Embed Size (px)
Citation preview
SIGHT AND LIFEMagazine Issue No 1/2009
Girl having porridge fortified with micronutrient powder at SedimosangDay Care Centre, Ivory Park, South Africa
Food Fortification as a Public Health Strategy
Food industries add vitamins and minerals to the products they manufacture for severalreasons: to bring back the micronutrients that are lost during production (restoration),to imitate the nutritional value of natural products that are replaced (equivalence), andto incorporate nutrients that are absent or present in lower amounts in the natural in-gredients (enrichment). In all such cases, the end results are fortified foods.Read more on p. 6
Food Fortification
Micronutrients in DOHaD
Zinc Intervention
Ready-to-Use Food
Global Food Security
ANEC III
Congress of Dietetics
Nutrition and Food Science
In Memoriam
A Day in the Life
Anemia-Control Programs
News
Letters to the Editor
Publications

Contents
Food Fortification as aPublic Health StrategyOmar Dary of A2Z/the USAID MicronutrientProject describes the requirements for successfulfood fortification strategies.
6
SIGHT AND LIFE
Correspondents
William S. BlanerMartin BloemGeorge BrittonIan Darnton-HillOmar DaryFrances R. DavidsonJohn W. Erdman JrPhilip Harvey
Richard F. HurrellRolf D.W. KlemmDonald S. McLarenRegina Moench-PfannerChristine Northrop-ClewesNoel W. SolomonsFlorentino S. SolonAlfred Sommer
David I. ThurnhamAndrew TomkinsEmorn WasantwisutKeith P. West JrYu XiaodongChittaranjan S.YajnikMichael B. Zimmermann
2
The Role of Micronutrientsin the Developmental Origins ofHealth and DiseaseMicronutrient deficiencies may play a significantrole, both in undernutrition and overnutrition andrelated health consequences. 16
Contents
Editorial 4
Food Fortification as a Public HealthStrategy and the Contributions of A2Z 6
The Role of Micronutrients in theDevelopmental Origins of Health andDisease 16
Systematic Reviews of ZincIntervention Strategies 26
Locally Produced Ready-to-Use Food(RUF) 29
Conference on Global Food Security 38
Third African NutritionalEpidemiology Conference 42
Report on the 15th InternationalCongress of Dietetics 46

Magazine Issue 1/2009Contents
3
Locally Produced Ready-to-Use Food(RUF)RUFs are a recent addition to the toolbox in thefight against malnutrition, revolutionizing thetreatment and care of severe and moderateacute malnutrition. 29
Monitoring Anemia-Control ProgramsAs iron deficiency affects all populations of theworld irrespective of race, culture or ethnicbackground, it is important that iron status iscorrectly monitored and the effects of iron treat-ment correctly interpreted. 59
Training in Nutritionand Food Science 47
In Memoriam:Norman Irving Krinsky 50
In Memoriam:John Lawrence Beard 54
A Day in the Life 56
Monitoring Anemia-ControlPrograms 59
NewsGlobal Financial and Food Crisis 67
Launch of the Marathi Healthy EyesActivity Book 68
Celebration of the 5th BillionVitamin A Capsule 69
Letters to the Editor 70
Publications 74

SIGHT AND LIFE Editorial
4
Social Innovation not only for EconomicRecovery, but also for Combating HiddenHunger and Poverty
As the world struggles to come to grips with the reali-ties of a global recession led by the most progressiveeconomic democracies, influential thinkers and poli-cy makers have started to look upon the idea of socialinnovation as a new guiding principle for economicrecovery efforts.
In the United States, the Obama Administration hascreated an Office of Social Innovation in the WhiteHouse. The Organization for Economic Cooperationand Development (OECD), meanwhile, has had aForum on Social Innovations under its LocalEconomic and Employment Development (LEED)program since 2000.
According to the working definition used by theOECD framework, “[social innovation] can concernconceptual, process or product change, organization-al change and changes in financing, and can deal withnew relationships with stakeholders and territories.”It goes on to state that social innovation seeks newanswers to social problems by identifying and deliv-ering new services, processes, competencies, jobs,and forms of participation that improve the quality oflife of individuals and communities. Social innova-tion is distinguished from economic innovationbecause “it is not about introducing new types of pro-duction or exploiting new markets in itself but aboutsatisfying new needs not provided by the market(even if markets intervene later) or creating new,more satisfactory ways…of giving people a place anda role in production.”
SIGHT AND LIFE’s fight against micronutrient defi-ciencies over the last 22 years originated under acharitable mindset, characterized by the fact that nofinancial returns to the giver are calculated to justifythe giving. Indeed, in many areas of assistance, char-ity remains the dominant motivation simply becausethe moral case is overwhelming, and the calculationand extraction of tangible returns for the provision ofoften critically needed resources to population groupsdeemed incapable of paying for those resourceswould be considered unethical.
Nonetheless, charityalone cannot createsustainable solutions tocomplex health andsocial problems, whoseroots are embeddedwithin equilibrious but inequitable distribution sys-tems and economic infrastructure that need a major‘re-invention.’ While charity has a place in providingshort- to medium-term relief to under- or unservedpopulations – and SIGHT AND LIFE will continue tosupport charitable efforts as we have done for overtwo decades – we do support efforts to foster socialinnovation approaches that result in lasting public,private and community partnerships to create new andsustained ways of solving social problems and meet-ing social needs – particularly in addressing the glob-al crisis of hidden hunger and its consequences,including nutritional anemia and the double burden ofmalnutrition.
As a knowledge-creating and knowledge-diffusingplatform in the field of micronutrient deficiencies andprogrammatic solutions to these, SIGHT AND LIFEseeks to increase its role in helping to develop socialinnovations that deliver on our mission as a philan-thropic initiative. As a start, since 2007, we haveactively initiated, built on and expanded partnershipactivities between our parent company, DSM, itsNutrition Improvement Program, and the UnitedNations World Food Programme (WFP) aimed atdeveloping, producing and distributing new and moreeffective multiple micronutrient product formulationstargeted to population groups at the bottom of thesocioeconomic pyramid. In the near future, we alsointend to promote pilot- or small-scale social innova-tions in the projects we assist through new grant-making and donation-giving policies.
In a world facing the greatest recession in recent his-tory as well as unbridled urbanization and ‘modern’lifestyles that amplify the frightening consequencesof an unhealthy lifestyle and diet, we clearly need toinvest in the most effective strategies in the fightagainst malnutrition and poverty. That includes bothcharity-driven approaches that bridge resource gapsand meet urgent needs in the short- and medium-terms, as well as social innovation approaches that
Welcome
SIGHT AND LIFE Magazine 2009;1:4–5
Magazine Issue 1/2009Editorial
5
allow cost reductions and long-term sustainability inthe production and distribution of public goods andservices.
If our editorial on social innovation has sparked yourinterest, we recommend the enclosed SIGHT ANDLIFE Annual Report 2008 for further reading, whichfeatures this as emerging topic as its theme.
This edition of the Magazine also includes a contri-bution on Food Fortification as a Public HealthStrategy, aptly prepared by our long-term correspon-dent Omar Dary (p. 6). Among other strategies, suchas dietary improvement and supplementation, foodfortification plays an important role as a publichealth intervention to close nutritional gaps in essen-tial micronutrients.
In her paper on the Role of Micronutrients in theDevelopmental Origins of Health and Disease,Christine Stewart reviews the effects of maternalmicronutrient status on risk factors for chronic dis-ease and poses questions for further research (p. 16).
Veronika Scherbaum and colleagues describe what ittakes to develop and locally produce a cereal-basedReady-to-Use Food (RUF) for moderately and mild-ly wasted children in Indonesia (p. 29). RUFs are arecent addition to the toolbox in the fight againstmalnutrition, revolutionizing the treatment and careof severe and moderate acute malnutrition.
Sadly, the scientific community and public at largehave lost two of our most distinguished scientists.
We pay tribute to Norman I. Krinsky and John L.Beard, who made major contributions in advancingthe field of micronutrients. Norman Krinsky ledcarotenoid and vitamin A research to unexploredheights (p. 50) and without John Beard, our knowl-edge of iron in the brain and neurobehavioral func-tion would still be significantly shallower (p. 54).
For this edition of the Magazine, our Day in the Lifefeature meets the SIGHT AND LIFE team inKaiseraugst, which has grown recently (p. 56). Ourrecent ‘addition,’ Jee Rah, and Anne-Catherine Freyand Svenia Sayer-Ruehmann talk about their specif-ic roles within SIGHT AND LIFE.
Last but not least, as a platform for the exchange ofprogrammatic and scientific information, we wouldlike the SIGHT AND LIFE Magazine to remain ever-evolving and adaptive to the new realities of themicronutrient field. We are, therefore, currently con-ducting a survey to gather our readers’ opinions.
We would very much appreciate it if you could par-ticipate in our reader survey, and share with us yourviews on the Magazine and your suggestions forways to improve it through the short questionnaire.More information about the survey is included onp. 37.
With best regards

SIGHT AND LIFE Food Fortification
6
Background
Food industries add vitamins andminerals to the products they man-ufacture for several reasons: tobring back the micronutrients thatare lost during production (restora-tion), to imitate the nutritionalvalue of natural products that arereplaced (equivalence), and toincorporate nutrients that are absentor present in lower amounts in thenatural ingredients (enrichment). Inall such cases, the end results arefortified foods.
Three types of food fortificationhave been identified: mass (staplesand condiments that are promotedby governments as public healthmeasures), targeted (complemen-tary foods and products aimed atspecific population groups), andmarket-driven (a strategy of thefood industry to attract consumerattention to the improved nutrition-al value of its products).1 Theincrease of micronutrient intakesthrough these and other nutritionalinterventions (e.g. supplementa-tion) should be sufficient to com-plement the usual diet for attainingthe required daily needs (or esti-mated average requirements, EAR)for most individuals of the popula-
tion. However, fortification levelsshould be regulated so individualsof the same population are notexposed to intakes above the toler-able upper intake levels (UL).Thus, to be effective and safe, foodfortification should be planned,regulated, and well supervised.
A justifiable, safe, efficacious,cost-efficient, and sustainable foodfortification program requires theintegrated efforts of various actorsin real partnerships. These effortsare the responsibility of the
research, public, private, and socialsectors. Figure 1 illustrates thevarious activities needed in foodfortification programs. The essen-tial and logical sequence of theseactivities is often not fully appreci-ated because this strategy is fre-quently promoted as the simpleintroduction of a fortified productor as an effort focused mainly onenacting mandatory fortificationstandards. Consequently, food for-tification projects are often ineffec-tive.
Food Fortification as a PublicHealth Strategy and theContributions of A2Z
Omar DaryA2Z/the USAID Micronutrient Project, Washington, DC, USA
Correspondence: Omar Dary, Project A2Z, Academy for EducationalDevelopment (AED), 1825 Connecticut Avenue NW # 800, Washington,DC 20009-5721, USAE-mail: [email protected]
Figure 1: Components and players in public health food fortifica-tion programs
An Efficacious and Sustainable Program
Cost-Effective AnalysisEconomists, Statisticians
MAIN PLAYERS
Impact AssessmentResearchers, Statisticians, Food and Biochemical Laboratories
Social Marketing and EducationFood Industry: Marketing Dept./Gov. Guidance
Governmental InspectionFood Control from MOH and M. of Economy/Food Labs
Quality Control and Assurance-FactoriesQuality Control Department
Implementation and Production of Fortified FoodProduction Department
Implementation and Production of Micronutrient PremixesPremix Manufacturers
Standards and RegulationsBureau of Standards
National Policies and StrategiesCentral Government
Science (Efficacy Trials), and AssessmentResearchers
ProgramM
onitoringand
Evaluation
SIGHT AND LIFE Magazine 2009;1:6–15

Magazine Issue 1/2009Food Fortification
7
The steps in Figure 1 suggest that, for the good imple-mentation of each activity, it is important to have ade-quate support of the instruments and actions from theprior steps. Nevertheless, a program of this type doesnot end when effectiveness is demonstrated. The topstep becomes the base of the following cycle, becausefood fortification programs should be conceptualizedas dynamic and under permanent evolution, respond-ing to modifications in the dietary pattern, environ-mental health conditions, and advances in scientificknowledge, technology and programmatic experience.Figure 2 shows the continuous rotation of the func-tional components of a food fortification program.
Premises for nutritional and health impact
The impact of any food fortification program is asso-ciated with the supply of adequate amounts ofbioavailable micronutrients to the target populations.Successful programs are those that: (a) provide suffi-cient additional intake of the required micronutrients(size of the provision) in response to (b) a nutritionalgap of specific micronutrients (magnitude of theneed), with the capacity to (c) reach a significant pro-portion of the target population (extension of the inter-vention, or coverage). Rarely does one fortificationvehicle fill all these requirements. However, in mostcases, adding micronutrients to foods will almostalways satisfy some of the nutritional needs of a pro-portion of the population. The magnitude of an indi-vidual’s benefit depends on the dietary habits of thepopulation, which determine both the degree of thedeficiency (among other causes, the basal provision ofmicronutrients by the usual diet) and the potential ofthe fortified food to deliver an important amount of theneeded micronutrient (which is a function of the con-sumed amount of the fortification vehicle and itsmicronutrient content). How the population benefits isin direct proportion to the market penetration of thefortified products. In most circumstances complemen-tary measures should be simultaneously implementedto reach the public health goal. Thus, to make suitableprogrammatic combinations, a strong assessment, andmonitoring and evaluation components are alwaysessential. Research institutions should assume theseroles but are generally absent in many current food for-tification and nutritional intervention efforts.
Beyond the scientific basis of food fortification pro-grams, the success depends on industries manufactur-ing high quality products following adequate standardsthat are well enforced by the government, and on con-sumer awareness of the product’s benefits when com-bined with good life habits and healthy diets.
Evidence
Several case studies of food fortification provide evi-dence that well-planned and managed fortification pro-grams can help reduce micronutrient deficiencies.
Salt iodization
The results from several countries with salt iodizationprograms demonstrated that: 1) they can achieve highcoverage; and 2) salt used at the household level cancontain adequate iodine (20–40 mg/kg) to improveiodine intake (usually 150–200% EAR for the averageperson) at current patterns of salt consumption (5–10g/day), to prevent goiter and other iodine deficiencydisorders. Salt can continue being a good iodine-delivery vehicle even when its daily consumptionshould decrease in response to programs for the pre-vention of chronic diseases, where it is only necessaryto proportionally increase the iodine content.2
Sugar fortification with vitamin A
In Central America, the coverage of vitamin A-forti-fied sugar is high (> 75%). The fortificant level pro-vides, on average, > 150% of the EAR. At this level ofcoverage and vitamin A supply, the population intakewas adequate to address vitamin A deficiency for thepopulation aged 36 months and older. Preventive sup-plementation is still used for children aged 6–24months to complete the provision and coverage of the
Figure 2: Dynamic cycle of the functional com-ponent of a food fortification program;modified from Eva Hertrampf, Instituteof Nutrition and Food Technology(INTA), Chile
Design
Program
Cost-Effectivness
Impact Assessment
Consumption
Implementation
Supervision
SafeEfficaciousSustainable
IntakeBiomarkers
National PoliciesStandards and Regulations
Premix ProductionFortification Process
QC/QAInspection
Science and Assessment
Social MarketingPurchasing
M & E

SIGHT AND LIFE Food Fortification
8
sugar fortification program.3
Nicaragua reduced the prevalenceof low serum retinol in pre-schoolaged children through preventivesupplementation and sugar fortifi-cation. Based on the actual retinolserum levels, Nicaragua can claimthat vitamin A deficiency in thecountry is controlled.4
Flour fortification with folic acid
Data from programs in Canada,5
Chile,6 Costa Rica,7 South Africa8
and the USA9 showed that, afterflour was fortified with folic acid,the prevalence of neural tubedefects plateaued at about7–10/10,000 – a decrease of20–85% in direct proportionto the magnitude of the preva-lence at baseline. Folateintakes increased, on average,50–200% EAR, which, ingeneral – with the exceptionof Chile – is far from levelsthat would increase the risk ofsome individuals reachingcurrent UL values. In theUSA, intakes are near orabove the UL values becauseof the simultaneous use offolic acid supplements ratherthan by the additional intakeof folic acid received fromfortified cereal flours.10
Therefore, if the folic acidcontent is chosen according toflour consumption, establish-ing a safe and efficacious for-tification program with folicacid is possible.
As with other examples, effective-ness is closely associated to a sig-nificant increase of the micronutri-ent intake through fortified foodconsumption and its accessibility tothe population at large. It is impor-tant to emphasize that the biologi-cal impact depends on the size ofthe micronutrient provision to in-dividuals and the population cover-age, and is not due to the simple
presence of fortified foods in themarket.11
Food and condiment fortificationwith iron
Recent fortification trials suggestthat it is possible to use some foodvehicles to provide sufficient ironto improve iron status. The fortifi-cation of maize flour in Kenya12
and fish sauce in Viet Nam13 withsodium iron ethylenediamine-tetraacetic acid (NaFeEDTA)improved the biomarkers associat-ed with iron status. In Cambodia, asimilar effect was obtained by com-
bining ferrous sulfate and citricacid in fish sauce.14 In Thailand,snacks made with wheat flour,sugar, margarine, and differenttypes of iron were also found effi-cacious to improve iron-status bio-markers.15 In all cases, the biologi-cal impact appears to be independ-ent of the iron type. The importantfact is to supply sufficient iron,depending on the specific bioavail-ability of each iron compound, toprovide 60–90% of the correspon-
ding EAR.16 Iron compounds withgood bioavailability are more like-ly to create efficacious programsbecause the iron intakes that areneeded are lower and, hence, easierto incorporate into food matricesthan those required for less-bioavailable iron forms.
Regrettably, the iron contents nec-essary for reaching good iron pro-visions are very difficult to attain inmost flour fortification programsbecause of sensorial incompatibili-ty between the iron compounds andthe food matrices. In any case, ironbioavailability of the diet is the fac-
tor that most influences a suc-cessful iron fortification pro-gram.17
Goal
The goal of food fortificationis to increase the micronutri-ent intake from the diet andprovide a public health bene-fit without the risk of excessintake. Well-designed pro-grams will help reducemalnutrition and, in turn, im-prove health, lessen morbidi-ty and decrease child mortali-ty. The A2Z Project is com-mitted to promoting compre-hensive fortification projectsthat address all food forti-fication components. Focusedon strengthening public sec-tor capacities – usually theweakest components – A2Z
emphasizes integrated monitoringand evaluation systems for allnutritional interventions so effec-tive and sustainable public healthnutrition programs are carefullydesigned, implemented and evalu-ated.
Strategy
Optimal implementation of fortifi-cation programs involves coordi-nating closely with research, pub-
Vegetable oil fortified with vitaminsA and D

Magazine Issue 1/2009Food Fortification
9
lic, private, and consumer organi-zations and institutions. A2Z pro-vides technical assistance to designand analyze policies and strategies;and develop standards, guidelines,and practical tools for quality con-trol, enforcement, and monitoring.The project shares lessons learnedand facilitates experience ex-changes among countries throughtechnical workshops and trainingsessions. A2Z also disseminatesinformational materials, includingdocumented cases, to the interna-tional community to increaseknowledge, improve programmingpractices, and strengthen globalsupport for micronutrient pro-grams.
A2Z’s contributions in foodfortification
A2Z’s global and country activitiesin food fortification support andinform each other and contribute toresults at both levels. A2Z has builtinstitutional capacity to design andimplement program components assummarized below.
Science and assessment
A practical method to identifycandidate food vehicles and for-mulations for mass fortification:Precise determinations of the nutri-tional gap and identification ofpotential food fortification vehiclesare commonly lacking in food for-tification programs. A2Z collabo-rated with Emory Universityresearchers11 to use the informa-tion gathered through householdincome and expenditure surveys toestablish a practical procedure toassess the need for and the poten-tial benefit of mass fortification.The method uses purchasing dataand household composition to esti-mate individual food intake interms of adult equivalents. Thetotal amount of food purchased bythe family is divided by the total
energy requirement of every mem-ber of the family, expressed as pro-portion of the energy requirementof the adult male (i.e. the ‘adultequivalent’). Thus, for example, anadult woman represents 0.79 of theenergy requirement of an adultmale, and a child aged 1–3 years is0.45 adult equivalents. The proba-ble food intake of each member ofthe family is then estimated bymultiplying the ‘adult equivalentintake’ for the proportion of thecorresponding adult equivalent val-ues.
The World Bank, the Inter-American Development Bank, andthe Pan-American Health Organi-zation (PAHO) are using themethod in some projects. In part-nership with GAIN, the WorldFood Programme, and MakerereUniversity in Uganda, A2Z is vali-
dating this method against tradi-tional food consumption surveys.A2Z plans to use the same methodfor other countries in East, Central,and Southern Africa (ECSA). Themethod was used in Cambodia toassess the potential impact and cov-erage of food fortification vehiclesfor sugar and fish sauce asdescribed in Figure 3.
Literature review and case stud-ies: The A2Z project advanced theunderstanding of food fortificationthrough a published literaturereview of food fortification formanaging nutritional anemia.16
Technical feasibility, cost, andexperience of rice fortification inCosta Rica, China, the Philippines,and the USA were also reviewed.The rice fortification report18 wasprepared with the Institute of FoodTechnologists of the United States.
Figure 3: Coverage and potential impact (in terms of estimatedaverage requirement, or EAR) if sugar is fortified withvitamin A and fish sauce is fortified with iron inCambodia. The blue segment in the pie chart shows themaximum coverage possible based on food use. The darkpurple segment illustrates the proportion of consumersthat use the food vehicle, but which might not be fortifi-able because of production/trade conditions. The columnillustrates the average additional intake of the addedmicronutrient for those individuals who have access to thefortified food; a food that supplies 20% EAR or more ofa specific micronutrient is considered a good source ofthat micronutrient.
0
50
40
30
Vit. A B2
B1
Niacin B6
Folate B12
Iron Zinc Iodine
20
10
%E
AR
Palm Sugar
Importers ( ~ 3)
Coverage and Potential Impact of Fortified Sugar
0
50
40
30
Vit. A B2
B1
Niacin B6
Folate B12
Iron Zinc Iodine
20
10
%E
AR
~ 9 Large andMedium Size
Producers
Hundreds of Small Producers
Coverage and Potential Impact of Fortified Fish Sauce
SIGHT AND LIFE Food Fortification
10
The report has been translated into Spanish by PAHOand is now being used in rice fortification feasibilitystudies in Nicaragua and Panama.
National policies
ECSA guidelines on food fortification: A2Z support-ed several workshops in the ECSA region to establishcommon policies for mass fortification (salt, oil, sugar,and wheat and maize flours) based on estimated con-sumption patterns of staple foods. Malawi, Kenya, andUganda have used these regional guidelines to formu-late their national standards and regulations.
Standards and regulations
The food fortification formulator: This spreadsheettool19 is available in English on the websites of A2Zand ECSA, and in Spanish on the website of the WorldFood Programme for Latin America. It ensures boththe safety and maximum efficacy of micronutrient lev-els in mass fortification, and predicts the potential pub-lic health impact of fortified foods. The tool can cur-rently be applied to salt, oil, sugar, two types of wheatflour, and three types of maize flour.
The minimum information required is an estimation ofthe per capita consumption and the proportion of thepopulation consuming the potential food vehicle. TheFormulator calculates the probable food intake of thedifferent gender and age groups based on the principleof adult equivalency, described earlier. Three to fourfortification formulations are suggested in accordancewith the consumption pattern. The formulator presentsresults of intake in terms of percent of EAR, theRecommended Nutrient Intake (RNI), and in absoluteamounts. Users can select the fortification levels thatbest meet the nutritional objectives and the allowablecost. Once the fortification levels have been selected,the formulator computes the quality control and regu-latory parameters. The tool also allows the user to for-mulate the micronutrient content of premixes for dif-ferent dilution factors.
Training sessions to promote the use of the Formulatorhave been offered in some ECSA countries. Similartraining activities were held in Central and SouthAmerica in workshops sponsored by FANCAP andPAHO/WHO, respectively.
Production of micronutrient premixes
ECSA regional certification procedure: Quality –and the expected effectiveness – of food fortificationdepends heavily on the micronutrient premix quality.In most countries, regulation and control of fortifiedfood products are absent. To address the problem, A2Zis supporting ECSA to establish a regional system tocertify micronutrient premixes.
Production of fortified foods
Collaboration to implement and improve nationalfood fortification programs: A2Z collaborates withother institutions to introduce fortification practices infood industries. Examples include the wheat flour for-tification project sponsored by GAIN in Uganda, andsalt iodization under UNICEF leadership in Cambodiaand HKI leadership in Guinea. A2Z works directlywith the Palestinian Authority in the West Bank onwheat flour and market-driven fortifications.
Advocacy for sugar fortification in Malawi andEcuador: A2Z collaborated with the Malawian officesof UNICEF and USAID, and with PAHO and theEcuadorian Institute of Food and Nutrition to promotesugar fortification with vitamin A. Both countries havestarted specific actions to introduce this intervention.
Women collecting food in Bangladesh after thecyclone Sidr
Magazine Issue 1/2009Food Fortification
11
Advocacy for wheat and maize flour fortification inTanzania: A2Z and the ECSA Health Secretariat (HS)work together with the National Working Group ofFood Fortification in Tanzania to introduce wheat andmaize flour fortification by large industries in thecountry.
Improving oil and wheat flour fortification pro-grams in the Philippines: A2Z built on previous proj-ects with the Filipino government to strengthen oil andwheat flour fortification.
Quality control and assurance (QC/QA)
Training food industry employees: A2Z providedtechnical instructions to the oil industry of Uganda andthe wheat flour industry of the West Bank to strength-en their quality control and assurance activities. Sometraining was also given to the oil and wheat flourindustries of the Philippines.
Manuals for food control for fortification pro-grams: A2Z worked with the ECSA HS to produceseveral food control manuals to cover the differentstages of the fortification process of several fortifiedproducts: salt, oil, sugar, wheat flour, and maize flour.INCAP and UNICEF/Guatemala translated these man-uals into Spanish for Central America.20
Governmental inspection
Manuals for inspecting and auditing fortified foods:The food control manuals included food inspection atfactories, importation sites, and retail stores and themost common analytical assays used in mass fortifica-tion. Many manuals, translated into Spanish byINCAP and UNICEF/Guatemala, have been adaptedand validated for Central America. Training work-shops using these manuals have been held in Malawi,Kenya, and Tanzania.
Food control rounds in Uganda: A2Z sponsored andprovided technical assistance to use the food controlmanuals of oil, salt, and maize and wheat flours inUganda. Three rounds of the system (auditing and col-lecting samples from factories, inspecting retail stores,examining imported products, and determining themicronutrient content in the collected fortified foods)have been done, covering most provinces of the coun-try. This experience will serve as a model for othercountries in the ECSA region.
Laboratory proficiency testing (LPT) exercise in theECSA region: A2Z and the ECSA HS conducted two
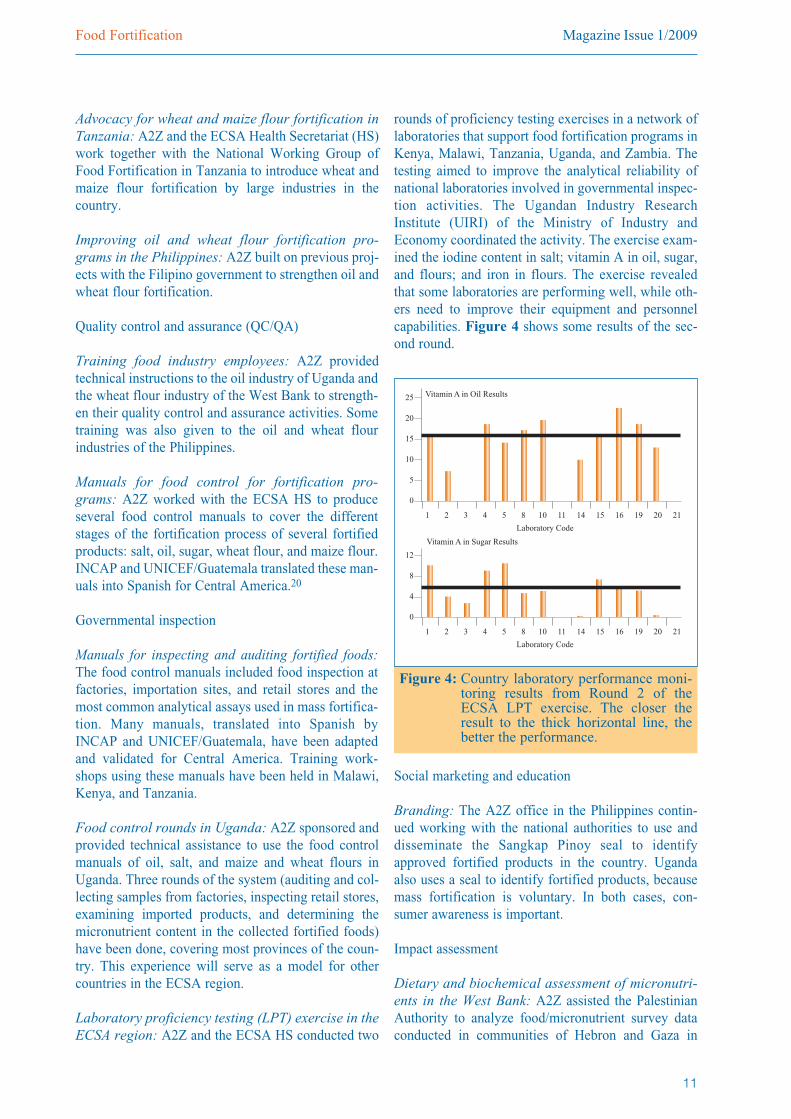
rounds of proficiency testing exercises in a network oflaboratories that support food fortification programs inKenya, Malawi, Tanzania, Uganda, and Zambia. Thetesting aimed to improve the analytical reliability ofnational laboratories involved in governmental inspec-tion activities. The Ugandan Industry ResearchInstitute (UIRI) of the Ministry of Industry andEconomy coordinated the activity. The exercise exam-ined the iodine content in salt; vitamin A in oil, sugar,and flours; and iron in flours. The exercise revealedthat some laboratories are performing well, while oth-ers need to improve their equipment and personnelcapabilities. Figure 4 shows some results of the sec-ond round.
Social marketing and education
Branding: The A2Z office in the Philippines contin-ued working with the national authorities to use anddisseminate the Sangkap Pinoy seal to identifyapproved fortified products in the country. Ugandaalso uses a seal to identify fortified products, becausemass fortification is voluntary. In both cases, con-sumer awareness is important.
Impact assessment
Dietary and biochemical assessment of micronutri-ents in the West Bank: A2Z assisted the PalestinianAuthority to analyze food/micronutrient survey dataconducted in communities of Hebron and Gaza in
Figure 4: Country laboratory performance moni-toring results from Round 2 of theECSA LPT exercise. The closer theresult to the thick horizontal line, thebetter the performance.
0
25
20
15
1 2 3 4 5 8 10 11 14 15 16 19 20 21
10
5
Vitamin A in Oil Results
Laboratory Code
0
12
1 2 3 4 5 8 10 11 14 15 16 19 20 21
8
4
Vitamin A in Sugar Results
Laboratory Code
SIGHT AND LIFE Food Fortification
12
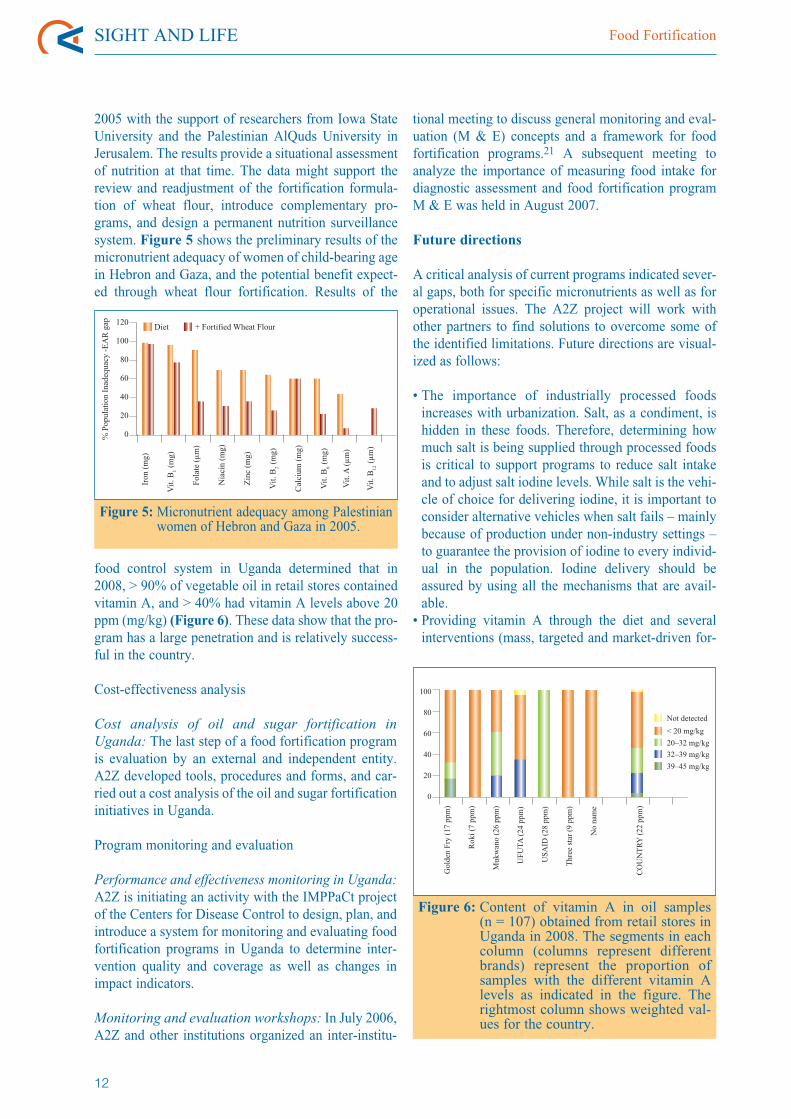
2005 with the support of researchers from Iowa StateUniversity and the Palestinian AlQuds University inJerusalem. The results provide a situational assessmentof nutrition at that time. The data might support thereview and readjustment of the fortification formula-tion of wheat flour, introduce complementary pro-grams, and design a permanent nutrition surveillancesystem. Figure 5 shows the preliminary results of themicronutrient adequacy of women of child-bearing agein Hebron and Gaza, and the potential benefit expect-ed through wheat flour fortification. Results of the
food control system in Uganda determined that in2008, > 90% of vegetable oil in retail stores containedvitamin A, and > 40% had vitamin A levels above 20ppm (mg/kg) (Figure 6). These data show that the pro-gram has a large penetration and is relatively success-ful in the country.
Cost-effectiveness analysis
Cost analysis of oil and sugar fortification inUganda: The last step of a food fortification programis evaluation by an external and independent entity.A2Z developed tools, procedures and forms, and car-ried out a cost analysis of the oil and sugar fortificationinitiatives in Uganda.
Program monitoring and evaluation
Performance and effectiveness monitoring in Uganda:A2Z is initiating an activity with the IMPPaCt projectof the Centers for Disease Control to design, plan, andintroduce a system for monitoring and evaluating foodfortification programs in Uganda to determine inter-vention quality and coverage as well as changes inimpact indicators.
Monitoring and evaluation workshops: In July 2006,A2Z and other institutions organized an inter-institu-
tional meeting to discuss general monitoring and eval-uation (M & E) concepts and a framework for foodfortification programs.21 A subsequent meeting toanalyze the importance of measuring food intake fordiagnostic assessment and food fortification programM & E was held in August 2007.
Future directions
A critical analysis of current programs indicated sever-al gaps, both for specific micronutrients as well as foroperational issues. The A2Z project will work withother partners to find solutions to overcome some ofthe identified limitations. Future directions are visual-ized as follows:
• The importance of industrially processed foodsincreases with urbanization. Salt, as a condiment, ishidden in these foods. Therefore, determining howmuch salt is being supplied through processed foodsis critical to support programs to reduce salt intakeand to adjust salt iodine levels. While salt is the vehi-cle of choice for delivering iodine, it is important toconsider alternative vehicles when salt fails – mainlybecause of production under non-industry settings –to guarantee the provision of iodine to every individ-ual in the population. Iodine delivery should beassured by using all the mechanisms that are avail-able.• Providing vitamin A through the diet and severalinterventions (mass, targeted and market-driven for-
Figure 5:Micronutrient adequacy among Palestinianwomen of Hebron and Gaza in 2005.
0
120
100
80
Iron
(mg)
Vit.
B1
(mg)
Fola
te(µ
m)
Nia
cin
(mg)
Zin
c(m
g)
Vit.
B2
(mg)
Cal
cium
(mg)
Vit.
B6
(mg)
Vit.
A(µ
m)
Vit.
B12
(µm
)60
40
20
%Po
pula
tion
Inad
equa
cy-E
AR
gap
Diet + Fortified Wheat Flour
Figure 6: Content of vitamin A in oil samples(n = 107) obtained from retail stores inUganda in 2008. The segments in eachcolumn (columns represent differentbrands) represent the proportion ofsamples with the different vitamin Alevels as indicated in the figure. Therightmost column shows weighted val-ues for the country.
0
100
80
Gol
den
Fry
(17
ppm
)
Rok
i(7
ppm
)
Muk
wan
o(2
6pp
m)
UFU
TA(2
4pp
m)
USA
ID(2
8pp
m)
Thr
eest
ar(9
ppm
)
No
nam
e
CO
UN
TR
Y(2
2pp
m)
60
40
20
Not detected
< 20 mg/kg
20–32 mg/kg
32–39 mg/kg
39–45 mg/kg
Magazine Issue 1/2009Food Fortification
13
tification, as well as periodical supplementation)should be carefully measured. The potential risks ofadverse effects from excessive intakes should bereduced to ensure safe, efficacious and widelyaccepted vitamin A programs.• Neural tube defects have been associated with folateand vitamin B12 deficiencies. In developing coun-tries, both deficiencies may be equally important.Therefore, programs to prevent neural tube defectsshould establish the magnitude of the nutritionalgaps of both micronutrients as one of their require-ments. Serum folate and biomarkers associated tovitamin B12 status seem to be relatively straightfor-ward for this objective.• The low bioavailability of minerals in most develop-ing country diets demands a serious review of theactual food fortification policies supported. New ironinterventions may be necessary to improve the ironstatus of needy populations in those countries.Furthermore, impact is closely associated to the qual-ity of iron compounds with good bioavailability.Special efforts to assure that the food industry isusing the recommended compounds would requireimproved analytical capabilities within these coun-tries – a costly but worthy investment.• Zinc is a mineral that is highly inadequate in the diet.Incorporating zinc into fortification formulas is gen-
erally feasible and simple. Although plasma/serumzinc is a good indicator to evaluate zinc status andintervention impact in populations, evidence of bio-logical impact is the main limitation in justifying theuse of zinc. This area deserves more attention andshould be developed simultaneously with the effortsto correct the nutritional gap.• Many negative consequences of micronutrient defi-ciencies are not only due to inadequacies of theabove-mentioned micronutrients; many others arealso involved. In the absence of biomarkers of statusfor most micronutrients, correcting deficient intakeswould be a good way to start the overall improve-ment of the human diet in the developing world.Therefore, practical methods to measure micronutri-ent intakes through the diet should be introduced,validated and extended.• The world population growth, the reduction of foodavailability for human consumption, and natural dis-asters are creating conditions leading to furtherreduced diversity in diets. Micronutrient statusshould be constantly surveyed simultaneously, withattention paid to sufficient food supply. The study ofthe evolution of the population nutritional status willincrease in importance in the years to come. It is crit-ical to identify which population sectors consumefortified foods in order to channel the resources and
• Systematize data analysis of the HouseholdIncome and Expenditure Surveys (HIES) to identi-fy food fortification vehicles and possible con-sumption patterns, and to propose fortification for-mulas for specific countries.
• Prepare articles and reports recognizing theimportance of the additional intake, bioavailability,and bioefficacy to predict the impact of food forti-fication programs.
• Publish documents that describe the importance ofdoing a comprehensive technical and economicalassessment before promoting wide-scale fortifica-tion programs (e.g., rice fortification).
• Develop a food fortification formulator to dissemi-nate principles and tools that support design, regu-lation, implementation, and control of food fortifi-cation programs.
• Advocate the extension of food fortification indeveloping countries: oil in Uganda and thePhilippines; sugar in Malawi and Ecuador; flours
in the West Bank, Tanzania and the Philippines;and rice in Nicaragua and Panama.
• Develop tools (manuals) and training to strengthenfood control actions by the food industries andgovernmental authorities.
• Facilitate field experiences at the national level toimplement food inspection and improve laboratoryreliability.
• Raise awareness for social marketing campaignsof fortified products to promote awareness aboutthe importance of fortified foods, while at thesame time preventing exaggerated and misleadingmessages.
• Promote global discussion to agree on M & Eterms and concepts, emphasize the importance ofassessing micronutrient intake as an importantcomponent of the food fortification programs, andencourage use of performance (process) and effec-tiveness (impact) M & E of food fortification pro-grams.
Box 1: Roundup of A2Z food fortification activities

