Embed Size (px)
Citation preview
Siddharth Pandya DO Neuroradiologist
Clinical Associate Professor NOVA Southeastern College of Osteopathic Medicine
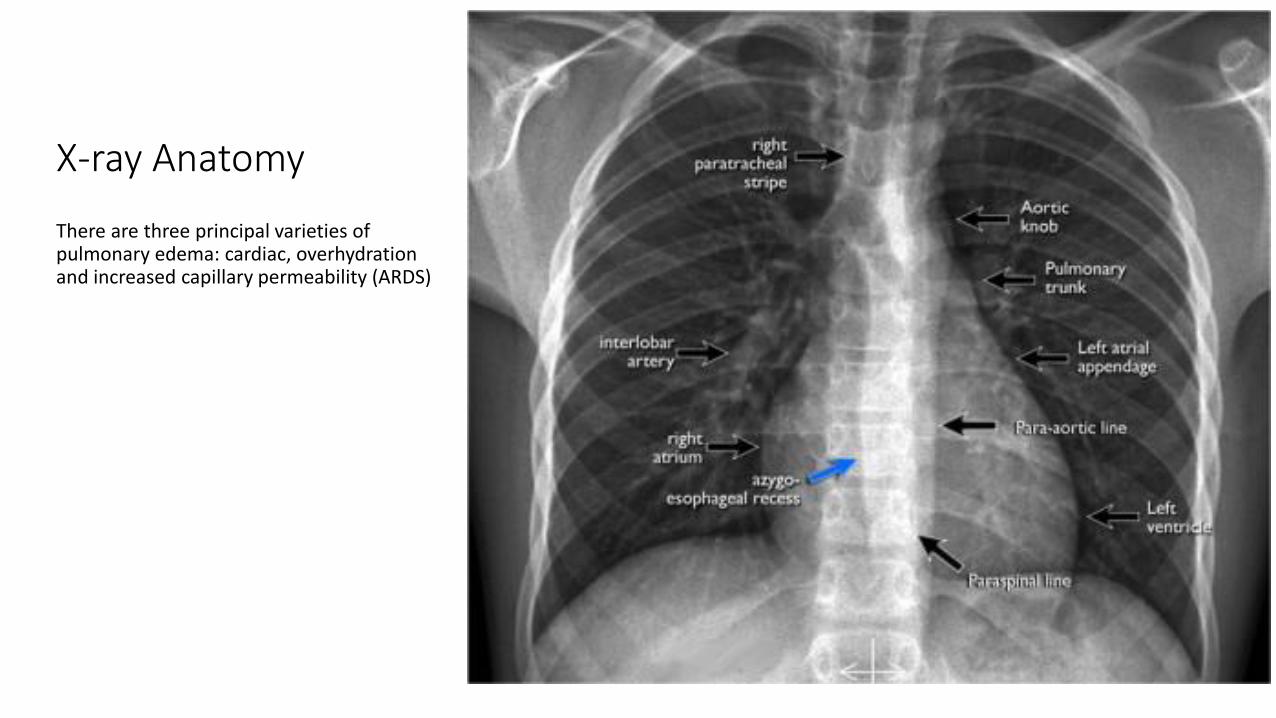
X-ray Anatomy
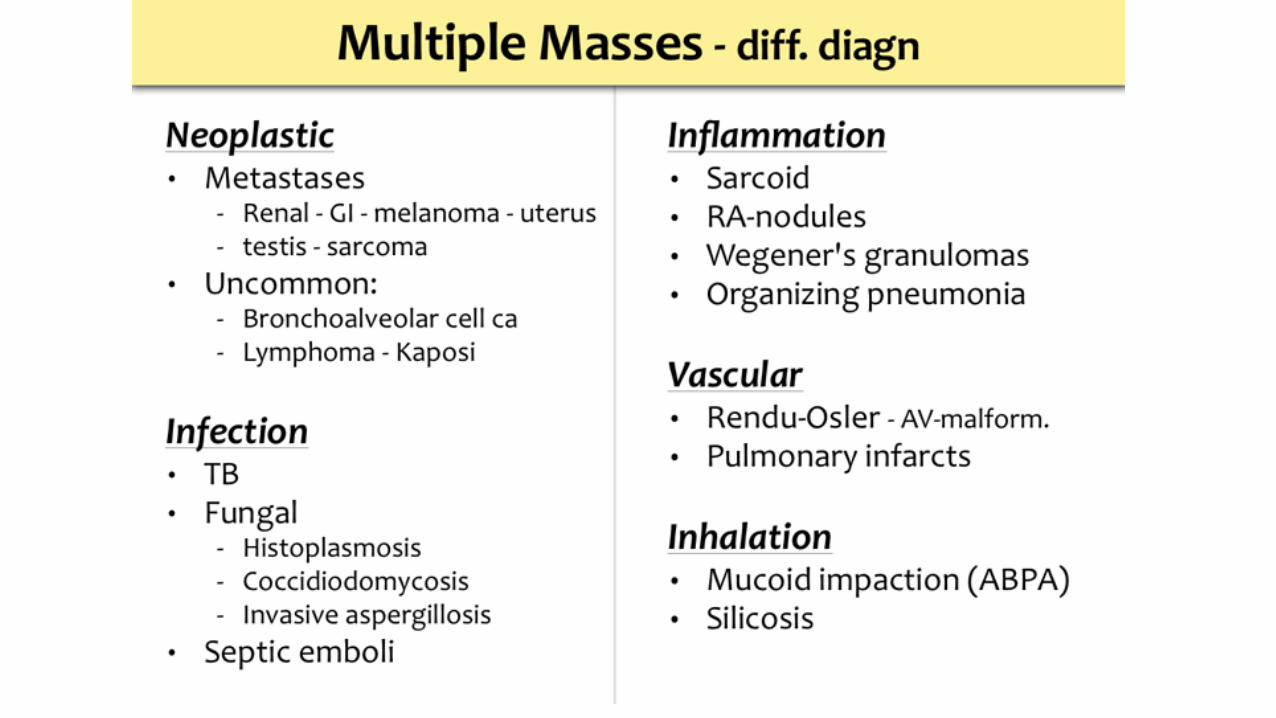
There are three principal varieties of pulmonary edema: cardiac, overhydration and increased capillary permeability (ARDS)
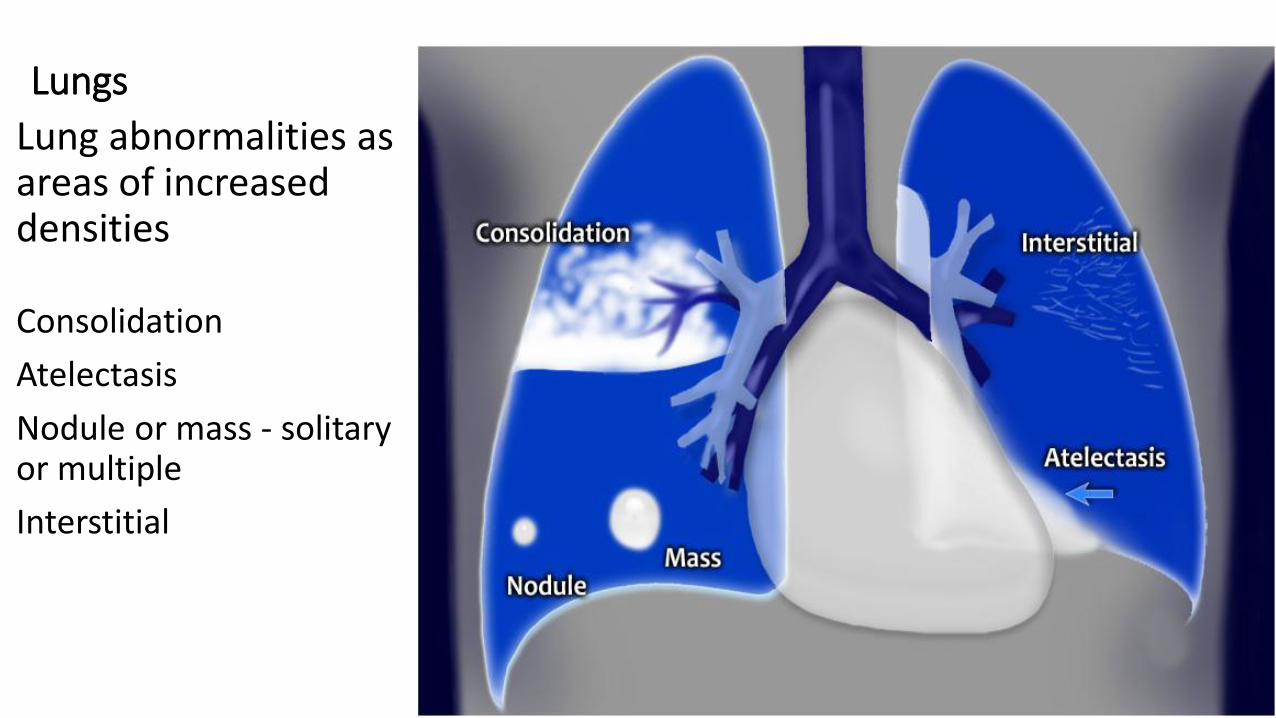
Lungs
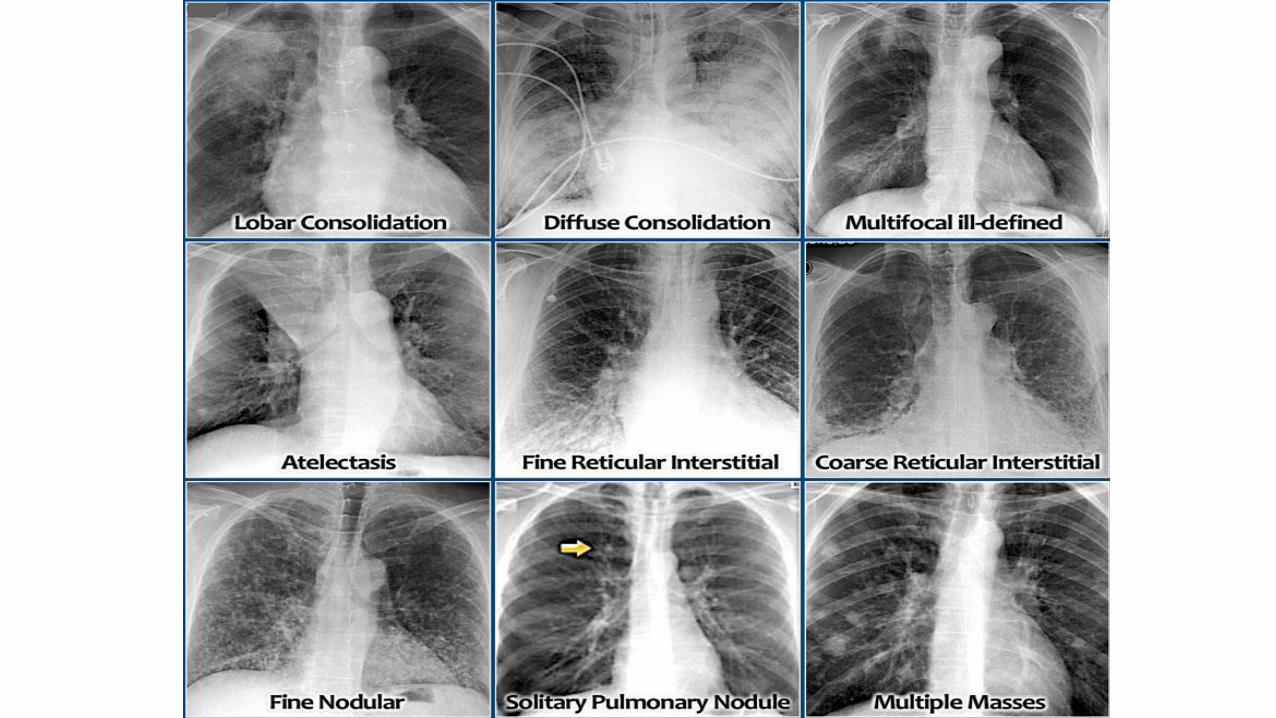
