Embed Size (px)
Citation preview

Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
SIG Robotics – Understanding
the Robotic Surgery Controversy and
Maximizing the Gains (Didactic)
PROGRAM CHAIR
Antonio R. Gargiulo, MD
PROGRAM CO-CHAIR
Douglas N. Brown, MD
Sawsan As-Sanie, MDMichael C. Pitter, MD
John P. Lenihan, MDSerene S. Srouji, MD
Mona E. Orady, MD

Professional Education Information Target Audience This educational activity is developed to meet the needs of residents, fellows and new minimally invasive specialists in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.

Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 3 Obeying Asimov’s First Law of Robotics: Safety, from Simulation to the Operating Room J.P. Lenihan ................................................................................................................................................... 4 Optimizing the Operating Environment for Robotic Surgery D.N. Brown ................................................................................................................................................. 11 Robotic Surgery Complications and Consideration for the Obese Patient S. As‐Sanie ................................................................................................................................................... 17 Robotic Surgeons Never Go Back: Madmen or Visionaries? A Critical Review of Benefits and Limitations of Gynecologic Robotics
A.R. Gargiulo .................................................................................................................................. 23 Robotic Myomectomy: Hybrid Technique to Single‐Incision S.S. Srouji ..................................................................................................................................................... 33 Robotic Hysterectomy: The Retroperitoneal Four‐Arm Approach M.C. Pitter ................................................................................................................................................... 39 Robotic Hysterectomy: Strategies for the Very Large Uterus M.E. Orady .................................................................................................................................................. 45 Resection of Endometriosis: When Is the Robot the Right Tool? A.R. Gargiulo ............................................................................................................................................... 55 Cultural and Linguistics Competency ......................................................................................................... 63

PG 105 SIG Robotics – Understanding the Robotic Surgery Controversy and Maximizing the Gains
(Didactic)
Antonio R. Gargiulo, Chair Douglas N. Brown, Co-Chair
Faculty: Sawsan As-Sanie, John P. Lenihan, Mona E. Orady, Michael C. Pitter, Serene S. Srouji
Robotic surgery in gynecology has entered the early majority phase of the innovation adoption curve with hundreds of surgeons training every year. Yet, a passionate controversy – highly reminiscent of the early days of video-assisted laparoscopy – envelops almost every aspect of this field. Robotic surgery, though implicitly enabling, creates a novel and unusual surgical environment where the patient is virtually displaced and a new type of operative proficiency is defined by the seamless integration of man and machine. It is widely recognized that most complications and dysfunctions of robotic surgery occur within the phase of transition from conventional surgery. This practice gap highlights the need for more intense preparation and training during this transition process. Led by an expert faculty of surgeons with decades of cumulative experience at the console, the course is divided into two sessions. Session one, in keeping with the goals stated above, will focus on safety and the optimal use of resources in the robotic program. Session two is composed exclusively of practical and interactive lectures, including high-definition video explaining safe techniques and best indications for the use of robotic surgical platforms. This didactic component is complemented by hands-on experience on fresh frozen cadavers and simulators. Both components represent a unique opportunity to close the knowledge and kinesthetic gaps between a surgeon using a robot and a robotic surgeon. Course Objectives: At the conclusion of this didactic activity, the clinician will be able to: 1) Discuss the current controversy surrounding the widespread adoption of robotic surgery in gynecology; 2) identify the appropriate cases to perform at any appropriate stage of the transition to robotic surgery; 3) recognize, troubleshoot and solve common and uncommon problems specific to robotic laparoscopy; 4) choose the most clinically-effective and cost-effective instrument and energy setups for their robotic operations; 5) integrate alternative robotic techniques (such as cosmetic, hybrid and single-incision approaches) to their armamentarium; and 6) define clear protocols for common robotic gynecologic operations.
Course Outline 8:00 Welcome, Introductions and Course Overview A.R. Gargiulo
8:05 Obeying Asimov’s First Law of Robotics: Safety, from Simulation to the Operating Room J.P. Lenihan
8:30 Optimizing the Operating Environment for Robotic Surgery D.N. Brown
8:55 Robotic Surgery Complications and Consideration for the Obese Patient S. As-Sanie
1

9:20 Robotic Surgeons Never Go Back: Madmen or Visionaries? A Critical Review of Benefits and Limitations of Gynecologic Robotics A.R. Gargiulo
9:45 Questions & Answers All Faculty
9:55 Break
10:10 Robotic Myomectomy: Hybrid Technique to Single-Incision S.S. Srouji
10:35 Robotic Hysterectomy: The Retroperitoneal Four-Arm Approach M.C. Pitter
11:00 Robotic Hysterectomy: Strategies for the Very Large Uterus M.E. Orady
11:25 Resection of Endometriosis: When Is the Robot the Right Tool? A.R. Gargiulo
11:50 Questions & Answers All Faculty
12:00 Course Evaluation/Adjourn
2

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor Consultant: Conceptus Incorporated Kimberly A. Kho* Frank D. Loffer, Executive Vice President/Medical Director, AAGL* Linda Michels, Executive Director, AAGL* M. Jonathan Solnik* Johnny Yi* SCIENTIFIC PROGRAM COMMITTEE Ceana H. Nezhat Consultant: Ethicon Endo-Surgery, Lumenis, Karl Storz Other: Medical Advisor: Plasma Surgical Other: Scientific Advisory Board: SurgiQuest Arnold P. Advincula Consultant: Blue Endo, CooperSurgical, Covidien, Intuitive Surgical, SurgiQuest Other: Royalties: CooperSurgical Linda D. Bradley* Victor Gomel* Keith B. Isaacson* Grace M. Janik Grants/Research Support: Hologic Consultant: Karl Storz C.Y. Liu* Javier F. Magrina* Andrew I. Sokol* FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Sawsan As-Sanie* Douglas N. Brown* Antonio R. Gargiulo Consultant: OmniGuide John P. Lenihan, Jr. Speakers Bureau: Intuitive Surgical Other: Proctor: Intuitive Surgical Mona E. Orady Consultant: OmniGuide Michael C. Pitter Speakers Bureau: Intuitive Surgical Serene S. Srouji* Asterisk (*) denotes no financial relationships to disclose.

Obeying Asimov’s First Law of Robotics: Safety, from Simulation to the Operating Room
John P. Lenihan Jr., MDClinical Associate Professor, OB GYN
University of Washington School of MedicineMedical Director of Robotics and MISMultiCare Health Systems, Tacoma WA
Disclosure:
Speakers Bureau: Intuitive Surgical
Other: Proctor: Intuitive Surgical
LEARNING OBJECTIVES
• At the conclusion of this activity, the participant will be able to list and compare the value of utilizing simulation to:
– 1. learn basic robotic skills
– 2. practice to competency
– 3. renew skills after long periods of inactivity
– 4. Use simulation to augment credentialling
Isaac Asimov: 1942
• The Three Laws of robotics are incorporated into almost all of the positronic robots appearing in his fiction, and cannot be bypassed, being intended as a safety feature.
Asimov’s Three Laws of Robotics
• A robot may not injure a human being or, through inaction, allow a human being to come to harm.
• A robot must obey the orders given to it by human beings, except where such orders would conflict with the First Law.
• A robot must protect its own existence as long as such protection does not conflict with the First or Second Law.
Are Robots Dangerous?• WALL STREET JOURNAL• May 4, 2010
• Surgical Robot Examined in Injuries
• By JOHN CARREYROU• DOVER, N.H.—Wentworth‐Douglass Hospital, a small community
hospital in this coastal New England town, used a college hockey game to showcase its new technological marvel: a $1.4 million surgical robot named after Leonardo da Vinci.
• As the University of New Hampshire battled the University of Vermont last season before a crowd of 6,000, hospital representatives invited fans to try out the robot between breaks in the action.
• The da Vinci robot is a massive machine that is used to perform minimally invasive surgery. But some experts warn that the robot can do more harm than good when wielded by inexperienced doctors. WSJ's John Carreyrou reports.
• At Wentworth‐Douglass, however, the robot has been used in several surgeries where injuries occurred. One patient operated on days after the hockey game was so badly injured that she required four more procedures to repair the damage. In earlier robotic surgeries, two patients suffered lacerated bladders.
• There's no evidence to suggest the injuries at Wentworth‐Douglass were caused by technical malfunctions. Surgeons who use the da Vinci regularly say the robot is technologically sound and an asset in the hands of well‐trained doctors. But they caution that it requires considerable practice.
4

Why Consider Simulation?
1. Hysterectomies are being performed less frequently in 20132. Outcomes are worse for low volumes surgeons and low volume centers3. Learning Curves are longer for robotic surgery than other forms4. Robotic Surgery Console Skills degrade faster than other approaches to surgery5. Surgical competency is harder to validate and certify for hospitals
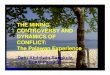
Nationwide Trends in Hysterectomy
1998 543,812
2000 619,255
2002 681,234
2004 600,302
2006 568,350
2008 491,785
2010 433,621
• Increasing use of medications
• Mirena
• Endometrial Ablation
• Embolization, MRI Focused US
• Less Surgeries for fibroids and AUB
• More Outpat Hysts
• CostsWright JD et al. Nationwide Trends in Inpat Hysterectomy in the US. Obstet Gynecol. Aug 2013 122(2), Part 1. 233-41
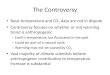
Effect of Surgical Volume on Outcomes for Laparoscopic Benign Hysterectomy
Outcome Low Volume High Volume p
Complications 6.2% 4.2% <.001
Overall Morbidity 5.8% 4.7% <.001
% Cases 2000‐06 39% 61%
% Cases 2007‐10 51% 49%
Hospital Costs $6,527 $5,561 <.001
2000-2010: 124,615 patients
Low Vol: < 6/ lap hysts/yr High Vol: > 14 lap Hysts/yr
Wallenstein MR et. al. Effects of Surgical Volume on Outcomes for Laproscopic Hysterectomy for Benign Conditions. April 2012 Obstet Gynecol.119(4); 710-16.
It looks so Easy!
The Reality: Long Learning Curves GYN Robotic Learning Curve Data
Studies• Lenihan & Kovanda, JMIG
2007: 50 ‐75 Cases• Payne & Dauterie, JMIG 2007:
50 cases, >100 to excel• Kho, Hilger et al., AJOG 2007:
Docking times – 20 cases for team
• Chong, Park et al. Int J Gyn Ca 2009: 50 ‐80 cases GYO’s
• Woelk et. al. Obstet Gynecol 2013: 91 Cases for GYO’s and UroGyns (Cum Sum Analysis)
Therefore, consider
• Learning Curves are longer than you think
• Do simple (Basic) cases for the first 15‐30 surgeries.
• Need to operate Frequently to get through the learning curve
• Low Volume Surgeons may never get through the Learning Curve
5

What happens to robotic skills if not used?
Reached Proficiency
12 weeks inactivity Post‐pig lab retraining
Dots and numbers 126 +/‐ 3(102‐150)
154 +/‐ 10(79‐236)
132 +/‐ 11(74‐315)
Peg board 266 +/‐ 3(229‐285)
356 +/‐ 10(293‐477)
316 +/‐ 10(252‐472)
Suture Pod 95 +/‐ 3(78‐129)
174 +/‐ 10(125‐282)
157 +/‐ 9(93‐231)
Adjusted time to complete trial … Mean +/- (range)
N=22 PG-2 to PG-5 Jennison E et al. Skills Degradation after Robotic Skills Training, Akron General Hospital 2010
P=.001 P=.001
Robotic Console Skills Degrade Quickly
Robotic Console Skills Degradation
• Jenison EL, et al Acquisition, Maintenance, and Degradation
– 4 weeks of inactivity can increase time needed for newly trained surgeons to perform robotic surgery exercises by 25% to 100%
• Training for 1hr bi‐weekly maintains surgical robot skills during robotic inactivity, and also decreases the time to complete a task that was not practiced
• Newly trained robotic surgeons should consider bi‐weekly practice during periods of Robotic Inactivity
Guseila LM, Jenison El et al. Maintaining Robotic Surgical Skills During Periods of Robotic Inactivity presented WRGC V, Chicago Aug 2013
What About Competency?
• Minimum Standards?
• Long Op Times?
• Excessive Complications?
• Anesthesia Concerns?
• Too many conversions?
The Future is Competency Based Credentialing
• Establish Metrics for Operative Standards
– Op Times, EBL, Complications rates, etc.
– Triggers should be determined locally or based on National Data Bases (> 2 SD’s from normal?)*
• Consider retraining or mentoring if a surgeon consistently falls outside standards
– Use of Simulators
– Use of Mentor Surgeons as assistants/proctors
• Include CME component
– Require Advanced courses, national or local meetings, etc.
Two Standard Deviations
MultiCare Health Systems RTLH Standards: 2009
Variable Mean Standard Dev. Median Sample Range
Age 44.85 10.37 44.00 27 ‐ 70
Body Mass
Index (BMI)
28.50 6.27 27.00 18 ‐ 51
Total Op Time
(TOT)
91.95 min 25.57 min 89.00 min 60 – 170 min
Robotic
Console Time
(RCT)
51.79 min 20.48 min 50.00 min 25 – 108 min
Estimated
Blood Loss
(EBL)
43.11 cc’s 25.72 cc’s 35.00 cc’s 10 – 150 cc’s
LOS 25 hours 6 hours 26 hours 10 – 84 hours
Uterine
Weights
189.91 grams 160.34 grams 141 grams 46‐1306 grams
6