SIGHT AND LIFE Food Fortification
14
attention to those who really needthem.• Overweight and obesity are rapid-ly increasing around the world,including developing countries.Many fortification vehicles arefoods whose consumption shouldnot be raised. This situationprompts special attention to healthclaims and social-marketing mes-sages associated with mass andmarket-driven fortification pro-grams to avoid deceiving and mis-leading messages prompted onlyfor profit interests. Establishingand enforcing regulations andstandards for labeling and adver-tising are priority areas in foodfortification.• Experience from several countriesreveals that many standards andregulations are confusing andcause conflicts because the foodindustry and the governmentinterpret them differently. Indus-try interprets minimum values asaverages, while the governmentuses them as absolute cut-offpoints. Furthermore, decisions are
often based on analytical assaysusing a very low number of sam-ples. These issues need to beurgently addressed.• The evolution of human nutritionand health must be assessed con-tinually. A comprehensive, inte-grated, and constant surveillancesystem should be implemented inall countries and regions to makeappropriate and timely decisions.Any nutritional interventionshould be justified and based onan assessment of the epidemio-logical situation. The perform-ance of implemented programsshould also be well documentedand shared. The improvement,appreciation, and permanence offood fortification programs aspart of public health strategiesmay depend on timely, transpar-ent, and well-distributed reports.Technical papers are also neededto share experiences and lessonslearned.
References
1. Allen L, Benoist B de, Dary O, HurrelR, eds. Guidelines on FoodFortification with Micronutrients.Geneva: World Health Organization,2006. Internet: http://www.who.int/nutrition/publications/micronutrients/9241594012/en/index.html (accessed20 February 2009).
Iodine• Supply of salt (and iodine) through commerciallyavailable foods is usually unknown.
• No accepted alternative vehicles exist to supplyiodine when access to industrially manufacturedsalt is restricted.Vitamin A• Total amount of vitamin A through the combinationof diet, food fortification, and supplementation mayalready be excessive for some populations.Folic Acid and Vitamin B12• Relative importance of folate and B12 deficienciesin neural tube defects in developing countries isunknown.Iron• Expected impact of iron fortification may be over-stated for populations whose diets are rich in ironabsorption inhibitors.
• Mechanisms to check for the use of good bioavail-able iron compounds in fortification are non-existent or weak.
Zinc• Insufficient evidence of impact for zinc interven-tions aimed to improve nutritional status.Other micronutrients• The importance of other micronutrients that partic-ipate in metabolic pathways is frequently neglectedbecause of the lack of specific biomarkers or func-tional indicators associated with their deficiencies.Micronutrients in a world under a food crisis• Food supply is threatened, and simultaneous atten-tion to micronutrients may be overlooked.Micronutrients in a double-burdened world• Intake increase of many fortification vehicles isundesirable in populations affected with chronicdiseases associated with unhealthy diets.Standards and enforcement• Conflicts have arisen between industry and govern-mental food control agencies because of the lack ofproper standards and inspection procedures.Program monitoring and evaluation• A frequent statement but rarely conducted.
Box 2: Identified gaps
Yellow peas from World FoodProgram

Magazine Issue 1/2009Food Fortification
15
2. World Health Organization (WHO). Salt as a Vehicle ofFortification. Geneva: WHO, 2007. Internet:h t t p : / /wh q l i b d o c .who . i n t / p u b l i c a t i o n s / 2 0 0 8 /9789241596787_eng.pdf (accessed 20 February 2009).
3. Mora JO, Dary O, Chinchilla D, Arroyave G. Vitamin A:Sugar Fortification in Central America – Experience andLessons Learned. MOST/The USAID MicronutrientProject/INCAP, 2000. Internet: http://www.mostproject.org/PDF/sugarlessonsEnglish.pdf (accessed 11 February2009).
4. Mora JO. Integrated System for Nutrition ProgramMonitoring and Evaluation. Conference at the Micro-nutrient Forum Meeting, Istanbul, Turkey, 2007. Internet:http://www.micronutrientforum.org/Meeting2007/Tuesday/T1425%20Mora%20for%20Sandino.pdf(accessed 20 February 2009).
5. Ray JG, Meier C, Vermeulen MJ, Boss S, Wyatt PR, ColeDEC. Association of neural tube defects and folic acid foodfortification in Canada. Lancet 2002;360:2047–8.
6. Lopez-Camelo JS, Orioli IM, Dutra MdG, et al. Reductionof birth prevalence rates of neural tube defects after folicacid fortification in Chile. Am J Med Genet2005;135A:120–5.
7. Tacsan L, Rivera MA. The Costa Rican experience:Reduction of neural tube defects following food fortifica-tion programs. Nutr Reviews 2004;62:(II)S40–3.
8. Sayed A, Bourne D, Pattinson R, Nixon J, Henderson B.Decline in the prevalence of neural tube defects followingfolic acid fortification and its cost-benefit in South Africa.Birth Defects Res Part A Clin Mol Tero 2008;82:211–6.
9. Honein MA, Paulozzi LJ, Mathews TJ, Erickson JD, WongL-Y C. Impact of folic acid fortification of the US food sup-ply on the occurrence of neural tube defects. J Am MedAssoc 2001;285:2981–6.
10. Yeung L, Yang Q, Berry RJ. Contribution of total dailyintake of folic acid to serum folate concentrations. JAMA2008;300:2486–7.
11. Imhoff-Kunsch B, Flores R, Dary O, Martorell R. WheatFlour Fortification is Unlikely to Benefit the Neediest inGuatemala. J Nutr 2007;137:1017–22.
12. Andang’o PEA, Osendarp SJM, Ayah R, et al. Efficacy ofiron-fortified whole maize flour on iron status of school-children in Kenya: a randomised controlled trial. Lancet2007;369:1799–1806.
13. Thuy PV, Berger J, Davidsson L, Khan NC, Lam NT, CookJD, Hurrell RF, Khoi HH. Regular consumption ofNaFeEDTA-fortified fish sauce improves iron status andreduces the prevalence of anemia in anemic Vietnamesewomen. Am J Clin Nutr 2003;78:284–90.
14. Longfils P, Monchy D, Weinheimer H, Chavasit V,Nakanishi Y, Schümann K. A comparative intervention trialon fish sauce fortified with NaFe-EDTA and FeSO4+citratein iron deficiency anemic school children in Kampot,Cambodia. Asia Pac J Clin Nutr 2008; 17:250–257.
15. Zimmermann MB, Winichagoon P, Gowachirapant S, HessSY, Harrington M, Chavasit V, Lynch SR, Hurrell RF.Comparison of the efficacy of wheat-based snacks fortifiedwith ferrous sulfate, electrolytic iron, or hydrogen-reducedelemental iron: randomized, double-blind, controlled trial inThai women. Am J Clin Nutr 2005;82:1276–82.
16. Dary O. The Importance and Limitations of FoodFortification for the Management of Nutritional Anemia. In:Kraemer K, Zimmermann MB, eds. Nutritional Anemia.Basel: SIGHT AND LIFE, 2007:315–36. Internet:http://www.sightandlife.org/pdf/NAbook.pdf (accessed 14February 2009).
17. Hoppe M, Hulthén L, Hallberg L. The importance ofbioavailability of dietary iron in relation to the expectedeffect from iron fortification. Eur J Clin Nutr 2008;62:761–69.
18. Alavi S, Bugusu B, Cramer G, Dary O, Lee T-C, Martin L,McEntire J, Wailes E. Rice Fortification in DevelopingCountries: A Critical Review of the Technical and Eco-nomic Feasibility. Project A2Z/USAID/AED/IFT, 2008.Internet: http://www.a2zproject.org/pdf/Food–Rice–Forti-fication–Report–with–Annexes–FINAL.pdf (accessed 11February 2009).
19. Dary O, Hainsworth M. The Food Fortification Formulator:Technical Determination of Fortification Levels andStandards for Mass Fortification. Project A2Z/USAID/AED, 2008. Internet: http://www.a2zproject.org/pdf/ Food–Fortification–Formulator.pdf (accessed 11 February 2009).
20. Guamuch M., Makhumula P, Dary O. Manuals for theControl and Inspection of Fortified Foods. Internet:http://www.sica.int/busqueda/Noticias.aspx?IDItem=33164&IDCat=3&IdEnt=29&Idm=1&IdmStyle=1 (accessed 28February 2009).
21. IMPPaCT/CDC, PAHO/WHO, A2Z/USAID. Monitoringand Evaluating Food Fortification Programs. 2008. Internet:http://www.a2zproject.org/pdf/Food–Fortification–M&E–July–2006–Consultation–AED–FINAL.pdf (accessed 23February 2009).
Fortified flour in China
SIGHT AND LIFE DOHaD and Micronutrients
16
Introduction
Undernutrition and micronutrientdeficiencies continue to be a prob-lem worldwide. An estimated 2 bil-lion people suffer from at least oneform of micronutrient deficiency.1
There is also a growing epidemic ofchronic disease, particularly indeveloping countries, where esti-mates show 80% of the burden ofchronic diseases may be felt.2
Many developing countries areexperiencing a double burden ofdisease with concurrent childhoodmalnutrition and adult obesity,3
sometimes even within the samehousehold.4
The field of research referred to asthe developmental origins of healthand disease (DOHaD) has high-lighted how malnutrition duringpregnancy or early childhood mayinfluence chronic disease riskdecades later. One of the mostwidely cited theories to explain thisis that of the ‘thrifty phenotypehypothesis,’ which proposes thatexposure to a deprived intrauterineenvironment may stimulate fetaladaptations to the growth rate,organ development, and metabolicpathways that may offer immediatesurvival benefits, but that mayresult in a greater risk of cardiovas-cular disease or type II diabetes inlater life,5 particularly if exposed toa more affluent postnatal environ-ment.6
The DOHaD hypothesis is of par-ticular relevance and concern todeveloping countries rapidly enter-ing the epidemiologic and nutri-tional transition. Over the course ofone generation, many societies are
experiencing rapid changes in dietand physical activity, so that popu-lations that may have experiencedundernutrition as infants and youngchildren may go on to becomeoverweight as adults.
To date, much of the literature hasfocused on how size at birth isassociated with blood pressure,insulin resistance or body composi-tion in later life. Yet, size at birthalone does not tell us how adequatethe mother’s diet was throughoutgestation. Deficiencies in micronu-trients, in particular, have beenfound to impact length of gestation,cognitive development, and organdevelopment, and a number ofwell-written reviews have exam-ined the effects of micronutrientson birth weight.7–10 There is now aneed to move beyond birth weightand explore how other aspects ofthe maternal diet may impact fetaldevelopment with consequenceswell beyond the neonatal period.
There have been a number of ran-domized controlled trials or obser-vational studies of maternal calci-
The Role of Micronutrients in theDevelopmental Origins of Healthand Disease
Christine P. StewartCenter for Human Nutrition, Department of Health, Johns HopkinsBloomberg School of Public Health, USA
Correspondence: Christine P. Stewart, Department of InternationalHealth, Rm. W2505, Johns Hopkins Bloomberg School of PublicHealth, Baltimore, MD 21205, USAEmail: [email protected]
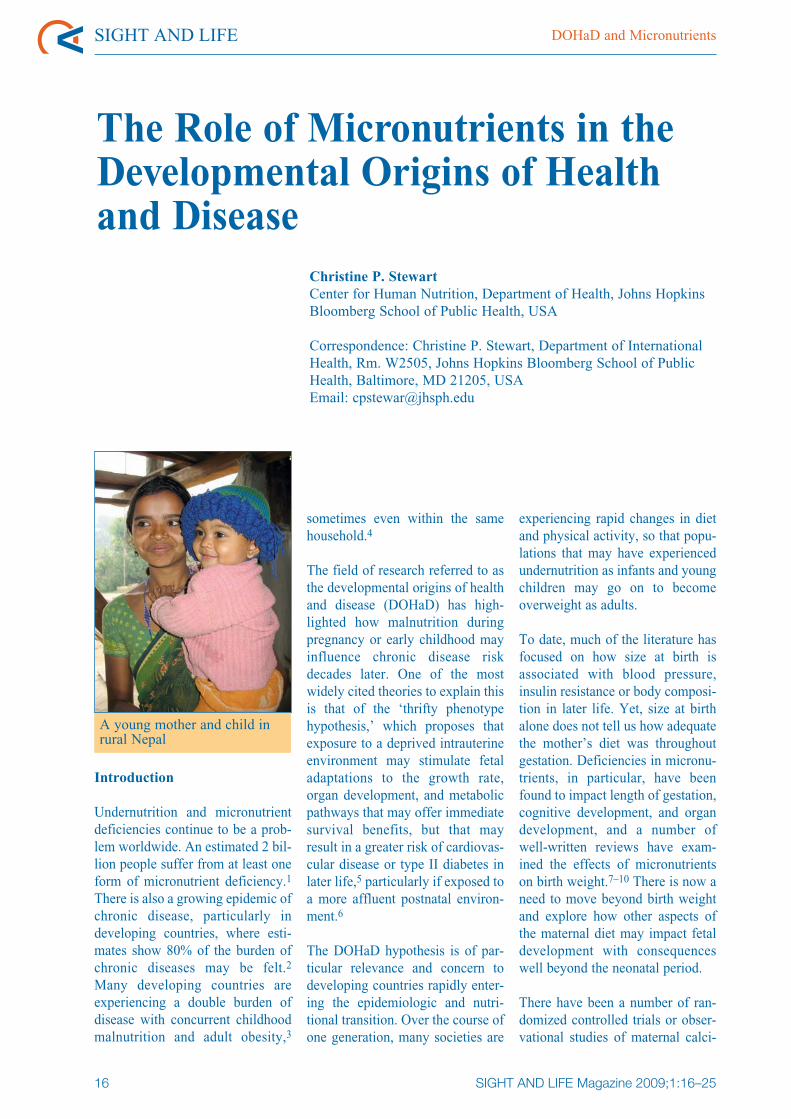
A young mother and child inrural Nepal
SIGHT AND LIFE Magazine 2009;1:16–25
Magazine Issue 1/2009DOHaD and Micronutrients
17
um or iron intake on cardiovascular risk factors amongchildren. Although there is limited data for othernutrients, there is evidence to suggest that folate,vitamin A and zinc may also be important in the devel-opmental origins of disease. The purpose of this articleis to review the studies of maternal micronutrientstatus on risk factors for chronic disease and posequestions for further research. This article is notintended to be a complete review of the proposedmechanisms of action, which have been morecomprehensively reviewed by others.11
Iron
Iron deficiency is the most common nutritional defi-ciency around the globe and is the most common causeof anemia.12 Anemia in pregnancy (defined as Hb < 11g/dL) is an observed risk factor for low birth weightand preterm delivery. Animal studies have demonstrat-ed that iron restriction during pregnancy causes eleva-tion in the offspring’s blood pressure13 and altered car-diovascular development,14 but these findings have notbeen consistently observed in humans.
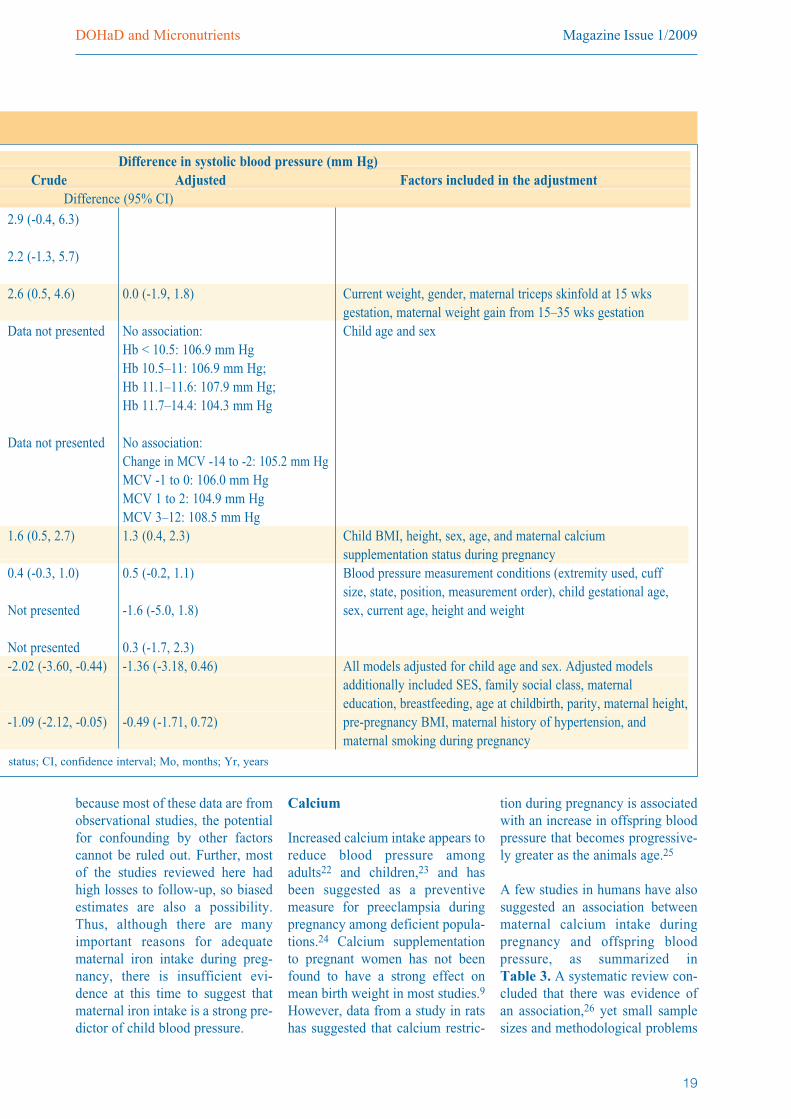
Some epidemiologic studies have noted a small nega-tive association between child blood pressure andmaternal iron intake or hemoglobin concentration dur-ing pregnancy, while others have observed either noassociation or a positive association. These studies aresummarized in Table 1. Two studies of 4-year-old15
and 9–11-year-old16 British children found no signifi-cant association between maternal hemoglobin con-centration and child blood pressure.
In a small study from Kingston, Jamaica, following77 children through 10–12 years of age, each g/dL fallin maternal hemoglobin during pregnancy was associ-ated with a rise in mean systolic blood pressure of2.6 mm Hg (95% CI: 0.5, 4.6), but this effect disap-peared after adjusting for the mother’s triceps skinfoldthickness during pregnancy.17 In this study, maternalskinfold thickness at 15 weeks gestation was stronglyinversely associated with child blood pressure, with anincrease of 10.7 mm Hg (95% CI: 5.8, 15.5) in systolicblood pressure for each log mm decrease in skinfoldthickness.17 Therefore, it is likely that overall maternalnutritional status played a much more important rolethan anemia alone in predicting the child’s blood pres-sure.
In contrast, a study of 518 5–9-year-old children fromArgentina noted an increase of 1.6 mm Hg (95% CI:0.5, 2.7) in child systolic blood pressure with eachstandard deviation increase in maternal hemoglobin
concentration during pregnancy.18 A study ofAmerican 3-year-old children was unable to documentany association between maternal hemoglobin concen-tration or mean corpuscular volume during pregnancy
and child blood pressure.19 However, less than 3% ofthe women involved in the study were anemic duringpregnancy, so the authors argue that more extreme irondeficiency may be needed for measurable effects tooccur.
Finally, a recent study of 7-year-old children in the UKconcluded that child systolic blood pressure was asso-ciated with maternal anemia during the first or secondtrimester (-2.0 mm Hg; 95% CI -3.6, -0.4) and thirdtrimester anemia (-1.1 mm Hg; 95% CI -2.1, -0.1), butthe effect was attenuated after adjustment for house-hold (social economic status), breastfeeding, maternalage at pregnancy, education, parity, height, pre-preg-nancy BMI, history of hypertension and smoking.20
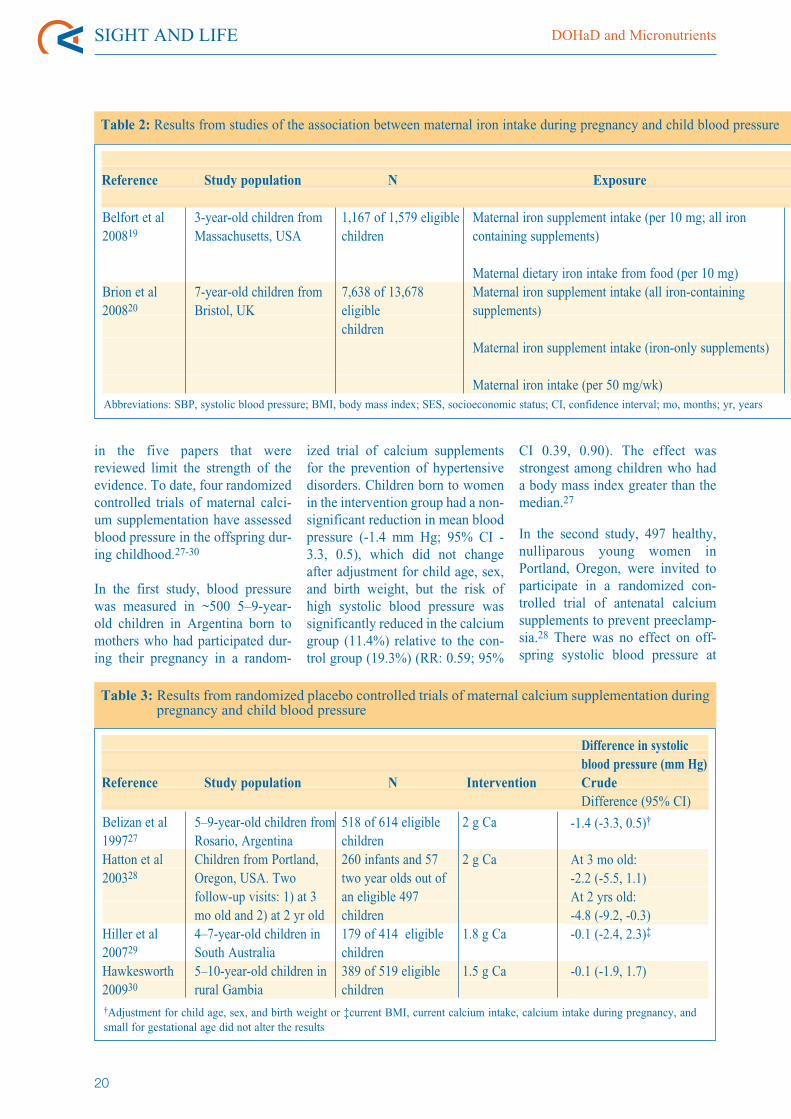
A few of these studies have also examined maternaliron intake during pregnancy, as summarized inTable 2. Among 3-year-old American children,systolic blood pressure increased by 0.4 mm Hg (95%CI: 0.1, 0.7) for every 10 mg increase in maternal firsttrimester iron intake, but was not associated withsecond trimester iron intake.19 In contrast to this study,maternal iron supplement usage was found to beinversely associated with child blood pressure among7-year-old British children.20 However, when restrict-ed to iron-only supplements, this association dis-appeared after adjustment for confounding factors,including household SES, breastfeeding, and maternalfactors during pregnancy. Similarly, maternal dietaryiron intake was unassociated with child blood pressure
Blood pressure measurement of a boy in Nepal

