Embed Size (px)
Citation preview
Simulating Quadriceps Muscle Atrophy and Activation Deficits during Gait
Julie ThompsonStanford University
Can’t hear us? Select Audio -> Integrated VoIP
-> Join Conference
Simulating Quadriceps Muscle Atrophy and Activation Deficits during Gait
5
Webinar Objectives
• Background on prevalence of quadriceps muscle weakness• 2 types of weakness: atrophy and activation deficit
• Motivating questions• How we addressed questions using OpenSim• Methodological details of simulating weakness• Major findings and take-away
• Thompson et al., Journal of Biomechanics; 46(13): 2165-72, 2013.
6
Background
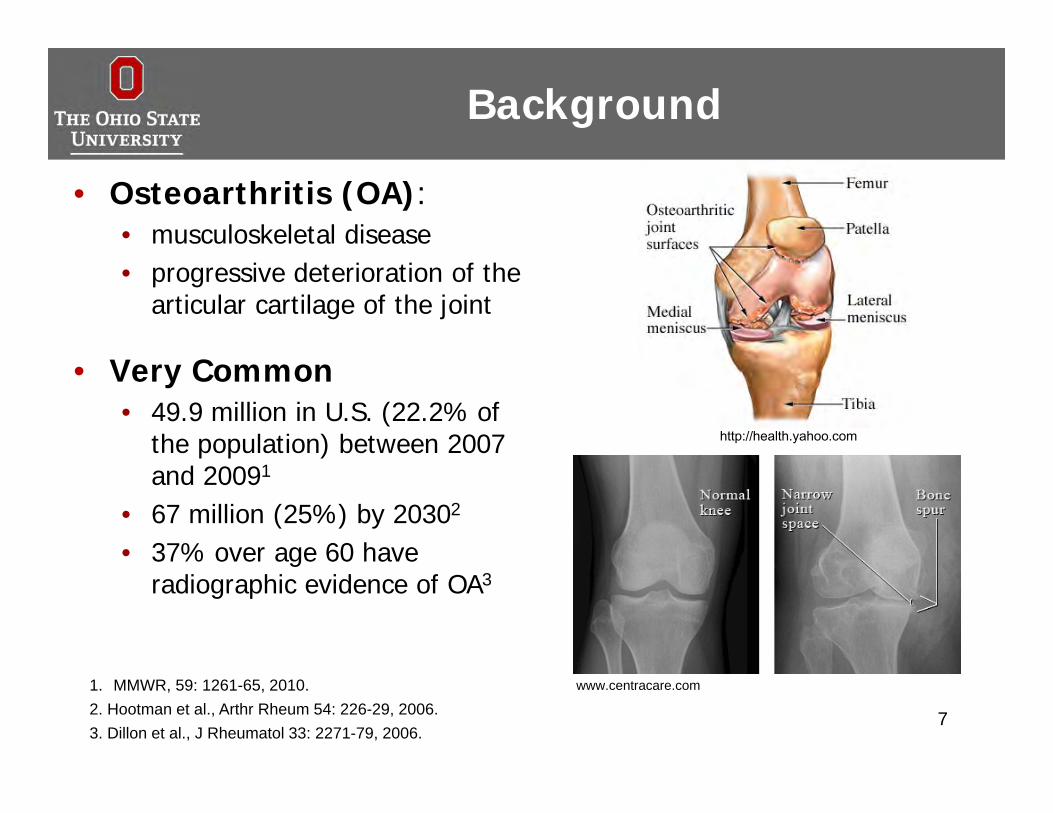
• Osteoarthritis (OA): • musculoskeletal disease • progressive deterioration of the
articular cartilage of the joint
• Very Common• 49.9 million in U.S. (22.2% of
the population) between 2007 and 20091
• 67 million (25%) by 20302
• 37% over age 60 have radiographic evidence of OA3
7
http://health.yahoo.com
www.centracare.com1. MMWR, 59: 1261-65, 2010.2. Hootman et al., Arthr Rheum 54: 226-29, 2006.3. Dillon et al., J Rheumatol 33: 2271-79, 2006.
Background
• Approximately 21.1 million adults in the U.S. report activity limitations due to symptoms of arthritis1
• Increased dependence and difficulty during activities2:• Climbing stairs, Walking
84. Moxley Scarborough et al., Gait Posture 10: 10-20, 1999.3. Lord et al., J Am Geriatr Soc 47: 1077-81, 1999.
5. Walsh et al., Phys Ther 78: 248-58, 1998.
unitednationsroadrunners.orgHealthsharenews.blogspot.com
www.besthealthtips4you.com
2. Fisher et al., SJRM 29: 213-21, 1997.1. MMWR, 59: 1261-65, 2010.
http://daiseypt.com/Articles/anatomyart/quads.htm
Background
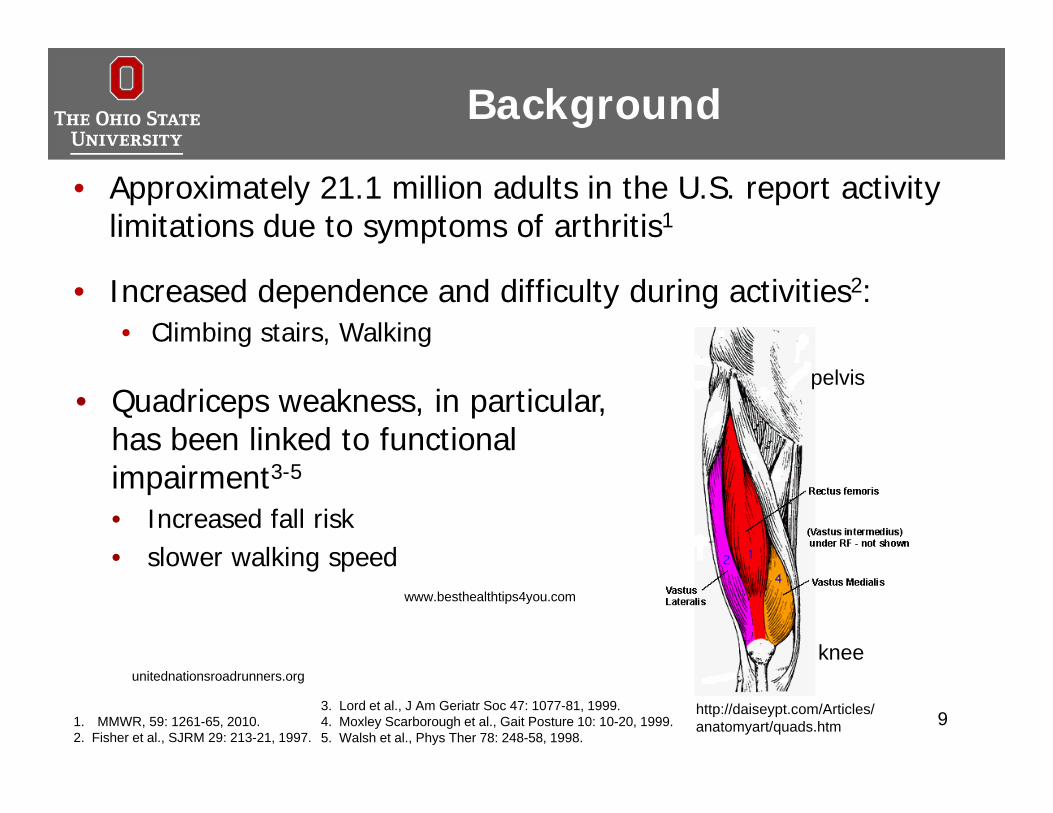
• Approximately 21.1 million adults in the U.S. report activity limitations due to symptoms of arthritis1
• Increased dependence and difficulty during activities2:• Climbing stairs, Walking
9
• Quadriceps weakness, in particular, has been linked to functional impairment3-5
• Increased fall risk• slower walking speed
4. Moxley Scarborough et al., Gait Posture 10: 10-20, 1999.3. Lord et al., J Am Geriatr Soc 47: 1077-81, 1999.
5. Walsh et al., Phys Ther 78: 248-58, 1998.
unitednationsroadrunners.orgHealthsharenews.blogspot.com
www.besthealthtips4you.com
2. Fisher et al., SJRM 29: 213-21, 1997.1. MMWR, 59: 1261-65, 2010.
http://daiseypt.com/Articles/anatomyart/quads.htm
pelvis
knee
Quadriceps Weakness
• Quadriceps weakness is one of the earliest and most common symptoms of OA1
• Two sources of muscle weakness:• Atrophy
• Decrease in number or size of muscle fibers
• Reduced voluntary activation• Inability to recruit (activate) all of the muscle’s motor units2
(groupings of muscle fibers)
92. Kent-Braun and Le Blanc, Muscle Nerve 19: 861-69, 1996.1. Fisher et al., Disab Rehab 19: 47-55, 1997.
Quadriceps Weakness
• Strength deficits• As high as 38% in late stage OA1
• As high as 64% after total knee replacement for treatment of knee OA2
• Activation deficits• As high as 34% in OA3
• Underlying mechanism relating quadriceps function to gait impairments is unknown
10
1. Petterson et al., JBJS Am-89: 2327-33, 2007.
3. Hassan et al., Ann Rheum Dis 60: 612-18, 2001.
2. Mizner et al., Phys Ther 83: 359-65, 2003.
Dynamic Computer Simulations
• Powerful tool for investigating cause-effect relationships1
• Allow us to determine individual roles of muscles in coordinated movement
• Predictive studies: how muscle function changes in response to rehab, surgery, or gait re-training