Lung abnormalities as areas of increased densities
Consolidation
Atelectasis
Nodule or mass - solitary or multiple
Interstitial
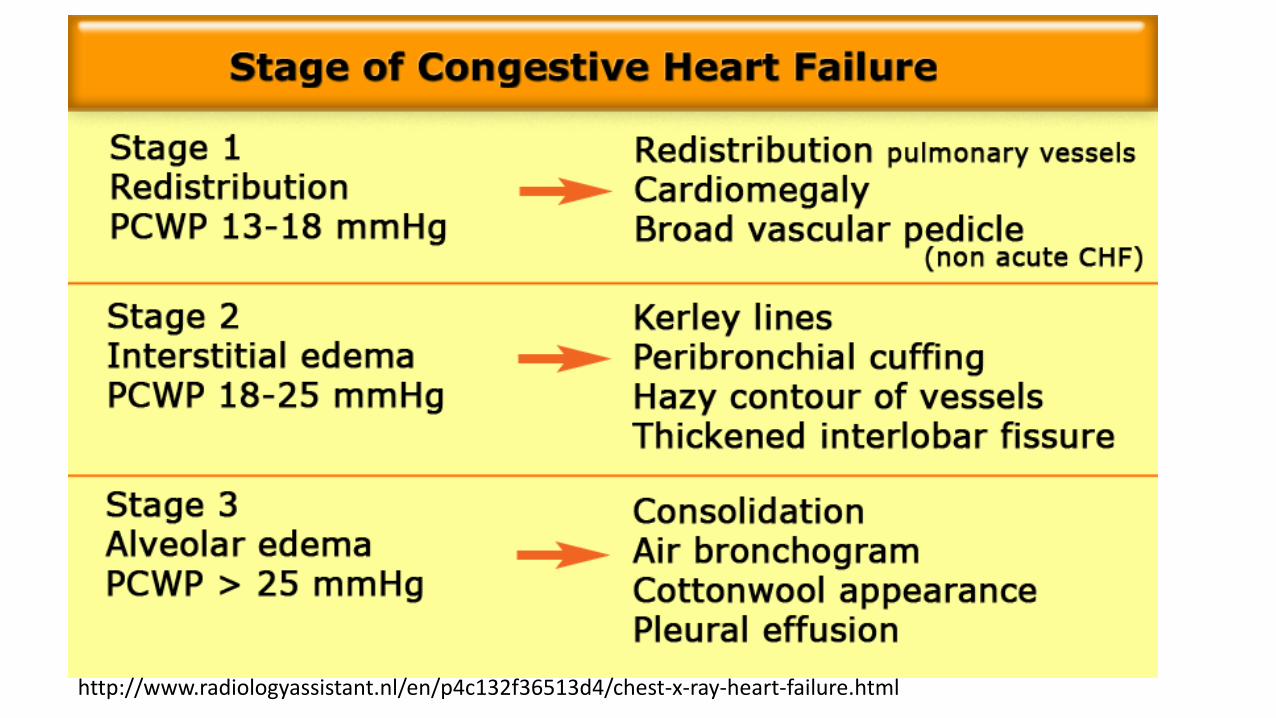
http://www.radiologyassistant.nl/en/p4c132f36513d4/chest-x-ray-heart-failure.html
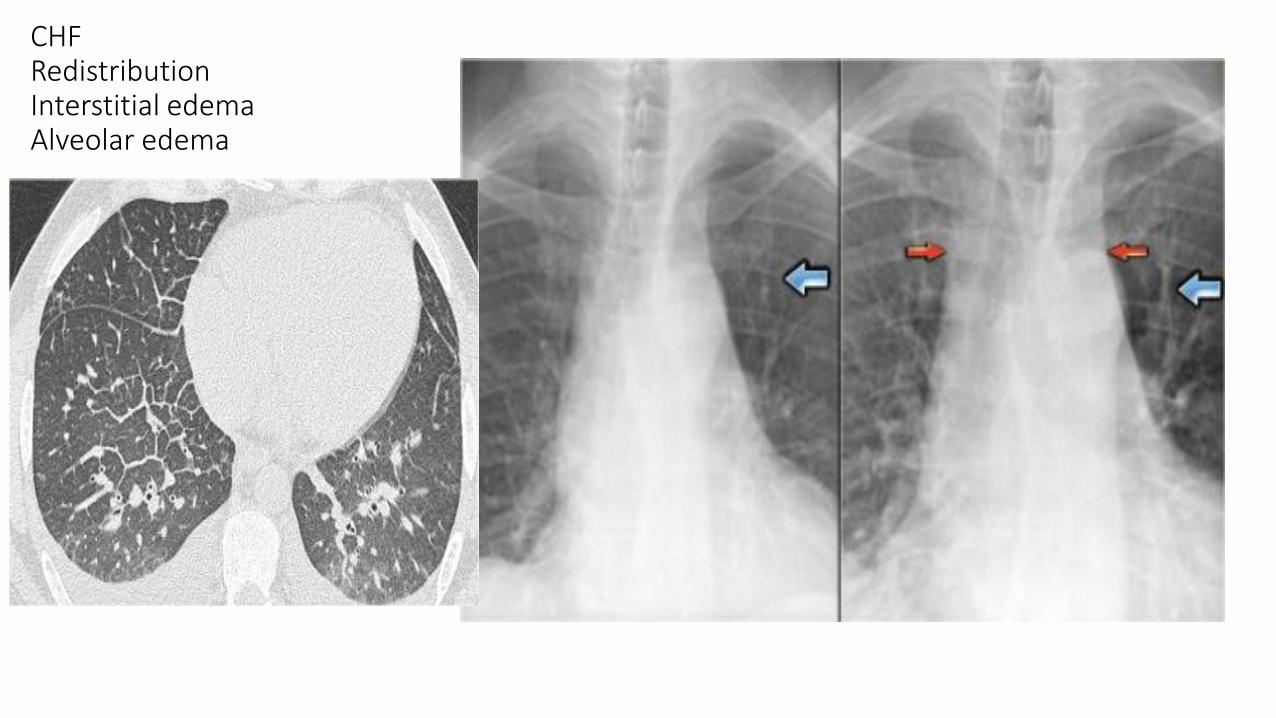
CHF Redistribution Interstitial edema Alveolar edema
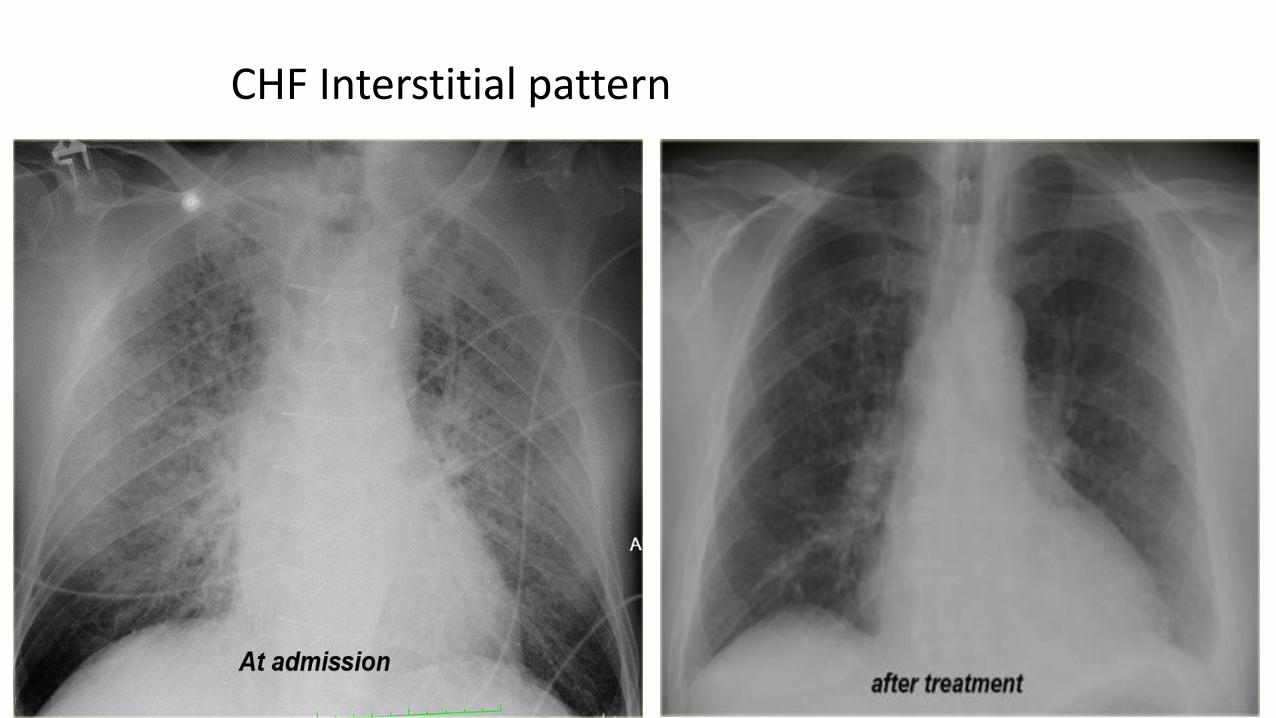
CHF Interstitial pattern
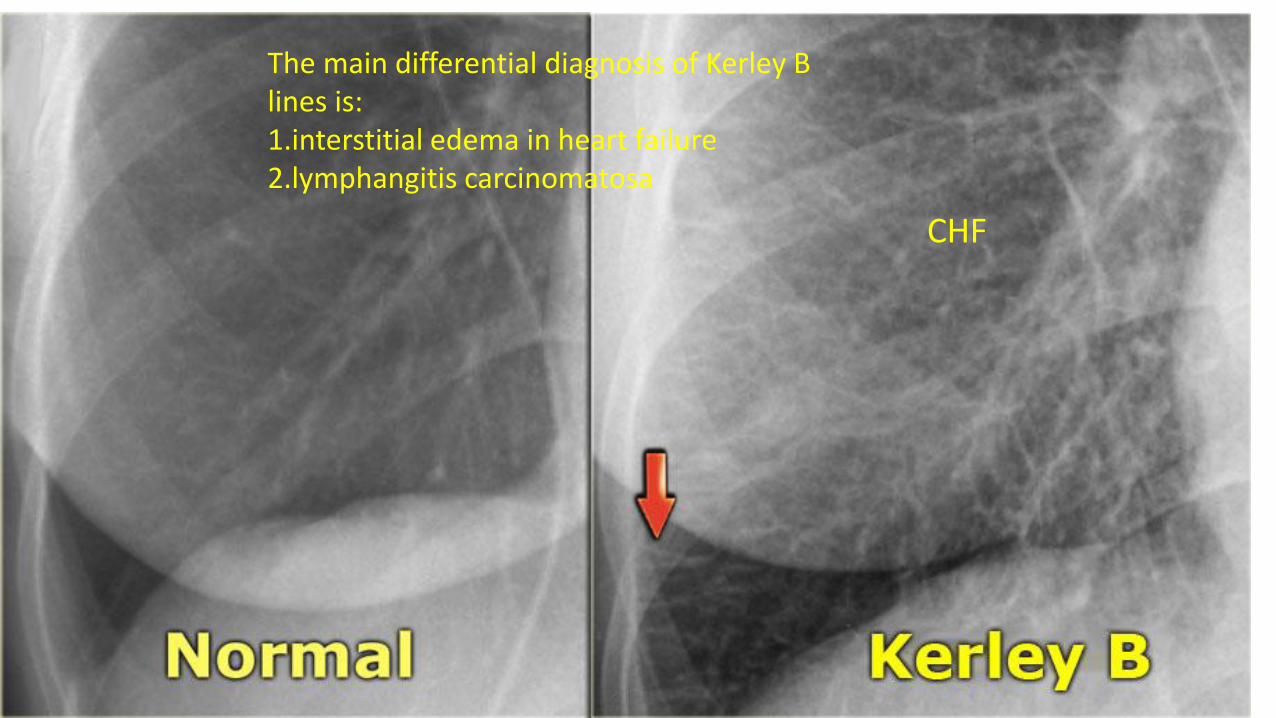
