Embed Size (px)
Citation preview

Simulation of ACL reconstruction dynamics for optimalrehabilitation planning
Andreas TsipouriarisUniversity of Patras,
Mechanical Engineering andAeronautics Department26500, Patras, Greece
Alexandros KogkasUniversity of Patras, Electrical
and Computer EngineeringDepartment
26500, Patras, [email protected]
Christina TriantafyllouUniversity of Patras, School of
Medicine26500, Patras, Greece
Konstantinos MoustakasUniversity of Patras, Electrical
and Computer EngineeringDepartment
26500, Patras, [email protected]
ConstantinosKoutsojannis
Technological and EducationalInstitute of Patras
26500, Patras, [email protected]
ABSTRACTThis paper presents a framework for simulated evaluationof the biomechanics of the human knee after anterior cruci-ate ligament (ACL) tear. Following the notion of the Vir-tual Physiological Human (VPH), a computational modelof both the kinematics and dynamics of the human kneeis developed that is subsequently simulated for typical mo-tions and activities. The proposed scheme provides a fea-sibility study on how VPH simulations can be used in apre-surgical step for optimal planning of several parametersrelated to the surgical procedure (e.g. physical vs. syntheticreconstruction, positioning, etc.). The effect of the choice ofthese parameters on the motor behaviour of the knee canbe estimated through the proposed simulation scheme, thusleading to a powerful clinical decision support system. Ex-perimental evaluation demonstrates the clinical potential ofthe proposed framework.
KeywordsVirtual physiological human, Simulation, ACL tear
1. INTRODUCTIONOne of the most common injuries in sports is related tothe partial or full tear of the anterior mainly, but also ofthe posterior cruciate ligament. Even if surgical reconstruc-tion practise can be nowadays considered being advanced,it is mainly based on expert judgement and less on objec-tive biomechanical evaluation of the patient’s physiology andeveryday activities, while patient-specific surgery customiza-tion is very rare.
1.1 Related workComputational modelling of human body parts is lately con-sidered to be an effective method for the study of mechanicalbehaviour of the knee joint. Single-phase and biphasic ana-lytical models of articular cartilage and their Finite Element(FE) or other simulations were first discussed in their arti-cle along with experimental studies by Huiskes and Chao[4]. Hasler et al presented the experimental methods andtheoretical models of articular cartilage and consequentlythe material properties for normal, pathologic, and repairedcartilages were discussed in [3]. Taylor and Miller workedon the macroscopic and microstructural constitutive modelsof cartilaginous tissues [13].
Weiss et al evaluated models of ligament in one-dimensionaland three-dimensional scales especially on the relationshipof microstructures and their mechanical behaviour [14]. Inanother work Provenzano et al examined the non-linear vis-coelastic models of ligaments based on the existing exper-imental data and evaluated their ability to predict the de-pendency on strain amplitude and frequency [12]. Elias andCosgarea analyzed different computational aspects of thepatellofemoral joint including modelling techniques, for ex-ample, patient-specific modelling, and clinical applications[2].
Mackerle published a deep study of articles between 1998and 2005 and provided an extensive list of publications indifferent areas of computational biomechanics including kneeand hip joints [8]. According to the previous knee jointmodels can be classified into analytical and computational.Analytical models with different degrees of accuracy havealready been published in the literature. These models wereused to describe the joint motion and kinematics in 2Dor 3D and to predict the loads in tendons, and ligaments[6],[11]. Other models included geometrical non-linearities[9],[10] and often effects of bones.
Although analytical models offered effective approaches todetermine knee kinematics, they had limited capacities todescribe the stress/strain patterns of cartilages, menisci, and

ligaments in 3D configurations. Moreover, the non-linear,anisotropic, and time-dependent response of the soft tissuescould not be captured using these approaches. In the ma-jority of joint models, articular cartilages were commonlymodelled as single-phase, linear elastic, homogeneous, andisotropic materials with constant stiffness [6],[11]. Concern-ing simulated replication of knee dynamics only a few ap-proaches have been presented in the past. A complete low-resolution model for disability simulation has been proposedin [5], while OpenSim, an open-source platform for biome-chanical simulation, has been introduced in [1].