SIGHT AND LIFE DOHaD and Micronutrients
18
Reference Study population N Exposure
Table 1: Results from studies of the association between maternal anemia during pregnancy and child blood pressure
Law et al199115
Godfrey et al199417
Whincup et al199416
Bergel et al200018
Belfort et al200819
Brion et al200820
4-year-old children fromSalisbury, UK
10–12-year-old childrenfrom Kingston, Jamaica9–11-year-old childrenfrom Carlisle, UK
5–9 year old children fromRosario, Argentina3-year-old children fromMassachusetts, USA
7-year-old children fromBristol, UK
405 of 638 eligiblesingleton children
77 of 112 eligiblesingleton children390 of 667 eligiblechildren
518 of 614 eligiblechildren1,167 of 1,579 eligiblechildren
1,255 of 2,500 eligiblesingleton children
Maternal anemia (Hb < 100 g/L) in pregnancy
Maternal mean corpuscular volume (MCV) inpregnancy < 80 flMaternal lowest Hb concentration in pregnancy(per 1g/dL decrease)Maternal lowest Hb concentration categoryduring pregnancy
Change in MCV during pregnancy
Maternal Hb during pregnancy (per 1 SDincrease; SD = 0.79)Maternal Hb during 1st trimester (per g/dL)
Maternal anemia in 1st trimester (< 11 g/dL)
Maternal anemia in 2nd trimester (< 10.5 g/dL)Maternal anemia in the 1st or 2nd trimester(Hb < 11 g/dL)
Maternal anemia in the third trimester (Hb < 11 g/dL)
after controlling for potential con-founders.20
It is possible that other componentsof the multivitamin supplementsmay have had a greater effect onchild blood pressure than ironalone. Our group has conducted arandomized controlled trial ofmaternal micronutrient supple-ments in rural Nepal21 and haverecently completed a follow-upwith ~94% of the survivingoffspring between the ages of
6–8 years. We did not observe anyeffect of maternal iron-folic acidsupplementation on mean childblood pressure, risk of hyperten-sion, or insulin resistance relativeto the controls.42 To our knowl-edge, this is the first study that hasexamined maternal iron supple-mentation in a developing countrysetting and the only one to have uti-lized a randomized controlled trialdesign.
Although there is a strong sugges-tion from animal studies that irondeficiency during fetal develop-ment may program later hyperten-sion, the evidence from humanstudies is inconsistent. Most of thestudies have been conductedamong developed country popula-tions or among women in urbanclinic settings, so it is possible thatfew of the women experienced alevel of deficiency that was greatenough to produce adverse effectsin the offspring. Additionally,
Abbreviations: Hb, hemoglobin; MCV, mean corpuscular volume; SBP, systolic blood pressure; BMI, body mass index; SES, socioeconomic
Magazine Issue 1/2009DOHaD and Micronutrients
19
Difference in systolic blood pressure (mm Hg)Crude Adjusted Factors included in the adjustment
Difference (95% CI)
2.9 (-0.4, 6.3)
2.2 (-1.3, 5.7)
2.6 (0.5, 4.6)
Data not presented
Data not presented
1.6 (0.5, 2.7)
0.4 (-0.3, 1.0)
Not presented
Not presented-2.02 (-3.60, -0.44)
-1.09 (-2.12, -0.05)
0.0 (-1.9, 1.8)
No association:Hb < 10.5: 106.9 mm HgHb 10.5–11: 106.9 mm Hg;Hb 11.1–11.6: 107.9 mm Hg;Hb 11.7–14.4: 104.3 mm Hg
No association:Change in MCV -14 to -2: 105.2 mm HgMCV -1 to 0: 106.0 mm HgMCV 1 to 2: 104.9 mm HgMCV 3–12: 108.5 mm Hg1.3 (0.4, 2.3)
0.5 (-0.2, 1.1)
-1.6 (-5.0, 1.8)
0.3 (-1.7, 2.3)-1.36 (-3.18, 0.46)
-0.49 (-1.71, 0.72)
Current weight, gender, maternal triceps skinfold at 15 wksgestation, maternal weight gain from 15–35 wks gestationChild age and sex
Child BMI, height, sex, age, and maternal calciumsupplementation status during pregnancyBlood pressure measurement conditions (extremity used, cuffsize, state, position, measurement order), child gestational age,sex, current age, height and weight
All models adjusted for child age and sex. Adjusted modelsadditionally included SES, family social class, maternaleducation, breastfeeding, age at childbirth, parity, maternal height,pre-pregnancy BMI, maternal history of hypertension, andmaternal smoking during pregnancy
because most of these data are fromobservational studies, the potentialfor confounding by other factorscannot be ruled out. Further, mostof the studies reviewed here hadhigh losses to follow-up, so biasedestimates are also a possibility.Thus, although there are manyimportant reasons for adequatematernal iron intake during preg-nancy, there is insufficient evi-dence at this time to suggest thatmaternal iron intake is a strong pre-dictor of child blood pressure.
Calcium
Increased calcium intake appears toreduce blood pressure amongadults22 and children,23 and hasbeen suggested as a preventivemeasure for preeclampsia duringpregnancy among deficient popula-tions.24 Calcium supplementationto pregnant women has not beenfound to have a strong effect onmean birth weight in most studies.9
However, data from a study in ratshas suggested that calcium restric-
tion during pregnancy is associatedwith an increase in offspring bloodpressure that becomes progressive-ly greater as the animals age.25
A few studies in humans have alsosuggested an association betweenmaternal calcium intake duringpregnancy and offspring bloodpressure, as summarized inTable 3. A systematic review con-cluded that there was evidence ofan association,26 yet small samplesizes and methodological problems
status; CI, confidence interval; Mo, months; Yr, years
SIGHT AND LIFE DOHaD and Micronutrients
20
in the five papers that werereviewed limit the strength of theevidence. To date, four randomizedcontrolled trials of maternal calci-um supplementation have assessedblood pressure in the offspring dur-ing childhood.27-30
In the first study, blood pressurewas measured in ~500 5–9-year-old children in Argentina born tomothers who had participated dur-ing their pregnancy in a random-
ized trial of calcium supplementsfor the prevention of hypertensivedisorders. Children born to womenin the intervention group had a non-significant reduction in mean bloodpressure (-1.4 mm Hg; 95% CI -3.3, 0.5), which did not changeafter adjustment for child age, sex,and birth weight, but the risk ofhigh systolic blood pressure wassignificantly reduced in the calciumgroup (11.4%) relative to the con-trol group (19.3%) (RR: 0.59; 95%
CI 0.39, 0.90). The effect wasstrongest among children who hada body mass index greater than themedian.27
In the second study, 497 healthy,nulliparous young women inPortland, Oregon, were invited toparticipate in a randomized con-trolled trial of antenatal calciumsupplements to prevent preeclamp-sia.28 There was no effect on off-spring systolic blood pressure at
Reference Study population N Exposure
Table 2: Results from studies of the association between maternal iron intake during pregnancy and child blood pressure
Belfort et al200819
Brion et al200820
3-year-old children fromMassachusetts, USA
7-year-old children fromBristol, UK
1,167 of 1,579 eligiblechildren
7,638 of 13,678eligiblechildren
Maternal iron supplement intake (per 10 mg; all ironcontaining supplements)
Maternal dietary iron intake from food (per 10 mg)Maternal iron supplement intake (all iron-containingsupplements)
Maternal iron supplement intake (iron-only supplements)
Maternal iron intake (per 50 mg/wk)Abbreviations: SBP, systolic blood pressure; BMI, body mass index; SES, socioeconomic status; CI, confidence interval; mo, months; yr, years
Difference in systolicblood pressure (mm Hg)
Reference Study population N Intervention CrudeDifference (95% CI)
Table 3: Results from randomized placebo controlled trials of maternal calcium supplementation duringpregnancy and child blood pressure
Belizan et al199727
Hatton et al200328
Hiller et al200729
Hawkesworth200930
5–9-year-old children fromRosario, ArgentinaChildren from Portland,Oregon, USA. Twofollow-up visits: 1) at 3mo old and 2) at 2 yr old4–7-year-old children inSouth Australia5–10-year-old children inrural Gambia
518 of 614 eligiblechildren260 infants and 57two year olds out ofan eligible 497children179 of 414 eligiblechildren389 of 519 eligiblechildren
2 g Ca
2 g Ca
1.8 g Ca
1.5 g Ca
-1.4 (-3.3, 0.5)†
At 3 mo old:-2.2 (-5.5, 1.1)At 2 yrs old:-4.8 (-9.2, -0.3)-0.1 (-2.4, 2.3)‡
-0.1 (-1.9, 1.7)
†Adjustment for child age, sex, and birth weight or ‡current BMI, current calcium intake, calcium intake during pregnancy, andsmall for gestational age did not alter the results
Magazine Issue 1/2009DOHaD and Micronutrients
21
3 months of age (-2.2 mm Hg; 95% CI -5.5, 1.1), but asignificant 4.8 mm Hg reduction (95% CI -9.2, -0.3) at2 years of age in the calcium group compared to thecontrols. However, the losses to follow-up weresubstantial; only 260 infants and 57 toddlers weremeasured at follow-up.28 Data were not presented onthe differences between participants and non-partici-pants, and no attempts were made to control for poten-tial differential losses to follow-up, so the potential forbias or confounding cannot be ruled out.
A third study conducted among 456 nulliparouswomen in South Australia found that maternal calciumsupplementation had no overall effect on offspringblood pressure at 4–7 years of age.29 Finally, recentdata from a study of 5–10-year-old offspring of
mothers who participated in a randomized controlledtrial of calcium supplementation during pregnancy inthe Gambia found no impact of supplementation onchild blood pressure, although the full results of thisstudy have yet to be published.30
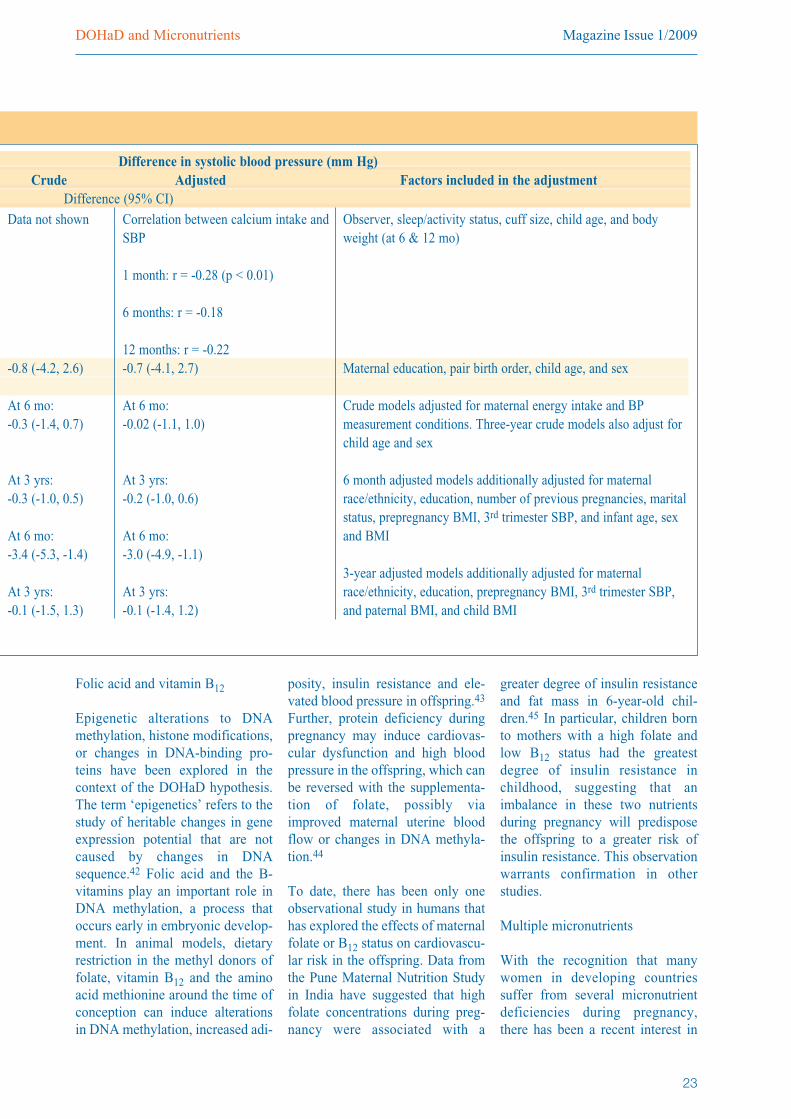
Observational data have provided mixed results, andare summarized in Table 4. Maternal calcium intakeduring pregnancy has been inversely associated withsystolic blood pressure in children at 1 month of age(r = -0.28, p < 0.01) and diastolic blood pressure at 6(r = -0.27, p < 0.01) and 12 months of age (r = -0.24, p< 0.05).31 It should be noted however that, in thisAmerican study population, more than 85% of womenconsumed amounts of calcium in excess of 1,200mg/day.
In a more recent study of pregnant women and theirchildren in Massachusetts, maternal calcium intakeduring pregnancy has been inversely associated withoffspring blood pressure at 6 months of age with anestimated 3.0 mm Hg reduction (95% CI: -4.9, -1.1) insystolic blood pressure per every 500 mg increment inmaternal supplemental calcium consumed.32 Theeffect was confined to calcium consumed in the formof supplements but not from food sources.32 However,this effect was not maintained through the age of3 years.33
Finally, one small study of twin pairs from Tasmaniafound that, at 9 years of age, children whose mothersreported taking supplemental calcium during pregnan-cy had lower levels of total and LDL cholesterol, lowertriglycerides, but no difference in blood pressure, fast-ing glucose, insulin, or HDL cholesterol.34 It is unfor-
Difference in systolic blood pressure (mm Hg)Crude Adjusted Factors included in the adjustment
Difference (95% CI)0.4 (0.1, 0.7)
-0.1 (-1.0, 0.9)-0.72 (-1.14, -0.31)
-1.03 (-2.28, 0.22)
-0.41 (-1.12, 0.30)
0.4 (0.1, 0.8)
0.2 (-0.8, 1.2)-0.58 (-1.06, -0.10)
-0.19 (-1.58, 1.20)
0.40 (-0.45, 1.26)
Blood pressure measurement conditions (extremity used, cuffsize, state, position, measurement order), child gestational age,sex, current age, height and weight
All models adjusted for child age and sex. Adjusted modelsadditionally included SES, family social class, maternaleducation, breastfeeding, age at childbirth, parity, maternal height,pre-pregnancy BMI, maternal history of hypertension, andmaternal smoking during pregnancy
Home-based blood pressure measurement inrural Nepal
SIGHT AND LIFE DOHaD and Micronutrients
22
tunate that in this study, the dosageof supplementation is unknown andother dietary factors during preg-nancy were not assessed. Further, itis unclear how these data fromtwins can be generalized to single-ton pregnancies.
In conclusion, there is little evi-dence of an association betweenmaternal calcium intake and off-spring blood pressure. The studiesamong humans, both randomizedcontrolled trials and observationalstudies, have not yielded strong orconsistent results. However, largelosses to follow-up and othermethodologic considerations limitthe ability to draw firm conclu-sions.
Other micronutrients
Vitamin A
Studies of vitamin A-deficient rats35
or retinoic acid receptor knockoutmice36 have demonstrated the essen-tial role that vitamin A plays innumerous aspects of fetal pul-monary, renal, and cardiac morpho-logical development. Moderate vita-min A deficiency will result inreductions in the relative weight offetal lungs, heart and liver,37 kidneydevelopment,38 and pancreatic dev-elopment39. However, there have notyet been any published studies inhumans that have explored theeffects of vitamin A deficiency dur-ing pregnancy on these long-termoutcomes in the offspring.
Zinc
A recent review suggested that zincmay play an important role in thefetal origins of disease through epi-genetic mechanisms.40 However,only one study utilizing a rat modelfound that moderate maternal zincdeficiency results in elevations inoffspring blood pressure, a reduc-tion in the number and size ofnephrons, a decrease in theglomerular filtration rate and anincrease in renal oxidative damage.The damage could not be overcomeby returning rats to the control diet,post-weaning.41 More research isneeded to better understand theeffects of maternal zinc status dur-ing pregnancy on long term chron-ic disease risk in the children.
Reference Study population N Exposure
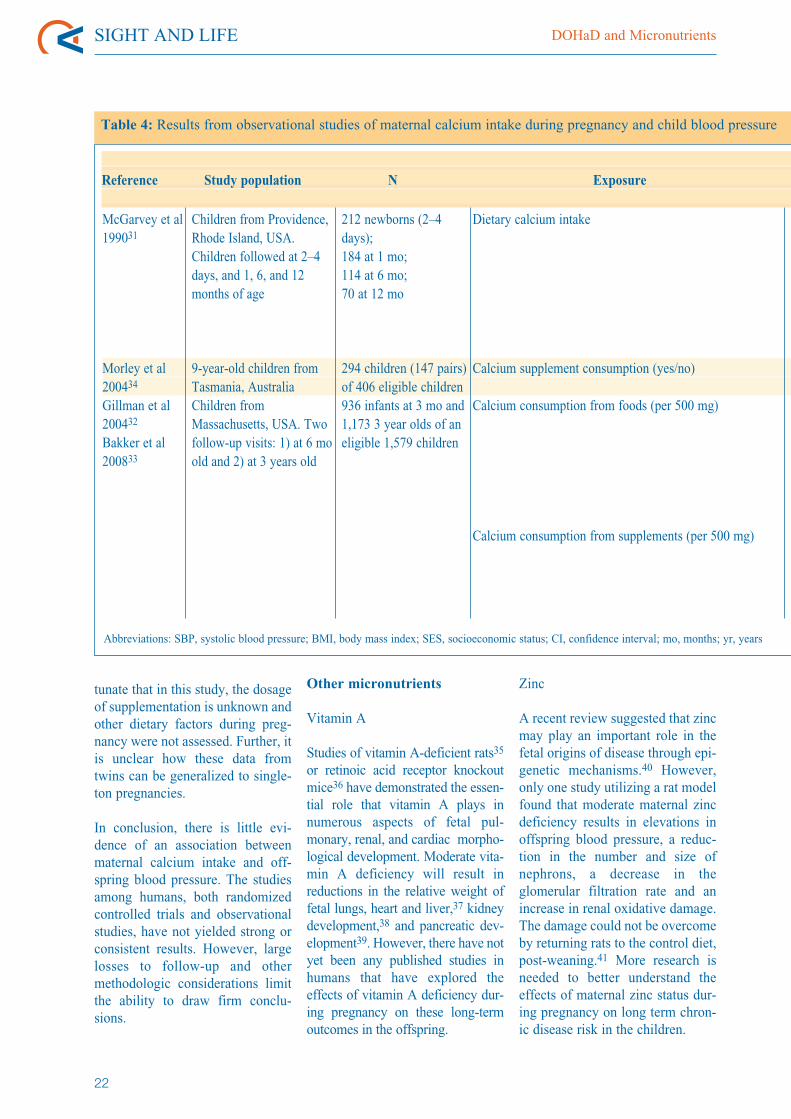
Table 4: Results from observational studies of maternal calcium intake during pregnancy and child blood pressure
McGarvey et al199031
Morley et al200434
Gillman et al200432
Bakker et al200833
Children from Providence,Rhode Island, USA.Children followed at 2–4days, and 1, 6, and 12months of age
9-year-old children fromTasmania, AustraliaChildren fromMassachusetts, USA. Twofollow-up visits: 1) at 6 moold and 2) at 3 years old
212 newborns (2–4days);184 at 1 mo;114 at 6 mo;70 at 12 mo
294 children (147 pairs)of 406 eligible children936 infants at 3 mo and1,173 3 year olds of aneligible 1,579 children
Dietary calcium intake
Calcium supplement consumption (yes/no)
Calcium consumption from foods (per 500 mg)
Calcium consumption from supplements (per 500 mg)
Abbreviations: SBP, systolic blood pressure; BMI, body mass index; SES, socioeconomic status; CI, confidence interval; mo, months; yr, years
Magazine Issue 1/2009DOHaD and Micronutrients
23
Folic acid and vitamin B12
Epigenetic alterations to DNAmethylation, histone modifications,or changes in DNA-binding pro-teins have been explored in thecontext of the DOHaD hypothesis.The term ‘epigenetics’ refers to thestudy of heritable changes in geneexpression potential that are notcaused by changes in DNAsequence.42 Folic acid and the B-vitamins play an important role inDNA methylation, a process thatoccurs early in embryonic develop-ment. In animal models, dietaryrestriction in the methyl donors offolate, vitamin B12 and the aminoacid methionine around the time ofconception can induce alterationsin DNA methylation, increased adi-
posity, insulin resistance and ele-vated blood pressure in offspring.43
Further, protein deficiency duringpregnancy may induce cardiovas-cular dysfunction and high bloodpressure in the offspring, which canbe reversed with the supplementa-tion of folate, possibly viaimproved maternal uterine bloodflow or changes in DNA methyla-tion.44
To date, there has been only oneobservational study in humans thathas explored the effects of maternalfolate or B12 status on cardiovascu-lar risk in the offspring. Data fromthe Pune Maternal Nutrition Studyin India have suggested that highfolate concentrations during preg-nancy were associated with a
greater degree of insulin resistanceand fat mass in 6-year-old chil-dren.45 In particular, children bornto mothers with a high folate andlow B12 status had the greatestdegree of insulin resistance inchildhood, suggesting that animbalance in these two nutrientsduring pregnancy will predisposethe offspring to a greater risk ofinsulin resistance. This observationwarrants confirmation in otherstudies.
Multiple micronutrients
With the recognition that manywomen in developing countriessuffer from several micronutrientdeficiencies during pregnancy,there has been a recent interest in
Difference in systolic blood pressure (mm Hg)Crude Adjusted Factors included in the adjustment
Difference (95% CI)
Data not shown
-0.8 (-4.2, 2.6)
At 6 mo:-0.3 (-1.4, 0.7)
At 3 yrs:-0.3 (-1.0, 0.5)
At 6 mo:-3.4 (-5.3, -1.4)
At 3 yrs:-0.1 (-1.5, 1.3)
Correlation between calcium intake andSBP
1 month: r = -0.28 (p < 0.01)
6 months: r = -0.18
12 months: r = -0.22-0.7 (-4.1, 2.7)
At 6 mo:-0.02 (-1.1, 1.0)
At 3 yrs:-0.2 (-1.0, 0.6)
At 6 mo:-3.0 (-4.9, -1.1)
At 3 yrs:-0.1 (-1.4, 1.2)
Observer, sleep/activity status, cuff size, child age, and bodyweight (at 6 & 12 mo)
Maternal education, pair birth order, child age, and sex
Crude models adjusted for maternal energy intake and BPmeasurement conditions. Three-year crude models also adjust forchild age and sex
6 month adjusted models additionally adjusted for maternalrace/ethnicity, education, number of previous pregnancies, maritalstatus, prepregnancy BMI, 3rd trimester SBP, and infant age, sexand BMI
3-year adjusted models additionally adjusted for maternalrace/ethnicity, education, prepregnancy BMI, 3rd trimester SBP,and paternal BMI, and child BMI

SIGHT AND LIFE DOHaD and Micronutrients
24
studying the potential benefits thatsupplementation with multiplemicronutrients may have for themother and child.10 However, todate, only one study has publisheddata on the effects of maternal sup-plementation on the health of theoffspring beyond infancy. Thisstudy, conducted in Janakpur,Nepal, followed 2–3-year-old chil-dren born to mothers enrolled in arandomized controlled trial of amultiple micronutrient supplement,containing 15 micronutrients, com-pared to iron-folic acid as the con-trol. Children whose mothers hadreceived the multiple micronutrientsupplement had a reduction in sys-tolic blood pressure of 2.5 mm Hg(95% CI: 0.5, 4.6) relative to thecontrols.46 In contrast, in a similarpopulation in rural Nepal, childrenaged 6–8 years whose mothers hadbeen enrolled in a randomized con-trolled trial of multiple micronutri-ents had no difference in bloodpressure relative to controls(Stewart CP, Christian PC, SchulzeKJ, LeClerq SC, West KP, andKhatry SK, unpublished).
Conclusions
While there is strong evidence fromanimal studies that micronutrientdeficiency during fetal develop-ment may have consequences wellbeyond the neonatal period, there ismuch to be learned in terms ofunderstanding the effects inhumans as well as the potentialmechanisms of action. Data onlong term cardiovascular risk fromhuman studies is equivocal or lack-ing for many micronutrients. Muchof the literature that does existcomes from observational data,which may suffer from confound-ing due to both measured andunmeasured factors. Further, themajority of studies have followed-up with subjects as children or ado-lescents, which may be too youngto demonstrate measurable effects.
Micronutrient deficiencies areprevalent in women from both thedeveloped and the developingworlds, but the full consequencesof these deficiencies have yet to befully understood. While there havebeen many randomized trials thathave explored the short-termeffects of micronutrient supple-mentation on birth weight, infantgrowth, and morbidity, much couldbe gained by following these chil-dren forward in time to determinewhat, if any, are the latent benefitsof supplementation.
Acknowledgement:
The author was supported under aProctor and Gamble doctoral fel-lowship and received additionalsupport from the Bill and MelindaGates Foundation, the UnitedStates Agency for InternationalDevelopment (USAID), and theSight and Life Institute. She wouldlike to thank her collaborators inNepal and at Johns HopkinsUniversity for their support of thiswork, including Parul Christian,Keith P. West, Jr., Kerry Schulze,James Tielsch, Joanne Katz, StevenLeClerq and Subarna Khatry. Shewould also like to thank SuchetaMehra for her valuable input duringthe preparation of this manuscript.
References
1. Sanghvi T, Van Ameringen M, BakerJ, Fiedler J, Borwankar R, Phillips M,et al. Vitamin and mineral deficien-cies technical situation analysis: areport for the Ten Year Strategyfor the Reduction of Vitamin andMineral Deficiencies. Food NutrBull 2007;28(1 Suppl Vitamin):S160–219.
2. WHO. Preventing Chronic Disease:A vital investment: A WHO globalreport. Geneva, Switzerland: WorldHealth Organization; 2005.
3. WHO/FAO. Diet, Nutrition and thePrevention of Chronic Diseases:Report of a Joint WHO/FAO ExpertConsultation. 2003;916.
4. Doak CM, Adair LS, Monteiro C,Popkin BM. Overweight and under-weight coexist within households inBrazil, China and Russia. J Nutr2000;130(12):2965–71.5. Hales CN, Barker DJ. The thriftyphenotype hypothesis. Br Med Bull2001;60:5–20.
6. Gluckman PD, Cutfield W, HofmanP, and Hanson MA. The fetal, neona-tal and infant environments – thelong-term consequences for diseaserisk. Early Hum Dev 2005;81:51–9.
7. Ramakrishnan U, Manjrekar R,Rivera J, Gonzalez-Cossio T, Marto-rell R. Micronutrients and PregnancyOutcome: A Review of the Litera-ture. Nutr res 1999;19(1): 103–59.
8. Merialdi M, Carroli G, Villar J,Abalos E, Gulmezoglu AM, KulierR, et al. Nutritional interventions dur-ing pregnancy for the prevention ortreatment of impaired fetal growth:an overview of randomized con-trolled trials. J Nutr 2003;133(5Suppl 2):1626S–31S.
9. Fall CH, Yajnik CS, Rao S, DaviesAA, Brown N, Farrant HJ. Micro-nutrients and fetal growth. J Nutr2003;133(5 Suppl 2):1747S–56S.
10. Haider BA, Bhutta ZA. Multiple-micronutrient supplementation forwomen during pregnancy. CochraneDatabase Syst Rev 2006;(4) (4):CD004905.
11. McMillen IC, Robinson JS. Develop-mental origins of the metabolic syn-drome: prediction, plasticity, andprogramming. Physiol Rev 2005;85(2):571–633.
12. World Health Organization. IronDeficiency Anemia Assessment,Prevention and Control: A guidefor program managers. 2001;WHO/NHD/01.3:132.
13. Gambling L, Dunford S, Wallace DI,Zuur G, Solanky N, Srai SK, et al.Iron deficiency during pregnancyaffects postnatal blood pressure in therat. J Physiol 2003;552(Pt 2):603–10.
14. Andersen HS, Gambling L, HoltropG, McArdle HJ. Maternal iron defi-ciency identifies critical windows forgrowth and cardiovascular develop-ment in the rat postimplantationembryo. J Nutr 2006;136(5):1171–7.
15. Law CM, Barker DJ, Bull AR,Osmond C. Maternal and fetal influ-ences on blood pressure. Arch DisChild 1991;66(11):1291–5.
16. Whincup P, Cook D, Papacosta O,Walker M, Perry I. Maternal factorsand development of cardiovascularrisk: evidence from a study of blood
Magazine Issue 1/2009DOHaD and Micronutrients
25
pressure in children. J Hum Hy-pertens 1994;8(5):337–43.
17. Godfrey KM, Forrester T, Barker DJ,Jackson AA, Landman JP, Hall JS, etal. Maternal nutritional status inpregnancy and blood pressure inchildhood. Br J Obstet Gynaecol1994;101(5):398–403.
18. Bergel E, Haelterman E, Belizan J,Villar J, Carroli G. Perinatal factorsassociated with blood pressure duringchildhood. Am J Epidemiol 2000Mar;151(6):594–601.
19. Belfort MB, Rifas-Shiman SL, Rich-Edwards JW, Kleinman KP, Oken E,Gillman MW. Maternal iron intakeand iron status during pregnancy andchild blood pressure at age 3 years.Int J Epidemiol 2008;37(2):301–8.
20. Brion MJ, Leary SD, Smith GD,McArdle HJ, Ness AR. Maternal ane-mia, iron intake in pregnancy, andoffspring blood pressure in the AvonLongitudinal Study of Parents andChildren. Am J Clin Nutr 2008;88(4):1126–33.
21. Christian P, Khatry SK, Katz J,Pradhan EK, LeClerq SC, ShresthaSR, et al. Effects of alternative mater-nal micronutrient supplements onlow birth weight in rural Nepal: dou-ble blind randomised communitytrial. BMJ 2003;326(7389):571.
22. van Mierlo LA, Arends LR, StreppelMT, Zeegers MP, Kok FJ, GrobbeeDE, et al. Blood pressure response tocalcium supplementation: a meta-analysis of randomized controlled tri-als. J Hum Hypertens 2006;20(8):571–80.
23. Gillman MW, Oliveria SA, MooreLL, Ellison RC. Inverse associationof dietary calcium with systolic bloodpressure in young children. JAMA1992;267(17):2340–3.
24. Villar J, Belizan JM. Same nutrient,different hypotheses: disparities intrials of calcium supplementationduring pregnancy. Am J Clin Nutr2000;71(5 Suppl):1375S–9S.
25. Bergel E, Belizan JM. A deficientmaternal calcium intake during preg-nancy increases blood pressure ofthe offspring in adult rats. BJOG2002;109(5):540–5.
26. Bergel E, Barros AJ. Effect of mater-nal calcium intake during pregnancyon children's blood pressure: a sys-tematic review of the literature. BMCPediatr 2007;7:15.
27. Belizan JM, Villar J, Bergel E, delPino A, Di Fulvio S, Galliano SV, etal. Long-term effect of calcium sup-plementation during pregnancy on
the blood pressure of offspring: fol-low up of a randomised controlledtrial. BMJ 1997;315(7103):281–5.
28. Hatton DC, Harrison-Hohner J, CosteS, Reller M, McCarron D. Gesta-tional calcium supplementation andblood pressure in the offspring. Am JHypertens 2003;16(10):801–5.
29. Hiller JE, Crowther CA, Moore VA,Willson K, Robinson JS. Calciumsupplementation in pregnancy and itsimpact on blood pressure in childrenand women: follow up of a ran-domised controlled trial. Aust N Z JObstet Gynaecol 2007;47(2):115–21.
30. Hawkesworth S. Conference on"Multidisciplinary approaches tonutritional problems". PostgraduateSymposium. Exploiting dietary sup-plementation trials to assess theimpact of the prenatal environmenton CVD risk. Proc Nutr Soc 2009;68(1):78–88.
31. McGarvey ST, Zinner SH, WillettWC, Rosner B. Maternal prenataldietary potassium, calcium, magne-sium, and infant blood pressure.Hypertension 1991;17(2):218–24.
32. Gillman MW, Rifas-Shiman SL,Kleinman KP, Rich-Edwards JW,Lipshultz SE. Maternal calciumintake and offspring blood pressure.Circulation 2004;110(14):1990–5.
33. Bakker R, Rifas-Shiman SL, Klein-man KP, Lipshultz SE, Gillman MW.Maternal Calcium Intake DuringPregnancy and Blood Pressure inthe Offspring at Age 3 Years: AFollow-up Analysis of the ProjectViva Cohort. Am J Epidemiol2008;168(12):1374–80.
34. Morley R, Carlin JB, Dwyer T.Maternal calcium supplementa-tion and cardiovascular risk fac-tors in twin offspring. Int J Epi-demiol;33(6):1304–9.
35. Antipatis C, Grant G, Ashworth CJ.Moderate maternal vitamin A defi-ciency affects perinatal organ growthand development in rats. Br J Nutr2000;84(1):125–32.
36. Mendelsohn C, Lohnes D, DecimoD, Lufkin T, LeMeur M, Chambon P,et al. Function of the retinoic acidreceptors (RARs) during develop-ment (II). Multiple abnormalities atvarious stages of organogenesis inRAR double mutants. Development1994;120(10):2749–71.
37. Ashworth CJ, Antipatis C. Micro-nutrient programming of develop-ment throughout gestation. Repro-duction 2001;122(4):527–35.
38. Bhat PV, Manolescu DC. Roleof vitamin A in determining nephronmass and possible relationshipto hypertension. J Nutr 2008;138(8):1407–10.
39. Matthews KA, Rhoten WB, DriscollHK, Chertow BS. Vitamin A defi-ciency impairs fetal islet develop-ment and causes subsequent glucoseintolerance in adult rats. J Nutr2004;134(8):1958–63.
40. Maret W, Sandstead HH. Possibleroles of zinc nutriture in the fetalorigins of disease. Exp Gerontol2008;43(5):378–81.
41. Tomat AL, Inserra F, Veiras L,Vallone MC, Balaszczuk AM, CostaMA, et al. Moderate zinc restrictionduring fetal and postnatal growth ofrats: effects on adult arterial bloodpressure and kidney. Am J PhysiolRegul Integr Comp Physiol 2008;295(2):R543–9.
42. Stewart CP, Christian P, Schulze KJ,LeClerq SC, West KP and KhatrySK, unpublished.
43. Sinclair KD, Allegrucci C, Singh R,Gardner DS, Sebastian S, Bispham J,et al. DNA methylation, insulinresistance, and blood pressure in off-spring determined by maternal peri-conceptional B vitamin and methion-ine status. Proc Natl Acad Sci U S A2007;104(49):19351–6.
44. Torrens C, Brawley L, Anthony FW,Dance CS, Dunn R, Jackson AA, etal. Folate supplementation duringpregnancy improves offspring car-diovascular dysfunction induced byprotein restriction. Hypertension2006;47(5):982–7.
45. Yajnik CS, Deshpande SS, JacksonAA, Refsum H, Rao S, Fisher DJ, etal. Vitamin B(12) and folate concen-trations during pregnancy and insulinresistance in the offspring: the PuneMaternal Nutrition Study. Diabeto-logia 2008;51(1):29–38.
46. Vaidya A, Saville N, Shrestha BP, deL Costello AM, Manandhar DS,Osrin D. Effects of antenatal multiplemicronutrient supplementation onchildren's weight and size at 2 yearsof age in Nepal: follow-up of a dou-ble-blind randomised controlled trial.Lancet 2008;371:492–9.

SIGHT AND LIFE Zinc Intervention Strategies
26
Introduction
Adequate zinc nutrition is critically important for chil-dren’s health and the achievement of their full growthpotential. The Lancet series on maternal and childundernutrition concluded that zinc deficiency increas-es the risk and severity of common childhood infec-tions, thereby contributing to excess morbidity andmortality in lower income countries,1 and the recentlyupdated Copenhagen Consensus on priorities foradvancing global welfare named zinc supplementationas one of the top-ranked interven-tions for reducing malnutritionand improving overall welfare2.Despite these compelling conclu-sions, there has been surprisinglylittle effort worldwide focused onthe prevention of zinc deficiency,in part because of the limited infor-mation that has been synthesized toassess the impact of different zincintervention strategies on childhealth outcomes.
To address this information gap,the Steering Committee of theInternational Zinc Nutrition Con-sultative Group (IZiNCG) has justcompleted a 2nd IZiNCG technicaldocument, which compiles andsystematically examines informa-
tion on the intervention strategies that have beendeveloped to control zinc deficiency. The documentwas published in the Food and Nutrition Bulletin(Food Nutr Bull 2009;30(1):S3–S186) and can bedownloaded for free at:h t t p : / /www . f oodandnu t r i t i o nbu l l e t i n . o r g /downloads/FNB_v30n1_Supplement_izinc.pdf andwww.izincg.org.
Separate chapters of the new IZiNCG technical docu-ment present the latest information on the expected
health and nutrition results that canbe achieved through zinc supple-mentation, fortification, and diet-based intervention strategies. Thechapter on preventive supplementa-tion includes meta-analyses of itsimpact on morbidity, mortality,growth and zinc status amonginfants and children,3 based on theresults of 55 intervention trials inwhich the effects of zinc supple-ments, with or without othermicronutrients, were comparedwith the results obtained from thesame preparations when zinc wasexcluded. The section on therapeu-tic zinc supplementation examinedthe severity and duration of select-ed infections, such as diarrhea,pneumonia, and malaria,4 in rela-
Systematic Reviews of ZincIntervention StrategiesA Technical Summary from the International ZincNutrition Consultative Group (IZiNCG)
Sonja Y. Hess1, Kenneth H. Brown1,21Department of Nutrition, University of California, Davis,California, USA2Helen Keller International, Dakar, Senegal
Correspondence: Sonja Y. Hess, Program in International andCommunity Nutrition, Department of Nutrition, University ofCalifornia, One Shields Avenue, Davis, CA, 95616, USAEmail: [email protected]
Special issue of the Food andNutrition Bulletin
SIGHT AND LIFE Magazine 2009;1:26–28

Magazine Issue 1/2009Zinc Intervention Strategies
27
tion to whether or not zinc supplements were includedin the treatment regimen. The document also systemat-ically reviews current evidence on the effects of zincsupplementation during pregnancy,5 the impact of zincfortification,6 and the results of dietary interventions toincrease zinc intake7–9.
Zinc supplementation in children
The results of available studies indicate that preventivezinc supplementation reduces the incidence of diarrheaby approximately 27% among young children aged> 12 months and decreases the incidence of acutelower respiratory tract infections by approximately15%.3 Overall, zinc supplementation reduces childmortality by approximately 6%. The impact of preven-tive zinc supplementation on child mortality seems tobe restricted to children aged > 12 months, in whomthe mortality reduction is approxi-mately 18%.
Some evidence further suggeststhat zinc supplementation mayreduce mortality among small-for-gestational-age infants, butthe number of studies is still toosmall to draw definitive conclu-sions. Preventive zinc supplemen-tation also increases linear growthand weight gain in young chil-dren, thereby contributing toreduced rates of stunting andunderweight.
Importantly, available research hasfound no evidence of adverseeffects on the status of othermicronutrients or of any functionalabnormalities when preventive zincsupplements are provided in the recommended doses.Thus, preventive zinc supplementation of children atrisk of deficiency is both safe and efficacious for avariety of health and nutritional outcomes.
The newly completed meta-analyses of therapeuticzinc supplementation confirm that provision of zincsupplements as adjunctive treatment for diarrheareduces the duration of acute episodes by ~0.5 daysand of persistent episodes by ~0.7 days.4 The resultstherefore support the recommendation by the WorldHealth Organization (WHO) and the United NationsChildren’s Fund (UNICEF) to include therapeutic zincsupplementation in diarrheal disease control pro-grams.10
Zinc supplementation during pregnancy
Preventive zinc supplementation was also examinedamong pregnant and lactating women.5 An earliermeta-analysis concluded that zinc supplementationduring pregnancy reduced the rate of preterm births by14%.11 Most studies found no significant impact ofmaternal zinc supplementation on infant birth weightbut a subset of studies conducted among underweightor zinc-deficient women suggests there may be a posi-tive effect of zinc supplementation in such women.Nevertheless, the number of relevant studies is limited,and more information is needed to confirm theseobservations. The impact of maternal zinc supplemen-tation during pregnancy on infant postnatal growth andrisk of infection is variable, and too few studies areavailable to permit reliable conclusions, especiallywith regard to longer term effects during the second
half of infancy and later childhood.
Zinc fortification
Despite the positive effect of zincfortification on total zinc absorp-tion, only a few studies have foundpositive impacts of zinc fortifica-tion on serum zinc concentrationsor functional indicators of zinc sta-tus.6 Nevertheless, because of thedesirability of increasing zincintake in populations at high riskfor zinc deficiency, the document-ed increase in total zinc absorptionthat occurs following zinc fortifica-tion, the absence of any adverseeffects of zinc fortification, and therelatively low cost of adding zinc toexisting fortification programs,public health planners should con-
sider including zinc in mass and targeted fortificationprograms in such populations. Because of the limitedavailable information on program impact, it will beimportant to evaluate the outcomes of such programs.
Dietary diversification or modification
A number of dietary intervention strategies have thepotential for improving zinc status. Breast milk is animportant potential source of zinc for infants andyoung children, and current international guidelinesfor the promotion and support of breastfeeding shouldbe viewed as appropriate programmatic components tosupport adequate zinc nutrition of young children.8
Other interventions to increase the availability, acces-
Foods rich in zinc

