Embed Size (px)
Citation preview

Simultaneous Biplane Coronaryand Pulmonary Arteriography:A Novel Technique for Definingthe Course of an Anomalous LeftMain Coronary Artery OriginatingFrom the Right Sinus of Valsalva
Andrew Wang, 1 MD, Mark W. Pulsipher, 1 MD,James Jaggers, 2 MD, Gail E. Peterson, 1 MD,Martin P. O’Laughlin, 3 MD, Thomas M. Bashore, 1 MD,and J. Kevin Harrison, 1* MD
We present a novel technique employing biplane cineangiogra-phy with simultaneous left coronary and pulmonary angiogra-phy to define the anomalous course of the left main coronaryartery when it originates from the right sinus of Valsalva. Thesebiplane cinearteriograms clearly define the relationship of theleft main coronary artery to the great vessels, allowing confidentdelineation of the interarterial variant from the other, benignvariants. We illustrate the advantages of this technique with twocases in which the course of the anomalous left main coronaryartery was incorrectly diagnosed using standard coronary arte-riography and magnetic resonance imaging. Cathet. Cardio-vasc. Diagn. 42:73–78, 1997. r 1997 Wiley-Liss, Inc.
Key words: coronary artery anomalies; congenital heart dis-ease; sudden death
INTRODUCTION
In adults referred for coronary angiography, congenitalcoronary artery anomalies are found in 0.6–1.3% [1,2] ofpatients. Although origin of the left main coronary arteryfrom the right sinus of Valsalva is an uncommon coronaryartery anomaly (1.3% of all coronary artery anomalies inone large series [2]), it remains a diagnostic challengebecause of the multiple possible pathways of the left main
coronary artery en route to the left side of the heart. Theleft main coronary artery may course 1) anterior to thepulmonary trunk, 2) within the ventricular septum be-neath the right ventricular infundibulum (septal course),3) between the aorta and pulmonary trunk (interarterialcourse), or 4) posterior to the aorta (Fig. 1). Accuratediagnosis of the pathway of an anomalous left maincoronary artery from the right aortic sinus is prog-nostically important, as the interarterial variant is associ-ated with symptoms of myocardial ischemia, syncope, andsudden cardiac death, and thus represents one ofthe few potentially serious coronary artery anomalies [3–9].The diagnosis of an anomalous coronary artery is
usually made by coronary arteriography. Although sev-eral angiographic techniques have been described todifferentiate the proximal course of a left main coronaryartery that originates from the right sinus of Valsalva,correct diagnosis remains difficult when using standardcoronary arteriography. Because the relationship of theproximal left coronary artery to the great vessels definesthe variants of this anomaly, simultaneous visualizationof the left main coronary artery and the great vessls (intwo angiographic views) should afford increased diagnos-tic accuracy and confidence.We herein present two cases of an anomalous origin of
the left main coronary artery from the right sinus ofValsalva that were incorrectly diagnosed by standardcoronary arteriography and magnetic resonance imaging.We describe a novel angiographic technique employingsimultaneous biplane coronary and pulmonary cineangiogra-phy to determine the proximal course of the anomalouscoronary artery in relation to the aorta and pulmonary trunk.
CASE 1
A 33-year-old woman was evaluated for a long historyof atypical chest pain unrelated to exertion and describedas sharp and pleuritic in nature. She was seen 1 monthbefore admission, diagnosed with pericarditis, and pre-scribed a course of corticosteroids and nonsteroidalantiinflammatory agents. She continued to have episodesof chest pain and underwent an exercise stress test, whichshowed no evidence of ischemia. Because of continuedepisodes of chest pain, cardiac catheterization was per-formed at another hospital; the results of this testindicated normal left ventricular function and origin ofthe left main coronary artery from the right sinus ofValsalva (Fig. 2). There was no evidence of significantobstructive coronary artery disease. Magnetic resonance
1Division of Cardiology, Department of Medicine, Duke UniversityMedical Center, Durham, North Carolina2Department of Surgery, DukeUniversityMedical Center, Durham,North Carolina3Division of Cardiology, Department of Pediatrics, Duke Univer-sity Medical Center, Durham, North Carolina
Contract Grant sponsor: National Institutes of Health, National Heart,Lung and Blood Institute; ContractGrant number: 2 T32 HL07101-21A.
*Correspondence to: Dr. J. Kevin Harrison, Box 3331, Duke UniversityMedical Center, Durham, NC 27710.
