Embed Size (px)
Citation preview

Sickle Cell Disease inSickle Cell Disease inPrimary CarePrimary Care
Kathryn Kathryn HassellHassell, M.D., M.D.Professor of Medicine, Division of HematologyProfessor of Medicine, Division of Hematology
Director, Colorado Sickle Cell TreatmentDirector, Colorado Sickle Cell Treatmentand Research Centerand Research Center
University of Colorado Denver Health Sciences University of Colorado Denver Health Sciences CenterCenter

ObjectivesObjectivesObjectivesObjectives•• Understand the basic Understand the basic pathophysiologicalpathophysiologicalp p y gp p y g
processes for acute and chronic complications processes for acute and chronic complications of sickle cell diseaseof sickle cell disease
•• Recognize acute complications of sickle cell Recognize acute complications of sickle cell disease, especially in the ambulatory settingdisease, especially in the ambulatory setting, p y y g, p y y g
•• Consider diagnostic and therapeutic Consider diagnostic and therapeutic approaches to complications of sickle cell approaches to complications of sickle cell disease, with a focus on outpatient disease, with a focus on outpatient managementmanagementmanagementmanagement

Sickle Cell DiseasesSickle Cell DiseasesSickle Cell DiseasesSickle Cell Diseases
One One --globin gene that has theglobin gene that has the
sickle cell mutationsickle cell mutationsickle cell mutationsickle cell mutation
++++Another ABNORMAL Another ABNORMAL --globin gene globin gene (S, C, E, O(S, C, E, OArabArab, D, DPunjabPunjab, etc or , etc or --thalassemia)thalassemia)

ObjectivesObjectivesObjectivesObjectives
•• Understand the basic pathophysiologicalUnderstand the basic pathophysiologicalUnderstand the basic pathophysiological Understand the basic pathophysiological processes for acute and chronic processes for acute and chronic complications of sickle cell diseasecomplications of sickle cell diseasecomplications of sickle cell diseasecomplications of sickle cell disease

Sickle hemoglobin polymerizationSickle hemoglobin polymerizationd f ti f RBCd f ti f RBC→ deformation of RBC→ deformation of RBC

RBC SicklingRBC SicklingRBC SicklingRBC Sickling
SS>SC>SA>SF ASSS>SC>SA>SF AS
Δ O2, K+, H20, [Hb]2, , 2 , [ ]

Hematologic CharacteristicsHematologic CharacteristicsBaseline HbBaseline Hb ReticRetic MCVMCV
HctHct
gg
Sickle cell anemia (HbSS) 6Sickle cell anemia (HbSS) 6--8 58 5--30% normal30% normalS gene + S gene 18S gene + S gene 18--27%27%
HctHct
SickleSickle--00thalassemia 6thalassemia 6--8 58 5--30% low*30% low*S gene + no A 18S gene + no A 18--27%27%
SickleSickle--hemoglobin C (HbSC) 10hemoglobin C (HbSC) 10--14 314 3--4% normal4% normalS gene + C gene 30S gene + C gene 30--38%38%
SickleSickle--++thalassemia 11thalassemia 11--14 314 3--4% low*4% low*S gene + some A 32S gene + some A 32--40%40%
*due to thalassemia *due to thalassemia –– DO NOT GIVE IRONDO NOT GIVE IRON

ImplicationsImplicationsImplicationsImplications
•• The expected degree of anemia dependsThe expected degree of anemia dependsThe expected degree of anemia depends The expected degree of anemia depends on the type of sickle cell diseaseon the type of sickle cell disease
–– Appropriate interpretation of CBC depends on Appropriate interpretation of CBC depends on awareness of expected resultsawareness of expected results
Hb7 5 /dl l (Hb7 5 /dl l (HbSSHbSS) l ill () l ill (HbSCHbSC)?)?•• Hb7.5 g/dl: normal (Hb7.5 g/dl: normal (HbSSHbSS) or severely ill () or severely ill (HbSCHbSC)?)?
–– Worsened anemia may represent:Worsened anemia may represent:•• Acute Acute decompensationdecompensation (e.g. (e.g. aplasticaplastic crisis, chest crisis, chest
syndrome, GI bleed, incomplete abortion)syndrome, GI bleed, incomplete abortion)U d l iU d l i bid diti ( llbid diti ( ll•• Underlying coUnderlying co--morbid conditions (e.g. collagen morbid conditions (e.g. collagen vascular disease, renal failure)vascular disease, renal failure)

Beyond Anemia: The Old TheoryBeyond Anemia: The Old TheoryBeyond Anemia: The Old TheoryBeyond Anemia: The Old Theory

Newer UnderstandingNewer UnderstandingNewer UnderstandingNewer Understanding
Sickle RBC interaction withSickle RBC interaction withpostpost--capillary venulescapillary venules
lo flolo flolow flowlow flowlow oxygen tensionlow oxygen tension
May also occur in arteriolesMay also occur in arteriolesMay also occur in arterioles,May also occur in arterioles,capillary bedscapillary beds

PathophysiologicPathophysiologic MechanismsMechanismsPathophysiologicPathophysiologic MechanismsMechanisms•• Abnormal cellular adhesion to endothelium Abnormal cellular adhesion to endothelium
(sickle RBC and WBCs)(sickle RBC and WBCs)
C tit ti l ti f WBC t d iC tit ti l ti f WBC t d i
Hebbel et al, Hebbel et al, NEJM NEJM 302:992, 1980302:992, 1980
•• Constitutive elevation of WBCs noted in Constitutive elevation of WBCs noted in some patients with sickle cell diseasesome patients with sickle cell disease
C l t d ith di i i h d i l iC l t d ith di i i h d i l i–– Correlated with diminished survival in Correlated with diminished survival in Cooperative Study of Sickle Cell DiseaseCooperative Study of Sickle Cell Disease
LeikenLeiken et al; et al; Pediatrics Pediatrics 84:500, 1989; 84:500, 1989; OkpalaOkpala, , Blood RevBlood Rev 18:65, 200418:65, 2004Platt et al, Platt et al, NEJMNEJM 330:1639, 1994330:1639, 1994

Pathophysiologic MechanismsPathophysiologic MechanismsPathophysiologic MechanismsPathophysiologic Mechanisms•• Direct damage to endotheliumDirect damage to endotheliumgg
–– Difficult to distinguish effect of RBC adhesion Difficult to distinguish effect of RBC adhesion itself from elements that enhance RBC itself from elements that enhance RBC adhesionadhesion
•• e.g. hypoxia, cytokinese.g. hypoxia, cytokines
•• Effects of sickle RBCsEffects of sickle RBCs
OOFree Hb/FeFree Hb/Fe WBCWBCOO22 HypoxiaHypoxia
Oxidant injuryOxidant injuryApoptosis Apoptosis
InfarctionInfarctionRBC AdhesionRBC Adhesion

