Embed Size (px)
Citation preview

SIMULTANEOUS TREATMENT OF LOWER EYELID DERMATOCHALASIS AND ABNORMAL-APPEARING SKIN
A L L E N M. P U T T E R M A N , M.D.
Chicago, Illinois
Abnormal, thin, crinkly, or pigmented nasal lower eyelid skin is sometimes associated with dermatochalasis (excessive skin). In these cases, excision of temporal lower eyelid skin by conventional cosmetic blepharoplasty draws and diffuses this abnormal skin temporally and worsens the appearance of the lower eyelid skin.
A new procedure in which excessive abnormal skin is excised nasally rather than temporally draws and diffuses the more normal temporal skin nasally and improves the appearance of the lower eyelid skin. This approach simultaneously resolved dermatochalasis and abnormal-appearing lower eyelid skin in six eyelids of three patients without complications.
Some patients want to improve the appearance of eyelids that not only have dermatochalasis (excessive skin) but also an abnormal skin quality or pigmentation. This abnormal skin is often located over the nasal one half or two thirds of the lower eyelids. In a conventional lower eyelid cosmetic blepharoplasty, the skin is excised at the temporal aspect of the lower eyelid.1 This stretches and diffuses abnormal nasal skin in a temporal direction and worsens the appearance of the lower eyelid skin.
I eliminate abnormal skin pigmentation and texture in the nasal lower eyelid region by excising skin at the nasal rather than temporal aspect of the lower eyelid. This stretches and diffuses normal temporal lower eyelid skin in a nasal direction, improving the appearance of the lower eyelid skin.
Accepted for publication April 14, 1983. From the Department of Ophthalmology, Univer
sity of Illinois Eye and Ear Infirmary, Chicago, Illinois. This study was supported in part by core grant EY1792 from the National Eye Institute. This study was presented before the American Society of Ophthalmic Plastic and Reconstructive Surgery, October 1982.
Reprint requests to Allen M. Putterman, M.D., 111 N. Wabash, Chicago, IL 60602.
M A T E R I A L AND M E T H O D S
The procedure is usually performed with the patient under local anesthesia supplemented with intravenous sedation.2 I use a méthylène blue marking pen to draw a line 1.5 to 2 mm below the eyelashes of the lower eyelid, beginning at the nasal end of the eyelid and extending 2 to 3 mm temporal to the lateral canthus (Fig. 1, A). The line is then continued in an almost horizontal direction in one of the temporal laugh lines for another 10 mm. A second line, beginning at the nasal end of the first line, is directed in an inferotemporal oblique direction for approximately 15 mm. I apply tetra-caine eyedrops to the eye and insert a scierai lens into the ocular cul-de-sac to protect the eye. I inject several milliliters of 2% lidocaine with epinephrine subcu-taneously over the entire lower eyelid and lateral canthus.
I use a No. 15 Bard Parker blade to incise the skin over the marked méthylène blue lines and then use Wescott scissors to dissect lower eyelid skin from the orbicularis oculi muscle (Fig. 1, B). The skin is usually dissected to the level of the inferior orbital rim (Fig. 1, C). The
6 © AMERICAN JOURNAL OF OPHTHALMOLOGY 96:6-9, 1983

VOL. 96, NO. 1 DERMATOCHALASIS AND ABNORMAL SKIN 7
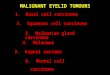
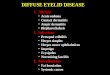
Fig. 1 (Putterman). The procedure. A, Marked line of proposed incision begins at the nasal end of eyelid and extends 10 mm temporal to lateral canthus. Another line begins at the nasal end of the first line and extends in an inferotemporal oblique direction for 15 mm. B, Dissection of lower eyelid skin flap. C, Reflection of lower eyelid skin flap. D, Skin flap is pulled in a superonasal direction. E, Excision of triangle of skin that overlaps superior edge of incision. F, Excision of triangle of skin that overlaps nasal edge of incision. G, Skin is closed with continuous 6-0 black silk sutures.
dissection, however, can be extended slightly inferior to the rim, if the derma-tochalasis and abnormal skin are abundant.
Any herniated orbital fat can be excised after the dissection of the skin flap. Usually, the orbicularis oculi muscle is open across the entire eyelid just above the inferior orbital rim. Fat that easily prolapses when gentle pressure is applied to the globe is clamped with a hemostat, sliced from the hemostat, and cauterized with a Bovie cautery. '
The lower eyelid skin flap is then pulled with slight tension nasally and superiorly (Fig. 1, D). The flap fills the curvature of the nasal lower eyelid convexity during this maneuver. The patient is asked to look upward, and the skin that drapes the incision site is excised. (If the patient is too sedated to look upward, I apply pressure to the globe through the upper eyelid. This elevates the lower eyelid to a level similar to that achieved on upgaze.) A small triangle of skin is excised vertically above the horizontal infralash incision (Fig. 1, E) and a slightly larger triangle of skin is excised nasally (Fig. 1, F).
I then suture the skin flap to the sur
rounding skin with a continuous 6-0 black silk suture run from the nasal end of the eyelid to the end of the inferonasal oblique incision (Fig. 1, G). I run a second suture continuously horizontally from the nasal end of the eyelid to the temporal end of the incision.
Postoperatively the patient applies ice compresses to the eyelid for 24 hours. If orbital fat is excised, vital eye signs are checked every 15 minutes for two hours to avoid possible blindness resulting from a retrobulbar hemorrhage.3
The skin sutures are removed four days postoperatively.
R E S U L T S
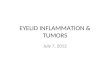
I have used this procedure to achieve simultaneous resolution of dermatochala-sis and abnormal-appearing lower eyelid skin in six eyelids of three patients (Fig. 2). There have been no complications during the six to 28 months of postoperative follow-up.
D I S C U S S I O N
I previously described a semicircular skin flap technique to reconstruct the eyelid defect resulting from excision of large tumors of the nasal eyelid skin.4