1.2 Motivation and contributionClinical practise in ACL reconstruction is mainly based onexpert judgement and less on objective evaluation of thepatient’s physiology and behavioural profile. Moreover, apredictive decision support system enabling the clinician topredict the result of specific surgical decisions on the mo-tor behaviour of the specific patient, would enable patient-specific customization and optimization of the surgical pro-cedure. The proposed scheme aims to provide a feasibilitystudy on how simulated virtual physiological humans couldhelp towards the aforementioned grand challenge.
The rest of the paper is organized as follows. Section 2describes some aspects of the computational model of theknee, while Section 3 discusses how it can be simulated ina physics-based manner. Section 4 describes the applica-tion scenarios and experiments performed, while Section 5concludes the paper.
2. KNEE MODEL PROPERTIESThe main biomechanical roles of the knee joint complex arefirst to allow locomotion with (a) minimum energy require-ments from the muscles and (b) stability, accommodatingfor different terrains and second to transmit, absorb andredistribute forces caused during the activities of daily life.
During rotation in knee joint flexion extension is up to 160deg of flexion (up to -5 deg flexion-hyperextension), varus-valgus is up to 6-8 deg in extension and internal-externalrotation is up to 25-30 deg in flexion. Additionally duringtranslation anterior-posterior is up to 5-10 mm, compressionup to 2-5 mm and medio-lateral is up to 1-2 mm. The kneejoint kinematics in the sagittal plane during gait can be sum-marized in: a) Extension: contact is located centrally. b)Early flexion: posterior rolling; contact continuously movesposteriorly and c) Deep flexion: femoral sliding; contact islocated posteriorly; the unlocking of the ACL prevents fur-ther femoral roll back.
Since the development of a highly detailed biomechanicalmodel of the knee was out of the scope of this paper, amultiresolutional model has been developed, emphasizing onaspects that are important for ACL tear reconstruction andrehabilitation.
The major physical element for the proposed model is thejoint and in particular the knee joint. Movable human jointsare divided into four main categories, according to their de-grees of freedom (DOF) [7], namely uniaxial, biaxial, poli-axial and plane joints. Even, if a perfectly accurate modelwould require a plane joint with a purely physics based sim-
ulation approach, in the proposed framework and in orderto make the simulation tractable a biaxial joint is consid-ered. Moreover, customization of the model is possible withrespect to muscle activation and contraction dynamics, sub-ject specific customization (weight, height), ACL position-ing and dynamics parameters, e.g. stiffness, damping, tearthreshold.
3. SIMULATIONThe backbone of the proposed framework is the simulationengine. It aims to predict, for specific actions, the muscleactivation necessary for their execution and the resultingligament forces.
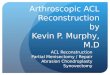
3.1 Simulation engineFigure 1 illustrates an overview of the proposed system. Itis mainly comprised of two independent entities, namely the“simulation” and “visual analytics” block. The simulationblock consists of the inverse kinematics and the inverse dy-namics modules, while supported by the action managementmodule.
Figure 1: Overview of the proposed framework
Inverse kinematics (IK) calculate the rotations necessary toachieve a desired end effector’s position and orientation. IKis the inverse problem of forward kinematics, which calculatethe position of a body and its end effector after applyinga series of joint rotations. The IK input parameters arethe desired end effector’s position and orientation and theoutput is a series of joint angles.
Based on a motion sequence defined through the IK proce-dure, inverse dynamics estimate the appropriate joint torquesthat are subsequently related to muscle forces, necessary topreform the specific motions.
The clinician can access the system through the visual an-alytics module that allows for model customization, tuningof critical parameters and visualization of the simulation re-sults. Moreover, it should be emphasized that the simulationplatform requires a formal definition of the musculoskeletalmodel to be simulated and a description of the action to beexecuted. These two requirements can be edited and cus-tomized by the visual analytics block that inherently servesas a clinical decision support system.
In the context of this work the authors emphasized on the

musculoskeletal modelling and simulation part, while thesimulation results are visually displayed. A full implemen-tation of the visual analytics block is left as future work.Finally, it should be mentioned that the proposed simula-tion framework is based on the OpenSim platform [1].
