Embed Size (px)
Citation preview

C L I N I C A L / T E C H N I C A L
24 oralhealth July 2007
Sudden loss of an anterior toothis a catastrophic event for apatient. The missing anterior
tooth has implications in how onepresents themselves to others andthe psychological effects of howwe feel about ourselves. Suddentooth loss in the esthetic zone ofthe anterior region can be due totrauma, periodontal disease, orendodontic failure. If the tooth isintact, it is easiest to use thattooth as a natural tooth ponticand bond it to the adjacent teethwith fiber reinforcement ribbonand adhesive composite resin.When the tooth is not usable adenture tooth or a composite resinpontic can be shaped to fit thespace of the missing tooth.
In the past there have been anumber of different techniquesdescribed in the restorative den-tistry literature for splinting
teeth and adding a natural toothpontic, denture tooth, or compos-ite resin tooth pontic. These pon-tics were connected to the adja-
cent teeth with adhesive compos-ite resins, wire, metal mesh,nylon, mesh and cast metalframeworks bonded to the adja-cent teeth.1-6 The inherent prob-lems with these materials when
placing a tooth pontic fixed to theadjacent teeth when replacing amissing tooth were their inabilityto be chemically incorporated intothe dental resin. Clinical failuresof these bridges were prevalentbecause these materials could notsupport the repeated loadingstresses placed on the bridge dur-ing normal and para-function.Another problem associated withthe placement of composite resinsplints with submerged wires andmesh grids that in order to pro-tect against breakage more bulkand thickness of composite resinwas necessary.7,8 This overbulk-ing of the restoration led to anincrease in food and plaque reten-tion resulting in making it moredifficult to clean around therestoration and maintain goodoral health.
The challenge to place a thin
Single Visit Natural Tooth Pontic Bridge with Fiber Reinforcement Ribbon
Howard E. Strassler, DMD, David Taler, and Luis Sensi, DDS, PhD
Sudden tooth loss in the esthetic zone
of the anterior regioncan be due to trauma,periodontal disease, or endodontic failure.

but strong, bonded compositeresin-based single visit bridgewas met with the introduction ofa high strength polyethylene,bondable, biocompatible, esthetic,easily manipulated, fiber ribbonsthat could be embedded into aresin structure. This author hasbeen using one brand of fiberreinforcement ribbon, RibbondReinforcement Ribbon, for almost13 years with good success.Ribbond is a bondable, polyethyl-ene, lock-stitch multidirectionalreinforcement ribbon for compos-ite resin. It has been reportedthat the lock-stitch weave of Rib-bond and Ribbond THM are easi-er for clinician’s to manipulateand use when compared to otherfiber materials. Also, research hasdemonstrated that the fiber rein-forcement architecture with Rib-bond Reinforcement Ribbons pro-vides for an increase in flexuralstrength and flexural modulus ofcomposite resins that resistscracking.9-11
One problem with glass fiberreinforcement materials, is thatthe glass fibers break and pullout of the composite resin whenthe composite develops a crackthat propagates to the glassfibers.12 In the case of a lock-stitch weave with a polyethylenefiber, the cracks stops at the nodeof the leno-lock-stitch weave ofthe fiber ribbon helping maintainthe integrity of the fiber rein-forcement.11 Karbhari and Stras-sler tested a variety of differentfiber reinforcement materials.
Their conclusion was that it iscrucial that the appropriateselection of fiber architectures bemade not just from a perspectiveof highest strength, but overalldamage tolerance and energyabsorption. Differences in weavesand architectures can result insubstantially different perfor-mance and appropriate selectioncan mitigate premature and cata-strophic failure.
