Embed Size (px)
DESCRIPTION
Silver Cross EMS September 2012 3 rd Trimester CME. Allergies and Anaphylaxis Presented by Silver Cross staff. System Updates!. Please remember… Region VII does not give Lidocaine for EZ-IO pain, even though your sales rep may have told you otherwise. - PowerPoint PPT Presentation
Citation preview
Silver Cross EMS September 2012 3rd Trimester CME
Allergies and AnaphylaxisPresented by Silver Cross staff
System Updates!• Please remember… Region VII does not give Lidocaine for EZ-
IO pain, even though your sales rep may have told you otherwise.
• The Region VII SMO Code 12 “Suspected Cardiac Patient” has added pregnancy as a contraindication to Aspirin
• Region VII has also added a new SMO for Suspension Trauma, Code 21b.
• As of September 1st – license and renewal fees are in place.• Sign up for our e-mail list for even more information! • Info on all these and more on the website…
www.silvercrossems.com
Our agenda
• Physiology and discussion of allergic reaction process.
• Physiology and discussion of anaphyaxis.• Specific information on anaphylactic shock.• Treatment of allergies and anaphylaxis• Drug of the month – Epinephrine• Strip of the month – Ventricular rhythms
Allergies
• An allergy is an exaggerated immune response or reaction to substances that are generally not harmful.
Anaphylaxis
• Immediate, systemic, life-threatening allergic reaction - major changes in cardiovascular, respiratory, and cutaneous systems
Antigens
• Antigen - induces formation of antibodies• Enters body by injection, ingestion, inhalation, or
absorption• Examples of common antigens associated with
anaphylactic reactions:– Drugs (penicillin, aspirin)– Envenomation (wasp stings)– Foods (seafood, nuts)– Pollens
Antibodies
• Protective protein substances developed by body in response to antigens– Bind to the antigen that produced them– Neutralizes antigens and removes from the body
• Antigen-antibody reaction protects body from toxins by activating immune response
Immune Response
• Immune responses are normally protective• Can become oversensitive or be directed toward
harmless antigens to which we are often exposed– When this occurs, the response is termed “allergic”– Antigen causing allergic response called an “allergen”
• Common allergens include drugs, insects, foods, and animals
Immune Response
• Healthy body responds to antigen challenge through collective defense system – immunity. – Natural, present at birth– Acquired, resulting from exposure to a specific
antigenic agent or pathogen– Artificially induced (immunization)
• Immunity may be active or passive
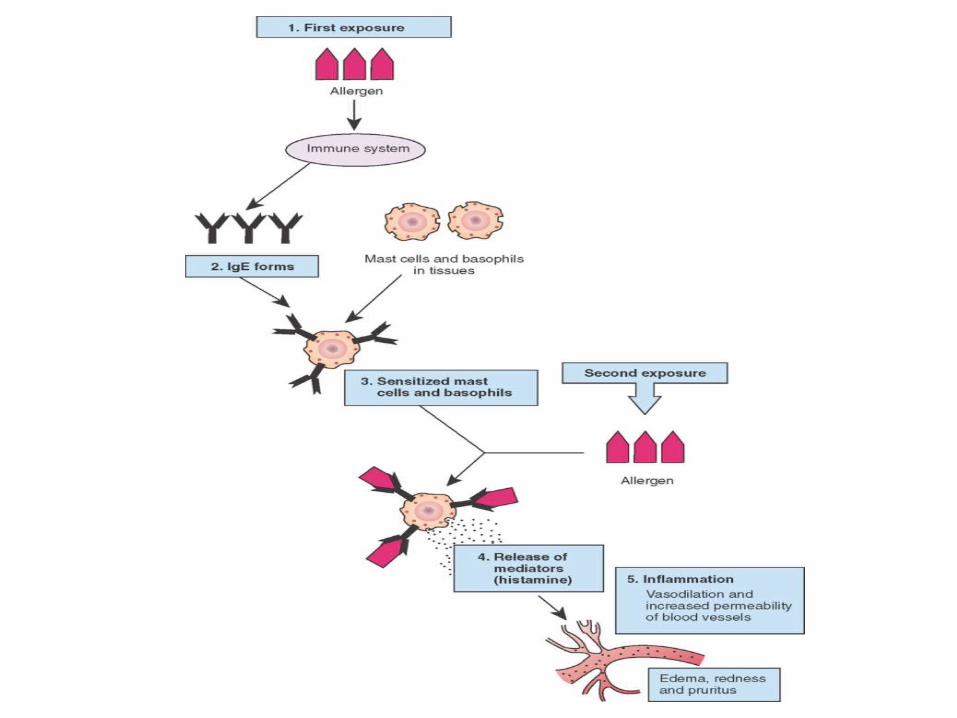
Allergic Reaction
• Increased physiological response to antigen after previous exposure (sensitization) to same antigen– When circulating antibody combines with specific
foreign antigen, results in hypersensitivity reactions
– Or to antibodies bound to mast cells or basophils (IgE)