111. Delp et al., IEEE Trans Biomed Eng 54: 1940-50, 2007.
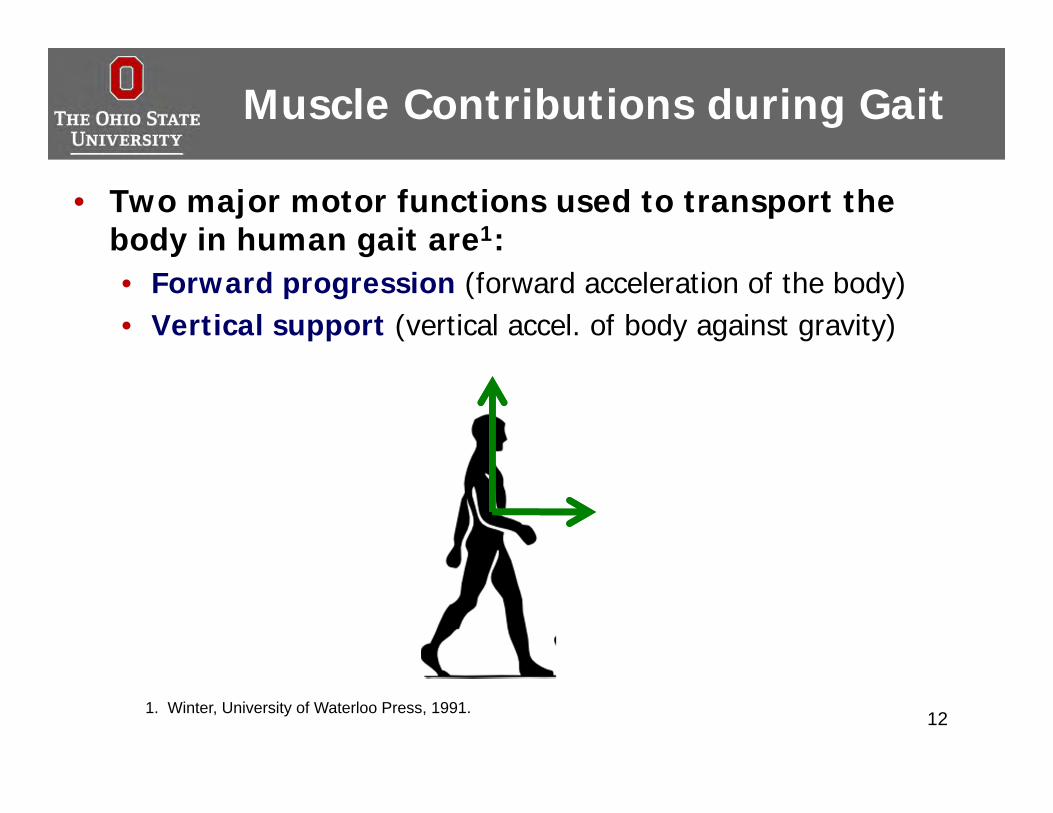
Muscle Contributions during Gait
• Two major motor functions used to transport the body in human gait are1:• Forward progression (forward acceleration of the body)• Vertical support (vertical accel. of body against gravity)
121. Winter, University of Waterloo Press, 1991.
Previous Research
• Previous research has investigated muscle function in healthy and some pathological populations1-6
• Main contributors to progression and support during gait are the quadriceps, gluteus maximus, and plantarflexors
• Muscle force generally increases with gait speed
131. Higginson et al., J Biomech 39: 1769-77, 2006.2. Liu et al., J Biomech 39: 2623-30, 2006. 5. Steele et al., J Biomech 43: 2099-105, 2010.
6. Van der Krogt et al., Gait Posture 36: 113-9, 2012.
4. Neptune et al., Gait Posture 19: 194-205, 2004.
3. Liu et al., J Biomech 41: 3243-52, 2008.
Motivating Questions
• Muscle compensations in populations with weak quadriceps
• Do other muscles compensate for weakness in the quadriceps? How?
• Do compensations differ between the two types of weakness (atrophy and activation failure)?
14
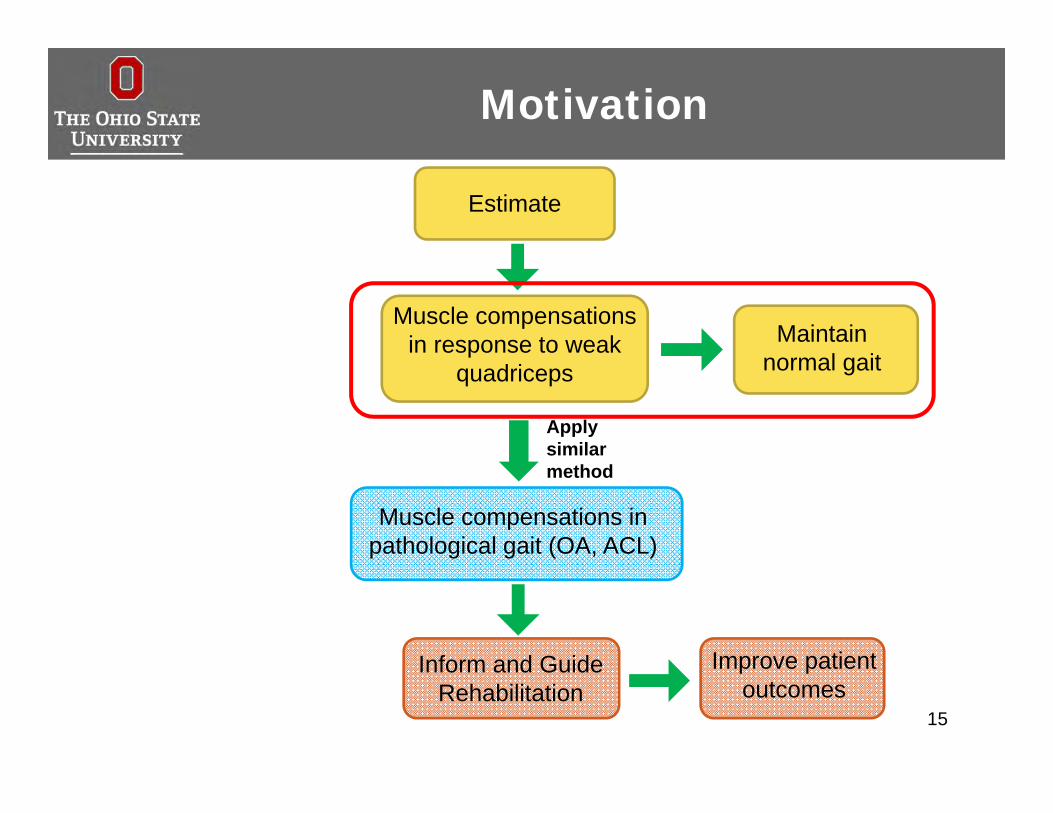
Motivation
15
Estimate
Maintain normal gait
Muscle compensations in response to weak
quadriceps
Improve patient outcomes
Inform and Guide Rehabilitation
Apply similar method
Muscle compensations in pathological gait (OA, ACL)
Purpose
• To estimate changes in muscle forces and contributions to support and progression to maintain normal gait in response to two sources of quadriceps muscle weakness: atrophy and activation failure
16
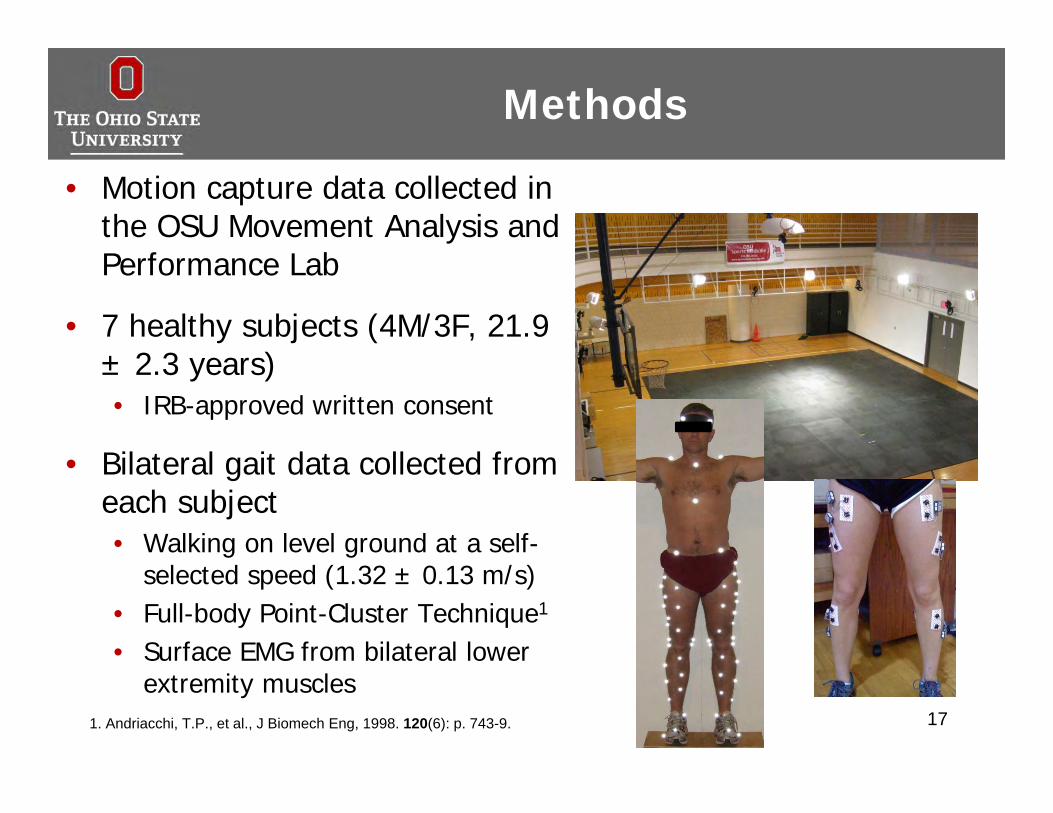
Methods
• Motion capture data collected in the OSU Movement Analysis and Performance Lab
• 7 healthy subjects (4M/3F, 21.9 ± 2.3 years)• IRB-approved written consent
• Bilateral gait data collected from each subject• Walking on level ground at a self-