The study provides details ofmaterials level response charac-teristics which are useful in selec-tion of the fiber reinforcementbased on specifics of applica-
tion.11 In a long term clinicalevaluation of splinting using theoriginal Ribbond ReinforcementRibbon including single visitbridges it has been reported thatover a period of 42-96 months(mean = 68.6 mos.) fiber rein-forced composite resins are highlysuccessful.12 Other clinically suc-cessful uses for fiber reinforce-ment ribbon have been describedin the dental literature including
periodontal splinting,13,14 restor-ation of the endodontically treat-ed tooth15,16 and for cross splint-ing teeth with large compositerestorations.17
When selecting reinforcementfiber ribbon to use in naturaltooth pontic single visit bridgesthe Ribbond offers not only excel-lent composite resin reinforce-ment but also ease of use and anassortment of widths of the fibersto manage a wide variety of clini-cal situations. The Ribbond’sunique and patented fiber weaveimparts a multidirectional rein-forcement to polymeric restora-tive resins.11,18
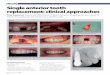
CASE REPORTA 48-year-old woman presented tothe dental school to participate ina periodontal research study. Aspart of the study any teeth with ahopeless prognosis would be ex-tracted. The patient had a chiefcomplaint of pain from the man-dibular left central incisor. Thetooth was very mobile (grade 3mobility) and was sensitive topercussion and palpation. Thedistofacial and distolingual sur-faces had periodontal probings of8 mm. Radiographs were takenand revealed severe bone loss(Fig. 1). The diagnosis was severeperiodontal disease and a peri-odontal abscess on the centralincisor (Fig. 2). The tooth had ahopeless prognosis and wasscheduled to be extracted. Theother mandibular incisors had agrade 2 mobility. As part of the
C L I N I C A L / T E C H N I C A L
July 2007 oralhealth 25
The tooth had a hopeless prognosis and was scheduled to be extracted.
FIGURE 1—Radiograph of severe peri-odontal bone loss on the mandibular leftcentral incisor.
FIGURES 2A & B—A) Facial view of the periodontally compromised central incisor. B)Lingual view of the periodontally compromised incisor.

therapy, the anterior teethwere scaled and root planed.The patient told us that shehad an important family eventand asked if there was any waythe tooth could be replaced thesame day it was removed. Thedecision was made to extractthe tooth and fabricate a singlevisit, bonded fiber ribbon rein-forced bridge using the crownof the extracted tooth as a nat-ural tooth pontic that wouldalso serve as a periodontalsplint.
The tooth was removed andthe extraction site had pres-sure applied with gauze for 30minutes to control the bleeding(Fig. 3). Before placement ofthe dental dam, the length ofthe natural tooth pontic wasdetermined by measuring thedistance from incisal edge ofthe central incisor to theextraction site. Some addition-al length was added so the pon-tic would be touching the gingi-val tissue when the extractionsite healed. The extracted toothwas measured with a periodon-tal probe to the length needed.The root was cut from the crownwith a 556 bur (SS White Burs)and then shaped with a flame-shaped finishing bur (SS WhiteBurs). The opening in the rootwhere the root canal was presentwas filled with a bonded compos-ite resin and the gingival aspectof the tooth was smoothed andshaped to be rounded.
To increase the bulk of compos-
ite resin at the connector areabetween the pontic and abutmentteeth and to create room for a dou-ble thickness of reinforcementfiber ribbon a channel with awidth of 3-4mm was cut in the lin-gual surface (Fig. 4). This was thesame width as the 3mm wideRibbond THM ReinforcementRibbon that was to be used forbonding and reinforcing the com-posite resin where the teeth were
to be connected. A dental dam wasplaced. The dental dam did nothave a hole punched for the tooththat was removed so that bleedingwould not contaminate the areabeing bridged during the bondingprocedure (Fig. 5).
The teeth were cleaned on thefacial and lingual surfaces usinga prophylaxis cup with a non-flu-oridated pumice paste. After the
C L I N I C A L / T E C H N I C A L
26 oralhealth July 2007
FIGURE 3—Facial view after extraction ofthe central incisor.
FIGURE 5—Placement of dental dam withno hole punched for extracted tooth.
FIGURE 7—Lingual view of Class 3 prep-arations on the abutment teeth for thebridge.
FIGURE 6—Diamond preparing facialinterproximal areas of incisors.
FIGURE 8—Dental floss placed on thefacial surfaces of the anterior teeth forthe length needed for the Ribbond THMReinforcement Ribbon.
FIGURES 4A & B—A) Extracted mandibular left central incisor. B) Natural tooth ponticafter filling in root canal space, shaping the root surface to be the pontic and plac-ing the lingual channel in the tooth crown.

