Embed Size (px)
Citation preview

Simultaneous GLP-1 andInsulin Administration AcutelyEnhances Their Vasodilatory,Antiinf lammatory, and AntioxidantAction in Type 2 DiabetesDiabetes Care 2014;37:1938–1943 | DOI: 10.2337/dc13-2618
OBJECTIVE
To test the hypothesis that the simultaneous administration of GLP-1 and insulinmay increase their vasodilatory, antiinflammatory, and antioxidant action in type2 diabetes.
RESEARCH DESIGN AND METHODS
In two groups of persons with type 2 diabetes, two sets of experiments wereperformed. The first group had two normoglycemic-normoinsulinemic clampswith or without GLP-1 and two normoglycemic-hyperinsulinemic clamps with orwithout GLP-1. The second group had two hyperglycemic-normoinsulinemicclamps and two hyperglycemic-hyperinsulinemic clamps with or without GLP-1.
RESULTS
During the normoglycemic-hyperinsulinemic clamp, flow-mediated dilatation(FMD) increased, while soluble intercellular adhesion molecule (sICAM-1), plasma8-iso-prostaglandin F2a (8-iso-PGF2a), nitrotyrosine, and interleukin (IL)-6 de-creased compared with normoglycemic-normoinsulinemic clamp. Similar resultswereobtainedwith the infusionofGLP-1during thenormoglycemic-normoinsulinemicclamp. The combination of hyperinsulinemia and GLP-1 in normoglycemia wasaccompanied by a further FMD increase and sICAM-1, 8-iso-PGF2a, nitrotyrosine,and IL-6 decrease. During the hyperglycemic-normoinsulinemic clamp, FMD signif-icantly decreased, while sICAM-1, 8-iso-PGF2a, nitrotyrosine, and IL-6 significantlyincreased. When hyperglycemia was accompanied by hyperinsulinemia or by thesimultaneous infusion of GLP-1, these phenomena were attenuated. The simul-taneous presence of hyperinsulinemia and GLP-1 had an increased beneficialeffect.
CONCLUSIONS
Our results show that the combination of insulin and GLP-1 is more effective thaninsulin or GLP-1 alone in improving endothelial dysfunction, inflammation, andoxidative stress in type 2 diabetes.
1Insititut d’Investigacions Biomediques AugustPi i Sunyer and CIBERDEM, Hospital Cl ınicBarcelona, Barcelona, Spain2Division of Metabolic Diseases, Center of Excel-lence for Cardiovascular Diseases, 2nd Universityof Naples, Naples, Italy3Metabolic and Nutrition Research Center onDiabetes, Italian National Research Center onAging, Istituto Nazionale Riposo e Cura Anziani–Istituto di Ricovero e Cura a Carattere Scientifico,Ancona, Italy4Department of Cardiovascular and MetabolicDiseases, Istituto di Ricovero e Cura a CarattereScientificoGruppoMultimedica, Sesto SanGiovanni,Italy
Corresponding author: Antonio Ceriello, [email protected].
Received 9 November 2013 and accepted 15January 2014.
© 2014 by the American Diabetes Association.See http://creativecommons.org/licenses/by-nc-nd/3.0/ for details.
Antonio Ceriello,1 Anna Novials,1
Silvia Canivell,1 Lucia La Sala,1
Gemma Pujadas,1 Katherine Esposito,2
Roberto Testa,3 Loredana Bucciarelli,4
Maurizio Rondinelli,4 and
Stefano Genovese4
1938 Diabetes Care Volume 37, July 2014
EMER
GINGTECHNOLO
GIESANDTH
ERAPEU
TICS

Recent evidence has demonstratedthat insulin has a vasodilatory and anti-inflammatory action in humans (1). Oneof the possible mechanisms involved inthese actions seems to be related to theantioxidant property of insulin (2,3).Apart from the well-documented in-
cretin effect of glucagon-like peptide 1(GLP-1), its role in the cardiovascularsystem also arouses interest. GLP-1has a direct action on the endothelium(4), and it has been demonstrated that itimproves endothelial function (5,6) andinflammation (6,7) in diabetes, possiblyincreasing the antioxidant defenses ofthe endothelium (8) and decreasing ox-idative stress generation (6,7).The combination of basal insulin and
GLP-1 is now proposed for the manage-ment of type 2 diabetes (9), while a re-cent report has shown that GLP-1 canenhance the vasodilatory effect ofinsulin in subjects with the metabolicsyndrome (10).Based on this evidence, the thera-
peutic option of combining insulin andGLP-1 may have a significant impact onthe cardiovascular risk profile of type 2diabetic patients. The aim of this studywas to evaluate the effect of addingGLP-1 to normal and increased insulinplasma levels, during both normo- andhyperglycemia, on several markers ofendothelial function, inflammation,and oxidative stress.
