Embed Size (px)
Citation preview

Significance of and Techniques to Reduce the Frequency of Positive
Surgical Margins
James A. Eastham, MDMemorial Sloan-Kettering Cancer Center
353 East 68th StreetNew York, NY 10591
NOTE: The following slides are to be used for medical education purposes only. Copyright belongs to Prous Science and Prous Science is not responsible for any modification or change made by the users to these slides.

Index
• Definition of a positive surgical margin• Significance of a positive surgical margin• Surgical techniques to reduce the frequency of a
positive surgical margin
• Key words: prostate, radical prostatectomy, surgical margin

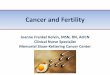
Definition of a Positive Surgical Margin
• At the time of specimen processing, the outer surface of the radical prostatectomy is inked to define the margins of resection

Definition of a Positive Surgical Margin
• A positive surgical margin is defined as “tumor on ink”, meaning the pathologist sees cancer cells directly in contact with ink at histological examination
Cancer cells abut the ink: positive margin

Significance of a Positive Surgical Margin
• Multiple series suggest that a positive surgical margin is an independent predictor of biochemical recurrence (BCR) after radical prostatectomy (RP)1-5
• This risk remains even after controlling for other known risk factors for BCR after RP, including pre-treatment PSA, RP Gleason score, presence or absence of extraprostatic cancer, presence or absence of seminal vesicle invasion and presence or absence of lymph node invasion

Multivariable Analysis of Risk of 10-year Progression after Radical Prostatectomy1
Variable HR (95%) CI p-value
+SM 1.52 (1.06-2.16) 0.002
Gleason sum 1.82 (1.55-2.14) <0.0005
ECE 2.24 (1.56-3.22) <0.0005
SVI 2.54 (1.81-3.56) <0.0005
LNI 2.32 (1.60-3.37) <0.0005
n=1389 patients (1983-2000)+SM: Overall: 12.9%; pT2: 6.8%; pT3: 23%

Significance of a Positive Surgical Margin1
• Even after controlling for other known risk factors of BCR after RP, a patient with a positive surgical margin is 1.5 times more likely to experience cancer recurrence than a patient with a negative surgical margin
• Of these clinical and pathological features, only the status of the surgical margins has the potential to be influenced by the surgeon

Significance of a Positive Surgical Margin
• Are positive surgical margins inherent in the nature of the cancer, like extracapsular extension, or can margins be influenced by the surgeon/surgical technique?

Surgeon’s Influence on the Likelihood of a Positive Surgical Margin2
• Equal access medical center• Academic and private practice urologists• 4629 RP performed by 44 individual surgeons
• Question: What are the predictors of a positive surgical margin at the time of RP?– Analysis included known clinical and histological
variables as well as surgical experience (number of RP performed) and individual surgeon

Multivariable Analysis for Risk of a +SM Based on Clinical and Pathological Parameters2
Variable p-value
Serum PSA level < 0.01
Extracapsular extension < 0.01
Seminal vesicle invasion 0.86
Lymph node involvement 0.56
Radical prostatectomy Gleason sum < 0.01
Surgical volume 0.01
Surgery date < 0.01
Surgeon 0.05

Individual Surgeon and +SM Study2
The rate of +SM in RP specimens varies widely within and among hospitals and surgeons, whether at an open staffing hospital or a cancer referral center, and cannot be explained by surgical volume alone
Wide variations in +SM rates persist even when corrected for all known cancer prognostic factors
Differences in surgical technique, while hard to define, seem to result in substantial differences in positive margin rates and long-term cancer control rates

What Can Be Done to Decrease the Risk of a Positive Surgical Margin?6-9
• Exposure and hemostasis• Appropriate extent of neurovascular bundle (NVB)
preservation• Wide dissection including Denonvilliers’ fascia, lateral
pedicle and bladder neck

What Can Be Done to Decrease the Risk of a Positive Surgical Margin at Open RP?
• Exposure and hemostasis– 8-10 cm lower midline incision– Slight flexion of table– Adequate retraction to expose the deep pelvis
• Author’s choice: Turner-Warwick retractor
• Appropriate extent of NVB preservation• Wide dissection including Denonvilliers’ fascia, lateral
pedicle and bladder neck


What Can Be Done to Decrease the Risk of a Positive Surgical Margin?
• Exposure and hemostasis– Prior to division of the dorsal venous complex
(DVC): suture-ligate the DVC at bladder neck, mid-prostate and pelvic floor
– Isolate DVC from urethra• Author’s choice: right-angled clamp and stainless steel wire
– Divide DVC with knife and oversew cut-edge• Appropriate extent of NVB preservation• Wide dissection including Denonvilliers’ fascia, lateral
pedicle and bladder neck

DVC ligated at bladder neck andmid-prostate

Division of the DVC over a guide wire. The DVC has been ligated proximally and distally. A right-angled clamp is passed beneath the DVC and grasps a wire. The DVC must be transected distal to all prostatic tissue.