PathophysiologicPathophysiologic MechanismsMechanismsPathophysiologicPathophysiologic MechanismsMechanisms
•• Nitric Oxide (NO): multiple effectsNitric Oxide (NO): multiple effectsNitric Oxide (NO): multiple effectsNitric Oxide (NO): multiple effects(vasoactive, antiplatelet, antioxidant, antiapoptotic)(vasoactive, antiplatelet, antioxidant, antiapoptotic)
•• NO depletion in sickle cell diseaseNO depletion in sickle cell disease–– HemolysisHemolysis→free hemoglobin scavenges NO→free hemoglobin scavenges NOHemolysisHemolysis→free hemoglobin scavenges NO→free hemoglobin scavenges NO
–– Continuous endothelial stimulation may Continuous endothelial stimulation may exhaust constitutive and inducible reservesexhaust constitutive and inducible reservesexhaust constitutive and inducible reservesexhaust constitutive and inducible reserves
–– Arginine, substrate for NO production, is Arginine, substrate for NO production, is d l d i i kl ll id l d i i kl ll idepleted in sickle cell patientsdepleted in sickle cell patients
Reiter and Gladwin, Reiter and Gladwin, Curr Opin Hematol Curr Opin Hematol 10:99, 200310:99, 2003

Pathophysiologic MechanismsPathophysiologic Mechanisms“ ” “ ”“ ” “ ”“Hyperviscous” vs. “Hyperhemolytic”“Hyperviscous” vs. “Hyperhemolytic”

ImplicationsImplicationsImplicationsImplications•• Most of the Most of the pathophysiologypathophysiology of sickle cell of sickle cell
disease has little to do with “disease has little to do with “sickledsickled” red ” red blood cellsblood cells
•• Future therapy will be likely directed at:Future therapy will be likely directed at:–– Inflammatory response modificationInflammatory response modification–– Reduction of RBC adhesionReduction of RBC adhesion–– NO supplementation/NO supplementation/subtratesubtrate repletionrepletion–– Alteration of vascular remodelingAlteration of vascular remodeling
•• Unfortunately, specific screening for Unfortunately, specific screening for underlying processes not yet availableunderlying processes not yet available

ObjectivesObjectivesObjectivesObjectives
•• Recognize complications of sickle cellRecognize complications of sickle cellRecognize complications of sickle cell Recognize complications of sickle cell disease, especially in the ambulatory disease, especially in the ambulatory settingsettingsettingsetting
C id di ti d th tiC id di ti d th ti•• Consider diagnostic and therapeutic Consider diagnostic and therapeutic approaches to complications of sickle cell approaches to complications of sickle cell di ith f t ti tdi ith f t ti tdisease, with a focus on outpatient disease, with a focus on outpatient managementmanagement

Sickle Cell Disease BurdenSickle Cell Disease BurdenSickle Cell Disease BurdenSickle Cell Disease Burden•• Autopsy Study (1929Autopsy Study (1929--1996)1996)
E id f i j t tE id f i j t t
–– Evidence of chronicEvidence of chronicorgan injury in 74%organ injury in 74%
Evidence of injury at autopsyEvidence of injury at autopsyChronic lung disease / Chronic lung disease / infarctsinfarcts 56.3%56.3%
organ injury in 74%organ injury in 74%of 306 casesof 306 cases
–– Chronic organ damageChronic organ damage
Chronic renal failure / Chronic renal failure / atrophy / infarctsatrophy / infarcts 37.9%37.9%
StrokeStroke 18.2%18.2%Chronic organ damageChronic organ damagemost common causemost common causeof death in >18 yrs oldof death in >18 yrs old
StrokeStroke 18.2%18.2%Liver failure/hepatitisLiver failure/hepatitis 10%10%CardiomegalyCardiomegaly 58.4%58.4%yy
(after infection) (after infection)
•• Cohort Study of 1056 pts 40Cohort Study of 1056 pts 40 yr f/u: 73% withyr f/u: 73% with
CHFCHF 9.9%9.9%ManciManci et al, et al, Br J Br J HaemHaem 123:359, 2003123:359, 2003
•• Cohort Study of 1056 pts, 40Cohort Study of 1056 pts, 40--yr f/u: 73% with yr f/u: 73% with chronic organ damage chronic organ damage PowarsPowars, , MedicineMedicine 83:363, 200583:363, 2005

Sickle Cell Disease BurdenSickle Cell Disease BurdenSickle Cell Disease BurdenSickle Cell Disease Burden•• HydroxyureaHydroxyurea FollowFollow--Up StudyUp Study
Cause of deathCause of death n (% of total population)n (% of total population)Pulmonary diseasePulmonary disease 21 (7%)21 (7%)Accident/HomicideAccident/Homicide 7 (2.3%)7 (2.3%)StrokeStroke 6 (2.0%)6 (2.0%)Hepatic diseaseHepatic disease 4 (1.3%)4 (1.3%)Renal diseaseRenal disease 4 (1.3%)4 (1.3%)Cardiovascular diseaseCardiovascular disease 3 (1.0%)3 (1.0%)Death during crisisDeath during crisis 9 (3.0%)9 (3.0%)S i /i f tiS i /i f ti 5 (1 7%)5 (1 7%)
15%15%
5%5%Sepsis/infectionSepsis/infection 5 (1.7%)5 (1.7%) 5%5%Steinberg, JAMA 289:1645, 2003

Sickle Lung DiseaseSickle Lung DiseaseSickle Lung DiseaseSickle Lung Disease
•• Present in up to 25Present in up to 25--40% of sickle cell patients40% of sickle cell patientsPresent in up to 25Present in up to 25 40% of sickle cell patients40% of sickle cell patients–– Initial restrictive patternInitial restrictive pattern
Subsequent progressive vascular changes inSubsequent progressive vascular changes in–– Subsequent progressive vascular changes in Subsequent progressive vascular changes in some patientssome patients
•• intimalintimal hyperplasia, hyperplasia, microinterstitalmicrointerstital fibrosis, fibrosis, plexiformplexiformyp p ,yp p , ,, pplesions may occurlesions may occur
–– May be indicated by presence of elevated May be indicated by presence of elevated tricuspidtricuspid regurgitantregurgitant (TR) jet velocity on echo(TR) jet velocity on echotricuspid tricuspid regurgitantregurgitant (TR) jet velocity on echo(TR) jet velocity on echo
Haque et al, Haque et al, Human Pathol Human Pathol 33:1037, 200233:1037, 2002

Sickle Lung DiseaseSickle Lung DiseaseSickle Lung DiseaseSickle Lung Disease
•• Annual screening echo recommendedAnnual screening echo recommendedAnnual screening echo recommendedAnnual screening echo recommended–– TR jet velocity of >2.5 mg/sec associated with TR jet velocity of >2.5 mg/sec associated with
1010--fold increased risk of death in adultsfold increased risk of death in adults1010 fold increased risk of death in adultsfold increased risk of death in adults
Gladwin, NEJM 350:886, 2004