Hypersensitivity Reactions
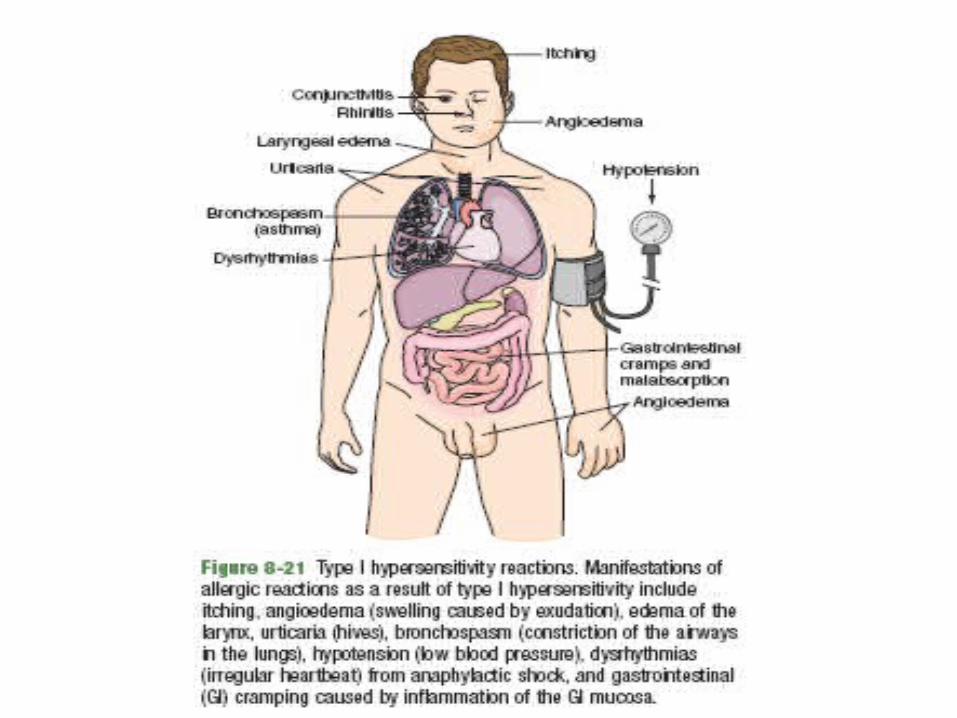
• Divided into four distinct types – Type I (IgE-mediated allergic reactions)– Type II (tissue-specific reactions)– Type III (immune-complex-mediated reactions)– Type IV (cell-mediated – localized allergic reactions)
• Agents that may cause hypersensitivity reactions (including anaphylaxis)– Drugs and biological agents– Insect bites and stings– Foods
Hypersensitivity Reactions
Localized Allergic Reaction
• Localized allergic reactions (type IV) do not manifest multi-system involvement
• Common signs and symptoms of localized allergic reaction include:– Conjunctivitis– Rhinitis– Angioedema– Urticaria– Contact dermatitis
Histamines• Promote vascular permeability
• Allows plasma to leak into interstitial space• Cause dilation of capillaries and venules
• Profound vasodilation further decreases cardiac preload, compromising stroke volume/cardiac output
• Cause contraction of nonvascular smooth muscle in GI tract and bronchial tree
– Associated increase in gastric, nasal, and lacrimal secretions, resulting in tearing and rhinorrhea
Histamines
• These physiological effects lead to:– Cutaneous flushing– Urticaria– Angioedema– Hypotension
• Onset very rapid– But short lived, quickly broken down by plasma
enzymes
Other Chemical Mediators• Other chemical mediators (heparin, neutrophil
chemotactic factor, and kinins) cause:– Fever– Chills– Bronchospasm– Pulmonary vasoconstriction
• These chemical processes can rapidly lead to:– Upper airway obstruction and bronchospasm– Dysrhythmias and cardiac ischemia– Circulatory collapse and shock
Don’t be shocked….
But this discussion has a lot to do with shock!
Anaphylactic Shock
• The body needs oxygen carried by blood for cellular metabolism– Perfusion
• Delivery of O2, other nutrients to cells
• Shock– Inadequate tissue perfusion causes too little
oxygen to cells
All Kinds of Shock are caused by one of three things…
• Causes: pump failure (heart)container failure (vessels)fluid failure (volume)
– Failure of heart = inadequate cardiac output– Failure of blood vessels = significant changes in
systemic vascular resistance– Inadequate blood volume = inadequate delivery of
oxygen to cells
Imagine a power steering pump
• Your car’s power steering needs a functioning pump, intact lines and enough fluid to work.– Failure of any one will cause power steering to
fail.
• Our bodies work the same way… Failure of our heart (pump), our vessels (lines) or
our blood flow (fluids) will cause the body to fail
Distributive shock – a vessel failure
• Anaphylaxis is a form of distributive shock.– Vessels dilate so much, blood stagnates in them
and can never fill them up properly.– Also called “container” failure
• It's like replacing the power steering lines in your car with lines that are twice as big.– They would need more fluid to fill them.– If not enough fluid, it will not flow properly.