What do all of these people have in common?
Practice, Practice, Practice!Practice!
Practice, Practice, Practice!Practice!
How much practice does it take to really get good?
10,000 hours!
Can Simulation Help? • Practice and rehearsal without
clinical consequences
• Reduces reliance on animal models
• Provides standardized experience
• Reduces costs: independently led, less OR resources to practice
• Enables efficient skill development through new surgeon learning curve
Benefits of Simulation
• Long known in Aviation Industry– Can practice basics as well as emergencies
• Current Simulators cover only basic skills– Actual DaVinci Robot – dry lab– Mimic Simulator dV Trainer (stand alone)– DaVinci Backpack Skills Simulator (Si)– RoSS Simulator
• Procedures based trainers now being released– Mimic, Red Llama, Lap Sim and others
• Can be factored into “Currency” for surgeons• Recent studies show pre‐op benefit for experienced surgeons
Robotic Simulators
Intuitive Backpack Skills Simulator
Mimic Dv Trainer
RoSS Simulator
7

Simulationis validated
• "Validating the Use of the Mimic dV‐Trainer for Robotic Surgery Skill Acquisition Among Urology Residents" Department of Urology, Columbia University: Korets R, Mues AC, Graversen JA, Gupta M, Benson MC, Cooper KL, Landman J, Badani KK.
• "Concurrent Validity Testing of a Virtual Reality Robotic Surgical Simulator"Lee JY, Kerbl DC, Mucksavage P, Etafy M, Huynh VB, McDougall EM
• Virtual reality simulator training equals mechanical robotic training in improving robotic‐assisted suturing skills. Halvorsen FH,Elle OJ,Dalinin VV et al. Surg Endos, 2006;20:1565‐69
• The role of surgical simulation in the learning curve of robotic assisted surgery.Al Bareeq R, Jayaraman S,Kiaii B et. al. J Robotic Surg 2008;2:11‐15.
• VR Robotic Surgery:Randomized blinded study of the dV‐Trainer robotic simulator. Lendvay TS. Stud Health Tech Inform. 2008;132:242‐44.
Warm Up Data
Benefit of Warm Up
In a study performed at Arizona State University, subjects performed standardized exercises as a preoperative warm-up, after which the standardized exercises were repeated in a randomized order. Performance metrics were measured during all trials.
VALIDATION:
Morristown NJ Protocol
Validation of a Robotic Surgery Simulator Protocol –Transfer of Simulator Skills to the Operating Room. Patrick Culligan, MD, Charbel Salamon, MS, MD Atlantic Health System, Morristown, NJ. AAGL, Las Vegas 11,2012
n=5 n=14 n=5
Results
First Supracervical Hysterectomy: Robotic Console TimeAverage time for novices to master protocols: 20 hrs. (9.7 – 38.2 hrs)
Instrument Precision
8

Needle Control Energy Applications
Suturing and Knot Tying NEW PARADIGM
• SEE ONE
• DO ONE
• TEACH ONE
• SEE ONE
• SIMULATE MANY
• DO ONE
Proposed Simulation Training Pathways
New Surgeon
• Basic Skills Drill
– Camera targeting
– Ring Walk 1
– Energy Use ‐1
– Peg Board ‐ 1
Annual Recertification Advanced
• Basic Skills Games
• Advanced Skills Team– Energy use 2 Dual Console
– Three arm drills Level 3 skills
– Needle driving Three arm skills
– Knot tying
* Validation Studies in progress
Future Simulation Development
• BASIC SKILLS
• VR Procedures
• Complications
9

Laparoscopic Hysterectomy Trainer for Residents
Port Placement Port & Instrument Selection
SimPraxis®
FRGS: Trains Psycho-Motor SkillsLap Hyst Trainer: Trains Cognitive Skills
SimPraxis® Platform Interactive Simulation Software
with High Fidelity Operating Room Video:
Medical Team
The Virtual Mentor
Back Table & Mayo Stand
HintsDidacticsText Box
Interactive Video
Steps
Tracking & Scoring
Verbal Prompts
Expandable Window
Simultaneous Alternate View
Other Current Developments: 2013• RTN: Residency Training Network:
– Baseline for standardized training of residents
• FLS, FRS, FRGS
• COEMIG (AAGL‐SRC)
• EMIG (ACOG)
Wright JD et al. Nationwide Trends in Inpat Hysterectomy in the US. Obstet Gynecol. Aug 2013 122(2), Part 1. 233-41
Wallenstein MR et. al. Effects of Surgical Volume on Outcomes for Laproscopic Hysterectomy for Benign Conditions. April 2012 Obstet Gynecol.119(4); 710-16.
Guseila LM, Jenison El et al. Maintaining Robotic Surgical Skills During Periods of Robotic Inactivity presented WRGC V, Chicago Aug 2013
Bareeq R, Jayaraman S, Kiaii B et. al. The role of surgical simulation in the learning curve of robotic assisted surgery. J Robotic Surg 2008;2:11-15.
Culligan P, Salamon C, Validation of a Robotic Simulator < Transferring SimulatorSkills to the Operating Room. AAGL, Las Vegas 11, 2012
Lenihan J. Navigating Credentialing, Privileging, and Learning Curves in Robotics With an Evidence and Experience-Based Approach., Clinical Obstetrics and Gynecology. Sep 2011, 54(3), 382-390. (Ed: Advincula A)
Thank You
10

Optimizing the Operating Room for
Robotic Surgery
Douglas N. Brown, MD, FACOG, FACS
Director, Center for Minimally Invasive Gynecologic Surgery
Massachusetts General Hospital
Harvard Medical School
Disclosure Slide
I have no financial relationships to disclose.
Objectives
At the conclusion of this activity, participants will be better able to:
Explain the evidenced based rational for the current controversy surrounding the adoption of robotic surgery in gynecology
Identify areas of pre-operative planning, operative set-up, and post-operative turnover, where a synergistic approach facilitates robotic operative productivity
Apply the knowledge learned to increase operating room efficiency in robotic surgery
Why Does Operating Room Optimization Matter ?
THE Major Criticism of Robotic Surgery
Takes Longer
Increase Cost
What Does the Data Tell Us ?
CONCLUSION: Robot-assisted laparoscopic hysterectomy andconventional laparoscopy compare well in most surgical aspects,but the robotic procedure is associated with longer operating times.
(Obstet Gynecol 2012;120:604–11)
CONCLUSION: Robotic-assisted sacrocolpopexy results in longeroperating time and increased pain and cost compared with theconventional laparoscopic approach.
(Obstet Gynecol 2011;118:1005–13)
CONCLUSION: Laparoscopy and robotics provided similar results for theperformance of adnexectomy, with similar blood loss, intraoperative andpostoperative complications, and length of hospital stay. Robotics meanoperating time was 12 minutes longer.
(Obstet Gynecol 2009;114:581–4)
CONCLUSION: Robotic surgery for tubal anastomosis was successfullyaccomplished without conversion to laparotomy. The robotic techniquefor tubal anastomosis required significantly prolonged surgical andanesthesia times over outpatient minilaparotomy (P<.001).
(Obstet Gynecol 2007;109:1375–80)
11

CONCLUSION: Robot-assisted laparoscopic myomectomy andlaparoscopic myomectomy have similar operative outcomes in a high-volume surgical practice. Operative time and intraoperative estimatedblood loss were significantly greater in the robot-assisted laparoscopicmyomectomy group, but the level of statistical significance forintraoperative estimated blood loss was marginal and the clinicalsignificance was undetermined. Use of barbed suture in thelaparoscopic myomectomy group may account for these differences.
(Obstet Gynecol 2012;120:284–91)
CONCLUSION: Laparoscopy is the least expensive surgical approachfor the treatment of endometrial cancer. Robotic is less costly thanabdominal hysterectomy when the societal costs associated withrecovery time are accounted for and is most economically attractive ifdisposable equipment costs can be minimized.
(Obstet Gynecol 2010;116:685–93)
How Can YouImprove Surgical Efficiency ?
Improve the Technology
Improve the Surgeon
Improve the Operating Environment
Improving Efficiency & TheOperating Environment
A Dedicated Robotic Operating Room
A Dedicated Robotic Surgery TEAM
A Dedicated Robotic Surgeon
The Surgeon Must Be All In...
MGH Operating Room
Photo/Video
A Dedicated Robotic Operating Room (s)
A Dedicated Robotic Surgery TEAM (s)
Surgeon
Circulator (s) (To start usually 2)
Surgical Scrub Tech (To start usually 2)
Surgical Assistant (s)
(Resident, Fellow, Physician Assistant)
Anesthesia
A Single Team is 5-7 Individuals
12

MGH Team Photo
Tips for Pre-Operative Set-Up
Synergy
Anesthesia/Circulator #1 Get Patient from Pre-op
Scrub Tech # 1 & Circulator # 2 - Back Table
Scrub Tech # 2 - Drapes da Vinci Patient Cart
Surgical Assistant (s) - Help with EVERYTHING
The Surgeon Should be Present AND
Should Direct/Assist/Help with EVERYTHING
Tips for Pre-Operative Set-Up
The Surgeon is the Team LEADER
Select Patients Appropriately
Perform Similar Surgery on the SAME Day
i.e.., 2 Myomectomies, 2 Hysterectomies, etc…
Limit the Instrumentation Needed Per Procedure
Uterine Manipulator, Trocars, Suction/Irrigation, Suture,
da Vinci Instrument Selection
(Grasper, Energy Source, Needle Driver)
Tips for Pre-Operative Planning
Patient is in The Operating Room
Synergy
Anesthesia - Intubation, IV access
Surgical Assistant (s), Circulator # 1
Position Patient, Prep Patient, Final Time-Out
Scrub Tech # 1 & Circulator # 2
Confirm Back Table
Set-up Auxiliary Equipment
(Ready for Incision/Insufflation/Foley/Ut Manipulator)
Scrub Tech # 2 – Standby da Vinci Patient Cart
Docking Tips Insufflate Abdomen
Drive the Robot into Position
Tip: Keep Patient in Supine Position
Tip: Use tape on the OR floor for OR Table and Robot
Positioning (Side Docking Position Perfection)
Then Place into Trendelenburg
Tip: Use the Robot Camera to Place Additional Trocars
Photo Photo
13

Video Demonstration
Port Placement
Once Trocars are Placed
Dock the Robotic Arms to the Ports
The Surgeon Moves to the Console
(If Dual Console, Fellow, Resident to Console)
The Surgery Begins…
Docking Tips
Driving & Docking the da Vinci System is a Team Event !Practice Continually !
Completion of Surgery
Synergy Anesthesia - Extubation
Circulator # 1 – Charting
Surgical Assistant (s), Scrub Tech # 1
Undock, Close Ports
Circulator # 2 & Scrub Tech # 2
Roll Out da Vinici System
Undrape, Clean, Prep for Next Case
Send Scopes/Instruments to Central Processing
Help Scrub Tech # 1 Clear Back Table
Completion of Surgery
Patient Exits the OR
Anesthesia & Circulator # 1
Recovery / Next Patient
Surgeon/Surgical Assistant (s)
Speak to Family / Next Patient
Circulator # 2 & Scrub Tech # 1 & # 2
Turnover & Set-Up for Next Case
Pause For Effect
14