C L I N I C A L / T E C H N I C A L
July 2007 oralhealth 27
teeth were thoroughly rinsed and dried, theinterproximal surfaces and contact areas of theteeth were cleaned and prepared with a mediumgrit gapped finishing strip (Soflex GappedFinishing Strips, 3M-ESPE). To improve stabi-lization of these periodontally mobile teeth andto minimize the thickness of the splint on theaesthetic interproximal aspect of the facial sur-faces of #22-27, a thin diamond (Pirana dia-mond, SS White Burs) with a high speed hand-piece with water spray was used to barrel intothe interproximal areas (Fig. 6).
Later, composite resin will be placed on thesefacial surfaces to improve cross stabilization ofthe teeth. The mesiolingual surface of the leftlateral incisor and mesiolingual surface of theright central incisor had Class 3 preparationsmade to further reinforce the bridge connectors
and create room for a double piece of fiber rein-forcement ribbon once the pontic was placed(Fig. 7). A double piece of fiber ribbon with com-posite resin placed in between both ribbons pro-vides additional strength and stability whenplacing a pontic by creating a laminated compos-ite beam.32
Ribbond THM Reinforcement Ribbon wasselected for the natural tooth pontic bridge-splint because of the research demonstratingexcellent physical properties when embeddedinto dental composites 27,28 and clinical successwith this reported technique.29 Because all theremaining mandibular incisors were mobile dueto periodontal disease, it was decided that all thelower incisors would be splinted with the fiberribbon to the canines. To measure the length offiber ribbon needed, a piece of dental floss wasplaced on the facial surfaces of the teeth, extend-ing from the mesial of the left mandibularcanine to the mesial of the right mandibularcanine (Fig. 8).
Another technique to determine the length offiber ribbon to be used, is to take the patient’s
The plasma-treated polyethylene fibers are susceptible to surface
contamination.

C L I N I C A L / T E C H N I C A L
July 2007 oralhealth 29
diagnostic casts and measure dental floss to thelingual surface of the anterior teeth on the cast.The plasma-treated polyethylene fibers are sus-ceptible to surface contamination. Therefore,when handling Ribbond a clean cotton pliers wasused. Using the floss as a template, a piece of3mm-wide Ribbond THM was taken from itspackage using the cotton pliers and cut to anequal length with the Ribbond scissors (Fig. 9).
It is important that the scissors supplied withthe Ribbond be used, because other scissors andeven a sharp scalpel will have difficulty provid-ing for a clean cut of the tough polyethylenefibers of the Ribbond THM. Another piece ofRibbond THM with a length from the mesial ofthe right mandibular central incisor to themesial of the left mandibular laterial incisor wasalso cut. This smaller piece would be placed inthe cavity preparations first to help strengthen
and reinforce the pontic connectors with theadjacent teeth. Once cut to length, to make thefiber ribbons more bondable to the restorativecomposite both fiber ribbons were wetted with anadhesive resin (SingleBond, 3M-ESPE). To evap-orate solvent from the adhesive resin, air wasblown on the ribbon for 10 seconds. Once the rib-bon fibers were wetted, they were blotted using apaper napkin to remove excess adhesive resin.
Once wetted with adhesive resin, Ribbond canbe handled like any resin material. The ribbonwas put aside and covered to avoid light until itwas ready to be placed on the teeth. The naturaltooth pontic was etched with a phosphoric acidetchant for 15 seconds, rinsed with water anddried. SingleBond adhesive was painted on theetched surfaces and into the prepared channel onthe lingual surface. It was also put aside until itwas time to bond it to place.
The teeth adjacent to the pontic in the mouthwere etched for 30 seconds with a 32% phosphor-ic acid gel being certain that etchant was placedon the lingual and facial surfaces (Fig. 10). The
The ribbon was put aside and covered to avoid light
until it was ready to be placed on the teeth.