selected speed (1.32 ± 0.13 m/s)• Full-body Point-Cluster Technique1
• Surface EMG from bilateral lower extremity muscles
171. Andriacchi, T.P., et al., J Biomech Eng, 1998. 120(6): p. 743-9.
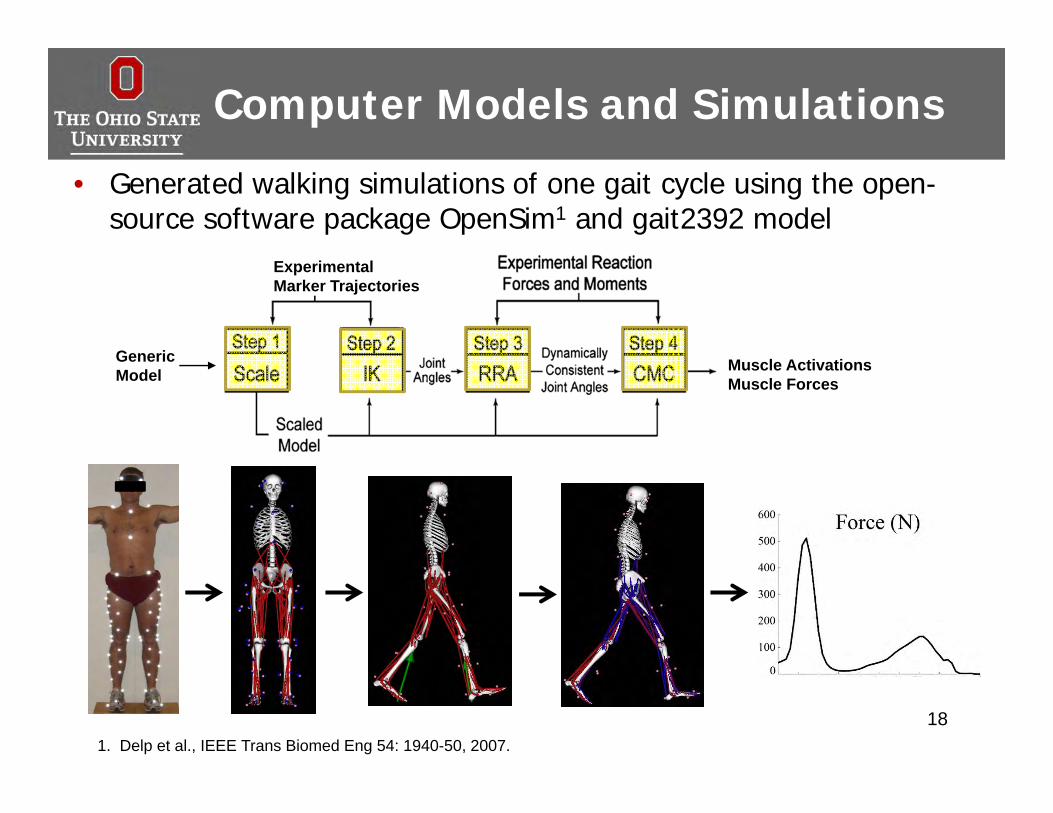
Computer Models and Simulations
• Generated walking simulations of one gait cycle using the open-source software package OpenSim1 and gait2392 model
181. Delp et al., IEEE Trans Biomed Eng 54: 1940-50, 2007.
Experimental Marker Trajectories
Muscle ActivationsMuscle Forces
Generic Model
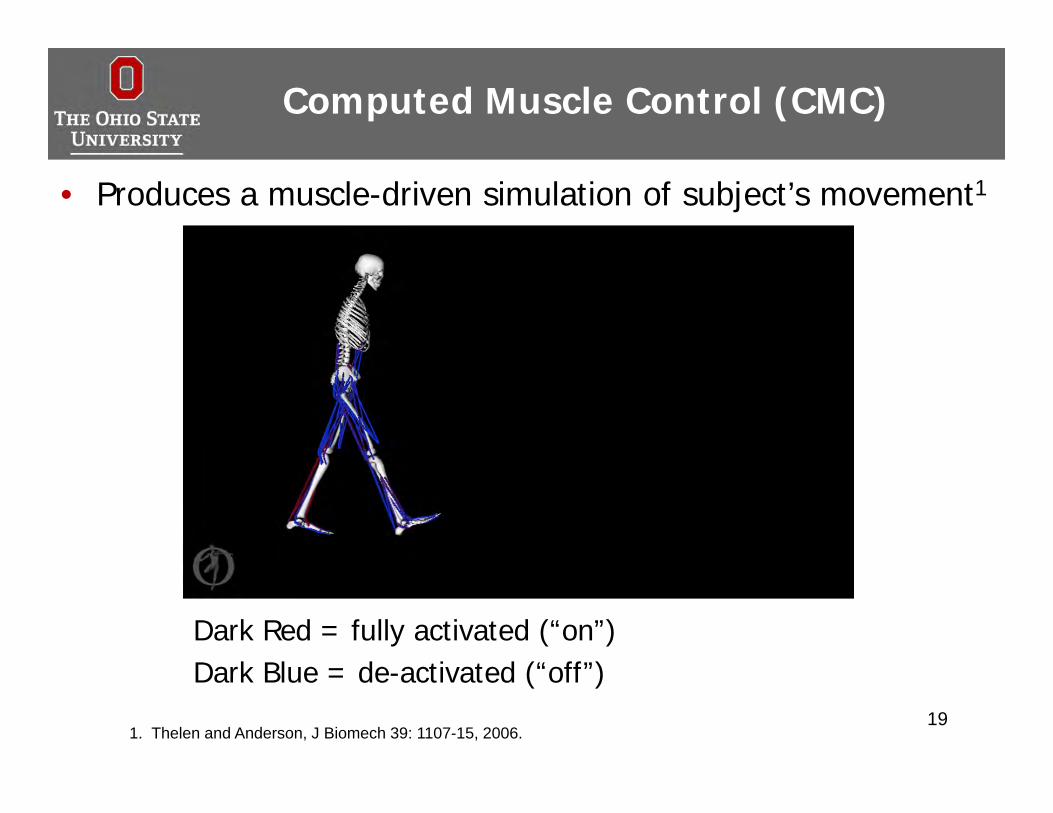
Computed Muscle Control (CMC)