The main differential diagnosis of Kerley B lines is: 1.interstitial edema in heart failure 2.lymphangitis carcinomatosa
CHF
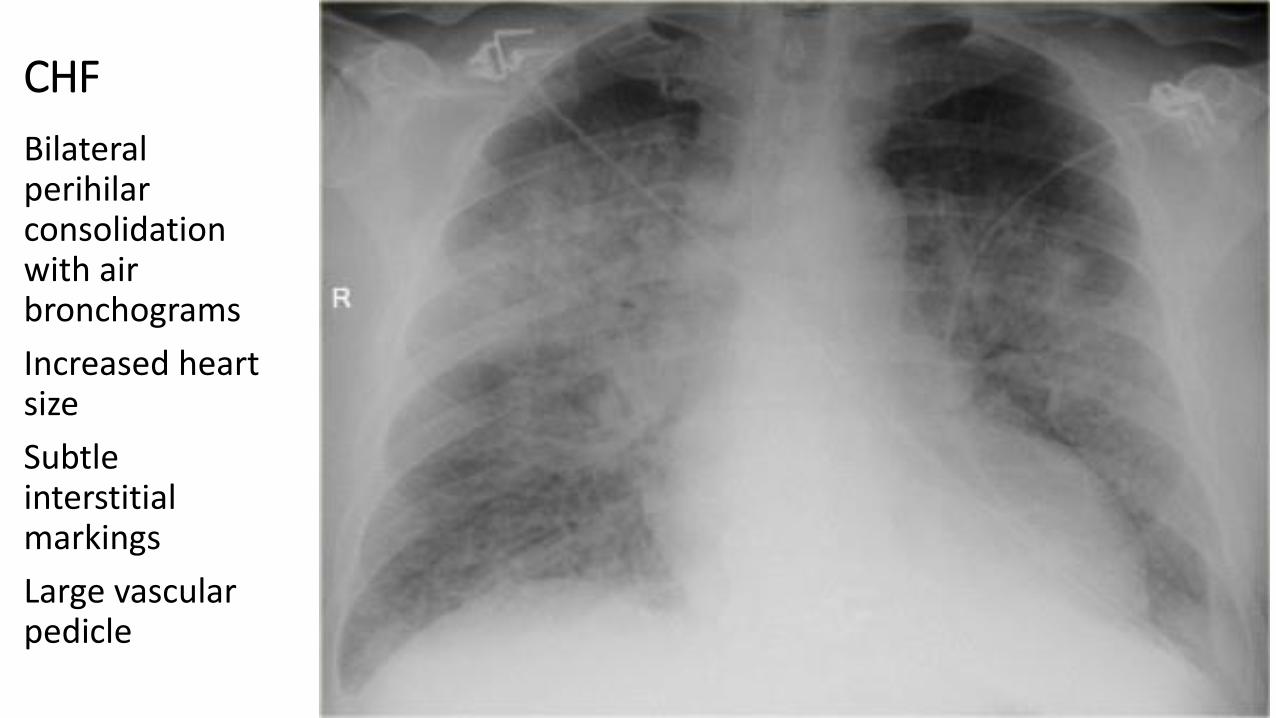
CHF
Bilateral perihilar consolidation with air bronchograms
Increased heart size
Subtle interstitial markings
Large vascular pedicle
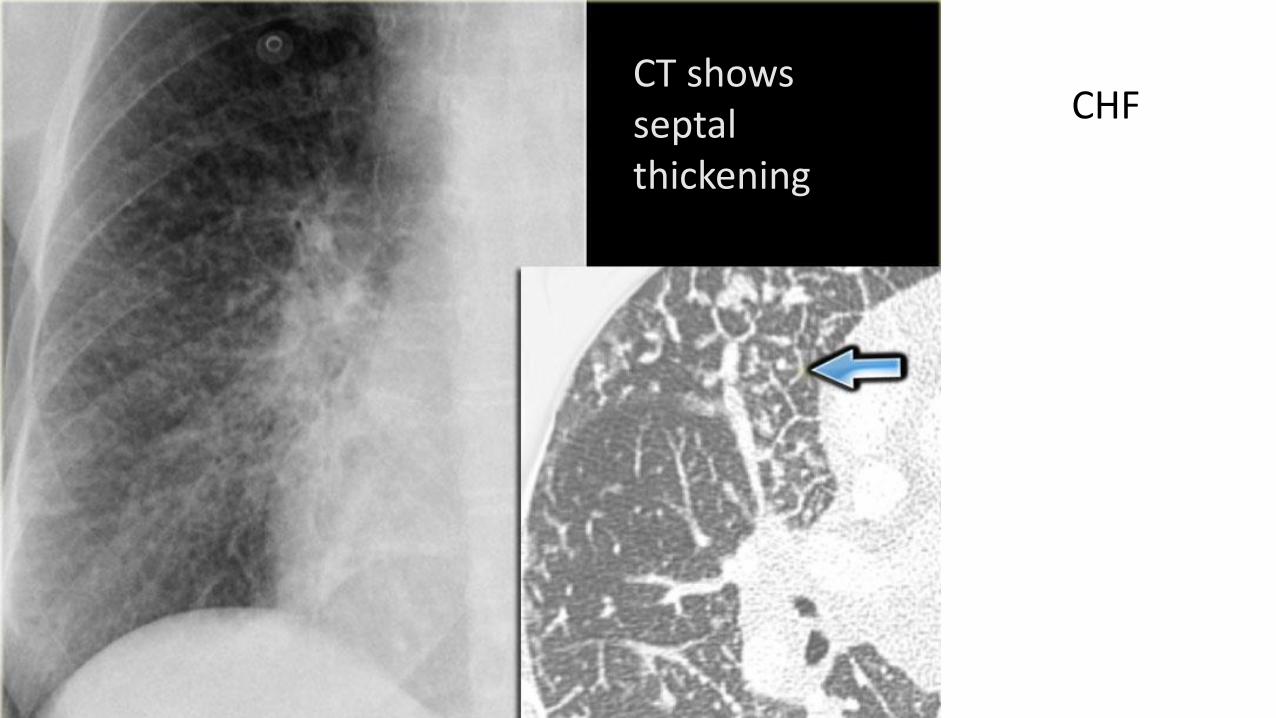
CT shows septal thickening
CHF
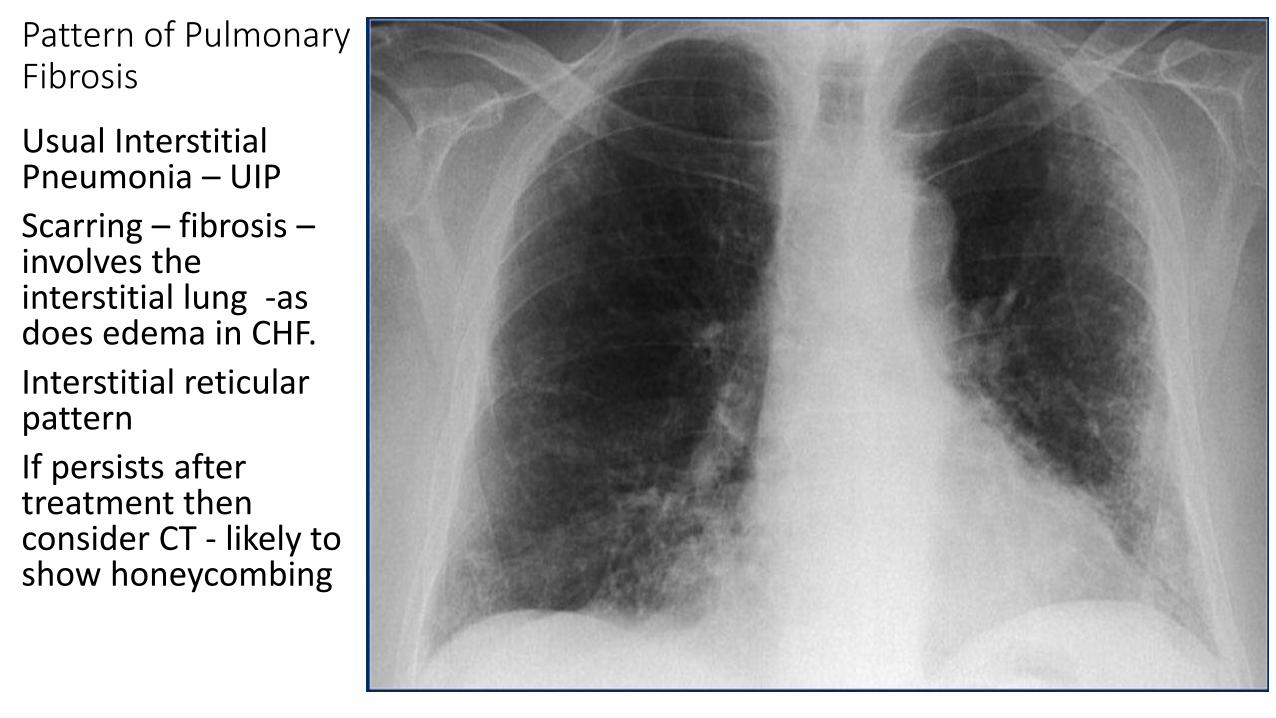
Pattern of Pulmonary Fibrosis
Usual Interstitial Pneumonia – UIP