SIGHT AND LIFE Zinc Intervention Strategies
28
sibility, and consumption of ani-mal-source foods, increase the zinccontent of plant-source foods, orincrease zinc absorption from thesefoods should enhance the con-sumers’ zinc status.7 However, rig-orous evaluations of large-scaledietary approaches are still lacking.In the future, biofortification alsoholds promise as a sustainableapproach to improve the zinc con-tent and/or bioavailability of staplefood crops 9.
Conclusion
There is now clear evidence of thebenefit of selected interventions toreduce the risk of zinc deficiency,and a global commitment is urgent-ly needed to: 1) conduct systematicassessments of population zinc sta-tus, and 2) develop interventions tocontrol zinc deficiency in the con-text of existing public health andnutrition programs.12 Such inter-ventions, if implemented at scaleand attaining high coverage, wouldhave a direct impact on achieving
several Millennium DevelopmentGoals, including reducing childmorbidity, mortality, and restrictedgrowth.
References
1. Black RE, Allen LH, Bhutta ZA,Caulfield LE, de Onis M, Ezzati M,et al. Maternal and child undernutri-tion: global and regional exposuresand health consequences. Lancet 2008;371(9608):243–60.
2. Horton S, Alderman H, Rivera JA.Copenhagen Consensus challenge pa-per: Hunger and malnutrition. Copen-hagen Consensus Center, 2008.
3. Brown KH, Peerson JM, Baker SK,Hess SY. Preventive zinc supplementa-tion among infants, preschoolers, andolder prepubertal children. Food NutrBull 2009;30(1):S12–40.
4. Haider BA, Bhutta ZA. The effectof therapeutic zinc supplementationamong young children with selectedinfections: a review of the evidence.Food Nutr Bull 2009;30(1):S41–59.
5. Hess SY, King JC. Effects of maternalzinc supplementation on pregnancyand lactation outcomes. Food Nutr Bull2009;30(1):S60–78.
6. Hess SY, Brown KH. Impact of zincfortification on zinc nutrition. FoodNutr Bull 2009;30(1):S79–107.
7. Gibson RS, Anderson VP. A review ofinterventions based on dietary diversi-fication/modification strategies withthe potential to enhance intakes of totaland absorbable zinc. Food Nutr Bull2009;30(1):S108–43.
8. Brown KH, Engle-Stone R, Krebs NF,Peerson JM. Dietary interventionstrategies to enhance zinc nutrition:Promotion and support of breast feed-ing for infants and young children.Food Nutr Bull 2009;30(1):S144–71.
9. Hotz C. The potential to improve zincstatus through biofortification of staplefood crops with zinc. Food Nutr Bull2009;30(1):S172–8.
10. World Health Organization, UNICEF.Clinical management of acute diarrhoea.Geneva: WHO/UNICEF joint statement.WHO/FCH/CAH/04.7, 2004.
11. Mahomed K, Bhutta Z, Middleton P.Zinc supplementation for improvingpregnancy and infant outcome.Cochrane Database Syst Rev 2007(2):CD000230.
12. Brown KH, Baker SK, IZiNCGSteering Committee. Galvanizingaction: Conclusions and next steps formainstreaming zinc interventions inpublic health programs. Food Nutr Bull2009;30(1):S179–84.
DSM Nutritional Products Ltd.P.O. Box 2676, CH-4002 BaselSwitzerland
DSM – the Life Sciences and Materials Sciences CompanyRoyal DSM N.V. creates innovative products and services in Life Sciencesand Materials Sciences that contribute to the quality of life. DSM’s productsand services are used globally in a wide range of markets and applications,supporting a healthier, more sustainable and more enjoyable way of life. Endmarkets include human and animal nutrition and health, personal care,
pharmaceuticals, automotive, coatings and paint, electrics and electronics,life protection and housing. DSM has annual sales of almost EUR 9.3 billionand employs some 23,500 people worldwide. The company is headquar-tered in the Netherlands, with locations on five continents. DSM is listed onEuronext Amsterdam. More information on DSM: www.dsm.com
DSM Nutritional Products is the world’s leading supplier of vitamins,carotenoids and other fine chemicals to the feed, food, pharmaceuti-cal and personal care industries. The business has sales of overEUR 2 billion and a long tradition as a pioneer in the discovery ofnew products, new formulations and attractive applications for allindustry segments. More information about DSM Nutritional Productscan be found at www.dsmnutritionalproducts.com
SIGHT AND LIFE, aa hhuummaanniittaarriiaann iinniittiiaattiivvee ooff DDSSMM,, wwoorrkkss ttoo ccoommbbaatt aallllffoorrmmss ooff mmiiccrroonnuuttrriieenntt ddeeffiicciieennccyy bbyy wwoorrkkiinngg wwiitthh gglloobbaall aanndd llooccaall ppaarrtt--nneerrss aanndd lleeaaddiinngg uunniivveerrssiittiieess ttoo ssuussttaaiinnaabbllyy aanndd ssiiggnniiffiiccaannttllyy iimmpprroovveehhuummaann nnuuttrriittiioonn aanndd hheeaalltthh.. www.sightandlife.org
UNLIMITED RESPONSIBILITYSIGHT AND LIFE IS A HUMANITARIAN INITIATIVE OF DSM
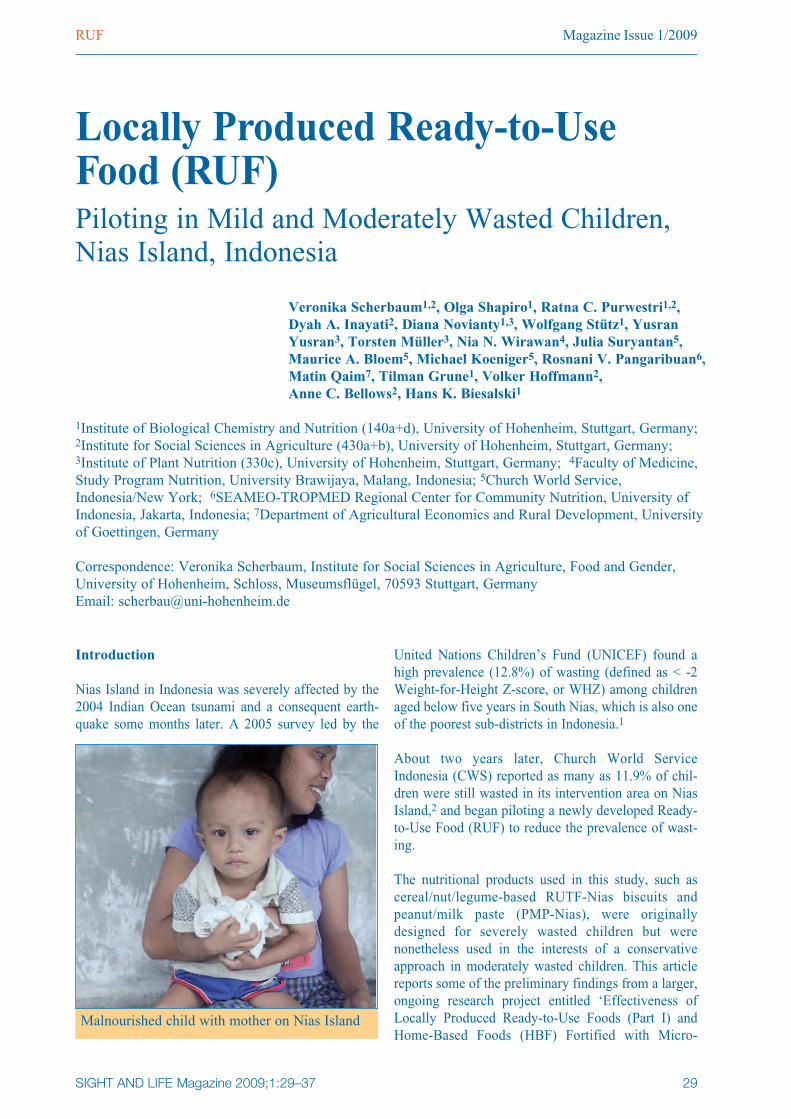
Magazine Issue 1/2009RUF
29
Introduction
Nias Island in Indonesia was severely affected by the2004 Indian Ocean tsunami and a consequent earth-quake some months later. A 2005 survey led by the
United Nations Children’s Fund (UNICEF) found ahigh prevalence (12.8%) of wasting (defined as < -2Weight-for-Height Z-score, or WHZ) among childrenaged below five years in South Nias, which is also oneof the poorest sub-districts in Indonesia.1
About two years later, Church World ServiceIndonesia (CWS) reported as many as 11.9% of chil-dren were still wasted in its intervention area on NiasIsland,2 and began piloting a newly developed Ready-to-Use Food (RUF) to reduce the prevalence of wast-ing.
The nutritional products used in this study, such ascereal/nut/legume-based RUTF-Nias biscuits andpeanut/milk paste (PMP-Nias), were originallydesigned for severely wasted children but werenonetheless used in the interests of a conservativeapproach in moderately wasted children. This articlereports some of the preliminary findings from a larger,ongoing research project entitled ‘Effec tiveness ofLocally Produced Ready-to-Use Foods (Part I) andHome-Based Foods (HBF) Fortified with Micro -
Locally Produced Ready-to-UseFood (RUF)Piloting in Mild and Moderately Wasted Children, Nias Island, Indonesia
Veronika Scherbaum1,2, Olga Shapiro1, Ratna C. Purwestri1,2, Dyah A. Inayati2, Diana Novianty1,3, Wolfgang Stütz1, YusranYusran3, Torsten Müller3, Nia N. Wirawan4, Julia Suryantan5,Maurice A. Bloem5, Michael Koeniger5, Rosnani V. Pangaribuan6,Matin Qaim7, Tilman Grune1, Volker Hoffmann2, Anne C. Bellows2, Hans K. Biesalski1
1Institute of Biological Chemistry and Nutrition (140a+d), University of Hohenheim, Stuttgart, Germany;2Institute for Social Sciences in Agriculture (430a+b), University of Hohenheim, Stuttgart, Germany;3Institute of Plant Nutrition (330c), University of Hohenheim, Stuttgart, Germany; 4Faculty of Medicine,Study Program Nutrition, University Brawijaya, Malang, Indonesia; 5Church World Service,Indonesia/New York; 6SEAMEO-TROPMED Regional Center for Community Nutrition, University ofIndonesia, Jakarta, Indonesia; 7Department of Agricultural Economics and Rural Development, Universityof Goettingen, Germany
Correspondence: Veronika Scherbaum, Institute for Social Sciences in Agriculture, Food and Gender,University of Hohenheim, Schloss, Museumsflügel, 70593 Stuttgart, Germany Email: [email protected]
Malnourished child with mother on Nias Island
SIGHT AND LIFE Magazine 2009;1:29–37
SIGHT AND LIFE RUF
30
nutrient Powder (Part II) forWasted Children in Nias, Indo -nesia.’
Objectives
The objectives of the study were to:
• Develop new recipes of cereal-based RUF, in the form of bis-cuits, for local production andconsumption by wasted childrenaged 6 to 60 months.• Compose a new vitamin and min-eral premix that would make themicronutrient specifications ofthe RUF-Nias biscuits compara-ble (but not identical) to that ofPlumpy’nut™ and reference dataof WHO, WFP, UN-SCN,UNICEF.3
• Explore baking time and temper-ature yielding the lowest loss ofmicronutrients; compare themicronutrient content of thebaked biscuits with the calculatedones; and study the stability of themicronutrient content of the bis-cuits after 3–4 weeks of storage atroom temperature.• Calculate the number of RUF-Nias biscuits needed to meetapproximately 50–60% of thedaily energy requirements of chil-dren aged 6 to 60 months.• Compare the costs of locally pro-duced PMP-Nias and cere-al/nut/legume-based RUF-Niasbiscuits.
Methodology
Product development and evaluation
Nine new recipes of RUF biscuitsusing local (Nias) and national(Indonesian) food sources weredeveloped in Germany4 and theirnutrient composition was analyzedat the Institute of Biological Che -m istry and Nutrition, UniversityHohenheim. The goal was to makethe macro- and micronutrient con-
tent of the biscuit similar (but notidentical) to that of Plumpy’nutTM.A vitamin and mineral premixwhich would enable this was final-ly produced by DSM NutritionalProducts, Singapore, for use in theproduction of RUF biscuits on NiasIsland.
In Nias, data on the constant avail-ability of ingredients to produce thebiscuits were collected through amarket survey and in-depth inter-views with key CWS staff. Basedon this information, four of theRUF recipes were used to producebiscuits that were field-tested inseven feeding centers. The biscuitswere examined for appearance,
color, texture, consistency, smelland taste under given local climateconditions. This organoleptic eval-uation was repeated after two tothree weeks to fulfil the demands ofweekly RUF distribution programs.The two recipes for biscuits mostfavoured by wasted children andtheir caretakers were selected andlocally produced.
The local production of PMP-Niasrelied on previous experience froma similar study in Uganda.5
Contrary to that experience, accept-ance issues occurred with the PMP-Nias during the field testing.Modifications to the recipe (includ-ing heating the oil, adding
skimmed milk powder instead ofwhole milk powder, explaining theimportance of peanuts) were there-fore made. However, caretakerscontinued to complain about per-ceived consequences for their chil-dren (such as diarrhea and consti-pation) when consuming PMP-Nias.
Based on this experience, a newintervention area was established inanother district, where caretakersdid not participate in the local pro-duction of PMP-Nias during thefirst month. Later, after the producthad been accepted and the caretak-ers observed the benefits for theirchildren (increased appetite andweight gain), they even started tovoluntarily assist in the productionof the PMP-Nias. In contrast to theoriginal problems with PMP-Nias,RUF-Nias biscuits were readilyaccepted and liked by the childrenand their caretakers.
Micronutrient stability test
Laboratory examination was per-formed to analyze the nutrient com-position of the biscuits using HighPerformance Liquid Chromato -graphy (HPLC) for vitamins A, E,C, and B1, and Atomic AbsorptionSpectrophotometry (AAS) for ironand zinc.
The composition of micronutrientsbefore baking and their deteriora-tion during baking and storagewere examined. Baking times andtemperatures were investigatedunder the following conditionsusing an electric oven:
170°C, 20 minutes; 170°C, 25 min-utes;180°C, 15 minutes; 180°C, 20minutes
Child participating in feedingprogram
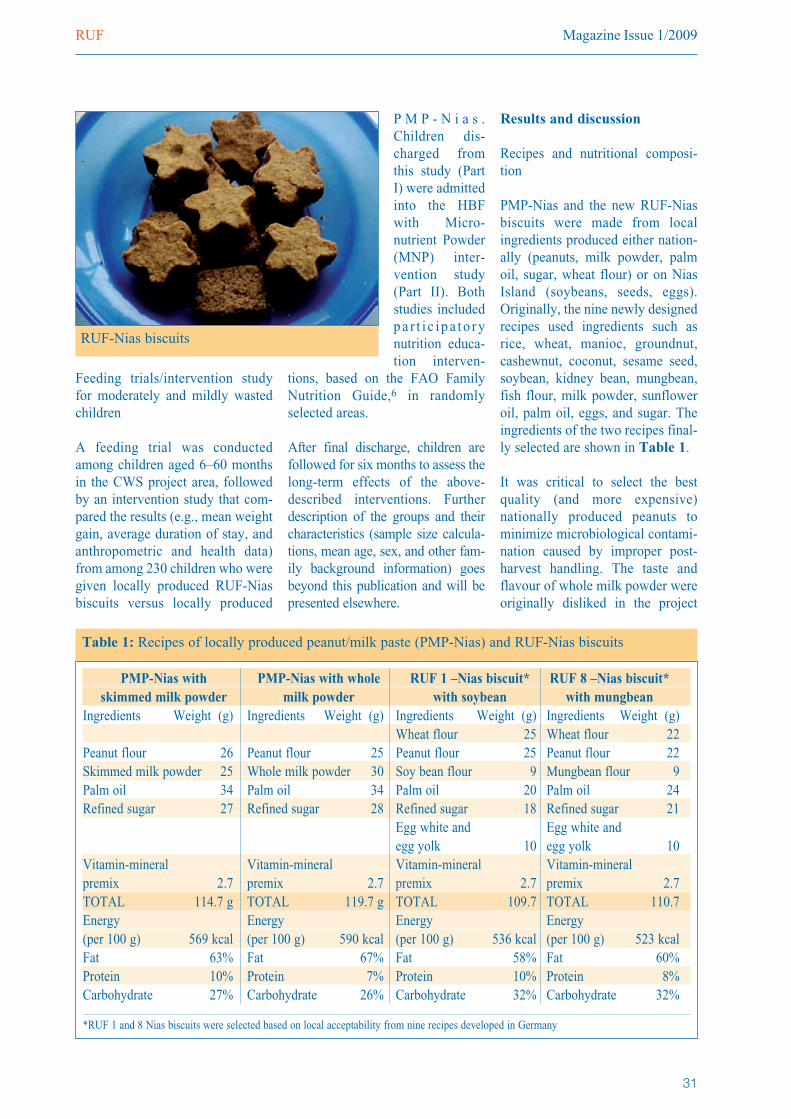
Magazine Issue 1/2009RUF
31
Feeding trials/intervention studyfor moderately and mildly wastedchildren
A feeding trial was conductedamong children aged 6–60 monthsin the CWS project area, followedby an intervention study that com-pared the results (e.g., mean weightgain, average duration of stay, andanthropometric and health data)from among 230 children who weregiven locally produced RUF-Niasbiscuits versus locally produced
P M P - N i a s .Chil dren dis-charged fromthis study (PartI) were admittedinto the HBFwith Micro -nutrient Powder(MNP) inter-vention study(Part II). Bothstudies includedpa r t i c ipa to rynutrition educa-tion interven-
tions, based on the FAO FamilyNutrition Guide,6 in randomlyselected areas.
After final discharge, children arefollowed for six months to assess thelong-term effects of the above-described interventions. Furtherdescription of the groups and theircharacteristics (sample size calcula-tions, mean age, sex, and other fam-ily background information) goesbeyond this publication and will bepresented elsewhere.
Results and discussion
Recipes and nutritional composi-tion
PMP-Nias and the new RUF-Niasbiscuits were made from localingredients produced either nation-ally (peanuts, milk powder, palmoil, sugar, wheat flour) or on NiasIsland (soybeans, seeds, eggs).Originally, the nine newly designedrecipes used ingredients such asrice, wheat, manioc, groundnut,cashewnut, coconut, sesame seed,soybean, kidney bean, mungbean,fish flour, milk powder, sunfloweroil, palm oil, eggs, and sugar. Theingredients of the two recipes final-ly selected are shown in Table 1.
It was critical to select the bestquality (and more expensive)nationally produced peanuts tominimize microbiological contami-nation caused by improper post-harvest handling. The taste andflavour of whole milk powder wereoriginally disliked in the project
PMP-Nias with PMP-Nias with whole RUF 1 –Nias biscuit* RUF 8 –Nias biscuit*skimmed milk powder milk powder with soybean with mungbean
Ingredients Weight (g) Ingredients Weight (g) Ingredients Weight (g) Ingredients Weight (g)Wheat flour 25 Wheat flour 22
Peanut flour 26 Peanut flour 25 Peanut flour 25 Peanut flour 22Skimmed milk powder 25 Whole milk powder 30 Soy bean flour 9 Mungbean flour 9Palm oil 34 Palm oil 34 Palm oil 20 Palm oil 24Refined sugar 27 Refined sugar 28 Refined sugar 18 Refined sugar 21
Egg white and Egg white and egg yolk 10 egg yolk 10
Vitamin-mineral Vitamin-mineral Vitamin-mineral Vitamin-mineral premix 2.7 premix 2.7 premix 2.7 premix 2.7TOTAL 114.7 g TOTAL 119.7 g TOTAL 109.7 TOTAL 110.7 Energy Energy Energy Energy(per 100 g) 569 kcal (per 100 g) 590 kcal (per 100 g) 536 kcal (per 100 g) 523 kcalFat 63% Fat 67% Fat 58% Fat 60%Protein 10% Protein 7% Protein 10% Protein 8%Carbohydrate 27% Carbohydrate 26% Carbohydrate 32% Carbohydrate 32%
*RUF 1 and 8 Nias biscuits were selected based on local acceptability from nine recipes developed in Germany
Table 1: Recipes of locally produced peanut/milk paste (PMP-Nias) and RUF-Nias biscuits
RUF-Nias biscuits

SIGHT AND LIFE RUF
32
Table 2: Micronutrient composition of Plumpy’nutTMand RUF-Nias biscuits in comparison to recommendations. Source: World Health Organization, the
World Food Programme, the United Nations System Standing Committee on Nutrition and the United Nations Children’s Fund. Community-Based
Management of Severe Acute Malnutrition. WHO, WFP, UN-SCN and UNICEF Joint Statement. Geneva: WHO/WFP/UN-SCN/UNICEF, 2007.
Micronutrients
WHO, WFP, UN-SCN,
Plumpy’nutTM
RUF 1-Nias
RUF 8-Nias
Premix
RUF 1-Nias
RUF 8-Nias
UNICEF (for 100 g)
(in 100 g)
biscuits
biscuits
biscuits
biscuits
Min
Max
Min
Max
No added premix
No added premix
(for 100 g)
(in 100 g)
(in 100 g)
Vitamins
Vitamin A µg
800
1100
800
1,200
49.0
40.8
930.0
979.0
970.8
Vitamin D µg
1520
1518
0.3
0.2
16.2
16.5
16.4
Vitamin C mg
50-
50132
0.3
054.0
54.3
54Thiamine B1mg
0.5
-0.5
0.8
0.1
0.1
0.8
0.9
0.9
Riboflavin mg
1.6
-1.6
20.1
0.1
1.8
1.9
1.9
Vitamin B6mg
0.6
-0.6
0.7
0.1
0.1
0.6
0.7
0.7
Vitamin B12µg
1.6
-1.6
2.0
0.1
0.1
1.8
1.9
1.9
Niacin mg
5-
5.0
5.9
4.0
3.5
7.7
11.7
11.2
Biotin µg
60-
6072
3.1
2.6
62.9
66.0
65.5
Folic acid µg
200
-200
230
52.0
53.4
203.8
255.8
257.2
Vitamin K µg
1530
1525
8.0
6.9
20.3
28.3
27.2
Vitamin E mg
20-
2025
3.9
3.2
16.2
20.1
19.4
Pantothenate mg
3-
33.7
0.7
0.6
3.3
4.0
3.9
Minerals
Calcium mg
300
600
300
600
58.0
32.3
287.9
345.9
320.2
Iron mg
1014
1014
3.1
1.8
10.8
13.9
12.6
Iodine µg
70140
70140
0.9
0.8
119.9
120.8
120.7
Zinc mg
1114
1114
1.6
1.1
13.3
14.9
14.4
Sodium mg
-290
-290
16.0
14.8
016.0
14.8
Potassium mg
1,110
1,400
1,100
1,400
353.0
202.5
600.9
953.9
803.4
Magnesium mg
80140
80140
69.0
44.4
22.6
91.6
67Phosphorus mg
300
600
300
600
206.0
141.8
144.7
350.7
286.5
Copper mg
1.4
1.8
1.4
1.8
0.5
0.3
1.8
2.3
2.1
Selenium µg
2040
2040
00
30.6
30.6
30.6
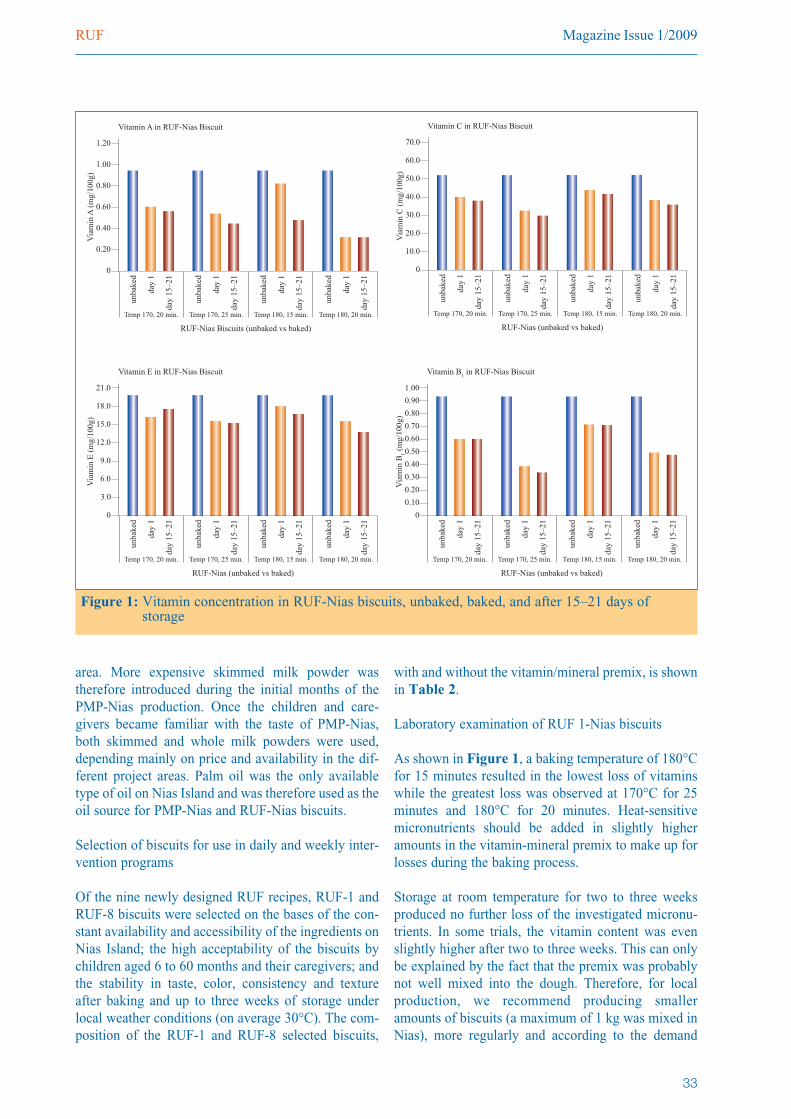
Magazine Issue 1/2009RUF
33
area. More expensive skimmed milk powder wastherefore introduced during the initial months of thePMP-Nias production. Once the children and care-givers became familiar with the taste of PMP-Nias,both skimmed and whole milk powders were used,depending mainly on price and availability in the dif-ferent project areas. Palm oil was the only availabletype of oil on Nias Island and was therefore used as theoil source for PMP-Nias and RUF-Nias biscuits.
Selection of biscuits for use in daily and weekly inter-vention programs
Of the nine newly designed RUF recipes, RUF-1 andRUF-8 biscuits were selected on the bases of the con-stant availability and accessibility of the ingredients onNias Island; the high acceptability of the biscuits bychildren aged 6 to 60 months and their caregivers; andthe stability in taste, color, consistency and textureafter baking and up to three weeks of storage underlocal weather conditions (on average 30°C). The com-position of the RUF-1 and RUF-8 selected biscuits,
with and without the vitamin/mineral premix, is shownin Table 2.
Laboratory examination of RUF 1-Nias biscuits
As shown in Figure 1, a baking temperature of 180°Cfor 15 minutes resulted in the lowest loss of vitaminswhile the greatest loss was observed at 170°C for 25minutes and 180°C for 20 minutes. Heat-sensitivemicronutrients should be added in slightly higheramounts in the vitamin-mineral premix to make up forlosses during the baking process.
Storage at room temperature for two to three weeksproduced no further loss of the investigated micronu-trients. In some trials, the vitamin content was evenslightly higher after two to three weeks. This can onlybe explained by the fact that the premix was probablynot well mixed into the dough. Therefore, for localproduction, we recommend producing smalleramounts of biscuits (a maximum of 1 kg was mixed inNias), more regularly and according to the demand
Figure 1: Vitamin concentration in RUF-Nias biscuits, unbaked, baked, and after 15–21 days of storage
1.20
1.00
0
0.80
0.60
0.40
unba
ked
day
1
day
15–2
1
0.20
Via
min
A (
mg/
100g
)
Vitamin A in RUF-Nias Biscuit
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
Temp 170, 20 min. Temp 170, 25 min. Temp 180, 15 min. Temp 180, 20 min.
RUF-Nias Biscuits (unbaked vs baked)
21.0
18.0
0
15.0
12.0
9.0
unba
ked
day
1
day
15–2
1
6.0
Via
min
E (
mg/
100g
)
Vitamin E in RUF-Nias Biscuit
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
Temp 170, 20 min. Temp 170, 25 min. Temp 180, 15 min. Temp 180, 20 min.
RUF-Nias (unbaked vs baked)
3.0
70.0
60.0
0
50.0
40.0
30.0
unba
ked
day
1
day
15–2
1
20.0
Via
min
C (
mg/
100g
)
Vitamin C in RUF-Nias Biscuit
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
Temp 170, 20 min. Temp 170, 25 min. Temp 180, 15 min. Temp 180, 20 min.
RUF-Nias (unbaked vs baked)
10.0
1.00
0.80
0
0.70
0.60
0.40
unba
ked
day
1
day
15–2
1
0.20Via
min
B1 (
mg/
100g
)
Vitamin B1 in RUF-Nias Biscuit
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
unba
ked
day
1
day
15–2
1
Temp 170, 20 min. Temp 170, 25 min. Temp 180, 15 min. Temp 180, 20 min.
RUF-Nias (unbaked vs baked)
0.90
0.50
0.30
0.10
(number of malnourished children admitted to the pro-gram).
Iron and zinc content in the RUF biscuits after bakingwas similar to the calculated amounts, confirming thatthe right amount of these essential minerals had beenmixed into the dough.
It is important to note that a kerosene stove was usedin Nias which cannot keep exact temperature.Therefore, the CWS staff was advised to bake theRUF-Nias biscuits until they were light brown (whichtook about 20 minutes at about 170–180°C).
Feeding recommendations
The RUF-Nias biscuits were mainly developed as analternative to locally produced PMP-Nias for wastedchildren aged 6–60 months during the rehabilitationphase. For younger children, especially infants aged6–12 months, the biscuits were crushed into smallquantities of boiled drinking water and offered by thespoonful. Mothers/caretakers were instructed to offerthe biscuits between family meals and after breastfeed-ing. Caretakers were informed that the biscuits are sup-plementary foods designed to support weight andheight gain in malnourished children. Originally, therecommended number of biscuits per day was calculat-
ed to cover about 50% of thedaily energy requirements ofindividual children, based on thechild’s weight. Energy require -ments were taken from FAO/ -WHO/UNU recommendationsfor children’s dietary energyintakes.7
After field testing, the number ofbiscuits to be consumed wasincreased by 10% to cover 60%of the daily energy requirementsof children, in line withIndonesian guidelines.8 The
increase takes into consideration the possible sharingof the biscuits within families. Children aged 6–24months, with a weight of about 6–10 kg received 4–7biscuits per day (50–90 g); children aged 2–5 years,weighing 10–15 kg, were given 7–11 biscuits (90–150g) per day.
As the locally produced PMP-Nias quickly sours underlocal temperatures of about 30°C, it was produced anddistributed on the same day with close supervision.The same holds true for commercially producedPlumpy’nut™, which can be used for only one dayafter the packaging is opened.9,10 (In the Uganda expe-rience, a local substitute of Plumpy’nut™ was pro-duced on a weekly basis because it could be stored ina refrigerator.5) For a child aged 6–24 months, with aweight range of 6–10 kg, half to one portion of PMP-Nias (50–100 g) was distributed each day; childrenaged 2–5 years, weighing about 10–15 kg, received1–1.5 portions per day (100–150 g).
Cost estimation
The costs of the RUF1-Nias biscuits and PMP-Niaswere calculated according to local prices for the ingre-dients (Table 3). In general, prices are higher on NiasIsland compared to other parts of Indonesia, mainlybecause transportation costs are exacerbated by
uneven deliveries resulting frombad weather.
Table 4 presents an overview ofthe calculated costs per 100 g oftwo locally-produced PMPs(Uganda and Nias) and theRUF1-Nias biscuits. The cost ofthe PMP produced in Uganda isincluded to illustrate the vari-ability of local production costs
SIGHT AND LIFE RUF
34
Ingredient PMP- Nias RUF 1-NiasPeanuts 0.55 – 0.57 0.46Wheat flour 0.40Soybean/mungbean 0.11Palm oil 0.39 0.20 – 0.30Sugar 0.27 0.18Egg 0.13Whole-, skim milk powder 1.44 - 2.99Vitamin/mineral premix 0.04 0.04Total 2.69 – 4.26 1.52 – 1.62
Table 3: Cost of ingredients per kg of PMP-Nias and RUF-1 (in euros)
RUF- PMP/RUF- RUF1-NiasPrice for 100 g, Uganda Nias biscuitsabout 500 kcal (2006) (2007) (2007)(in euros)
0.22 – 0.30 0.27 – 0.43 0.15 – 0.16
Table 4: Price comparison (Note: the calculation does not include costsof equipment and salaries for NGO staff responsible for pro-duction, distribution and monitoring)