Sickle Lung DiseaseSickle Lung DiseaseSickle Lung DiseaseSickle Lung Disease•• Conflicting data regarding TR jet velocityConflicting data regarding TR jet velocity
–– Cause of deaths in adults unclear; may not be Cause of deaths in adults unclear; may not be due to cardiopulmonary diseasedue to cardiopulmonary diseaseChild h l f l t d TRChild h l f l t d TR–– Children have same prevalence of elevated TR Children have same prevalence of elevated TR jet velocity, but not associated mortalityjet velocity, but not associated mortality
Lee, Lee, Br J Br J HaematolHaematol 146:437, 2009146:437, 2009,, ,,
–– Some studies question the importance of Some studies question the importance of elevated TR jet velocity in absence of “true” elevated TR jet velocity in absence of “true” pulmonary hypertensionpulmonary hypertension
vanBeersvanBeers, , Am J Am J HematolHematol 83:850, 200883:850, 2008
–– Recent study ofRecent study of sildenafilsildenafil closed early futile toclosed early futile toRecent study of Recent study of sildenafilsildenafil closed early, futile to closed early, futile to show difference in 6show difference in 6--minute walk test minute walk test

ImplicationsImplicationsImplicationsImplications•• Symptoms ofSymptoms of dyspneadyspnea, shortness of breath,, shortness of breath,Symptoms of Symptoms of dyspneadyspnea, shortness of breath, , shortness of breath,
hypoxia and intermittent chest pain may hypoxia and intermittent chest pain may indicate pulmonary hypertensionindicate pulmonary hypertension–– Full pulmonary evaluation, including echo and Full pulmonary evaluation, including echo and
ultimately right heart ultimately right heart cathcath may be neededmay be needed•• “Heart failure” (elevated JVD edema) is“Heart failure” (elevated JVD edema) is•• Heart failure (elevated JVD, edema) is Heart failure (elevated JVD, edema) is
almost always due to almost always due to rightright--sidedsided heart failureheart failure–– May be associated with intermittent renalMay be associated with intermittent renal–– May be associated with intermittent renal May be associated with intermittent renal
failurefailure•• Annual screening echo may reveal elevated Annual screening echo may reveal elevated g yg y
TR jet, prompt early referral for evaluationTR jet, prompt early referral for evaluation

Sickle Cell Disease and the HeartSickle Cell Disease and the HeartSickle Cell Disease and the HeartSickle Cell Disease and the Heart
•• Flow murmurs are common due to anemiaFlow murmurs are common due to anemiaFlow murmurs are common due to anemiaFlow murmurs are common due to anemia–– Does not usually represent Does not usually represent valvularvalvular diseasedisease
•• Ventricular hypertrophy diastolic dysfunctionVentricular hypertrophy diastolic dysfunctionVentricular hypertrophy, diastolic dysfunction Ventricular hypertrophy, diastolic dysfunction may develop howevermay develop however–– In general, cardiac output is highIn general, cardiac output is highg , p gg , p g–– Pulmonary edema is not expectedPulmonary edema is not expected
•• Classic coronary artery disease does not occurClassic coronary artery disease does not occur–– Risk factors (e.g. Risk factors (e.g. ↑ ↑ cholesterol) uncommoncholesterol) uncommon–– Sickle RBCs do not appear to induce remodeling Sickle RBCs do not appear to induce remodeling
or occlude coronary arteriesor occlude coronary arteries

Sickle Cell Anemia (Sickle Cell Anemia (HbSSHbSS))d S i Bl d Pd S i Bl d Pand Systemic Blood Pressureand Systemic Blood Pressure
•• SBP 80SBP 80--100, DBP 50100, DBP 50--60 not uncommon60 not uncommonSBP 80SBP 80 100, DBP 50100, DBP 50 60 not uncommon60 not uncommon•• Recent Nigerian study notes lower diastolic and Recent Nigerian study notes lower diastolic and
mean arterial pressure, wider pulse pressuremean arterial pressure, wider pulse pressurep , p pp , p p
•• “Relative” hypertension associated with “Relative” hypertension associated with Oguanobi, J Cardiol 2010, epub
pulmonary and renal disease pulmonary and renal disease (SBP 120(SBP 120--139, DBP 139, DBP 7070--89)89) GorduekGorduek, , Am J HemAm J Hem 83:15, 200883:15, 2008

Sickle NephropathySickle NephropathySickle NephropathySickle Nephropathy
•• CKI occurs 10CKI occurs 10--15% of sickle cell patients15% of sickle cell patientsCKI occurs 10CKI occurs 10 15% of sickle cell patients15% of sickle cell patients
•• Clinical course: resembles diabetic eventsClinical course: resembles diabetic events–– Initial Initial hyperfiltrationhyperfiltration and enlarged and enlarged glomeruliglomeruli–– MicroalbuminuriaMicroalbuminuria//proteinuriaproteinuria–– Focal segmental Focal segmental glomerulosclerosisglomerulosclerosis (FSGS)(FSGS)

Sickle Cell Disease andSickle Cell Disease and ProteinuriaProteinuriaSickle Cell Disease and Sickle Cell Disease and ProteinuriaProteinuria
•• Common finding in adult sickle cell anemiaCommon finding in adult sickle cell anemiaCommon finding in adult sickle cell anemiaCommon finding in adult sickle cell anemia–– MicroalbuminuriaMicroalbuminuria: 30: 30--50%50%–– MacroalbuminuriaMacroalbuminuria: 20: 20--30%30%–– Also seen in up to 30% of other types (e.g. Also seen in up to 30% of other types (e.g. HbSCHbSC))
GuaschGuasch, , J Am Soc J Am Soc NephrolNephrol 17:2228, 200617:2228, 2006
•• Improves/resolves with ACEImproves/resolves with ACE--inhibitor therapyinhibitor therapy–– Persistent for up to 18 months after discontinuationPersistent for up to 18 months after discontinuation
R l ti l llR l ti l ll t l t d d it l/l BPt l t d d it l/l BP–– Relatively wellRelatively well--tolerated despite normal/low BPtolerated despite normal/low BPFalk RJ. N Engl J Med 326:1992; Foucan L. Am J Med 104:339, 1998
•• Unclear if this changes the progression toUnclear if this changes the progression to•• Unclear if this changes the progression to Unclear if this changes the progression to renal failurerenal failure

Sickle NephropathySickle NephropathySickle NephropathySickle Nephropathy
•• Creatinine lost through tubuleCreatinine lost through tubule → creatinine→ creatinineCreatinine lost through tubule Creatinine lost through tubule → creatinine → creatinine doesdoes notnot represent GFRrepresent GFR
Creatinine does not rise until GFR falls to lessCreatinine does not rise until GFR falls to less–– Creatinine does not rise until GFR falls to less Creatinine does not rise until GFR falls to less than ~ 30 ml/minthan ~ 30 ml/min
Guasch, Guasch, Kidney IntKidney Int49:786, 199649:786, 1996
–– Creatinine clearance also significantly Creatinine clearance also significantly g yg yoverestimates actual GFRoverestimates actual GFR