Scarring – fibrosis – involves the interstitial lung -as does edema in CHF.
Interstitial reticular pattern
If persists after treatment then consider CT - likely to show honeycombing
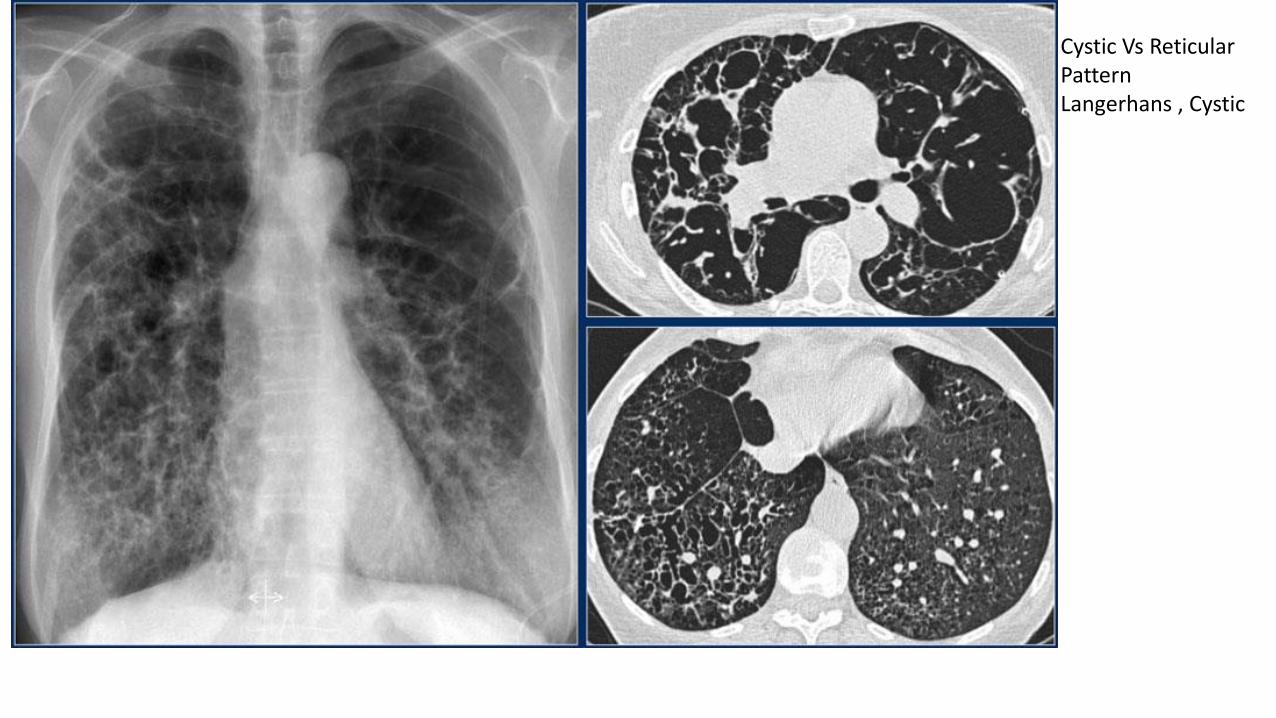
Cystic Vs Reticular Pattern Langerhans , Cystic
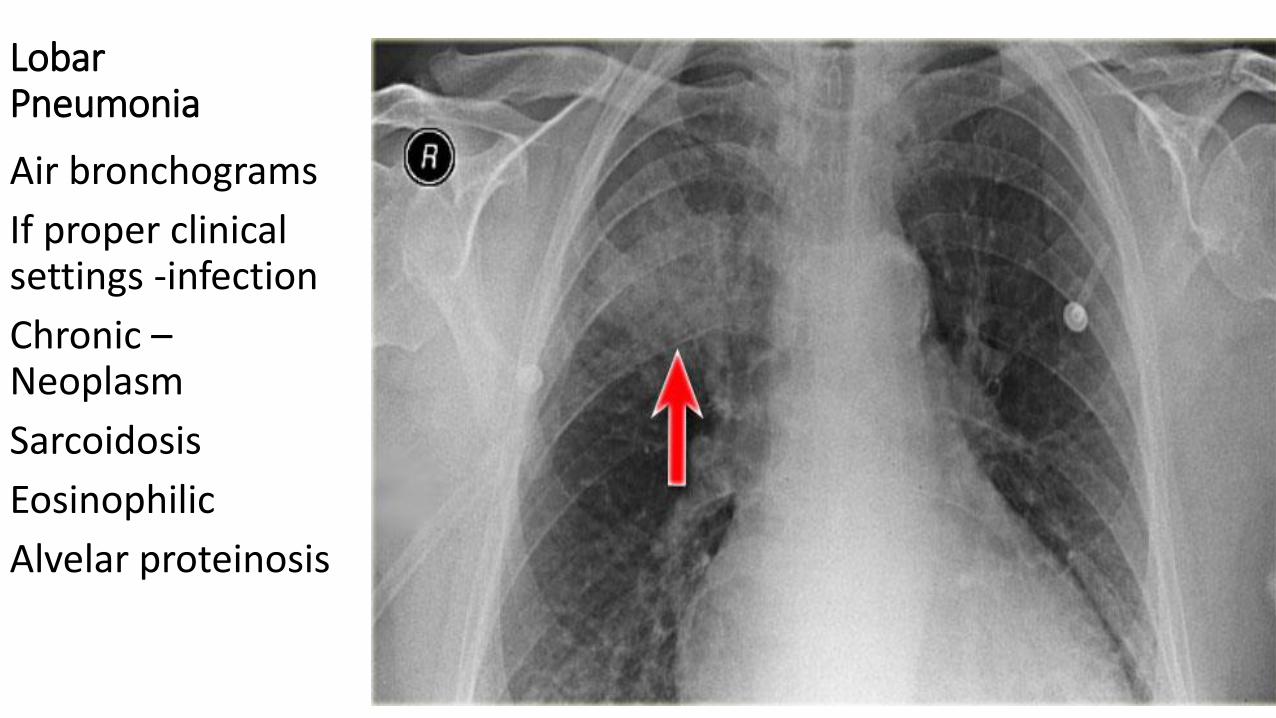
Lobar Pneumonia
Air bronchograms
If proper clinical settings -infection
Chronic – Neoplasm
Sarcoidosis
Eosinophilic
Alvelar proteinosis