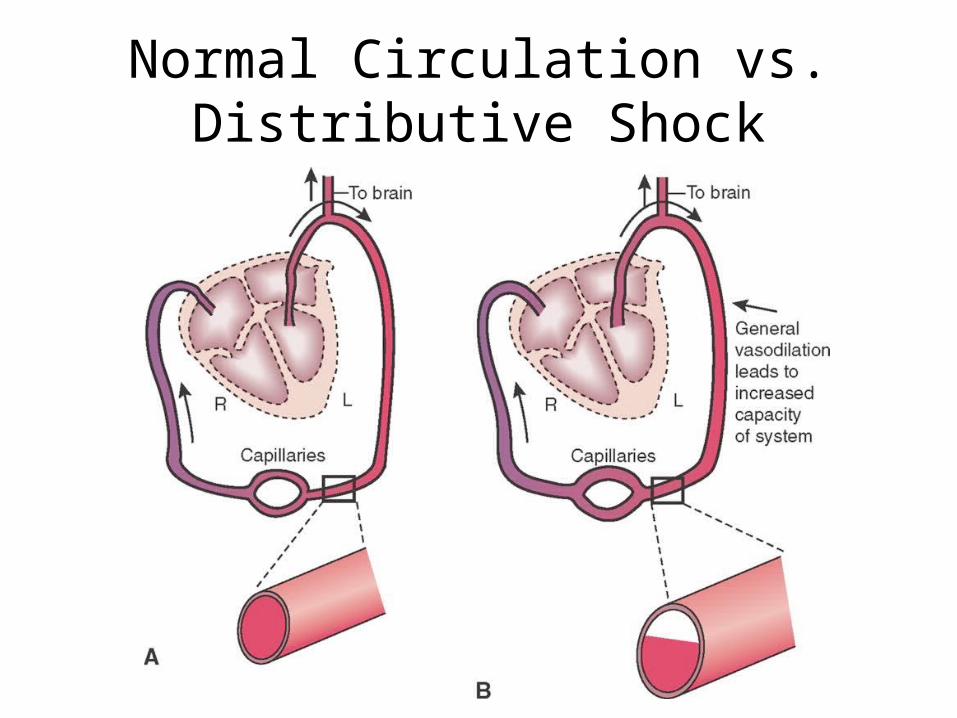
Normal Circulation vs. Distributive Shock
Anaphylactic shock/anaphylaxis– Etiology/causes
• Dust, pollen, mold, animal dander• Foods: milk, eggs, nuts, shellfish, beans• Latex/rubber products• Blood components• Antibiotics• Insect venom (hymenoptera)• Local anesthetics• Vitamins• NSAIDS (ASA, ibuprophen), IV contrast dyes • Radiocontrast media• Aspirin
Early (compensated) shock
• Early (compensated) shock– Physical exam
• Assess heart rate – probably elevated• Assess presence & volume of peripheral pulses• Assess blood pressure – may still be normal
– Reversible if cause identified, corrected– Uncorrected progresses to next stage
Late (decompensated) shock
– Compensatory mechanisms fail– Epinephrine & norepinephrine – vasoconstriction– Precapillary sphincters dilate
• blood rushes into capillary beds
– Postcapillary sphincters constricted • causing stagnation of blood
– Blood pressure falls– Altered mental status– Anaerobic metabolism occurs (acidosis)
Anaphylactic shock/anaphylaxis
– Findings• Angioedema• Inability to speak, tightness in throat, stridor, DIB,
wheezing, hoarseness, cough• Retractions, accessory muscle use, ↓ breath sounds• Tachycardia, ↓ BP• Diaphoresis, urticaria/flushing, pruritis, pallor/cyanosis• N/V/D, abdominal pain/cramps, incontinence• AMS, anxiety, restlessness, feeling of impending doom
Anaphylactic shock/anaphylaxis
– Skin• Diaphoresis• Urticaria• Flushing • Pruitis• Angioedema• Pallor• Cyanosis

Urticaria as a result of an allergic reaction.
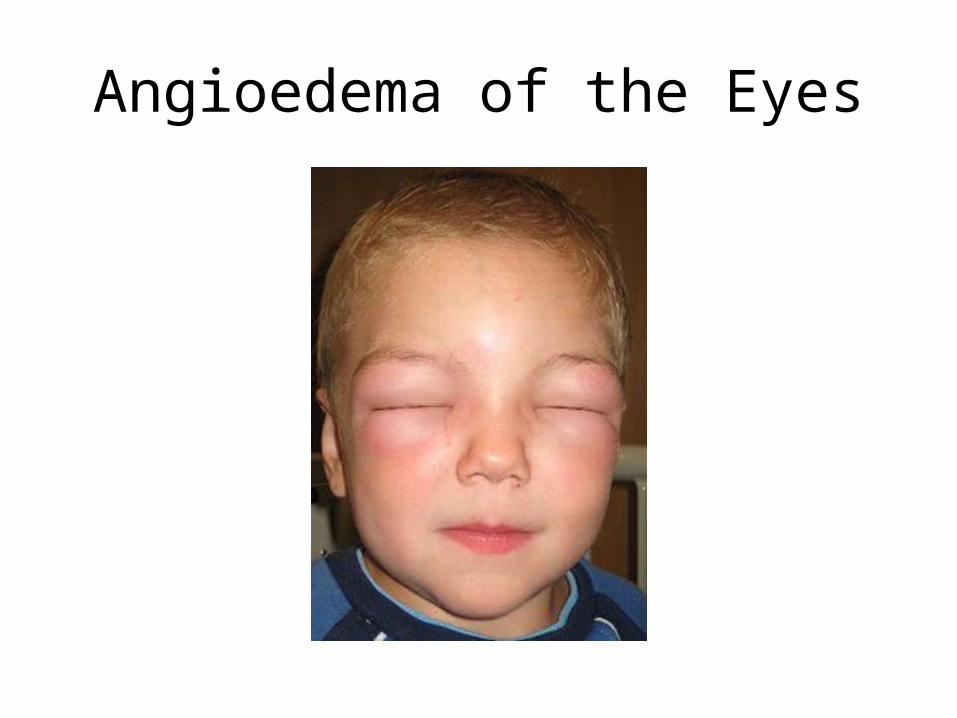
Angioedema of the Eyes

Bee Sting and Angioedema of the LipsBee Sting and Angioedema
Anaphylactic shock/anaphylaxis
– Respiratory findings• FBAO• Pulmonary embolism• Reactive airway disease• Tension pneumothorax• Panic attack• Vasovagal syncope
Anaphylactic shock/anaphylaxis
– Gastrointestinal & genitourinary findings• Nausea, vomiting and diarrhea• Abdominal pain• Cramping• Incontinence
Initial Assessment• Airway and breathing
– Airway assessment critical• Most deaths from anaphylaxis
from upper airway obstruction
– Evaluate for voice changes, stridor, barking cough
– Tightness in neck, dyspnea suggest airway obstruction
– Airway of unconscious patient should be evaluated, secured
– If airflow impeded, perform endotracheal intubation.