ImplicationsImplicationsImplicationsImplications•• Screening for Screening for proteinuriaproteinuria probably warrantedprobably warranted
–– Evaluation for other causesEvaluation for other causes–– Consider therapy with ACE inhibitor or ARBConsider therapy with ACE inhibitor or ARB
•• Don’t rely on Don’t rely on creatininecreatinine to assess renal functionto assess renal function–– CreatinineCreatinine of >1.0 mg/dl (even >0.7of >1.0 mg/dl (even >0.7--0.8) may 0.8) may
represent significant renal insufficiencyrepresent significant renal insufficiencyrepresent significant renal insufficiencyrepresent significant renal insufficiency–– Pay attention to “expected” values given Pay attention to “expected” values given
weight/muscle mass (normal may be <0.5)weight/muscle mass (normal may be <0.5)g ( y )g ( y )•• Clinical suspicion for underlying renal diseaseClinical suspicion for underlying renal disease
–– Relative hypertension (SBP>120?, DBP>80?)Relative hypertension (SBP>120?, DBP>80?)–– Worsening anemia (Worsening anemia (epoepo deficiency)deficiency)

Sickle Cell and StrokeSickle Cell and StrokeSickle Cell and StrokeSickle Cell and Stroke
•• LargeLarge--vessel ischemic stroke affects up to 10%vessel ischemic stroke affects up to 10%LargeLarge vessel ischemic stroke affects up to 10% vessel ischemic stroke affects up to 10% of of HbHb SS patients by the age of 20SS patients by the age of 20
•• Adults at risk for CNS hemorrhage Adults at risk for CNS hemorrhage MM f tif ti–– MoyaMoya--moyamoya formationformation
–– AneurysmsAneurysms

Sickle Cell and StrokeSickle Cell and StrokeSickle Cell and StrokeSickle Cell and Stroke
•• Large vessel occlusion:Large vessel occlusion:Large vessel occlusion:Large vessel occlusion:
–– Exuberant intimal hyperplasiaExuberant intimal hyperplasia–– Proliferation of fibroblasts and smooth muscleProliferation of fibroblasts and smooth muscle–– Focal splitting of internal elastic laminaFocal splitting of internal elastic lamina–– Medial necrosisMedial necrosis–– Damage to vaso vasorum?Damage to vaso vasorum?
•• CNS Hemorrhage:CNS Hemorrhage:
–– Above changes Above changes → focally weakened vessels→ focally weakened vessels

Sickle Cell and CNS InjurySickle Cell and CNS InjurySickle Cell and CNS InjurySickle Cell and CNS Injury
•• Silent infarction andSilent infarction and neurocognitiveneurocognitiveSilent infarction and Silent infarction and neurocognitiveneurocognitivedysfunction noted in children and adults dysfunction noted in children and adults without a history of overt strokewithout a history of overt strokeyy
•• Up to 50% of individuals have MRI findings: Up to 50% of individuals have MRI findings: infarction, ischemia or atrophyinfarction, ischemia or atrophyinfarction, ischemia or atrophyinfarction, ischemia or atrophy–– Predilection to frontal lobe area in some studiesPredilection to frontal lobe area in some studies
•• NeurocognitiveNeurocognitive deficits in documented indeficits in documented inNeurocognitiveNeurocognitive deficits in documented in deficits in documented in otherwise neurologically intact otherwise neurologically intact HbSSHbSS adultsadults
Wong andWong and PowarsPowars HemHem OncOnc ClinClin NANA 19:839 2005;19:839 2005;Wong and Wong and PowarsPowars, , Hem Hem OncOnc ClinClin NANA 19:839, 2005;19:839, 2005;Gold, Gold, PediatrPediatr Hem Hem OncOnc 25:409, 200825:409, 2008
VichinskyVichinsky, , JAMAJAMA 303:1823, 2010 303:1823, 2010

ImplicationsImplicationsImplicationsImplications
•• A severe or atypical headache in an adultA severe or atypical headache in an adultA severe or atypical headache in an adult A severe or atypical headache in an adult sickle cell patients (with or without sickle cell patients (with or without neurologic symptoms) is a CNS bleed until neurologic symptoms) is a CNS bleed until g y p )g y p )proven otherwiseproven otherwise–– Urgent nonUrgent non--contrasted head CTcontrasted head CTgg
•• Impairment ofImpairment of neurocognitiveneurocognitive function mayfunction mayImpairment of Impairment of neurocognitiveneurocognitive function may function may significantly impact on comprehension of significantly impact on comprehension of disease and adherence to therapydisease and adherence to therapypypy

Sickle RetinopathySickle RetinopathySickle RetinopathySickle Retinopathy
•• Occurs in 11Occurs in 11--45% of sickle cell patients45% of sickle cell patientsOccurs in 11Occurs in 11 45% of sickle cell patients45% of sickle cell patients
•• Arteriolar vasoArteriolar vaso--occlusion occlusion → hairpin loops and → hairpin loops and AV t b l bl d flAV t b l bl d flAV anatamoses → abnormal blood flow → AV anatamoses → abnormal blood flow → neovascularization (sea fan formation)neovascularization (sea fan formation)
•• Venular occlusion → Venular occlusion → sea fan infractionsea fan infraction
•• Retinal detachment,Retinal detachment,hemorrhage blindnesshemorrhage blindnesshemorrhage, blindnesshemorrhage, blindness

ImplicationsImplicationsImplicationsImplications
•• Annual dilated ophthalmologic examinationAnnual dilated ophthalmologic examinationAnnual dilated ophthalmologic examinationAnnual dilated ophthalmologic examination
Ch i i i (“fl t ” l f i lCh i i i (“fl t ” l f i l•• Change in vision (“floaters”, loss of visual Change in vision (“floaters”, loss of visual acuity or visual field) is an ophthalmologic acuity or visual field) is an ophthalmologic emergencyemergencyemergencyemergency–– Urgent ophthalmology consultUrgent ophthalmology consult

Other Affected OrgansOther Affected OrgansOther Affected OrgansOther Affected Organs
•• Hip and Shoulder JointsHip and Shoulder JointsHip and Shoulder JointsHip and Shoulder Joints–– AvascularAvascular necrosis, bone infarctsnecrosis, bone infarcts
•• SkinSkin•• SkinSkin–– Leg ulcersLeg ulcers
S lS l•• SpleenSpleen–– SplenicSplenic sequestration may occur in sequestration may occur in HbSCHbSC and and
th “ ild ” fth “ ild ” fother “milder” formsother “milder” forms•• GallstonesGallstones
–– Assumed to be present, no intervention unless Assumed to be present, no intervention unless symptomaticsymptomatic

Spared (?) Vascular BedsSpared (?) Vascular BedsSpared (?) Vascular BedsSpared (?) Vascular Beds
•• LiverLiverLiverLiver–– Most injury due to iron deposition or infectionMost injury due to iron deposition or infection
No recognized chronic “sickleNo recognized chronic “sickle hepatopathyhepatopathy””–– No recognized chronic sickle No recognized chronic sickle hepatopathyhepatopathy–– Acute hepatic sequestration may occurAcute hepatic sequestration may occur
Remember: AST LDH are RBC enzymes!Remember: AST LDH are RBC enzymes!–– Remember: AST, LDH are RBC enzymes!Remember: AST, LDH are RBC enzymes!
•• GI tractGI tractG t actG t act–– Rare case reports of intestinal ischemia only Rare case reports of intestinal ischemia only
in acutely in acutely hypotensivehypotensive patients on patients on yy ypyp ppvasopressorsvasopressors