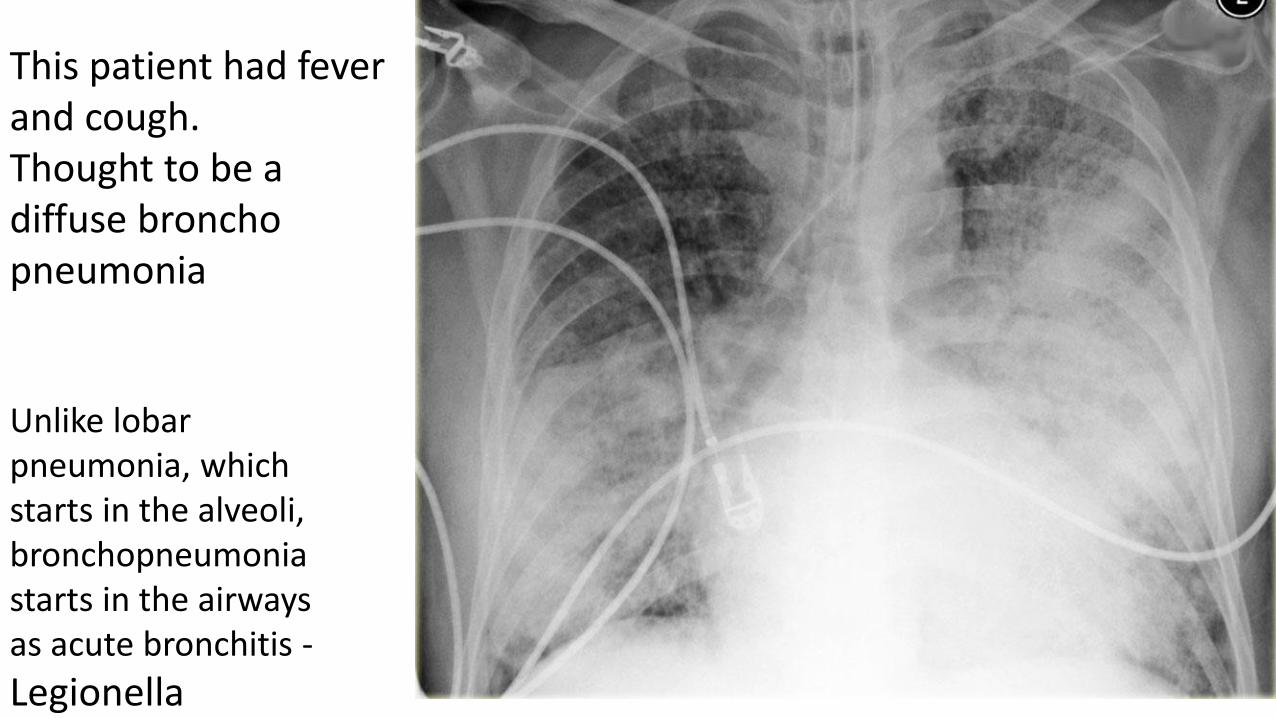
This patient had fever and cough. Thought to be a diffuse broncho pneumonia
Unlike lobar pneumonia, which starts in the alveoli, bronchopneumonia starts in the airways as acute bronchitis -
Legionella
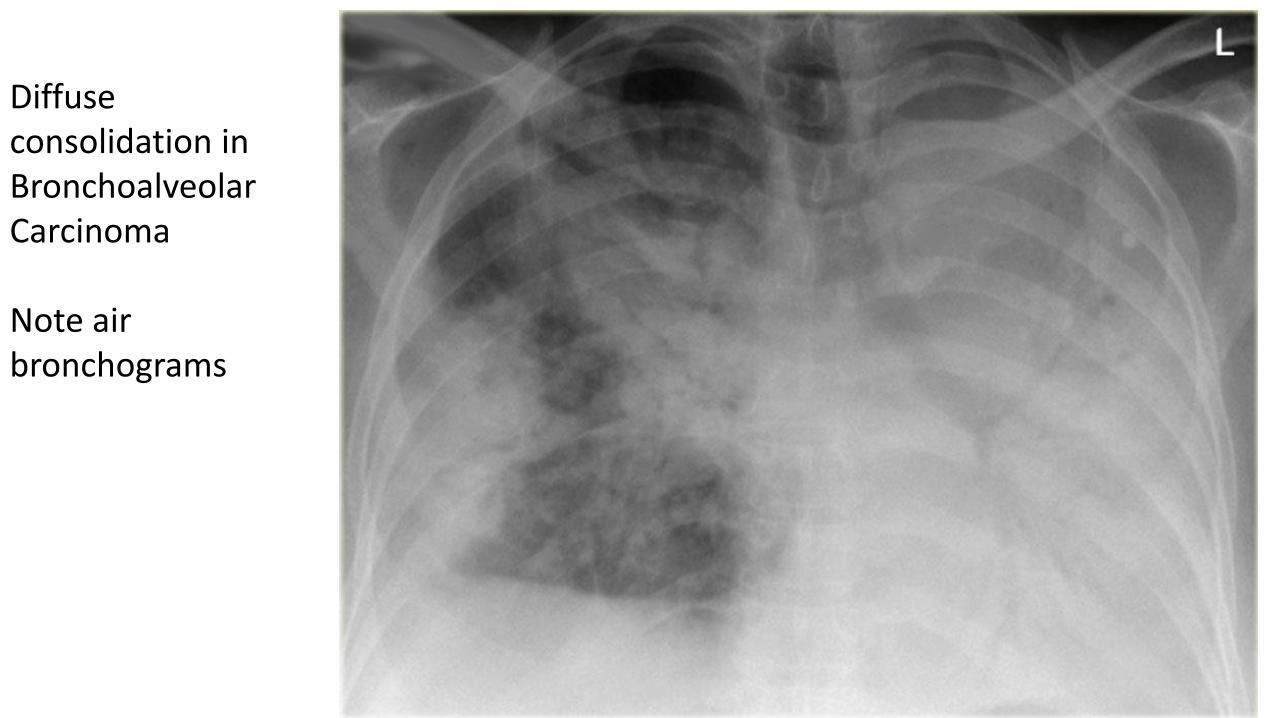
Diffuse consolidation in Bronchoalveolar Carcinoma Note air bronchograms
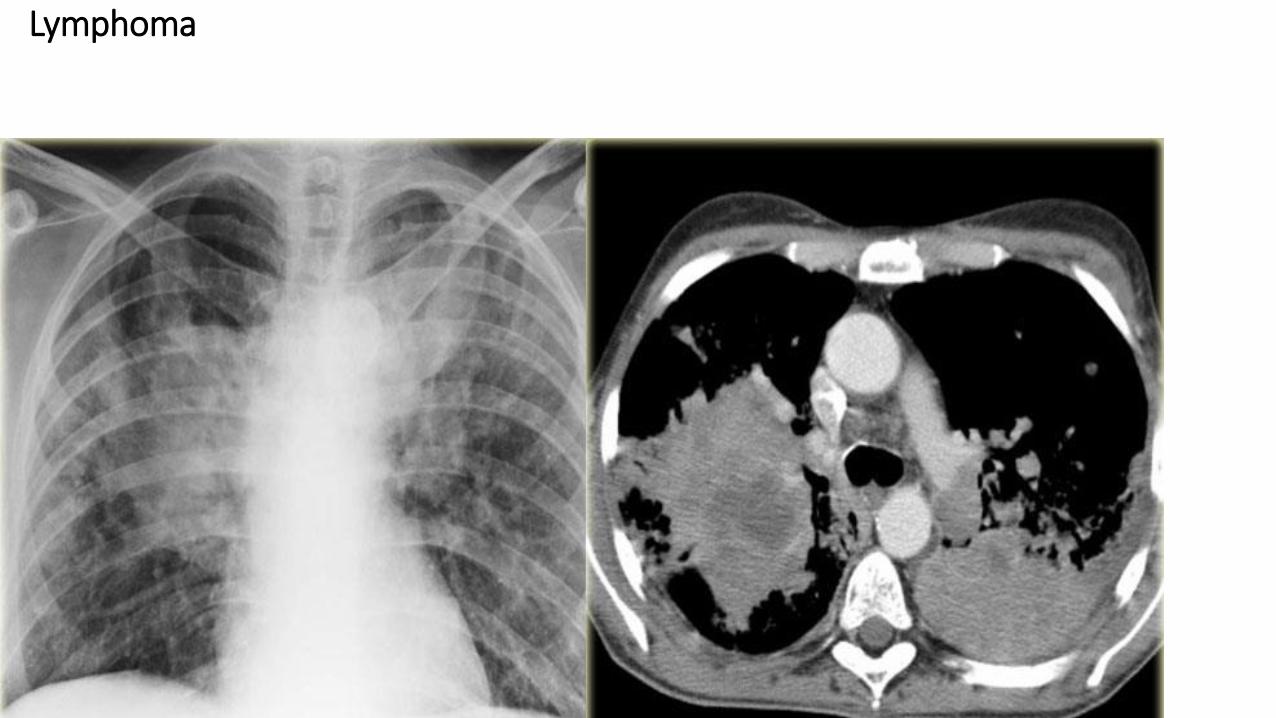
Lymphoma
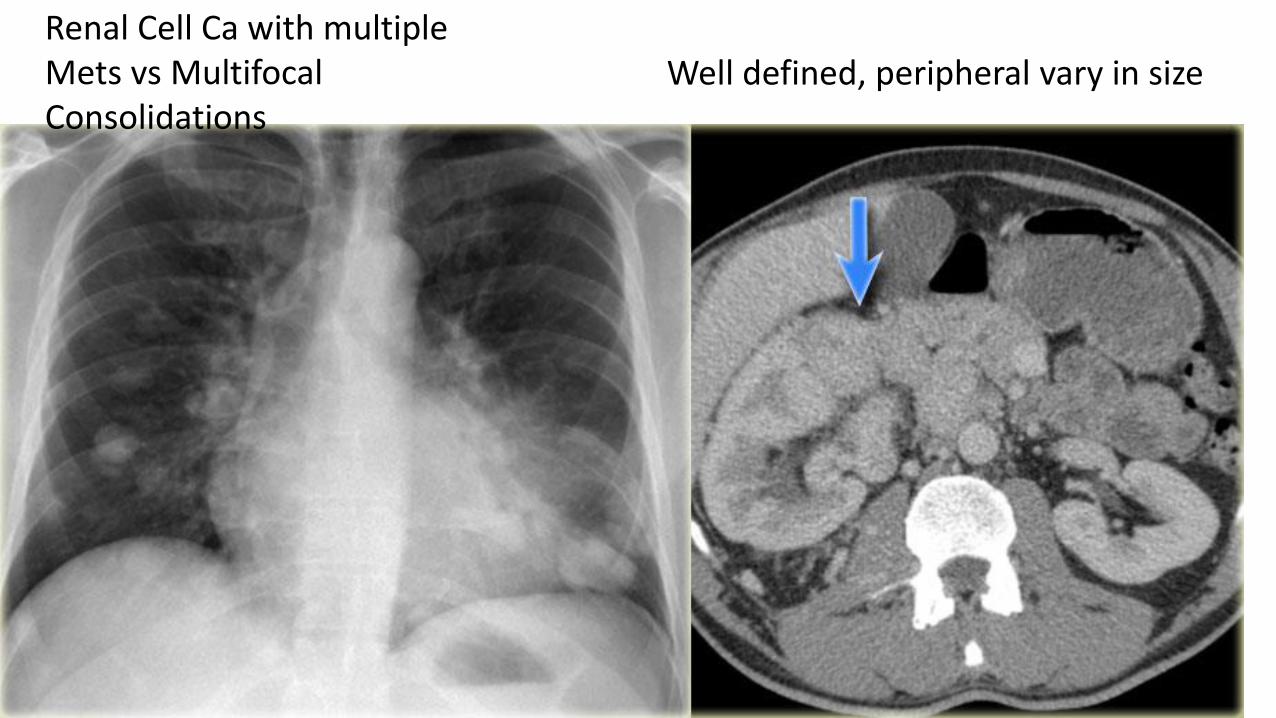