RESEARCH DESIGN AND METHODS
Two groups of 12 matched type 2 di-abetic patients participated in thestudy. Baseline characteristics of thestudy groups are shown in Table 1.The study was approved by one of theethics committees of our institutions,and written consent from the study sub-jects was obtained.Ten patients were on diet alone, and
the other 14 patients were on metfor-min, which was discontinued at least 4weeks before the study. In none of thetype 2 diabetic patients was retinopa-thy, nephropathy, or neuropathy pres-ent. Five patients had hypertensiontreated with an ACE inhibitor, whichwas withheld on the study days. Noneof the subjects were on statin or antiox-idant supplementation.Synthetic GLP-1 (7–36)amide was
purchased from PolyPeptide Laborato-ries (Wolfenbuttel, Germany), and thesame lot number was used in all studies.
Study DesignSubjects were admitted to the researchcenter the evening before the experi-ment. All subjects received an eveningmeal and received a continuous low-dose infusion of insulin to normalizeplasma glucose. The insulin infusionwas adjusted overnight to maintainblood glucose between 4.4 and 7.2mmol/L and stopped 2 h before the startof each experiment.
After a 12-h overnight fast, subjectswere placed in a supine comfortable po-sition with a room temperature be-tween 208 and 248C. Intravenous lineswere inserted into a large antecubitalvein of one arm for infusions andinto a dorsal vein of the contralateralarm for blood sampling. Patency waspreserved with a slow saline infusion(0.9% NaCl). The study began after thesubjects had rested for 30 min.
Octreotide infusion (25 mg i.v. bolusfollowed by a 0.5 mg/min infusion,Longastatina; Italfarmaco, Milan, Italy)to block the release of endogenous in-sulin was started 5 min before the prim-ing glucose pulse and was interrupted atthe end of the clamp.
Group 1 had, in a randomized orderand on different days, with at least a1-week interval, two normoglycemic-normoinsulinemic clamps (11) (glucoseinfusion to maintain the concentrationof 5 mmol/L), with or without GLP-1, andtwo normoglycemic-hyperinsulinemicclamps (insulin infusion 0.1 mU/kg/min
and constant glucose infusion tomaintainthe concentration of 5 mmol/L) with orwithout GLP-1.
Group 2 had, in a randomized orderand on different days, with at least a1-week interval, two normoglycemic-normoinsulinemic clamps (glucose infu-sion to maintain the concentration of15 mmol/L), with or without GLP-1, andtwo normoglycemic-hyperinsulinemicclamps (insulin infusion 0.1 mU/kg/minand constant glucose infusion tomaintainthe concentration of 15 mmol/L) with orwithout GLP-1.
All experiments lasted 2 h. GLP-1 wasinfusedat a rateof 0.4pmol z kg21 zmin21,according to the methodology of Naucket al. (12).
At baseline and at 1 and 2 h, plasmaglucose, flow-mediated dilatation (FMD),nitrotyrosine, plasma 8-iso-prostaglandinF2a (8-iso-PGF2a), soluble intercellularadhesion molecule (sICAM-1), and inter-leukin (IL)-6 were measured.