– If severe laryngeal/epiglottic edema, needle cricothyrotomy indicated
– Monitor patient closely for signs of respiratory distress
• Circulation– Assess pulse quality, rate, and
location frequently
History
• May be difficult to obtain but critical to rule out other medical emergencies– Question patient regarding the chief complaint
and the rapidity of onset of symptoms• Signs and symptoms of anaphylaxis usually appear
within 1 to 30 minutes of introduction of the antigen
Significant Past Medical History
• Previous exposure and response to the suspected antigen– Not always reliable
• Method of introduction of the antigen• Chronic or current illness and medication use
– Preexisting cardiac disease or bronchial asthma– Prescribed Epi-Pen
Physical Examination
• Assess and frequently reassess vital signs• Inspect face and neck for angioedema, hives,
tearing, and rhinorrhea.– Note presence of erythema or urticaria on other
body regions• Assess lung sounds frequently to evaluate
effectiveness of interventions• Monitor ECG
EMS Drug TherapyEpinephrineFluid resuscitation for hypovolemia• Antihistamines to antagonize the effects of histamine
Benadryl (diphenhydramine)50mg IVP slowly over 2-3 minutes50mg IM if no IV
• Beta agonists to improve alveolar ventilationAlbuterol nebulizer
• Corticosteroids to prevent a delayed reactionSolu-medrol (methylprednisolone)
125mg IVPNo longer just for long transports
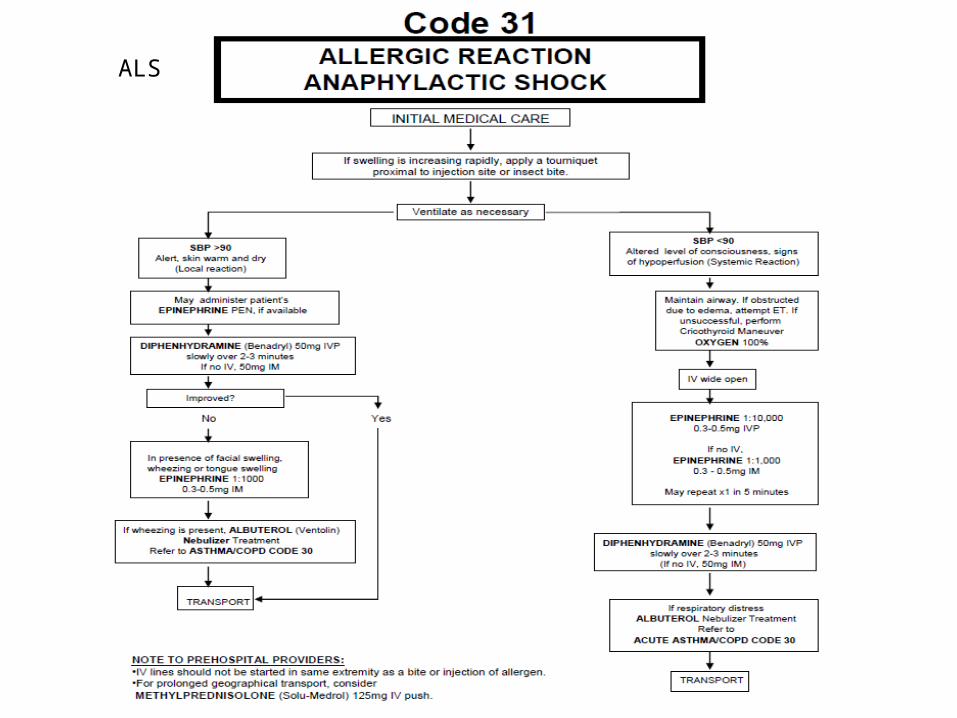
ALS
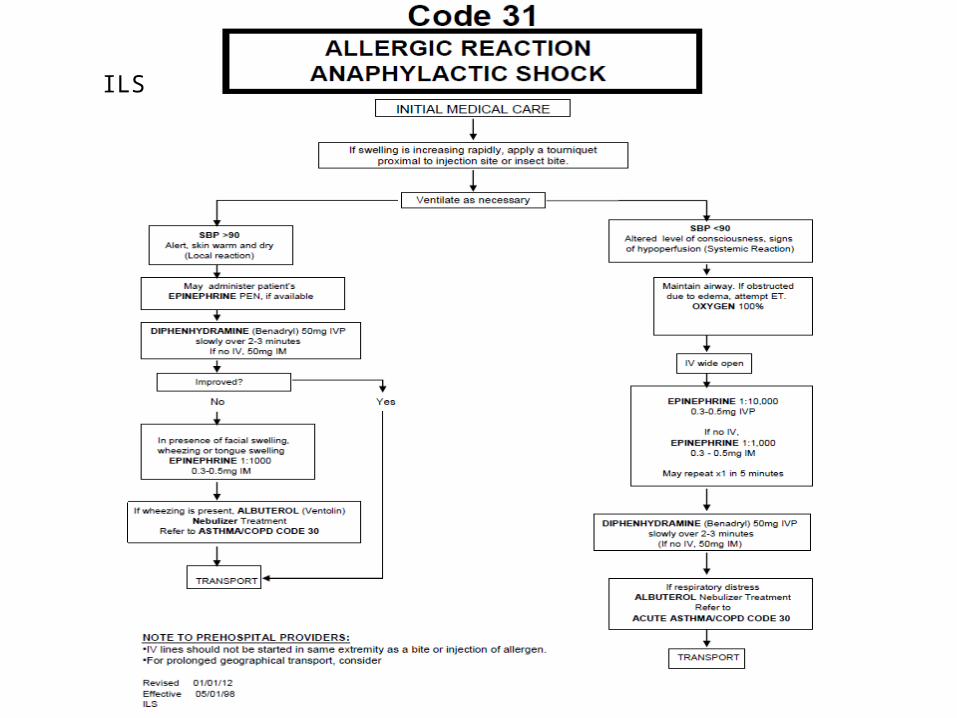
ILS
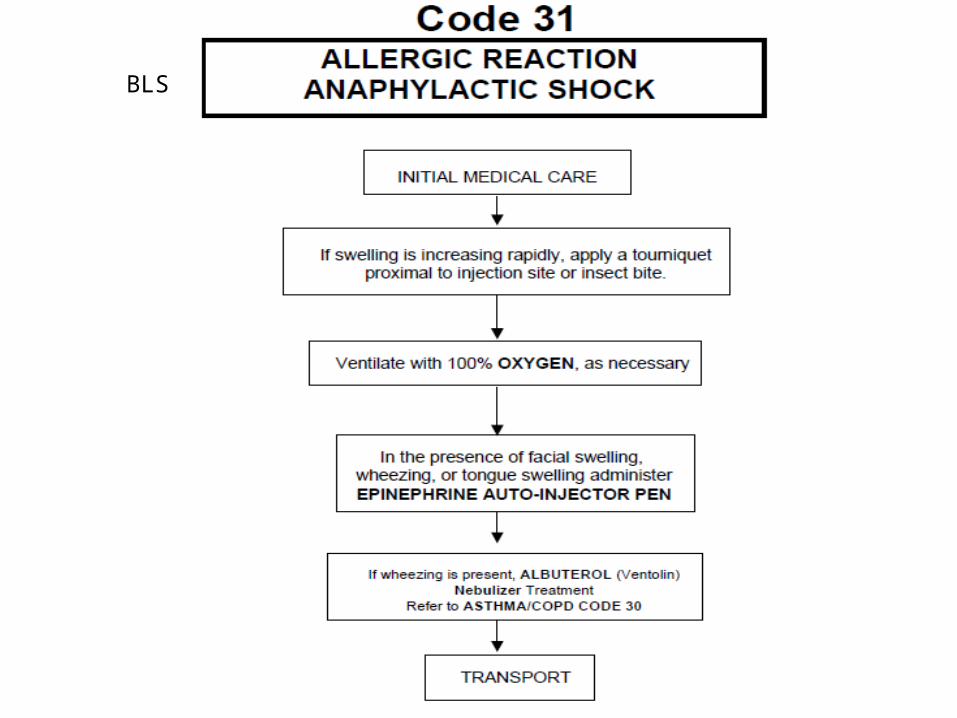
BLS
Prevention and Patient Education
• Clearly document allergic reactions• Always ascertain history of allergies before
administering any medication• Medications that are highly allergenic should
be given orally rather than parenterally– When parenteral medication is given, the patient
should be observed for 20 to 30 minutes
Prevention and Patient Education
