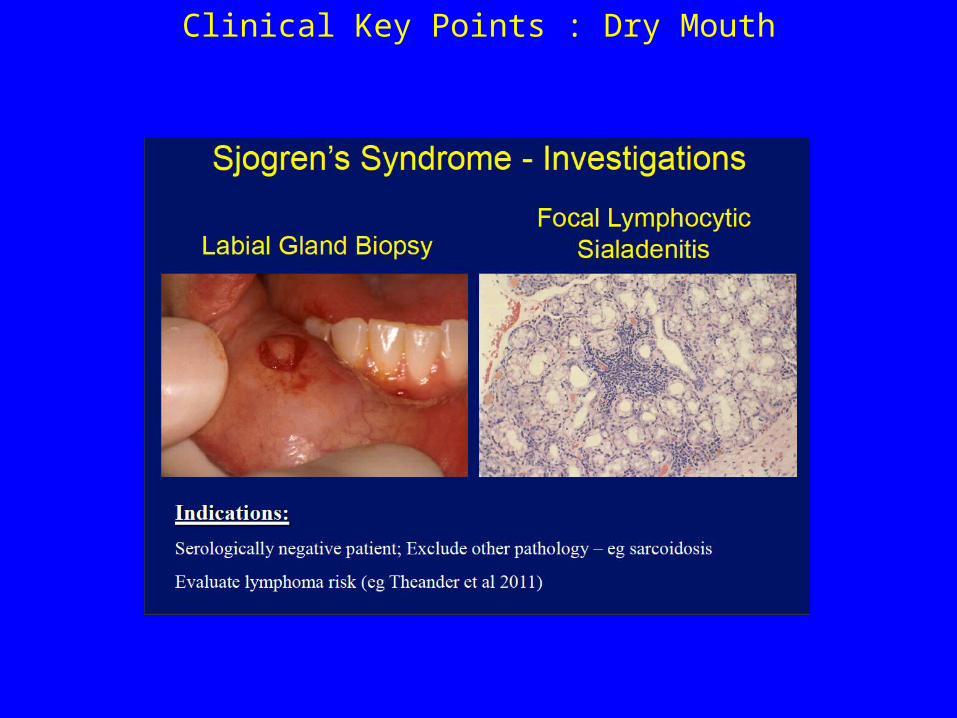
Clinical Key Points : Dry Mouth
Dry and Painful Mouth-1
• If you thought that Dentists did not care about SS, then wait until you see their Dental Care Plans --
The answer to all problems is a $25,000 tooth implant.
Dry and Painful Mouth-2
• Must treat underlying oral candida (which is erythematous spots on roof of mouth) before anything will work.
• Candida often lurks under dentures–
• Patients would rather run naked through clinic than remove a denture.
Dry and Painful Mouth-3
• Angular cheilitis the most obvious hint.
• Treatment of oral candida is a slow process involving multiple steps.
• Use website for education.
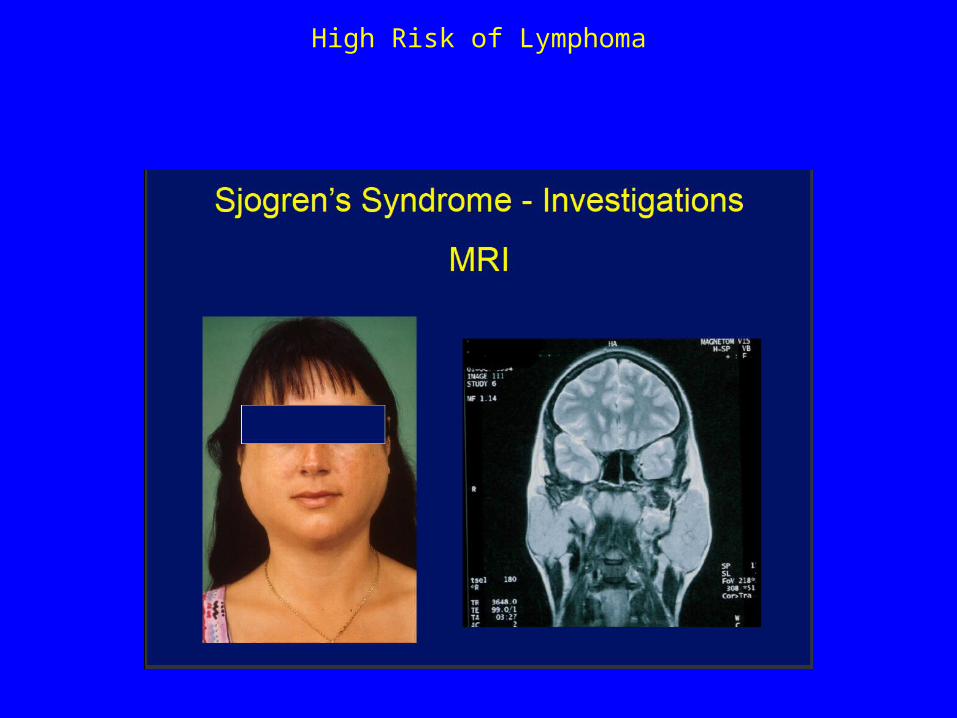
High Risk of Lymphoma
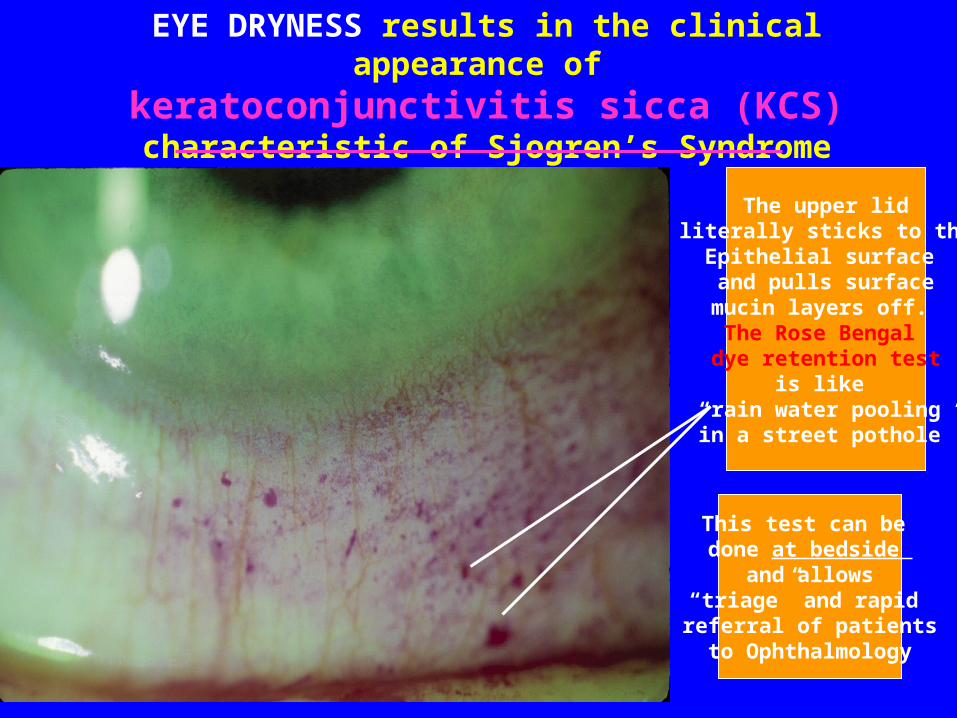
EYE DRYNESS results in the clinical appearance of keratoconjunctivitis sicca (KCS)characteristic of Sjogren’s Syndrome
The upper lidliterally sticks to theEpithelial surface and pulls surfacemucin layers off. The Rose Bengal dye retention test
is like “rain water pooling in a street pothole”
This test can be done at bedside