Magazine Issue 1/2009RUF
35
The World Health Organization (WHO) revised itsguidelines for the management of severe malnutri-tiona in 1999 and introduced therapeutic milk forseverely malnourished children with medical com-plications – a treatment that has been successfullyimplemented in hospitals worldwide. However,therapeutic milk powder requires clean water forreconstitution as well as close supervisionbecause, if left unrefrigerated in hot climates, milkserves as a favorable medium for bacterial growth.In much of the world, caretakers are required tostay for multiple weeks in clinics with their mal-nourished child, which causes considerable incon-venience for other family members too.
To reach more children at an earlier stage and tobring the services directly to communities, a foodspread called Plumpy’nut™ was developed forseverely malnourished children without clinicalcomplications. This product can be given as part ofa home-based treatment under a system of weeklysupervision.b
Plumpy’nut™, the first Ready-to-Use TherapeuticFood RUTF developed, is nutritionally compara-ble to therapeutic milk, and is made of peanut but-ter, milk powder, vegetable oil, sugar, and a vita-min-mineral mix. Packed in air-tight sachets,Plumpy’nut™ has a relatively long shelf life andcan be immediately consumed without furtherpreparation. In several studies, Plumpy’nut™(whether imported or locally produced) enabledsimilar weight gain in severely malnourished chil-dren as therapeutic milk under hospital-basedcare.c–d RUTFs have thus been successfully usedin Community-based Therapeutic Care programs,reducing the constraints posed by lack of access toclean water and caretaker separation from fami-lies.
For efficiency, the blanket distribution of anRUTF is recommended. Plumpy’nut™, however,
which is mainly produced in industrialized coun-tries, can be too expensive for blanket distributionon a large scale.e In order to reduce costs, increasecoverage, supplement local diets, and support localeconomies, experts are advocating the productionof RUTFs from locally available ingredients incountries with a high prevalence of malnutri-tion.f–g
A successful approach in treating and preventingmild-to-moderate malnutrition prevents conditionsfrom worsening to severe forms of malnutrition.Recently, several products for treating and pre-venting different forms of malnutrition have beenproposed by the UN World Food Programme(WFP), under its partnership with DSM.h
References for Box 1
a. World Health Organization. Management of severe malnu-trition: a manual for physicians and other senior healthworkers. Geneva: WHO, 1999.
b. Bahwere P, Binns P, Collins S, Dent N, Guerrero S, HallamS, Khara T, Lee J, Mollison S, Myatt M, Saboya M, SadlerK, Walsh A. Community-based Therapeutic Care (CTC) aField Manual. Oxford: CTC Research and DevelopmentProgramme, 2006.
c. Diop el HI, Doussou NI, Ndour MM, Briend A, Wade S.Comparison of the efficacy of a solid ready-to-use food anda liquid, milk-based diet for the rehabilitation of severelymalnourished children : a randomized trial. Am J Clin Nutr2003;78:302–7.
d. Krumbein T, Scherbaum V, Biesalski HK. Locally pro-duced Ready-to-Use Therapeutic Food (RUTF) in an inpa-tient setting in Uganda. Emergency Nutrition Network(ENN) Field Exchange 2006;28:21–3.
e. Enserink M. The peanut butter debate. Science Magazine2008;322:36–38.
f. Collins S, Henry CJK. Alternative RUTF formulations.Emergency Nutrition Network 2004;2:S35–7.g. Manary MJ. Local production and provision of ready-to-use therapeutic food (RUTF) spread for the treatment ofsevere malnutrition. Food Nutr Bull 2006;27(3):S83–9.
h. World Food Programme/DSM. Ten minutes to learn aboutnutrition programming. SIGHT AND LIFE Magazine3/2008, Supplement.
Box 1: Ready-to-Use Therapeutic Food (RUTF)
in different research sites, to date.The cost calculation was based onthe average price of the ingredientsused in Nias in 2007 (1 euro wasapproximately Rp 12,000). Thecost of 100 g of PMP-Nias wasbetween 27 and 43 euro cents,
depending on the type of milk pow-der (whole or skimmed milk),while the cost of the vitamin-min-eral premix to produce 100 g ofRUF biscuits or PMP-Nias was 0.4euro cents. This price does notinclude the cost of transportation
from DSM Singapore to Jakarta,which was borne by DSM.
Preliminary results
Of the 230 moderately/mildly wast-ed ( -3 to < -1.5 WHZ) children

admitted into the ongoing RUF-Nias intervention study (Part I),
152 recovered successfully (dis-charged at > -1.5 WHZ).
Despite the higher cost of the PMP-Nias, the RUF-Nias biscuits result-ed in better weight gain. The bestweight gain (5.5 g per kg bodyweight per day) was achievedthrough the use of the biscuits com-bined with participatory nutritioneducation, followed by the use ofthe biscuits alone (3.7 g per kgbody weight per day), and finallyby the use of the PMP-Nias (3.5 gper kg body weight per day) indaily intervention programs. Datafrom weekly programs indicatesimilar results but somewhat lowerweight gains.
The average length of participationin the program was approximately3–5 weeks. In the Part II study, ofthe 210 mildly wasted ( -1.5 to <-1 WHZ) children admitted into theongoing Home-Based Foods withMicronutrient Powder intervention,
SIGHT AND LIFE RUF
36
Box 2: Energy and macronutrient content (per 100 g)
Figure A: Proposed feeding programs according to nutritional status
TFP: Inpatient Therapeutic Feeding ProgramsOTP: Outpatient Therapeutic Feeding ProgramSFP: Supplementary Feeding Program
Plumpy’nut™ PMP-Nias* Average of 9 RUF recipes
520–550 kcal 569–590 kcal 500–536 kcal10–12 % protein 7–10 % protein 8–14 % protein45–60 % fat 63–67 % fat 31–58 % fat28–45 % carbohydrate 26–27 % carbohydrate 31–44 % carbohydrateNutriseta (*whole/skim milk) Shapiro, 2007b
The amount of RUF1-Nias biscuits needed each day was calculated asfollows:• 100g of biscuit dough contains 536 kcal;• 8 individual biscuits are made from about 100 g dough;• 1 individual biscuit weighs about 13 g and contains about 67 kcal.
References for Box 2a. Nutriset. Plumpy’nut™, F-100 therapeutic milk in spread form, 2008.b. Shapiro O. Development of Ready-to-Use Food (RUF) for malnourished chil-dren in Indonesia. Diploma Thesis. Germany: Institute of Biological Chemistryand Nutrition, University of Hohenheim, Stuttgart, 2007.
Magazine Issue 1/2009RUF
37
101 children were discharged suc -cess fully ( -1 WHZ). Accom -panying participatory nutrition edu-cation also improved weight gain inthis study.
Recommendations
Given the efficacy of locally pro-duced RUF-Nias biscuits (withoutmilk powder) in improving weightgain among moderately/mildlywasted children, the biscuits shouldnext be tested and compared withPMP-Nias for use in treatingseverely wasted children. RUF-Nias biscuits with milk powder(providing high quality protein andessential fatty acids) should also betested for an impact on weight gainamong severely and moderatelywasted children; if successful,RUF-Nias biscuits would be appro-priate for a wider range of malnu-trition problems.
Given the improved weight gainamong wasted children whoreceived RUF in combination withnutritional training for their care-takers, the results further suggestthat participatory nutrition educa-tion should accompany nutritioninterventions.
Acknowledgements
This ongoing research has been part-ly sponsored by DAAD, SIGHTAND LIFE, Eiselen Foun dation,Neys van Hoogstraten Foundation,and Church World ServiceIndonesia. We would like to thankthem for their continuous supportand encouragement.
References
1. UNICEF. The Second Health andNutrition Assessment in NanggroeAceh Darussalam Province and NiasIsland, September 2005. Jakarta:UNICEF, 2005.
2. Church World Service (CWS). HasilAssessment di Gunung Sitoli, Nias.Jakarta: CWS, 2007.
3. World Health Organization, the WorldFood Programme, the United NationsSystem Standing Committee onNutrition and the United NationsChildren’s Fund. Community-BasedManagement of Severe Acute Mal -nutrition. WHO, WFP, UN-SCN andUNICEF Joint Statement. Geneva:WHO/WFP/UN-SCN/UNICEF, 2007.
4. Shapiro O. Development of Ready-to-Use Therapeutic Food (RUTF) for mal-nourished children in Indonesia. DiplomaThesis. Germany: Institute of BiologicalChemistry and Nutrition, University ofHohenheim, Stuttgart, 2007.
5. Krumbein T, Scherbaum V, BiesalskiHK. Locally produced Ready-to-UseTherapeutic Food (RUTF) in an inpa-tient setting in Uganda. EmergencyNutrition Network (ENN) FieldExchange 2006;28:21-23.
6. Burgess A, Glasauer P. FamilyNutrition Guide. Rome: Food andAgriculture Organization of the UnitedNations, 2004.
7. World Health Organization. Report ofa joint FAO/WHO/UNU expert con-sultation. Energy and protein require-ments. WHO Technical Report SeriesNo. 724. Geneva: WHO.
8. Departemen Kesehatan RI. AngkaKecukupan Gizi 2004 bagi orangIndonesia. Indonesian NutritionNetwork, Departemen Kesehatan RI,2004. Internet: http://www.gizi.net/lain/gklinis/AKG2004.htm (accessedNovember 21, 2008).
9. Nutriset. Website of local produc -tion of Plumpy’nut™ and infor -mation about the product. Internet:http://www.nutriset.fr (accessedAugust 22, 2008).
10. Nutriset. Storage Conditions andChanges in Products, 2008. NutrisetInstruction Manual for Local Pro -duction of Plumpy’nut™, 2008.
Child receiving PMP-Nias
Reader Survey on-goingQuestionnaire available at: www.sightandlife.org Closing date: 30 June 2009
As a platform for the exchange of programmatic and scientific information, we would like the SIGHT AND LIFEMagazine to remain ever-evolving and adaptive to the new realities of the micronutrient field. We are, therefore,currently conducting a survey to gather our readers’ opinions.
We would very much appreciate it if you could participate in our survey, and share with us your views on theMagazine and your suggestions for ways to improve it through a short online questionnaire. This should only take5 to 10 minutes of your time and would be a great help to us in making the Magazine better suit-ed to meet your information and knowledge needs.
Readers who dedicate some of their time to answering this survey will be included in a lucky drawafter the survey period to receive rewarding prizes.
SIGHT AND LIFE Global Food Security Conference
38
An innovative and timely gathering was convened on thecampus of McGill University in Montreal, Canada, overtwo days and six working sessions on September 25–26,2008, with developing country participants from Haitiand Guatemala in the Western Hemisphere; Uzbekistan,India and China in Asia; and Ethiopia, Nigeria, Moroccoand Kenya in Africa.
The nation’s tradition of international concern and itsmajor agricultural potential accounted for the timing andlocation of the meeting. In fact, the momentum for thisconference emanated from the University’s Faculty ofAgriculture, under the leadership of its dean, Dr ChandraMandramootoo.
Speakers in the first working session, entitled ‘Voicesfrom the Field,’ highlighted key topics, including the sta-tus of food and agricultural production, food insecurity,
and the issues and possible solutions for diverse nationsand regions of the world. Current data on production andprices of food, risk of hunger, and the contributing fac-tors for both were brought to the forum by residents ofthe various countries from different disciplinary back-grounds.
Among the factors mentioned as determinants of localfood availability were climate change, soil erosion,dependency on natural rainfall, and post-harvest losses.In some settings, food safety standards can be a hin-drance to the abundance of foodstuffs. Although foodprices have risen acutely in the past months, the fractionof family income spent for food had been falling over thepast three decades. Controversy raged regarding thedegree to which liberalization of food trade has acted asan aide or an obstacle to maintaining food. This is truefor Haiti, which has no option but to import food fromthe world market, and China, which is debating theoption of integration with – or isolation from – worldfood trade and international price norms. In fact, 84% ofthe total rate of inflation in China is attributable to theincrease in the cost of food.
The second session, which covered the ‘World FoodSituation,’ synthesized national case studies into morecomprehensive and integrated descriptions and analyses.Representatives from a potpourri of organizations andinstitutions related to agriculture, either in its productionor distribution sense, contributed to the discussions.
Conference on Global Food SecurityMcGill University, Montreal, Canada
Noel W. SolomonsCenter for Studies of Sensory Impairment, Aging and Metabolism(CeSSIAM), Guatemala City, Guatemala
Correspondence: Noel W. Solomons, Center for Studies of SensoryImpairment, Aging and Metabolism (CeSSIAM), 17 a Avenida 16-80,Zona 11, Guatemala City, GuatemalaEmail: [email protected]
A person who has food has many, many problems . . .A person who has no food has only one problem.
Chinese Proverb
SIGHT AND LIFE Magazine 2009;1:38–41
Magazine Issue 1/2009Global Food Security Conference
39
Among the entities represented on the program wereMcGill University, the International Rice ResearchInstitute, the International Food Policy Research Institute(IFPRI), the Farm Foundation, and the Inter-AmericanInstitute for Cooperation on Agriculture.
The discussion began by framing the recent WorldHealth Organization analysis of the world food situationin terms of recent changes that have brought on the cri-sis. The adaptive measures in the face of food shortageinclude reducing the number, size and diversity of foodsin meals. Grains used for biofuels compete for land andwater, and IFPRI has called for a moratorium on usinggrains for biofuels. The underlying contributors to foodinflation are export bans on cereals and edible oils andprice speculation. With the intimate linkage of food tohuman survival, aggressive regulation of speculation canbe advocated. IFPRI has written a major policy paper onthe crisis that summarizes a four-point package (see Box 1).
Rice became the centerpiece of discussion, as it is themost widely consumed of the staple grains. Technicaladvances were highlighted, including a hybrid variety ofrice that can produce substantial yields even when total-
ly submerged, as during the monsoon season inBangladesh. There is a need, however, for rebuildinghuman resources for the research endeavor to create anew ‘green revolution’ for this important crop.Responses came from a panel of three discussants repre-senting the Canadian Faculties of Agriculture andVeterinary Medicine, the Organization for EconomicCooperation and Development (OECD), and theCanadian Federation of Independent Grocers.
The third session pursued ‘The Underlying Factors forthe Food Crisis,’ with speakers from five entities: theInternational Federation of Agricultural Producers, theGeorge Morris Centre, the Carnegie Endowment forInternational Peace, the Canadian Centre for PolicyAlternatives, and the African Rice Centers. Climatic fac-
tors led the discussion: Droughts in Australia disruptedthe world wheat trade, with ripple effects throughout theglobe. In Bangladesh, severe effects from flooding werefelt. However, it is more productive to examine factorson a local or regional basis, as impacts are variabledepending on geography. The fallacy in a one-size-fits-all approach to solutions was decried, and the necessityfor nuance in resolving the problems was highlighted.
The response panel included representatives from PulseCanada, the Canadian Agro-Food Policy Institute andMcGill University. Much was made of the differentialimpact on incomes from increasing food prices, depend-ing on whether households or nations are net producersor net consumers of food. In settings where farmers arenet producers of food, increased family incomes andimproved wellbeing arises when food prices rise.Assuring better incomes across all sectors would be astrategy by which farmers could benefit while othergroups still have purchasing power to face higher foodcosts.
The ‘International Response to the Crisis’ was the topicof the fourth session. Its task was to integrate the factsand insights of the first three blocks. United Nations, andinternational and bilateral agencies were represented,including the World Food Programme (WFP), the Foodand Nutrition Organization, the International Federationof the Red Cross and Red Crescent, OECD, and theInternational Commission on Irrigation and Drainage(ICRD). It was clear that WFP and the Red Cross/RedCrescent are primed to humanitarian assistance inresponse to the negative consequences of food scarcity,with targeting and focusing being key to strategies.Within Africa, there is an acknowledgement that theareas with the highest endemicity for HIV merit specialattention. No mention was made of micronutrients, forti-fication or the nutritional quality of the diet. The ration-al use of water for irrigation is key to the support of foodagriculture.
Panelists from the International Crop Research Institutefor the Semi-Arid Tropics, McGill University, and theCarnegie Endowment for International Peace led the dis-cussion, which highlighted the potential for using non-conventional crops suited to arid lands, such as sorghumand cow peas. At least 1.6 billion people live in semi-aridclimes. An important point, however, was the delin-eation between short-term measures to mitigate the suf-fering and long-term strategies for development.
The fifth session, entitled ‘Getting Food to the People:Success Stories,’ accommodated speakers from theCanadian Foodgrain Bank, the Nanking Agricultural
• Expand emergency and humanitarian assistance• Eliminate export restrictions on food• Promote crop production programs with short-termimpact
• Change policies for directing grain and oil seed tobiofuels
Box 1: Four point response package of theInternational Food Policy ResearchInstitute

SIGHT AND LIFE Global Food Security Conference
40
University in China, the Ministry ofAgriculture of Guyana, theBiotechnology for SustainableDevelopment in Africa Foundation,and ICRD. An important strategicpoint came up in this session: theneed for a twin track. The first is tomeet the immediate needs of thehungry. The second is for action tostrengthen livelihoods, as the impactis most serious for those who werehungry before the crisis. Interestingcontrasts were drawn between thetwo Asian countries whose com-bined populations make up over one-third of humanity, China and India.China has one-fifth of the world’spopulation, with 10% of the arable
land but only one-fourth of the worldaverage per capita water availability.China has a mixed strategy ofdomestic production and trade to fillits food needs. India has one-sixth ofthe world’s population, balancedwith one-sixth of the arable land.Forty percent of the crop land is irri-gated, but 60% is monsoon-rainfalldependent. While up to 70% of theIndian laborforce is dedicated toagriculture, the sector contributesonly 25% of gross domestic product(GDP). India is currently self-suffi-cient in food.
For sub-Saharan Africa, the situationis distinct. Most of the processingand profits for materials from Africaare generated outside of Africa.When it comes to food for humanconsumption, there is a widespreadskepticism about quality controlstandards in Africa. A case-study ofthe plant, Moringa (Moringaoleifera), an African food plant usedin a food supplement was cited. Itssuccessful production for local andfor international markets is an exam-ple to be followed, and allows for theoptimism for the motto ‘trade notaid’ to become the standard forAfrica, as well.
Deans of agriculture from theUniversity of Laval in Quebec Cityand the University of Prince EdwardIsland, and a representative of the
Canadian Food Security PolicyGroup constituted the discussantpanel. The points made included thatthe problems of getting food to peo-ple will eventually affect everyone,political will and collaboration willbe needed to meet the challenges,and one cannot expect a unique solu-tion to multifaceted problems.
The topic of the sixth and last seg-ment of the program was ‘The WayForward: Elements of a Frameworkfor Managing the Crisis andConcluding Remarks.’ The Hono -rable Michael Chong, Member ofthe Canadian Parliament forWellington-Halton Hills District,was the keynote speaker for the finalsession. He drew some considera-tions of Canada in the world at large,including features on Canadian soiland features overseas. The keypoints of MP Chong’s discourse areincluded in Box 2.
A prestigious panel for this lastsession included the High Com -missioners to Canada from Kenyaand Nigeria, the Minister ofAgriculture of Guyana, theMoroccan General Council ofAgricultural Development, a pastorwho leads a faith-based reliefagency, the Deputy Minister of theNova Scotian Department ofAgriculture, and a representative ofthe Food and Agricultural
• Urban sprawl is a major factor in reduction of arableland devoted to cultivation. The growth of citiesaround the Great Lake Basin has environmental con-sequences, including damaging the aquifers of theregion. Water levels in the Great Lakes are at low orrecord low levels.
• Climate change is a reality, and Canada should signon to the efforts to cap carbon emissions into the environment.
• Increased cost of crude oil is a threat to the model offood trade, growing in one location and consuming in
another. Canada must continue to avoid the practiceof ‘dumping’ excess agricultural production intocountries in which it will suppress the price andadversely affect local production.
• Biotechnology is not the whole solution to the foodsecurity problem, but it is part of the solution.
• The economics of agriculture in Canada are a threatto food security. It is unprofitable to be a farmer.Higher price for food is inevitable, and it needs to beframed within popular expectation.
Box 2: Key Points raised by the Honorable MP Michael Chong
The topics of Food Security inChina, with respect to rising pricesand the search for policy solutions,were analyzed by Dr Jing Zhu,agricultural economist at the Nan -king University in the Peo ple'sRepublic of China.
Magazine Issue 1/2009Global Food Security Conference
Organization (FAO), and a former Canadian prime min-ister, Joe Clark, who is currently a Professor at theMcGill Centre for Developing-Area Studies. The speak-ers tried to impart some notes of wisdom on the overallthemes to carry the effort forward. It was emphasizedthat the farmer needs to be at the cen-ter of food policy considerations, andthat women are often the farmers indeveloping countries. Technologiesto improve the in come of farmersmust be applied. Beyond the smallfarm sector, general civil society is aprincipal stakeholder, along with theprivate sector and academia.
The most inspirational words camefrom Rev. Jim Cornelius and Prof.Clark. The former is a church pastorwho runs the faith-based CanadianFoodgrains Bank. He urged a strate-gy to decide on one thing to do dif-ferently to make a difference for hun-gry people, build collaborative net-works, turn the food crisis to theadvantage, and give surplus to those who do not have.The latter urged the attendees to build on the momentumof the conference, starting with the simple “doable”actions. He further urged a triple alliance of public, pri-vate, and people partnership. With this alliance, more-over, corporate responsibility should come from beyondthe agro- and food-industry sectors, including the inter-national mining sector in the case of Canada.
In summary, the two-day meeting allowed a variety ofspeakers from diverse geographical experiences and pro-fessional backgrounds to share their reflections on theworld food crisis. It was evident that it was easier to findinstances of grave consequences of food insecurity thanto cite successful case studies of successful responses.
Policy makers are grappling with multiple options, and itis timely to have all of the ideas aired and discussed.
A memorable phrase from the meeting was from Prof.Clark: “Paradigms do not just shift – they get shoved.”
This crystallized a consensus thatconventional ways of viewing agri-culture, food trade and familyincomes need to be re-evaluated.Demography, climate and waterresources are important constraints,as are the fuel costs to transportgrains from producer to consumernations.
Perhaps it was disappointing that theelements to shove the paradigm evenfurther did not arise. The sense of themeeting seemed to be simply to getthings back to the state they werebefore the crisis, without a real cri-tique of what might have been wrongwith nutritional adequacy and healthin pre-crisis times. The acuteness and
severity of the crisis may have drained the optimism tomove the agenda to a third way; this would continue tomove the bulk of humanity from a precarious and mar-ginal (albeit calorically adequate) diet to a secure andquality diet.
Key reflection from the conference• If you have no water, you have no food security.• Hunger is the result of poverty and the cause ofpoverty.• Preventing the distraction of hunger allowspeople to work and hopefully receive an incomethat lifts them out of poverty.
Her Excellency, Judith MbulaBahemuka, the Kenyan HighCommissioner to Canada, speakingat the McGill Conference onGlobal Food Security
The Guidebook Nutritional Anemia isnow available in
English, French and Spanish
SIGHT AND LIFE ANEC III
42
The 3rd African Nutritional Epidemiological Con -ference (ANEC III) was held in Cairo, Egypt, fromOctober 13–16, 2008. Prof. Ashraf Shaalan, of Egypt’sNational Research Centre (NRC), was the Conferencechairman, while Prof. Anna Lartey, of the Universityof Ghana, chaired the international ScientificCommittee. They jointly guided the three days of aca-demic sessions.
Held at the NRC, at the center of Cairo, theConference saw over 250 attendees gathered on thetheme, ‘The Epidemiological and Nutritional Tran -sition in Developing Countries: Accelerating progressfor nutrition in Africa.’ A total of 25 countries –including 14 African countries – were represented.
Unique to this conference were special awards cere-monies for two venerable leaders of human and publichealth nutrition: Prof. Nevin Scrimshaw, from theUSA, and Prof. Mohammed Gabr, from Egypt. Thecareer trajectory and contributions of Dr Scrimshawwas narrated and interpreted by two of his former stu-dents, Noel Solomons and Ricardo Uauy. The narra-tive extended from his founding of the Institute ofNutrition of Central America and Panama inGuatemala, to his leadership of the InternationalNutrition Foundation, with stops as department chairat the Massachusetts Institute of Technology, presidentof the International Union of Nutritional Science(IUNS), vice-rector at the United Nations University,
and World Food Prize Laureate, along the way. A mas-sive birthday cake honored the 90 years of this lion ofhuman and clinical nutrition, whose creative impacthas been felt in every region of the globe, including thelength of Africa. Although unable to travel to Cairo inperson, Prof. Scrimshaw addressed the assembly byway of a video message.
Prof. Gabr, a native of Cairo, distinguished himselfthrough his publications on pediatrics and pediatricnutrition, as the former president of IUNS, and the ex-Minister of Health of Egypt. Prof. Osman Galal, cur-
Third African NutritionalEpidemiology Conference Cairo, Egypt
Nadia Fanou Fogny1, Abdul-Razak Abizari2, Noel W. Solomons31Department of Nutrition and Food Sciences, Faculty of AgronomicSciences, University of Abomey Calavi, Benin; 2Department ofCommunity Nutrition, School of Medicine and Health Sciences,University for Development Studies, Ghana; 3Center for Studies ofSensory Impairment, Aging and Metabolism (CeSSIAM), GuatemalaCity, Guatemala
Correspondence: Noel W. Solomons, Center for Studies of SensoryImpairment, Aging and Metabolism (CeSSIAM), 17 a Avenida 16-80,Zona 11, Guatemala City, GuatemalaEmail: [email protected]
Key messages from ANEC III • Malnutrition (undernutrition, obesity, micronu-trient deficiencies and associated diseases) arestill public health concerns in Africa.
• Research and interventions, capacity buildingand partnerships (public-private-community)are key actions to contribute to the sustainableimprovement of nutrition and food security incommunities.
• The dissemination of research results is anotherway to help communities in raising awarenessabout their conditions.
• Advocating for better integration of nutritionconcerns in government policies will also strong-ly boost better nutrition among communities
SIGHT AND LIFE Magazine 2009;1:42–45
Magazine Issue 1/2009ANEC III
43
rent secretary general of IUNS, recounted the distin-guished accomplishments of Dr Gabr in the context ofEgyptian society and international projection.
Keynote addresses
Fifteen keynote addresses were programmed to pro-vide a voice for an equal number of distinguished pro-fessionals from Africa and around the world. Theirtitles are listed in Box 1. On the one hand, they attestto the seriousness with which the double burden ofhealth concerns – implicit in the thematic key term of‘nutrition transition’ – was brought into the meetingprogram. On the other hand, although vitamin andmineral topics were treated in many of the keynote dis-courses, only that by Dr Kenneth Brown, regionaladvisor for Helen Keller International, based in Dakar,Senegal, was explicitly related to a micronutrient.
Dr Brown spoke on ‘Scaling up NutritionInterventions: Examples of programs for preventingzinc deficiency.’ He reviewed the evidence for theexistence of endemic zinc deficiency in low-incomenations, and the impact that zinc supplementation andfortification have had in controlled, efficacy field tri-als. He then addressed the challenges and, to someextent, frustrations related to an agenda of getting pub-lic health interventions onto a scale to cover the needsof all vulnerable segments of the population.Appropriate technology, cost, political will, program-matic integration, and long-term sustainability wereamong the issues identified.
Tutankhamen
• Global nutritional challenges: Accelerating progressfor nutrition in Africa
• The role of nutrition in the attainment of theMillennium Development Goals
• Epidemiological and nutrition transition: Global perspectives and examples of successful approaches
• Epidemiological and nutrition transition: How muchprogress has been made in addressing the double burden of disease in sub-Saharan Africa
• Facing nutrition transition under the double burden:Challenges and potential programs in Africa
• Training and capacity-building needs for nutrition inAfrica
• Cancer trends in Africa: a cause for concern?
• Innovation in the management of malnutrition indeveloping countries
• Tackling obesity in Africa: Pragmatic approaches• Scaling up nutrition interventions: Examples of programs to prevent zinc deficiency
• Interventions among school-aged children in developing countries
• Current trends in HIV/AIDS and their implicationsfor human and economic development
• Biodiversity: A tool for addressing nutrition problemsin Africa
• The challenge of breaking the cycle of poverty andhunger in an unequal world
• Ensuring community participation and scaling upnutrition through NGO work
Box 1: Titles of the keynote addresses in the plenary sessions of the 3rd African NutritionalEpidemiology Conference
SIGHT AND LIFE ANEC III
44
Plenary sessions
The ANEC III program featuredthree plenary symposia. The firstwas sponsored by Unilever andentitled ‘Advancing Nutrition andHealth in Africa: The Power ofPartnership,’ which included pre-sentations from industry, a privateconsultancy, academia and theUnited Nations system. The secondin this series was entitled ‘FoodBiotechnology and Biodiversity inAfrica,’ which included topics suchas probiotics, transgenic fish, wildfoods, protein quality and iron- fortified whole maize flour. Thefinal symposium, ‘Recent Ad-vanc es in Amino Acid Research,’was held to honor Prof. Scrimshawand the field he pioneered. After avideo presentation from the hon-oree, six presenters covered anarray of advances in understandingamino acid requirements and thebioactive functions of specificamino acids.
The two workshops in the programwere astutely tailored to the needs
of modern nutritional epidemio -logy. The first was entitled ‘Vali -dation of Dietary Assessment In -struments’ and provided a usefulorientation on the nuances of fieldapproaches to assessing dietaryintake and exposures. The secondwas entitled ‘How to Use the NewWHO Child Growth Standards’and provided clarity on the WorldHealth Organization’s new stan-dards and an orientation to theonline tools available to analyzesurvey databases.
Forward-looking themes and pro-jections of Africa’s future charac-terized the two roundtable panelpresentations that closed the pro-ceedings. One roundtable panelwas on public-private partnershipsand included speakers from GAIN,Unilever, Nestlé, the World FoodProgramme and UNICEF in aninteractive discussion about im -proving nutritional health in Africa.The other roundtable panel consid-ered research and training needs forthe nutrition profession in Africa. Itdrew together the experiences of
the Nutritional Leadership Programin Africa and comparisons withother efforts across the continent aswell as in the USA and the UK.
Free-paper program
Interspersed among the invited pre-sentations, the organizers pro-grammed almost 200 free-paperssubmitted by students, younginvestigators and seasoned profes-sionals from around the world.Sixteen oral-presentation sessionson free-papers were presented,which numbered a total of 87papers. Of these, 15 were explicitlyrelated to micronutrients of interestto the readership of the Magazine(Box 2). Specifically named inthese free-paper titles were multi-ple micronutrients (four papers),iron (four papers), zinc (twopapers), and ascorbic acid, folicacid, and iodine (one paper each).
A total of 98 free-papers wereincluded in the poster sessions(Box 3).Vitamin A is mentioned infour, iron in three, zinc in two, and
• Clinical rickets in rural Kenyan preschoolers• Goiter and iodine status in Bedouin children living insouth Sinai
• Prevention of neural tube defect by identifying lowfolate intake in Egyptian women
• Food insecurity is associated with food consumptionpatterns and anthropometric measures but not serummicronutrient levels in adults in rural Tanzania
• Moringa oleifera leaf improves iron status of intakesaged 6–12 months in Nigeria
• Analysis of protein and mineral content of dark cocoadrink: possible benefits for cardiovascular health
• Dietary zinc intakes and serum concentrations ofschool children aged 5–10 years in central Uganda
• Zinc deficiency among primary school children of arural coastal community in north Eastern Kentira,Morocco
• Assessment of iron status and anemia among school-age children in rural communities in Nigeria
• Impact of maternal deficiency of iron, calcium andmagnesium on pregnancy outcome in Mallawy,District, El Minia Governate, Egypt
• Serum ascorbic acid levels in third trimester of preg-nancy and ascorbate content of maternal breast milk
• Maternal micronutrient levels and risk of neural tubedefects on the newborn: A retrospective study
• Intake of selected nutrients among asymptomaticHIV-positive pregnant adults from two socioeconom-ically disparate Ghanian settings
• Food-based strategy to improve iron status of preg-nant women in Nigeria
Box 2: Free-paper themes explicitly related to micronutrients in the oral presentation program