• Patients with known allergies should:– Receive information regarding medical
identification tags, bracelets, or cards– Contact their physician for Epi-pen prescription for
epinephrine if they have a history of anaphylaxis.
Drug O’ the Month - Epinephrine
Sympathetic agonist
Epinephrine is a naturally occurring catecholamine. It is a potent α- and β-adrenergic stimulant; however, its effect on β-receptors is more profound.
Mechanism of Action
Epinephrine acts directly on α- and β-adrenergic receptors. Its effect on β-receptors is much more profound, and includes the following:Increased heart rate (Beta)Increased cardiac contractile force (Beta)Increased electrical activity in the myocardium (Beta)Increased systemic vascular resistance (Alpha)Increased blood pressure (Beta)Increased automaticity (Beta)
Pharmacokinetics
Onset< 2 minutes (IV/ET)
Peak effects< 5 minutes (IV/ET)
Duration5-10 minutes (IV/ET)
Half-life5 minutes
Indications
Cardiac arrest AsystoleVentricular fibrillationPulseless ventricular tachycardiaPEA (pulseless electrical activity)
Severe anaphylaxisSevere reactive airway disease
Precautions
Should be protected from lightCan be deactivated by alkaline solutions such as
sodium bicarbonateThe IV line must be adequately flushed between
administrations of epinephrine and sodium bicarbonate.
Side Effects
PalpitationsAnxietyTremulousnessHeadacheDizzinessNauseaVomitingIncreased myocardial oxygen demand
Interactions
The effects of epinephrine can be intensified in patients who are taking antidepressants.
Dosage
Cardiac arrest (adult) 1 mg of 1:10,000 IV/IO every 3-5 minutes
Cardiac arrest/bradycardia (pediatrics)0.01 mg/kg of 1:10,000 IV (0.1 ml/kg) every 3-5
minutes.
Dosage (cont.)
Severe anaphylaxis (adult) 1:10,000 0.3 – 0.5 mg IV/IO1:1,000 0.3 – 0.5 mg IM (if no IV/IO)
Severe anaphylaxis (pediatrics)0.01 mg/kg of 1:1,000 IMRepeat every 5-15 minutes
Dosage (cont.)