What Does the Data Tell Us ?
Dedicated Robotics Team Reduces Pre-Surgical Preparation Time
Lasser MS, Patel CK, Elsamra SE, Renzulli JF, Halebilian GE, Pareek G.
CONCLUSION: The use of a consistent staff candecrease preoperative setup times and, therefore,the overall length of surgery.
(Indian J Urol. 2012 Jul;28(3):263-6)
What Does the Data Tell Us ?
RESULTS: From July 2009 through June 2011, 1295 roboticcases were performed. Profitability was associated with case time,payor mix, and procedure type (all P < .05). Urogynecology casetime decreased from 220-179 minutes (P . .012) and pediatricsurgery from 418-258 minutes (P . .019)
CONCLUSION: Robotic operative efficiency has a large impact onoverall profitability regardless of surgical specialty.
(Am J Obstet Gynecol. 2013 Mar 25)
The 4 R’s
Right Patient
Right Surgical Procedure
Right Surgeon
Right Timing
The 7 P’s
Proper
Pre-Operative
Preparation
Prevents
Piss-Poor
Performance
Final Thoughts
This is a TEAM Effort
Move with a Purpose
Inspire Your Team to be Motivated
Be Positive, Be Gracious, Be Present...
Be a True LEADER!
References1. Dimitri Sarlos, MD, LaVonne Kots, MD, Nebojsa Stevanovic, MD, Stefanie von Felten, PhD, and Gabriel Scha¨r, MD.
Robotic Compared With Conventional Laparoscopic Hysterectomy. Obstet Gynecol 2012;120:604–11.
2. Marie Fidela R. Paraiso, MD, J. Eric Jelovsek, MD, Anna Frick, MD, MPH, Chi Chung Grace Chen, MD, and Matthew D. Barber, MD, MHS. Laparoscopic Compared With Robotic Sacrocolpopexy for Vaginal Prolapse. Obstet Gynecol2011;118:1005–13.
3. Javier F. Magrina, MD, Mercedes Espada, MD, Raquel Munoz, MD, Brie N. Noble, and Rosanne M. C. Kho, MD. Robotic Adnexectomy Compared With Laparoscopy for Adnexal Mass. Obstet Gynecol 2009;114:581–4.
4. Allison K. Rodgers, MD, Jeffrey M. Goldberg, MD, Jeffrey P. Hammel, MS, and Tommaso Falcone, MD. Tubal Anastomosis by Robotic Compared With Outpatient Minilaparotomy. Obstet Gynecol 2007;109:1375–80.
5. Jason C. Barnett, MD, John P. Judd, MD, Jennifer M. Wu, MD, Charles D. Scales Jr, MD, Evan R. Myers, MD, and Laura J. Havrilesky, MD. Cost Comparison Among Robotic, Laparoscopic, and Open Hysterectomy for Endometrial Cancer. Obstet Gynecol 2010;116:685–93.
6. Ehab E. Barakat, MD, Mohamed A. Bedaiwy, MD, Stephen Zimberg, MD, Benjamin Nutter, Mohsen Nosseir, MD, and Tommaso Falcone, MD. Robotic-Assisted, Laparoscopic, and Abdominal Myomectomy: A Comparison of Surgical Outcomes. Obstet Gynecol 2011;117:256–65.
7. Lasser MS, Patel CK, Elsamra SE, Renzulli JF, Halebilian GE, Pareek G. Dedicated Robotics Team Reduces Pre-Surgical Preparation Time. Indian J Urol. 2012 Jul;28(3):263-6.
8. Geller EJ, Matthews CA. Impact of robotic operative efficiency on profitability Am J Obstet Gynecol. 2013 Mar 25.
15

Thank You
16

Robotic Surgery Complications and Considerations for the Obese Patient
Sawsan As‐Sanie, MD MPHAssistant Professor
Director, Minimally Invasive Gynecologic Surgery and Fellowship
University of Michigan
Disclosures
I have no financial relationships to disclose.
Objectives
1. Describe surgical complications associated with robotic surgery
2. Identify strategies to avoid such complications
3. Discuss special considerations for the obese patient
Surgical complications are uncommon
• Major surgical complications are uncommon
• Complications with robotic procedures are not more likely than with traditional laparoscopy
• Significantly less morbidity than open cases
Wright JD, et al. JAMA. 2013 Feb 20;309(7):689-98Patzkowsky KE, et al. JSLS. 2013 Jan-Mar;17(1):100-6.
Complications may be related to surgeon experience & hospital volume
Wallenstein MR, et al. Obstet Gynecol. 2012. Apr;119(4):709-16.
Robotics is a tool and most surgical complications are not unique to robotic approach
• Vascular
• Bowel
• Urinary tract (bladder, ureter)
• Know your anatomy!
17

Perioperative Neuropathies
• Incidence varies, depending on type of surgery, surgical approach, patient position, length of surgery, patient risk factors
– Range 1.9 – 10 %
• Nerve injuries represent approximately 1/3 of all anesthesia ‐ associated medicolegal claims in the United States
Elevated risk of nerve injury ?
• Nerve injuries may be related to inappropriate or unstable patient positioning
• Risk elevated in prolonged surgery, patients with medical comorbidities, steep trendelenberg
• Surgeon is not in constant, direct contact with patient
Brachial Plexus•Anterior nerve roots of C5 – T1
•Pass behind clavicle, under axillary artery, over first rib
•Motor & sensory nerves innervate shoulder, scapula, and upper extremity
Brachial Plexus Ulnar nerve
• Passes across the elbow in the olecranon groove, between the medial epicondyle and the ulnar bone
• Sensory & motor innervation to medial 4th & 5th finger
Location of ulnar nerve in supination vs. pronation Peroneal nerve
• Arises from the posterior tibial branch of sciatic nerve
• Fixed at head of fibula
• Particularly sensitive to compression injury
• Symptoms: Sensory loss over the lateral aspect of the leg below the knee and the dorsum of the foot, foot drop
18

Complications to consider
• Combination of steep trendelenberg and prolonged surgery can increase risk of rare complications
– Orbital edema, retinal detachment, permanent loss of vision
– Cerebral edema, laryngeal edema
– Rhabdomyolysis, compartment syndrome of lower extremity
– Pressure alopeciaAwad H, et al. J Clin Anesth. 2012 Sep;24(6):494-504
Key aspects of appropriate position• Gel, foam, or beanbag to prevent slippage
• Avoid shoulder blocks
• Hip flexion 170°
• Hip abduction <90°
• Minimal external rotation of hip
• Arms padded at elbows and wrists, thumbs up or arms supinated
• Arms should not hang over side of bed, use bed extension if necessary
• Avoid bunching of foam or sheet in axilla
Robot Malfunction
• Uncommon, but may lead to conversion to alternative surgical approach
• Resultant patient injury extremely rare
• Fail‐safe mechanisms to prevent patient injury
• Reported robot malfunction rate may be inversely related to hospital volume of robotic procedures.
Zorn KC, et al. J Endourol. 2007 Nov;21(11):1341-4.
Robot Malfunction
• Insulation failures
• Uncontrolled arms
– Never leave arms in patient if away from console
– Always keep all arms in view
– Make sure don’t toggle arms accidentally
– Excessive force of arms
Obesity epidemic
• 35.7% of American adults and 16.9% of children are obese (BMI>30)
• By 2030, obesity rates could exceed 44% nationally, and over 50% in some states
• Obesity is associated with increased risk of other medical comorbidities that predispose patients to greater surgical risk
Increased surgical risks in the obese
Intraoperative challenges
• Difficult intubation
• Airway obstruction
• Higher expiratory airway pressure
Postoperative risks
• Wound infection
• Pneumonia
• Atelectasis
• DVT/PE
• ileus
19

Robotic surgery is feasible and safe in obese patients
Gallo et al. JSLS. 2012 Jul-Sep;16(3):421-7
Robotic surgery is feasible and safe in obese patients
Gallo et al. JSLS. 2012 Jul-Sep;16(3):421-7
Impact of abdominal wall thickness on trocar range of motion
Zorn KC. Robotic surgery techniques for obese patients. Can Urol Assoc J. 2010, 4(4):255-6.
Special considerations for the obese
• Patient positioning to reduce risk of nerve injury
• Distorted landmarks for trocar placement
• Adequate retraction of bowel to allow for adequate visualization of critical structures
Patient positioning
• Gel pad, foam pad, or bean bag in direct contact to patient back and buttocks
• Avoid use of shoulder brackets
• Padded elbows and wrists
• Extended arm supports
• Avoid bunching of padding or draping under axilla
Patient positioning
• Panniculus is stretched downward and taped to patient’s thigh
• Use bony landmarks, not umbilicus, to guide trocar placement
Geppert B, et al. Acta Obstet Gynecol Scand. 2011, 90(11):1210‐7.
20

Port Placement
Geppert B, et al. Acta Obstet Gynecol Scand. 2011, 90(11):1210‐7.
Tips for improving visualization
• Minimum trendelenburg necessary
• retract bowel prior to docking
• Additional 5mm assist trocar
• Suture sigmoid epiploica to left lower quadrant abdominal wall
• 10mm paddle retractor if above is insufficient
Caution!
Do not lose track of time… Prolonged operative time is a significant risk marker for surgical morbidity
Checklist for 2nd time‐out in extended robotic surgeries
1. Wright JD, Ananth CV, Lewin SN, Burke WM, Lu YS, Neugut AI, Herzog TJ, Hershman DL. Robotically assisted vs laparoscopic hysterectomy among women with benign gynecologic disease. JAMA. 2013 Feb 20;309(7):689‐98.
2. Patzkowsky KE, As‐Sanie S, Smorgick N, Song AH, Advincula AP. Perioperative outcomes of robotic versus laparoscopic hysterectomy for benign disease. JSLS. 2013 Jan‐Mar;17(1):100‐6.
3. Wallenstein MR, Ananth CV, Kim JH, Burke WM, Hershman DL, Lewin SN, Neugut AI, Lu YS, Herzog TJ, Wright JD. Effect of surgical volume on outcomes for laparoscopic hysterectomy for benign indications. Obstet Gynecol. 2012 Apr;119(4):709‐16.
4. Awad H, Walker CM, Shaikh M, Dimitrova GT, Abaza R, O'Hara J. Anesthetic considerations for robotic prostatectomy: a review of the literature. J Clin Anesth. 2012 Sep;24(6):494‐504.
5. Zorn KC, Gofrit ON, Orvieto MA, Mikhail AA, Galocy RM, Shalhav AL, Zagaja GP. Da Vinci robot error and failure rates: single institution experience on a single three‐arm robot unit of more than 700 consecutive robot‐assisted laparoscopic radical prostatectomies. J Endourol. 2007 Nov;21(11):1341‐4.
6. Andonian S, Okeke Z, Okeke DA, Rastinehad A, Vanderbrink BA, Richstone L, Lee BR. Device failures associated with patient injuries during robot‐assisted laparoscopic surgeries: a comprehensive review of FDA MAUDE database. Can J Urol. 2008 Feb;15(1):3912‐6.
7. Zorn KC. Robotic surgery techniques for obese patients. Can Urol Assoc J. 2010, 4(4):255‐6.
8. Song JB, Vemana G, Mobley JM, Bhayani SB. The second "time‐out": a surgical safety checklist for lengthy robotic surgeries. Patient Saf Surg. 2013 Jun 3;7(1):19
21

9. Geppert B, Lönnerfors C, Persson J. Robot‐assisted laparoscopic hysterectomy in obese and morbidly obese women: surgical technique and comparison with open surgery. Acta Obstet Gynecol Scand. 2011, 90(11):1210‐7.
10. Gallo T, Kashani S, Patel DA, Elsahwi K, Silasi DA, Azodi M. Robotic‐assisted laparoscopic hysterectomy: outcomes in obese and morbidly obese patients. JSLS. 2012 Jul‐Sep;16(3):421‐7
22