C L I N I C A L / T E C H N I C A L
30 oralhealth July 2007
teeth were then rinsed with anair-water spray for 10 secondsand gently dried. A resin adhe-sive, SingleBond was applied tothe etched enamel surfaces, thetooth preparations and facialinterproximal areas, using a dis-posable brush. A medium viscosi-ty micromatrix hybrid compositeresin in preloaded tubes (PrismaTPH3, Dentsply/Caulk) was dis-pensed onto the facial surfaces ofthe mandibular left lateral incisorand right central incisor. Thetooth pontic was picked up with acotton pliers and placed in thearea where it was extracted withthe root side pushing into the rub-ber dam and incisal edge heightat the same height as the adja-cent central incisor (Fig. 11). Thefacial surfaces were light curedfor 20 seconds (Fig. 12).
The Class 3 preparations andthe channel in the natural tooth
pontic were prepared again to becertain the channel and Class 3preparations were in line and thesurfaces were ready to be etchedagain. The remaining teeth on thefacial interproximal and lingual
surfaces were etched with thephosphoric acid etchant for 30 sec-onds, rinsed with an air-waterspray and dried. Interproximalmatrix strips were placed at themost distal surfaces of mandibu-
lar canines to maintain separa-tion. In the past, wedges wereplaced to minimize excess compos-ite in the gingival interproximalembrasure areas. With wedgesthere is always the potential thathighly mobile teeth could besplinted in a different position. Aninnovative technique for minimiz-ing excessive composite resin inthese areas has been described.36
The technique is the place-ment of a medium or heavy vis-cosity polysiloxane impressionmaterial using an impressionsyringe in these gingival embra-sure areas. It is important thatthe impression material is placedafter tooth etching, rinsing anddrying to avoid the trapping ofmoisture that can occur if thetechnique is done earlier. Thisuse of elastomeric impressionmaterial assures a passive place-ment of the blockout. For this
FIGURE 9—Using special Ribbond scis-sors, the Ribbond THM has been cut tolength of dental floss template.
FIGURE 10—The facial interproximal ofthe abutment teeth were etched withphosphoric acid.
FIGURE 11—After etching, adhesive andcomposite resin placement on facial sur-faces, natural tooth pontic of lateral incisorplaced between the right central incisorand left lateral incisor using cotton pliers.
FIGURE 12—Pontic was light cured to sta-bilize it for the continued procedure.
FIGURE 13—After etching and rinsing allthe remaining teeth to be restored, amedium-bodied polysiloxane was placedas blockout into the gingival embrasurespaces.
FIGURE 14—Composite resin placed onthe facial interproximal surfaces.
In the past, wedges were placed to minimize excess composite in the
gingival interproximalembrasure areas.

C L I N I C A L / T E C H N I C A L
July 2007 oralhealth 33
case, a medium bodied fast set-ting poly vinyl siloxane impres-sion material (ExaMix, GCDental) was syringed into thegingival embrasure spaces (Fig.13). The remaining facial inter-proximal surfaces had compositeresin placed, shaped and lightcured for 20 seconds (Fig. 14). Thefacial composite resin serves toseal the interproximal areasagainst recurrent caries and pro-vides an 180° wrap of compositeresin to each of the splintedteeth. This will stabilize each
tooth and prevent breakage of thefinal splint-bridge. This step isimportant because once splinted,the interproximal surfaces can-not be adequately cleansed.
Composite resin was placed onthe facial interproximal surfacesand shaped to minimize excessand light cured. The purpose ofthis facial composite resin is toseal the interproximal areasagainst recurrent caries and toprovide for a 180° wrap of com-posite resin to each of the splint-
ed teeth. This will function asa cross-splint of each tooth toprevent tooth movement andbreakage of the final splint.This step is important becauseonce splinted, the interproxi-mal surfaces of adjacent teethcan not be cleaned adequately.The composite resin was thenplaced onto the lingual surfacefrom mid-canine to mid-canine. By placing the pre-loaded tube tip at a rightangle to the lingual surfaces ofthe teeth, the composite resin
was placed in the middle of theteeth and into the lingual grooveprepared in the natural toothpontic (Fig. 15).
The shorter piece of the 3mm-wide Ribbond THM ribbon waspicked up and embedded into thecomposite resin so that it couldbe placed into the Class 3 prepa-rations and lingual channel inthe natural tooth pontic.Additional composite must becovering the fiber ribbon so thatwhen the longer fiber ribbon was
FIGURE 15—Composite resin placed onthe lingual surfaces and into the Class 3preparations and lingual groove in nat-ural tooth pontic.