Severe asthma/COPD (adult) 1:1,000 0.01 mg/kg up to 0.3 mg IM (with medical
control approval)

Epi-pen autoinjector
Strip O’ the Month – Ventricular Rhythms
The Ventricles
Ventricles are the heart’s least efficient pacemakerNormally generate impulses at a rate of 20 to 40 beats/min
May assume responsibility for pacing the heart if:The SA node fails to discharge
An impulse from the SA node is generated but blocked as it exits the SA node
The rate of discharge of SA node is slower than that of ventricles
An irritable site in either ventricle produces an early beat or rapid rhythm
Premature Ventricular Complexes (PVCs)
Arise from an irritable focus within either ventricle
A PVC:Is premature, occurring earlier than the next expected sinus beat
QRS is typically equal to or greater than 0.12 seconds
PVC depolarizes ventricles prematurely and in an abnormal manner
T wave is usually in the opposite direction of the QRS complex
PVCs – Patterns
Pairs (couplets): two sequential PVCs
Runs or bursts: three or more sequential PVCs are called “ventricular tachycardia” (VT)
Bigeminal PVCs (ventricular bigeminy): every other beat is a PVC
Trigeminal PVCs (ventricular trigeminy): every third beat is a PVC
Quadrigeminal PVCs (ventricular quadrigeminy): every fourth beat is a PVC
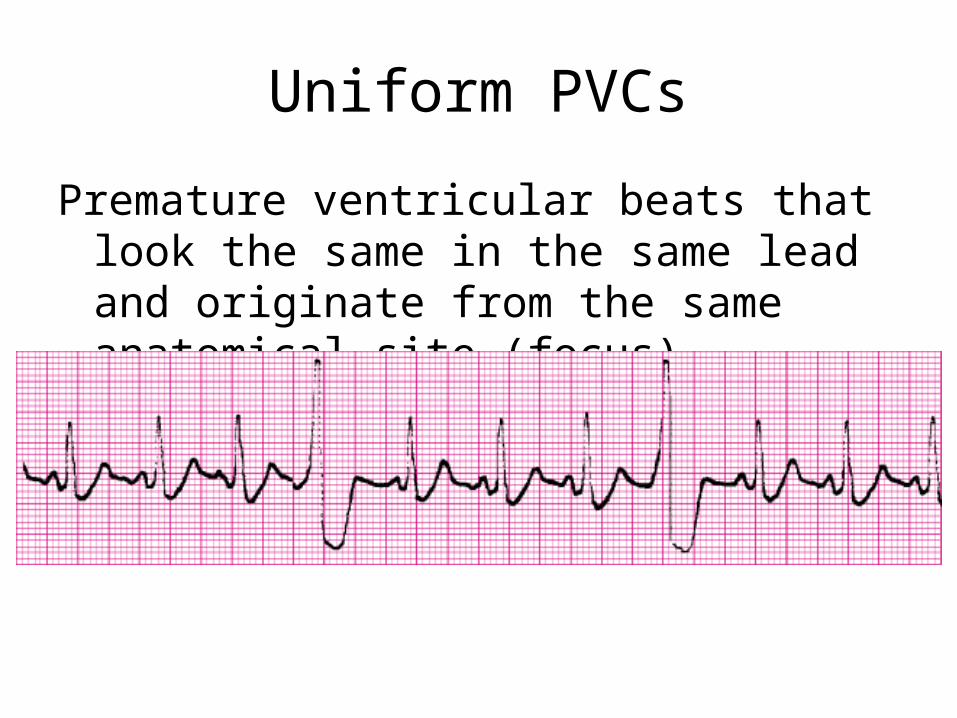
Uniform PVCs
Premature ventricular beats that look the same in the same lead and originate from the same anatomical site (focus)
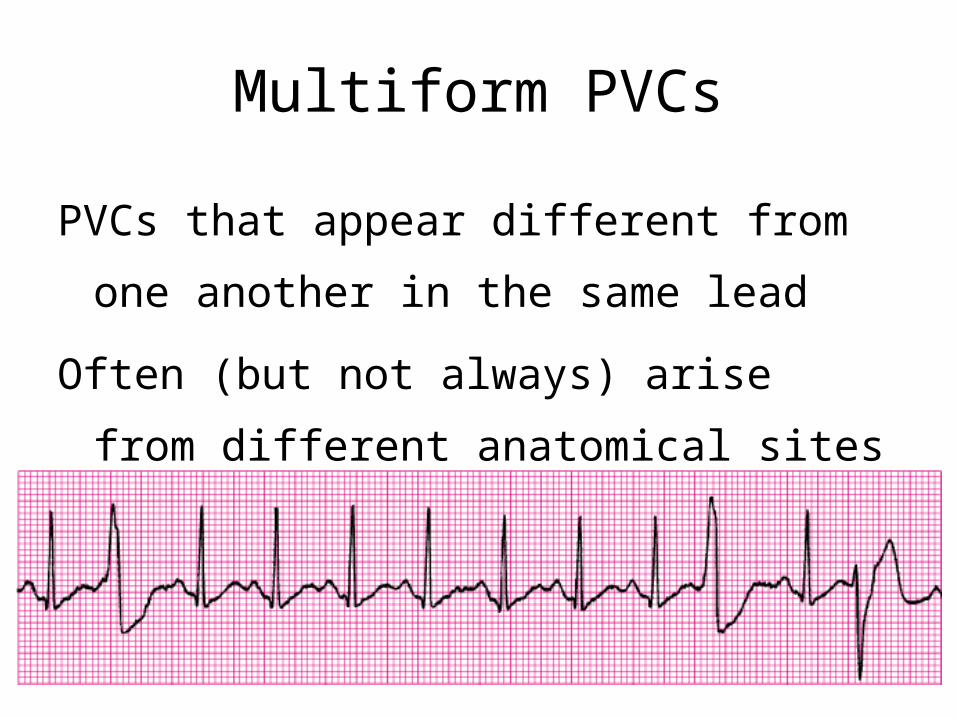
Multiform PVCs
PVCs that appear different from one another in
the same lead
Often (but not always) arise from different
anatomical sites
PVCs – CausesNormal variant
Hypoxia
Stress, anxiety
Exercise
Digitalis toxicity
Acid-base imbalance
Myocardial ischemia
Electrolyte imbalanceHypokalemia
Hypocalcemia
Hypercalcemia
Hypomagnesemia
Congestive heart failure
Increased sympathetic tone
Acute myocardial infarction
StimulantsAlcohol
Caffeine
Tobacco
MedicationsSympathomimetics
Cyclic antidepressants
Phenothiazines
PVCs – Clinical Significance
PVCs may or may not produce palpable pulses
Patients may be asymptomatic or complain of:Palpitations
“Racing heart”
Skipped beats
Chest or neck discomfort
If the PVCs are frequent, signs of decreased cardiac output may be present
PVCs – Intervention
Treatment of PVCs is dependent on the:Cause
Patient’s signs and symptoms
Clinical situation
Most patients experiencing PVCs do not require treatment with antidysrhythmic medications
Idioventricular Rhythm (IVR)