8 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1983
Fig. 2 (Putterman). Left, Preoperative appearance of a patient with abnormal-appearing nasal lower eyelid skin. Right, After the procedure the patient has resolution of abnormal-appearing skin. Excessive skin was also excised in the upper eyelids.
This new procedure is an extension of ing skin temporally through the usual that technique. conventional cosmetic blepharoplasty ap-
The nasal skin is sometimes darkly pig- proach moves the abnormal skin tempor-mented compared to the lighter, more ally and diffuses it throughout the eyelid, normal temporal skin. In other cases, the thereby worsening the appearance of the skin quality is abnormal and it has a lower eyelid skin. This new procedure crinkly texture. In either instance, excis- pulls the more normal temporal skin in a
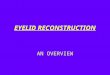
Fig. 3 (Putterman). Testing the suitability of thetechnique. Top left, Lower eyelid of patient withcrinkly nasal lower eyelid skin. Top right, Pullinglower eyelid skin nasally diffuses normal temporalskin throughout the eyelid and improves the qual ityof the lower eyelid skin. Bottom left, Pulling lowereyelid skin temporally diffuses abnormal nasal skinthroughout eyelid and worsens the appearance of thelower eyelid skin.

VOL. 96, NO. 1 DERMATOCHALASIS AND ABNORMAL SKIN 9
nasal direction, so that more normal skin appears throughout the eyelid postopera-tively.
Pulling the lower eyelid skin nasally with a finger is a simple way to determine the suitability of candidates for this procedure preoperatively (Fig. 3, top left and top right). The improvement observed in the quality and color of the skin as the more normal temporal skin diffuses throughout the eyelid simulates the expected postoperative appearance. Conversely, if drawing the skin temporally with a finger worsens the appearance of the lower eyelid skin, the standard bleph-aroplasty approach can be ruled out (Fig. 3, bottom left).
A possible complication of this new procedure is a postoperative ectropion. This can be avoided by having the patient look upward when determining the amount of skin to excise above and nasal to the incision sites. If the patient is too sedated to assume upgaze, pushing on the eye through the upper eyelid elevates the lower eyelid to the position it takes on upgaze. (If the amount of skin to excise is determined while the patient is gazing in primary position or down gaze, too much skin will be removed and an ectropion will result on upgaze postoperatively be
cause the lower eyelid moves 3 to 5 mm from downgaze to upgaze.) It is also important to realize that a concavity over the nasal end of the lower eyelid is common. It is necessary, therefore, to allow the skin to fill this curvature when determining the amount of lower eyelid skin to excise.
In some patients the degree of abnormal skin quality or pigmentation is too great in comparison with the amount of eyelid dermatochalasis. In these cases, the procedure cannot completely eliminate all the abnormal-appearing skin, but it does improve the quality of lower eyelid skin, leaving a slight amount of abnormal tissue nasally.
REFERENCES 1. Putterman, A. M.: Surgical treatment of lower
eyelid dermatochalasis, herniated orbital fat and hypertrophie orbicularis. A skin flap approach. In Putterman, A. M. (ed.): Cosmetic Oculoplastic Surgery. New York, Grune and Stratton, 1982, pp. 117-133.
2. Katzen, L., and Karvelis, J.: Anesthesia, analgesia and amnesia. In Putterman, A. M. (ed.): Cosmetic Oculoplastic Surgery. New York, Grune and Stratton, 1982, pp. 89-97.
3. Putterman, A. M.: Temporary blindness after cosmetic blepharoplasty. Am. J. Ophthalmol. 80:1081, 1975.
4. Putterman, A. M.: Semicircular skin flap in reconstruction of nonmarginal eyelid skin defects. Am. J. Ophthalmol. 84:708, 1977.