and allows“triage” and rapid referral of patientsto Ophthalmology


Rash distinct from SLE(erythema annulare)
Arthritis distinct from RA
We are also looking atAdditional Targets of Interests
• Chemokines and their receptors (CCR) on vascular cells and lymphocytes
• TLR receptors: SLAC-15 that links Toll receptor and type 1 IFN• Methylation modulators and siRNA• Neural mediator circuits:• Receptors on cornea--substance P (TRPV1), VIP and CGRP pain
receptors• TRPM8, TRPA1, and CGRP in trigeminal ganglion neurons• Trigeminal ganglion neurons- MCP-1, MIP-2,• CCR and CCL at the blood brain barrier
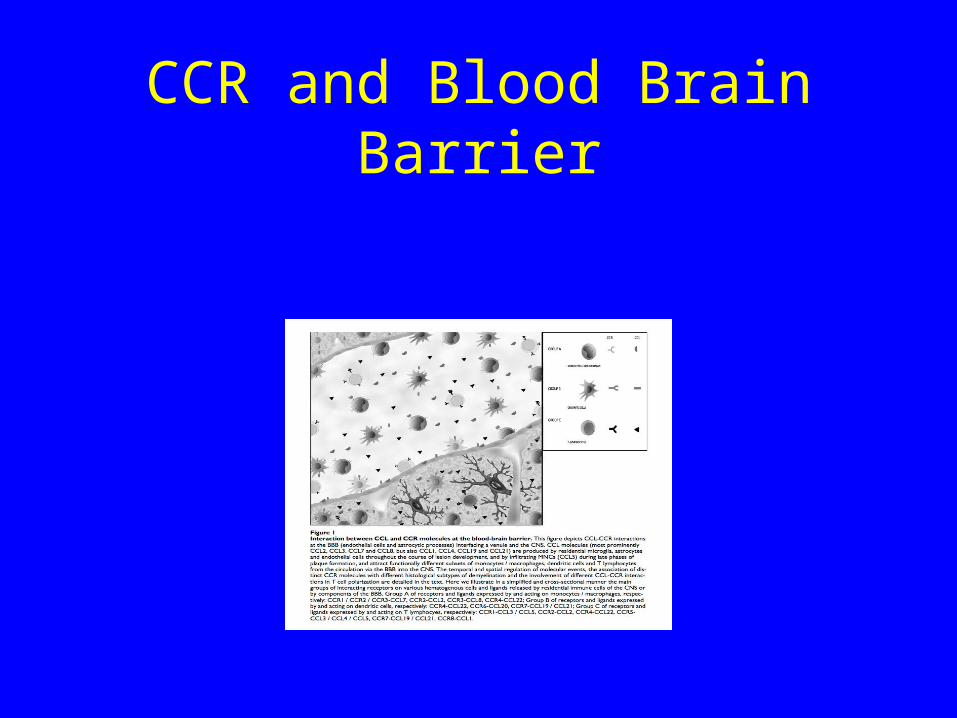
CCR and Blood Brain Barrier
The tsp-null mouse allows us to look at the interaction of peripheral inflammation and microglial cells
• Activation of microglial cells through mTor/AKT
• In absence of thrombospondin, constitutive activation of Th17 and IFN-activates microglial cells
• Nociceptive (pain) pathway occurs through smad3 and non-smad pathways that involve mTor/AKT pathways in cranial nerve V

The main cytokine targets match those identified in genome wide screens*