Biochemical and ClinicalMeasurementsCholesterol, triglycerides, HDL choles-terol, LDL cholesterol, and plasma nitro-tyrosine were measured according tothe methodology of Ceriello et al. (13).Plasma glucose was measured by theglucose-oxidase method, HbA1c byhigh-performance liquid chromatogra-phy and insulin by microparticle enzymeimmunoassay (Abbott Laboratories,Wiesbaden, Germany). 8-iso-PGF2a
Table 1—Baseline characteristics of the type 2 diabetic patients
Group 1 Group 2
Sex (male/female) 9/3 8/4
Age (years) 53.2 6 2.3 52.7 6 1.3
BMI (kg/m2) 26.8 6 1.4 26.2 6 2.1
HbA1c (%) 8.1 6 0.5 8.0 6 0.4
HbA1c (mmol/mol) 65 6 3.2 65 6 3.0
Resting diastolic blood pressure (mmHg) 79.3 6 1.2 78.5 6 1.5
Resting systolic blood pressure (mmHg) 115.2 6 1.4 117.3 6 1.6
Total cholesterol (mmol/L) 4.32 6 0.3 4.22 6 0.4
Triglycerides (mmol/L) 1.1 6 0.4 1.3 6 0.2
HDL-C (mmol/L) 1.4 6 0.2 1.3 6 0.3
LDL-C (mmol/L) 2.0 6 0.2 2.1 6 0.4
FMD (%) 6.3 6 0.5 6.5 6 0.3
8-iso-PGF2a (pg/mL) 65.4 6 3.2 69.4 6 3.0
Nitrotyrosine (mmol/L) 0.77 6 0.07 0.77 6 0.04
sICAM-1 (ng/mL) 170.5 6 12.5 176.5 6 13.5
IL-6 (pg/mL) 220.35 6 11.1 227.35 6 11.3
Data are means 6 SEM. HDL-C, HDL cholesterol; LDL-C, LDL cholesterol.
care.diabetesjournals.org Ceriello and Associates 1939

(Cayman Chemical, Ann Arbor, MI),sICAM-1 (British Biotechnology, Abingdon,U.K.) and IL-6 (R&D Systems, Minneapolis,MN), were determined with commerciallyavailable kits.Endothelial function atmacrovascular
level was evaluated by measuring theFMD of the brachial artery (6,7). Theexamination was carried out in a tem-perature and light-controlled room onsubjects who were lying comfortablyflat on a couch. Brachial arteries in thisstudy were imaged with a standardultrasound system (Vivid 7 ECHO ma-chine; GE Vingmed System V) connectedwith a 12 MHz linear transducer probe.The ultrasound system was connectedto a personal computer equipped with aframe grabber and artificial neural net-work wall detection software (vessel im-age analysis). Brachial artery FMD wasdetermined using protocol similar topublished studies (6,7).At the endof the study each day, 250mg
sublingual glyceryl trinitrate was adminis-tered to assess endothelium-independentvasodilatation. The intraobserver variabil-ity for repeated measurements of restingarterial diameter was 0.026 0.02 mm.
Statistical AnalysisThe sample size was selected accord-ing to previous studies (5–7,10). Dataare expressed as means 6 SE. TheKolmogorov-Smirnov algorithm wasused to determine whether each vari-able had a normal distribution. Compar-isons of baseline data among the groupswere performed using unpaired Studentt test or Mann-Whitney U test whereindicated. The changes in variablesduring the tests were assessed by two-way ANOVA with repeated measures orKolmogorov-Smirnov test where indi-cated. If differences reached statisticalsignificance, post hoc analyses with two-tailed paired t test or Wilcoxon signedrank test for paired comparisons wasused to assess differences at individualtime periods in the study. Statisticalsignificance was defined as P , 0.05.
RESULTS
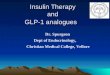
Normoglycemic ClampsIn normoglycemic-normoinsulinemicconditions, all of the parameters re-mained unchanged (Fig. 1). During thenormoglycemic-hyperinsulinemic clamp,FMD increased, while sICAM-1, 8-iso-PGF2a, nitrotyrosine, and IL-6 decreased
compared with normoglycemic-normoinsulinemic clamp (Fig. 1). GLP-1infusion during the normoinsulinemic-normoinsulinemic clamp also increasedFMD, and decreased sICAM-1, 8-iso-PGF2a, nitrotyrosine, and IL-6 comparedwith normoglycemic-normoinsulinemicclamp (Fig. 1). The combination of hy-perinsulinemia andGLP-1, in normoglyce-mia, was accompanied by a further FMDincrease and sICAM-1, 8-iso-PGF2a, nitro-tyrosine, and IL-6 decrease (Fig. 1).