A Critical Review of the Benefits
and Limitations of Gynecologic Robotics
Antonio GargiuloMedical Director, Center for Robotic Surgery
Brigham and Women’s Health CareHarvard Medical School
Gargiulo 2013Gargiulo 2013
Consultant: OmniGuide
Participants should be able to :
• Interpret relevant scientific publications on benefits
and limitations of robotic gynecologic surgery
• Describe the ergonomic limitations of laparoscopy
and their occupational and bioethical correlates
• Identify relevant areas of clinical investigation in the
field of gynecologic robotics
Gargiulo 2013Gargiulo 2013
The Most Expensive Hysterectomy.
MS Baggish. J Gynecol Surg, 1992
Operative Laparoscopy: Surgical Advance or
Technical Gimmick?
RM Pitkin. Obstet Gynecol, 1992
Breaking New Ground or Just Digging a Hole? An
Evaluation of Gynecologic Operative Laparoscopy.
FM Howard. J Gynecol Surg, 1992
Gargiulo 2013Gargiulo 2013
23

Changing hysterectomy patterns after introduction of
laparoscopically-assisted vaginal hysterectomy
MB Harris and DL Olive. Am J Obstet Gynecol, 1994
LAVH can decrease the number of patients requiring
a laparotomy for hysterectomy, but at a much greater
cost (average cost $11,932 for LAVH vs. $7031 for
abdominal hysterectomy).
Gargiulo 2013Gargiulo 2013
Hospital cost comparison between abdominal, vaginal
and laparoscopy-assisted vaginal hysterectomy.
C Nezhat et al. Obstet Gynecol, 1994
The use of laparoscopy to perform a hysterectomy was
associated with much higher cost.
Predicted savings associated with shorter hospital stay
failed to offset the exorbitant intraoperative costs.
Gargiulo 2013Gargiulo 2013
Costs and charges associated with three alternative
techniques of hysterectomy.
JH Dorsey et al. N Engl J Med, 1996
Despite shorter hospital stays, in-hospital charges and
costs for laparoscopically assisted vaginal
hysterectomy are higher than for either alternative
procedure.
Gargiulo 2013Gargiulo 2013
A randomized trial with a cost-consequence analysis after
laparoscopic and abdominal hysterectomy.
M Ellström et al. Obstet Gynecol, 1998
A randomized comparison and economic evauation of
laparoscopic-assisted hysterectomy and abdominal
hysterectomy. MA Lumsden et al. BJOG, 2000
Cost effectiveness analysis of laparoscopic hysterectomy
compared with standard hysterectomy: results from a
randomised trial. M Sculpher et al. BMJ, 2004
Gargiulo 2013Gargiulo 2013
Surgical approach to hysterectomy for benign gynecological
disease N Johnson et al. Cochrane Datab Syst Rev, 2005
“Further research is required to define the role of the newer
approaches to hysterectomy, such as total laparoscopic
hysterectomy (TLH)”.
When robotic hysterectomy was approved by the FDA,
TLH was not a proven cost-effective alternative to TAH.
Only 14% of hysterectomies in the USA were
laparoscopic at 18 years from its introduction.
Gargiulo 2013Gargiulo 2013
24

At 10 years from FDA approval, 90% of radical
prostatectomies performed robotically.
No definitive evidence of higher safety over open
prostatectomy to justify the increased cost.
Hu et al. JAMA, 2009 (RALP more complications than RP)
Bolenz et al. Eur Urol, 2010 (RALP costs more than RP)
WHY !?
Gargiulo 2013Gargiulo 2013
The NSQIP database (identifies complications up to 30
days post-operatively) was queried 2005-2010 for robotic
plus laparoscopic vs. open prostatectomy.
JJ Liu et al. Urology, 2013
First evidence: clinical superiority of RALP/LP over RP
Using the right database for the question was key!
Gargiulo 2013Gargiulo 2013
RALP/LP RRP P‐value
Blood Transfusion 1.34% 21.4% <0.0001
Major Complications 4.98% 9.04% <0.0001
Death 0.05% 0.39% 0.01
Tracking the rise of robotic surgery for prostatic cancer
“A large, randomized clinical trial comparing the
approaches seems out of the realm of possibility at this
point… and may not even be that informative.
If you have an expert surgeon doing either procedure you
are likely to have an excellent outcome.”
NCI Bulletin, August 2011
Gargiulo 2013Gargiulo 2013
Recruitment period: 5 years
Number of Surgeons: 5
Number of robotic hysterectomies (RH): 26
Average number of enrolled RH/year/surgeon: 1
Paraiso et al. Am J Obstet Gynecol, 2013
Gargiulo 2013Gargiulo 2013
JD Wright et al. JAMA 2013
25

• Largest non-inferiority study to date.
• The rise of robotic hysterectomy correlates with
the fall of abdominal hysterectomy.
• … but the focus is on the $2000 difference.
JD Wright et al. JAMA 2013Gargiulo 2013Gargiulo 2013
• DOES NOT REPORT ON CONVERSION RATE
(converted cases were billed as laparotomy).
Conversion rates are 6% for LH, vs 1% for RH, as
reported by advanced MIS teams.
KE Patzkowsky et al. JSLS, 2013
• The Perspective database does not capture post-
discharge complications (transfusions, readmissions)
• The above may artificially decrease the cost of LH
Gargiulo 2013Gargiulo 2013
“A recent JAMA study found that… robotics added an average
of $2000 per procedure without any demonstrable benefit.”
Incorrect: the study showed decrease of open hysterectomy
Gargiulo 2013Gargiulo 2013
“If most women… chose a vaginal or laparoscopic
procedure… dramatic savings to our health system.”
Unrealistic: will address in myomectomy section
“An estimated $960 million to 1.9 billion will be added
to the health care system if robotic surgery is used for
all hysterectomies each year”.
Incorrect: the direct and indirect savings from
avoidance of open hysterectomy would compensate!
26

ACOG is implying that minimally invasive
hysterectomy has a complexity comparable to
minimally invasive cholecystectomy.
After 20 years of stifling advanced minimally
invasive gynecologic surgery, ACOG is now
implying that our specialty is ready to offer it to
“most women”, hence we do not need robots.
Gargiulo 2013Gargiulo 2013
RCTs show superior outcome of LM over AMMais et al. Am J Obstet Gynecol, 1996
Seracchioli et al. Hum Reprod, 2000
Palomba et al. Fertil Steril, 2007
“There are robust surgical outcome data supporting the use of a minimally invasive approach such as laparoscopy and hysteroscopy over laparotomy”.
Falcone and Parker, Obstet Gynecol, 2013
Gargiulo 2013Gargiulo 2013
41.1% returned
39.9% included in analysis
94.7% practice gynecology
91.5% perform laparoscopy
3.1% perform LM in over 50% of cases
24.5% perform LM
Questionnaires distributed to 100% of Canadian Ob/Gyn
G Liu et al. J Obstet Gynecol Can, 2010
Gargiulo 2013Gargiulo 2013
Intramural Fibroid (81%)
Fibroid > 5 cm (54%)
> 3 Fibroids (53%)
Posterior Fibroid (29%)
Previous surgery (14%)
Obese patient (25%)
Clinical deterrents to performing LM
G Liu et al. J Obstet Gynecol Can, 2010
Gargiulo 2013Gargiulo 2013
Lack of training (71%)
Operative time constraints (53%)
Lack of equipment (52%)
Insufficient evidence to support (35%)
High cost (25%)
Higher complication rate (27%)
Barriers to performing LM
G Liu et al. J Obstet Gynecol Can, 2010
Gargiulo 2013Gargiulo 2013
“…research in pure science leads to revolutions, and revolutions, whether political or industrial, are exceedingly profitable things if you are on the winning side.”
Sir J.J. Thomson, Nobel Prize in Physics, 1906
27

TIME since technique adoption
PR
OF
ICIE
NC
Y
Gargiulo 2013Gargiulo 2013
• Ethically impossible to design studies like Stefanidis’ on
Human Subject: THEY WILL NEVER BE DONE
• Reported learning curves (LC) for gynecologic robotic
procedures vary with definition of technical competence
• A comparative study in gynecology does not yet exist.
• Radical prostatectomy (RP) comparative LC study:
LC Open RP: 250-1000 cases
LC Laparoscopic RP: 200-750 cases
LC Robotic RP: 40 cases
H Abboudi et al. Br J Urology, 2013
n Findings Limitations
Nezhat et al. 2009
15 vs. 34 Longer OR time for RM (234 vs. 203 min)
Small study, includes RM learning curve
Bedient et al. 2009
40 vs. 41 No difference(141 vs. 166 min)
Small study, includes RM learning curve
Barakat et al. 2011
89 vs. 93 Higher tumor load in RM.No difference (181 vs. 155 min)
High-volume RM vs. low-volume LM teams
Gargiulo et al. 2011
174 vs. 115
Longer OR time for RM (195 vs 118 min)
LM barbed suture 70%RM barbed suture 5%
Perioperative outcomes of RM and LM are comparable. Pundir et al, J Minim Invasive Gynecol, 2013 (Meta-analysis)
Gargiulo 2013Gargiulo 2013
• Raising the threshold for open conversion• Cervical and retroperitoneal pathology
• Surgery in the frozen pelvis
• Surgery in the obese patient
• Minimizes assistant factor
• Posing ethical challenge as technical enabler • Shortened learning curve
• Standardized simulation
• Improved ergonomics (vision, dexterity, posture)
Gargiulo 2013Gargiulo 2013
Patients benefit while surgeons suffer: an
impending epidemic.
A Park et al. J Am Coll Surg, 2010
87% of SAGES members respondents reported
physical symptoms or injuries.
Strongest predictor: high case volume
(eye and back symptoms also low case volume).
No relationship with height, age, practice length.
28

Work-related musculoskeletal disorders when
performing laparoscopic surgery.
MW Stomberg, Surg Laparosc Endosc Percutan
Tech, 2010
More than 70% of laparoscopists reported one or
more symptom (pain, fatigue, stiffness).
Lower back, neck shoulders most affected.
Headache and visual discomfort also reported.
Longer workload/ageing: more disorders (p<0.01).
Female surgeons: more disorders (p<0.01).
Physical strain and urgent need for ergonomic
training among gynecologic oncologists who
perform minimally invasive surgery.
J Franasiak et al, Gynecol Oncol, 2012
88% of SGO members respondents reported
physical discomfort related to MIS.
52% reported PERSISTENT pain.
29% received formal treatment:
• Physical therapy: 29%
• Medical management: 28%
• Surgery: 13%
• Time off: 1%
Physical strain and urgent need for ergonomic
training among gynecologic oncologists who
perform minimally invasive surgery.
J Franasiak et al, Gynecol Oncol, 2012
Direct relationship with: height, glove size, age
and female gender.
Association with Patient BMI: for laparoscopic, but
not for robotic surgery.
Pain avoidance behaviors:
• Modify positions: 78%
• Limited cases/day or total cases: 17%
• Spread cases in week: 6%
Work-related upper limb musculoskeletal
disorders in paediatric laparoscopic surgery.
A multicenter survey.
C Esposito et al, J Pediatr Surg, 2013
78.2% of laparoscopists with over 10 year
experience have work-related shoulder symptoms.
44% of these require analgesics ≥ twice weekly.
Attitudes:
1) 1) 55% think pain related to laparoscopy;
2) 2) 43% think laparoscopy good for patients but
damaging to surgeons;
3) 3) 65% think robotic surgery improves ergonomics
MM Lux et al. J Endourol, 2010
29

• Minimizing cosmetic impact in Women’s Health• Reduced port laparoscopy
• Single port laparoscopy
• Exponential development of electronics• Miniaturization and multi-channel technology
• Safe Natural Orifice Transluminal Endoscopic Surgery
• Enhanced vision and pathology targeting
• Centers of Excellence in Telesurgery
• Automation
• Decreased production/operation costsThe Singularity is Near: When Humans Transcend BiologyR Kurtzweil, 2005
The Singularity is Near: When Humans Transcend BiologyR Kurtzweil, 2005
Gargiulo 2013Gargiulo 2013
30