• Produces a muscle-driven simulation of subject’s movement1
191. Thelen and Anderson, J Biomech 39: 1107-15, 2006.
Dark Red = fully activated (“on”)Dark Blue = de-activated (“off”)
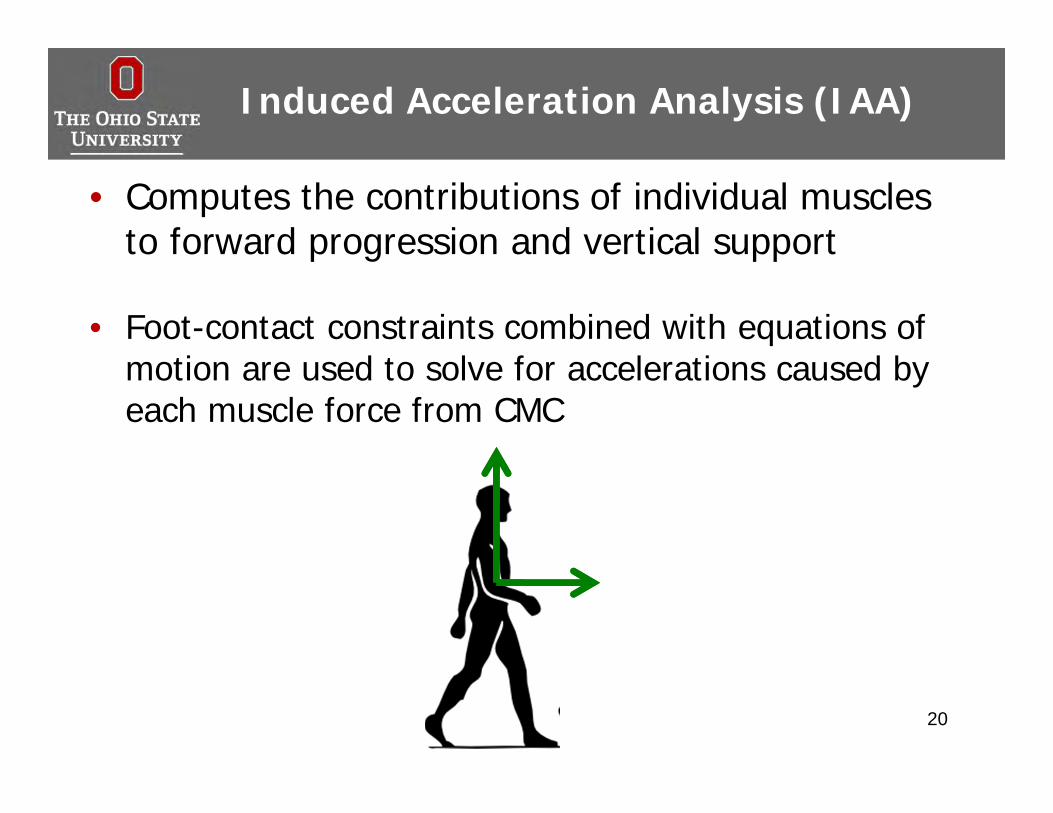
Induced Acceleration Analysis (IAA)
• Computes the contributions of individual muscles to forward progression and vertical support
• Foot-contact constraints combined with equations of motion are used to solve for accelerations caused by each muscle force from CMC
20
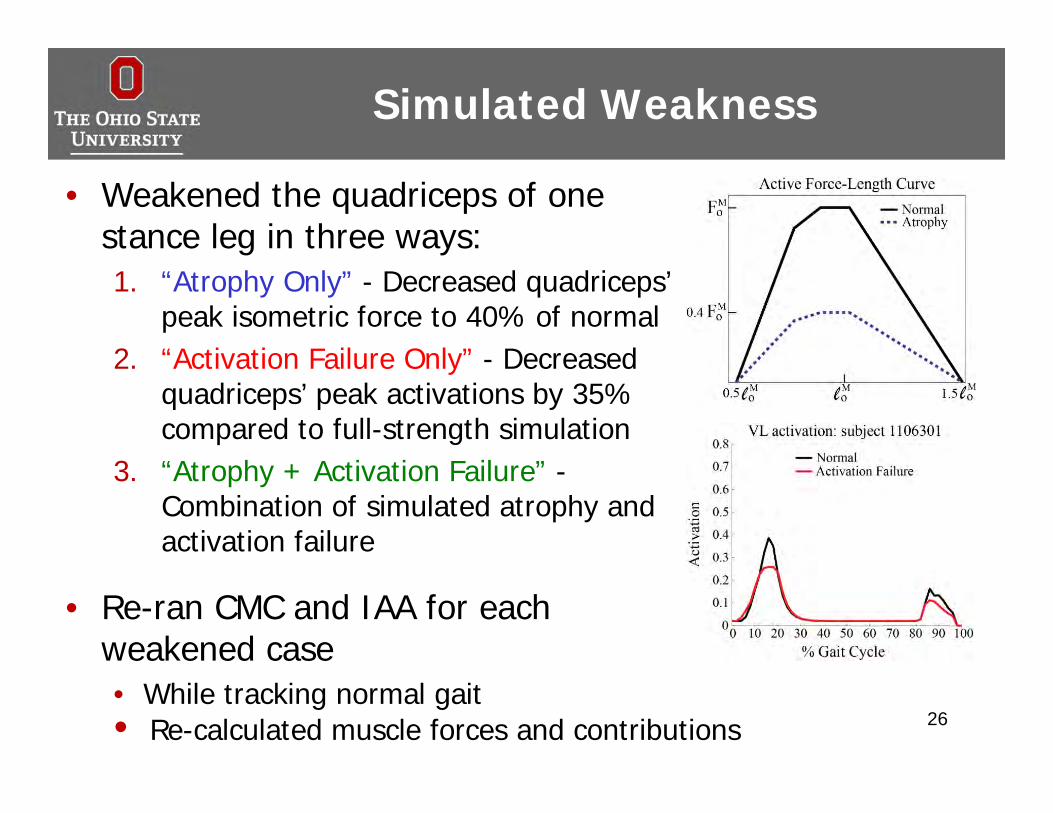
• Weakened the quadriceps of one stance leg in three ways:
Simulated Weakness
21
Simulated Weakness
22
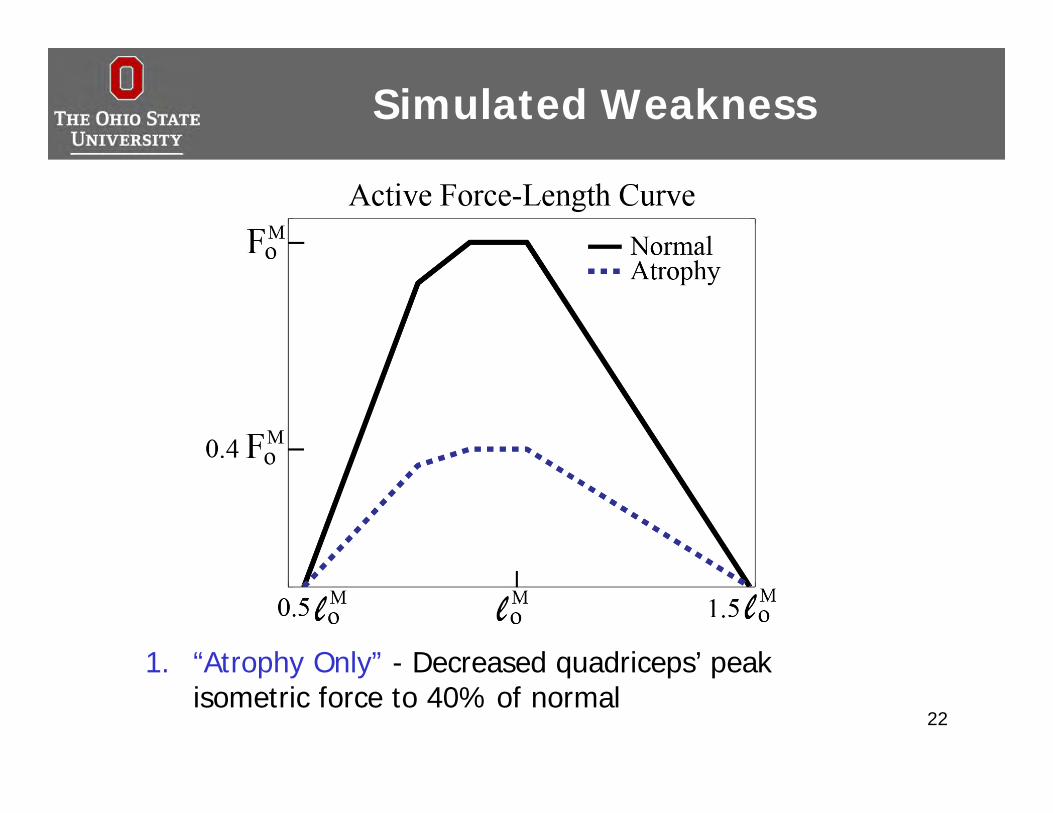
1. “Atrophy Only” - Decreased quadriceps’ peak isometric force to 40% of normal
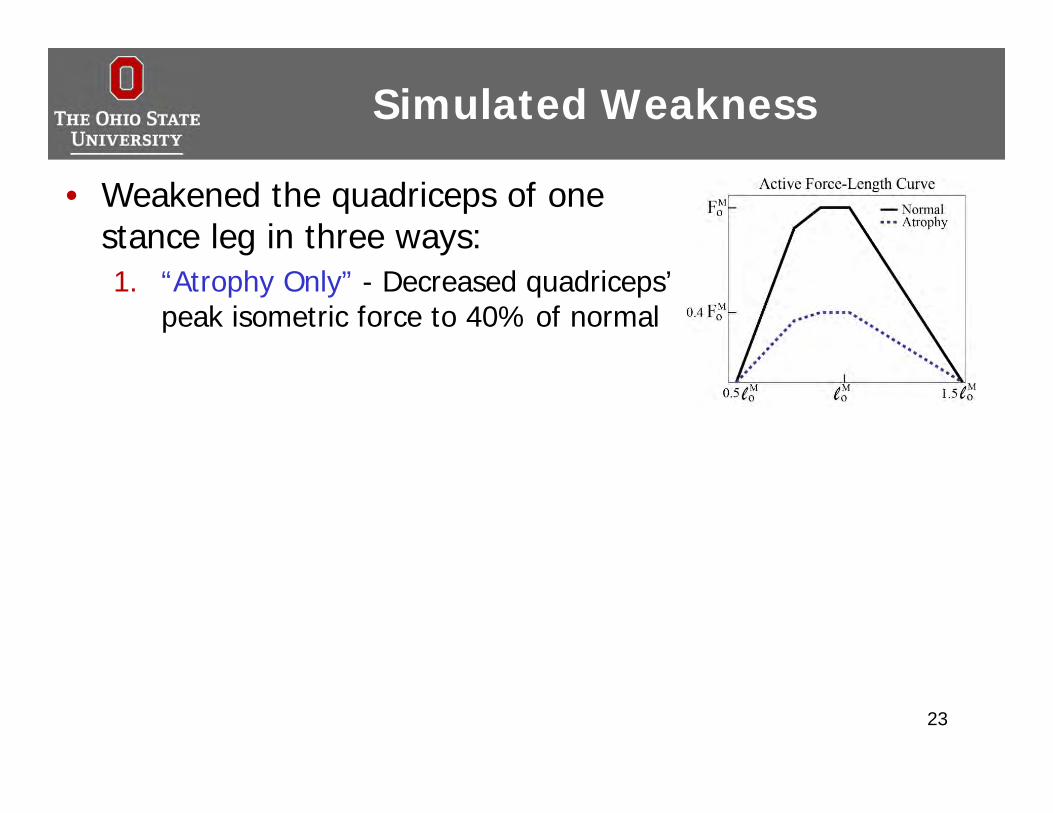
• Weakened the quadriceps of one stance leg in three ways:1. “Atrophy Only” - Decreased quadriceps’
peak isometric force to 40% of normal
Simulated Weakness
23
Simulated Weakness
24
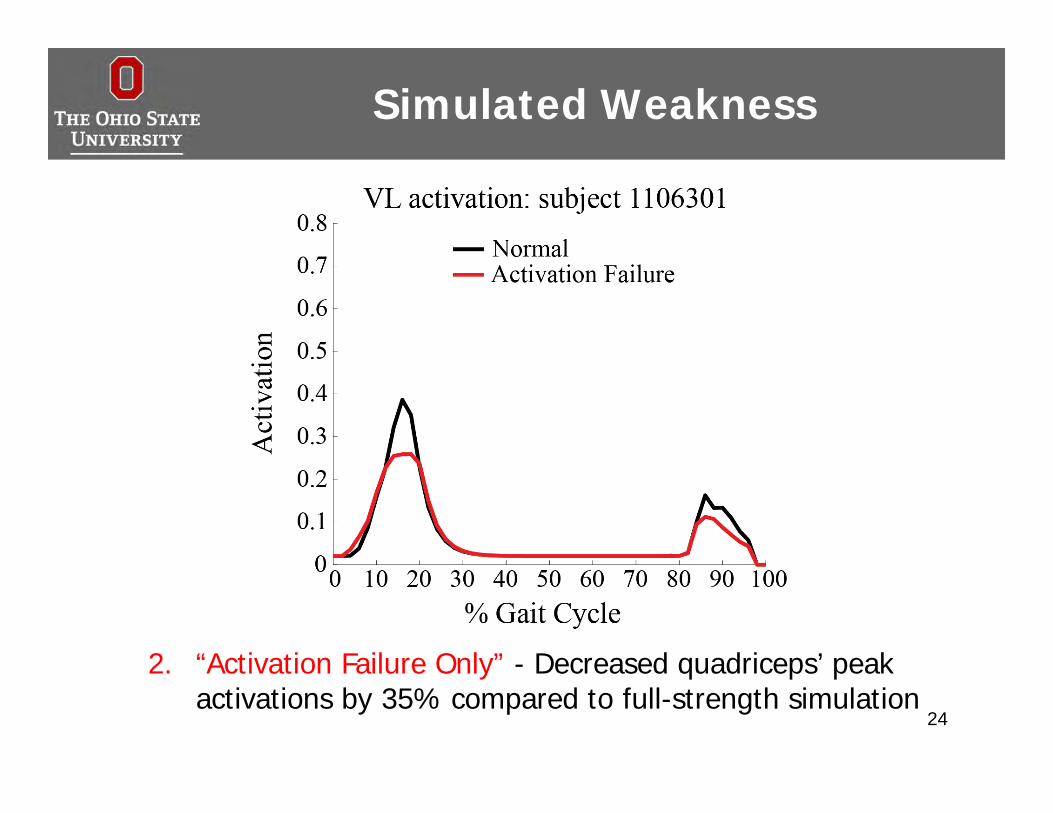
2. “Activation Failure Only” - Decreased quadriceps’ peak activations by 35% compared to full-strength simulation
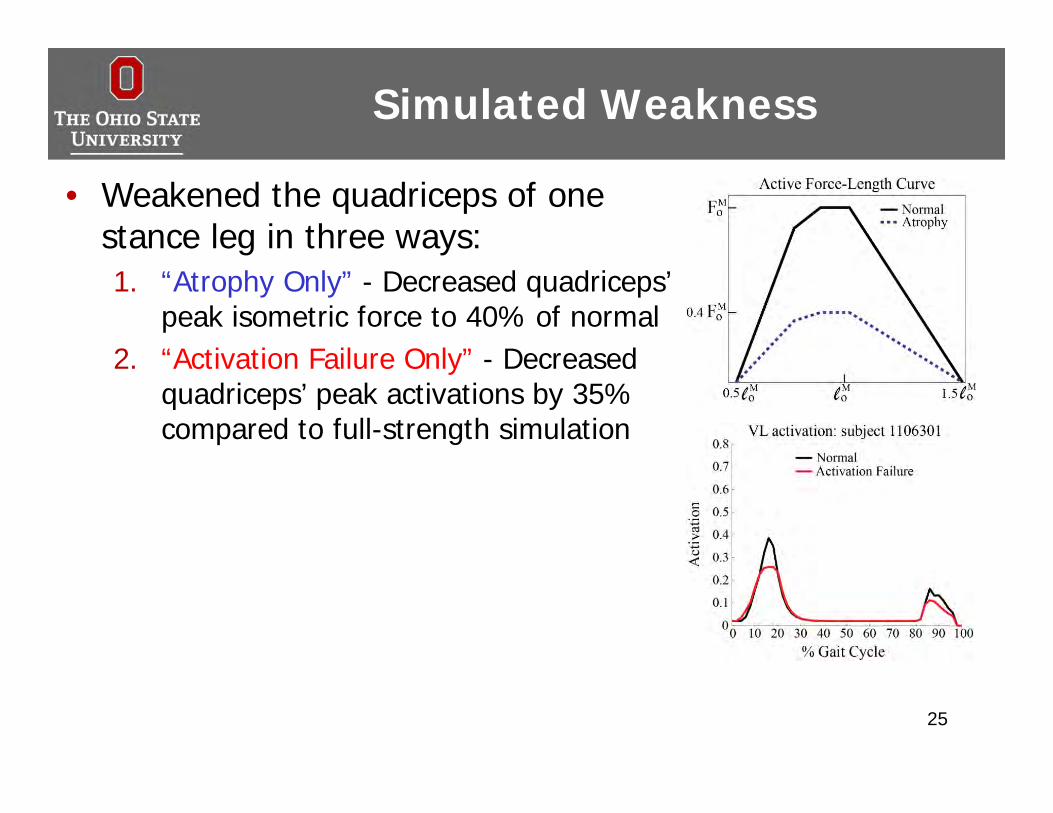
• Weakened the quadriceps of one stance leg in three ways:1. “Atrophy Only” - Decreased quadriceps’