FIGURE 16—The ribbon was placed andfurther adapted using a burnisher.
FIGURE 17—After fiber ribbon placementembedding the ribbon into the compos-ite resin so it is well adapted to the lin-gual tooth surfaces.
FIGURE 18—Using a thin plastic filling instrument, the fiber reinforcement ribbon isclosely adapted to the lingual surfaces pushing the fiber ribbon deep into the inter-proximal areas.
FIGURE 19—Flowable composite resinplaced over the top of the ribbon.
FIGURES 20A & B—A) Lingual view of final esthetic result of the natural tooth ponticbridge reinforced with Ribbond THM and bonded composite resin. B) Facial viewof the natural tooth pontic bridge reinforced with Ribbond THM and bonded com-posite resin.

C L I N I C A L / T E C H N I C A L
34 oralhealth July 2007
placed on the lingual surface from canine to canineit would be as a double thickness of fiber at theconnector between the pontic and adjacent teeth.This double thickness creates a beam effect fur-ther reinforcing the composite resin at the connec-tors. The fiber ribbon is placed on the other lingualsurfaces so it would be at mid-tooth.
Using plastic filling instruments and burnish-
ers the Ribbond THM was embedded into the com-posite resin starting at the left canine and movingaround the arch to the right canine (Fig. 16).Using a gloved finger wetted with adhesive resinthe ribbon is further pushed into the compositeresin so it is covered with composite. The ribbonwas further adapted on the lingual and interprox-imal surfaces using a cotton pliers and plastic fill-ing instrument. It is important that the ribbon beas closely adapted to the lingual surfaces of theteeth as possible (Fig.17).
Figure 18 demonstrates the placement of theRibbond fiber reinforcement ribbon by holdingthe wetted Ribbond into position with a finger ofinstrument against the tooth to avoid pulling outthe fiber that has been closely adapted to theteeth and pushed deep into the interproximalareas of the teeth. Excess composite resin wasremoved before light curing. The lingual surfaceswere then light cured for 20 seconds for eachtooth to be certain that the ribbon and compositeresin were completely cured.
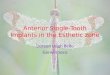
At this time the ribbon may be visible and notcompletely covered with an adequate thickness ofcomposite resin, as was the case with this patient.For this reason a high strength, wear resistant,flowable composite resin (Gradia Flowable, GCDental) was applied to smooth the irregular lingualsurface and provide an even thickness of compositecovering the ribbon (Fig. 19). The flowable compos-ite resin on the lingual surface was light cured foran additional 10 seconds for each tooth. The com-posite resin was shaped, finished, and polished toremove any excess restorative material and achievean aesthetic result. This was accomplished withfinishing diamonds on a high speed handpiece.
The composite resin was further finished usingaluminum oxide impregnated silicone composite
FIGURES 21A & B—A) Lingual view of fiber reinforced splint-bridge at 6 months. B) Facial view of fiber reinforced splint-brige at6 months.

C L I N I C A L / T E C H N I C A L
36 oralhealth July 2007
resin polishing points (Enhance,Dentsply/Caulk. The compositeresin was then polished using acomposite resin polishing paste.The rubber dam was removedand the splint was checked forocclusion and aesthetic appear-ance. It is important to adjustthe occlusion because the naturaltooth pontic has been placed inan esthetic position. For thispatient, the tooth position beforeextraction was above the incisalplane. At placement, the incisaledge was placed to be inline withthe other incisal edges.
Since the teeth are now joinedtogether, it is important that thepatient have demonstrated tothem techniques and devices forcleaning the gingival embrasureareas. The patient was shown theuse of a proximal brush to cleanthe embrasure areas. For thispatient, the final result is a toothin the place on the same day asthe extraction (Fig. 20). The nat-ural tooth pontic fixed partialdenture is functioning well sixmonths after placement. (Fig. 21.)
CONCLUSIONThe research has demonstratedgood durability for the techniquedescribed in this article.
This author’s experience is thatusing this technique — the groovein the pontic on the lingual surface,Class 3 preparations on the adja-
cent teeth and composite resin onthe facial interproximal surfaces,these bridges can provide a patientwith many years of service. OH
Howard E. Strassler, DMD isProfessor and Director of OperativeDentistry, Department of Endodon-tics, Prosthodontics, and Operative
Dentistry, University of MarylandDental School, Baltimore, Maryland.