Magazine Issue 1/2009ANEC III
45
iodine, folic acid, vitamin B12 andvitamin C in one each among thetitles. A multiple micronutrientcontext was explicit in one title andimplicit in another.
Conclusions
The shores of the Nile and theshadow of the Pyramids of Gizarepresent a splendid setting for anyevent. This meeting in Africa wasmade all the more impressive bythe diversity of geographical repre-sentation, superb organization, andbroad development of the program.The ANEC III program gave a seri-ous and contemporary treatment torelevant nutritional and publichealth problems affecting Africawith rigorous and scholarly evi-dence. The organizers took a big-tent approach in two important andfavorable respects. Although themeeting was dedicated, in name, to nutritional epidemiology, allaspects of nutrition from biochemi-cal to clinical to population wereincluded. Moreover, the participa-tion of private and corporate enti-
ties, both in final sponsorship andplenary presentations, advanced thereality of private-academic-publicpartnership.
Authors’ acknowledgements
We are grateful to SIGHT ANDLIFE, INF, IUNS, Unilever and all
other sponsors for granting fellow-ships to many of the participants toattend ANEC III, which gave us theopportunity to meet, share knowl-edge and create networks withstakeholders from around theworld.
Former participants of the African Nutrition Leadership Program attendingthe ANEC III
• Contribution of food-based interventions to the con-sumption of vitamin A-rich foods among children6–36 months of age in Salelugu-Nanton District ofNorthern Ghana
• Provitamin A carotenoids content of dried fermentedcassava roots: Influence of food fortification
• Effect of steam-drying on the content of β-carotene,vitamin C and total lipids in squashes (Cicurita spp.)from Cameroon
• A study on iodine stability under different storageconditions
•Wild leafy vegetable consumption in the BuheraDistrict of Zimbabwe: A potential means of improv-ing micronutrient nutrition in resource-poor commu-nities in developing countries
• The impact of consumption of traditional Food Multi-Mix (FMM) recipe on serum ferritin and iron nutri-
tional status among low-income pregnant women inGauteng, South Africa
• Production and acceptability of Edam cheese fortifiedwith zinc
• Homocysteine: Vitamin B12 and folic acid plasmalevels in relation to cognitive function in Egyptianelderly group
• A study of anemia among pregnant women inOuagadowgoa: Links with diet and consequences forfetal growth
• Iron and zinc nutritional status of women in theirreproductive age in urban Africa
• Maternal vitamin A deficiency during pregnancy: A disaster waiting to happen
• Infant and follow-up milk-based formula and ironfortification in relation to iron deficiency in Egypt
Box 3: Free-paper themes explicitly related to micronutrients in the poster presentation program
SIGHT AND LIFE Congress of Dietetics
46
Dietitians and nutritionists from around the world con-vened, shared research findings, and discussed issues,policies and education relating to nutrition and theactivities of dietitians at the 15th InternationalCongress of Dietetics (ICD), held in Yokohama,Japan, on September 8–11, 2008.
On the theme, ‘Global Dietetic Linkage andCooperation for Human Health,’ the congress exploredapproaches to new solutions to global food and nutri-
tion issues. A particular focus was the double burdenof malnutrition, where both over- and undernutritionaffects the same population. Lifestyle-related chronicdiseases are no longer only a problem among devel-oped country populations, they are also increasinglyaffecting rapidly urbanizing developing country popu-lations. The globalization of diets, both healthy andharmful, requires global cooperation to ensure ade-quate nutrition and health among all populations.
Programs on various topics in dietetics were organ-ized during the congress. Program sessions consistedof lectures by high-profile speakers from around theworld on the latest topics in nutrition and food, clini-cal nutrition, food service management, public healthnutrition, education, and dietetics skills. The congresscreated opportunities for participants to present onand share their activities and experiences, and to dis-cuss topics with experts from various sectors.
The International Congress of Dietetics is an interna-tional conference held every four years by theInternational Confederation of Dietetic Associations(ICDA). ICDA is comprised of national dietetic asso-ciation members from around the world, representingabout 150,000 dietetics professionals. The firstInternational Congress of the ICDA was held in 1952in the Netherlands; successive Congresses have con-tinued to serve as a way for members to meet andreceive support from beyond national and regionalboundaries.
Report on the 15th InternationalCongress of Dietetics Yokohama, Japan
Cao Thi Thu HuongNational Institute of Nutrition, Hanoi, Vietnam
Correspondence: Cao Thi Thu Huong, National Institute of Nutrition(NIN), Department of Micronutrient Research and Application, 48 Tang Bat Ho Street, Hanoi, VietnamEmail: [email protected]
Delegation of NIN attending the ICD. From left toright: Pham Van Thuy, Nguyen Thi Lam, Cao ThiThu Huong, Pham Thu Huong, Vu Thi Thu Hien
SIGHT AND LIFE Magazine 2009;1:46
Magazine Issue 1/2009FINSA
47
able development programs. Train -ing in nutrition and food science forthe different participants contribut-ing directly or indirectly to thisdevelopment represents one certainway of achieving this integrationand, in turn, reducing the effects ofmalnutrition in Africa. To this end,the Department of Nutrition andFood Science, at the Faculty ofAgronomic Sciences at Abomey-Calavi University in Benin, hasbeen running a program ofInternational Training in Nutritionand Food Science (known under itsFrench acronym, FINSA) since1992.
The implementation of this trainingprogram resulted from recommen-dations made at a regional seminarto introduce education on humannutrition in agricultural training.This seminar was organized jointlyby the United Nations Food andAgriculture Organization (FAO),the International Course in FoodScience and Nutrition at theInternational Agricultural Centre(ICFSN/IAC, Wageningen, theNetherlands), and the Faculty ofAgronomic Sciences (FSA) in
Cotonou, and held on 11–13 No -vember 1987.
FINSA 2008 took place at the FSAfrom 18–30 August 2008 andincluded three courses:
• Food and Nutrition Security andDevelopment: the Impact of theHIV/AIDS Pandemic;• Infant Nutrition, Care of Chil -dren of Mothers Affected byHIV/AIDS, and Production ofSupplementary Foods; and• Planning of Community NutritionPrograms (CNPs)
Context of the training
The food crisis in Africa is a majorconcern of governments, NGOsand development partners. Toreduce the effects of food and nutri-tion insecurity due to the ever-increasing rate of infection anddeath, and low productivity, institu-tions and public authorities havestarted implementing various pro-grams of action in various fields,including nutrition, public health,environment, and livelihoods. Theaims of such programs are to
Introduction
The food and nutrition situationamong populations in sub-SaharanAfrica remains of concern and isaggravated by the dual action ofdemographic growth and degrada-tion of the ecological bases of foodproduction.
To deal with this situation, it isincreasingly being recommendedthat food and nutrition considera-tions be integrated into all sustain-
Training in Nutrition and Food SciencePlanning of Community Nutrition Programs
Nada BenajibaAssociation Marocaine de Solidarité et de Développement (AMSED)et Equipe de Recherche en Nutrition et Alimentation, Rabat,Morocco
Correspondence: Nada Benajiba, Association Marocaine deSolidarité et de Développement (AMSED) et Equipe de Rechercheen Nutrition et Alimentation, Ibn Tofail University, 65 Avenue JohnKennedy, 10000 Rabat, MoroccoEmail: [email protected]
Installation in areas of data col-lection and getting ready forfield work
SIGHT AND LIFE Magazine 2009;1:47–49
SIGHT AND LIFE FINSA
48
achieve poverty reduction based on strong communityparticipation. Toward this, UN agencies and otherinstitutions have put into place CNPs in severalAfrican countries. Following comparative evaluationstudies of these programs, shortfalls were revealed interms of planning, implementation, and monitoringand evaluation. These shortfalls may be corrected, inpart, by training CNP managers.
Through short regional training courses on the plan-ning of CNPs, FINSA equips participants with the nec-essary tools so they can subsequently undertake effec-tive interventions to guarantee food and nutrition secu-rity at the local level, within a context of sustainabledevelopment.
Objectives
FINSA’s objectives are to:
• provide participants with knowledge of the methodsused in identifying food and nutrition security prob-lems;• enable participants to empower the community;• enable participants to design and plan a food andnutrition security program;• provide participants with a global understanding ofCNP implementation; and• increase participants’ capacities in CNP monitoringand evaluation.
Participants
A total of 16 participants from Niger,Cameroon, Burkina Faso, Guinea, Mali,Senegal, Cote d’Ivoire, and Morocco attend-ed this course. Participants came from differ-ent backgrounds and affiliations, includingdoctors in public health, nutritionists, andmanagers of NGOs for development andinternational affairs. This diversity resultedin extraordinary exchanges during discus-sions in the different course sessions. Theadditional expertise of different membersaided the development of the interventionstrategy for a CNP.
Overview of training
The training was participative and gave pri-ority to field work. It comprised sessions thatclarified and provided knowledge, case stud-
ies and group work. Training took place over a two-week period, characterized by an impressive amountof information and knowledge. Highly qualified train-ers facilitated the different sessions, favoring a partic-ipative approach involving exchange and communica-tion between participants. The course was organizedaround two modules:
Module 1: Process of planning CNPs
The module contained theoretical sessions on the mon-itoring of food and nutrition security programs, advo-cacy in nutrition, nutrition in emergency situations,and the impact of HIV/AIDS on food security in urbanhouseholds. During this module, the experience of theNGO, PLAN Benin, regarding community nutrition inthe country was presented. The focus was on the CNP,which is a set of activities aimed at resolving nutrition-al problems within a community with its full participa-tion and cooperation. These programs can improve thenutritional situation in many countries, provided theyare community-based.
The key factors for a successful CNP include respond-ing to the community’s dominant problems, involvingother development sectors, and using local resources.Home visits are essential in terms of monitoring theimplementation of the CNP within the community. Aparticipatory approach is essential and a determiningelement in the success of any CNP because programimplementation will be easier with the support of thecommunity, which must be involved from the initialconceptualization of the CNP and consideration of:
The most touching moment of the FINSA. Picture taken atthe end of the field work witnessing the human and effec-tive relationship which was developed with members ofHouékèhonou village.
Magazine Issue 1/2009FINSA
49
• making optimum use of local knowledge;• limiting dependence on external resources;• promoting leadership within the community;• adapting programs to the socioeconomic and culturalcontext and conditions;• enhancing service access for vulnerable people; and• incorporating the CNP in the global developmentplan.
The planning of nutritional interventions at the villagelevel is carried out in accordance with the 3A cycle(Assessment, Analysis and Action). The CNP planningprocess identifies and analyzes the problem, definesdifferent strategies and feasibility criteria, and thendevelops a plan of implementation.
Module 2: Implementation, monitoring and evaluationof a CNP
This module gave participants the opportunity tofamiliarize themselves with different techniques,methods, and participative approaches to implement aCNP at the local level. Participants went through thewhole process of planning a CNP, starting from theidentification of the problem to the development of afull intervention strategy, with the complete participa-tion of the concerned community. Participants wereasked to develop a CNP in the village ofHouèkèhonou.
The process of developing a CNP follows a sequenceof activities that starts with a preparatory phase duringwhich the teams contact the representatives of the vil-lage and provide information on its activities.Questionnaires to identify potential food security prob-lems facing the community are pre-pared based on a detailed study ofthe village. Data collection follows,with teams carrying out the surveysand collecting complementaryinformation. Analysis of the resultshelped to determine the interven-tion required and ways to involvethe villagers in the strategy to bedeveloped; this was followed bycommunity consultations that ledto the finalization of the strategyand the program.
Certification
At the closing ceremony of the training program, cer-tificates of participation were awarded to participantsby the former dean of FSA and founder of FINSA, thevice dean of FSA, and the director of FINSA.
Conclusion
My participation in FINSA contributed considerably tomy advancement and benefited me on different levels.On a professional level, it has helped me to gainknowledge in the planning of CNPs, which comple-ments my training in nutrition. The course improvedmy understanding of the importance of communityinvolvement during the whole planning process. Theirinput largely facilitated the development of the inter-vention strategy. Moroccan delegates attended thisFINSA course for the first time in 2008. The estab-lished contacts will ensure closer cooperation andsharing of experiences between countries in NorthAfrica and sub-Saharan Africa.
On a personal level, visiting the village and communi-cating with the villagers was a wonderful experiencewhich motivates me to further commit myself in con-tributing to the nutrition agenda in Africa.
Acknowledgements
Special thanks to SIGHT AND LIFE and NestléFoundation for the financial support, to Mrs NajatSarhani (AMSED) for the institutional support, andProf. Hassan Aguenaou (Ibn Tofail University) for theacademic and scientific supervision.
Group work preparing the CNP for Houékèhonou village
SIGHT AND LIFE In Memoriam
50
Norman Irving Krinsky, a scientistwho led the field of carotenoidresearch to unexplored places,passed away on November 28,2008, after more than a half centu-ry of dedication to research withthese plant pigments. Dr Krinskygave his gift of looking at nature’syellows, oranges and reds, and dis-covering the secrets to their impor-tance in our lives. Few researchpublications on carotenoids will notinclude a reference to Dr Krinsky’swork.
Born in Michigan’s Upper Penni -sula, Dr Krinsky (or Norman, as hewas known to both impressionable
graduate students and professorsalike) grew up in Chicago andbegan his college education at theage of 16 years at the University ofIllinois at Urbana-Champaign. Atthe time, he was not particularlysure of where he wanted to focushis studies. His interests weremany and varied. He was not a par-ticularly scholarly student, receiv-ing his first ‘A’ in psychology.
However, this changed with hisparents’ move to California.Norman’s search for directionfound him moving to the WestCoast in his junior year. The inter-section between Norman and bio-chemistry began at the Universityof Southern California, where hereceived a BSc and MSc in this
field. During his master’s degree,in his collaborations with Harry J.Deuel, a noted lipid biochemist, helearned a standard that carried himthrough his career: “If something’sworth doing, it’s worth doingright.”
To our fortune, he found a lot of“somethings” to do with caro -tenoids. This began in 1952, whenhe was awarded a PhD in biochem-istry with a dissertation entitled‘Studies of Carotenoid and VitaminA Complexes with Protein inPlasma and Tissues.’ In this work,Norman explored the transport ofvitamin A and carotenoids in plas-ma of several species. It was novelwork at the time as the biologicalimportance of carotenoids to
A Scientist Who Added Color to theWorld of Carotenoid Research: Norman I. Krinsky, 1928–2008
Elizabeth J. Johnson, Guangwen Tang, Kyung-Jin Yeum, XiangDong Wang, and Robert M. RussellTufts University, Jean Mayer USDA Human Nutrition Research Centeron Aging, Boston, USA
Correspondence: Robert M. Russell, Tufts University, Jean MayerUSDA Human Nutrition Research Center on Aging, 711 WashingtonStreet, Boston MA 02111, USAEmail: [email protected]
“The real voyage of discovery consists not in seeking new land-scapes but in having new eyes.”
Marcel Proust
SIGHT AND LIFE Magazine 2009;1:50–53
Magazine Issue 1/2009In Memoriam
51
health, beyond a vitamin A role, was not well recog-nized.
This interest in the biochemistry of carotenoids was anideal platform for the next phase of his illustriouscareer. In 1953, an opportunity brought Norman acrossthe country to Harvard University. As a US PublicHealth Service Postdoctoral Fellow, he worked withGeorge Wald, who received a Nobel Prize in Medicinefor his work with vitamin A and vision. Norman con-tinued his work with Wald with a postdoctoral fellow-ship from the National Council to Combat Blindness.In their work together, they investigated vision in avariety of species, including the frog (from whichNorman enjoyed a nice repas of legs after the experi-ments were completed).
The experience at Harvard was one that Norman trulycherished. He easily settled into the intellectual envi-ronment of the University. Cambridge fed into hisbroad interests, which included both the sciences andnon-sciences. He was at Harvard for seven years, dur-ing the latter part of which he discovered his love ofteaching while serving as an instructor and lecturer inthe Department of Biology.
In 1960, Norman became an assistant professor at theTufts University School of Medicine, where heremained for the rest of his career. Norman realized inthese early days that the importance of carotenoidsspanned across many forms of life. His studies in algaeand bacteria laid down some of the ground work forthe biochemical conversions and function of variouscarotenoids in these organisms.1,2 Sprinkled through-out these decades were studies employing the conven-tional laboratory rat,3,4 evaluating β-carotene metabo-lism. His work with rabbits looked at the conversion ofcarotenoids to vitamin A and retinoic acid.5 The mon-key model allowed for exploration into the biologicalcontrol of carotenoids in the primate retina.6,7
However, it was his collaborations using the ferretmodel that were particularly interesting. This workspawned from the epidemiological studies had shownthat dietary and plasma levels of carotenoids wererelated to decreased risk of lung cancer. Contrary tothese observations, intervention studies using pharma-cological doses of β-carotene showed that smokerswere at a greater risk of lung cancer. Norman and hislongtime collaborators, Robert M. Russell and Xiang-Dong Wang, proposed that large doses of β-carotene,in an oxidatively stressed environment, e.g. smokers’lungs, were oxidized to compounds that were harm-ful.8
This was the beginning of the realization that, whiledietary intakes of carotenoids were probably protectiveagainst disease, pharmaceutical doses of β-carotenecould have adverse effects due to diminished retinoicacid receptor-β gene expression and overexpression oftumor promoting genes. In fact, when it came todietary carotenoids, Norman was known to say “Get itfrom your food.” There was no magic bullet in hismind. Norman continued with his collaborations withRussell and Wang with work on a second pathway bywhich carotenoids are broken down and the biologicalsignificance of this. Following the molecular identifi-cation of excentric carotene cleavage enzyme by vonLintig’s group in Germany, they cloned and character-ized this enzyme from ferrets and demonstrated thatthe enzyme effectively cleaved an excentric bond ofcis isomers of lycopene,9 which are the predominantforms of lycopene in mammalian tissues. This workprovided valuable insights into the mechanisms under-lying the actions of carotenoids via their metabolites.
An additional significant contribution that Normanmade to the field of carotenoids was his support of thestudies that evaluated the bioconversion of carotenoidsin various food vehicles to vitamin A. Norman, RobRussell, and Guangwen Tang at Tufts (as well as othergroups) showed that the bioavailability of vitamin Afrom β-carotene varied considerably from one foodsource to another. Prior to this work it was believedthat three molecules of β-carotene were equivalent toone molecule of vitamin A (6 to 1 by weight). Throughtheir studies in human subjects they found that theratio was actually much higher and varied, dependingon the food. For example, in spinach, the ratio was20:1.10 This led to the realization that not only was theamount of carotenoid contained in a food of impor-tance, but also the amount that was available forabsorption from the gut into the body. These findingswere of such importance that Norman was invited tochair the panel that set the recommended dailyallowance of antioxidants. The World Health Or -ganization changed its recommendations to 12:1 inlight of this work.11 The significance of this work can-not be underestimated given that vitamin A deficiencyis a major public health issue in developing countries,where the dietary source of vitamin A is primarilythrough carotenoid food sources.
In collaboration with Giancarlo Aldini at theUniversity of Milan and Kyung-Jin Yeum at Tufts,Norman developed a unique assay to measure antioxi-dant capacity in both the aqueous and lipid compart-ments of plasma.12 Unlike other assays, this assay cap-tures the antioxidant activities of fat-soluble antioxi-

SIGHT AND LIFE In Memoriam
52
dant nutrients (such as carotenoids) as well as water-sol-uble antioxidant nutrients in vivo. Furthermore, Normanand his colleagues demonstrated that the activities ofantioxidant nutrients in human plasma depend on thelocalization of attacking radical species, providinginformation for practical applications to optimizeantioxidant defenses in the human body.13
Norman did not limit himself to the study of a fewcarotenoids. He covered many, from astaxanthin14 tozeaxanthin.15 Work with astaxanthin and canthaxanthinfound these carotenoids to be potent antioxidant inmembranes.14 His work with the macular pigments,lutein and zeaxanthin16,17 helped in our understandingof factors related to the uptake of these carotenoids intothe eye, which is believed to be important to eye health.Studies using supplementatal lycopene found this toreduce lymphocyte DNA damage in postmenopausalwomen.18 Over the years, he collected the spectrum ofover 70 carotenoids, which are now available at DrKrinsky’s Notebook (http://hnrc.tufts.edu/11921096 8 7 0 3 6 /HNRCA -P a g e h n r c a 2w s _ 1 1 9 2 1 0 9687099.html). This website contains a treasure trove ofNorman’s handwritten notes and data needed to producethese spectra.
Apart from his work in the field of carotenoids andantioxidants, Norman was deeply interested in therecent advances of others. This was reflected in themany conferences and committees that he helped organ-ize. In 1981, the increasing interest in the field of freeradicals and related oxidants in relation to health anddisease initiated a Gordon conference on ‘Oxy-Radicalsin Biology and Medicine.’ Norman was a part of thisinitiative and was the first chair of a conference thatcontinues today. By the early 1990s, the nutritional sci-ence community realized that there were carotenoids ofinterest beyond the major ones found in diet and humantissues. This led to the initiation of another conference.In 1992, he chaired the first Gordon ResearchConference on the ‘Chemistry and Biology ofCarotenoids,’ which also continues to this day. Normanattended every one of these conferences except the last,in 2007, to which he attempted to go, but fell ill. Hisabsence was felt, as at these meetings he would be at thefront, intent on the topic at hand, ready with commentsand questions, often accompanied with tact and goodhumor.
From his early years at Harvard and throughout his richand colorful career at Tufts, Norman was continuallyinvolved with students and teaching. He loved theresearch, but was passionate about the teaching and hewanted others to carry on that passion. When he retired
from Tufts in 2001, he and his wife established theNorman & Susan Krinsky Excellence in TeachingAward for students in the Sackler School of GraduateBiomedical Sciences and the Medical School at Tufts.This award honors Norman’s 40 years of service in theSackler School and is meant to recognize individualswho have shown sustained teaching excellence. To date,this award has been presented to 15 PhD and MD stu-dents, in fields ranging from biochemistry to ge netics to immunology to microbiology and phar ma -cology.
Retirement came easily to Norman. His varied interestsfound him involved in a number of intellectual and com-munal activities, such as serving as a docent at theHarvard Semitic Museum and as an active member ofthe Wellness Community’s Men’s Cancer SupportGroup. He continued to be an engaged participant inresearch at Tufts, sharing his insights on the projects athand. All of this is a testament to his commitment tobeing a responsible member of the communities towhich he belonged.
Dr Krinsky continued his sincere, dedicated interest inand communication of carotenoids with publications upuntil the year of his death.19,20 These works were remi-niscent of those that began his career, with publicationsthat contained several co-authors – a testimony to hisgiving and sharing of his gift of bringing new eyes toview and study these special colors that surround us.
Norman passed away the day after Thanksgiving in2008, an occasion he celebrated with his loving family.He leaves his wife, a daughter and son, their spouses,and two grandchildren. His wit, wisdom, and wonderwill be missed by all.
Norman ‘by numbers’
• 80 years of age 137 peer-reviewed publica-tions• 56 years in carotenoid research 123 co-authors• 49 years at Tufts 112 times as an invitedspeaker• 47 journals published in 66 book chap-ters/invited reviews • > 30 carotenoids researched 33 professionalhonors• 13 professional society memberships 1st chairof Gordon Research Conference on Carotenoids • Contributions to carotenoid research: unlimited

Magazine Issue 1/2009In Memoriam
53
References
1. Krinsky NI, Goldsmith TH. The carotenoids of the flagellat-ed algae. Euglena gracilis. Arch Biochem Biophys1960;91:271-279.
2. Matthews MM, Krinsky NI. The relationship betweencarotenoid pigments and resistance to radiation in non-pho-tosynthetic bacteria. Photoche Photobiol 1965;4:813-817.
3. Krinsky NI, Matthews-Roth MM, Welankiwar S, SehgalPK, Lausen NCG, Russett M. The metabolism of [14C]-β-carotene and the presence of the other carotenoids in ratsand monkeys. J Nutr 1990;120:81-87.
4. Wang X-D, Tang G-W, Fox JG, Krinsky NI, Russell RM.Enzymatic conversion of β-carotene into β-apo-carotenalsand retinoids by human, monkey, ferret, and rat tissues.Arch Biochem Biophys 1991;285:8-16.
5. Wang X-D, Russell RM, Liu C, Stickel F, Smith D, KrinskyNI. β-Oxidation in rabbit liver in vitro and in the perfusedferret liver contributes to retinoic acid biosynthesis from β-apo-carotenoic acids. J Biol Chem 1996;271:26490-26498.
6. Snodderly DM, Shen B, Land RI, Krinsky NI. Dietarymanipulation of plasma carotenoid concentrations of squir-rel monkeys (Saimiri sciureus). J Nutr 1997;127:122-129.
7. Matthews-Roth MM, Welankiwar S, Sehgal PK, LausenNCG, Russett M, Krinsky NI. Distribution of[14C]canthaxanthin and [14C]lycopene in rats and mon-keys. J Nutr 1990;120:1205-1213.
8. Wang X-D, Liu C, Bronson RT, Smith DE, Krinsky NI,Russell RM. Retinoid signaling and activator protein-1expression in ferrets given β-carotene supplements andexposed to tobacco smoke. J Natl Cancer Inst 1999;91:60-66.
9. Hu KQ, Liu C, Ernst H, Krinsky NI, Russell RM, Wang X-D. The biochemical characterization of ferret carotene-9',10'-monooxygenase catalyzing cleavage of carotenoiddsin vitro and in vivo. J Biol Chem 2006;281:19327-12338.
10. Tang G, Qin J, Dolnikowski GG, Russell RM, Grusak MA.Spinach or carrot can supply significant amounts of vitaminA as assessed by feeding with intrinsically deuterated veg-etables. Am. J Clin Nutr 2005;82:821-828.
11. Vitamin and mineral requirements in human nutrition, 2nded. World Health Organization, Food and AgriculturalOrganization of the United Nations 2004.
12. Aldini G, Yeum KJ, Russell RM, Krinsky NI. A selectivefluorescence method to monitor aqueous and lipid plasmaoxidizbility. Free Radic Biol Med 2001;31:1043-1050.
13. Yeum K-J, Aldini G, Chung H-Y, Krinsky NI, Russell RM.The activities of antioxidant nutrients in human plasmadepend on the localization of attacking radical species. JNutr 2003;133:2688-2691.
14. Palozza P, Krinsky NI. Astaxanthin and canthaxanthin arepotent antioxidants in a membrane model. Arch BiochemBiophys 1992;297:291-295.
15. Krinsky NI, Landrum JT, Bone RA. Biologic mechanism ofthe protective role of lutein and zeaxanthin in the eye. AnnRev Nutr 2003;23:171-201.
16. Handelman GJ, Snodderly DM, Krinsky NI, Russett MD.Biological control of primate macular pigment.Biochemical and densitometric studies. Invest OphthalmolVis Sci 1991;32:257-267.
17. Hammond BR, Jr., Johnson EJ, Russell RM, et al. Dietarymodification of human macular pigment density. InvestOphthalmol Vis Sci 1997;38:1795-801.
18. Zhao X, Aldini G, Johnson EJ, et al. Modification of lym-phocyte DNA damage by carotenoid supplementation inpostmenopausal women. Am J Clin Nutr 2006;83:163-169.
19. Qin J, Yeum K-J, Johnson EJ, Krinsky NI, Russell RM,Tang G. Determination of 9-cis β-carotene and zeta-carotene in biological samples. J Nutr Biochem2008;19:612-618.
20.Muzhingi T, Yeum K-J, Russell RM, Johnson EJ, Qin J.Determination of carotenoid content in 46 yellow maizelines, and the effect of saponification and cooking oncarotenoid contents. Int J Vitam Nutr Res 2008;78:112-120.
For more on tributes to Norman Krinsky,see:
“Norman Krinsky: helped redefine diet guidelinesacross globe” Boston Globe, 10 December 2008(www.boston.com/bostonglobe/obituaries/articles/2008/12/10/norman_krinsky_helped_redefine_diet_guidelines_across_globe/)Oxygen Club of California News:www.oxyclubcalifornia.org/occ_news.cfm,December 2008“Norman Krinsky, A Pioneering Biochemist”Tufts Medicine, Tufts Medical Alumni Associa -tion and Tufts University Office of Publicationsvol 68 (1), p 34 (2009)
SIGHT AND LIFE In Memoriam
54
John Beard, one of the world’smost renowned iron researchers,died February 13, 2009. Hereceived his MS in biochemistryfrom the University of Californiaand his PhD in nutrition fromCornell University. He served as aPenn State faculty member for thepast 25 years and was recentlynamed ‘Distinguished Professor’in the Nutritional Sciences depart-ment this past December. Johnwas a well-respected colleaguewith a genuine desire to providethe highest quality teaching andresearch opportunities to bothgraduate and undergraduate stu-dents. He had an unparalleledcommitment to science, his col-leagues, and his students.
In Memoriam: John Lawrence BeardOctober 30, 1947 – February 13, 2009
Laura E. Murray-KolbDepartment of International Health, Johns Hopkins BloombergSchool of Public Health, Baltimore, USA
Correspondence: Laura E. Murray-Kolb, Center for HumanNutrition, Department of International Health, Johns HopkinsBloomberg School of Public Health, 615 North Wolfe Street,Baltimore, MD 21205, USAEmail: [email protected]
John was considered to be one of the most influential and well-respect-ed experts in the world today on iron in the brain and neurobehavioralfunction. His research has been instrumental in changing the way scien-tists think about how the brain uses iron, it has influenced approaches todietary supplementation in developing countries, and has offered newperspectives for the treatment of clinical disorders. In addition to under-standing the correlation between iron and brain function, John was mostinterested in translating these findings into ‘real world’ applications, inorder to help those most in need. Some of his recent research on studiesassessing the usefulness of iron fortification in staple foods such as riceand beans has had profound public health implications. He has alsorecently demonstrated the importance of iron status in postpartumdepression and the impact of iron in Restless Legs Syndrome.
John was known to conduct studies of the highest quality and findingsfrom his studies were often cited and used when setting public policy.Additionally, his knowledge of iron biology and the impact of iron defi-ciency on human health were highly sought after as evidenced by theconstant invitations that he received to speak at national and internation-al meetings. He was known for ‘thinking outside the box’ and providinga rational, objective viewpoint. His findings have been published inmore than 150 peer-reviewed manuscripts – including more than 60 arti-cles in the past five years alone. As he was in the midst of conductingand writing up findings from multiple other studies, his name willundoubtedly appear on many more research articles to come.
In addition to outstanding teaching and research contributions, John wasgenerous with his service to the field. He was President-elect of theAmerican Society for Nutrition, a member of the American Journal ofNutrition and the Journal of Nutrition editorial boards, an associate edi-tor of the Journal of Nutrition for the past nine years, and chaired sever-
SIGHT AND LIFE Magazine 2009;1:54–55
Magazine Issue 1/2009In Memoriam
55
al committees. Additionally, he served on committeesof many other national as well as international publichealth organizations.
While his professional accomplishments are remark-able, those of us privileged to have called him ourmentor recognize that it was the everyday manner inwhich he conducted himself which is his greatestlegacy. Among the students at Penn State, Dr Beardhad the reputation of being intimidating as a result ofhis deep knowledge of the field and his uncanny abil-ity to formulate questions that required a great amountof thinking in order to provide an adequate answer.Because his reputation preceded him, most of his
graduate students were rather anxious the first timethey met him. I remember well the nervousness that Ifelt the first time I walked into his office to discuss hisresearch and the possibility of becoming his graduatestudent. I quickly learned that his reputation as anincredibly intelligent and articulate scientist was welldeserved. However, what also came across was hispassion for the field and his desire to impart hisknowledge to others. While I was still rather intimi-dated, I started to sense that underneath it all, he careddeeply. That was 13 years ago, and in the ensuingyears, John became one of my favorite people.
Over the last 13 years, I have worked closely withJohn on many projects, including studies of iron andcognition in the USA and South Africa, and studies oniron biofortification in the Philippines. As such, I’vehad many opportunities to witness John’s character,firsthand. I learned that despite his many accolades,John was a humble person, eager to impart his knowl-edge to others, and always kind to everyone. He wasexcited to watch my own knowledge grow and pushed
me to my limit, constantly encouraging me toimprove, and always believing that I could reach thatnext level.
One of John’s greatest gifts to his students was the giftof time. He had an ‘open door’ policy with his stu-dents. During my seven years as his graduate student,John never once told me that he didn’t have time forme. As a result, I have spent many, many hours in hisoffice, discussing issues, wrestling with problems,and agonizing over decisions, during which time hepatiently listened and guided me. I learned so verymuch from him during those times.
Even after graduating and moving on, John kept inclose touch. It became very evident to me that Johnwas eager to see his students succeed and was soproud of their accomplishments. He continued to offeradvice and encouragement and act as a soundingboard. But, John went above and beyond, caring aboutour personal lives in addition to our professional lives.During every conversation, he would ask me how myhusband was doing and he called multiple times theweek after my son was born to make sure that momand baby were doing fine. Since then, he was eager tohear about every ‘milestone’ that my son reached.John was a phenomenal and tough mentor to his stu-dents who taught us as much about life as he did aboutscience. I have no doubt that my professional success-es are a direct result of the time that he invested in meand I will be forever grateful for that.
John’s direct legacy on this earth ended much toosoon for our liking. But, each of us who knew andlearned from him has the opportunity to ensure thathis indirect legacy continues. This will occur everytime we patiently guide our students, enthusiasticallyimpart our knowledge to others, passionately conductour research, labor over the wording of a grant until itis just right, or publish our research findings – as Johnalways reminded us, “It’s not really research until it’spublished!”
Although John gave tirelessly of himself in order toadvance the nutrition field, his first passion was hisfamily. John is survived by his wife, Diane Brannon,and sons, Zachary and Matthew Beard. His love forthem was evident by the proud manner in which heconstantly spoke of them and the gentle way in whichhe interacted with them. John was truly a remarkablehusband, father, scientist, colleague, mentor, andfriend. He will be sorely missed.
John Beard (left) with Xingen Lei at the banquetof the last Trace Elements in Man and Animals(TEMA) conference, Pucon, Chile, 2008

My responsibilities in my new jobfall into two main areas. Within theframework of the DSM-WFP part-nership, my role is to provide tech-nical expertise concerning the stud-ies and programs which are con-ducted. I am therefore responsiblefor ensuring that such studies andprograms are properly designed,implemented and evaluated.
I also have to ensure that the dataprovided is analyzed using appro-priate and accurate methodologies,so that well-founded conclusionsmay be drawn from the informationcollected. The dissemination of
information is also an importantpart of my role, which means that Ido a lot of writing and also liaiseclosely with the relevant institu-tions and publications.
Simple messages
I also have a separate role withinSIGHT AND LIFE. I am responsi-ble for developing information,communication and educationmaterials on a range of nutritionaltopics including nutritional anemia,hidden hunger and micronutrientpowders. A lot of these subjects arehighly complex, so my job is totranslate the advanced scientificconcepts into easily accessibleterms. We need simple messagesfor the beneficiaries of programs indeveloping countries, and so I haveto make this material easy to under-stand. I also help with the editing ofSIGHT AND LIFE magazine andwill be working closely with thesummer intern who will be comingfrom Johns Hopkins University toevaluate grant applications. So bothmy roles are very interesting andoffer me a great deal of variety.
My background is in internationalnutrition. My Bachelor’s degree
was in Food and Nutrition fromEwha Women’s University inSeoul, Korea. My Masters was inFood Science and Human Nutritionfrom the University of Illinois atUrbana-Champaign, and my Ph.D.was in International Nutrition fromJohns Hopkins Bloomberg Schoolof Public Health in Baltimore,Maryland. I did an internship withSIGHT AND LIFE last year,spending much of my time evaluat-ing grant proposals, and I enjoyedthis very much. I was thereforeextremely interested in the opportu-nity of coming back to Switzerlandto work in this newly created role.
Improving the WFP’s foodbasket
Much of my time at the moment isspent on supporting the efficacytrial for NutriRiceTM which we willbe conducted in India. Our object isto demonstrate the efficacy andeffectiveness of this specially forti-fied form of rice: this is a prerequi-site for the inclusion of such prod-uct in the WFP’s food basket,which helps to provide nutrition toapproximately 90 million of theworld’s most impoverished peo-ple. I therefore work very closely
SIGHT AND LIFE A Day in the Life
56
Meet the SIGHT AND LIFE Teamin Kaiseraugst
Jee Hyun Rah, MS, PhD, joined SIGHT AND LIFE as NutritionManager for DSM’s partnership with the United Nations WorldFood Programme (WFP) in February 2009. She talks about her role,which is a new one within SIGHT AND LIFE.
Jee Hyun Rah
SIGHT AND LIFE Magazine 2009;1:56–58

Magazine Issue 1/2009A Day in the Life
57
with Klaus Kraemer, Anne-Catherine Frey andSvenia Sayer-Ruehmann. I also have close contactwith numerous colleagues from DSM and with thepeople running the NutriRiceTM trials in India.
Working for SIGHT AND LIFE means a great deal tome. Despite its small size as an organization, SIGHTAND LIFE plays an enormously influential role ininternational nutrition and has terrific potential fordoing good in the world. Scientists and other academ-ics are continually developing new insights into therelationship between nutritional intake and health,and these insights need to be communicated in clear-ly intelligible form to the people who are runningprograms in the field. I enjoy reading SIGHT ANDLIFE magazine and am particularly looking forwardto helping with the editing of it. It is a great source ofnew knowledge in the field of international nutrition,but I think it could do even more to bridge the gap
between academia on the one hand and programs inthe field on the other.
And another thing dear to my heart…I very much enjoy living in Switzerland, but the restof my family is in South Korea, where I grew up. Itherefore spend a lot of my free time staying in touchwith them. Before dedicating myself very intensely tothe study of international nutrition, I used to be a jazzpianist. With my PhD behind me now, I am lookingforward to the opportunity to play jazz piano oncemore, which is very dear to my heart.
Anne-Catherine Frey and Svenia Sayer-Ruehmann, assistants
To have a real influence in the world, SIGHT ANDLIFE has to operate very efficiently and make themaximum use of its resources. This would be unthink-
Helping to Build StrongerSocieties
DSM’s partnership with the United NationsWorld Food Programme
‘We cannot be successful, nor can we call ourselvessuccessful, in a society that fails’
Feike Sijbesma, CEO DSM
DSM’s belief in the importance of building success-ful societies is the inspiration for our partnership withthe United Nations World Food Programme (WFP).Hunger is the number one cause of death in theworld, killing more people than AIDS, malaria andtuberculosis combined. A related global scourge is atype of under-nutrition referred to as hidden hunger,whereby people have enough food to survive, buthave access only to a diet which lacks key(micro)nutrients. ‘Hidden hunger’ is associated witha wide range of chronic diseases as well as physicaland cognitive underdevelopment. As the world’slargest manufacturer of micronutrients and vitamins,DSM is strongly committed to help in the fightagainst global hunger.
The largest humanitarian agency in the world, WFPprovides food aid to an average of 90 million people,including 58 million hungry and malnourished chil-dren, in 80 of the world’s poorest countries. By sup-
porting WFP in defining a (micro)nutrient strategy,we support the building of stronger societies that canmake a positive contribution to the world economy inyears to come. This requires creating a global alliancecomprising a wide variety of stakeholders such asUNHCR, UNICEF, WHO and GAIN (GlobalAlliance for Improved Nutrition) who are dedicatedto helping meet the needs of the ultra-poor.
In 2008 WFP and DSM received recognition for theirrole in these efforts in the form of an ICIS(International Chemical Information Services)Innovation Award. This was given for the develop-ment of MixMe™ micronutrient sachets.
Initiated in 2007, our partnership with WFP led toactivities on many fronts during 2008. Drawing onthe expertise in micronutrient science of SIGHTAND LIFE as well as the support of our commercialNutrition Improvement Program (NIP), we providedmuch-needed assistance in Bangladesh, Kenya,Nepal and Zambia, as well as supporting WFP at itsheadquarters in Rome. DSM employees and seniormanagers made their professional skills and experi-ence available in a range of projects run by WFP,reporting back on their experiences in widely readweb logs.
Source: The DSM Triple P Report 2008

able without the efforts of ourassistants Anne-Catherine Frey andSvenia Sayer-Ruehmann. Anne-Catherine and Svenia talk abouttheir daily work in our offices inKaiseraugst, Switzerland.
Anne-Catherine has been withSIGHT AND LIFE since 1999 andSvenia since 2006. Anne-Catherineworks four days a week and Sveniatwo, dividing between them themany tasks necessary for thesmooth operation of our organiza-tion.
“A lot of our work involves thebasic administration which youwould expect to be necessary with-in any comparable organization,”says Anne-Catherine. “We support
Klaus Kraemer in many ways –organizing his diary, for instance,and making his travel arrangementsfor him. Klaus travels extensivelyin his role as Secretary General ofSIGHT AND LIFE, and his workwould not be possible withoutextensive support from the officehere.
“We help to arrange meetings andconferences, to develop presenta-tions, to update the SIGHT ANDLIFE website, to maintain theSIGHT AND LIFE archive, andalso, of course, to put togetherSIGHT AND LIFE Magazine. Thisinvolves liaising with contributorsas well as with our graphic designagency and printer. We are alsoresponsible for organizing ship-ments of educational material andmicronutrient sachets and payingthe grants without which the bene-ficiaries of our programs would notbe able to do their work in the field.
Mission-critical
“This element of our work is mis-sion-critical: when we make a ship-ment, we know that there are peo-ple waiting eagerly for the goods toarrive and when we make a grantpayment we know that there arepeople equally eagerly awaiting thearrival of the funds, without whichthey cannot deliver their programs.It can be difficult and time-con-
suming to deal with thecustoms authorities,but this is some-thing we have toaccept as part andparcel of ourwork.”
“We work on the third floor of theheadquarters of DSM NutritionalProducts, which is situated inKaiseraugst near Basel, Switzer -land,” says Svenia. “We haverecently moved across the corridorfrom a small office to a bigger oneand are in the process of personal-izing our new space with picturesof projects from all around theworld. It’s terribly important for usto see the results of our work in thefield. We are based here inSwitzerland, but we always enjoyhearing about what SIGHT ANDLIFE is doing worldwide, whetherthe news comes via email, letters orphotographs, or in the form ofKlaus’s reports when he returnsfrom his travels abroad.
Making a positive difference
“I think it’s very important to bothof us to have a job which is not onlyinteresting and varied but whichalso gives us the opportunity tomake a positive difference in theworld. If there was one thing Icould change about my job, I wouldincrease the budget available toSIGHT AND LIFE and expand thestaff. We are a very small team butI believe that we are a real force forgood.”
SIGHT AND LIFE A Day in the Life
Anne-Catherine Frey
Svenia Sayer-Ruehmann
58