Comparative study of outcome data on 6 procedures (open vs. MIS): cholecystectomy, colectomy, fundoplication, ventral hernia repair, appendectomy and hysterectomy.
• Reduced hospital stay
• Reduced hospital costs
• Reduced societal costs (faster return to work)
• Increased operating room time/costs
• Increased surgical equipment costs
“As both the outcome value and the level of operating room resources are greater, MIS warrants reimbursement that meets or exceeds that of open procedures”.AR Roumm et al. Surg Innov, 2005
Gargiulo 2013Gargiulo 2013
The Most Expensive Hysterectomy.
MS Baggish. J Gynecol Surg, 8 (2) , 57-8, 1992
Operative Laparoscopy: Surgical Advance or Technical
Gimmick? RM Pitkin. Obstet Gynecol, 79:3, 441-2, 1992
Breaking New Ground or Just Digging a Hole? An Evaluation
of Gynecologic Operative Laparoscopy.
FM Howard. J Gynecol Surg, 8 (3): 143-58, 1992
Changing hysterectomy patterns after introduction of
laparoscopically-assisted vaginal hysterectomy
MB Harris and DL Olive. Am J Obstet Gynecol, 171 (2): 340-
3, 1994Gargiulo 2013Gargiulo 2013
Hospital cost comparison between abdominal, vaginal and
laparoscopy-assisted vaginal hysterectomy.
C Nezhat et al. Obstet Gynecol, 83 (5): 713-6, 1994
Costs and charges associatred with three alternative
techniques of hysterectomy.
JH Dorsey et al. N Engl J Med, 335 (7): 512-3, 1996
A randomized trial with a cost-consequence analysis after
laparoscopic and abdominal hysterectomy.
M Ellström et al. Obstet Gynecol, 91 (1) : 30-4, 1998
Gargiulo 2013Gargiulo 2013
A randomized comparison and economic evauation of
laparoscopic-assisted hysterectomy and abdominal
hysterectomy. MA Lumsden et al. BJOG, 107 (11), 1386-91,
2000
Cost effectiveness analysis of laparoscopic hysterectomy
compared with standard hysterectomy: results from a
randomised trial. M Sculpher et al. BMJ, 328 (7432): 134,
2004
Surgical approach to hysterectomy for benign gynecological
disease. N Johnson et al. Cochrane Database Syst Rev, (1)
CD003677, 2005
Gargiulo 2013Gargiulo 2013
Cost comparison of robotic, laparoscopic, and open radical
prostatectomy for prostate cancer. C Bolenz et al. Eur Urol,
57(3), 453-8, 2010
Comparative effectiveness of minimally invasive vs open
radical prostatectomy. J Hu et al. JAMA, 302(14): 1557-64
National Cancer Institute (NCI) Cancer Bulletin. August 9, Vol
8(16), 2011
Perioperative outcomes for laparoscopic and robotic
prostatectomy using the national surgical quality
improvement program (NSQIP) database.
JJ Liu et al. Urology, 189(4S):151
Gargiulo 2013Gargiulo 2013
31

Robotically assisted vs laparoscopic hysterectomy among
women with benign gynecologic disease. JD Wright et al.
JAMA, 309(7): 689-98, 2013
Perioperative outcomes of robotic vs laparoscopic
hysterectomy for benign disease. KE Patzkowsky et al.
JSLS, 17(1): 100-6, 2013
Laparoscopic versus abdominal myomectomy: a prospective,
randomized trial to evaluate benefits in early outcome. V
Mais et al. Am J Obstet Gynecol 174: 654-8, 1996
Gargiulo 2013Gargiulo 2013
Fertility and obstetric outcome after laparoscopic
myomectomy of large myomata: a randomized comparison
with abdominal myomectomy. R Seracchioli et al. Hum
Reprod 15: 2663-8, 2000
A multicenter randomized, controlled study comparing
laparoscopic versus minilaparotomic myomectomy:
reproductive outcomes. Palomba et al. Fertil Steril 88: 933-
41, 2007
Surgical management of leiomyomas for fertility or uterine
preservation. T Falcone and WH Parker, Obstet Gynecol 121
(4): 856-68, 2013
Gargiulo 2013Gargiulo 2013
The laparoscopic myomectomy: a survey of Canadian
gynecologists. G Liu et al. J Obstet Gynecol Can 32 (2): 129-
148, 2010
Robotic assistance improves intracorporeal suturing
performance and safety in the operating room while
decreasing operator workload. D Stefanidis et al. Sug
Endosc 2492):377-82, 2010
A randomized trial comparing conventional and robotically
assisted laparoscopic hysterectomy. Paraiso et al. Am J
Obstet Gynecol, 208: 368, 2013
Gargiulo 2013Gargiulo 2013
Learning curves for urological procedures. H Abboudi et al.
Br J Urology June 18, 2013 doi: 10.1111/bju.12315 [Epub]
Robotic-assisted vs. abdominal and laparoscopic
myomectomy: systematic review and meta-analysis. Pundir
et al, J Minim Invasive Gynecol 20 (3): 335-45, 2013
Patients benefit while surgeons suffer: an impending
epidemic. A Park et al. J Am Coll Surg, 2010
Work-related musculoskeletal disorders when performing
laparoscopic surgery. MW Stomberg, Surg Laparosc Endosc
Percutan Tech, 2010
Gargiulo 2013Gargiulo 2013
Physical strain and urgent need for ergonomic training
among gynecologic oncologists who perform minimally
invasive surgery.J Franasiak et al. Gynecol Oncol, 2012
Work-related upper limb musculoskeletal disorders in
paediatric laparoscopic surgery. A multicenter survey. C
Esposito et al. J Pediatr Surg, 2013
The Singularity is Near: When Humans Transcend BiologyR Kurtzweil, Viking Press, 2005
Ergonomic evaluation and guidelines for for use of the
daVinci Robot system. MM Lux et al. J Endourol 24(3):371-5
Gargiulo 2013Gargiulo 2013
Minimally invasive: minimally reimbursed? An examination of
six laparoscopic surgical procedures. AR Roumm et al. Surg
Innov 13(1):16, 2005
Gargiulo 2013Gargiulo 2013
32

SERENE SROUJI MD
BRIGHAM AND WOMEN’S HOSPITAL
I have no financial relationships to disclose.
• Develope a preoperative assessment to plan appropriate surgical approach
• Describe the steps of a traditional robotic myomectomy and techniques utilized to optimize reproductive outcomes
• Identify suitable patients for different robotic myomectomy approaches including hybrid robot-assisted laparoscopic myomectomy, cosmetic robotic myomectomy, and single incision robotic myomectomy
HISTORY OF ROBOTIC MYOMECTOMY
Operative Outcomes Mean + SD (95% CI)
Diameter of Myomas (cm) 7.9 + 3.5, (6.63‐9.13)
Myoma weight (gm) 223.2 + 244.1 (135.8‐310.6)
Operating time (min) 230.8 + 83, (201.6‐260)
Estimated blood loss (mL) 169 + 198.7, (99.1‐238.4)
Number of myomas 1.6 (range 1‐5)
Advincula Journal Am Assoc Gyn Laparoscopists 2004
35 Cases attempted with conversion rate 8.6%
Barakat Obstet Gynecol 2011
ROBOTIC (RM) vs. LAPAROSCOPIC (LM) vs. ABDOMINAL MYOMECTOMY (AM)
RM (n=89) LM (n=93) AM (n=393)
Weight myoma (gm)* 223 (85,391) 96.7 (49, 227) 263 (90.5, 449)
Surgical time (min)** 181 (151, 265) 155 (98,200) 126 (95, 177)
Blood loss (mL)*** 100 (50, 212) 150 (100, 200) 200 (100, 437)
Hospital stay (d)*** 1 (1,1) 1 (0,1) 3 (2,3)
*RM=AM>LM**AM=LM, LM=RM, AM<RM***LM=RM<AM
PREGNANCY AFTER ROBOTIC MYOMECTOMY107 myomectomies, 127 pregnancies and 92 deliveriesPregnancy CharacteristicsMode of conception Spontaneous 77 (60.6%)
ART 50 (39.4%)Time to conception 9.3 months (0.71‐65.4)SAB (<14 weeks) 21 (16.5%)
Delivery CharacteristicsAge at Delivery 36 years (23‐51)AMA 59 (64%)EGA 37.3 weeks (24.4‐41.7)Premature delivery
< 28 weeks 2 (2.2%)28‐32 weeks 1 (1.1%)32‐35 weeks 13 (14.1%)
Adhesions 10 (11.4%)
** One uterine rupture (1.1%) occurred at 33 weeks Pitter Hum Repro 2013
33

PLANNING SURGERY
• MRI has superior sensitivity as compared to other imaging modalities for detecting myomas and ruling out adenomyosis
• MRI can be used to “map” out procedure, given lack of haptic feedback
Dueholm Fert Steril 2001
OPTIMIZING OUTCOMES
TREAT PREOPERATIVE ANEMIA
• Women with Hgb <9.0 g/dL given iron x 3wks,
• Intravenous iron increased Hgb 3.0 g/dL
• Oral iron increased Hgb 0.8 g/dL
• Women with Hgb ~10 g/dL treated for 12 weeks
• 74% had Hgb>12 g/dL on GnRH + iron
• 46% had Hgb >12g/dL on iron only
Kim Acta Haem 2009, Wurnig Eur Surg Res 2001
OPTIMIZING OUTCOMES
MINIMIZE BLOOD LOSS
• Vasopressin results in significant decrease in blood loss
• Utilize a 7‐inch, 22‐gauge needle through accessory port or suprapubic/transabdominal
• Use dilute solution 0.2 U/mL, and limit dose– Case reports of bradycardia, cardiac arrest and pulmonary edema
• Utilize horizontal hysterotomy if possible
Hobo Obstet & Gynecol 2009; Kongnyuy Cochrane Database Syst Rev 2011
OPTIMIZING OUTCOMESMINIMIZE BLOOD LOSS & DECREASE OPERATIVE TIME
44 women undergoing laparoscopic myomectomy randomized to unidirectional barbed suture vs. continuous suture with intracorporeal knots
• Less time for hysterotomy repair
• 11.5 + 4.1 minutes vs. 17.4 + 3.8 minutes, p<0.01
• Less blood loss
• ΔHgb 0.6 + 0.3 g/dL vs. 0.9 + 0.4 g/dL, p=0.004
Alessandri J Min Invas Gynecol 2010
OPTIMIZING OUTCOMES
AVOID MYOMETRIAL DAMAGE
• Review of risk factors for uterine rupture:
• Electrosurgery
• Hematoma formation due to lack of multilayer closure
• Utilize ultrasonic energy or laser energy for hysterotomy
Parker J Minim Invasive Gynecol 2010
OPTIMIZING OUTCOMES
AVOID ROBOTIC ARM COLLISIONS
• Utilize bariatric trocar for camera trocar (150mm)
• Elevates camera arm to decrease collisions and increases range of motion of robotic arms
34

OPTIMIZING OUTCOMES
DECREASE ADHESION FORMATION
• Robotic myomectomy resulted in only 11% adhesive disease at time of C‐section
• Antiadhesion barriers shown by Cochrane review to prevent adhesions at laparotomy
Pitter Human Reprod 2013
1
8 mmda Vinci port
8 mmda Vinci ports
12 mmassistant port
2
Uterine Mass
12 mm camera port(10 cm above top of mass)
1
8 mmda Vinci port
8 mmda Vinci ports
12 mmassistant port
2
Uterine Mass
12 mm camera port(10 cm above top of mass)
3
HYBRID ROBOT-ASSISTED MYOMECTOMY
• Described in 2007 to overcome limitations of robot in cases with large myomata
– Decrease in traction/countertraction due to “pop off” safety feature in robotic tenaculum
– Reduced field of movement due to robotic arms
HYBRID ROBOT-ASSISTED MYOMECTOMY
• Patient selection
– Multiple large myomata >8cm
– Uterine fundus at level of umbilicus
– Large exophytic fundal fibroid what would obstruct visualization
HYBRID ROBOT-ASSISTED MYOMECTOMY
KEYS TO SUCCESS
• Supra‐umbilical camera port incision
• Utilize 4 arm approach
• Swift docking of robot after enucleation of myoma
• Repair of incision prior to enucleation of remaining myomata
35