David Taler is a dental student atthe University of Maryland DentalSchool, Baltimore, Maryland.
Luis Sensi, DDS, PhD, AssistantProfessor, Department of Endodontics,Prosthodontics, and Operative Den-tistry University of Maryland DentalSchool, Baltimore, Maryland.
Oral Health welcomes this originalarticle.
REFERENCES1. Ibsen RL. One-appointment technique using an adhe-
sive composite. Dental Survey. P. 20-22, February, 1973.2. Jordan RE, Suzuki M, Sills PS, et al. Temporary fixed
partial dentures fabricated by means of a acid-etchresin technique: a report of 86 cases followed up to 3years. J Amer Dent Assoc 96:994-1101, 1978.
3. Miller TE, Barrick JA: Pediatric trauma and polyethylenereinforced composite fixed partial denture replacements:a new method. J Canad Dent Assoc 59:252-59, 1993
4. Lee GTR. Utilization of a natural tooth in acid-etchbridging. J Dent Child 55:201-204, 1988.
5. Livaditis GJ and Thompson VP. Etched castings: animproved retentive mechanism for resin-bondedretainers. J Prosthet Dent. 47:52-58, 1982
6. Breault LG, Manga RK. The reinforced tooth pontic.General Dent 45:474-476, 1997.
7. Strassler HE, Haeri A, Gultz J. New generation bond-ed reinforcing materials for anterior periodontal toothstabilization and splinting. Dent Clin North Am43(1):105-126, 1999.
8. Pollack RP. Non-crown and bridge stabilization ofseverely mobile, periodontally involved teeth- a 25 yearperspective. Dent Clin North Am 43(1):77-103, 1999.
9. Christensen G: Reinforcement fibers for splintingteeth. In CRA Newsletter 21(10):1, 1997.
10. Strassler HE, Karbhari V, Rudo D. Effect of fiber rein-forcement on flexural strength of composite. J DentRes (Special Issue), 80:221, (abstract no. 854), 2001.
11. Karbhari VM, Strassler H. Effect of fiber architecture onflexural characteristics and fracture of fiber-reinforcedcomposites. Dent Mater. 2006 epub Nov 7, 2006 in Press
12. Karbhari VM, Rudo DN, Strassler HE. The developmentand clinical use of leno-woven UHMWPE ribbon in den-tistry. Proceedings of the Society for Biomaterials.(abstract issue), 29:15 (abstract no. 529), 2003.
13. Strassler HE, Tomona N, Spitznagel JK Jr. Stabilizingperiodontally compromised teeth with fiber-reinforcedcomposite resin. Dent Today. 22(9): 102-9, 2003.
14. Strassler HE, Brown C. Periodontal splinting with athin high-modulus polyethylene ribbon. CompendContin Educ Dent. 22:696-704, 2001.
15. Newman MP, Yaman P, Dennison J, Rafter M, Billy E.Fracture resistance of endodontically treated teethrestored with composite posts. J Prosthet Dent, 89:360-367, 2003.
16. Belli S, Erdemir A, Yildrirm C. Reinforcement effect ofpolyethylene fibre in root-filled teeth: comparison of tworestoration techniques. Int Endod J. 39:136-42, 2006.
17. Belli S, Cobankara FK, Eraslan O, Eskitascioglu G,Karbhari V. The effect of fiber insertion of fracture resis-tance of endodontically treated molars with MOD cav-ity and reattached fractured lingual cusps. J BiomedMater Res B Appl Biomater 79:35-41, 2006.
18. Rudo DN, Karbhari VM. Physical behaviors of fiberreinforcement as applied to tooth stabilization. DentClin North Am. 43(1):7-35, 1999.
19. Hughes TE, Strassler HE. Minimizing excessive com-posite resin when fabricating fiber-reinforced splints. JAmer Dent Assoc, 131:977-979, 2000.
Since the teeth arenow joined together, it is important that the patient havedemonstrated to
them techniques anddevices for cleaning
the gingival embrasure areas.