Received 6 January 1997; Revision accepted 23 March 1997
Catheterization and Cardiovascular Diagnosis 42:73–78 (1997)
r 1997 Wiley-Liss, Inc.

imaging with gradient echo was performed, and theproximal left main coronary artery was thought to coursebetween the ascending aorta and pulmonary trunk. Thepatient was referred to our institution for cardiac surgery.Right and left heart catheterization was repeated. A 7F
145°-angled pigtail catheter (Cordis, Miami, FL) wasplaced with its distal end in the main pulmonary artery.The left main coronary artery was cannulated with a 6FJudkins right-4 catheter (Mallinckrodt, St. Louis, MO).The left main coronary artery was hand-injected with 10ml of radiocontrast and a simultaneous pulmonary arterio-gram (40 ml of radiocontrast at 30 ml/s) was performedby using biplane cineangiography (30° right anterioroblique (RAO) and 60° left anterior oblique (LAO)projections). The left main coronary artery was seen toform a caudal and posterior loop before branching intothe left anterior descending and left circumflex coronaryarteries (Fig. 3). Levophase imaging of the ascendingaorta confirmed that the left main coronary artery had aposterior course around the aorta (Fig. 4). The rightcoronary artery originated normally from the right sinusof Valsalva, directly adjacent to the anomalous leftcoronary ostium. The ostium of the left main coronaryartery was normal in appearance, and there was nosignificant obstructive coronary artery disease visualizedin any of the coronary arteries. The patient was reassuredabout the noncardiac nature of her chest pain and hasremained stable.
CASE 2
A 39-year-old man was evaluated for an episode ofacute chest pain. The patient reported the sudden onset of
substernal chest pressure at rest with radiation of thediscomfort to both shoulders, associated with diaphoresisand pallor. The chest pain lasted approximately one hour.He reported similar episodes of chest discomfort associ-ated with strenuous exertion which had occurred over thepast four years. His risk factors for coronary arterydisease were hypertension and tobacco use.The patient was admitted to another hospital and a
myocardial infarction was ruled out by serial electrocar-diograms and creatine kinase isoenzyme measurements.Cardiac catheterization demonstrated normal left ventricu-lar function. The right coronary artery originated nor-mally from the right sinus of Valsalva and had a twosevere obstructive lesions in its midportion. The left maincoronary artery originated from the right sinus of Valsalvaand was thought to course posteriorly around the aortabefore bifurcating into the left anterior descending andleft circumflex arteries (Fig. 5). There was no significantobstructive disease in the left coronary artery.The patient was referred to our institution and under-
went right and left heart catheterization. The same type ofangled pigtail catheter was placed with its distal end inthe right ventricular outflow tract. The left main coronaryartery was difficult to cannulate and was reached with a6F Amplatz left-1 catheter (Cordis, Miami, FL). The leftmain coronary artery was hand injected with 10 ml ofradiocontrast and a pulmonary arteriogram (40 ml ofradiocontrast power injected at 30 ml/s) was simulta-neously performed using biplane cineangiography in the30° RAO and 60° LAO projections (Fig. 6). The initialcourse of the left main coronary artery was cranial andposterior, just superior to the pulmonic valve, and be-tween the ascending aorta and pulmonary trunk (Fig. 7).The ostium of the left main coronary artery was normaland no significant obstructive lesions were seen in the leftcoronary artery.The patient subsequently underwent cardiac surgery
with direct visualization of the anomalous left maincoronary artery between the ascending aorta and pulmo-nary trunk. Aortoplasty was performed in which theproximal, intramural portion of the left main coronaryartery was unroofed fromwithin the aorta, with relocationof its ostium to the left sinus of Valsalva and resuspensionof the aortic commissure between the right and leftsinuses of Valsalva [10]. The right coronary artery wasbypassed with anastomosis of the right internal mammaryartery to the distal right coronary artery. The patient hadan uneventful postoperative course and has had norecurrence of chest pain.
DISCUSSION
Defining the course of an anomalous origin of the leftmain coronary artery from the right sinus of Valsalva is adiagnostic challenge with important prognostic and thera-
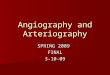
Fig. 1. The four possible courses of an anomalous left maincoronary artery (LCA) originating from the right sinus of Val-salva in relation to the great vessels: anterior free wall course(1); septal course (2); interarterial course (3); and retroaorticcourse (4). The right coronary artery (RCA) is also illustrated. A,aortic valve; PT, pulmonary trunk.