During the normoglycemic-normoinsulinemic clamp, the glucose in-fusion rate (GIR) was 3.26 0.4mg/kg/minand 3.5 6 0.5 mg/kg/min adding GLP-1(P = NS). During the normoglycemic-hyperinsulinemic clamp, GIR was 4.3 60.6 mg/kg/min and 4.7 6 0.5 mg/kg/minadding GLP-1 (P = NS).
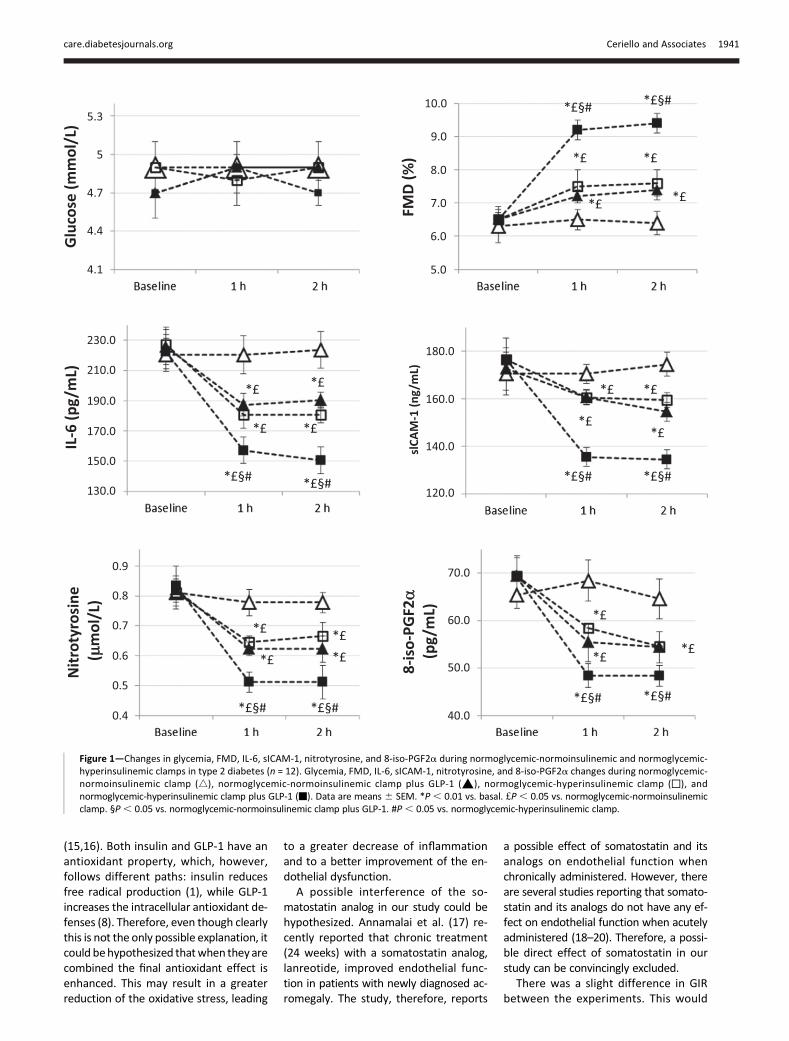
Hyperglycemic ClampsDuring the hyperglycemic-normoinsu-linemic clamp, FMD significantly de-creased, while sICAM-1, 8-iso-PGF2a,nitrotyrosine, and IL-6 significantly in-creased (Fig. 2). When hyperglycemiawas accompanied by hyperinsulinemiaor by the simultaneous infusion ofGLP-1, all these phenomena were signif-icantly attenuated: FMD decreased less,while sICAM-1, 8-iso-PGF2a, nitrotyro-sine, and IL-6 were less increased(Fig. 2). The simultaneous presence ofhyperinsulinemia and infusion of GLP-1had even better effect (Fig. 2).