• HLA-DR (T-cell), CTLA and IFN-• NF-K /IkB
• Homing receptor (CXCR5)
• Type I IFN –IRF5, STAT4, TLR3/7/9 and pkR (cytoplasmic sensor)
• B-cell activation –BLK, BAFF, IL12, and A20 (TNFAIP3)
• * Most of these targets do not map to the encoded protein but to upstream sites of RNA transcription that are not translated (presumed epigenetic sites such as methylation)
Previously Studied in SS
• Anti-CD20 –glandular and extraglandular
• BAFF (Blys)-ACR 2012 abstracts*
• Abatacept (CD40 L)-ACR 2012
• Allogeneic mesenchymal cells-ACR 2012 abstracts and article in Blood
• www.rheumatology.org/wren/acrsearch.asp?zoom_query=acr%20abstracts%202012&st=nocache&actn=search&dt=12/24/2012%202:29:59%20P
Other Inhibitors of IFN
a. Initial trials of anti-type 1 IFN had infusion reactions and only
modest efficacy
b. Medi 546 (type 1 IFN-R antagonists) now in phase 1 (scleroderma) and juvenile SLE phase 2 trial
Dry and Painful Mouth-4
• Different toothpastes and mouth • rinses (again, use websites for • education).
• Avoid mouth breathing by keeping • sinuses open.
• Use cool water humidifiers, air purifiers • at bedside at night.