A ventricular escape or “idioventricular” rhythm (IVR) is three or more sequential ventricular escape beats occurring at a rate of 20 to 40 beats/min
Idioventricular Rhythm – Causes
Myocardial infarction
Digitalis toxicity
Metabolic imbalances
Idioventricular Rhythm – Clinical Significance
Possible signs and symptoms due to the slow
ventricular rate:Severe hypotension
Weakness
Disorientation
Lightheadedness
Loss of consciousness
Idioventricular Rhythm – Intervention
Avoid lidocaine!May abolish ventricular activity, possibly causing asystole
If the patient is symptomatic because of the slow rate and/or loss of atrial kick:Atropine may be ordered
Transcutaneous pacing (TCP) may be attempted
Ventricular Tachycardia (VT)
VT exists when three or more PVCs occur in immediate succession at a rate higher than 100 beats/minNon-sustained VT
A short run lasting less than 30 seconds
Sustained VT
Persists for more than 30 seconds
VT may occur with or without pulses
Patient may be stable or unstable
Ventricular Tachycardia (VT)
VT may originate from an ectopic focus in either
ventricleThe QRS complex is wide and bizarre
P waves, if visible, bear no relationship to QRS complex
The ventricular rhythm is usually regular but may be slightly irregular
Ventricular Tachycardia (VT)
Monomorphic VTQRS complexes are of the same shape and amplitude
Polymorphic VTQRS complexes vary in shape and amplitude
Ventricular Tachycardia – Causes
Sustained monomorphic VT is often associated with underlying heart disease, particularly myocardial ischemiaRarely occurs in patients without underlying structural heart disease
Ventricular Tachycardia – Other Causes
Cardiomyopathy
Cyclic antidepressant overdose
Digitalis toxicity
Valvular heart disease
Mitral valve prolapse
Trauma
Myocardial contusion
Invasive cardiac procedures
Acid-base imbalance
Electrolyte imbalanceHypokalemia
Hyperkalemia
Hypomagnesemia
Increased production of catecholamines
Fright
Cocaine abuse
Ventricular Tachycardia – Clinical Significance
Signs and symptoms vary
Syncope may occur because of an abrupt onset of VTThe patient’s only warning symptom may be a brief period of
lightheadedness
Ventricular Tachycardia – Clinical Significance
Signs and symptoms of hemodynamic compromise related to the tachycardia may include:
Shock
Chest pain
Hypotension
Shortness of breath
Pulmonary congestion
Congestive heart failure
Acute myocardial infarction
Decreased level of consciousness
Ventricular Tachycardia – Intervention
Treatment is based on the patient’s presentation