The cut edges of the DVC areoversewn; the last bite being taken through the periosteum of the pubis

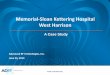
What Can Be Done to Decrease the Risk of a Positive Surgical Margin?
• Exposure and hemostasis• Appropriate extent of NVB preservation
– Thorough assessment of risk of cancer in the area of the NVB
– Selection of appropriate plane of dissection• Intra-, Inter- or Extrafascial dissection
• Wide dissection including Denonvilliers’ fascia, lateral pedicle and bladder neck


IntraInter
Extra
Rectum
Prostate
NVB
LevatorAni Muscle
Prostatic Capsule
Pubic bone
Endorectal MRI of prostate demonstrating the NVB andpossible planes of dissection7, 10

(R) Cavernous(R) Cavernousnervenerve
ProstateProstate
FeetFeet
HeadHead
The extent of NVBpreservation is a balance between attempts to optimize the recovery of potency while at the same time removing all the cancer (a negative surgical margin). The majority of screen-detected prostate cancers will be candidates for complete NVB preservation (intrafascial dissection).

Apical Dissection with Nerve Sparing1) Incision of lateral pelvic fascia above the nerve 2) Dissection of the NVB from apical third of the prostate 3) Sharp division of post layer of prostatorectal (Denonvilliers’) fascia

Click on the link below to start the video. The initial mobilization of the NVB is complete. The scissors sharply incise Denonvilliers’fascia exposing the yellow fat of the anterior rectal wall

Wide resection of the right NVB in the area of a large, palpable cancer. The dissection is facilitated by starting the dissection laterally such that all periprostatic tissue can be resected

Transection of the Bladder NeckWide dissection of the lateral pedicles around the base, and transection of the bladder neck above the prostate, will reduce the risks of positive margins. “Bladder neck preservation” does not improve continence.
There should be ample tissue in the angle between the base of the prostate and the seminal vesicles. Leave more
tissue here

Conclusions
• Positive surgical margins are an adverse prognostic feature at the time of RP
• Of all prognostic factors, this is the only one modifiable by surgical technique
• Most patients can undergo preservation of the majority of the tissue at the NVB and still have complete resection of their cancer (negative surgical margin)
• Patient selection, complete resection of Denonvilliers’ fascia and wide resection at the bladder neck have been shown to reduce the incidence of a positive surgical margin

References1. Swindle, P., Eastham, J.A., Ohori, M., Kattan, M.W., Wheeler,
T., Maru, N., Slawin, K., Scardino, P.T. Do margins matter? The prognostic significance of positive surgical margins in radical prostatectomy specimens. J Urol 2005, 174: 903-907.
2. Eastham, J.A., Kattan, M.W., Riedel, E., Begg, C.B., Wheeler, T.M., Gerigk, C., Gonen, M., Reuter, V., Scardino, P.T. Variations among individual surgeons in the rate of positive surgical margins in radical prostatectomy specimens. J Urol 2003, 170: 2292-2295.
3. Karakiewicz, P., Eastham, J., Graefen, M., Cagiannos, I., Stricker, P., Klein, E., Cangiano, T., Schröder, F., Scardino, P., Kattan, M. Prognostic impact of positive surgical margins in surgically treated prostate cancer: Multi-institutional assessment of 5831 patients. Urology 2005, 66: 1245-1250.
4. Ward, J.F., Zincke, H., Bergstralh, E.J., Slezak, J.M., Myers, R.P,, Blute, M.L. The impact of surgical approach (nerve bundle preservation versus wide local excision) on surgical margins and biochemical recurrence following radical prostatectomy. J Urol 2004, 172:1328-1332.

References5. Palisaar, R-J., Noldus, J., Graefen, M., Erbersdobler, A., Haese,
A., Huland, H. Influence of nerve-sparing (NS) procedure during radical prostatectomy (RP) on margin status and biochemical recurrence. Eur Urol 2004, 47: 176-184.
6. Eastham, J.A., Scardino, P.T. Radical prostatectomy for clinical stage T1 and T2 prostate cancer. In: Comprehensive Textbook of Genitourinary Oncology 2002, 722-738 (Ed. Vogelzang, N) Philadelphia: Lippincott Williams & Wilkins.
7. Montorsi, F., Salonia, A., Suardi, N. Improving the preservation of the urethral sphincter and neurovascular bundles during open radical retropubic prostatectomy. Eur Urol 2005, 48: 938–945.
8. Walsh, P.C., Partin, A.W., Epstein, J.I. Cancer control and quality of life following anatomical radical retropubic prostatectomy: results at 10 years. J Urol 1994, 152: 1831-1835.

References
9. Naya, Y., Slaton, J.W., Troncoso, P., Okihara, K., Babaian, R.J. Tumor length and location of cancer on biopsy predict side specific extraprostatic cancer extension. J Urol 2004, 171: 1093-1097.
10. Graefen, M., Walz, J., Huland, H. Open retropubic nerve-sparing radical prostatectomy. Eur Urol 2006, 49: 38–48.