Embed Size (px)
Citation preview

Single fiber electromyography (SFEMG) measurements of fiber density and jitter are used in the diagnosis of a variety of peripheral nervous system dis- orders. However, the normal values of these measurements for most mus- cles and age groups are not well documented in the literature. We present a retrospective and prospective multicenter collection of SFEMG jitter and fiber density data from control subjects obtained for the purpose of defining reference values for many muscles and different ages. The data and calcu- lated upper limits for fiber density, individual pair jitter, and mean jitter are presented for each muscle in tabular and graphical format, for different age groups. Key words: jitter fiber density mean MCD single fiber electromyography
reference values MUSCLE & NERVE 151151-161 1992
SINGLE FIBER EMG REFERENCE VALUES: A COLLABORATIVE EFFORT
AD HOC COMMITTEE* OF THE AAEM SPECIAL INTEREST GROUP ON SINGLE FIBER EMG, JAMES M. GILCHRIST, MD, COORDINATOR
Since its development b Stalberg and Ekstedt nearly three decades ago,' single fiber electromy- ography (SFEMG) has been used by an increasing number of practitioners, and is recognized as an excellent method for detecting abnormal neuro- muscular transmi~sion.~ Fiber density (FD) mea- surement by SFEMG is useful in neuropathic dis- orders as an electrophysiological manifestation of reinnervation.6 Because SFEMG is time consum- ing, it is difficult for practitioners to collect SFEMG reference values for their own laborato- ries. Most electromyographers use values from a few muscles in younger subjects (see Stalberg and
*L/st of participants: Coordinator-James M Gilchrist, MD, Department of Neurology, Brown University. Providence, RI; (in alphabetical order) Paul E. Barkhaus. MD, Department of Neurology, Minneapolis VA Medi- cal Center, Minneapolis, MN, Vera Bril, MD, Division of Neurology, Tor- onto General Hospital. Toronto, Ontario, Canada; Jasper Daube, MD, Department of Neurology, Mayo Clinic, Rochester, MN; Jo DeMeirsman, MD, Department of Physical Medicine and Rehabilitation, University of Leuven, Leuven, Belgium; James F Howard, Jr., MD, Department of Neurology, University of North Carolina, Chapel Hill, NC; Charles Jablecki, MD. Department of Neurosciences, University of California at San Diego, San Diego. CA; Donald B Sanders, MD, Division of Neurol- ogy, Duke University, Durham, NC; Erik Stalberg. MD. Department of Clinical Neurophysiology, University of Uppsala, Uppsala, Sweden; Joze Trontelj, MD, Institute of Clinical Neurophysiology, University of Ljubljana, Ljubljana, Yugoslavia Statistical analysis-John Pezzullo, PhD, Informa- tion Technology Center, Rhode Island Hospital, Providence, RI
This data was presented in preliminary form at the Annual Meeting of the AAEM in 1987, 1988, 1989, and 1990
Address correspondence to Dr. James M. Gilchrist, 110 Lockwood Street, Providence, RI 02903 Reprints not available
Accepted for publication February 14, 1991
CCC 0148-639X1921020151-011 $04.00 0 1992 John Wiley & Sons, Inc.
Trontelj'). T o obtain reference values from a wider range of muscles and different age groups, a collaborative effort was Organized to permit Val- ues obtained from many laboratories to be shared. These data could then identify the need for addi- tional values and allow coordinated acquisition of missing values.
Following a retrospective survey of SFEMG reference data previously acquired by several EMG laboratories, a prospective acquisition of SFEMG reference data was organized. This collab- orative effort obtained reference data from a large number of muscles, assured data for each muscle were available from adequate numbers of control subjects, and acquired data over a large age range.
METHODS
The study was initially designed as a retrospective collection of reference values from SFEMG practi- tioners. Prospective acquisition of additional SFEMG reference data was then undertaken by those and additional participants. Participants were selected because: (1) they were known to have collected SFEMG reference data previously, and (2) the three original participants (DBS, ES, JG) were familiar with their use of SFEMG. All participants were asked to send their data, as un- processed as possible, to the study coordinator (JG) for collation. The retrospective data were col- lected without control for methods of data acquisi- tion, analysis or storage but investigators, in gen-
Single Fiber EMG MUSCLE & NERVE February 1992 151