74 Wang et al.

peutic implications. This definition is difficult with stan-dard coronary angiography because the left main coro-nary artery can have one of four possible routes to the leftventricle before bifurcating into the left anterior descend-ing and left circumflex arteries. Simultaneous biplanecinearteriography of the left coronary artery and thepulmonary artery trunk (or right ventricular outflow tract)with continued levophase imaging of the ascending aortaallows visualization of the coronary artery relationship tothe great vessels and affords certainty in making thecorrect diagnosis. The 30° RAO and simultaneous 60°LAO projections provide the clearest definition of the
relationship between coronary artery and great vessels.We have attempted to illustrate these concepts in thesingle frame figures in this manuscript. Delineation ofthese structures is even clearer from the cineangiographicimage loops. Digital subtraction, where available, can beemployed to enhance the levophase images of the coro-nary artery-ascending aorta relationship.The relationship of the left main coronary artery to the
great vessels is prognostically important as the interarte-rial course of the left main coronary artery (between theaorta and pulmonary trunk) is strongly associated withclinically significant events such as myocardial ischemia,
Fig. 2. Coronary arteriogram of the anomalous left main coro-nary artery (large arrow) arising from the right sinus of Val-salva (Case 1). a: Anteroposterior view. b: 60° left anterioroblique view. The origin of the right coronary artery is visualizedby contrast reflux and is directly adjacent to the anomalousorigin of the left main coronary artery. An angled pigtail cathe-ter (small arrow) is positioned in the right ventricular outflowtract.
Fig. 3. Simultaneous biplane arteriograms of the pulmonarytrunk (PT) and left main coronary artery (arrow). a: 30° RAOprojection. b: 60° LAO projection. These images demonstratethat the left main coronary artery does not course between thegreat vessels but rather forms a caudal and posterior loop. Theleft main artery courses posterior to the aorta and then leftwardbefore branching into the left anterior descending and leftcircumflex coronary arteries.
Anomalous Left Main Coronary Artery 75

exertional syncope, and sudden cardiac death [3–9],whereas the other variants have largely benign prognoses.The potential mechanism of these adverse events inindividuals with an anomalous left main coronary arterycoursing between the great vessels includes 1) an abnor-mal, ‘‘slitlike’’ orifice of the left main coronary artery dueto the acute angle formed by the left main coronary arteryfrom the right sinus of Valsalva as it initially coursesposteriorly [13,14], and 2) compression of the left maincoronary artery between the aorta and pulmonary arterycausedbyoutwardexpansionof the roots of bothgreat vesselsduring exertion [4]. Patients, especially young or symptom-atic patients, inwhomananomalous leftmain coronary arteryarising from the right sinus of Valsalva with the interarterial
course is diagnosed should undergo surgical correction byeither coronary artery bypass grafting or aortoplasty.The two cases presented above demonstrate the diffi-
culty in diagnosing the course of the left main coronaryartery when it originates from the right sinus of Valsalva.In the first case, the patient was diagnosed as having ananomalous origin of the left main coronary artery withinterarterial course after standard coronary arteriographyand magnetic resonance imaging, but was subsequentlydemonstrated by simultaneous biplane coronary andpulmonary arteriography to have a benign variant, with aposterior course of the left main coronary artery aroundthe aorta. In the second case, the patient was initiallydiagnosed as having a benign variant following standardcoronary arteriography but was subsequently shown bysimultaneous arteriography to have an anomalous leftmain coronary artery with an interarterial course betweenthe aorta and pulmonary trunk. The diagnosis in this casewas confirmed by direct visualization at the time ofsurgery and corrected by aortoplasty.Previous reports have described the angiographic ap-
pearances of the four variants of this coronary anomaly[9-12]. The detection of septal perforators originatingfrom the left main coronary artery is specific for a septalcourse of the anomalous left coronary artery [8]. Serotaand colleagues [11] described the ‘‘dot and eye’’ methodto delineate the course of the left main coronary arteryarising from the right sinus of Valsalva. Ishikawa andBrandt [12] described the different proximal courses ofthe left main coronary artery with respect to the craniocau-dal and anteroposterior axes in the 30° RAO projection,and these angiographic appearances remain useful in thetwo cases presented here. Others have advocated placinga catheter in the main pulmonary artery to aid indetermining the course of the anomalous coronary arteryin relation to the pulmonary artery [15]. However, noneof these techniques fully addresses the need to visualizethe proximal course of the anomalous left main coronaryartery in relation to both great vessels. The methodillustrated by our two cases, involving simultaneousinjection of the anomalous left main coronary artery andpulmonary trunk with levophase imaging of the ascend-ing aorta, improves the visualization and spatial differen-tiation of these structures. The limitations to this methodare minimal and include an increased amount of intravas-cular radiocontrast (,40 ml) and a minimal increase inthe duration of the procedure.Recent studies have also described the usefulness of
noninvasive techniques, including transesophageal echo-cardiography and magnetic resonance angiography, fordelineating the proximal course of a left main coronaryartery originating from the right sinus of Valsalva.Fernandes and coworkers [16] reported that transesopha-geal echocardiography confirmed the course of the left
Fig. 4. Levophase imaging of the ascending aorta (smallarrows) with simultaneous anomalous left main coronary arteri-ography, demonstrating that the left main coronary artery (blackarrow) courses posterior to the aorta. a: 30° RAO projection. b:60° LAO projection.