HYBRID ROBOT-ASSISTED MYOMECTOMY
1
8 mmda Vinci port
8 mmda Vinci ports
12 mmassistant port
3
Uterine Mass
12 mm camera port(10 cm above top of mass)
COSMETIC PORT PLACEMENT
• 427 women surveyed regarding surgical incision preference
• 250 (58.5%) respondents
– Traditional Laparoscopy 56.4% **
– Single Incision 41.1%
– Robotic Surgery 2.5%
Bush Journ Min Invas Gyn 2011**p<0.05 over single and robotic
INCISION PREFERENCE
Bush Journ Min Invas Gyn 2011
COSMETIC ROBOTIC MYOMECTOMY
Characteristic Mean + Standard Deviation
BMI (kg/m2) 26.4 + 5.7
Weight myomas (gm) 99.6 + 76.2
Number myomas 3.2 + 2.5
Estimated blood loss (mL) 110.1 + 222.6
Operative time (mins) 159.9 + 46.7
Unpublished internal data
COSMETIC ROBOTIC MYOMECTOMY
KEYS TO SUCCESS
• Uterus <12 week size
• Utilize short instruments through assistant port
• Not suitable for narrow pelvis
• Arm #3 should be used instead of Arm #2 to increase range of motion
36

COSMETIC ROBOTIC MYOMECTOMY
18 mmda Vinci port
8 mmda Vinci ports3
Uterine Mass
12 mm camera port(30 degree “UP”)
SINGLE INCISION LAPAROSCOPY IN GYNECOLOGY
Metanalysis of 6 RCT and 15 observational studies to evaluate surgical outcomes in gynecology
• 2085 patients: 899 SIL, 1186 conventional
• Mean operative time 6.97 minutes longer for adnexal surgery (p=0.045)
• Mean operative time equal for hysterectomy
• No difference in risk of complications
Murji Obstet & Gynecol 2013
SINGLE INCISION ROBOTIC MYOMECTOMY
SINGLE INCISION ROBOTIC MYOMECTOMY SINGLE INCISION ROBOTIC MYOMECTOMY
KEYS TO SUCCESS
• Uterus <12 week size
• Utilize OMNI GUIDE laser for increased flexibility with enucleation
• Arm #3 should be used instead of Arm #2 to increase range of motion
• Ideal for women with BMI>25 kg/m2
37

SINGLE INCISION ROBOTIC MYOMECTOMY CONCLUSIONS
1. Performing adequate preoperative assessment with MRI and correction of anemia optimizes patient outcomes
2. Utilizing vasopressin and barbed suture will decrease blood loss
3. Utilizing a bariatric camera trocar and #3 arm for cosmetic and single port approach minimizes arm collisions
4. Tailoring robotic port placement in myomectomy patients will improve ease of myoma enucleation while maximizing cosmetic outcome
1. Advincula AP, Xu X, Goudeau S, Ransom SB. Robot-assisted laparoscopic myomectomy versus abdominal myomectomy: A comparison of short-term surgical outcomes and immediate costs, Journal of Minimally Invasive Gynecology, 2007, 14, 698-705.
2. Advincula AP, Song A, Burke W, Reynolds RK. Preliminary experience with robot-assisted laparoscopic myomectomy, The Journal of the American Associatin of Gynecologic Laparoscopists, 2004, 11, 511-518.
3. Barakat EE, Bedaiwy MA, Zimberg S, Nutter B, Nosseir M, Falcone T. Robot-assisted, laparoscopic, and abdominal myomectomy: a comparison of surgical outcomes, Obstetrics & Gynecology, 2011, 117, 256-265.
4. Murji A, Patel VI, Leyland N, Choi M. Single-incision laparoscopic in gynecologic surgery, Obstetrics & Gynecology, 2013, 121, 819-828.
5. Bush AJ, Morris SN, Millham FH, Isaacson KB. Women’s preferences for minimally invasive incisions, The Journal of Minimally Invasive Gynecology, 2011, 18, 640-643.
6. HoboR, Netsu S, Koyasu Y, Tsutsumi O. Bradycardia and cariac arrest caused by intramyometrial injection of vasopressin during a laparoscopically assisted myomectomy, Obstetrics & Gynecology, 2009, 113, 484-486.
7. Alessandri F, Remorgida V, Venturini PL, Ferrero L. Unidirectional barbed suture vs. continuous suture with intracorporeal knots in laparoscopic myomectomy: a randomized study, Journal of Minimally Invasive Gynecology, 2008, 17, 725-729.
8. Einarsson KI, Chavan NR, Suzuki Y, Jonsdottir G, Vellinga TT. Use of bidirectional barbed suture in laparoscopic myomectomy: Evaluation of perioperative outcomes, safety, and efficacy, Journal of Minimally Invasive Gynecology, 2011, 18, 92-95.
9. Pitter MC, Gargiulo AR, Bonaventura LM, Lehman JS, Srouji SS. Pregnancy outcomes following robot-assisted myomectomy, Human Reproduction, 2013 28, 99-108.
10.Parker WH, Einarsson J, Istre O, Dubuisson JB. Risk factors for uterine rupture after laparoscopic myomectomy, Journal of Minimally Invasive Gynecology, 2010, 17, 551-554.
11. Dueholm M, Lundorf E, Hansen E, Ledertoug S, Olesen F. Evaluation of the uterine cavity with magnetic resonance imaging, transvaginal sonography, hystersonographic examination, and diagnostic hysteroscopy, Fertility and Sterility, 2001, 76, 350-357.
12.Kim YH, Chung, HH, Kang SB, Kim SC, Kim YT. Safety and usefulness of intravenous iron sucrose in the management of preoperative anemia in patients with menorrhagia: a phase IV, open label, prospective, randomzied study. Acta Haematol, 2009, 121, 37-41.
13.Stovall TG, Muneyyirci-Delale O, Summitt RL Jr, Scialli AR. GnRH agonist and iron versus placebo and iron in the anemic patient before surgery for leiomyomas: a randomized controlled trial, Obstetrics and Gynecology, 1995, 86, 65-71.
14.Ahmad G, Duffy JM, Farquhar C, Vail A, Vanderkerckhove P, Watson A. Barrier agents for adhesion prevention after gynecological surgery. The Cochrane Database of Systematic Reviews 2008, Art. No. CD000475.
38

Michael C Pitter, MD, FACOGChief, Minimally Invasive & Gyn Robotic Surgery
Newark Beth Israel Medical Center,Newark, NJ
Speakers Bureau: Intuitive Surgical
To review the controversies surrounding the use of the robot for hysterectomy for benign pathology.
To discuss the appropriate indications for robotic approach.
To illustrate the advantage of the 3rd instrument arm for addressing complex pathology.
To review pelvic anatomy – an absolute pre requisite for safe operation.
Laparoscopy circa 1990’s
Value of Randomized Control Trials
39

Wright JAMA Article Mar 2013
ACOG President Statement Mar 2013
Cost perceptions
Safety Perceptions Wall St Journal Kitsap Trial 1-800-BAD-ROBOT
Premier Data Base
Did not control for Learning Curve (2007-2010)
Did not control for BMI, Ut size, or prior surgery
Discarded Lap Conversions
Cost analyses done three ways, none normalized data
Robotic Surgery IS Laparoscopy.
It’s an enabling technology.
Has made a difference in converting from laparotomy to laparoscopy in Gyn Surgery.
Studies are ongoing as expected.
It’s not going away.
“When hysterectomy is necessary; the demonstrated safety, efficacy, and cost-effectiveness of vaginal hysterectomy and laparoscopic hysterectomy mandate that they be the procedure of choice.”
“Surgeons without the requisite training and skills required for the safe performance of VH or LH should enlist the aid of colleagues who do or should refer patients requiring hysterectomy to such individuals for their surgical care.”
JMIG October 2010
40

Surgical Field
Distorted Anatomy
Complex Pathology
Large Uterus
Obesity
Instrumentation
Learning Curves
Surgeon Experience/ Comfort Level
Training
Endometriosis.
Obliteration of anterior/posterior cul de sac.
Broad Ligament Myomas.
2 D Image4 – 6 fold magnificationRigid straight sticksCounter‐IntuitiveHaptics
Surgical FieldObesityInstrumentationLearning CurvesSurgeon ExperienceTraining
3 D Image10 fold magnificationWristed instrumentsIntuitive“Visual” Haptics
InstrumentationLearning CurvesSurgeon ExperienceTraining
CONVENTIONAL LAPAROSCOPY ROBOTIC ASSISTED LAPAROSCOPY
Open Surgery Through Laparoscopic AccessComparison of the Obstacles to MIS
• Lack of Haptics.• Surgeon is remote from the patient.• Different training paradigm.
• Visual Haptics.• Side Docking.• Review and learn pelvic anatomy !!• Think out of the box.• Use EEA Sizers.• Fill the Bladder.
Knowledge of Pelvic Anatomy !!!!
41

Knowledge of Pelvic Anatomy … Do you know where you are??? !!!!
Place the 4th arm on your dominant side*. Try to keep all instruments in view but avoid tunnel vision. You are your best assistant (but don’t get in your way). Think open surgery not rigid straight stick laparoscopy.When swapping, move the other instruments out of the way. Clutch and swap as often as necessary. 4th instrument arm is primarily used for retraction and exposure. 4th instrument is your suturing assistant.
Complex pathology. The 20 + week size uterus or large volume tumors. Prior Operations. Difficult to access pathology.
Multiple Myomectomy. Closure of the hysterotomy defect in layers. Large volume tumors.
Stage IV Endometriosis. The Obliterated Cul-de-sac.
Sacrocolpopexy Suture intensive operation.
42

43

Da Vinci platform is merely a tool…a means to an end.
Robotic surgery does not create a skilled surgeon or guarantee better outcomes.
May allow surgeons to address more complicated pathology in a minimally invasive fashion.
Use good clinical judgement when selecting cases.
Robotic Surgery is Laparoscopic Surgery.
Knowledge of Pelvic Anatomy is requisite.
Get Facile with the 3rd Arm !!!
44

Robotic Hysterectomy: Strategies for the Very
Large Uterus
Director of Robotic Surgery EducationWomen’s Health Institute
The Cleveland Clinic Foundation
Consultant: OmniGuide
Understand the advantages and disadvantages of robotic assistance and its use in complex hysterectomy.
Techniques for overcoming the challenges of the large uterus will be discussed. Umbilicus
Kidneys
Fibroid Uterus
3D HD visualization with 8 or 12 mm camera
Stability of camera and instruments
7-degrees of freedom in range of motion
Enhanced dexterity Tremor reduction Improved ergonomics
Large uteri pose difficulty laparoscopicallysecondary to difficult access to uterine vasculature and colpotomy with straight sticks.
May result in increased:
◦ Blood loss
◦ Complications
◦ Conversions
45

Robot has extended laparoscopic hysterectomy to larger uteri because of:
◦ Enhanced Vision 3D and HD
◦ Increased range of motion Dissection around large
Structures
◦ Improved Control: Stability of Camera Retraction Ability of Fourth
Arm
Provides dexterity for complex dissections (e.g endometriosis, adhesions, broad lig fibroids)
Improved visualization and access around the cervix for colpotomy
Easier vaginal cuff closure Complication rates are
comparable to conventional TLH Studies have reported
decreased EBL, conversion to laparotomy, and length of stay.
Overcoming Challenges: ◦ Exposure: 3D vision, 3rd Arm, Uterine
Manipulation, Assistant ports.◦ Finding the Anatomy: Dissecting the
ureters and uterine arteries.
Minimizing Blood Loss: ◦ Dissection is facilitated◦ Allows staying in the Correct Plane◦ Control of bleeding as you go along
MIS option for patients with indications that may have necessitated laparotomy:
◦ Multiple prior surgeries ◦ High body mass index ◦ Large fibroids ◦ Known severe adhesive disease ◦ Extensive endometriosis
Most patient’s with a large uterus is a potential robotic hysterectomy candidate.
Rule out possible malignancy first or consider bagging uterus for morcellation.
Consider exam under anesthesia and/or diagnostic laparoscopy before deciding to proceed.
Key is mobility and access into retro-peritoneal space.
Start slow and increase gradually
46