eral, used the recoriimeridatioris for performing SFEMC; of Stalberg and Tronte!J.7
The prospective data collection was performed using a single iiber- EMG electrode (a 0.45 mm needle cannula with a 25 pni wire core, exposed at a side port 3 to 5 mm from the tip); filter settings of 500 Hz for the low filter, and no lower than 10,000 Hz for the high filter. ‘The peak-to-peak amplitude of acceptable action potential was greater than 200 FV, with a rise tinie from the positive to the negative peak of less than 300 ps. Action potential shape remained constant with consecutive discharges; the positive phase of the first potential fell at least 100 pV between any two potentials used for measurements. Action poten- tial pairs with an interpotential interval (IPI) < 150 p s or >4000 p s were riot used for jitter measure- ment, For fiber density measurement, the ampli- tude of‘ one potential was maximized by adjusting the electrode position. The number- of time-locked acceptable action potentials was counted at 20 dif- ferent recording sites, and the electrode was moved enough between recording sites to lose all previously recorded potentials.
Each worker was assigned 2 muscles and asked to ohtain data from 15 sutjects, all either less than 60 years of age, or greater than or equal to 60 years of age. Muscle assignnients were redundant to allow irilcr-iiivestigator comparison for each rriuscle and each age group. At least 20 action po- tential pairs were requested for jitter analysis from each contr-ol subject, thougli fewer than 20 but niore thaii 5 were acceptable. Jitter was defined as the variability in consecutive IPIs for individual action potential pairs and was calculated as t he incan consecutive difference (MCI)) using the for- mula:
The mean jitter for each muscle, or mean MCD for each muscle, was the average jitter of all the action potential pairs from that muscle ana- lyzed for each subject. T h e fiber density of each muscle was calculated as the average number of action potentials recorded from 20 different sites in that muscle.
The data for each muscle was plotted against age, along with a fitted least squares curve and an associated upper (one-tail) 95th percentile enve- lope. An equation of the form Y = a + b (age“) was found empirically to represent the general age dependence seen in most of the data. The up-
per envelope differs from the fitted curve by 1.65 times the standard deviation of the individual points from the curve. If the data are normally distributed, only 5% of measurements from nor- mal subjects would be expected to lie outside the envelope. A logarithmic transformation was ap- plied to the SFEMG data whenever the non- normal distribution of points empirically war- ranted it.
Jitter values for individual action potential pairs represented a niore complex problem, with each patient having a cluster of values within the overall cluster of data. We felt it important to ad- here to the pre-existing definition of normal which allows 2 nieasureinents out of 20 to exceed the stated normal value,“.“ as otherwise normal patients not infrequently have 1 or 2 values out- side norniaL7 Accordingly, the third highest jitter value out of 20 for each subject was plotted. Whenever a greater or lesser number of measure- ments had been made in any subject, we deter- mined a theoretical “third highest out of 20” by a weighted interpolation scheme based on the statis- tical distribution of the ninety-fifth percentile.
RESULTS
Investigators from 9 laboratories contributed data. ‘l’hey will be referred to as institutions A through I. The numbers and ages of control subjects var- ied at each laboratory, as did the muscles studied. Data were collected over a wide time period, some k i n g over a decade old. There were 3 types of control subjects: (1) volunteers; (2) patients re- ferred to the EMG lab for an unrelated problem in an unstudied limb; and ( 3 ) patients referred to evaluate a related problem, e.g., myasthenia gravis, but subsequently were found not to have it. Obviously, the latter were the least desirable and were riot used in the prospective survey, but could not be eliminated from the retrospective survey as it was often irnpossible to identify them.
Equipment was conventional, with all partici- pants using a standard SFEMC; needle electrode. Low frequency filter settings were 500 Hz, except for institutions C and D, which used a low fre- quency filter setting of 800 Hz for their retrospec- tive studies. A variety of jitter analysis techniques were used, often at the same institution, and changed with time, e.g., the earliest jitter data were measured from photosensitive paper, using pencil and ruler. Digitizing boards and electro- myographs capable of measuring jitter directly (e.g., DISA Jittermaster, TECA Mystro, Nicolet Viking) were used at various centers; one center
152 Single Fiber EMG MUSCLE & NERVE February 1992