76 Wang et al.

main coronary artery in nine patients in whom thediagnosis was made by standard coronary angiography.Others have reported that the proximal course of ananomalous left main coronary artery was accuratelydefined by magnetic resonance angiography [17–20]. Inthe case above, the initial, incorrect diagnosis of aninterarterial course may have resulted from the magneticresonance technique, as visualization of the coronaryartery is difficult with conventional cine gradient echomagnetic resonance imaging [18]. In addition, the use ofmagnetic resonance angiography for this purpose islimited to patients in sinus rhythm and without contraindi-cations to magnetic resonance imaging, such as thepresence of an indwelling pacemaker.
In conclusion, in patients with a left main coronaryartery originating from the right sinus of Valsalva,simultaneous biplane angiography of the left coronaryartery and pulmonary trunk, including levophase imagingof the ascending aorta, is useful for diagnosing the courseof the anomalous left main coronary artery and itsrelationship to the great vessels. Simultaneous 30° RAOand 60° LAO projections are optimal for defining theserelationships. These images readily distinguish the be-nign variants in which the left coronary artery coursesposterior to the aorta or anterior to the pulmonary artery.
Fig. 5. Coronary arteriogram of the anomalous left main coro-nary artery (large arrow) arising from the right sinus of Valsalva(Case 2). a: 30° RAO cranial projection. b: 60° LAO cranialprojection. An angled pigtail catheter (small arrow) is positionedin the right ventricular outflow tract. The adjacent ostium of theright coronary artery can be seen in panel b. Fig. 6. (Case 2) Biplane arteriography of the right ventricular
outflow tract (RV) and pulmonary trunk (PT) with simultaneousarteriography of the anomalous left main coronary artery (ar-rows), defining the anomalous left main coronary artery coursebetween the aorta and pulmonary trunk. a: 30° RAO projection.b: 60° LAO projection.
Anomalous Left Main Coronary Artery 77

The interarterial course between the great vessels is alsoclearly defined by using this technique. Visualization ofthe left main coronary artery superior to the pulmonicvalve and the absence of septal perforators originatingfrom the left main excludes a septal course. A craniopos-terior course of the proximal segment confirms aninterarterial course of the anomalous left main coronaryartery originating from the right sinus of Valsalva, andallows confident identification of the individuals whorequire surgical correction.
ACKNOWLEDGMENTS
Dr. Andrew Wang is supported by the National Insti-tutes of Health, National Research Service Award 2 T32HL07101-21A from the National Heart, Lung and BloodInstitute.
REFERENCES
1. Alexander RW, Griffith GC: Anomalies of the coronary arteriesand their clinical significance. Circulation 14:800–805, 1956.
2. Yamanaka O, Hobbs RE: Coronary artery anomalies in 126,595
patients undergoing coronary arteriography. Cathet CardiovascDiagn 21:28–40, 1990.
3. Liberthson RR, Dinsmore RE, Bharati S, Rubenstein JJ, CaulfieldJ, Wheeler EO, Harthorne JW, Lev M: Aberrant coronary arteryorigin from the aorta. Circulation 50:774–779, 1974.
4. Cheitlin MD, De Castro CM, McAllister HA: Sudden death as acomplication of anomalous left coronary artery from the anteriorsinus of Valsalva. Circulation 50:780–787, 1974.