Renal Cell Ca with multiple Mets vs Multifocal Consolidations
Well defined, peripheral vary in size
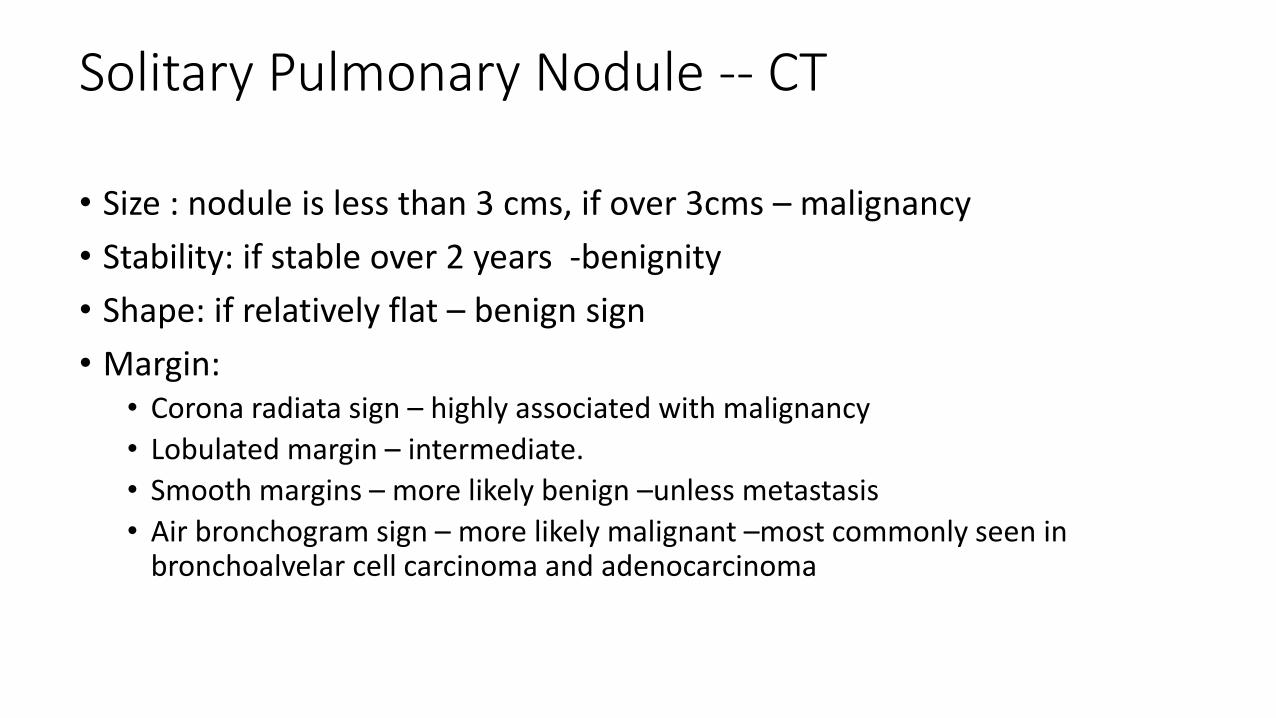
Solitary Pulmonary Nodule -- CT
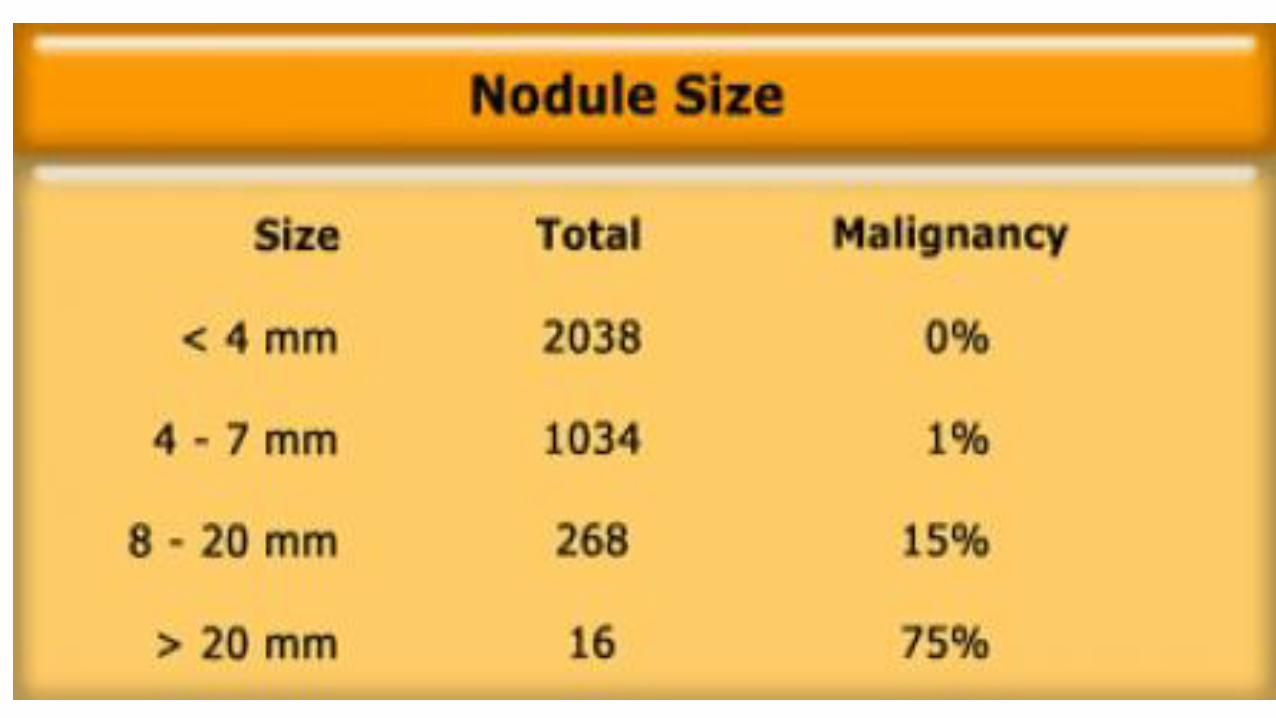
• Size : nodule is less than 3 cms, if over 3cms – malignancy
• Stability: if stable over 2 years -benignity
• Shape: if relatively flat – benign sign
• Margin: • Corona radiata sign – highly associated with malignancy
• Lobulated margin – intermediate.