did not supply this information. Several partici- pants used the computerized jitter analysis pro- gram of Antoni' for at least a portion of their data collection.
The data were not compared by analysis method, but previous comparisons found no dif- ference in the results from different jitter analysis techniques3 One institution, H, collected data for the same age group and muscles twice, 1 year apart, using different analysis techniques, and found no significant difference between the re- sults.
Fiber density values were obtained for 11 mus- cles (Fig. 1; data for the abductor digiti minimi [ADM], sternocleidomatoid [SCM], tongue, and flexor carpi radialis are not presented, but are available on request). For most muscles, FD in- creased with age. Significant differences ( P < 0.05; 3-way factorial analysis of variance [ANOVA]) were noted between values obtained for the same muscle and age from some institu- tions (Table 1).
When data collected prospectively were com- pared between laboratories, significant differences were still seen. One institution, C, consistently had the lowest FD values, while another institution, A, had the highest. We feel this variation represents the subjective aspect of fiber density analysis that should be reflected in any reference values to be widely used. Three or more action potentials were recorded at a single site in 17% of subjects, but in only 3% of subjects were 4 or more potentials re- corded at any single site.
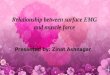
Jitter values for mean MCD were obtained for 11 muscles (Fig. 2; data for the ADM, SCM, and tongue are not presented but are available on re- quest). The mean MCD was greater after age 60 years in all muscles, and varied between institu- tions (P < 0.05; 3-way factorial ANOVA) but less dramatically than did fiber density (Table 2). Mus- cles could be separated into 3 groups based on the mean of mean MCD values. The mean of mean MCDs in the extensor digitorum communis (EDC), orbicularis oculi, orbicularis oris, tongue, and deltoid was 27 to 28 ps. The tibialis anterior, quadriceps, and abductor digiti quinti had mean of mean MCDs significantly higher (30 to 38 ps; P < 0.02), and the frontalis, biceps, and sternoclei- domastoid had mean of mean MCDs significantly lower (23 to 25 ps; P < 0.02) than these values.
Jitter values for individual action potential pairs were available for 11 muscles (Fig. 3; data for the ADM, tongue, and SCM are not pre- sented, but are available on request). Jitter mea-
surement increased after age 60 years in all mus- cles except the tibialis anterior. Action potential pair jitter values taken as a mean varied between some laboratories (P < 0.05; 3-way factorial ANOVA) (Table 3).
T o test the hypothesis that some laboratories may have excluded outliers (e.g., action potential pairs with jitter > 100 ~ s ) prior to data acquisi- tion, w e removed the action potential pair with maximum jitter from each subject and recalcu- lated mean jitter (Table lc). This resulted in less difference among laboratories. Comparing the change in mean jitter for each laboratory after ex- clusion of the maximal jitter pair reveals a dispro- portionately small number of outliers from labora- tories with the least change in mean jitter (e.g., in the EDC, institutions C and D had the smallest change after exclusion of maximum jitter values, and contributed only 3% and 0% of the outliers, but 20% and 8% of the total data, although the data from institutions A and B had 80% and 13% of the outliers and 58% and 9% of the total data), implying that institutions C and D excluded outli- ers prior to data acquisition. The effect of these outliers is not a factor when the third-highest value is used to calculate normal values, as we have done. Logarithmic transformation was used for the graphs of the frontalis, orbicularis oris, or- bicularis oculi, sternocleidomastoid, and abductor digiti quinti muscles.
Extreme outliers (greater than 4 SD from the mean) were present in a minority of muscles but, in each, skewed the data toward a higher upper limit. We eliminated any individual data point ex- ceeding 4 SD above the mean, and recalculated the mean and SD. Six curves were affected: tibialis anterior fiber density (1 data point eliminated), tibialis anterior mean MCD (2 data points elimi- nated), and EDC. 0. oculi, tibialis anterior, and frontalis jitter (1, 1, 2, and 1 datapoints elimi- nated, respectively).
Blocking of neuromuscular transmission was seen infrequently. Jitter exceeded 100 ps in 0% to 2% of action potential pairs, depending on the muscle, but in at least one pair in 10.5% of all muscles (85 of 809). Jitter greater than 100 ps was seen in more than one pair in fewer than 1% of muscles. Low jitter (less than 10 ps) was seen in 0% to 2% of pairs, except in the sternocleidomas- toid, where low jitter was found in 4% of action potential pairs. Low jitter was seen in at least one action potential pair in 14.7% of muscles. Action potential pairs with jitter less than 10 were seen in 98 of 556 studies (19.6%) in subjects less than 60
Single Fiber EMG MUSCLE & NERVE February 1992 153