Plenty of Time for Organ DamagePlenty of Time for Organ DamagePlenty of Time for Organ DamagePlenty of Time for Organ Damage•• Life Expectancy as of 1992 (1972)Life Expectancy as of 1992 (1972)
HbHb SS 42SS 42 4848–– HbHb SS: 42SS: 42--48 years48 years–– HbHb SC: 60SC: 60--69 years69 years–– HbHb AA: 70AA: 70--75 years75 years
•• HbHb SS Jamaican study as of 2001 (1978)SS Jamaican study as of 2001 (1978)–– HbHb SS: 53SS: 53--58 years58 years
HbHb AA: 71AA: 71 76 years76 years–– HbHb AA: 71AA: 71--76 years76 years•• HydreaHydrea followfollow--up study for up study for HbHb SS (1996)SS (1996)
–– 299 severely affected enrolled (mean age 32)299 severely affected enrolled (mean age 32)–– 75% still alive 9 years later75% still alive 9 years later
•• Cohort (Cohort (HbSSHbSS) born after 1975: 50) born after 1975: 50--55 yrs 55 yrs Platt et alPlatt et al NEJMNEJM 330:1639 1994;330:1639 1994; CharacheCharache et alet al NEJMNEJM 332:1317 1995;332:1317 1995;Platt et al, Platt et al, NEJM NEJM 330:1639, 1994; 330:1639, 1994; CharacheCharache et al, et al, NEJM NEJM 332:1317, 1995; 332:1317, 1995; Steinberg et al, Steinberg et al, JAMAJAMA 289:1645, 2003; 289:1645, 2003; WierengaWierenga et al, et al, LancetLancet 357:680, 2001357:680, 2001PowarsPowars, , MedicineMedicine 83:363, 200583:363, 2005

Acute Sickle Cell EventsAcute Sickle Cell EventsAcute Sickle Cell EventsAcute Sickle Cell Events
•• Acute pain events (“crisis”)Acute pain events (“crisis”)Acute pain events ( crisis )Acute pain events ( crisis )•• Acute chest syndromeAcute chest syndrome
A t l i tA t l i t•• Acute neurologic eventsAcute neurologic events–– Ischemic stroke (children>adults)Ischemic stroke (children>adults)–– Hemorrhage (adults)Hemorrhage (adults)
•• PriapismPriapismpp•• Acute hepatic sequestrationAcute hepatic sequestration•• AcuteAcute splenicsplenic sequestration (nonsequestration (non--HbSSHbSS))•• Acute Acute splenicsplenic sequestration (nonsequestration (non--HbSSHbSS))

Acute Sickle Cell EventsAcute Sickle Cell EventsAcute Sickle Cell EventsAcute Sickle Cell Events
•• Acute insult toAcute insult to endotheliumendotheliumAcute insult to Acute insult to endotheliumendothelium–– hypoxiahypoxia–– cytokines (inflammation infection)cytokines (inflammation infection)cytokines (inflammation, infection)cytokines (inflammation, infection)
•• Consequences of acute endothelial injuryConsequences of acute endothelial injury–– enhanced cellular adhesion (RBC, WBC)enhanced cellular adhesion (RBC, WBC)–– vascular disruption and inflammationvascular disruption and inflammation
id ti / f i i jid ti / f i i j•• oxidative/reperfusion injuryoxidative/reperfusion injury•• endothelial retraction endothelial retraction → tissue edema→ tissue edema
acute vasoconstrictionacute vasoconstriction–– acute vasoconstrictionacute vasoconstriction

Acute Sickle Cell EventsAcute Sickle Cell Events
Acute endothelial injuryAcute endothelial injury with RBC adhesion in with RBC adhesion in postpost--capillary venules, vasoconstrictioncapillary venules, vasoconstriction

Management of Acute EventsManagement of Acute EventsManagement of Acute EventsManagement of Acute Events
•• ReverseReverse pathophysiologicpathophysiologic factorsfactorsReverse Reverse pathophysiologicpathophysiologic factorsfactors–– Pain control (reduces physiologic stress)Pain control (reduces physiologic stress)–– Treat inflammation/infectionTreat inflammation/infectionTreat inflammation/infectionTreat inflammation/infection–– Maintain NORMAL volume: excess fluid may Maintain NORMAL volume: excess fluid may
promote acute chest syndromepromote acute chest syndromepromote acute chest syndromepromote acute chest syndrome–– Maintain NORMAL oxygen: no benefit to Maintain NORMAL oxygen: no benefit to
excess oxygenexcess oxygen•• Transfusion for acute endTransfusion for acute end--organ damageorgan damage
–– Doesn’t reduce duration uncomplicated pain crisisDoesn’t reduce duration uncomplicated pain crisisp pp p

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies•• Transfusion TherapyTransfusion Therapy
–– “Dilutes out” sickle RBCs“Dilutes out” sickle RBCs
l d t t k ifl d t t k if HbSHbS 30%30%•• precludes recurrent stroke if precludes recurrent stroke if HbSHbS<30%<30%•• reduces abnormal flow in cerebral vessels in reduces abnormal flow in cerebral vessels in
children with sickle cell disease (remodeling?)children with sickle cell disease (remodeling?)children with sickle cell disease (remodeling?)children with sickle cell disease (remodeling?)Adams, Adams, J Child J Child NeurolNeurol 15:344, 200015:344, 2000
Provides healthy RBCs which mayProvides healthy RBCs which may–– Provides healthy RBCs, which may Provides healthy RBCs, which may
•• restore RBC restore RBC vasodilatoryvasodilatory capacity (e.g. NO)capacity (e.g. NO)•• provide “sump” for toxins (e.g. FFA ?)provide “sump” for toxins (e.g. FFA ?)

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies
•• Transfusion TherapyTransfusion TherapyTransfusion TherapyTransfusion Therapy
–– InfectionInfection–– AlloimmunizationAlloimmunization
•• Precluded by minorPrecluded by minor--antigen matchingantigen matching•• Always request minorAlways request minor--antigen matched blood antigen matched blood
(at least C, D, E, (at least C, D, E, KellKell))I O l dI O l d–– Iron OverloadIron Overload
•• Precluded by exchange transfusionPrecluded by exchange transfusion•• OralOral chelatorchelator available (available (deferasiroxdeferasirox))•• Oral Oral chelatorchelator available (available (deferasiroxdeferasirox))

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies
•• Bone Marrow TransplantBone Marrow TransplantBone Marrow TransplantBone Marrow Transplant
–– The cure: “a permanent transfusion”The cure: “a permanent transfusion”
–– Only 17% of eligible recipients have suitable Only 17% of eligible recipients have suitable HLAHLA--matched sibling donormatched sibling donorgg
–– Selection criteria in evolution (risk v. benefit)Selection criteria in evolution (risk v. benefit)
–– MiniMini--allogeneicallogeneic transplantation results in transplantation results in frequent rejectionfrequent rejection
Hoppe and Walters, Curr Opin Oncol 13:85, 2001;Iannone et al, Biol Blood Marrow Transplant 9:519, 2003