During the hyperglycemic-normoin-sulinemic clamp, GIR was 4.5 6 0.3mg/kg/min and 4.4 6 0.4 mg/kg/minadding GLP-1 (P = NS). During thehyperglycemic-hyperinsulinemic clamp,GIR was 6.16 0.5 mg/kg/min and 6.460.2 mg/kg/min adding GLP-1 (P = NS).Endothelial-independent vasodilatationwas not affected in any of the experi-ments (data not shown).
CONCLUSIONS
This study confirms that both insulin andGLP-1 have a vasodilatory, antiinflam-matory, and antioxidant action (1–7).However, in this study, for the firsttime in type 2 diabetes, we show thatwhen GLP-1 and insulin are simulta-neously infused their vasodilatory, anti-inflammatory, and antioxidant action isenhanced. It is worthy of interest thatthe effect of GLP-1 is almost equivalentto that of hyperinsulinemia and is pres-ent in both normo- and hyperglycemia.
Our data are partially in the same di-rection of thework of Tesauro et al. (10),which showed an enhancement of thevasodilatory action of insulin by GLP-1 inthe metabolic syndrome. In the study ofTesauro et al. (10), GLP-1 was active inimproving vasodilation only in the pres-ence of hyperinsulinemia, while ourstudy confirms that GLP-1 has a directeffect on endothelial function even innormoinsulinemia. In the same direc-tion is the evidence that GLP-1 can in-duce endothelial vasodilation in normalsubjects (14). Moreover, it is worthy ofinterest that in the study of Tesauro et al.(10), a lack of the effect of GLP-1 wasreported in the obese subjects withoutthe metabolic syndrome (10). A possibleexplanation is that people with the met-abolic syndromediffer fromother people,responding differently to GLP-1, as alsosuggested by Tesauro et al. (10).
It must also be underlined that in ourstudy, GLP-1 was infused systemically,whereas in the study of Tesauro et al.(10) it has been given locally. Therefore,other potential factors might have beeninvolved in the effects of GLP-1 on en-dothelial function.
Furthermore, our study shows thatthe antiinflammatory and antioxidantaction of insulin and GLP-1 is also en-hanced when they are acutely adminis-tered in type 2 diabetes. Evidence iscumulating showing that both insulinand GLP-1 alone have such characteris-tics (1–7); however, in our opinion, thepossibility that when they are combinedthe single property of each of them isamplified is very interesting for the pos-sible clinical implications.
The combination of insulin and GLP-1RA analogs is today receiving a lot ofattention as a possible therapeuticchoice for the management of type 2diabetes (9). The evidence that this com-bination cannot only improve the meta-bolic control but also significantlyimpact on the cardiovascular risk profileof the diabetic patients is certainly ofgreat interest. Of course, specific clinicaltrials are needed to confirm the useful-ness of this therapeutic possibility.
The mechanism by which GLP-1 andinsulin reciprocally enhance their prop-erties remains speculative.
In diabetes, but not only in diabetes,it has been suggested that oxidativestress can favor the appearance of en-dothelial dysfunction and inflammation
1940 Effect of GLP-1 on Insulin Action Diabetes Care Volume 37, July 2014
(15,16). Both insulin and GLP-1 have anantioxidant property, which, however,follows different paths: insulin reducesfree radical production (1), while GLP-1increases the intracellular antioxidant de-fenses (8). Therefore, even though clearlythis is not the only possible explanation, itcould behypothesized thatwhen they arecombined the final antioxidant effect isenhanced. This may result in a greaterreduction of the oxidative stress, leading
to a greater decrease of inflammationand to a better improvement of the en-dothelial dysfunction.
A possible interference of the so-matostatin analog in our study could behypothesized. Annamalai et al. (17) re-cently reported that chronic treatment(24 weeks) with a somatostatin analog,lanreotide, improved endothelial func-tion in patients with newly diagnosed ac-romegaly. The study, therefore, reports
a possible effect of somatostatin and itsanalogs on endothelial function whenchronically administered. However, thereare several studies reporting that somato-statin and its analogs do not have any ef-fect on endothelial function when acutelyadministered (18–20). Therefore, a possi-ble direct effect of somatostatin in ourstudy can be convincingly excluded.