peak isometric force to 40% of normal2. “Activation Failure Only” - Decreased
quadriceps’ peak activations by 35% compared to full-strength simulation
Simulated Weakness
25
• Weakened the quadriceps of one stance leg in three ways:1. “Atrophy Only” - Decreased quadriceps’
peak isometric force to 40% of normal2. “Activation Failure Only” - Decreased
quadriceps’ peak activations by 35% compared to full-strength simulation
3. “Atrophy + Activation Failure” -Combination of simulated atrophy and activation failure
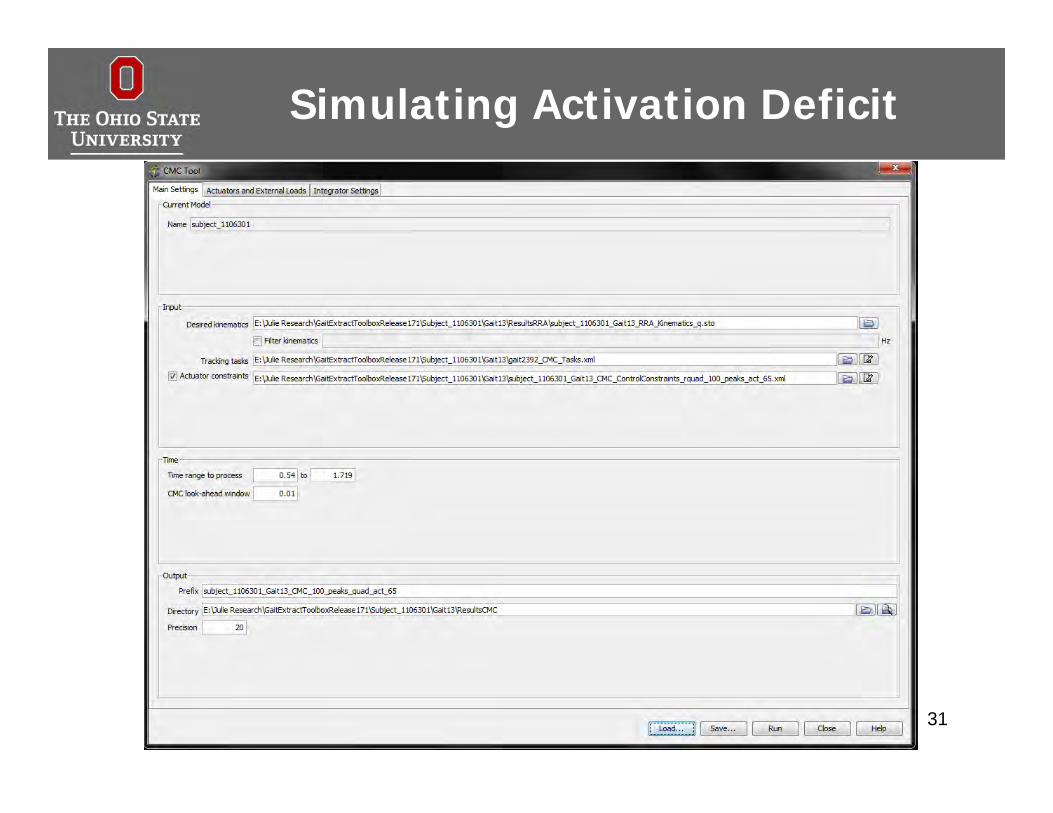
• Re-ran CMC and IAA for each weakened case• While tracking normal gait
Simulated Weakness
26• Re-calculated muscle forces and contributions
Simulating Atrophy
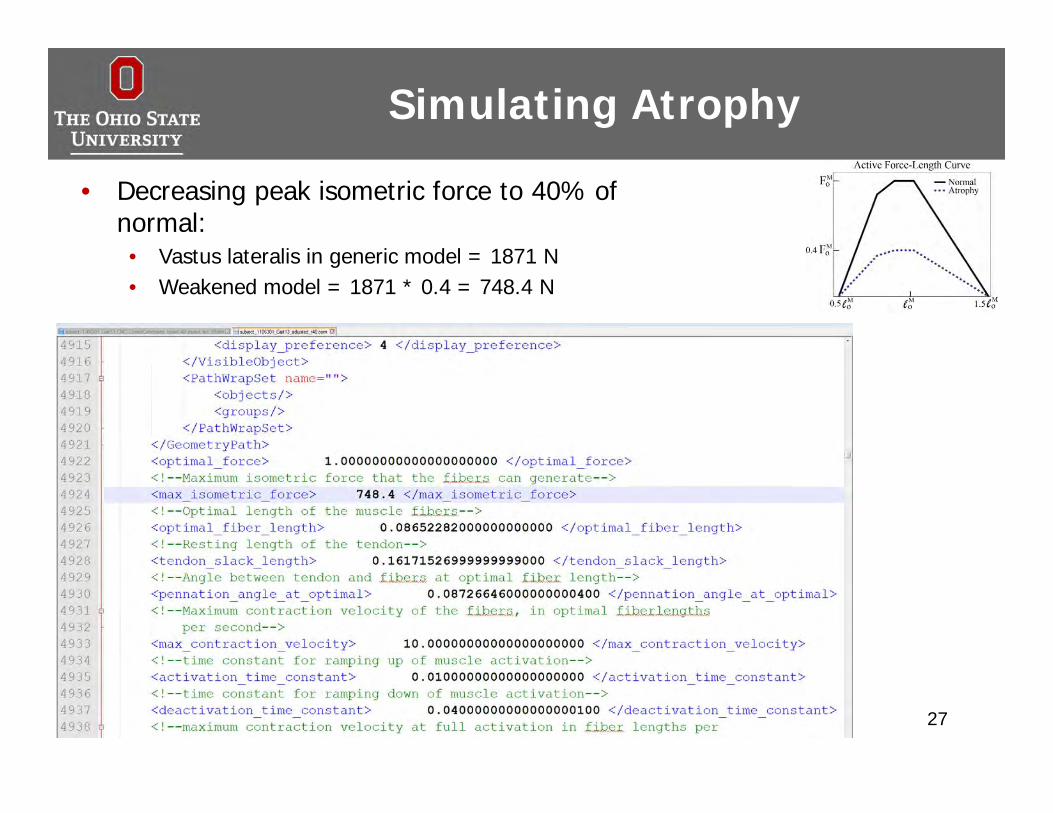
• Decreasing peak isometric force to 40% of normal:• Vastus lateralis in generic model = 1871 N• Weakened model = 1871 * 0.4 = 748.4 N
27
Simulating Atrophy
28
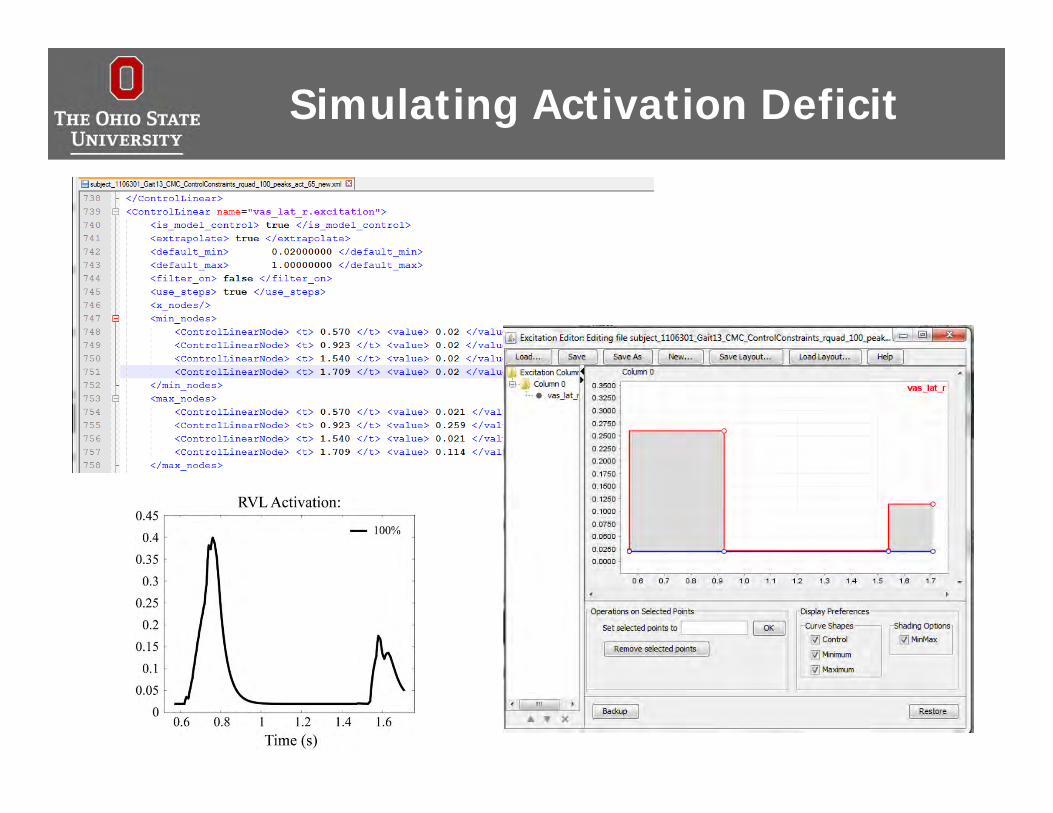
Simulating Activation Deficit
29
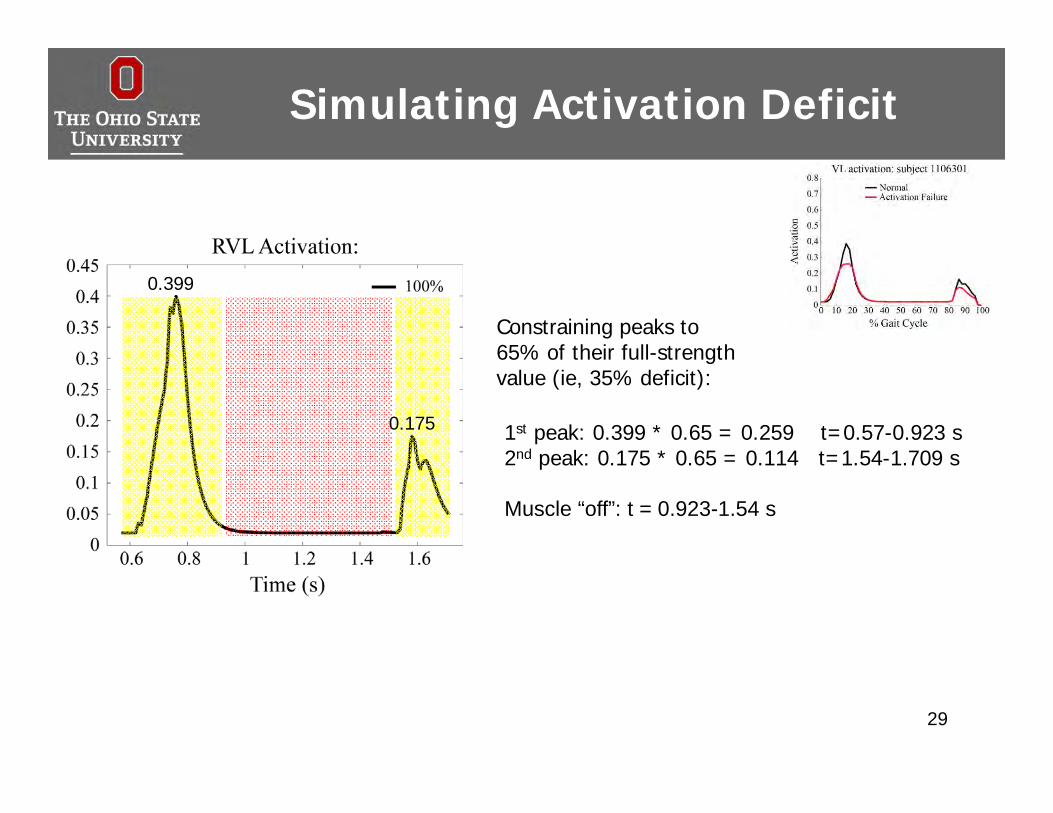
0.399
0.175 1st peak: 0.399 * 0.65 = 0.259 t=0.57-0.923 s2nd peak: 0.175 * 0.65 = 0.114 t=1.54-1.709 s
Muscle “off”: t = 0.923-1.54 s
Constraining peaks to 65% of their full-strength value (ie, 35% deficit):