Stable but symptomatic patients are treated with:Oxygen therapy
IV access
Administration of ventricular antidysrhythmic to suppress the rhythm
Ventricular Tachycardia – Intervention
Unstable patient with a pulseUsually a sustained heart rate of 150 beats/min or more
If signs and symptoms are a result of rapid rate:Administer oxygen
IV access
Sedate (if awake and time permits)
Electrical therapy
If the patient is pulseless:Begin CPR until a defibrillator is available
Ventricular Tachycardia – Intervention
When unclear whether a regular, wide-QRS tachycardia is VT or SVT, treat the rhythm as VT until proven otherwise.
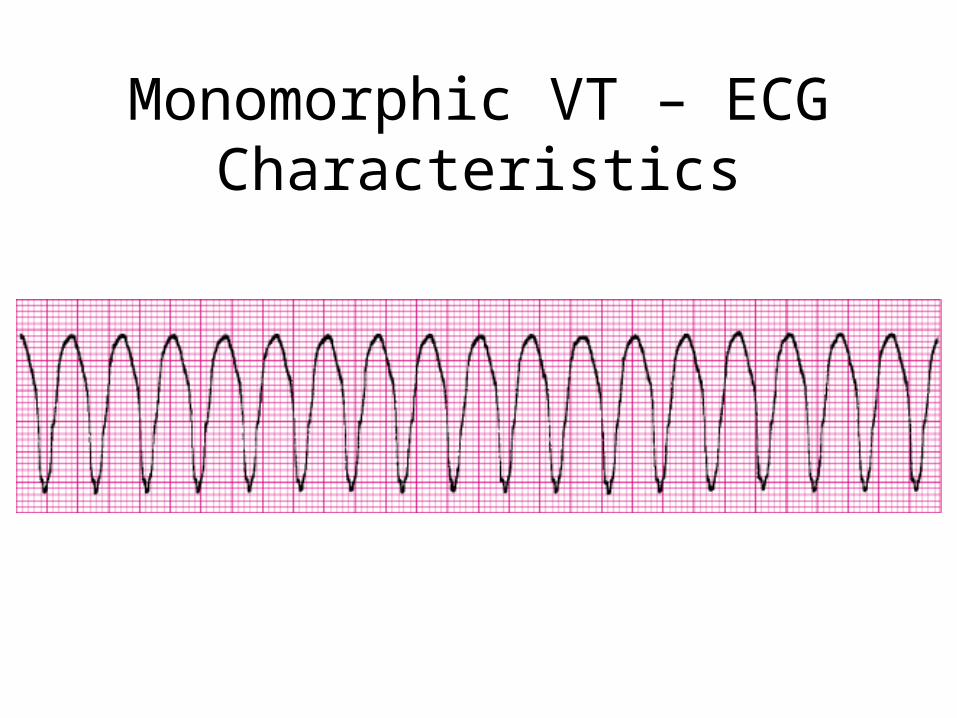
Monomorphic VT – ECG Characteristics
Torsade de Pointes (TdP)
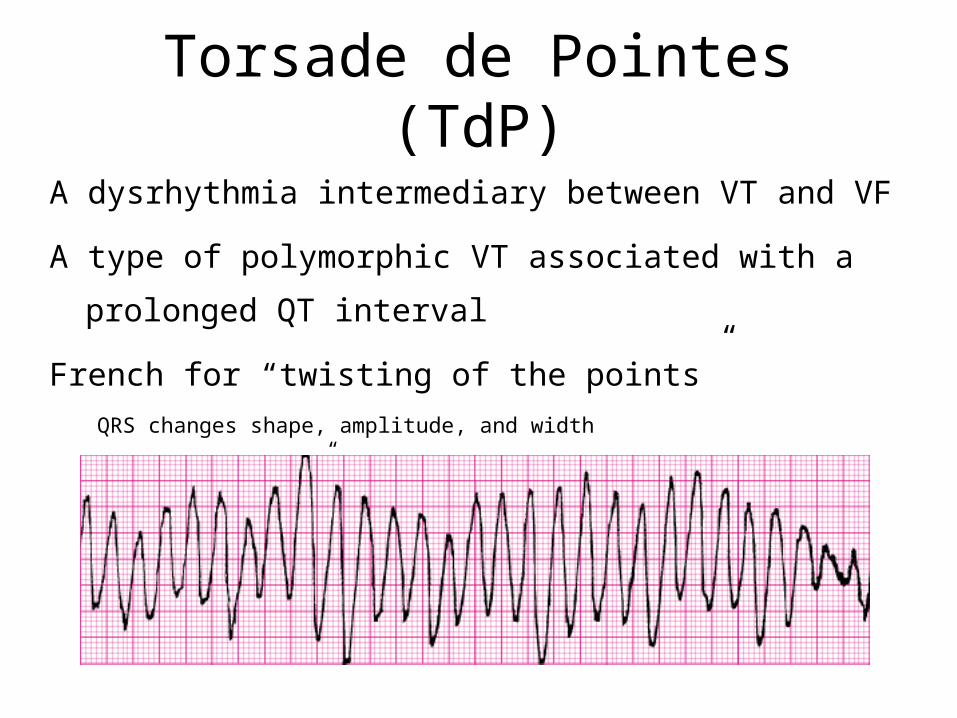
A dysrhythmia intermediary between VT and VF
A type of polymorphic VT associated with a prolonged QT interval
French for “twisting of the points”QRS changes shape, amplitude, and width
Appears to “twist” around the isoelectric line, resembling a spindle
Ventricular Fibrillation (VF)
VF is a chaotic rhythm that originates in the ventricles
No organized depolarization of the ventriclesVentricular myocardium quivers
No effective myocardial contraction and no pulse
Resulting rhythm is irregularly irregular with chaotic deflections that vary in shape and amplitude
No normal-looking waveforms are visible
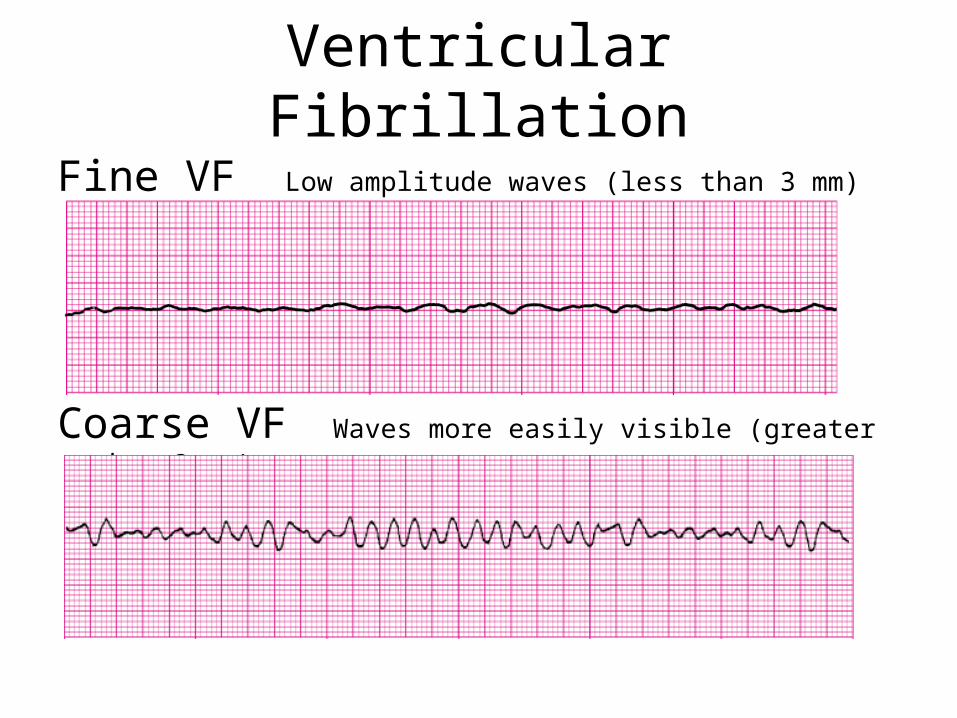
Ventricular Fibrillation
Fine VF Low amplitude waves (less than 3 mm)
Coarse VF Waves more easily visible (greater than 3 mm)
Ventricular Fibrillation
Because artifact can mimic VF, always check the patient’s pulse before beginning treatment for VF
The patient in VF is unresponsive, apneic, and pulseless
VF – Causes
Extrinsic factorsIncreased sympathetic nervous system activity
Vagal stimulation
Metabolic abnormalities
Hypokalemia
Hypomagnesemia
Antidysrhythmics and other medications
Psychotropics
Digitalis
Sympathomimetics
Environmental factors
Electrocution
Intrinsic factorsHypertrophy
Ischemia
Myocardial failure
Enhanced AV conduction
Bypass tracts
“Fast” AV node
Abnormal repolarization
Bradycardia
VF – Intervention
Begin CPR until a defibrillator is available
On arrival of the defibrillator, deliver unsynchronized
shocks
Perform endotracheal intubation, establish IV access
Administer medications per current resuscitation
guidelines
Questions!
Please type in the text box if you are watching the live presentation.
Otherwise feel free to give us a call at 815-300-7140 or email [email protected].
Thank you!