Many potential benefits over traditional surgical approaches, including: ◦ Significantly less pain than laparotomy◦ Minimal blood loss and need for transfusion ◦ Fewer complications◦ Shorter hospital stay (1-2 days)◦ Quicker recovery and return to nl activities (2-4 wks)◦ Small incisions for minimal scarring ◦ Better outcomes and patient satisfaction, in many
cases
Pre-robotic (n=100) da Vinci (n=100) Last 25
da Vinci
Age (years) 43.5 43.2
BMI 28.8 28.8
Estimated blood loss (ml) 113 61
Hospital stay (days) 1.6 1.1
TAH rate 20% 4% 0%
Conversions (subset of TAH) 9% 4% 0%
Avg uterine weight of conversions 359.5 1387.5
TAH due to adhesions 8% 0%
Operative times (skin-to-skin) 92.4 119 78.7
Retrospective Review of Hysterectomy: Pre-Robotic versus da Vinci
History◦ Parity – a consideration for vaginal access◦ Prior surgery – to anticipate adhesions◦ Symptomatology – for treatment counseling◦ Past Medical History – to assess anesthesia
concerns and peri-operative medical care
Examination:◦ Size - >16 wks size consider robotic approach◦ Fibroid Type - Broad Ligament or cervical Fibroids
Consider a robotic approach◦ Fibroid Location – Posterior and anterior may hinder
visualization. ◦ Mobility – lateral mobility most critical◦ Cervix characteristics - assess size, shape, position for
uterine manipulator placement.◦ Access to Vasculature – in lateral fornices above cervix◦ Scar Locations – to anticipate adhesions or fixed uterus.
Pathology◦ Endometrial Pathology recommended if
morcellation is likely in patient’s >35 or in patients at risk for hyperplasia: PCOS Obesity Prior history
◦ PAP smear history and recent pap to determine candidacy for supra-cervical hysterectomy if desired.
Imaging◦ Ultrasound For uteri <16 weeks is ok.
◦ CT scan May substitute for MRI if very large bulky uterus. Beware of hydronephrosis. May request Tri-axial CT scan images.
◦ MRI Gives best imaging indicating size and location of fibroids May be needed for pre-operative planning for extremely
complex cases.
47

Benefit of Robotic Surgery◦ Less pain and Faster Recovery.
Risks of Laparoscopy◦ Especially visceral injury.
Risk of Conversion to Laparotomy◦ Every patient must be counseled in this regard.
Pre and Post-operative care◦ Set expectations for discharge.
Same benefit of other minimally invasive techniques:◦ Significantly less pain than laparotomy◦ Minimal blood loss and need for transfusion ◦ Fewer complications◦ Shorter hospital stay (1-2 days)◦ Quicker recovery and return to nl activities (2-4 wks)◦ Small incisions for minimal scarring ◦ Better outcomes and patient satisfaction
Balance with time required for surgery.
A learning curve exists: 20-90 cases Need skilled assistant and a team approach Time for extraction of the uterus is added to
the time for the procedure. May increase cost significantly
Positioning and Padding to prevent injury
Work with anesthesia to restrict fluid
Examination under anesthesia is mandatory
Team approach allows for efficiency◦ Ask for special equipment ahead of time◦ Ensure everyone is aware of difficulties and the plan
of action at the beginning of the case.
DORSAL LITHOTOMY POSITION◦ Allen’s Stirrups with padded cushions.◦ Both Arms Tucked.◦ Take care with positioning to prevent nerve injury.
PREVENTION OF SLIDING IN MAXIMUM TRENDELENBURG◦ Tuck and Tape◦ Shoulder pads/brace◦ Egg crate sponge◦ Bean Bag
Shown to be most important during the Learning Curve.
Very important in more difficult cases.
May be determining factor for success of the case.
Uterine Positioning System assists with uterine manipulation, and can eliminate need for vaginal assist.
48

V-care
Rumi◦ Arch ◦ Pivoting◦ Strongly consider UPS The best assistant is you!
Others
Dependent on size of the Uterus
Considerations:◦ Size and shape of the uterus◦ May want to remain just above fundus
if adnexa is accessible.◦ Assess with 5 mm LUQ camera first
(this can remain as accessory)◦ 30 degree camera can lower your
camera port further
SMALL MEDIUM
LARGE JUMBO
THE TARGET ORGAN IS THE OVARY!!! NOT THE FUNDUS!!! Docking◦ Center docking – help if ports are very high◦ Side-docking - allows vaginal access
Assistant Port Placement◦ Left vs Right◦ Lateral vs Medial
Instruments◦ Coagulation PK cautery Fenestrated Bipolar Ligasure
◦ Cutting Monopolar scissors Monopolar hook
◦ Manipulation Prograsp Long tip forceps Tenaculum
Use your Landmarks:◦ Round Ligaments◦ Adnexa◦ Colpotomy ring◦ Anatomy is the “roadmap”
Approach is dependent on what you can see:◦ Anterior Approach◦ Posterior Approach◦ Side-wall Approach
49

Take what you can get! ◦ Start on easier side◦ If you are not making progress change to other side◦ Go as far as you can get down one side before
switching
Stay hemostatic!◦ Blood will distort tissue planes and anatomy.◦ Be gentle◦ Use pneumoperitoneum to help you
Fibroids may distort adnexa Find origin and course of IP ligament May need to take down in layers Be aware of uterine accessory vasculature
Ureter is easiest to find at pelvic brim medial and inferior to IP.
Use pneumoperitoneum and gentle dissection to enter broad ligaments hemostatically.
Entry into the Retroperitoneal Triagle◦ Gives you access to the vasculature.
Find the Landmarks!! ◦ Push up maximally on colpotomy ring
Beware of collateral vessels.◦ Stay far lateral to the uterus
Back-filling the bladder is helpful, especially with previous C-section
Take down to 1 cm below the colpotomy ring to allow for cuff closure.
Exposure is Key Efficient application of energy Consider starting at angles Troubleshooting if no manipulator present
50

EEA sizer may be placed to elevate cervix and delineate fornices for colpotomy when cervix is inaccessible.
Anchor the angles to the utero-sacral ligament for support
Take the bladder down further than 1 cm. Take wider bites including vaginal “fascia” Evert edges to visualize mucosa Always check vaginally after procedure Cystoscopy after vaginal cuff closure is
important. May use interrupted or V-lock suture
In situ Morcellation or Mechanical Morcellation
Bivalve or Quarter then string or bob
Vaginal Morcellation
Consider bagging the uterus if concern about pathology exists.
Consider Mini-laparotomy for extremely large uteri.
Same principles apply:◦ Exposure is Key! Pull, push, lift, or compress! Use angled camera if needed◦ Gain mobility by entering and opening
retroperitoneal space making peritoneal outline◦ Find the anatomy and release at adnexa and
round ligament◦ Start on easier side and Take what you can get May need to improvise. Keep moving!
51

Treat like the small uterus Early ambulation and early feeding
encourages fast recovery Start prophylactic GI regimen immediately Toradol reduces narcotic useage May discontinue foley catheter within 6 hours
after procedure
Several studies show good outcomes Key is decreased laparotomy in more complex
cases Greater ability to accomplish minimally invasive
procedure in complex cases Lower blood loss and length of stay has been
noted Equivalent complication rates to laparoscopic
or vaginal hysterectomy
Reference: JRS
The Effect of Uterine Weight on Robotic Assisted Total Laparoscopic
Hysterectomy Outcomes Study Design◦ Retrospective cohort analysis via chart review
Study Population (n=135):◦ All patients who underwent Robotic-assisted
hysterectomy at Henry Ford Health System (HFHS) Hospitals since the inception of this procedure at HFHS were included (January 2008-May2010)
◦ Surgeries were performed by 6 surgeons who were trained and began performing the procedure during this period.
Uterine weight was recorded from the pathology report
Outcomes were collected from the electronic medical record as follows:◦ Procedure duration (“cut” to “close” times)◦ Estimated blood loss (EBL)◦ Hemoglobin change (Pre minus Post-operative
Hgb)◦ Length of stay (LOS)◦ Complications (immediate and delayed major and
minor complications from detailed chart review)
Demographics and other covariates were also obtained from the medical record included Body Mass Index (kg/m2) and race. The effect of BMI on RH outcomes wee assessed in a separate analysis.
Patients with confounders were excluded including those: Who underwent supra-cervical hysterectomy With concomitant uro-gynecologic procedures Who underwent hysterectomy for malignancy
Statistical analyses included Spearman correlations and Wilcoxon rank sum tests.
52

N=110 Total Mean SD Min Median Max
Age (years) 135 45.7 7.4 30 45 68
Race Black White Other
(N, % of total) 83 (61.5%)
50 (37.0%)
2
(1.5%)
N=110 Total Mean SD Min Median Max
Uterine Weight
133 262.4 242.7 47 170 1290
Category < 250 grams 250-500 grams > 500 grams
(N, % of total) 87
(65.4%)
28
(21.1%)
18
(13.5%)
BMI (kg/m2) 135 31.1 7.6 14.8 30.3 56.2
BMI Category Underweight<18.5
Normal18.5-25
Overweight25-29.9
Obese30-34.9
Morbid35+
(N, % of total) 3 (2%)
28 (21%)
34(25%)
34 (25%)
36
(26%)
Procedure Duration
Estimated Blood Loss
Length of Stay
Hemoglobin Change
Spearman Correlation
0.53 0.30 0.14 -0.09
P-value <0.001 0.0005 0.10 0.30
There is statistically significant correlation between uterine weight and Procedure Duration.
There is statistically significant correlation between uterine weight and Estimated Blood Loss, BUT NOT hemoglobin change.
Procedure Duration
(min)
Estimated Blood Loss
(mL)
Length of Stay
(days)
Hemoglobin Change
(g/dL)
Uterine Weight(N)
Median (Range)
Median (Range)
Median (Range)
Median (Range)
<250 grams(N=87)
150
(80-534)
50
(10-450)
1
(1-14)
-1.3
(-3.7 - 0.4)
250-500 grams(N=26-28)
205.5
(96-388)
87.5
(10-1000)
1
(1-3)
-1.65
(-4.4 - 0.9)
≥500 grams(N=18)
294.5
(152-625)
100
(25-500)
1.5
(1-11)
-2.1
(-4.0 - 0.5)
Major Complication
Minor Complication
Any Complication
Number
(Rate %)
12
(8.9%)
15
(11.1%)
27
(20%)
Wilcoxon Rank Sum Test p-value
0.96 0.76 0.79
Major Complication was defined as an visceral injury, or complication that caused increased hospital stay, re-admission, or re-operation.
Minor Complication was defined as any complaint that required evaluation and treatment.
There were 10 re-admissions (7.4%) and 3 blood transfusionsthat were unrelated to uterine weight.
There is a strong correlation between uterine weight and procedure duration.
The increase in median was at a maximum of 145 minutes between the smallest and largest uterine weight categories.
This increase in procedure duration did nottranslate into an increase in length of stay or complications.
53

There is a correlation with estimated blood losswith a 50 mL increase in medians between the smallest and largest uterine weight groups.
Only reflected as a trend in decrease in peri-operative hemoglobin.
Possible small increased blood loss is not clinically significant and did not result in an increase in blood transfusions for patients with larger uteri.
Robotic-assisted total laparoscopic hysterectomy can be performed safely on patients with large Uteri.
Although procedure duration is increased slightly, there are no substantial impact on blood loss, post-operative length of stay, or complications.
MOST patients can be approached with a minimally invasive approach.
Studies have shown benefit to the patient without increasing risk.
Benefit for the Patient-◦ No need for Laparotomy!◦ Less Pain, Less Bleeding, Faster recovery.
The Future-◦ What is the limit of daVinci surgery? Only limited by what we will try........
Umbilicus
Kidneys
Fibroid Uterus
a) Abdominal Hysterectomyb) Vaginal Hysterectomyc) Total Laparoscopic Hysterectomyd) Laparoscopic Assisted Vaginal Hysterectomye) Robotic Hysterectomy
54