3.2 Parameterization and customizationThe table below describes the allowable parameterization ofthe knee model. “ACL positioning” refers to the positioningof the artificial ACL, usually tendon, on the bone that isconsidered as a critical parameter for surgical ACL recon-struction. The “Dynamics parameters” differ if a physical orsynthetic transplant is considered. “Model customization”and“Muscle parameters”relate actually to a rough personal-ization of the subject, while the “Actions” parameter reflectsthe potential activities that can be simulated.
Parameter type Variable
ACL positioning Tendon position coordinatesDynamics parameters Stifness, Damping, TearModel customization Weight, Height
Actions Activities to simulateMuscle parameters Activation dynamics
Table 1: Parameters and the corresponding compu-tational variables that can be tuned by the clinicianso as to drive the simulation
It should be emphasized that the values of these parametersreflect different strategies in ACL tear rehabilitation. Theultimate functionality of the proposed framework is to al-low the clinician to fine tune these parameters and proceedto a personalized rehabilitation plan, based on the patientsphysical and behavioural profile.
4. APPLICATION AND EXPERIMENTSThe clinical potential of the proposed framework has beeninvestigated in the context of ACL surgical reconstruction.In particular, the framework aims to provide decision sup-port with respect to several rehabilitation parameters, likesurgical reconstruction or not, artificial ligament surgical po-sitioning, etc. Of critical importance is the estimation of lig-ament and muscle loads in performing specific actions withrespect to the rehabilitation strategy adopted.
The behavioural result of each choice is demonstrated inmuscle and ligament forces, while performing a leg “swing”action. Figure 2 illustrates screenshots of the latter.
(a) (b) (c) (d)
Figure 2: Key-frames of the swing activity
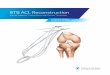
Figure 3 illustrates the comparison between 6 indicative per-formed experiments regarding the exerted forces on the pos-terior cruciate ligament (PCL) over time for the “swing” ac-tion. The paremeterization of the experimental models liesto the mass scaling and the positioning of the anterior cru-ciate ligament (ACL).
For the performed experiments, the Computed Muscle Con-trols (CMC) and Inverse Dynamics tools where incorporated[1]. The CMC tool computes muscle excitation levels atspecified time intervals, that will drive the generalized co-ordinates (e.g., joint angles) of a dynamic musculoskeletalmodel towards a desired kinematic trajectory. CMC doesthis by using a combination of proportional-derivative (PD)control and static optimization. The inverse dynamics tooluses the CMC generated motion of the model to solve theequations of motion for the unknown generalized forces.
Regarding the mass parameterization of the musculoskeletalmodel, two different instances were chosen; an initial form ofthe model and a second version of an increased mass by 20%.In each scenario, four different ACL positioning states wherechosen; the absence of the ACL and presence of the ACL inthree different positions. The location of the ACL refers toits contact point on the tibia, moving it in a relatively twodimensional plane, forming an equilateral triangle.
Each diagram represents the comparison of the exerted forceson the PCL, between the absence of the ACL scenario andthe three simulated positioning states, on each one of the twomass scaled models. For the baseline weighted model, “type2” positioning seems optimal in terms of the force appliedon the PCL, while for the weight scaled model the optimalpositioning choice is of “type 1”. The relative differentiationof the exerted forces on the PCL is prominent, providinga decision support framework for the planning of the ACLsurgical reconstruction.
5. DISCUSSION AND CONCLUSIONSThe aim of this work is to provide a feasibility study on theuse of virtual physiological human (VPH) knee models foroptimal rehabilitation and reconstruction planning of ACLtear. A computational model of both the kinematics and dy-namics of the human knee is developed that is subsequentlysimulated for custom motions and activities. The proposedscheme provides a feasibility study on how VPH simulationscan be used in a pre-surgical step for optimal planning of sev-eral parameters related to the surgical procedure. The effectof the choice of these parameters on the motor behaviour ofthe knee can be estimated through the proposed simulationscheme, thus leading to a powerful clinical decision supportsystem.