o 0 C , a- 0
0 :8 0 :
a
154

, -
0
a
n 0 -N
* :. . . 0 : o a
. T O
9 f
9 x R c 9 c)
J
a
a
. a
.
a
.
:* . :.
m
9 c
9 c
155

a
i
156

70.0
1 M
ean
MCD
- 95%
Upp
er N
orm
al L
imits
20.0
-
10.0
-
0.01
(I.ol
0
W
00
0.
w
e
0
Dat
a
-m U
.L
. * Avo
ng.
. -
1
Mus
cle:
Tib
ialis
Ant
erio
r
00
0
0
a A
vora
g.
00
50
.0-,
0
0
30.0
{
20.0
.1
0
Dat
a
-85%
U
.L
s 8 A
vora
go
Mea
n M
CD
- 95%
Upp
er N
orm
al L
lmlts
M
urck
: O
rbku
laris
Orls
10
.0,
0
I -
-
-9
0
0
'p,?
,,a
'"'
0.
W
, . , ?. -
3 ...
......
......
...
......
......
,P,, . A
0
ace.
- o
w
0
I
*-
0
.* 9
- 0
0
20.0
.I 0
10.0
I 0
Dat
a
-85%
U
.L
Upp
*r
AaIm
5
4a.4
10
40.4
15 4a.4
20 49.3
25 4S.3
30 48.2
35 40.1
40 48.D
45 48.7
50 40.5
55
40.2
80 47.a
85 47.5
70 47.0
75 40.4
80
45.8
85
45.1
UP
Wr
Am
LIm
u E
34.8
10 34.7
15 34.7
20 34.7
2E
34.0
30
34
.0
35
3E.l
45
35
.8
10
30.0
0
0
30.4
8
0
37.0
70 30.3
80
40.2
80
42
.5
40 35.3
80
a7.8
711
aa.2
8s 41.3 B
Mea
n M
CD
- 95
% U
pper
Nor
mal
Lim
its
Mus
cle:
E
xt. D
ig. C
omm
.
0
0
40.0
- 0
0
0
0
m
oceoo
0
cm
o
oo
eo
ow
0 0
O
0
a':
a2
00
0
w 0
0
0
co
.O
o
0
0
0
O
20.0
- 0 0
0
0
0
Dat
a 1 lo*ol
-85%
U
.L
# 8 A
vora
p.
0.04.
-.
-.
-.
-.
, -
- -
. .
- -
- -
I
0 25
5
0
75
10
0
Ag.
(v
an
)
FIG
UR
E 2.
(A,
B)
Gra
phic
al a
nd ta
bula
r pr
esen
tatio
n of
mea
n M
CD
refe
renc
e va
lues
for
8 m
uscl
es. O
rdin
ate
scal
e is
not
nec
essa
rily,
the
sam
e on
adj
acen
t gra
phs.
UP
p.1
A
anLl
mu
5 34.8
10 34.8
15 34.8
25
30 35.0
35.1
20
a4
.0
35 35.2
40
35.4
45 35.8
so 35.8
SE
ao
.2
8s
~7
.1
7~
38
3
05
a0
.0
80
38
.8
70 37.7
80
30.1
80
00.0
up
p.r
Aanm
5
S5.
0 10
as.)
15
20
35.8
36
.0
25
ao
ao
.~
38.2
aE
S8.
8 4
0
37.1
4
5
a8.a
EO
85
aa
.0
40.1
80
8
8
4i.
a
42.8
TO
44
.a
75
40
.8

J 5 t
0 1 : L. 0
-0 c
I
I
P t
a
158

0 0 c
n I-
P o f n E
8 <
n (Y
0
0 0 c J
5 € t " d . I i
i - . 0 :
- 0
- 0
x m x
m 8 N
8 t
j m o m o m o m o m o m o m o m o m o r r ~ ~ n n * * m r n o o ~ ~ o o ~
0 z J 5
I
0
0
I
... a 8 I- 8
o + $ ! $ s 5 : U P
159