There was a slight difference in GIRbetween the experiments. This would
Figure 1—Changes in glycemia, FMD, IL-6, sICAM-1, nitrotyrosine, and 8-iso-PGF2a during normoglycemic-normoinsulinemic and normoglycemic-hyperinsulinemic clamps in type 2 diabetes (n = 12). Glycemia, FMD, IL-6, sICAM-1, nitrotyrosine, and 8-iso-PGF2a changes during normoglycemic-normoinsulinemic clamp (4), normoglycemic-normoinsulinemic clamp plus GLP-1 (▲), normoglycemic-hyperinsulinemic clamp (N), andnormoglycemic-hyperinsulinemic clamp plus GLP-1 (-). Data are means 6 SEM. *P , 0.01 vs. basal. £P, 0.05 vs. normoglycemic-normoinsulinemicclamp. §P , 0.05 vs. normoglycemic-normoinsulinemic clamp plus GLP-1. #P, 0.05 vs. normoglycemic-hyperinsulinemic clamp.
care.diabetesjournals.org Ceriello and Associates 1941
mean a higher “glucose turnover” that initself could be of relevance for endothelialdysfunctionor its improvement.However,in our opinion, a higher glucose turnoveris not supposed to ameliorate endothelialdysfunction. On the contrary, higher intra-cellular concentrations of glucose, accord-ing to the available literature (15), couldmean increased intracellular oxidativestress. In this respect, we believe thatour results are further strengthened.In conclusion, this study shows, for
the first time, that GLP-1 and insulin
reciprocally enhance their vasodilatory,antioxidant, and antiinflammatory action,suggesting a further rationale for usingtheir combination in the clinical practice.
Duality of Interest. No potential conflicts ofinterest relevant to this article were reported.Author Contributions. A.C. contributed todata research, discussion, writing the manu-script, and reviewing and editing the manu-script. A.N. and L.B. contributed to dataresearch, discussion, and reviewing and editingthe manuscript. S.C., K.E., R.T., M.R., and S.G.
contributed to discussion and reviewing andediting the manuscript. L.L.S. and G.P. contrib-uted to data research and discussion. A.C. is theguarantor of this work and, as such, had fullaccess to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.
References1. Dandona P, Chaudhuri A, Ghanim H,Mohanty P. Insulin as an anti-inflammatoryand antiatherogenic modulator. J Am Coll Car-diol 2009;53(Suppl.):S14–S202. Dandona P, Aljada A,Mohanty P, et al. Insulininhibits intranuclear nuclear factor kappaB
Figure 2—Changes in glycemia, FMD, IL-6, sICAM-1, nitrotyrosine, and 8-iso-PGF2a during hyperglycemic-normoinsulinemic and hyperglycemic-hyperinsulinemic clamps in type 2 diabetes (n = 12). Glycemia, FMD, IL-6, sICAM-1, nitrotyrosine, and 8-iso-PGF2a changes during hyperglycemic-normoinsulinemic clamp (4), hyperglycemic-normoinsulinemic clamp plus GLP-1 (▲), hyperglycemic-hyperinsulinemic clamp (N), andhyperglycemic-hyperinsulinemic clamp plus GLP-1 (-). Data are mean 6 SEM. *P , 0.01 vs. basal. £P , 0.05 vs. hyperglycemic-normoinsulinemicclamp. §P , 0.05 vs. hyperglycemic-normoinsulinemic clamp plus GLP-1. #P , 0.05 vs. hyperglycemic-hyperinsulinemic clamp.