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies
•• HydroxyureaHydroxyureaHydroxyureaHydroxyurea
I d ti f f t l h l biI d ti f f t l h l biInduction of fetal hemoglobinInduction of fetal hemoglobin

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies
•• HydroxyureaHydroxyurea reduces sickle hemoglobinreduces sickle hemoglobinHydroxyureaHydroxyurea reduces sickle hemoglobin reduces sickle hemoglobin polymerizationpolymerization
–– Less Less hemolysishemolysis with improved anemia with improved anemia I d MCV (lI d MCV (l HbHb i )i )–– Increased MCV (lower Increased MCV (lower HbHb concentration)concentration)

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies
•• Clinical Effects ofClinical Effects of HydroxyureaHydroxyureaClinical Effects of Clinical Effects of HydroxyureaHydroxyurea
–– 50% reduction is acute pain events and acute 50% reduction is acute pain events and acute chest syndromechest syndrome
–– Apparent improvement in mortality, correlatedApparent improvement in mortality, correlatedApparent improvement in mortality, correlated Apparent improvement in mortality, correlated with with HbFHbF response; persistent even after 17 response; persistent even after 17 yrs of followyrs of follow--upup
–– No evidence of reduction in chronic organ No evidence of reduction in chronic organ injury (Babyinjury (Baby--HUG study)HUG study)injury (Babyinjury (Baby--HUG study)HUG study)
CharacheCharache et al, et al, NEJM NEJM 332:1317, 1995; 332:1317, 1995; SteinbergSteinberg et al, et al, JAMAJAMA 289:1645, 2003289:1645, 2003Steinberg, Steinberg, Am J Am J HematolHematol 85:409, 201085:409, 2010

DiseaseDisease--Modifying TherapiesModifying TherapiesDiseaseDisease Modifying TherapiesModifying Therapies
•• Clinical Effects ofClinical Effects of HydroxyureaHydroxyureaClinical Effects of Clinical Effects of HydroxyureaHydroxyurea
–– Takes 2Takes 2--3 months of daily therapy to see 3 months of daily therapy to see changes in fetal hemoglobinchanges in fetal hemoglobin
–– Occasional patient benefits within 4Occasional patient benefits within 4--6 weeks6 weeksOccasional patient benefits within 4Occasional patient benefits within 4 6 weeks 6 weeks (symptoms improve)(symptoms improve)
P h d t h t l i t i it (ANC 1P h d t h t l i t i it (ANC 1 2 000)2 000)–– Pushed to hematologic toxicity (ANC 1Pushed to hematologic toxicity (ANC 1--2,000)2,000)
–– Not an acute intervention; close followNot an acute intervention; close follow--upup;; pp
Charache et al, Charache et al, NEJM NEJM 332:1317, 1995; 332:1317, 1995; SteinbergSteinberg et al, et al, JAMAJAMA 289:1645, 2003289:1645, 2003

Coordinated, Comprehensive Coordinated, Comprehensive H l h C N d dH l h C N d dHealth Care NeededHealth Care Needed
•• Sickle cell gene does not protect againstSickle cell gene does not protect againstSickle cell gene does not protect against Sickle cell gene does not protect against other and more common diseasesother and more common diseases–– Asthma, COPD, collagen vascular diseases,Asthma, COPD, collagen vascular diseases,Asthma, COPD, collagen vascular diseases, Asthma, COPD, collagen vascular diseases,
sarcoidosissarcoidosis, diabetes, malignancy, peptic ulcer , diabetes, malignancy, peptic ulcer disease, disease, Crohn’sCrohn’s, ulcerative colitis, etc., ulcerative colitis, etc.
•• Having sickle cell disease does not eliminate Having sickle cell disease does not eliminate the need for routine health care maintenancethe need for routine health care maintenance–– Specialists are notoriously poor at primary careSpecialists are notoriously poor at primary care–– Each specialist focuses on their own areaEach specialist focuses on their own area

Primary Care: What to Look For?Primary Care: What to Look For?Primary Care: What to Look For?Primary Care: What to Look For?
•• Everything as for anyone elseEverything as for anyone elseEverything as for anyone elseEverything as for anyone else•• Additional annual screening:Additional annual screening:
Retinal examRetinal exam–– Retinal examRetinal exam–– Urinalysis for protein, serum Urinalysis for protein, serum creatininecreatinine–– EchoEcho–– EchoEcho
•• If on transfusions:If on transfusions:FerritinFerritin for iron overloadfor iron overload–– FerritinFerritin for iron overloadfor iron overload
–– Hepatitis/HIV if indicatedHepatitis/HIV if indicated•• If onIf on hydreahydrea: CBC: CBC neutrophilneutrophil countcount•• If on If on hydreahydrea: CBC, : CBC, neutrophilneutrophil countcount

Pain in Sickle Cell DiseasePain in Sickle Cell DiseasePain in Sickle Cell DiseasePain in Sickle Cell Disease
•• Acute, intermittent, unpredictable, severeAcute, intermittent, unpredictable, severeAcute, intermittent, unpredictable, severe Acute, intermittent, unpredictable, severe episodes called “crisis”episodes called “crisis”–– Typical duration said to be 7Typical duration said to be 7--10 days10 daysypyp yy–– Associated by some patients with deathAssociated by some patients with death–– Onset may occur in early infancyOnset may occur in early infancyy y yy y y
•• Chronic pain may develop in adolescence and Chronic pain may develop in adolescence and adulthoodadulthood–– Not necessarily acute vasoNot necessarily acute vaso--occlusionocclusion
•• Other pain still occurs (e.g. injury, menses, SLE)Other pain still occurs (e.g. injury, menses, SLE)–– To be distinguished from acute vasoTo be distinguished from acute vaso--occlusionocclusion

Pain in Sickle Cell DiseasePain in Sickle Cell DiseasePAIN TYPEPAIN TYPE ORIGINS & SYNDROMESORIGINS & SYNDROMESNocioceptiveNocioceptive
Deep somaticDeep somatic VasoVaso--occlusion, bone infarction, priapismocclusion, bone infarction, priapism--Superficial somaticSuperficial somatic Leg ulcersLeg ulcersVisceralVisceral Splenic/hepatic sequestration splenicSplenic/hepatic sequestration splenicVisceral Visceral Splenic/hepatic sequestration, splenic Splenic/hepatic sequestration, splenic
infarction, cholelithiasisinfarction, cholelithiasisNeuropathicNeuropathic
Peripheral neuropathyPeripheral neuropathy VasoVaso--occlusion, neuropathiesocclusion, neuropathiesCentral neuropathicCentral neuropathic CNS damage, central sensitization (?)CNS damage, central sensitization (?)
MixedMixed VasoVaso--occlusionocclusionMixed Mixed VasoVaso occlusionocclusionBreakthroughBreakthrough
Incident (movement)Incident (movement) VasoVaso--occlusion, skeletal damageocclusion, skeletal damageNonincidentNonincident Transient flares of pain during analgesiaTransient flares of pain during analgesia
Adapted from Niscola, Adapted from Niscola, Pain MedicinePain Medicine 10:470, 200910:470, 2009