Table 1. Summary of fiber density results* for the extensor digitorum comrnunis muscle, per laboratory.
Table 2. Summary of mean MCD* results for the extensor digitorum cornmunis muscle, per laboratory.
Lab. Age < 60 60 < Age < 70 Age > 70 Lab. All ages Age <60 Age >60
A 1.46 2 .15 1.54 2 .17 2.00 2 .41 A 28.3 ? 5 5 27.9 ? 5.5 31.0 t 4.4 (N = 119) (N = 21) (N = 31) (N = 160) (N = 141) (N = 19)
B 1.45 2 .14 - - B 27.6 ? 3.2 27.6 t 3.2 -
C 1.38 2 .08 1.55 2 .18 1.69 5 .18 C 27.3 ? 4.5 26.4 ? 3.8 31.3 t 5.7
(N = 20) (N = 26) (N = 26)
(N = 69) (N = 18) (N = 7) (N = 55) (N = 45) (N = 10)
- D 27.3 ? 5.6 27.3 ? 5.6 D 1.41 t .16 - -
(N = 3) (N = 4) (N = 4)
(N = 17) (N = 2) (N = 1) (N = 26) (N = 22) (N = 4)
(N = 22) (N = 7) (N = 25) (N = 25)
(N = 228) (N = 63) (N = 46) (N = 296) (N = 238) (N = 58)
E 1.46 ? .10 1.53 ? . l l 1.70 E 26.5 k 4.3 26.4 ? 4.5 26.9 ? 3.7
H - 1.58 2 ,151 1.74 ? .28 H 26.5 ? 3.8 - 26.5 t 3.8
All 1.43 ? .16 1.56 * .16 1.91 ? .38 All 27.7 ? 4.9 27.5 ? 4.9 28.9 2 4.9
*Mean ? SD; N = Number of sublects studfed. 'Mean t SD; N = Number of subjects studied
years of age and in 21 of 253 studies (8.3%) in subjects greater than 60 years of age. Jitter greater than 100 p s was seen in at least one action poten- tial pair in 49 studies (8.8%) in subjects less than 60 years of age, and in 36 studies (14.2%) in sub- jects greater than 60 years of age. Jitter values greater than 100 or less than 10 p s were seen in different action potential pairs in the same study in 2.3% of all studies (19 of 809), which is more than would be expected by chance (1.5%).
DISCUSSION The SFEMG reference data are based on retro- spective and prospective data acquired from sev- eral different laboratories and investigators, and is not free of statistical aberrations. Nonetheless, these data should be useful in SFEMG laboratories using the same techniques. Occasional papers have reported control values from a small popula- tion or few muscles, but only once has a broad de- lineation of normal values for several muscles and ages been attempted as done by Stalberg and T r ~ n t e l j . ~ Even these normal values were obtained from a relatively small number of subjects, partic- ularly for jitter, for few muscles (6 for jitter, 8 for fiber density) and, for the most part, from subjects less than 50 years of age.7 We felt this situation could best be addressed by a multicenter collabo- rative collection of SFEMG normal data. The data of Stalberg and Trontrelj7 are included in this col- lection.
A major question is whether these reference
values are valid for laboratories other than those in which they were obtained. This question could also be asked about using any values for normal limits. From our study, this appears to be a prob- lem more for FD than forjitter measurements, as jitter values do not vary much among laboratories. Despite its objective underpinning, there is a sig- nificant subjective aspect to the selection of action potentials to be counted for fiber density measure- ments. The different low frequency filter setting used at institution C may explain why that labora- tory's fiber density values were consistently the lowest, but does not explain variations among lab- oratories using the same filter settings. Other pos- sible explanations for these differences include different criteria used to determine whether there were single or multiple potentials when the IPI was quite short; and failure to consistently and ad- equately move the SFEMG needle between re- cording sites, resulting in either too few or too many single potentials being counted.
It is our opinion that the reference data for normal limits described accurately represents the findings in people without neuromuscular disease and improves upon pre-existing values in several ways: the bias in any one laboratory was diluted by the multicenter nature of the collection; there was a wider range of muscles and ages represented; and larger numbers of subjects were used to de- termine the normal limits.
Human physiologic data are frequently nonpa- rametric and the SFEMG reference values are no
160 Single Fiber EMG MUSCLE & NERVE February 1992