1942 Effect of GLP-1 on Insulin Action Diabetes Care Volume 37, July 2014

and stimulates IkappaB in mononuclear cellsin obese subjects: evidence for an anti-inflammatory effect? J Clin Endocrinol Metab2001;86:3257–32653. Monnier L, Colette C, Mas E, et al. Regulationof oxidative stress by glycaemic control: evi-dence for an independent inhibitory effect ofinsulin therapy. Diabetologia 2010;53:562–5714. Mudaliar S, Henry RR. Effects of incretin hor-mones on beta-cell mass and function, bodyweight, and hepatic and myocardial function.Am J Med 2010;123(Suppl.):S19–S275. Nystrom T, Gutniak MK, Zhang Q, et al. Ef-fects of glucagon-like peptide-1 on endothelialfunction in type 2 diabetes patients with stablecoronary artery disease. Am J Physiol EndocrinolMetab 2004;287:E1209–E12156. Ceriello A, Esposito K, Testa R, Bonfigli AR,Marra M, Giugliano D. The possible protectiverole of glucagon-like peptide 1 on endotheliumduring the meal and evidence for an “endo-thelial resistance” to glucagon-like peptide 1in diabetes. Diabetes Care 2011;34:697–7027. Ceriello A, Novials A, Ortega E, et al. Glucagon-like peptide 1 reduces endothelial dysfunc-tion, inflammation, and oxidative stress inducedby both hyperglycemia and hypoglycemia intype 1 diabetes. Diabetes Care 2013;36:2346–2350
8. Oeseburg H, de Boer RA, Buikema H, van derHarst P, van Gilst WH, Sillje HH. Glucagon-likepeptide 1 prevents reactive oxygen species-induced endothelial cell senescence throughthe activation of protein kinase A. ArteriosclerThromb Vasc Biol 2010;30:1407–14149. van der Klauw MM, Wolffenbuttel BH. Thecombination of insulin and GLP-1 analogues inthe treatment of type 2 diabetes. Neth J Med2012;70:436–44310. Tesauro M, Schinzari F, Adamo A, et al. Ef-fects of GLP-1 on forearm vasodilator functionand glucose disposal during hyperinsulinemia inthe metabolic syndrome. Diabetes Care 2013;36:683–68911. DeFronzo RA, Tobin JD, Andres R. Glucoseclamp technique: a method for quantifying in-sulin secretion and resistance. Am J Physiol1979;237:E214–E22312. Nauck MA, Heimesaat MM, Orskov C, HolstJJ, Ebert R, Creutzfeldt W. Preserved incretinactivity of glucagon-like peptide 1 [7-36 amide]but not of synthetic human gastric inhibitorypolypeptide in patients with type-2 diabetesmellitus. J Clin Invest 1993;91:301–30713. Ceriello A, Mercuri F, Quagliaro L, et al. De-tection of nitrotyrosine in the diabetic plasma:evidence of oxidative stress. Diabetologia 2001;44:834–838
14. Okerson T, Chilton RJ. The cardiovasculareffects of GLP-1 receptor agonists. CardiovascTher 2012;30:e146–e15515. Giacco F, Brownlee M. Oxidative stress anddiabetic complications. Circ Res 2010;107:1058–107016. Rashid K, Sinha K, Sil PC. An update on ox-idative stress-mediated organ pathophysiology.Food Chem Toxicol 2013;62:584–60017. Annamalai AK, Webb A, Kandasamy N, et al.A comprehensive study of clinical, biochemical,radiological, vascular, cardiac, and sleep param-eters in an unselected cohort of patients withacromegaly undergoing presurgical somato-statin receptor ligand therapy. J Clin EndocrinolMetab 2013;98:1040–105018. Marfella R, Verrazzo G, Acampora R, et al.Glutathione reverses systemic hemodynamicchanges induced by acute hyperglycemia inhealthy subjects. Am J Physiol 1995;268:E1167–E117319. Marfella R, Nappo F, De Angelis L,Siniscalchi M, Rossi F, Giugliano D. The effectof acute hyperglycaemia on QTc duration inhealthy man. Diabetologia 2000;43:571–57520. Esposito K, Nappo F, Marfella R, et al. Inflam-matory cytokine concentrations are acutely in-creased by hyperglycemia in humans: role ofoxidative stress. Circulation 2002;106:2067–2072
care.diabetesjournals.org Ceriello and Associates 1943






![GLP-1 Receptor Agonists for Type 2 Diabetes and Their Role ... · GLP-1RA vs. other injectables Insulin [37–40] - 1.0 to - 1.8 vs. - 0.9 to - 1.9e - 2.5 to - 4.1 vs.? 0.8 to ? 2.3f](https://img.pdfslide.us/doc/110x75/6132fd13dfd10f4dd73accc1/glp-1-receptor-agonists-for-type-2-diabetes-and-their-role-glp-1ra-vs-other.jpg)