Simulating Activation Deficit
30
Simulating Activation Deficit
31
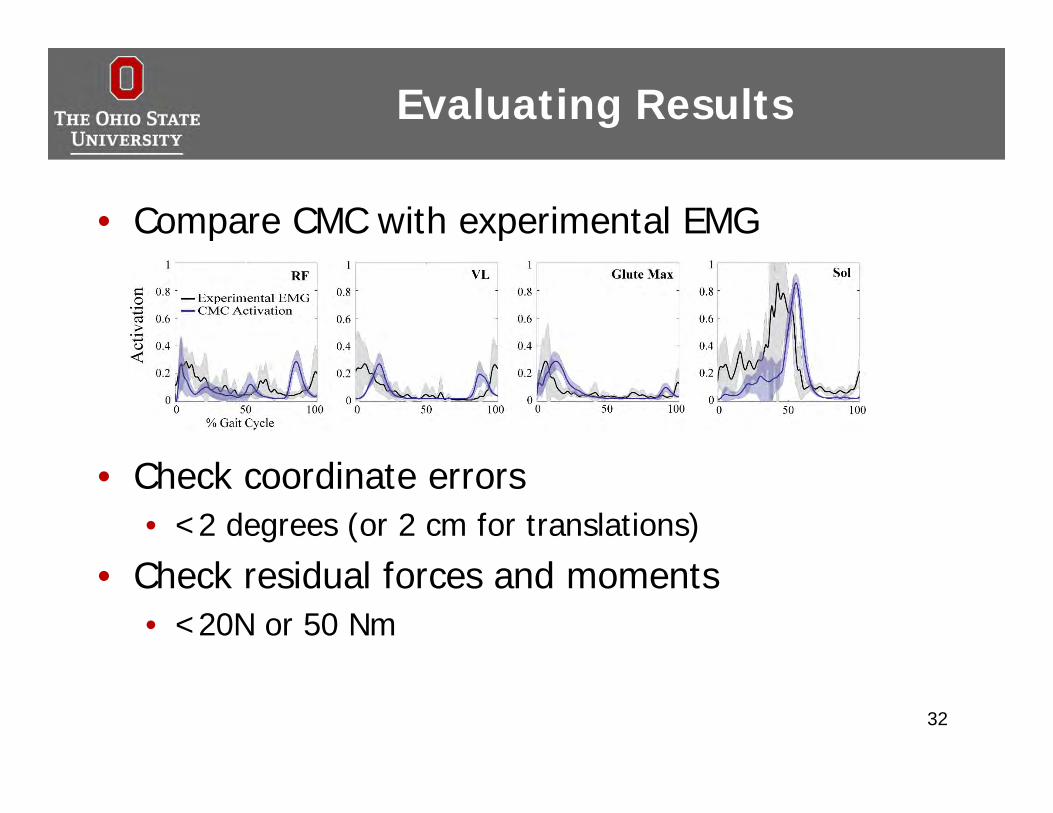
Evaluating Results
• Compare CMC with experimental EMG
32
• Check coordinate errors• <2 degrees (or 2 cm for translations)
• Check residual forces and moments• <20N or 50 Nm
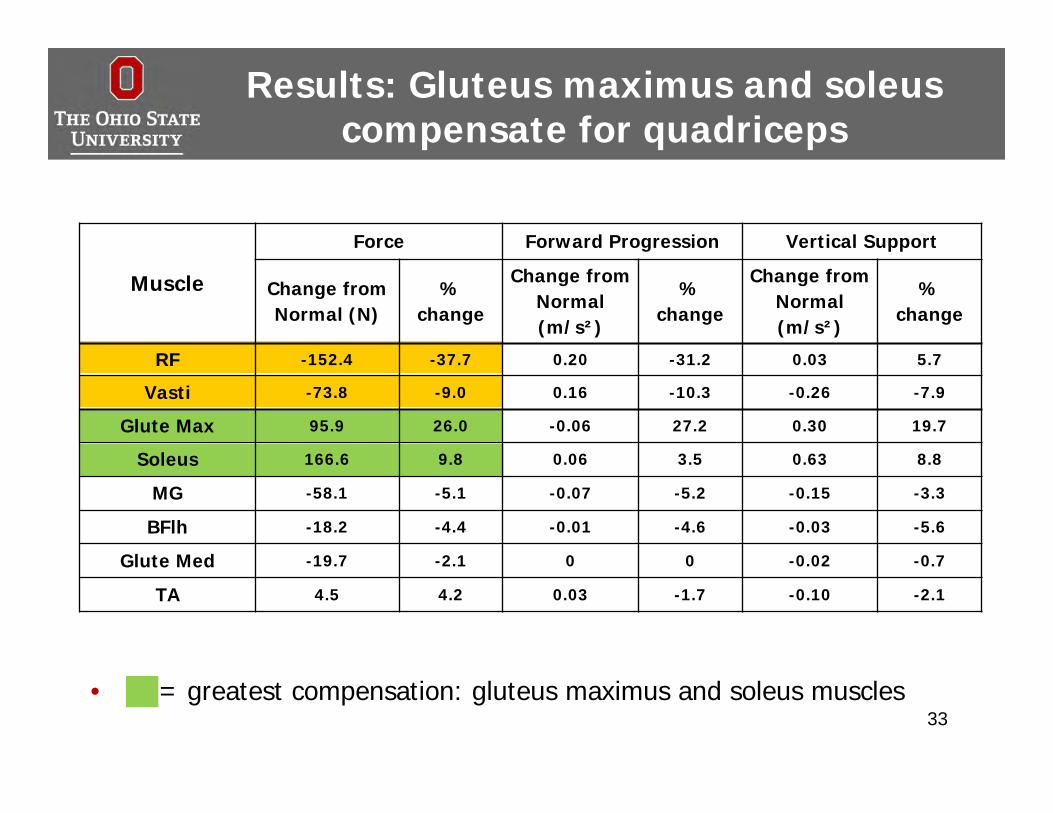
Results: Gluteus maximus and soleus compensate for quadriceps
33
Muscle
Force Forward Progression Vertical Support
Change from Normal (N)
% change
Change from Normal (m/s²)
% change
Change from Normal (m/s²)
% change
RF -152.4 -37.7 0.20 -31.2 0.03 5.7
Vasti -73.8 -9.0 0.16 -10.3 -0.26 -7.9
Glute Max 95.9 26.0 -0.06 27.2 0.30 19.7
Soleus 166.6 9.8 0.06 3.5 0.63 8.8
MG -58.1 -5.1 -0.07 -5.2 -0.15 -3.3
BFlh -18.2 -4.4 -0.01 -4.6 -0.03 -5.6
Glute Med -19.7 -2.1 0 0 -0.02 -0.7
TA 4.5 4.2 0.03 -1.7 -0.10 -2.1
• = greatest compensation: gluteus maximus and soleus muscles
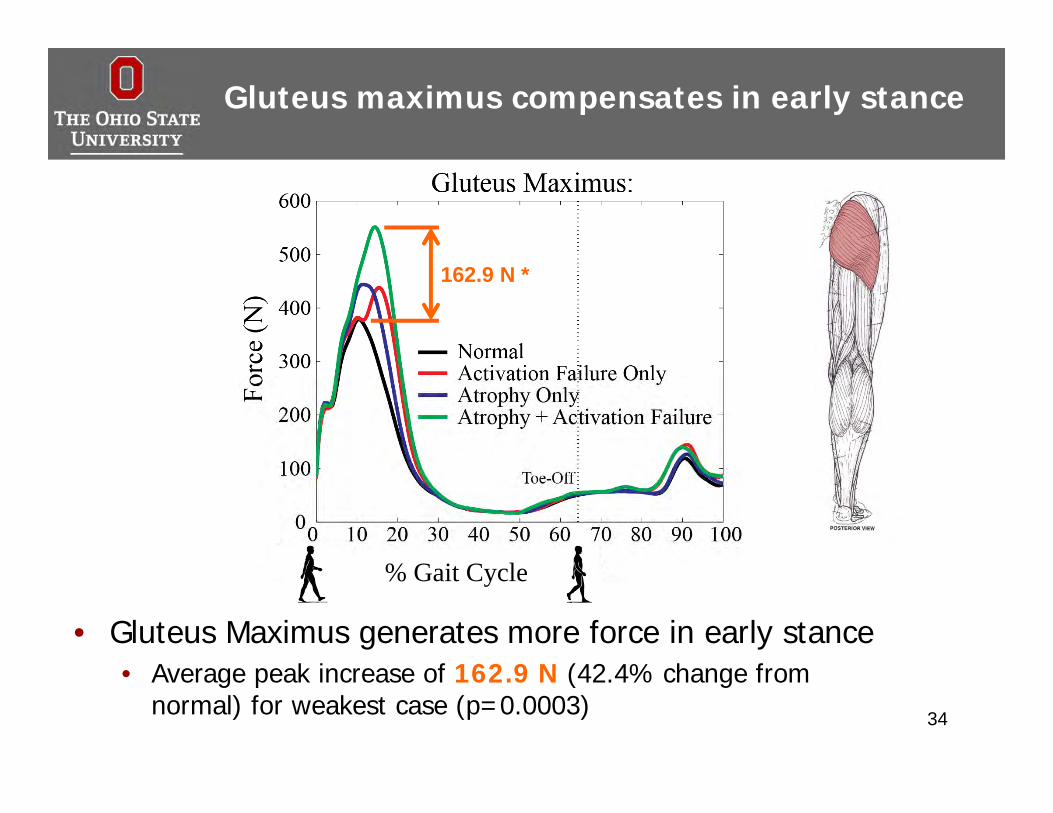
Gluteus maximus compensates in early stance
34
• Gluteus Maximus generates more force in early stance• Average peak increase of 162.9 N (42.4% change from
normal) for weakest case (p=0.0003)
162.9 N *
% Gait Cycle
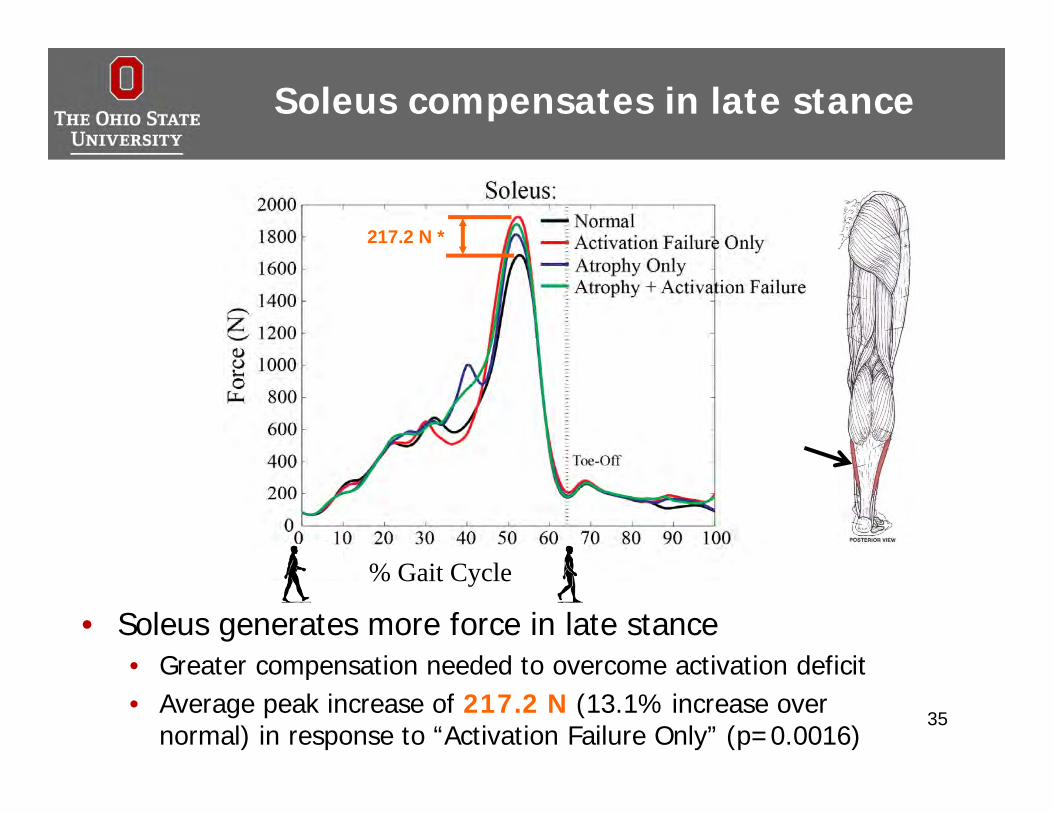