Table 3. Summary of jitter in action potential pairs’ for the extensor digitorum communis muscle, per laboratory ~ ~~~~
All ages Age <60 Age >60
All Minus Age Minus Age Minus ages maximurn <60 maximum > 60 maximum
A 28.5 SD = 17.4 N = 3025
B 29.0 SD = 20.6 N = 456
C 27.3 SD = 10.6 N = 1051
D 28.0 SD = 9.6 N = 73
E 26.5 SD = 9.6 N = 434
H 28.1 SD = 11.9 N = 219
All 28.1 SD = 15.7 N = 5259
26.3 SD = 10.2 N = 2860
26.5 SD = 6.8 N = 430
26.2 SD = 9.0 N = 998
26.8 SD = 8.1 N = 68
25.4 SD = 8.2 N = 412
26.3 SD = 7.6 N = 205
26.2 SD = 9.4 N = 4974
28.2 SD = 16.9 N = 2605
29.0 SD = 20.6 N = 456
26.1 SD = 9.9 N = 761
28.0 SD = 9.6 N = 73
26.5 SD = 9.7 N = 352
-
27.8 SD = 15.7 N = 4248
26.1 SD = 10.0 N = 2463
26.5 SD = 6.8 N = 430
24.9 SD = 8.2 N = 722
26.8 SD = 8.1 N = 68
25.4 SD = 8.3 N = 334
-
25.9 SD = 9.2 N = 4018
30.6 SD = 20.2 N = 420
-
30.6 SD = 11.6 N = 290
-
26.7 SD = 9.2 N = 82
28.1 SD = 11.9 N = 219
29.7 SD = 15.8 N = 1011
27.8 SD = 11.1 N = 397
-
29.4 SD = 10.2 N = 276 -
25.6 SD = 8.0 N = 78
26.3 SD = 7.6 N = 205
27.7 SD = 10.0 N = 956
*Mean, SD = Standard deviation, N = Number of sub]ecfs studied
exception. Simple histograms of numerical values versus age demonstrate that FD and jitter have non-Gaussian distribution for virtually all muscles. A variety of nonparametric analyses were tried, including logarithmic and square root transforma- tions, percentile rank-order sorting, and quadratic regression. The best visual fit for fiber density, mean MCD, and jitter came from the polynomial function Y = a + b (age3).
This collection was undertaken with the prime motive of supplying physicians doing SFEMG with accurate reference data, so that clinical SFEMG would rest on a firmer scientific basis. However, these values should not be construed as absolutes. Users must define for themselves how these refer- ence data fit their own practice of SFEMG.
Our recommendations are that a fiber density study should be considered abnormal only if it ex- ceeds the 95% upper limit for the patient’s age. Action potential counts greater than 4 at a single recording site are rare in normal subjects and sug- gest abnormality. Our recommended criteria of abnormality for a jitter study are either: a value for mean MCD above the 95% upper limit for age for that muscle; or jitter greater than the 95% up-
per limit for action potential pairs in more than 2 action potential pairs in a muscle (or > lo% of pairs, if more than 20 action potential pairs are analyzed). As with any electrophysiologic finding, any abnormality should be interpreted in light of the clinical situation.
REFERENCES
1. Antoni L, Stalberg E, Sanders DB: Automated analysis of neuromuscular ‘Ijitter.” Cornput Prog Med 1983; 16: 175- 188.
2. Ekstedt J , Stalberg E: A method of recording extracellular action potentials of single muscle fibers and measuring their propagation velocity in voluntarily activated human muscle. Bull Am Assoc EMG Electrodzap 1963;10:16.
3. Sanders DB, Howard JF: Single fiber electromyogrdphy in myasthenia gravis. Muscle Nerve 1986;9:809-819.
4. Sanders DB, Howard JF, Johns T K : Single fiber electromy- ography in myasthenia gravis. Neurology 1979;29:68- 76.
5. Stalberg E, Ekstedt J , Broman A: The electromyogrdphic jitter in normal human muscles. Ebclroencephalogr Clin Neu- rophysiol 1971 ;31:429-438.
6. Stalberg E, Schwartz MS, Trontelj JV: Single fibre electro- myography in various processes affecting the anterior horn cell.] Neural Sci 1975;24:403-415.
7. Stalberg E, Tronteij J : Single Fiber Electromyography. Old Woking, Surrey, Mirvalle Press, 1979.
Single Fiber EMG MUSCLE & NERVE February 1992 161