Magazine Issue 1/2009Monitoring Anemia-Control
59
Background
Iron deficiency, with or withoutiron-deficiency anemia, affects allpopulations of the world irrespec-tive of race, culture or ethnic back-ground. Children, adolescentwomen and women of child-bear-ing age are especially prone todeveloping iron-deficiency anemia(IDA), and this is despite iron beingthe fourth most common elementon earth.1
Early estimates suggested iron defi-ciency was responsible for anemiain approximately 15% of theworld’s population and its overallprevalence was quoted to be around50% in developing and 10% indeveloped countries.2 This situa-tion has not improved and recentestimates put the worldwide preva-lence of anemia for the period1993–2005 at 24.8% and, in eachage and gender group studied, thehighest prevalence rates occurred
in Africa. Anemia is particularlycommon in infants and preschool-age children, with a global preva-lence of 47% but this reachesalmost 65% in Africa.3 Anemialeads to impaired physical workperformance, cognitive impair-ment, adverse pregnancy outcomesand developmental delays in tod-dlers.4
There is evidence that iron is need-ed for lymphocyte activation andproliferation as part of the acutephase response,5 but there is alsoevidence that iron deficiency maybe protective against infectious dis-ease1 or that excess iron is harm-ful6. Routine prophylactic supple-mentation with oral iron and folicacid or placebo to preschool chil-dren in areas with high malariatransmission was associated with a12% increase in morbidity and 15%more deaths in the iron recipients.7
In view of the conflicting factorsaffecting iron metabolism, it is
important that iron status is correct-ly monitored and the effects of irontreatment correctly interpreted.
Causes of anemia
While iron deficiency is the princi-pal cause of anemia there aremany other factors that con-tribute.8 Several micronutrientshave been shown to be directlyinvolved in hemoglobin synthesis,such as folate, vitamin B12, andcopper, but vitamin A deficiency(VAD) is the micronutrient de -ficiency most frequently associat-ed with iron deficiency. In a recentstudy on anemia-associated micro -nutrient deficiencies in Mexicanpreschool children, only 30% ofthose with iron deficiency did nothave a deficiency of retinol, folateor vita min C but VAD was moststrongly associated with iron defi-ciency in children both with andwithout anemia (Table 1).9
Monitoring Anemia-Control Programs
David I. Thurnham
Correspondence: David I. Thurnham, 46 High Street, LittleWilbraham, Cambridge CB21 5JY, UKEmail: [email protected]
Percentage with low plasma retinol concentration1
Iron deficient2,3 (N = 94) No iron deficiency (N = 50)Anemia 40.6 16.0No anemia 27.7 11.9
1 Plasma retinol concentration < 0.7 µmol/L2 Iron deficiency when % transferrin saturation < 16% and hemoglobin < 110 g/L3 Significantly higher prevalence of low plasma retinol concentration in both anemic and non-anemic children. From Villapedo et al9
Table 1: Anemia-associated micronutrient deficiencies in Mexican preschool children
SIGHT AND LIFE Magazine 2009;1:59–66
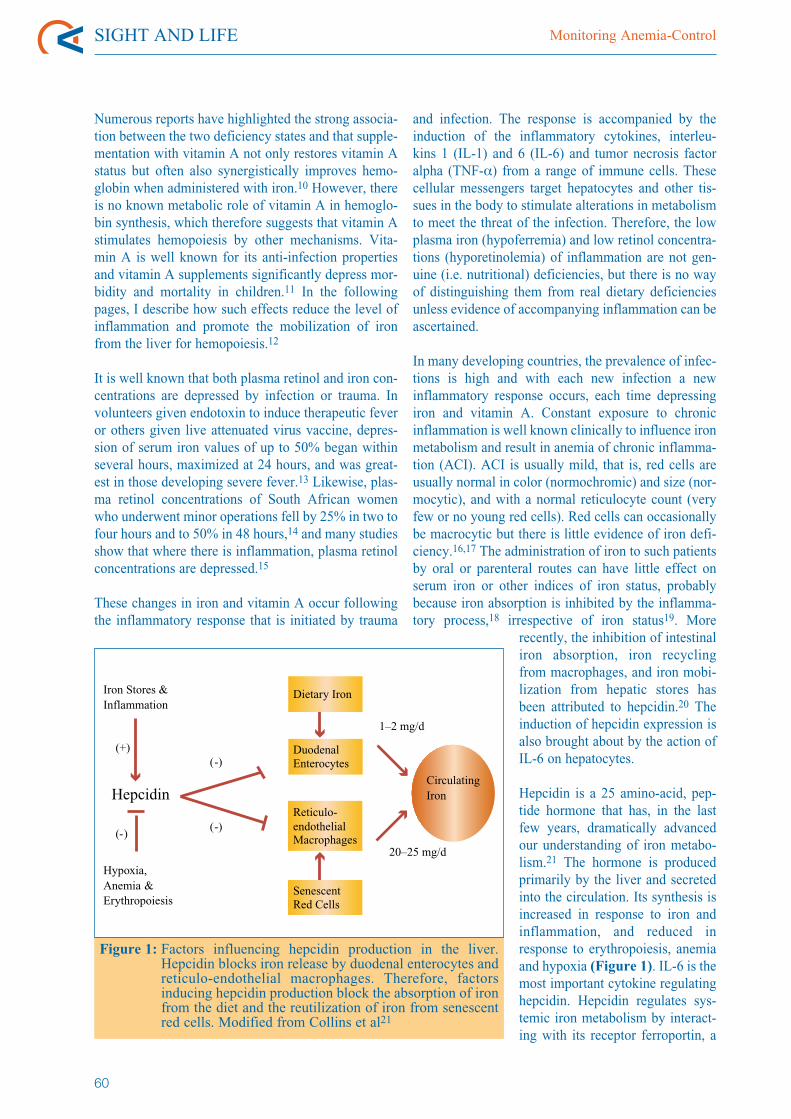
Numerous reports have highlighted the strong associa-tion between the two deficiency states and that supple-mentation with vitamin A not only restores vitamin Astatus but often also synergistically improves hemo-globin when administered with iron.10 However, thereis no known metabolic role of vitamin A in hemoglo-bin synthesis, which therefore suggests that vitamin Astimulates hemopoiesis by other mechanisms. Vita -min A is well known for its anti-infection propertiesand vitamin A supplements significantly depress mor-bidity and mortality in children.11 In the followingpages, I describe how such effects reduce the level ofinflammation and promote the mobilization of ironfrom the liver for hemopoiesis.12
It is well known that both plasma retinol and iron con-centrations are depressed by infection or trauma. Involunteers given endotoxin to induce therapeutic feveror others given live attenuated virus vaccine, depres-sion of serum iron values of up to 50% began withinseveral hours, maximized at 24 hours, and was great-est in those developing severe fever.13 Likewise, plas-ma retinol concentrations of South African womenwho underwent minor operations fell by 25% in two tofour hours and to 50% in 48 hours,14 and many studiesshow that where there is inflammation, plasma retinolconcentrations are depressed.15
These changes in iron and vitamin A occur followingthe inflammatory response that is initiated by trauma
and infection. The response is accompanied by theinduction of the inflammatory cytokines, interleu -kins 1 (IL-1) and 6 (IL-6) and tumor necrosis factoralpha (TNF-α) from a range of immune cells. Thesecellular messengers target hepatocytes and other tis-sues in the body to stimulate alterations in metabolismto meet the threat of the infection. Therefore, the lowplasma iron (hypoferremia) and low retinol concentra-tions (hyporetinolemia) of inflammation are not gen-uine (i.e. nutritional) deficiencies, but there is no wayof distinguishing them from real dietary deficienciesunless evidence of accompanying inflammation can beascertained.
In many developing countries, the prevalence of infec-tions is high and with each new infection a newinflammatory response occurs, each time depressingiron and vitamin A. Constant exposure to chronicinflammation is well known clinically to influence ironmetabolism and result in anemia of chronic inflamma-tion (ACI). ACI is usually mild, that is, red cells areusually normal in color (normochromic) and size (nor-mocytic), and with a normal reticulocyte count (veryfew or no young red cells). Red cells can occasionallybe macrocytic but there is little evidence of iron defi-ciency.16,17 The administration of iron to such patientsby oral or parenteral routes can have little effect onserum iron or other indices of iron status, probablybecause iron absorption is inhibited by the inflamma-tory process,18 irrespective of iron status19. More
recently, the inhibition of intestinaliron absorption, iron recyclingfrom macrophages, and iron mobi-lization from hepatic stores hasbeen attributed to hepcidin.20 Theinduction of hepcidin expression isalso brought about by the action ofIL-6 on hepatocytes.
Hepcidin is a 25 amino-acid, pep-tide hormone that has, in the lastfew years, dramatically advancedour understanding of iron metabo-lism.21 The hormone is producedprimarily by the liver and secretedinto the circulation. Its synthesis isincreased in response to iron andinflammation, and reduced inresponse to erythropoiesis, anemiaand hypoxia (Figure 1). IL-6 is themost important cytokine regulatinghepcidin. Hepcidin regulates sys-temic iron metabolism by interact-ing with its receptor ferroportin, a
SIGHT AND LIFE Monitoring Anemia-Control
60
Figure 1: Factors influencing hepcidin production in the liver.Hepcidin blocks iron release by duodenal enterocytes andreticulo-endothelial macrophages. Therefore, factorsinducing hepcidin production block the absorption of ironfrom the diet and the reutilization of iron from senescentred cells. Modified from Collins et al21
Dietary Iron
Duodenal Enterocytes
Reticulo-endothelialMacrophages
SenescentRed Cells
Circulating Iron
1–2 mg/d
20–25 mg/d
Iron Stores &Inflammation
Hypoxia,Anemia &Erythropoiesis
Hepcidin
(+)
(-)
(-)
(-)

Magazine Issue 1/2009Monitoring Anemia-Control
61
trans-membrane iron-exporter pro-tein. Ferroportin is abundantlyexpressed on the cell surface mem-brane of reticulo-endothelial (RE)macro phages, i.e., resident macro -phages in the liver, spleen and bonemarrow, and on the basolateralmembrane of the duodenal entero-cytes. Hepcidin inhibits ironrelease at these sites by binding toferroportin and the complex isinternalized and degraded. REmacrophages are especially impor-tant for the re-use of 20–25 mg irondaily from senescent red cells andduodenal enterocytes release 1–2mg dietary iron into the circulationeach day. RE iron normally under-goes rapid turnover, thus iron reten-tion in this cell population acutelylowers circulating iron concentra-tions.21,22
As indicated earlier, anemia is verycommon in the developing worldfrom an early age and a recent
study in Gambian infants providedpersuasive evidence that the con-stant pressure of morbidity was aprincipal cause in the developmentof anemia over the first 12 monthsof life.23 Infants are rarely anemicwhen born as the oxygen concen-tration in utero is relatively low(hypoxic) and results in high hemo-globin concentrations at birth.However, as the oxygenation of theblood improves, erythropoiesisceases and hemoglobin concentra-tions drop over the first two monthsof life, mainly due to hemodilutionand natural red cell senescence(Table 2).24
The information in Table 2 wasobtained from the placebo-con-trolled vitamin A supplementationstudy in Gambian infants. As therewere no differences attributable tothe supplement, the data were com-bined. In the study, morbidity datawere collected by field workers
every two weeks, and blood wascollected for hemoglobin and plas-ma acute phase protein measure-ments from apparently healthyinfants at birth, 2 months, 5months, 9 months and 12 months,in a study lasting approximately 2.5 years. Morbidity was highthroughout the first 12 months oflife (Table 3) but the constantexposure of these infants to sick-ness appeared to stimulate striking-ly similar rates of increase in C-reactive protein (CRP), α1-acidglycoprotein (AGP), and, threemonths later, anemia.
It is very tempting to concludefrom the development of thesechanges in the infants thatinflammation was the major causeof anemia in the Gambian infants.Figure 2 shows that overall mor-bidity affected 30% of children inthe first three months of life whenthere was very little anemia and lit-
Anemia in Gambian infants1, 2
Age (months) Hemoglobin g/L % < 90 g/LCord 135 102 110 155 109 159 98 4512 90 75
1 Hemoglobin concentrations are means2 From Darboe et al23
Table 2: Hemoglobin concentrations and anemia prevalence in Gambian infants during the first year of life
Morbidity rates in Gambian infants1, 2 aged 1–12 monthsAge (months) Diarrhea Vomiting Fever Cough Other Total1 to 3 4.03 1.6 5.6 10.3 9.1 314 to 6 3.0 1.5 7.2 12.3 8.7 337 to 9 4.2 1.6 9.5 14.1 10.3 4010 to 12 2.0 1.0 6.3 10.9 8.7 29
1 220 infants recruited over approximately 2.5 years and followed for 12 months. Morbidity data were collected during community visits twice a week.2 From Darboe et al3 Average number of days during which infants had symptoms, over a period of 90 days
Table 3: Morbidity rates in Gambian infants during first 12 months of life
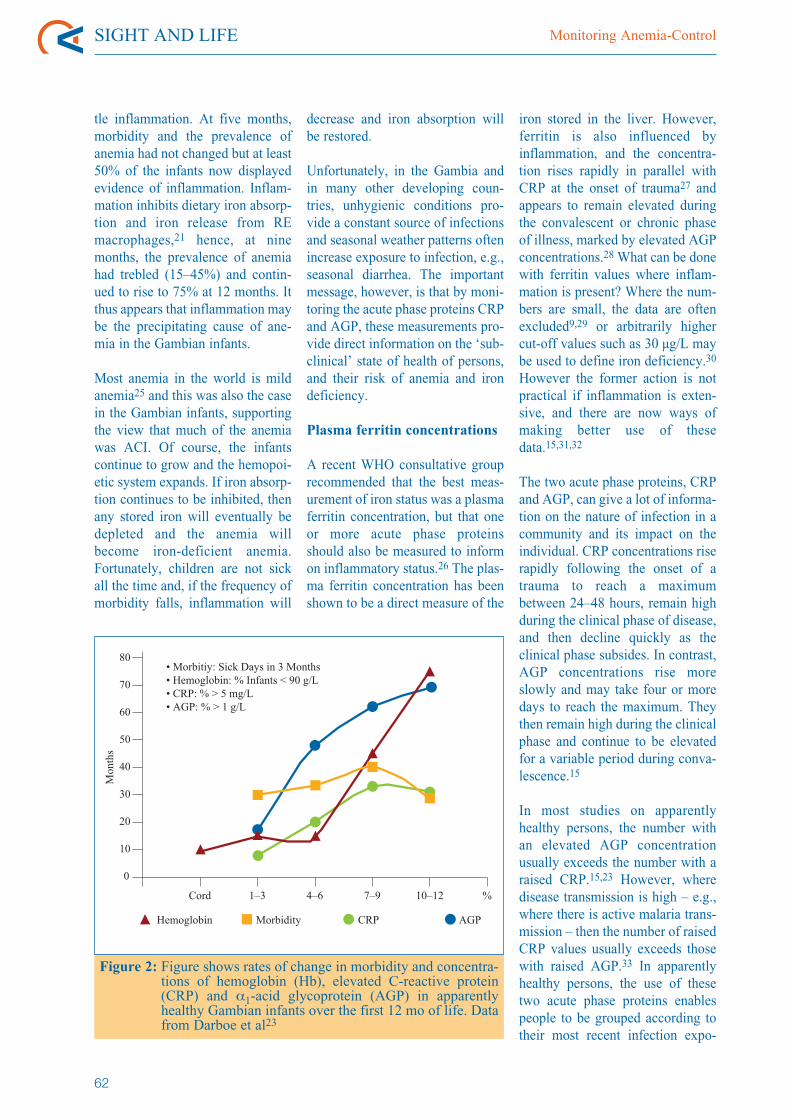
tle inflammation. At five months,morbidity and the prevalence ofanemia had not changed but at least50% of the infants now displayedevidence of inflammation. Inflam -mation in hibits dietary iron absorp-tion and iron release from REmacro phages,21 hence, at ninemonths, the prevalence of anemiahad trebled (15–45%) and contin-ued to rise to 75% at 12 months. Itthus appears that inflammation maybe the precipitating cause of ane-mia in the Gambian infants.
Most anemia in the world is mildanemia25 and this was also the casein the Gambian infants, supportingthe view that much of the anemiawas ACI. Of course, the infantscontinue to grow and the hemopoi-etic system expands. If iron absorp-tion continues to be inhibited, thenany stored iron will eventually bedepleted and the anemia willbecome iron-deficient anemia.Fortunately, children are not sickall the time and, if the frequency ofmorbidity falls, inflammation will
decrease and iron absorption willbe restored.
Unfortunately, in the Gambia andin many other developing coun-tries, unhygienic conditions pro-vide a constant source of infectionsand seasonal weather patterns oftenincrease exposure to infection, e.g.,seasonal diarrhea. The importantmessage, however, is that by moni-toring the acute phase proteins CRPand AGP, these measurements pro-vide direct information on the ‘sub-clinical’ state of health of persons,and their risk of anemia and irondeficiency.
Plasma ferritin concentrations
A recent WHO consultative grouprecommended that the best meas-urement of iron status was a plasmaferritin concentration, but that oneor more acute phase proteinsshould also be measured to informon inflammatory status.26 The plas-ma ferritin concentration has beenshown to be a direct measure of the
iron stored in the liver. However,ferritin is also influenced byinflammation, and the concentra-tion rises rapidly in parallel withCRP at the onset of trauma27 andappears to remain elevated duringthe convalescent or chronic phaseof illness, marked by elevated AGPconcentrations.28 What can be donewith ferritin values where inflam-mation is present? Where the num-bers are small, the data are oftenexcluded9,29 or arbitrarily highercut-off values such as 30 µg/L maybe used to define iron deficiency.30
However the former action is notpractical if inflammation is exten-sive, and there are now ways ofmaking better use of thesedata.15,31,32
The two acute phase proteins, CRPand AGP, can give a lot of informa-tion on the nature of infection in acommunity and its impact on theindividual. CRP concentrations riserapidly following the onset of atrauma to reach a maximumbetween 24–48 hours, remain highduring the clinical phase of disease,and then decline quickly as theclinical phase subsides. In contrast,AGP concentrations rise moreslowly and may take four or moredays to reach the maximum. Theythen remain high during the clinicalphase and continue to be elevatedfor a variable period during conva-lescence.15
In most studies on apparentlyhealthy persons, the number withan elevated AGP concentrationusually exceeds the number with araised CRP.15,23 However, wheredisease transmission is high – e.g.,where there is active malaria trans-mission – then the number of raisedCRP values usually exceeds thosewith raised AGP.33 In apparentlyhealthy persons, the use of thesetwo acute phase proteins enablespeople to be grouped according totheir most recent infection expo-
SIGHT AND LIFE Monitoring Anemia-Control
62
Figure 2: Figure shows rates of change in morbidity and concentra-tions of hemoglobin (Hb), elevated C-reactive protein(CRP) and α1-acid glycoprotein (AGP) in apparentlyhealthy Gambian infants over the first 12 mo of life. Datafrom Darboe et al23
80
60
0
50
40
30
10
• Morbitiy: Sick Days in 3 Months• Hemoglobin: % Infants < 90 g/L• CRP: % > 5 mg/L• AGP: % > 1 g/L
70
20
Cord 1–3 4–6 7–9 10–12 %
Hemoglobin CRPMorbidity AGP
Mon
ths
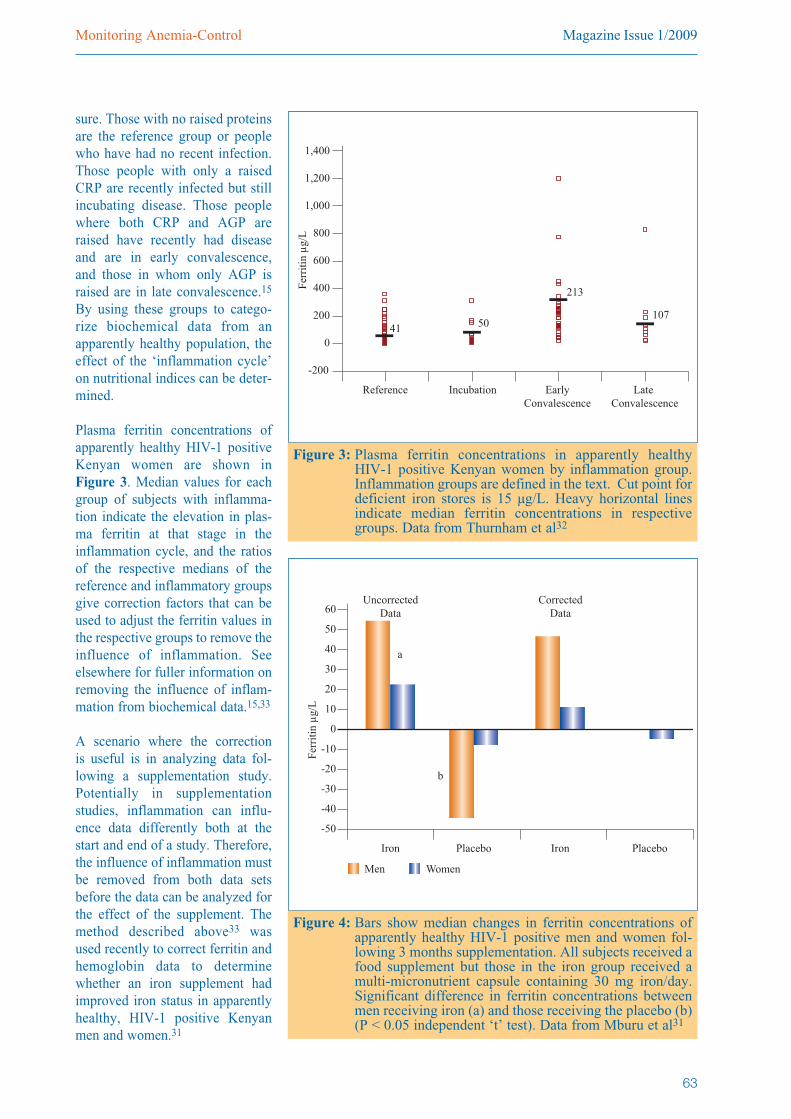
Magazine Issue 1/2009Monitoring Anemia-Control
63
sure. Those with no raised proteinsare the reference group or peoplewho have had no recent infection.Those people with only a raisedCRP are recently infected but stillincubating disease. Those peoplewhere both CRP and AGP areraised have recently had diseaseand are in early convalescence,and those in whom only AGP israised are in late convalescence.15
By using these groups to catego-rize biochemical data from anapparently healthy population, theeffect of the ‘inflammation cycle’on nutritional indices can be deter-mined.
Plasma ferritin concentrations ofapparently healthy HIV-1 positiveKenyan women are shown inFigure 3. Median values for eachgroup of subjects with inflamma-tion indicate the elevation in plas-ma ferritin at that stage in theinflammation cycle, and the ratiosof the respective medians of thereference and inflammatory groupsgive correction factors that can beused to adjust the ferritin values inthe respective groups to remove theinfluence of inflammation. Seeelsewhere for fuller information onremoving the influence of inflam-mation from biochemical data.15,33
A scenario where the correction is useful is in analyzing data fol-lowing a supplementation study.Po tentially in supplementationstudies, inflammation can influ-ence data differently both at thestart and end of a study. Therefore,the influence of inflammation mustbe removed from both data setsbefore the data can be analyzed forthe effect of the supplement. Themethod described above33 wasused recently to correct ferritin andhemoglobin data to determinewhether an iron supplement hadimproved iron status in apparentlyhealthy, HIV-1 positive Kenyanmen and women.31
1,400
1,000
-200
800
600
400
0
1,200
20041 50
213
107
Late Convalescence
Reference Incubation EarlyConvalescence
Ferr
itin
µg/
L
Figure 3: Plasma ferritin concentrations in apparently healthy HIV-1 positive Kenyan women by inflammation group.Inflammation groups are defined in the text. Cut point fordeficient iron stores is 15 µg/L. Heavy horizontal linesindicate median ferritin concentrations in respectivegroups. Data from Thurnham et al32
60
40
-50
30
20
10
-40
50
-30
Iron IronPlacebo Placebo
0
-10
-20
UncorrectedData
CorrectedData
Men Women
a
b
Ferr
itin
µg/
L
Figure 4: Bars show median changes in ferritin concentrations ofapparently healthy HIV-1 positive men and women fol-lowing 3 months supplementation. All subjects received afood supplement but those in the iron group received amulti-micronutrient capsule containing 30 mg iron/day.Significant difference in ferritin concentrations betweenmen receiving iron (a) and those receiving the placebo (b)(P < 0.05 independent ‘t’ test). Data from Mburu et al31

Median plasma ferritin concentra-tions for the women at baseline areshown in Figure 3 for the fourinflammation categories. Ferritinconcentrations in the men weresimilarly distributed, except theconcentrations were much higher.There were no overall changes inhemoglobin in men or women in response to the supplements,whether the data were corrected ornot. In contrast, there were positiveeffects on ferritin in men andwomen who received additionaliron, whether corrected or not.Correction did, however, lessen theapparent negative effects of theplacebo treatment on ferritin(Figure 4).
More importantly, knowledge ofthe inflammation status of the sub-jects at baseline and three monthsrevealed that the response to theiron supplement by those withinflammation at both time-points
was different to that in those whonever showed evidence of inflam-mation. Iron status improved inresponse to iron in both those withinflammation and without. How -ever, in those with no inflamma-tion, there was a significantincrease in hemoglobin and a non-significant improvement in ferritin,but in those with inflammation,only ferritin improved (Figure 5).
These data clearly indicate thatwhere there is evidence of inflam-mation, even mild inflammation inapparently healthy persons, thatinflammation influences the distri-bution of iron. Where there isinflammation, iron mobilization issuppressed and any iron absorbedis retained as ferritin. In contrast,those with no inflammation wereable to absorb iron and mobilize itfor the synthesis of hemoglobin, soless was available for storage asferritin (Figure 5).
What to measure to monitoriron status?
As indicated earlier, hepcidin is animportant regulator of iron metabo-lism in both health and dis-ease.21,22,34,35 In chronic inflamma-tory conditions, increased hepcidinlevels correlate with increased fer-ritin levels,36 suggesting that hep-cidin production remains high dur-ing inflammation, and it would betempting to suggest that hepcidinmight provide a single biomarker toreplace both CRP and AGP.However, recent human evidencesuggests that hepcidin increasedbefore ferritin35 in the early stagesof inflammation, whereas ferritincorrelated very closely with CRPconcentrations at that time in otherhuman experiments.27 Therefore,from the point of view of interpret-ing the influence of inflammationon ferritin, CRP may be a betterbiomarker of acute inflammatoryeffects on ferritin than hepcidin.
Other biomarkers of inflammationinclude the cytokines but most haverelatively short life-spans. Cyto -kines like IL-1 and IL-6, TNF-α,interferons like IFN-γ, and othersare increased by inflammation buttheir life-span is often short as anti-inflammatory cytokines (e.g., IL-10) are also stimulated to counter-act or restrict the inflammatoryresponse. The biological effects ofcytokines are also determined bythe receptor concentration in targettissues, thus cytokine concentrationin blood may not correlate withbiological activity. Cytokines arealso more likely to be elevatedwhen symptoms of disease arepresent. Thus cytokines are notlikely to be useful for studies onapparently healthy persons.
Since most studies obtain cross-sectional data with which to assessiron status, it is important to be ableto relate the life span of the inflam-
SIGHT AND LIFE Monitoring Anemia-Control
64
160
120
0
100
80
60
140
Hb HbFerritin Ferritin
40
20
P < 0.05
Baseline 3 Months
P < 0.05NS
NS
No Inflammation Inflammation at both Baseline and3 Months
Figure 5: Changes in hemoglobin (g/L) and ferritin (µg/L) forapparently healthy subjects with and without inflamma-tion. The subjects are the same as those in Figure 4 how-ever only the iron-supplemented groups are included andresponses are shown for men and women combined.Responses are shown for subjects with and withoutinflammation at both baseline and 3 months. Paired ‘t’-tests were used to explore the differences. Data fromMburu et al31

Magazine Issue 1/2009Monitoring Anemia-Control
65
mation biomarkers to that of theiron biomarkers of interest. In thecase of ferritin, both ferritin andCRP increase at a similar rate follo w ing inflammation. Howeverplas ma ferritin concentrationsremain ele vated for a longer periodof time than CRP but the acutephase proteins have longer half-lives than the cytokines and, AGPtogether with CRP appear to be ele-vated over a similar time period tothat of ferritin as explainedabove.28, 33 It may also be possibleto use a similar approach to quanti-fy the effects of disease on ferritinduring the clinical phase to quanti-fy iron stores but such informationis not currently available.
Hemoglobin provides informationon whether a person is anemic.Hemoglobin synthesis takes place inthe bone marrow and is sensitive toiron availability and to inflamma-tion. However, the red cell has amean half-life of 120 days so theconcentration of hemoglobin in theblood reflects iron availability andinflammation over that period. Thehemoglobin concentration in theblood is therefore cushioned fromthe effects of inflammation, and it isonly when inflammation is pro-longed that hemoglobin concentra-tions will fall as in the anemia ofinflammation. Therefore, the pres-ence of anemia only tells you thatthere has been a shortage of iron forsome period of time but it cannot tellyou whether this is due to a dietarydeficiency or chronic inflammation.Other biomarkers are needed to pro-vide that information.
Lastly, plasma transferrin receptor(sTfR) concentrations are sensitivemarkers of iron deficiency. The con-centration of sTfR on cell mem-branes increases when iron is lack-
ing in the cytosol and the amount inserum is proportional to the amounton cell membranes.37 There is amuch smaller effect of inflammationon sTfR38 than ferritin but, current-ly, there is no universally acceptedstandard or gold standard methodfor sTfR.39
It is therefore suggested that hemo-globin, ferritin, CRP and AGPshould be used to provide the mini-mum amount of information in anysurvey to assess iron status. Hemo -globin can be easily measured in thefield using the HemoCue® hemo-globinometer. The machine is readi-ly standardized and easy to use.Hemoglobin has other advantages inthat it is a well accepted biomarkerof iron status and the ease of obtain-ing results in field studies is oftenwell received by mothers. Plasmaferritin and sTfR concentrations arerecommended as the best indices ofiron status,40 but ferritin is preferredfor the reasons outlined above.Where possible, these measure-ments should be done on venous orcapillary blood as serum suitablystored (< -20°C) as quickly as possi-ble after collection and centrifuga-tion. A number of methods areavailable and additional micro-tech-niques are being developed to assessferritin, sTfr, retinol-binding proteinand CRP measurements using as lit-tle as 30 µL of serum in total.41
Others have extended this to includeAGP.42 *
ELISA techniques on dried bloodspot (DBS) material are also beingdeveloped41-43 to enable the collec-tion of materials in field circum-stances where electricity may not beavailable. Once DBS are properlydried, they can be stored at -20°Cfor up to 15 months.42 However,collection and storage of DBS underhumid tropical conditions where
there is no electricity does presentproblems and CRP is particularlysensitive to damage if stored atambient temperatures,43 althoughothers report no effect of storage forthree days at very warm ambienttemperatures.44 Nevertheless, forsafest results, DBS should be driedquickly, stored with a desiccant andrapidly transferred to -20°C.43
Collection of capillary bloodwhether for plasma or DBS hasother problems because the finger-stick used is often painful, andsqueezing the finger to restrain thechild or obtain the blood alters thecomposition.
In conclusion, venous blood isalways to be preferred for the mostaccurate measurements. Capillaryblood for either plasma or DBS cannow be processed to provide infor-mation on both iron and inflamma-tion biomarkers. Transport of plas-ma or serum samples requires elec-tricity to provide refrigeration forsample stability. Long-term storageof DBS also requires refrigerationbut DBS provide a stable and con-venient medium for transport. Thebiggest problem seems to be thedrying of the blood spot before stor-age, particularly in areas wherethere is no electricity to increase thespeed of drying. The use of suitableracking for the blood spot papersand a hot box with desiccantexposed to tropical sunshine may bea ‘low-tech’ solution45 but experi-ments still need to be done to testand refine the process.
References
1. Denic S, Agarawal MM. Nutritional irondeficiency: an evolutionary perspective.Nutrition 2007;23:603–14.
2. DeMaeyer EM, Adiels-Tegman M. Theprevalence of anemia in the world. WorldHealth Stat Q 1985;38:302–16.
*It has recently come to my attention that PATH has initiated development activities for a multiplex micronutrient assessment toolthat will assay ferritin, AGP, CRP and in addition, transferrin receptors and retinol binding protein in one dilution. This will bevery welcome news for nutritionists wanting to interpret nutritional biomarkers in the presence of inflammation.
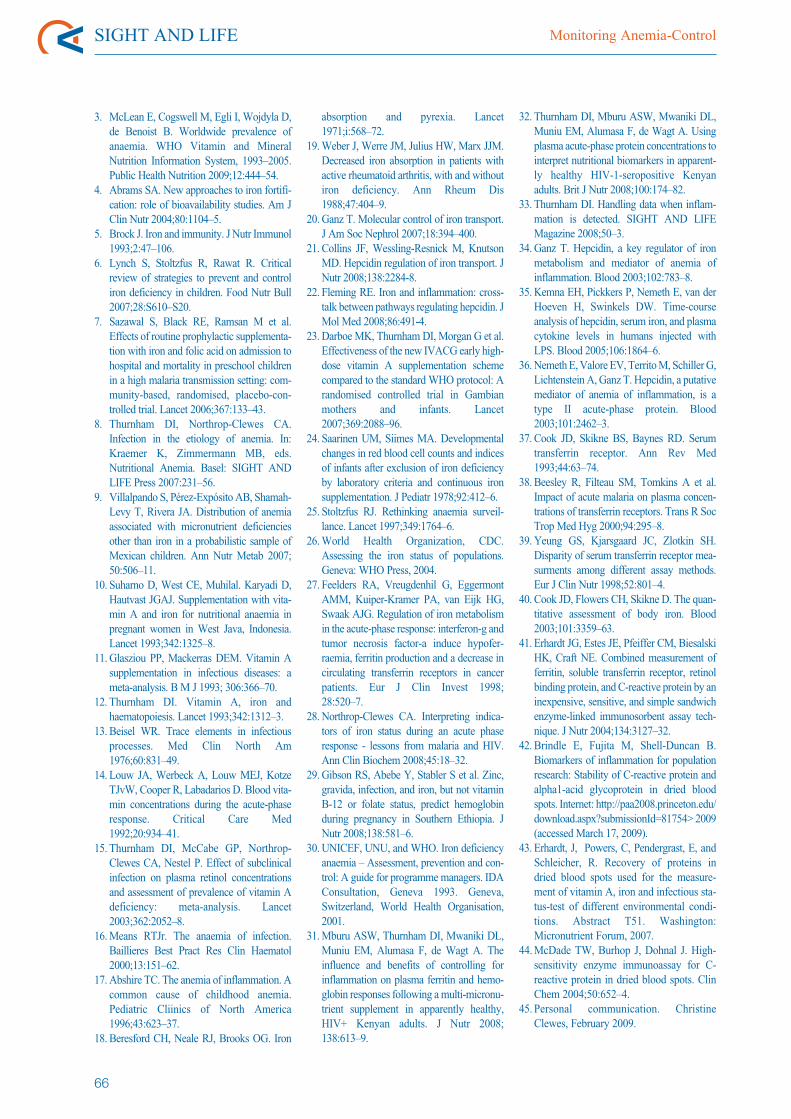
3. McLean E, Cogswell M, Egli I, Wojdyla D,de Benoist B. Worldwide prevalence ofanaemia. WHO Vitamin and MineralNutrition Information System, 1993–2005.Public Health Nutrition 2009;12:444–54.
4. Abrams SA. New approaches to iron fortifi-cation: role of bioavailability studies. Am JClin Nutr 2004;80:1104–5.
5. Brock J. Iron and immunity. J Nutr Immunol1993;2:47–106.
6. Lynch S, Stoltzfus R, Rawat R. Criticalreview of strategies to prevent and controliron deficiency in children. Food Nutr Bull2007;28:S610–S20.
7. Sazawal S, Black RE, Ramsan M et al.Effects of routine prophylactic supplementa-tion with iron and folic acid on admission tohospital and mortality in preschool childrenin a high malaria transmission setting: com-munity-based, randomised, placebo-con-trolled trial. Lancet 2006;367:133–43.
8. Thurnham DI, Northrop-Clewes CA.Infection in the etiology of anemia. In:Kraemer K, Zimmermann MB, eds.Nutritional Anemia. Basel: SIGHT ANDLIFE Press 2007:231–56.
9. Villalpando S, Pérez-Expósito AB, Shamah-Levy T, Rivera JA. Distri bution of anemiaassociated with micro nutrient deficienciesother than iron in a probabilistic sample ofMexi can children. Ann Nutr Metab 2007;50:506–11.
10. Suharno D, West CE, Muhilal. Karyadi D,Hautvast JGAJ. Supple men tation with vita-min A and iron for nutritional anaemia inpregnant women in West Java, Indonesia.Lancet 1993;342:1325–8.
11. Glasziou PP, Mackerras DEM. Vitamin Asupplementation in infectious diseases: ameta-analysis. B M J 1993; 306:366–70.
12. Thurnham DI. Vitamin A, iron andhaematopoiesis. Lancet 1993;342:1312–3.
13. Beisel WR. Trace elements in infectiousprocesses. Med Clin North Am1976;60:831–49.
14. Louw JA, Werbeck A, Louw MEJ, KotzeTJvW, Cooper R, Labadarios D. Blood vita-min concentrations during the acute-phaseresponse. Critical Care Med1992;20:934–41.
15. Thurnham DI, McCabe GP, Northrop-Clewes CA, Nestel P. Effect of subclinicalinfection on plasma retinol concentrationsand assessment of prevalence of vitamin Adeficiency: meta-analysis. Lancet2003;362:2052–8.
16.Means RTJr. The anaemia of infection.Baillieres Best Pract Res Clin Haematol2000;13:151–62.
17. Abshire TC. The anemia of inflammation. Acommon cause of childhood anemia.Pediatric Cliinics of North America1996;43:623–37.
18. Beresford CH, Neale RJ, Brooks OG. Iron
absorption and pyrexia. Lancet1971;i:568–72.
19.Weber J, Werre JM, Julius HW, Marx JJM.Decreased iron absorption in patients withactive rheumatoid arthritis, with and withoutiron deficiency. Ann Rheum Dis1988;47:404–9.
20. Ganz T. Molecular control of iron transport.J Am Soc Nephrol 2007;18:394–400.
21. Collins JF, Wessling-Resnick M, KnutsonMD. Hepcidin regulation of iron transport. JNutr 2008;138:2284-8.
22. Fleming RE. Iron and inflammation: cross-talk between pathways regulating hepcidin. JMol Med 2008;86:491-4.
23. Darboe MK, Thurnham DI, Morgan G et al.Effectiveness of the new IVACG early high-dose vitamin A supplementation schemecompared to the standard WHO protocol: Arandomised controlled trial in Gambianmothers and infants. Lancet2007;369:2088–96.
24. Saarinen UM, Siimes MA. Develop mentalchanges in red blood cell counts and indicesof infants after exclusion of iron deficiencyby laboratory criteria and continuous ironsupplementation. J Pediatr 1978;92:412–6.
25. Stoltzfus RJ. Rethinking anaemia surveil-lance. Lancet 1997;349:1764–6.
26.World Health Organization, CDC.Assessing the iron status of populations.Geneva: WHO Press, 2004.
27. Feelders RA, Vreugdenhil G, Egger montAMM, Kuiper-Kramer PA, van Eijk HG,Swaak AJG. Regulation of iron metabolismin the acute-phase response: interferon-g andtumor necrosis factor-a induce hypofer-raemia, ferritin production and a decrease incirculating transferrin receptors in cancerpatients. Eur J Clin Invest 1998;28:520–7.
28. Northrop-Clewes CA. Interpreting indica-tors of iron status during an acute phaseresponse - lessons from malaria and HIV.Ann Clin Biochem 2008;45:18–32.
29. Gibson RS, Abebe Y, Stabler S et al. Zinc,gravida, infection, and iron, but not vitaminB-12 or folate status, predict hemoglobinduring pregnancy in Southern Ethiopia. JNutr 2008;138:581–6.
30. UNICEF, UNU, and WHO. Iron deficiencyanaemia – Assessment, prevention and con-trol: A guide for programme managers. IDAConsultation, Geneva 1993. Geneva,Switzerland, World Health Organisation,2001.
31.Mburu ASW, Thurnham DI, Mwaniki DL,Muniu EM, Alumasa F, de Wagt A. Theinfluence and benefits of controlling forinflammation on plasma ferritin and hemo-globin responses following a multi-micronu-trient supplement in apparently healthy,HIV+ Kenyan adults. J Nutr 2008;138:613–9.
32. Thurnham DI, Mburu ASW, Mwaniki DL,Muniu EM, Alumasa F, de Wagt A. Usingplasma acute-phase protein concentrations tointerpret nutritional biomarkers in apparent-ly healthy HIV-1-seropositive Kenyanadults. Brit J Nutr 2008;100:174–82.
33. Thurnham DI. Handling data when inflam-mation is detected. SIGHT AND LIFEMagazine 2008;50–3.
34. Ganz T. Hepcidin, a key regulator of ironmetabolism and mediator of anemia ofinflammation. Blood 2003;102:783–8.
35. Kemna EH, Pickkers P, Nemeth E, van derHoeven H, Swinkels DW. Time-courseanalysis of hepcidin, serum iron, and plasmacytokine levels in humans injected withLPS. Blood 2005;106:1864–6.
36. Nemeth E, Valore EV, Territo M, Schiller G,Lichtenstein A, Ganz T. Hepcidin, a putativemediator of anemia of inflammation, is atype II acute-phase protein. Blood2003;101:2462–3.
37. Cook JD, Skikne BS, Baynes RD. Serumtransferrin receptor. Ann Rev Med1993;44:63–74.
38. Beesley R, Filteau SM, Tomkins A et al.Impact of acute malaria on plasma concen-trations of transferrin receptors. Trans R SocTrop Med Hyg 2000;94:295–8.
39. Yeung GS, Kjarsgaard JC, Zlotkin SH.Disparity of serum transferrin receptor mea-surments among different assay methods.Eur J Clin Nutr 1998;52:801–4.
40. Cook JD, Flowers CH, Skikne D. The quan-titative assessment of body iron. Blood2003;101:3359–63.
41. Erhardt JG, Estes JE, Pfeiffer CM, BiesalskiHK, Craft NE. Combined measurement offerritin, soluble transferrin receptor, retinolbinding protein, and C-reactive protein by aninexpensive, sensitive, and simple sandwichenzyme-linked immunosorbent assay tech-nique. J Nutr 2004;134:3127–32.
42. Brindle E, Fujita M, Shell-Duncan B.Biomarkers of inflammation for populationresearch: Stability of C-reactive protein andalpha1-acid glycoprotein in dried bloodspots. Internet: http://paa2008.princeton.edu/download.aspx?submissionId=81754> 2009(accessed March 17, 2009).
43. Erhardt, J, Powers, C, Pendergrast, E, andSchleicher, R. Recovery of proteins indried blood spots used for the measure-ment of vitamin A, iron and infectious sta-tus-test of different environmental condi-tions. Abstract T51. Washington:Micronutrient Forum, 2007.
44.McDade TW, Burhop J, Dohnal J. High-sensitivity enzyme immunoassay for C-reactive protein in dried blood spots. ClinChem 2004;50:652–4.
45. Personal communication. ChristineClewes, February 2009.
SIGHT AND LIFE Monitoring Anemia-Control
66

