Embed Size (px)
Citation preview

Simulation
Proposed Device
Modified Helium Dilution1Standard Helium Dilution
Conclusion
Above: Schematic Diagram of the proposed device.
Right: Image of constructed prototype device. From top down: anesthesia bag in closed container, Collins Helium sensor, Millipore peristaltic pump
Our proposed device consists of 5 necessary components as well as an optional computer for data collection and analysis:
• Helium Sensor: The Collins Helium Sensor (Collins Medical, Braintree, MA) used in our prototype measures helium concentrations from 0-15%
• Pump: The Millipore peristaltic pump (Millipore, Billerica, MA) provides a variable flow rate to maintain gas flow across the helium analyzer as well as aid gas mixing within the sensing circuit
• Valve: A simple 3-way valve allows for selection of gas input to the neonate, either directly from the ventilator or from the sensing circuit.
• Anesthesia bag in airtight container: This component serves to maintain ventilator support for the neonate during measurement. The pressure exerted by the ventilator on the rubber anesthesia bag is transferred into the sensing circuit thus maintaining ventilator support.
•Ventilator: The sensing circuit is designed so that any ventilator or CPAP device can be used. At the Vanderbilt Children’s Hospital, the Evita 4 (Draeger Medical, Telford, PA) is the most commonly used.
Testing of the prototype device did not yield reliable results. We believe this was due to inadequate gas mixing within the sensing circuit.
Helium dilution is a commonly used method of measuring the functional residual capacity. The patient breathes from a known volume of gas with a known helium concentration. After the gas has had time to equilibrate with the patient’s lungs, the concentration is measured again. The FRC can be calculated using the equation below:
FRC VCiC f
1
Where Ci and Cf are the initial and final Helium concentrations, respectively, and V is the initial volume.
While potentially any gas can be used, Helium has some distinct advantages:• It is physiologically inert. It is not absorbed by the blood in any appreciable amount.• It is relatively common and inexpensive.
Standard helium dilution does have a drawback as well, it requires a closed system. Any leaks, like those from an uncuffed endotracheal tube, will make the measurement invalid.
Ane
sthe
sia
Bag
Ventilator
Pump
He Sensor
The standard helium dilution method can be modified to account for the effects of a leaky system. By assuming the leak can be expressed as an exponential function of time and measuring the helium concentration at 2 time points, we can estimate the equilibrium concentration if no leak was present using this equation:
C
f CHe' (t2)
CHe' (t1)
CHe' (t2)
t2 t2 t1
This estimate of the final concentration can then be used in the standard helium dilution equation to calculate the FRC.
Previous researchers have used this method with excellent results:•In Vitro
•Confirmed expected exponential relationship•Real vs. Calculated: r = 0.995, p<0.001
•In Vivo
CPAP (cm H2O)
0 3
FRC (ml/kg) 22.0 1.9 25.8 1.4
N 15 30
The Problem• Too small a FRC can result in the inability to oxygenate blood and
possibly death if blood entering the lung actually exits the lung without coming into contact with an exchangeable gas surface—shunting
• Current trial and error methods used to adjust ventilator settings can cause too much PEEP or CPAP which in turn can cause barotraumas, preventing the blood from going into the lung
• If ventilation techniques fail due to lack of oxygenation a patient is placed on ECMO (Extracorporeal Membrane Oxygenation) which constitutes a high probability of mortality
Background
Functional Residual Capacity (FRC) • Volume remaining in the lungs at resting
expiratory level• Equivalent to the alveolar volume (Va)
which contains 60-70% of the total lung volume
• Normal FRC in adults is 1.8 to 3.4 L• Estimated FRC in healthy neonates is ~25
mL
The Division of Neonatology at Vanderbilt Children’s Hospital has an interest in determining the Functional Residual Capacity (FRC) in neonates who are mechanically ventilated. Methods to determine FRC must be simple, non-invasive, and allow free access to neonates. Additionally, the method must be employed in the Neonatal Intensive Care Unit (NICU) which includes 60 intensive and intermediate beds, a 3 bed ECMO unit, and 10 bed intensive care nursery.
Determination of Ventilator Settings • X-rays can be used to help determine PEEP and O2 saturation level• Trial and error from years of experience is used to make adjustments to get sufficient oxygenation
Market Potential
Design Goals• Avoid complicated, dangerous, or invasive procedures • Uncooperative nature of an infant• Compatibility with any standard ventilator • Compact and mobile • Allow continued free access to the neonate• Compensate for leaks due to uncuffed endotracheal tubes
• No current patents on such a device• Standard Ventilation Costs at Vanderbilt Medical Center = $2000/day • ECMO Cost at Vanderbilt Medical Center = $5000/day • Reduces hospital costs because knowing FRC could prevent resorting to ECMO
Measurement of Functional Residual Capacity in Mechanically Ventilated Neonates
Douglas Anderson1, David Lammlein2, and Janine McKinnon1
Advisor: Dr. Bill Walsh, M.D.3
1 Vanderbilt University Department of Biomedical Engineering2 Vanderbilt University Department of Mechanical Engineering
3 Children’s Hospital at Vanderbilt University Division of Neonatology
Social Impact
This device has the potential to save many lives by eliminating the need for more dangerous or complicated procedures. The resulting impact on the friends and family of critically ill neonates will be profound. In addition, the procedure poses no environmental hazard as it uses helium, an inert gas, in its testing
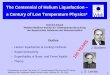
Circuit Helium Concentration vs. Time
6
6.5
7
7.5
8
8.5
9
0 20 40 60 80 100 120
Time (sec)
Hel
ium
Co
nce
ntr
atio
n (
%)
No Leak
Leak = 0.1 mL/sec
Lung Oxygen Content vs Time
0
50
100
150
200
250
0 20 40 60 80 100 120
Time (sec)
Oxy
gen
Par
tial
Pre
ssu
re (
mm
Hg
)
Leak = 0.1 mL/sec
No Leak
Our proposed device was simulated using a simple, two compartment model. For a circuit volume of 185 mL1, a neonate with a FRC of 26.5 mL1,2 and using normal parameters for ventilated neonates2 both the concentration of helium in the measuring circuit and oxygen content of the lungs were simulated for 2 leak states.
We calculated the FRC from the helium concentration data at 45 seconds in the no leak data at 45 and 60 seconds in the leak data:
No Leak: 26.5 mLLeak: 25.6 mL
• Modified Helium Dilution can be used to measure the FRC of a ventilated neonate with reasonable accuracy, even in a leaky system
• For a neonate with normal ventilation parameters, the oxygen content of the lungs remains at safe levels over the measurement period
• To ensure adequate gas mixing, the total volume of the sensing circuit must remain as low as possible without compromising the neonates oxygen levels
AcknowledgementsWe would like to sincerely thank Dr. Walsh and Dr. Paul King for their continued support and advice. We would like to thank Dr. Dan Lindstrom for aiding our equipment search. Finally, we would especially like to thank Chris Lynn, whose help on this project is immeasureable.
1Schwartz, JG, Fox, WW, Shaffer, TH. “A Method for Measuring Functional Residual Capacity in Neonates with Endotracheal Tubes.” IEEE Trans. Biomed. Engr. May 1978. 25(3): 304-307.2Szymankiewicz, M, Vidyasagar, D, Gadzinowski, J. “Predictors of successful extubation of preterm low-birth-weight infants with respiratory distress syndrome.” Pediatr Crit Care Med. 2005. 6(1): 44-49