Even if the potential use of such a framework is evident,there are several issues that still need to be considered. Evenif, by definition, the proposed scheme aims to provide rela-tive evaluations of different rehabilitation treatment strate-gies as mentioned in Section 4 a clinical validation of thesimulation results is still necessary. Moreover, it is still im-portant to allow interaction of the existing knee models withsoft tissues like the menisci that is also a major direction forfuture work.

(a) (b) (c)
(d) (e) (f)
Figure 3: Exerted forces on the posterior cruciate ligament (PCL) over time for the swing action. In eachdiagram the red curve corresponds to the baseline, where no ACL is present. The blue curve correspondsto the reconstruction in different positioning (”type 1”, “type 2”, “type 3”) for the specific the mass scaledmodel. In the top row the diagrams correspond to the baseline model and the bottom row to the mass scaled(120%) model.
6. ACKNOWLEDGEMENTSThis work is partially funded by the EC FP7 project NoTremor:Virtual, Physiological and Computational NeuromuscularModels for the Predictive Treatment of Parkinson’s Disease,Grant Agreement No. 610391.
7. REFERENCES[1] S. Delp, F. Anderson, A. Arnold, P. Loan, A. Habib,
C. John, E. Guendelman, and D. Thelen. Opensim:Open-source software to create and analyze dynamicsimulations of movement. Biomedical Engineering,IEEE Transactions on, 54(11):1940–1950, Nov 2007.
[2] J. Elias and A. Cosgarea. Computational modeling:an alternative approach for investigatingpatellofemoral mechanics. Sports Medicine andArthroscopy Review, 15(2):89–94, 2007.
[3] E. Hasler, W. Herzog, and J. Wu. Articular cartilagebiomechanics: theoretical models, material properties,and biosynthetic response. Critical Reviews inBiomedical Engineer, 27(6):415–488, 1999.
[4] R. Huiskes and E. Y. S. Chao. A survey of finiteelement analysis in orthopedic biomechanics: the firstdecade. Journal of Biomechanics, 16(6):385–409, 1983.
[5] N. Kaklanis, P. Moschonas, K. Moustakas, andD. Tzovaras. Virtual user models for the elderly anddisabled for automatic simulated accessibility andergonomy evaluation of designs. Springer InternationalJournal of Universal Access in the InformationSociety, 12(4):403–425, November 2013.
[6] L. Li and K. Gu. Reconsideration on the use of elasticmodels to predict the instantaneous load response ofthe knee joint. Proceedings of the Institution ofMechanical Engineers H, 225(9):888–896, 2011.
[7] A. Maciel, L. Nedel, and C. Freitas. Anatomy basedjoint models for virtual human skeletons. IEEEComputer Animation, Geneva, 2002.
[8] J. Mackerle. Finite element modeling and simulationsin orthopedics: a bibliography 1998-2005. ComputerMethods in Biomechanics and Biomedical Engineering,9(3):149–199, 2006.
[9] S. Masouros, A. Bull, and A. Amis. Mainbiomechanical roles of the knee joint complex. OrthopTrauma, 24:84–91, 2010.
[10] S. Messier, C. Legault, R. Loeser, S. V. Arsdale,C. Davis, W. Ettinger, and P. DeVita. Does highweight loss in older adults with knee osteoarthritisaffect bone-on-bone joint loads and muscle forcesduring walking? Osteoarthritis and Cartilage,19(3):272–280, 2011.
[11] E. Pena, B. Calvo, M. Martinez, and M. Doblare. Athree-dimensional finite element analysis of thecombined behavior of ligaments and menisci in thehealthy human knee joint. Journal of Biomechanics,39(9):1686–1701, 2006.
[12] P. Provenzano, R. Lakes, and D. Corr. Application ofnonlinear viscoelastic models to describe ligamentbehavior. Biomechanics and modeling inmechanobiology, 1(1):45–57, 2002.
[13] Z. Taylor and K. Miller. Constitutive modeling ofcartilaginous tissues: a review. Journal ofBiomechanics, 22(3):212–229, 2006.
[14] J. Weiss, J. Gardiner, and B. Ellis. Three-dimensionalfinite element modeling of ligaments: technicalaspects. Medical Engineering and Physics,27(10):845–861, 2005.