Magazine Issue 1/2009News
67
NewsThe World Food Crisis: A Wake-Up Call to Save a Generation ofChildren
Calling for “a wake-up call to save this generation ofchildren,” a group of eminent scientists met early thisyear to map out more effective responses to the globalfinancial and food crises that would not only protectjobs and infrastructure, but also the lives and futureproductivity of the world’s poorest people.
“Without immediate action, we are exposing ourselvesand our children to greater shocks than those we facetoday,” declared the group in a statement. “We knowwhat to do – we call upon the world’s leaders to do it.”
The seriousness of the message was underscored bythe credentials of the 14 scientists, who hail from anivy league of international development institutionsand academia, including the World Bank, the UnitedNations World Food Programme (WFP), the JohnsHopkins Bloomberg School of Public Health, theUnited Nations Children’s Fund (UNICEF), SIGHTAND LIFE, the International Food Policy Research
Institute (IFPRI), Harvard Medical School and Schoolof Public Health, Stanford University, and theFriedman School of Nutrition Science and Policy,Tufts University.
Meeting at Castel Gandolfo, Italy, on 25 January 2009in their personal (not organizational) capacities, theywere united in their conviction on the need to placenutrition back at the centre of actions to mitigate the
worst effects of high food prices, job losses and thegeneral economic downturn. Compelling evidenceshows that improving nutrition protects health, pre-vents disability, boosts economic productivity andsaves lives. The billions lost by the world’s financialmarkets pale in significance compared to the econom-ic losses due to growing hunger and its effects onhuman capital, according to the group.
Pulling together current best practice and science, thegroup concluded that not enough of what is known towork is being done. Some of the most cost-effectiveinterventions include tackling deficiencies in vitaminsand minerals, including the distribution of vitamin Acapsules to prevent blindness and reduce mortality, theuse of zinc tablets in the treatment of diarrhea, and thefortification of salt with iodine to protect mental capac-ity. These and other essential nutrients should also beensured in the food supply through fortification anddietary diversification supported by agricultural growth. But it is not just about more food, the group insists; itis about reinforcing the nurture of mother and child.Exclusive breastfeeding practice for the first sixmonths of life is still insufficiently supported and prac-ticed, effective antenatal care is inaccessible to far toomany pregnant women and appropriate low cost, qual-ity foods for infants and toddlers remains an unmetneed.
Additionally, short-term ac -tions are crucial to bufferingthe most vulnerable to eco-nomic or climatic shocks. Forexample, in West Africa,severe malnutrition has beenreduced over the past year incountries such as Niger andBurkina Faso by a combina-tion of targeted food distribu-tion, increased vaccinationcoverage, bed nets to ward offmalaria, and education ofmothers in the best ways toensure the future growth anddevelopment of their surviving
children. Therefore, immediate investments toimprove the nutritional wellbeing of mothers as well astheir children generate short-term rewards but evengreater long-term returns.
The workshop was made possible through an educa-tional grant from SIGHT AND LIFE. It is planned topublish the proceedings of the meeting as a supple-ment to The Journal of Nutrition.
Participants of the workshop at Castel Gandolfo, Italy
SIGHT AND LIFE Magazine 2009;1:67–69

SIGHT AND LIFE News
68
In February 2009 SIGHT AND LIFE and its partnersin India launched a Marathi-language version of thewidely popular Healthy Eyes Activity Book, com-monly referred to by its acronym, HEAB, inAurangabad, Maharashtra.
The Marathi translation of the HEAB was undertak-en by volunteers committed to the education of chil-dren in Maharashtra in their local language for eyecare, with support from the Nutrition ImprovementProgram of India. SIGHT AND LIFE provided finan-cial support to print 5,000 copies of the MarathiHEAB for distribution to schools in Maharashtra.
The HEAB, which was first developed by theInternational Center for Eye Health (ICEH) and SightSavers International, then adopted and supported bySIGHT AND LIFE for wide distribution, was pub-lished to meet the need for eye health communicationspecifically targeted to and accessible by children. Ithas been published in more than 10 languages, withthe addition of Marathi.
In 2007, SIGHT AND LIFE and ICEH produced thesecond edition of the HEAB. The HEAB has provento be a unique and effective tool for educating chil-dren in eye health. SIGHT AND LIFE has supported
Ceremony for the launch of the Marathi Healthy Eyes Activity Book
Meeting participants and their affiliations:
Mr H. Alderman (World Bank)Dr M. Bloem (United Nations World Food Programme)Mr H. Brinkman (United Nations World Food Programme)Dr P. Christian (Johns Hopkins Bloomberg School of Public Health)Dr I. Darnton-Hill (UNICEF)Dr K. Kraemer (SIGHT AND LIFE)Dr M. Ruel (International Food Policy Research Institute) Dr R. Semba (Johns Hopkins Bloomberg School of Public Health)Dr K. Sztam (Children’s Hospital of Boston, Harvard Medical School)Mr A. Thorne-Lyman (United Nations World Food Programme, Harvard School of Public Health)Dr P. Timmer (Stanford University)Dr P. Webb (Friedman School of Nutrition Science and Policy, Tufts University)Dr K. West (Johns Hopkins Bloomberg School of Public Health)
Communicated by:Jane Badham, JB Consultancy, PO Box 67396, Bryanston 2021, Gauteng, South AfricaEmail: [email protected]
Launch of the Marathi Healthy Eyes Activity Book

many educational projects around the world usingthis book, providing grants for its translation andprinting in local languages.
External reference: http://www.v2020.org/news.asp?section=000100010010&articleID=976&newsletterID=383
Communicated by: Kailash Baviskar, Maharashtra University of HealthSciences, Department of Public Health, CommunityOphthalmology, Shivagi Maidan, Aurangabad431001, Maharashtra, IndiaEmail: [email protected]
Magazine Issue 1/2009News
69
Canada’s MicronutrientInitiative Celebrates 5 BillionthVitamin A Capsule Canada’s Micronutrient Initiative (MI) celebrated itsrole in saving over two million children’s livesworldwide with the manufacture of its five billionthvitamin A capsule in November 2008.
“It only takes two doses of vitamin A every year,from age six months to five years – that’s about ninecapsules – to help save a child’s life,” explained MIPresident Venkatesh Mannar. “Vitamin A is a simple,cost-effective way to boost children’s immune sys-tems so that their bodies can fight off deadly infec-tions, such as measles, and get the best start in life.
MI’s vitamin A child survival program reaches chil-dren in over 70 countries around the world. Since1997, the organization has provided for more than75% of the developing world’s need for vitamin A.
Supported by the Canadian International Develop -ment Agency (CIDA), MI’s vitamin A program isone of Canada’s most successful international devel-opment stories. Each capsule costs only about twocents to manufacture; the manufacture of five billioncapsules highlights Canada’s commitment to savingchildren’s lives. The vitamin A capsules manufac-tured in Canada are donated primarily to UNICEF,which then distributes them through national childhealth programs.
MI is an Ottawa-based international nonprofit organ-ization dedicated to ensuring that the world’s mostvulnerable – especially women and children – indeveloping countries get the vitamins and minerals
they need to survive and thrive, through supplemen-tation and food fortification programs. Its mission isto develop, implement and monitor innovative, costeffective and sustainable solutions for hidden hunger,in partnership with others.
Communicated by: Aynsley Morris, The Micronutrient Initiative, 180Elgin Street, Suite 1000, Ottawa, Ontario K2P 2K3,Canada.Email: [email protected] Web: www.micronutrient.org
Welcome ceremony for Klaus Kraemer
Venkatesh Mannar, President of the MicronutrientInitiative, celebrates millions of children’s livessaved with the manufacture of MI’s 5 billionthvitamin A capsule.

SIGHT AND LIFE Letters to the Editor
70
Dear Sir,
We would like to report an obser-vation, which was made during ascreening of around 2,900 childrenand adolescents from slums ofKolkata, Howrah, and 24 ParganasSouth districts in India for ocularsigns of vitamin A deficiency(VAD). These children and adoles-cents attended the free medical dis-pensaries of our NGO in 2008 forvarious medical reasons.
Bitot’s spots were found to bemore frequent among the school-age children and adolescents thanin the age group of the preschool-ers. We found 52 children and ado-lescents with Bitot’s spots; theFigure shows their age distribu-tion.
We recorded a history of consump-tion of a vitamin A supplement inthe previous six months for each ofthe screened children and adoles-cents, and searched in their avail-able medical documents for such asupplementation. The Figuresummarizes the occurrence ofBitot’s spots in all screened chil-dren, whether they had received avitamin A supplement during theprevious six months or not.
The following observations arerestricted to those children andadolescents, who did not receivesuch a supplement:
• The frequency of Bitot’s spots inthe different age groups wasfound to be 2.7% for the childrenin the age group of 1–5 years,and to be 4.9% for those in theage group of 6–16 years. Asthese figures relate only tochildren without a history of
vita min A supplementation, weare sure that vitamin A supple-mentation of the preschoolerswas not the reason for theobserved lower frequency ofBitot’s spots in this age group.• The frequency of night blindnesswas 1.4% among the preschool-ers, while it was not determinedamong the older children andadolescents. However, several ofthe children and adolescentsbetween 6 and 16 years of agewho were found with Bitot’sspots were also night-blind.• Keratomalacia was observedwith a frequency of 0.14%among preschoolers, while it wasnot observed among children ofschool age and adolescence.
Of note, maternal night blindnessvaried between 1.5% and 10.6%among the screened mothers fromdifferent slums of the said dis-tricts. Bitot’s spots were rarelyseen also in pregnant women andmothers up to six months after
delivery, with and without con-comitant night blindness in thesame patient.
These observations were made inchildren and adolescents fromhigh-risk slums in Kolkata,Howrah and 24 Parganas Southdistricts, which our NGO selectedfor its medical work due to theobvious poverty of the area. Thementioned data can therefore notbe generalized to the entire childor adolescent population of thesaid districts. We screened chil-dren and adolescents who attendedfree medical dispensaries for vari-ous health reasons, mostly due tominor illnesses. Their vitamin Astatus may therefore not even begeneralized to the healthy childand adolescent population of thesame high-risk slums. However,even for the highly localized set-ting of a busy medical OPD in aslum, it is useful to know the fre-quency of xerophthalmia amongits pediatric patients.
Letters to the Editor
Bitot's spots in school-age child
SIGHT AND LIFE Magazine 2009;1:70–73
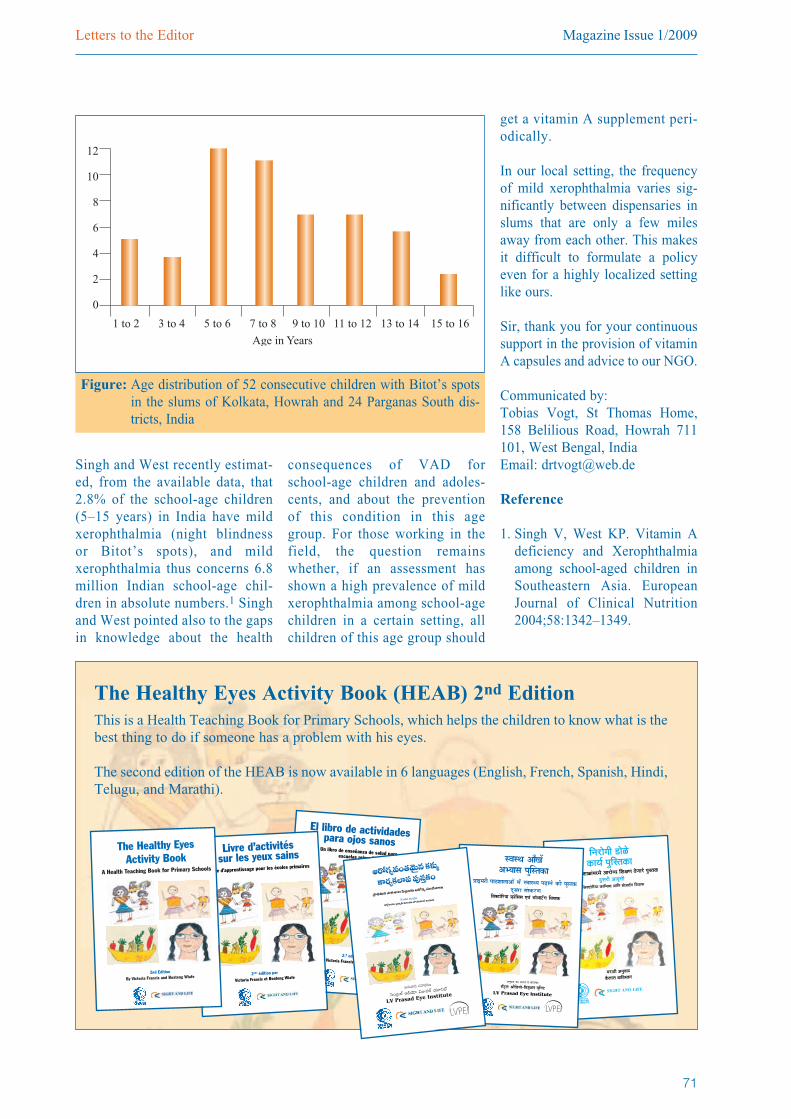
Magazine Issue 1/2009Letters to the Editor
71
Singh and West recently estimat-ed, from the available data, that2.8% of the school-age children(5–15 years) in India have mildxerophthalmia (night blindnessor Bitot’s spots), and mildxerophthalmia thus concerns 6.8million Indian school-age chil-dren in absolute numbers.1 Singhand West pointed also to the gapsin knowledge about the health
consequences of VAD forschool-age children and adoles-cents, and about the preventionof this condition in this agegroup. For those working in thefield, the question remainswhether, if an assess ment hasshown a high prevalence of mildxerophthalmia among school -agechildren in a certain setting, allchildren of this age group should
get a vitamin A supplement peri-odically.
In our local setting, the frequencyof mild xerophthalmia varies sig-nificantly between dispensaries inslums that are only a few milesaway from each other. This makesit difficult to formulate a policyeven for a highly localized settinglike ours.
Sir, thank you for your continuoussupport in the provision of vitaminA capsules and advice to our NGO.
Communicated by: Tobias Vogt, St Thomas Home,158 Belilious Road, Howrah 7 11101, West Bengal, IndiaEmail: [email protected]
Reference
1. Singh V, West KP. Vitamin Adeficiency and Xerophthalmiaamong school-aged children inSoutheastern Asia. EuropeanJournal of Clinical Nutrition2004;58:1342–1349.
Figure: Age distribution of 52 consecutive children with Bitot’s spotsin the slums of Kolkata, Howrah and 24 Parganas South dis-tricts, India
0
12
8
6
4
2
10
1 to 2 3 to 4 5 to 6 7 to 8 9 to 10 11 to 12 13 to 14 15 to 16
Age in Years
El libro de actividades para ojos sanosUn libro de enseñanza de salud para escuelas primarias
2.ª ediciónpor Victoria Francis y Boateng Wiafe
Livre d’activités sur les yeux sains
Livre d’apprentissage pour les écoles primaires
2nde édition par
Victoria Francis et Boateng Wiafe
The Healthy EyesActivity Book
A Health Teaching Book for Primary Schools
2nd Edition
By Victoria Francis and Boateng Wiafe
The Healthy Eyes Activity Book (HEAB) 2nd EditionThis is a Health Teaching Book for Primary Schools, which helps the children to know what is thebest thing to do if someone has a problem with his eyes.
The second edition of the HEAB is now available in 6 languages (English, French, Spanish, Hindi,Telugu, and Marathi).
º´ÉºlÉ +ÉÄJÉ å+¦ªÉÉºÉ É ÖκiÉE É
|ÉÉ<¨É®úÒ ÉÉ`¶ÉɱÉÉ+É å ¨É å º´ÉɺlªÉ ÉgøÉxÉ ä E òÒ É ÖºiÉE òn ÚùºÉ® úÉ ºÉƺE ò® úhÉ
ò
+xÉÖ´ÉÉnù EòÉ +É®Æú¦É ´É EòɪÉǦÉÉ®ú:ºÉå]Åõ±É +ÉèÊb÷ªÉÉä-Ê´ÉVÉÖ+±É ªÉÚÊxÉ]õ
LV Prasad Eye Institute
P~ÀQƺ=O`«"≥∞ÿ# Hõà◊√§
HÍ~°ºHõÖÏѨ ѨÙã¨ÎHõO
„áê^äŒq∞Hõ áê~î°âßÅ Ñ≤šʼnõΩ P~ÀQƺ ã¨O^ÕâßÅ∞
J#∞"å^Œ ã¨Ç¨ÏHõ~°
ÃãO„@Öò P_çÜ≥∂ qA=Öò Ü«¸x\ò
LV Prasad Eye Institute
Ô~O_»= =Ú„^Œ
qHÀìiÜ«∂ „á¶êxûãπ =∞iÜ«Ú ÉÁÜ≥∞>ˇOQ∑ qÜ«∂Ѷπ
6 g∞@~°¡ ^Œ∂~°O #∞O_ç LѨÜ≥∂yOK«O_ç (37= ¿Ñl K«∂_»O_ç)
6 g∞@~°¡ ^Œ∂~°O #∞O_ç LѨÜ≥∂yOK«O_ç (37= ¿Ñl K«∂_»O_ç)
6 g∞@~°¡ ^Œ∂~°O #∞O_ç LѨÜ≥∂yOK«O_ç (37= ¿Ñl K«∂_»O_ç)
6 g∞@~°¡ ^Œ∂~°O #∞O_ç LѨÜ≥∂yOK«O_ç (37= ¿Ñl K«∂_»O_ç)
6 g∞@~°¡ ^Œ∂~°O #∞O_ç LѨÜ≥∂yOK«O_ç (37= ¿Ñl K«∂_»O_ç)
SIGHT AND LIFE Letters to the Editor
72
Dear Sir,
The administration of Bijilo Lower Basis School in theGambia – on behalf of the teachers, students and par-ents – are very glad to inform you that we have receivedyour wonderful donation of 500 copies of the HealthyEyes Activity Book and a lot of color pencils. The parent-teacher committee and the Regional EducationDirectorate are all aware of these donations. Personnelfrom the eye care unit of our department have beeninvited to see the books and were similarly veryamazed.
We have thought it wise to organize a school-basedtraining workshop for teachers on the use of the books.It will involve all the 31 teachers in our school, twofrom each of the four neighboring schools, representa-tives from the Regional Education Directorate, fourresource persons and four school management commit-tee members (parents). The training will be a whole dayprogram on a Saturday, and will involve about 51 par-ticipants.
We would also like to highlight some constraints facingour school, at which over 1,000 children are enrolled,most of whom come from poor families:
• Our school feeding program has been phased out foralmost six years now; however, we believe that poor
parents normally send their kids to school just to easethe number of cups of rice they must cook at home.
• Due to the lack of staff quarters for teachers to stay inthe school, all our staff members must travel to theschool each day; having staff quarters at the schoolwould add to the security of the school and ensureteachers are there on time.
• Our school field is not fenced, and sometimes teach-ers and pupils face problems when having their phys-ical education lessons or games in such an open area.
• We have started working on the school garden butthere is lack of gardening materials, which are expen-sive to buy and we do not have the funds to buy them.
• Learning materials, like exercise books, pencils,erasers, are a big problem too; 80% of our studentscome from poor families, who are generally unable tobuy stationery for their children.
On behalf of the teachers, pupils and parents of BijiloSchool, we most profoundly thank SIGHT AND LIFEfor the wonderful gesture of your donation. We assureyou that the books will be put to good use. We furtherhope you can assist further and add to the developmentof education in our school, in particular, and theGambia, in general.
Communicated by: Kebba Fatty, Headmaster, and Isatou Joof, DeputyHead Mistress, Bijilo Lower Basis School, the Gambia
Children from Bijilo Lower Basis School in Gambia with fortified biscuits from SIGHT AND LIFE whicharrived at the school after we received the above letter

Magazine Issue 1/2009Letters to the Editor
73
Dear Sir,
With this letter, I would like toinform you about the effects of theMixMe™ and the biscuits thatSIGHT AND LIFE has donated tothe children of the Sedimosang DayCare Center in Ivory Park, SouthAfrica.
Ivory Park is a very poor townshipwhere lots of elderly people,orphans and child-headed familiessurvive below the poverty line.Because of HIV and AIDS, manychildren depend on the care of theirgrandparents, aunts or the oldestchild in the family. A lot of prob-lems arise because of their povertyand lack of access to food. In theareas directly surrounding Sedimo -sang are three poor schools thatreceive a government grant to pro-vide children with one meal a day.Such meals consist of ‘maispap’ – acornflour-based dish – which isusually the only thing the childrenreceive.
The kids of Sedimosang are veryhappy with the MixMe™ and bis-cuits! In the beginning, we werelearning how to get the bestresults with Mix Me™ and we
were monitoring the kids. By theend of last year, we got our firstevaluation. The most importantprogress is that the kids are muchmore aware and have better con-centration. We followed some ofthe children who where alwaysvery tired and apathetic. We slow-ly saw them changing; they start-
ed being active and were moreattentive to others. With them, weeven see a healthy form of naugh-tiness. Great results!
In January of this year, when thenew school year started, new kidscame in. Normally, we have about84 kids, but this year, 104 kidswere enrolled. Sedimosang is nowfully packed. We have to ‘fight’with parents, grannies and otherswho take care of these children –all because the news aboutMixMe™ spread around and noweveryone wants to have their kidsadmitted to Sedimosang! Also, wehave been monitoring the newchildren and, again, we see notice-able results. One child, whoalways had a cold and had neverbeen interested in playing at all, isnow doing much better. He reallyenjoys coloring and painting.
We would also like to thank DSM’sNutrition Improvement Programfor the beautiful MixMeTM
T-shirts. The kids wear themproudly as a school uniform!
One of our other projects is the KeA Bona Eye Clinic. Clinic DirectorHenny Stege and his staff ex -pressed their concerns about thelarge number of children with eyeproblems they meet every day inthe various schools in Ivory Park.One of the main causes seems to bemalnutrition. It would be veryinteresting to see if the clinic willalso see changes as soon as we startwith MixMe™ and biscuits at theprimary schools.
In addition to the kids, the poorestelderly people who visit our soupkitchen, Supa di Mama, nowreceive the biscuits. They are verygrateful as well and the biscuitsmean a lot to them. Many of theseelderly people live off a small grant,from which they not only have tofeed and support themselves butalso their grandchildren. They cometo Supa di Mama twice a week andthey spend the whole day there. Notonly do they enjoy a meal with thebiscuits, they make a social happen-ing out of it: helping each other,talking with each other, and theyeven started their own exercise pro-gram, including playing soccer!This activity program started after adiscussion about the biscuits andthey are now ‘showing off’ how fitthey have become. It is amazing tosee how much power your contribu-tion gives to these people!
On behalf of all people involved inSouth Africa: Baie dankie en baiegroete!
Communicated by: Trees Stege, Sedimosang Day CareCenter, PO Box 39207, Moreleta -park 0044, South AfricaEmail: [email protected]
Children of the Sedimosang Day Care Center having porridge withadded MixMeTM
SIGHT AND LIFE Publications
74
Pediatric Nutrition in Practice
Koletzko B, Cooper P, Makrides M, Garza C, Uauy R,Wang W (Eds.). Pediatric Nutrition in Practice. Basel:
S. Karger AG, 2008.
Adequate nutrition is ofutmost importance duringinfancy and childhood,due to the rapid growthand development thatcharacterizes this phaseof life. As many studieshave shown, ensuringan appropriate amountand composition ofnutrients for infantsand young children arecritical for growth,functional out comes(such as cognition andimmune response),and long-term well-being.
Paediatric Nutrition in Practice provides concise infor-mation to readers who seek quick guidance on practi-cal relevant issues in the nutrition of infants, childrenand adolescents. Its editors have distilled this informa-tion into a compact reference book for busy physiciansand other healthcare professionals who often find itdifficult to devote sufficient time to study elaborateand extensive books on just one aspect of their prac-tice.
Key topics covered in the book include general aspectsof childhood nutrition; nutrition of healthy infants,children and adolescents; and nutritional challenges inspecial conditions and diseases. It also includes WHOGrowth Standards Charts, the CDC and Euro GrowthCharts, and Reference Nutrient Intakes for Infants,Children and Nutrition.
A global editorial board provides the book with aninternational perspective, confronting challenges bothin affluent and poorer populations, and contributes fur-ther to the unique worth of this book.
For more information, please visit http://www.karger.com/Ped-Nutrition-Practice.
Entrepreneurship in the Social Sector
Jane Wei-Skillern, James E. Austin, Herman B.Leonard, Herman Leonard, Howard Stevenson.Entrepreneurship in the Social Sector. California:Sage Publications, 2007.
The emerging field of social entrepreneurship has ledthe way to a remarkable revolution in which entrepre-neurs are transforming the social sector through theapplication of busi -ness know-how. En -tre preneurship in theSocial Sector intro-duces and developsthe concept of socialenterprise organiza-tions, which arecharacterized, firstand foremost, bytheir social missionas well as by theirinnovative combi-nations of socialand commercialapproaches.
Building on theflagship SocialEnterprise MBA elective course atHarvard Business School, the book focuses on devel-oping the knowledge and skills for creating, lead-ing, or supporting social purpose organizationsthrough the application of entrepreneurial and man-agerial skills. Social entrepreneurship is defined as
PublicationsEditor’s note: SIGHT AND LIFE reviews recent publications whichmay be of particular interest to our readers. However, no publicationsother than SIGHT AND LIFE publications are available from us, nordo we have any privileged access to them.
SIGHT AND LIFE Magazine 2009;1:74–75

Magazine Issue 1/2009Publications
75
an innovative, social value-creating activity thatcan occur within or across the nonprofit, business,or government sector. Creating and building sus-tainable social entrepreneurial initiatives not onlyrequires the application and adaptation of businessskills to the social enterprise context, but also thedevelopment of new conceptual frameworks andstrategies tailored specifically to them.
Among its key features, the book provides clearexamples of social enterprise activity from a rangethe nonprofit, business, and government contexts.Not least of such examples are the HarvardBusiness School case studies included, whichaddress critical components of social entrepreneur-ship, including start-up, funding, growth, alliancesand collaboration, and performance measurement.The case studies include not only US cases but alsoa number in international settings. The furtherinclusion of the latest social enterprise researchprovides readers with detailed analyses and frame-works on the key themes and ideas illustratedthroughout the book.
This book will not only deepen interest and under-standing of the practice of social entrepreneurshipamong students, instructors, and practitioners alikebut will also enable social entrepreneurs to achievemission impact as effectively, efficiently, and sus-tainably as possible, and enable them to pursuesocial or non-profit entrepreneurship more strategi-cally in the areas of business, management, market-ing, and public policy.
For more information, please visit http://www.sagepub.com/booksProdDesc.nav?level1=W00&currTree=Subjects&prodId=Book230730.
Nutrition Manual for Humanitarian Action
Mourey A. Nutrition Manual for HumanitarianAction. Geneva: International Committee of theRed Cross (ICRC), 2008.
Written by a nutrition advisor to the ICRC for 24years, this publication contains the distillation ofAlain Mourey’s unique insights on nutrition issues inhumanitarian contexts from his experience of theworld’s worst conflicts and resulting nutritionalcrises.
While nutritional action has, for decades, remainedlargely confined to directly responding to cases ofmalnutrition, Mourey considers nutrition in its
broadest sense and derives practical recommenda-tions for humanitarian action. The manual providesthe scientific basis for action through an in-depthunderstanding of nu trition, which in cludes the socialdimensions of food. It further demonstrates the inter-relations between nutrition and other relevant sec-tors, notably the economy,placing nutritionwithin the legalframework set byinternational human-itarian law, remind-ing readers thatnutritional actionsare not simply tech-nical, but also pertainto the protection ofvictims’ rights intimes of conflict.
Mourey links hisanalysis of the impactof armed conflict andvulnerability with theneed for integratedapproaches in recom-mended responses. This overall approach is definedin chapters devoted to ‘classical’ nutritional inter-ventions, such as general food distributions andnutritional rehabilitation, with an emphasis on plan-ning. He goes further in encouraging the examina-tion of their relevance in terms of context and alter-native forms of response, based on a multidiscipli-nary analysis.
The book delivers on many fronts, not least of whichis the coherent linking of scientific theory with prac-tice, providing the basis for a professional standardfor nutrition responses in humanitarian action. It isavailable in English and French, and can be down-loaded online at http://www.icrc.org/Web/eng/siteeng0.nsf/html/p0820.

Colophon
SIGHT AND LIFE Magazine Incorporating the XerophthalmiaClub Bulletin
Publisher: SIGHT AND LIFEEditor: Klaus KraemerEditorial team: Jee Rah, Anne-Catherine Frey,Svenia Sayer-Ruehmann,
Communication consultancy andtext writing: Frederico Graciano,Jonathan Steffen
Layout and graphics: GAS - graphic art studio,Grenzach-Wyhlen
Printer: Burger Druck, Waldkirch
Language services:transparent, Berlin
Opinions, compilations and figurescontained in the signed articles donot necessarily represent the pointof view of SIGHT AND LIFE andare solely the responsibility of theauthors.
SIGHT AND LIFEDr Klaus KraemerSecretary GeneralPO Box 21164002 Basel, SwitzerlandPhone: +41 61 815 8756Fax: +41 61 815 8190Email: [email protected]
ISBN 978-3-906412-54-2
SIGHT AND LIFE is a humanitarian initiative of DSM
Photo credit: Mike Bloem, p. 8 and 10