Soleus compensates in late stance
• Soleus generates more force in late stance• Greater compensation needed to overcome activation deficit• Average peak increase of 217.2 N (13.1% increase over
normal) in response to “Activation Failure Only” (p=0.0016)35
217.2 N *
% Gait Cycle
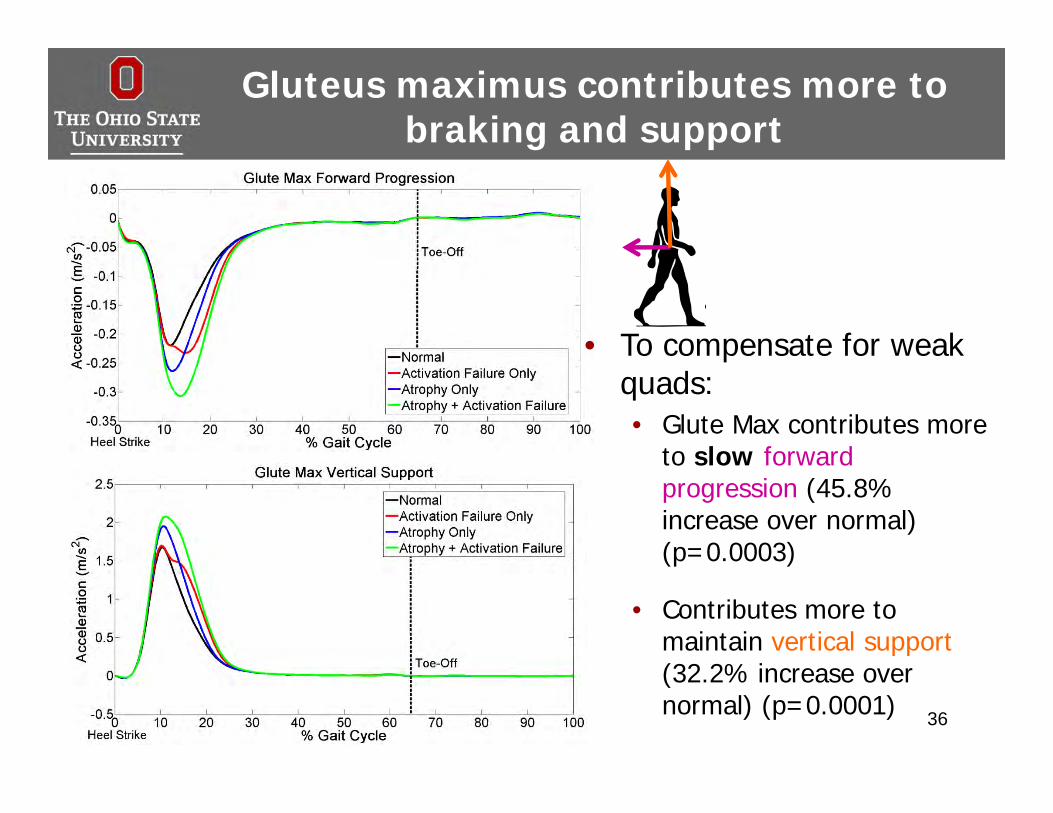
Gluteus maximus contributes more to braking and support
36
• To compensate for weak quads:• Glute Max contributes more
to slow forward progression (45.8% increase over normal) (p=0.0003)
• Contributes more to maintain vertical support (32.2% increase over normal) (p=0.0001)
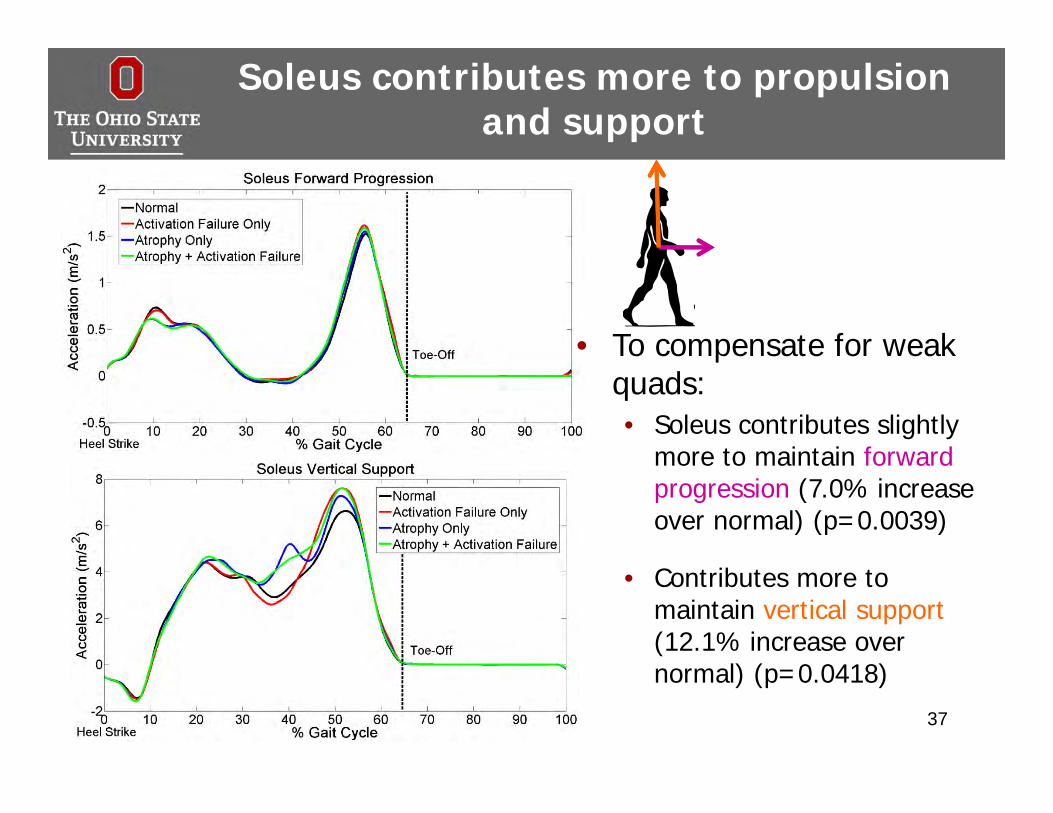
Soleus contributes more to propulsion and support
37
• To compensate for weak quads:• Soleus contributes slightly
more to maintain forward progression (7.0% increase over normal) (p=0.0039)
• Contributes more to maintain vertical support (12.1% increase over normal) (p=0.0418)
Discussion
• First study to develop muscle-driven simulations investigating the two sources of quadriceps weakness:• Atrophy • Activation failure
• To maintain normal gait pattern, gluteus maximusand soleus show greatest potential to compensate for weak quadriceps• Different responses to atrophy and activation failure
38
Discussion