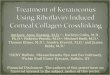
Utilization of Healthcare for Pain: Utilization of Healthcare for Pain: The Exception, Not the RuleThe Exception, Not the Rule
40
50
pepe
30
40
Phe
noty
Phe
noty r = 0r = 0
0 < r < 10 < r < 11 31 3
20
rcen
t of P
rcen
t of P 1 < r < 31 < r < 3
3 < r < 63 < r < 6> 6> 6
0
10Per
Per
> 6> 6
0Hb SSHb SS Hb SCHb SC SBSB++ThalThal SBSBooThalThal
Adapted from Platt et al, Adapted from Platt et al, NEJMNEJM 325:11, 1991325:11, 1991

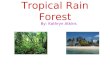
Pain in Sickle Cell DiseasePain in Sickle Cell DiseasePain in Sickle Cell DiseasePain in Sickle Cell Disease
•• Old cohort study dataOld cohort study dataOld cohort study dataOld cohort study data–– Acute crisis rate (utilization):Acute crisis rate (utilization):
Hb SSHb SS 0 8 events/year0 8 events/yearHb SSHb SS 0.8 events/year0.8 events/yearHb SHb Sββoothalassemiathalassemia 1.0 events/year1.0 events/yearHb SHb Sββ+thalassemia+thalassemia 0 4 events/year0 4 events/year
–– For HbSS:For HbSS:5 2% f ti t ht f 35 2% f ti t ht f 3 10 i i /10 i i /
Hb SHb Sββ+thalassemia+thalassemia 0.4 events/year0.4 events/year
•• 5.2% of patients sought care for 35.2% of patients sought care for 3--10 crisis/year10 crisis/year•• These patients accounted for 32.9% of all These patients accounted for 32.9% of all
episodesepisodespp
Platt et al, NEJM 325:11, 1991

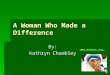
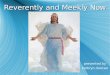
Survival by Pain RatesSurvival by Pain RatesSurvival by Pain RatesSurvival by Pain RatesProjected Median Survival for CSSCD Subjects Projected Median Survival for CSSCD Subjects >> 2020
50
55
45
50
ars
40Yea
30
35
< 1 1 < t < 3 > 3< 1 1 < to < 3 > 3Yearly Pain Rate
Platt et al, NEJM 325:11, 1991

Adult Sickle Cell PainAdult Sickle Cell Pain –– PiSCESPiSCESAdult Sickle Cell Pain Adult Sickle Cell Pain PiSCESPiSCES•• PPain ain iin n SSickle ickle CCell ell EEpidemiology pidemiology SStudy tudy
(PiSCES)(PiSCES)(PiSCES)(PiSCES)•• 232 patients, aged 16232 patients, aged 16--64, completed up to 180 64, completed up to 180
d il i di id il i di idaily pain diariesdaily pain diaries–– Mean number of diaries: 158Mean number of diaries: 158
Included if at least 30 diariesIncluded if at least 30 diaries–– Included if at least 30 diariesIncluded if at least 30 diaries–– 31,017 diaries available31,017 diaries available–– Subjects:Subjects:SubjectsSubjects
•• Mean age 32.6 yearsMean age 32.6 years•• 87% HS graduates87% HS graduates
76% single 61% female76% single 61% female•• 76% single, 61% female76% single, 61% female•• 66% Hb SS66% Hb SS
Smith, Smith, Ann Intern MedAnn Intern Med 148:94, 2008148:94, 2008

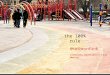
Adult SCD Pain CommonAdult SCD Pain CommonB M d A HB M d A HBut Managed At HomeBut Managed At Home
PiSCES data from 31,017 daily pain PiSCES data from 31,017 daily pain
Crisis Crisis –– Utilization 3.5%Utilization 3.5%
y py pdiaries from 232 patients patientsdiaries from 232 patients patients
Crisis Crisis –– No utilization 12.7%No utilization 12.7%
Pain Pain –– Not Crisis 38.3%Not Crisis 38.3%
No Pain 45.5%No Pain 45.5%
Smith, Smith, Ann Intern MedAnn Intern Med 148:94, 2008148:94, 2008

Adult Sickle Cell PainAdult Sickle Cell Pain -- PiSCESPiSCESAdult Sickle Cell Pain Adult Sickle Cell Pain PiSCESPiSCES•• Frequency of painFrequency of pain
–– More than half of patients had pain more than half More than half of patients had pain more than half the timethe time29% h d i l d29% h d i l d–– 29% had pain nearly every day29% had pain nearly every day
–– 15% rarely had pain15% rarely had painIntensity of pain correlates with characterizationIntensity of pain correlates with characterization•• Intensity of pain correlates with characterization Intensity of pain correlates with characterization of pain:of pain:
Crisis Crisis -- utilizationutilization 5.9 5.9 ±± 0.10.1Crisis Crisis -- no utilization no utilization 5.0 5.0 ±± 0.10.1Pain Pain –– not crisisnot crisis 3.9 3.9 ±± 0.10.1No painNo pain 0.0 0.0 ±± 0.00.0
Smith, Smith, Ann Intern MedAnn Intern Med 148:94, 2008148:94, 2008

Adult Sickle Cell Pain Adult Sickle Cell Pain -- PiSCESPiSCES•• Few differences between men and womenFew differences between men and women
ParameterParameter MalesMales FemalesFemalesDays with pain (%)Days with pain (%) 58.6%58.6% 56.5%56.5%N b f i i d 6N b f i i d 6 7 77 7 9 69 6Number of pain episodes over 6 mosNumber of pain episodes over 6 mos 7.77.7 9.69.6Mean pain scores in crisis/not in crisisMean pain scores in crisis/not in crisis 5.5/2.55.5/2.5 5.6/2.25.6/2.2Hb SSHb SS -- Days in crisis (%)Days in crisis (%) 18 5%18 5% 11 6%11 6%
N diff i di t i t fN diff i di t i t f
Hb SS Hb SS Days in crisis (%)Days in crisis (%) 18.5%18.5% 11.6%11.6%Hb SS Hb SS -- Days of utilization (%)Days of utilization (%) 5.1%5.1% 2.7%2.7%
–– No difference in distress or interference scores No difference in distress or interference scores overall or during crisisoverall or during crisis
–– Women reported higher bodily pain score (SFWomen reported higher bodily pain score (SF--36)36)–– Women reported higher bodily pain score (SFWomen reported higher bodily pain score (SF--36)36)
McClish, McClish, J of Women’s HealthJ of Women’s Health 15:146, 200615:146, 2006