5. Barth CW, Roberts WC: Left main coronary artery originatingfrom the right sinus of Valsalva and coursing between the aorta andpulmonary trunk. J Am Coll Cardiol 7:366–373, 1986.
6. Kimbiris D, Iskadrian AS, Segal BL, Bemis CE: Anomalous aorticorigin of coronary arteries. Circulation 58:606–615, 1978.
7. Roberts WC, Shirani J: The four subtypes of anomalous origin ofthe left main coronary artery form the right aortic sinus (or fromthe right coronary artery). Am J Cardiol 70:119–121, 1992.
8. Chaitman BR, Lesperance J, Saltiel J, Bourassa MG: Clinical,angiographic, and hemodynamic findings in patients with anoma-lous origin of the coronary arteries. Circulation 53:122–131, 1976.
9. Moodie DS, Gill C, Loop FL, Sheldon WC: Anomalous left maincoronary artery originating from the right sinus of Valsalva. JThorac Cardiovasc Surg 80:198–205, 1980.
10. Mustafa I, Gula G, Radley-Smith R, Durrer S, Yacoub M:Anomalous origin of the left coronary artery from the anterioraortic sinus: a potential cause of sudden death. J Thorac Cardio-vasc Surg 1981;82:297–300.
11. Serota H, Barth CW, Seuc CA, Vandormael M, Aguirre F, KernMJ: Rapid identification of the course of anomalous coronaryarteries in adults: The ‘‘dot and eye’’ method. Am J Cardiol65:891–898, 1990.
12. Ishikawa T, Brandt PWT: Anomalous origin of the left maincoronary artery from the right anterior aortic sinus: Angiographicdefinition of anomalous course. Am J Cardiol 55:770–776, 1985.
13. Benson PA, LackAR: Anomalous aortic origin of the left coronaryartery. Arch Pathol 86:214–216, 1968.
14. Cohen LS, Shaw LD: Fatal myocardial infarction in an 11-year oldboy associated with a unique coronary artery anomaly. Am JCardiol 19:420–423, 1967.
15. Chu E, Cheitlin MD: Diagnostic considerations in patients withsuspected coronary artery anomalies. Am Heart J 126:1427–1436,1993.
16. Fernandes F, Alam M, Smith S, Khaja F: The role of transesopha-geal echocardiography in identifying anomalous coronary arteries.Circulation 88:2532–2540, 1993.
17. Doorey AJ, Wills JS, Blasetto J, Goldenberg EM: Usefulness ofmagnetic resonance imaging for diagnosing an anomalous coro-nary artery coursing between aorta and pulmonary trunk. Am JCardiol 74:198–199, 1994.
18. Manning WJ, Li W, Cohen SI, Johnson RG, Edelman RR:Improved definition of anomalous left coronary artery by magneticresonance coronary angiography. Am Heart J 130:615–616, 1995.
19. McConnell MV, Ganz P, Selwyn AP, Li W, Edelman RR, ManningWJ: Identification of anomalous coronary arteries and theiranatomic course by magnetic resonance coronary angiography.Circulation 92:3158–3162, 1995.
20. Post JC, van Rossum AC, Bronzwaer JGF, de Cock CC, HofmanMBM, Valk J, Visser CA: Magnetic resonance angiography ofanomalous coronary arteries A new gold standard for delineatingthe proximal course? Circulation 92:3163–3171, 1995.
Fig. 7. (Case 2) Arteriogram of the right ventricular outflowtract (RV) in the 60° LAO projection, with simultaneous arteriog-raphy of the anomalous left main coronary artery (large arrow)originating from the right sinus of Valsalva. The left maincoronary artery origin is superior to the level of pulmonic valve(small arrow) and initially has a cranial and posterior course,confirming that the left main coronary artery lies between theaorta and pulmonary trunk.
78 Wang et al.


























![Case Report Unruptured right sinus of Valsalva aneurysm in ... · Sinus of Valsalva aneurysm (SVA) is a relatively rare heart disease in humans that is often congenital [1]. Overall,](https://img.pdfslide.us/doc/110x75/5fce3c69c541ea4a936c31c6/case-report-unruptured-right-sinus-of-valsalva-aneurysm-in-sinus-of-valsalva.jpg)