• Limitations• Forced simulations to track healthy
gait• Activation deficit assumptions• Generic musculoskeletal model
• Future work in impaired populations (OA)• Patient-specific muscle properties• Evaluation of compensation
strategies through clinical interventions 39
Take-Home Message
• Gluteus maximus and soleus muscles may be potential targets for strength training during rehabilitation
• Understanding compensation strategies that are necessary to maintain normal gait provides a foundation to investigate role of muscle weakness in pathological gait
40
Paper reference
41
Thompson et al., Gluteus maximus and soleus compensate for simulated quadriceps atrophy and activation failure during walking, Journal of Biomechanics Sept; 46(13): 2165-72, 2013.
• Contact info: [email protected]
Acknowledgments
• Co-authors:• Robert Siston, PhD• Ajit Chaudhari, PhD• Laura Schmitt, PT, PhD• Thomas Best, MD, PhD
• OSU staff and students:• Mike McNally• Becky Lathrop• Jay Young• Molly Mollica• Michelle Cullen• Laura Henkel
• Funding sources: • NSF Graduate Research Fellowship • The Ohio State University Graduate
Fellowship program
• OpenSim team:• Scott Delp• Jen Hicks• Jeff Reinbolt• Kat Steele• Ajay Seth• Sam Hamner• Ayman Habib• Tim Dorn