Antonio GargiuloMedical Director, Center for Robotic Surgery
Brigham and Women’s Health CareHarvard Medical School
Gargiulo 2013Gargiulo 2013
Consultant: OmniGuide
Participants should be able to :
• Interpret available scientific publications on benefits
and limitations of robotics in endometriosis surgery
• Describe the role of robotics in the three different
manifestations of pelvic endometriosis
• Identify relevant areas of clinical investigation in the
use of robotics in endometriosis surgery
Gargiulo 2013Gargiulo 2013
Endometriosis Fertility Index: is it better than the present staging systems? GD Adamson. Curr Opin Obstet Gynecol, 2013
• The revised ASRM classification system does not
predict pregnancy rates (either spontaneous or ART)
• The only classification system that predicts a clinical
outcome (spontaneous pregnancy rates) is the EFI
• The upcoming AAGL classification system will be
based on both pain and fertility
Gargiulo 2013Gargiulo 2013
• Peritoneal Endometriosis
• Ovarian Endometriosis
• Deep Infiltrating Endometriosis
Laparoscopic management of peritoneal endometriosis, endometriotic cysts, and rectovaginal adenomyosis.
J Donnez et al. Ann NY Acad Sci, 2003
Gargiulo 2013Gargiulo 2013
Laparoscopic surgery for pelvic pain associated with endometriosisTZ Jacobson et al. Cochrane Database Sys Rev, 2009
• Five RCT included in metanalysis
• Most patients with mild-minimal endometriosis
• Metanalysis demonstrated an advantage of
laparoscopic surgery compared to diagnostic
laparoscopy only (OR of 5.72, 95% CI 3.09 to 10.6)
Gargiulo 2013Gargiulo 2013
55

Surgical treatment of endometriosis: location patterns of disease at reoperation.E Taylor and C Williams. Fertil Steril, 2010
• ASRM 1-2 endo recurred in 37% of pelvic regions
after surgical treatment
• More likely to recur in a treated pelvic region that an
adjacent or distant pelvic region (RR 2.54)
Gargiulo 2013Gargiulo 2013
Laparoscopic surgery for subfertility associated with endometriosisTZ Jacobson et al. Cochrane Database Sys Rev, 2010
• Two RCT (Marcoux and Gruppo Italiano) included
• All patients with mild-minimal endometriosis
• Metanalysis demonstrated no advantage of
laparoscopic surgery compared to diagnostic
laparoscopy only (OR of 1.33, 95% CI 0.60 to 2.94)
when considering delivery rates.
Gargiulo 2013Gargiulo 2013
• Sharp excision, bipolar diathermy and carbon dioxide
laser ablation are the three main treatment options
• Excision and ablation are preferred by many, based
on risk of neighboring tissue damage with diathermy
• However, animal data and human studies do not
show a significant advantage of either technique.
Wallwiener at al. Fertil Steril, 2009
MP Radosa et al. Eur J Obster Gynecol, 2010
J Wright et al. Fertil Steril, 2005
Gargiulo 2013Gargiulo 2013
• The role of computer-assisted surgery in peritoneal
endometriosis is unclear
• Advantage of magnified stereoscopic vision in
identification and treatment of peritoneal lesions HAS
has not been studied
• Advantage of fluorescence imaging with intravenous
indocianine green in identification and treatment of
peritoneal lesions has not been studied
Gargiulo 2013Gargiulo 2013
Case control study: longer operating times and similar
safety compared to conventional laparoscopy.
Gargiulo 2013Gargiulo 2013
Robotic versus standard laparoscopy for the treatment of endometriosis C Nezhat et al. Fertil Steril, 2010
Gargiulo 2013Gargiulo 2013
56

• Constitute oncologic risk
• Cause pelvic pain
• Decrease ovarian reserve
• Contribute to infertility
• Interfere with ART
Gargiulo 2013Gargiulo 2013
• Observation with regular imaging
• Medical treatment
• Drainage-Biopsy-Coagulation (DBC)
• Stripping
Gargiulo 2013Gargiulo 2013
Asymptomatic (no pain, no infertility)
• Without prior histologic diagnosis: surgery if over 4 cm, observation otherwise (ESHRE guidelines)
• With prior histologic diagnosis: observation
• Medical treatment to prevent recurrence or to slow growth
Gargiulo 2013Gargiulo 2013
Pelvic Pain• Surgical treatment must be first line
• Medical treatment only after surgery
• Stripping and DBC both effective
• Stripping has advantages over DBC: Reduced recurrence rate of pain
Gargiulo 2013Gargiulo 2013
RJ Hart et al
Cochrane Database of Systematic Reviews, 2008
Infertility: no other causes• Surgical treatment must be first line
• Cumulative pregnancy rate is substantial
• Stripping and DBC both effective
• Stripping has advantages over DBC:Higher rate of spontaneous pregnancy
Gargiulo 2013Gargiulo 2013
Hart et al
Cochrane Database of Systematic Reviews, 2008
Infertility: no other causes• Review of 14 studies (no RCTs)
• 1500 patients
• Overall weighted mean pregnancy rate was 50% with 24 month follow-up
• Even assuming half, NNT is 4
P Vercellini et al, Hum Reprod 2009
Gargiulo 2013Gargiulo 2013
57

Mutifactorial Infertility• Surgery does not increase fecundity
• Swift access to ART should be considered
• No effect of Stripping or DBC on ART clinical pregnancy rate, and Stripping can decrease oocyte output.
Benschop et al
Cochrane Database of Systematic Reviews, 2010
Gargiulo 2013Gargiulo 2013
• We are removing ovarian cortex.
• However, normal follicles only in cyst wall pedicle at ovarian hilum
L Muzii et al. Fertil Steril, 2007
• Bipolar cauterization of the pseudo-cyst bed can damage the ovarian hilum
• Bilateral endometrioma: double trouble!
• Consider DBC over stripping in select cases
Gargiulo 2013Gargiulo 2013
Control ovary Operated ovary
Nargund et al. 1996 8.9+5.1 6.3+5.2*
Loh et al. 1999 3.6 4.6
Donnez et al. 2001 6.6+3.5 5.2+3.0
Ho et al. 2002 6.1+4.1 2.9+2.6*
Somigliana et al. 2003 4.2+2.5 2.0+1.5*
Wong et al. 2004 5.2+0.8 5.6+0.9
* = significantly different
Oocytes retrieved by different surgical teams
Gargiulo 2013Gargiulo 2013
• Skilled laparoscopists
• Hemostatic matrix
• Regenerated celluloseand
• Ovarian vasopressin injection
• Ovarian suturing
• Partial stripping with laser ablation
• Role of robotic surgery
Gargiulo 2013Gargiulo 2013 Gargiulo 2013Gargiulo 2013
58

• Definition: subperitoneal invasion by endometriotic lesions that exceeds 5 mm in depth
• Vaginal and rectal ultrasound and MRI imaging have high sensitivity and specificity in highly trained centers
M Bazot et al. Fertil Steril, 92(6): 1825-33, 2009
• Surgery is essential
Gargiulo 2013Gargiulo 2013 Gargiulo 2013Gargiulo 2013
M Bazot et al. Fertil Steril, 2009
M Bazot et al. Fertil Steril, 2009
Normal anatomy of the anterior compartment.
©2011 by Radiological Society of North America
Coutinho A et al. Radiographics 2011
©2011 by Radiological Society of North America
Normal anatomy of the posterior compartment.
Coutinho A et al. Radiographics 2011©2011 by Radiological Society of North America
Normal anatomy of the posterior compartment.
Coutinho A et al. Radiographics 2011
59

©2011 by Radiological Society of North America
Endometriosis of the vesico-uterione pouch
Coutinho A et al. Radiographics 2011©2011 by Radiological Society of North America
Bladder endometriosis with ureteral involvement
Coutinho A et al. Radiographics 2011
©2011 by Radiological Society of North America
Endometriotic involvement of the retrocervical area
Coutinho A et al. Radiographics 2011
Endometriotic involvement of the uterosacral ligaments
©2011 by Radiological Society of North America
Coutinho A et al. Radiographics 2011
©2011 by Radiological Society of North America
Coutinho A et al. Radiographics 2011
Sigmoid endometriosis
• Expanding the horizons: robot-assisted reconstructive surgery of the distal ureter.
SK Williams et al. J Endourol, 2009
• Robotic-assisted laparoscopic partial bladder resection for the treatment of deep infiltrative endometriosis.
C Liu et al. J Min Gynecol Surg, 2009
Gargiulo 2013Gargiulo 2013
60

• Robotic treatment of colorectal endometriosis: technique, feasibility and short-term results. A Ercoli et al. Hum Reprod, 2012
• Deep infiltrating colorectal endometriosis treatedwith robotic-assisted rectosigmoidectomy. RM Neme et al. JSLS, 2012
Gargiulo 2013Gargiulo 2013 Gargiulo 2013Gargiulo 2013
Endometriosis Fertility Index: is it better than the present staging systems? GD Adamson. Curr Opin Obstet Gynecol. 25(3):186-92, 2013
Laparoscopic management of peritoneal endometriosis, endometriotic cysts, and rectovaginal adenomyosis.J Donnez et al. Ann NY Acad Sci 997: 274-81, 2003
Laparoscopic surgery for pelvic pain associated with endometriosis. TZ Jacobson et al. Cochrane Database Sys Rev, 4, 2009
Surgical treatment of endometriosis: location patterns of disease at reoperation. E Taylor and C Williams. Fertil Steril, 93(1): 57-612010
Gargiulo 2013Gargiulo 2013
The extent of adhesion induction through electrocoagulation and suturing in an experimental rat study. Wallwiener at al. Fertil Steril, 93(4):1040-4, 2009
Coagulation versus excision of primary superficial endometriosis: a 2 year follow-up. MP Radosa et al. Eur J Obster Gynecol, 150:195-8, 2010
A randomized trial of excision versus ablation for mild endometriosis. J Wright et al. Fertil Steril, 83:1830-6, 2005
Robotic versus standard laparoscopy for the treatment of endometriosis. C Nezhat et al. Fertil Steril 2010 94(7): 2758-60
Gargiulo 2013Gargiulo 2013 Gargiulo 2013Gargiulo 2013
The European Society for Human Reproduction and Embryology. Guidelines for the treatment of Endometriosis.(Guidelines.endometriosis.org). Updated 2007
Excisional surgery versus ablative surgery for ovarian endometriomata. RJ Hart et a. Cochrane Database Syst Rev, 2009
Surgery for endometriosis-associated infertility: a pragmatic approach. P Vercellini et al. Hum Reprod 24(2):254-69, 2009
Interventions for women with endometrioma prior to assisted reproductive technology. L Benshop et a. Cochrane Database Syst Rev, 2010
61

Gargiulo 2013Gargiulo 2013
Histologic analysis of endometriomas: what the surgeon needs to know. L Muzii et al. Fertil Steril, 87(2):362-6, 2007
Diagnostic accuracy of physical examination, transvaginalsonography, rectal endoscopic sonography, and magnetic resonance imaging to diagnose deep infiltrating endometriosis. M Bazot et al. Fertil Steril, 92(6): 1825-33, 2009
MR Imaging in Deep Pelvic Endometriosis: A Pictorial Essay. Coutinho A et al. Radiographics 2011;31:549-567
Gargiulo 2013Gargiulo 2013
Expanding the horizons: robot-assisted reconstructive surgery of the distal ureter. SK Williams et al. J Endourol23(3): 257-61, 2009
Robotic-assisted laparoscopic partial bladder resection for the treatment of deep infiltrative endometriosis.C Liu et al. J Min Gynecol Surg, 16(2):244, 2009
Robotic treatment of colorectal endometriosis: technique, feasibility and short-term results. A Ercoli et a,. Hum Reprod27(3):722-6, 2012
Deep infiltrating colorectal endometriosis treated withrobotic-assisted rectosigmoidectomy. RM Neme et al. JSLS 17(2): 227-34, 2012
62

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsian
Indo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
63