Sickle Cell Pain:Sickle Cell Pain:H lthH lth R l t d Q lit f LifR l t d Q lit f LifHealthHealth--Related Quality of LifeRelated Quality of Life
•• PiSCES Study using SFPiSCES Study using SF--3636PiSCES Study using SFPiSCES Study using SF 3636–– Patients with SCD:Patients with SCD:
•• Worse than the general population in all categoriesWorse than the general population in all categoriesWorse than the general population in all categories Worse than the general population in all categories except mental healthexcept mental health
•• Comparable or worse than asthma, cystic fibrosis, Comparable or worse than asthma, cystic fibrosis, h di l i ti th di l i ti themodialysis patientshemodialysis patients
–– Strong correlation with painStrong correlation with pain•• Less physical functioning physical and emotionalLess physical functioning physical and emotional•• Less physical functioning, physical and emotional Less physical functioning, physical and emotional
role, bodily pain, general health, vitality, social role, bodily pain, general health, vitality, social function with increased pain, especially crisisfunction with increased pain, especially crisis
•• No change in mental healthNo change in mental health domaindomain
McClish, McClish, Health and Qual Life OutcomesHealth and Qual Life Outcomes 3:50, 20053:50, 2005

Adult Sickle Cell Pain Adult Sickle Cell Pain -- PiSCESPiSCES•• Role of depression and anxietyRole of depression and anxiety
–– 27% (64/168) depressed by PHQ questionnaire27% (64/168) depressed by PHQ questionnaire•• Higher than general AfricanHigher than general African--American populationAmerican population•• Comparable to other chronic conditions (e.g. DM)Comparable to other chronic conditions (e.g. DM)
–– Impact on pain and utilizationImpact on pain and utilizationNot depressedNot depressed DepressedDepressed
Days in pain (%)Days in pain (%) 49 6%49 6% 71 1%71 1%Days in pain (%)Days in pain (%) 49.6%49.6% 71.1%71.1%Days in crisis (%)Days in crisis (%) 14.7%14.7% 16.7%16.7%Days using opioid at home (%)Days using opioid at home (%) 40.5%40.5% 58.3%58.3%y g p ( )y g p ( )Hospitalization (median % days)Hospitalization (median % days) 2.82.8 2.772.77ED visits (median % days)ED visits (median % days) 1.351.35 1.341.34Unscheduled clinic visits (% days)Unscheduled clinic visits (% days) 1.261.26 1.631.63Scheduled clinic visits (% days)Scheduled clinic visits (% days) 1.891.89 2.822.82

Substance Abuse in the CommunitySubstance Abuse in the Communityyy•• General population figures (college kids):General population figures (college kids):
Use in the last yearUse in the last year–– Use in the last yearUse in the last yearSubstanceSubstance CaucasiansCaucasians HispanicHispanic AfricanAmericansAfricanAmericansMarijuanaMarijuana 3838--41%41% 4040--45%45% 1818--33%33%MarijuanaMarijuana 3838--41%41% 4040--45%45% 1818--33%33%CocaineCocaine 33--5%5% 4.44.4--6.5%6.5% 0.70.7--1.8%1.8%Pain medsPain meds 8.28.2--8.9%8.9% 8.78.7--9.8%9.8% 4.94.9--6.4%6.4%
•• Estimated addiction and substance abuse in the Estimated addiction and substance abuse in the ii l 6 4l 6 4 8 8%8 8%
Pain medsPain meds 8.28.2 8.9%8.9% 8.78.7 9.8%9.8% 4.94.9 6.4%6.4%McCabe, J Ethn Subst Abuse 6:75, 2007
community atcommunity at--large: 6.4large: 6.4--8.8% 8.8% Solomon, Solomon, BloodBlood 111:997, 2008111:997, 2008
•• Substance abuse in health care providers: 10Substance abuse in health care providers: 10--15%15%Substance abuse in health care providers: 10Substance abuse in health care providers: 10 15%15%BaldisseriBaldisseri, , CritCrit Care MedCare Med 35(35(SupplSuppl 2):2106, 20072):2106, 2007

Sickle Cell and Substance AbuseSickle Cell and Substance Abuse•• Addiction and substance abuse estimates for Addiction and substance abuse estimates for
adult sickle cell cohortsadult sickle cell cohorts ≤ gen’l population≤ gen’l populationadult sickle cell cohorts adult sickle cell cohorts ≤ gen l population≤ gen l population–– Cincinnati, 1988 14/160 (9%)Cincinnati, 1988 14/160 (9%)–– Philadelphia, 1992 0/501 (0%)Philadelphia, 1992 0/501 (0%)p , ( )p , ( )–– London, 2002 4/800 (0.5%)London, 2002 4/800 (0.5%)–– New Haven, 2007 8/96 (8.3%)New Haven, 2007 8/96 (8.3%)
Solomon, Solomon, BloodBlood 111:997, 2008111:997, 2008
•• Alcohol abuse in sickle cell Alcohol abuse in sickle cell –– PiSCESPiSCES31% f h t t it i f b31% f h t t it i f b–– 31% of cohort met criteria for abuse31% of cohort met criteria for abuse
–– No difference in pain between abusers and No difference in pain between abusers and nonabusers equal/less utilization by abusersnonabusers equal/less utilization by abusersnonabusers, equal/less utilization by abusersnonabusers, equal/less utilization by abusers
•• Better physical quality of life reported by abusersBetter physical quality of life reported by abusersLevenson, Levenson, Am J AddictionAm J Addiction 16:383, 200716:383, 2007

Sickle Cell and Pain BehaviorsSickle Cell and Pain Behaviors•• Pseudoaddiction: behaviors to obtain pain Pseudoaddiction: behaviors to obtain pain
di ti b f l t ll d idi ti b f l t ll d imedication because of poorly controlled painmedication because of poorly controlled pain–– Distinguished when behaviors resolve with effective Distinguished when behaviors resolve with effective
pain managementpain managementpain managementpain management•• Pain Coping Strategies in SCD: Pain Coping Strategies in SCD:
pseudoaddiction (vs. addiction) associated with:pseudoaddiction (vs. addiction) associated with:pseudoaddiction (vs. addiction) associated with:pseudoaddiction (vs. addiction) associated with:–– Disputes and arguments over pain medicationDisputes and arguments over pain medication–– Active coping behaviors, e.g. distractionActive coping behaviors, e.g. distraction
•• “I do anything to get my mind off the pain”“I do anything to get my mind off the pain”
–– Use of overUse of over--thethe--counter medicationcounter medication
Elander, Elander, J Pain Symptom ManagJ Pain Symptom Manag 27:156, 200427:156, 2004Lusher, Lusher, Clin J PainClin J Pain 22:316, 200622:316, 2006

Coordinated Care forCoordinated Care forSi kl C ll DiSi kl C ll DiSickle Cell DiseaseSickle Cell Disease
•• Sickle cell disease is about more than pain and Sickle cell disease is about more than pain and requires comprehensive carerequires comprehensive care
•• Fewer than 50% of all adults with sickle cellFewer than 50% of all adults with sickle cellFewer than 50% of all adults with sickle cell Fewer than 50% of all adults with sickle cell disease receive care from specialistsdisease receive care from specialists
•• The number of adults will grow withThe number of adults will grow with•• The number of adults will grow with The number of adults will grow with improvements in life expectancyimprovements in life expectancy
•• All providers need to understand the basic All providers need to understand the basic tenets of sickle cell disease management and tenets of sickle cell disease management and incorporate new therapies as they developincorporate new therapies as they developincorporate new therapies as they developincorporate new therapies as they develop

SCC
SC
CNC CN
Colorado Sickle Cell Care NetworkColorado Sickle Cell Care Network