• Smooth margins – more likely benign –unless metastasis
• Air bronchogram sign – more likely malignant –most commonly seen in bronchoalvelar cell carcinoma and adenocarcinoma
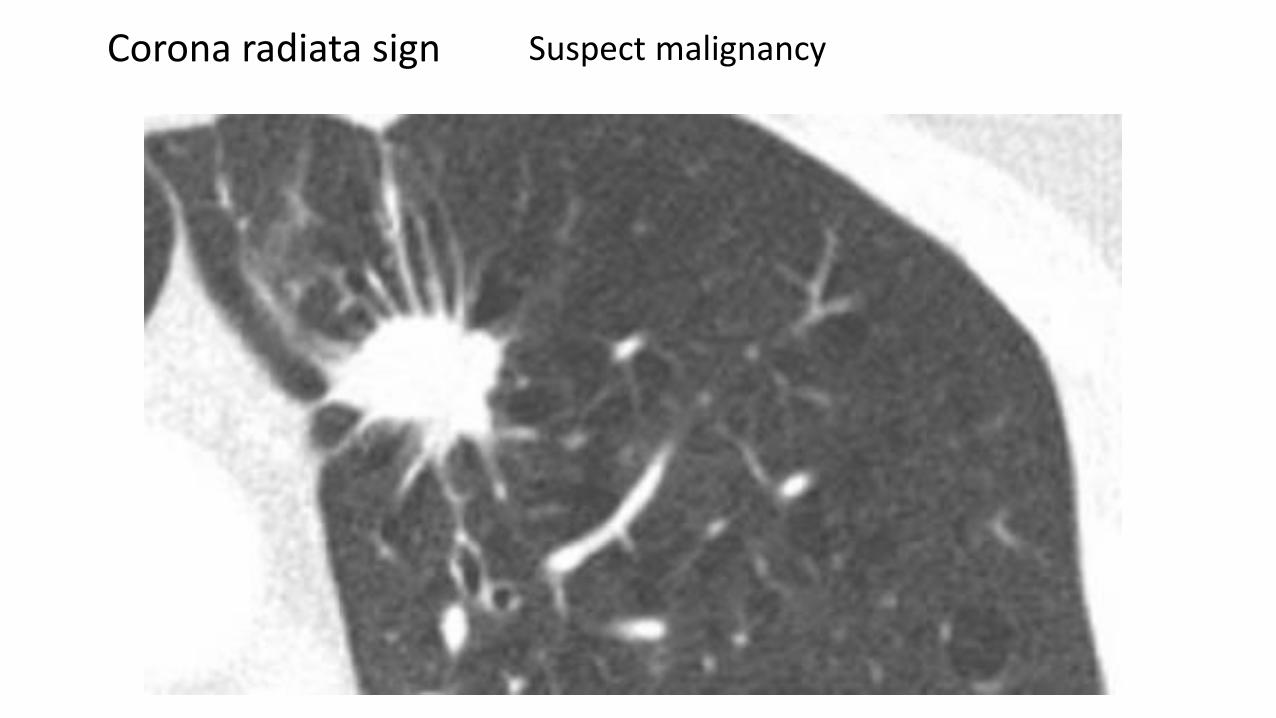
Corona radiata sign Suspect malignancy
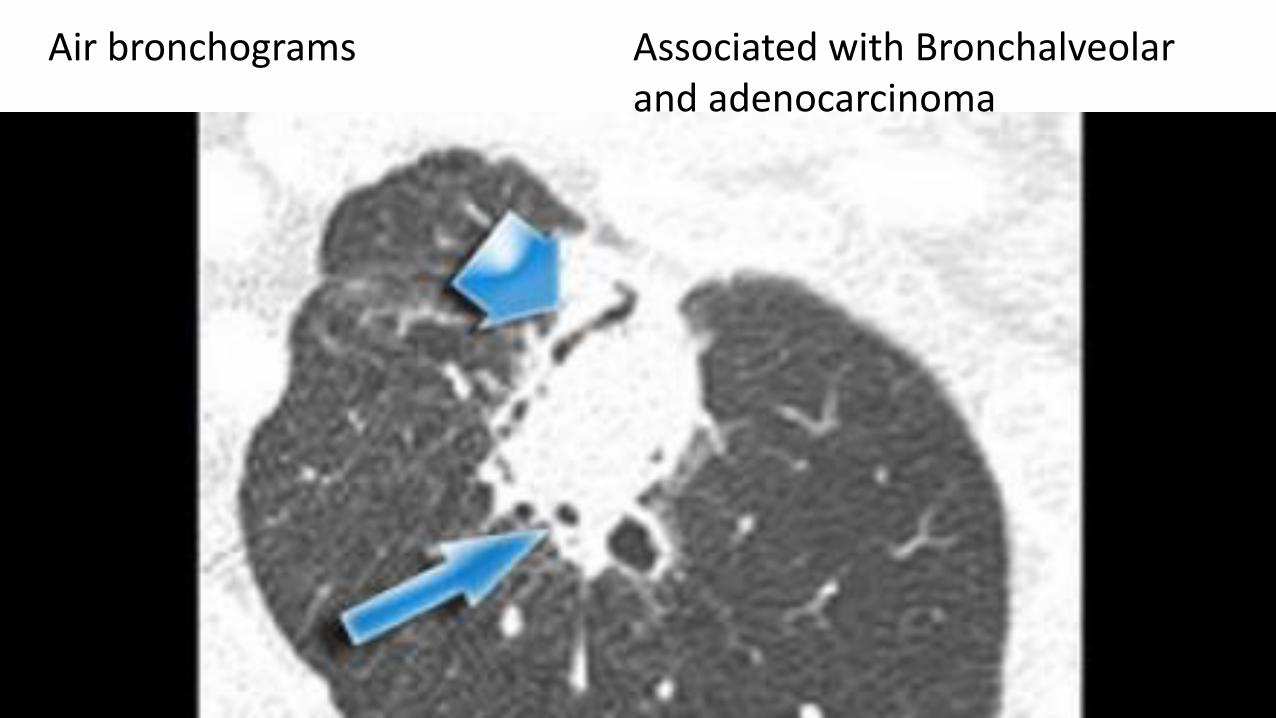
Air bronchograms Associated with Bronchalveolar and adenocarcinoma
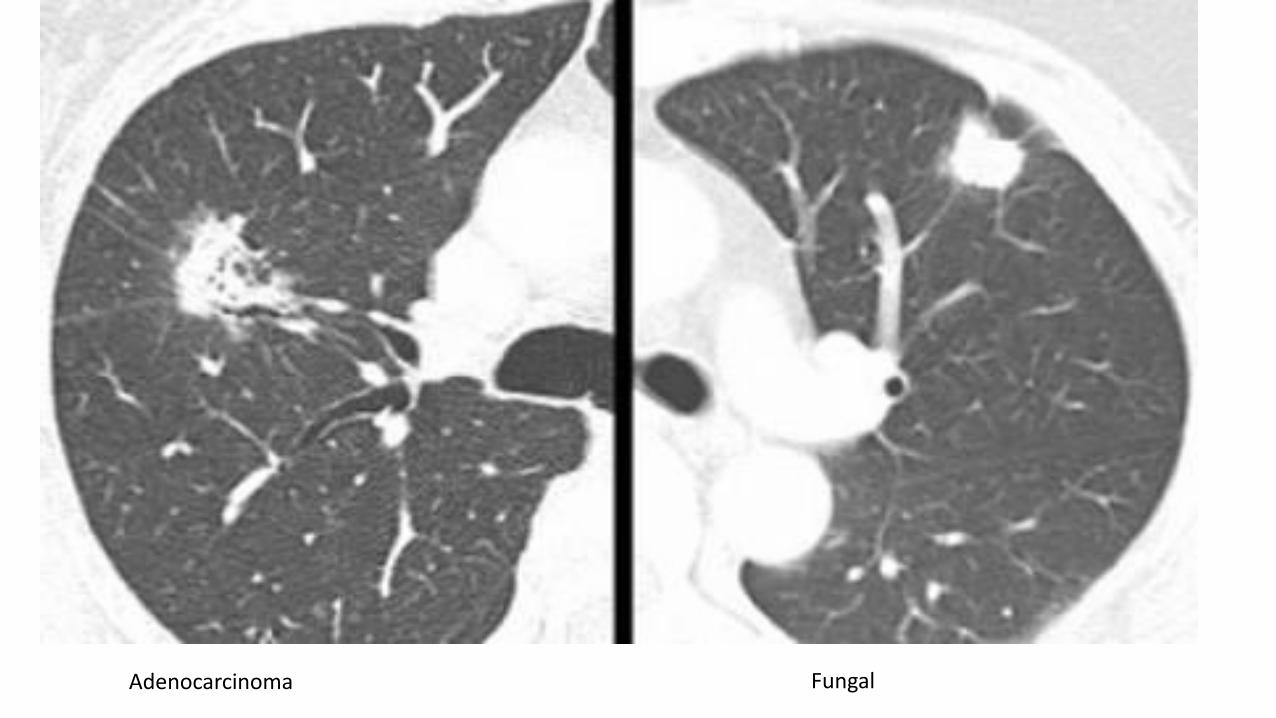
Adenocarcinoma Fungal
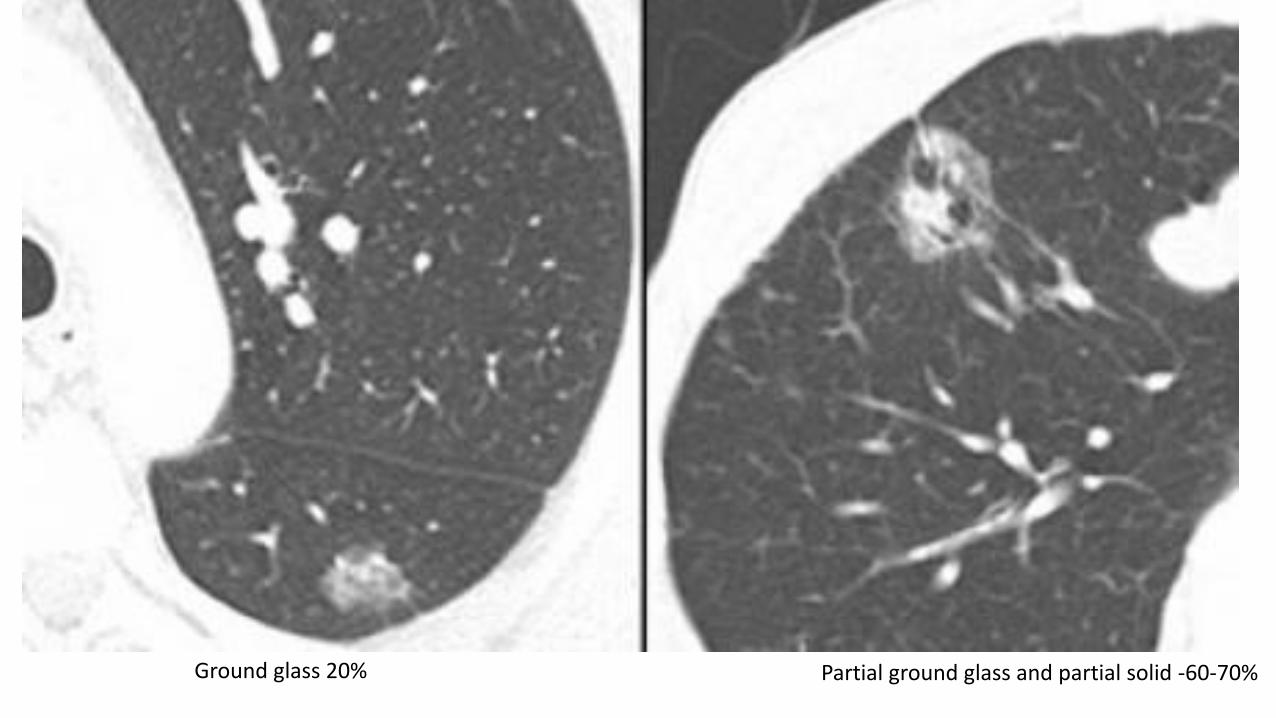
Ground glass 20% Partial ground glass and partial solid -60-70%
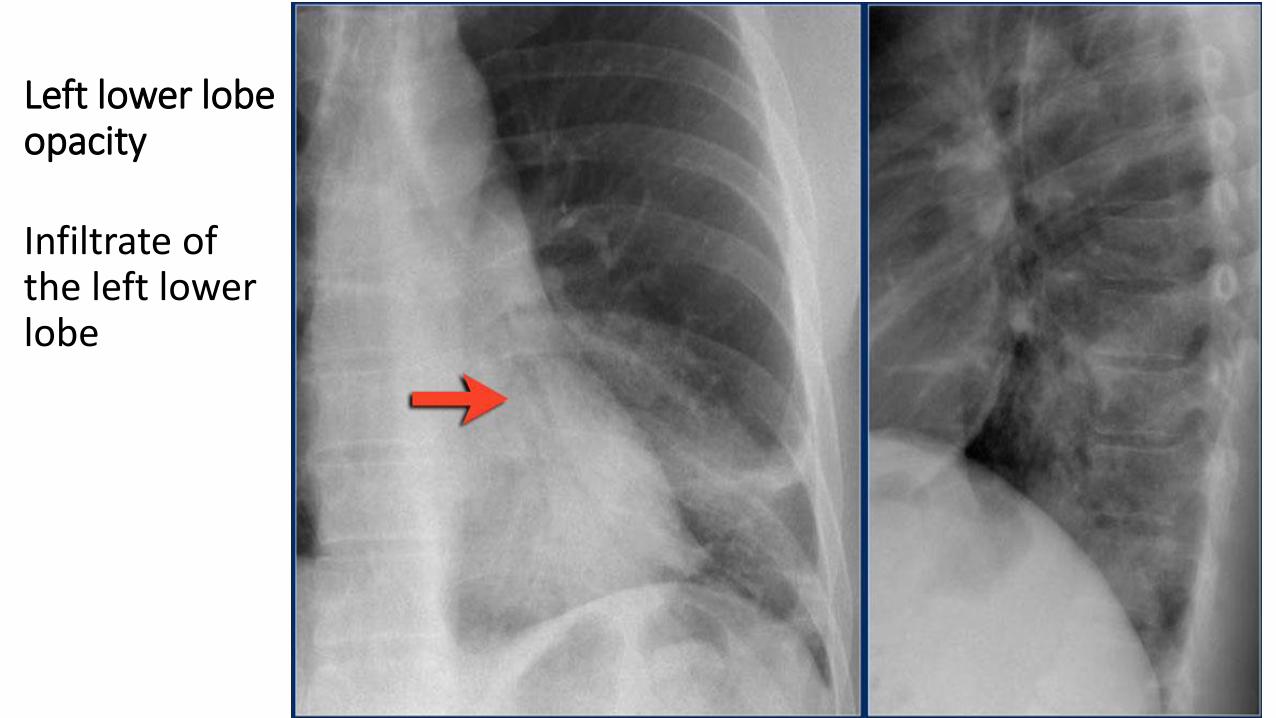
Left lower lobe opacity
Infiltrate of the left lower lobe
1.Heart Failure (HF) (Congestive Heart Failure) in Merck manual 2.Radiographic analysis of vascular distribution: a review (PDF) by Carle Ravin Presented as part of a Conference on Chest Radiology 1982 3.Pulmonary artery-bronchus ratios in patients with normal lungs, pulmonary vascular plethora, and congestive heart failure. by J H Woodring April 1991 Radiology, 179, 115-122. 4.American College of Radiology ACR Appropriateness Criteria: Congestive Heart Failure 5.The Radiologic Distinction of Cardiogenic and Noncardiogenic Edema (PDF) by Eric Milne et al American Journal of Roentgenology, Vol 144, Issue 5, 879-894 6.The vascular pedicle of the heart and the vena azygos. Part II: Acquired heart disease. by M Pistolesi, E N Milne, M Miniati and C Giuntini July 1984 Radiology, 152, 9-17. 7.Radiology Assistant http://www.radiologyassistant.nl/en/p4c132f36513d4/chest-x-ray-heart-failure.html Simone Cremers, Jennifer Bradshaw, Herfkens Albert Schweitzer Hospital, Dordecht & Medical Center Alkmaar, The Netherlands.





























